#diy health
Text
DIY Dental Preventative Care
We've prepared a fresh batch of Nano-Silver-Fluoride Cavity Prophylaxis for free distribution. One batch is ~100 x 1ml doses. Offer good until we run out...until we make another batch.
If you'd like one (or more?) email your mailing address to [email protected] (this is an encrypted email, and we delete every request once fulfilled - no storing of your personal info here!) and we will get 1ml (or more?) into the mail for you at no charge!

Nano Silver Fluoride (NSF)
Nano silver particles have the ability to remineralize enamel, in adult and children’s teeth [yes also “baby teeth” aka “milk teeth”] even at a low concentration. It is bactericidal to a wide range of organisms like Streptococcus mutans, Enterococcus faecalis, and Escherichia coli. It has anti-biofilm properties as well.
HOW?
ANTI-BACTERIAL – Silver ions in solution are toxic to bacterial cells, and are especially effective against acid-producing bacteria, like S. mutans, the bug that causes dental caries (cavities), so it mechanically kills the infection already there.
PREVENTS BIOFILM FORMATION – A two-drop treatment lasts about a year, and during that time prevents new bacteria from colonizing the tooth surface, e.g. prophylaxis against new infections. This preventative strategy does not select for a population, so it doesn’t create drug-resistant bacteria! (phew!)
REMINERALIZATION – Nano Silver Fluoride not only
prevents further decay of the dentin, it can actually help to rebuild and recover from damage that has already occured.
So, how do I use this inexpensive, completely safe, super-effective treatment???
CLEAN
This is a critical step as you do not want any particles of trapped food to prevent the solution from making contact with the tooth surface.
To prepare the tooth, first brush your teeth, then floss. Because the solution is itself anti-bacterial, it is not required to rinse with antiseptic mouthwash, or to debride the tooth surface any further.
DRY
Moisture will prevent the Tooth Seal from bonding properly with the tooth. Dry the tooth using cotton balls or paper towels. Place dry cotton balls or paper towels between the cheek and gum to keep the cheek away from the tooth, and to soak up any saliva being produced.
Keep saliva away from the tooth during the process.
APPLY
Two drops placed on a cavity or on a tooth you’d like to protect, creates a concentration of encapsulated silver that adheres to the surface of the tooth and provides protection for about a year. If you use a cotton swab to apply, add one additional drop to account for what gets absorbed by the swab.
The solution should be left in contact with the tooth surface for 2 minutes.
• Do not lick your teeth during that time.
• Don’t eat or drink for 2 hours after application.
If necessary, repeat the process in 10-12 months.
Further reading, including a bibliography, can be found here:
https://fourthievesvinegar.org/tooth-seal/
5 notes
·
View notes
Text
7 Simple Home Remedies for Insomnia
7 Simple Home Remedies for Insomnia
Before diving into the content of 7 Simple Home Remedies for Insomnia, I would like to recommend a book that I believe would be a precious resource The Home Doctor — Practical Medicine for Every Household. This book is a unique companion for the nonprofessional that you can use when help isn’t on the way or to manage common affections that do not bear seeing a croaker
Yes, drug can be expensive in the United States, compared to other advanced countries. The reasons for this include high costs of exploration and development, lack of price regulation, and the fact that the United States doesn’t have a universal healthcare system. This means that cases and insurance companies must pay for the cost of medicines and treatments, which can lead to advanced prices for drug. also, the cost of healthcare in the US is advanced in general, which also contributes to the high cost of drug.
• This book is a great resource for anyone interested in natural and holistic mending styles.
• It covers a wide range of common affections and ails, and provides detailed information on how to treat them using natural remedies and tone- care ways.
• The book is written by educated medical professionals and is backed by scientific exploration.
• The book’s approach is easy to understand and follow, which makes it accessible to people of all periods and backgrounds.
• It’s an excellent companion for those who want to take control of their own health and heartiness.
• The book is also a great resource for those who want to learn further about precautionary care and how to help ails before they do.
It’s a must- read for anyone looking to ameliorate their overall well- being and live a healthier, happier life.
What is Insomnia
Insomnia is a common sleep disorder that affects millions of people worldwide. It is characterized by difficulty falling asleep, staying asleep, or both. Insomnia can be caused by a variety of factors, including stress, anxiety, depression, chronic pain, medication side effects, and poor sleep hygiene. It can lead to a host of negative consequences, including fatigue, irritability, poor concentration, and an increased risk of accidents and illnesses. In this blog post, we will explore 7 simple home remedies that can help alleviate insomnia and improve sleep quality.
Bottom of Form
There are several home remedies for insomnia that you can try. Here are a few:
1. Establish a routine: Go to bed and wake up at the same time every day, even on weekends. This will help regulate your body’s internal clock.
2. Relax before bed: Try to relax your mind and body before bed. This can include activities such as reading, taking a warm bath, or practicing yoga.
3. Avoid stimulating activities: Avoid activities that can keep you awake, such as watching TV or using your phone or computer right before bed.
4. Avoid caffeine, nicotine, and alcohol: These substances can interfere with your ability to fall asleep.
5. Avoid big meals and heavy snacks: Eating too close to bedtime can cause indigestion and discomfort that can keep you awake.
6. Make your bedroom comfortable: Keep your bedroom dark, cool, and quiet. Use comfortable bedding and pillows.
7. Consider herbal remedies: Some herbs such as valerian root, passionflower, and melatonin supplements may help with insomnia.
Herbal teas (such as chamomile or valerian root)
Herbal teas, such as chamomile and valerian root, can be helpful in treating insomnia as they contain compounds that have a calming and sedative effect on the body.
Chamomile tea, for example, is known for its calming properties and is often used as a natural remedy for insomnia, anxiety and stress. It contains compounds called apigenin and luteolin which bind to specific receptors in the brain and promote relaxation.
Valerian root tea, on the other hand, has been used for centuries as a natural remedy for insomnia and anxiety. It contains compounds called valerenic acid and valepotriates which have a sedative effect on the body. These compounds interact with the GABA receptors in the brain which help to promote relaxation and reduce anxiety.
Essential oils (such as lavender or cedarwood)
Essential oils, such as lavender and cedarwood, can be helpful in treating insomnia as they contain compounds that have a calming and sedative effect on the body.
Lavender oil, for example, is known for its calming and relaxing properties and has been traditionally used to help with insomnia, anxiety, and stress. The aroma of lavender oil has been shown to have a calming effect on the nervous system, which can promote relaxation and help improve sleep.
Cedarwood oil is also known for its calming and sedative properties. It contains compounds called sesquiterpenes which have been shown to have a relaxing effect on the nervous system, helping to reduce anxiety and promote sleep.
It’s important to note that essential oils should be used with caution and in low concentrations. Some people may have an allergic reaction to certain oils, so it’s best to do a patch test before using them
Relaxation techniques (such as deep breathing or yoga)
Relaxation techniques, such as deep breathing and yoga, can be helpful in treating insomnia as they can promote relaxation and reduce stress and anxiety.
Deep breathing exercises, for example, can help to slow down the heart rate and lower blood pressure, promoting a state of relaxation. The practice of diaphragmatic breathing, where you focus on breathing deeply into your diaphragm, can help to release tension and promote relaxation.
Yoga is another relaxation technique that can be helpful for insomnia. Yoga combines physical postures, breathing exercises, and meditation to help reduce stress and anxiety. Certain yoga poses, such as legs-up-the-wall pose, can help to relax the body and calm the mind. Yoga also helps to reduce tension and improve sleep.
Relaxation techniques can be incorporated into a bedtime routine to help prepare the body and mind for sleep. It’s best to practice these techniques at least 30 minutes before bedtime and in a quiet, dark, and cool environment.
Dietary changes (such as avoiding caffeine or eating a high-protein snack before bed)
Dietary changes, such as avoiding caffeine or eating a high-protein snack before bed, can be helpful in treating insomnia as they can affect the hormones and neurotransmitters that regulate sleep.
Caffeine, for example, is a stimulant that can disrupt sleep by blocking the action of adenosine, a hormone that regulates sleep. Caffeine can also increase the release of certain neurotransmitters, such as dopamine and norepinephrine, that can make it harder to fall asleep. It’s recommended to avoid consuming caffeine, especially in the evening and before bedtime.
Eating a high-protein snack before bed can also be beneficial for insomnia. Proteins contain the amino acid tryptophan which is converted into serotonin and melatonin, hormones that regulate sleep. Eating a snack that contains both carbohydrates and protein before bed can also help to regulate blood sugar levels, which can improve sleep.
It’s important to note that dietary changes alone may not be enough to cure insomnia, and it may require a combination of lifestyle changes and other treatments.
Creating a bedtime routine
Creating a bedtime routine can be helpful in treating insomnia as it can signal to the body that it is time to wind down and prepare for sleep.
A bedtime routine can include activities such as reading a book, taking a warm bath, or practicing relaxation techniques. These activities can help to relax the body and mind, promoting a sense of calm and reducing stress and anxiety. A consistent bedtime routine can also help to regulate the body’s circadian rhythm, the internal body clock that regulates sleep and wake cycles.
It’s also important to establish a consistent sleep schedule, going to bed and waking up at the same time every day, even on weekends or days off. This can help to regulate the body’s circadian rhythm, making it easier to fall asleep and wake up at the desired times.
It’s recommended to establish a bedtime routine that allows at least 30 minutes to wind down before going to bed and to keep the bedroom environment quiet, dark, and cool.
Bedroom environment (such as keeping it dark and cool)
The bedroom environment can play a big role in the quality of sleep. Keeping the bedroom dark and cool can help to promote better sleep and alleviate insomnia.
Darkness signals to the body that it is time to sleep and triggers the release of melatonin, a hormone that regulates the sleep-wake cycle. A dark room can help to suppress the production of cortisol, a hormone that can keep you awake. Blackout curtains or an eye mask can be used to block out light, while a cool room temperature can help to regulate the body’s core temperature, which can fall as you sleep. A cool room temperature can also help to prevent night sweats and hot flashes, which can disrupt sleep.
It’s recommended to keep the bedroom at a cool temperature, between 60 and 67 degrees Fahrenheit. It’s also important to minimize noise and eliminate any sources of light in the bedroom. A comfortable mattress and pillows can also improve the quality of sleep. It’s always best to consult with a healthcare professional before trying any new remedies, especially if you’re pregnant, nursing, or taking any medications.
Avoiding electronic devices before bed
Avoiding electronic devices before bed can be beneficial in treating insomnia as the blue light emitted by screens can disrupt the body’s natural sleep-wake cycle.
The blue light emitted by electronic devices can suppress the production of melatonin, a hormone that regulates the sleep-wake cycle. This can make it more difficult to fall asleep and stay asleep. Additionally, the content on electronic devices can be stimulating and can keep the mind active, making it harder to relax and fall asleep.
It’s recommended to avoid using electronic devices for at least 30 minutes to an hour before bed. Instead, engage in activities that promote relaxation, such as reading a book, taking a warm bath, or practicing relaxation techniques.
If you must use electronic devices before bed, consider using a blue light filter or adjusting the device’s settings to reduce the amount of blue light emitted. It’s also a good idea to keep electronic devices out of the bedroom to create a designated sleep space. It’s always best to consult with a healthcare professional before trying any new remedies, especially if you’re pregnant, nursing, or taking any medications.
“I highly recommend “The Home Doctor — Practical Medicine for Every Household” to anyone looking for practical and effective ways to take charge of their health and well-being. This book is a valuable resource for anyone looking to learn more about home remedies and natural healing techniques.”
#home remedies#insomnia#natural healing#herbal medicine#diy health#alternative medicine#home treatment#self-care#holistic health#wellness#kitchen medicine
1 note
·
View note
Text
#80s#80s aesthetic#90s#90s aesthetic#art#autos#design#diy#health & fitness#clothes#60s aesthetic#60s music#60s#70s aesthetic#70s music#70s#70s fashion#80s fashion#80s horror#90s runway#90s fashion#early 2000s#retro aesthetic#retro
580 notes
·
View notes
Text
We've all seen a feelings wheel, but have you ever seen a NEEDS wheel?
This was a first for me when my therapist showed it to me—so now I'm sharing it with you.
Like!!
I'm allowed to need "Make"?
And "For"?!
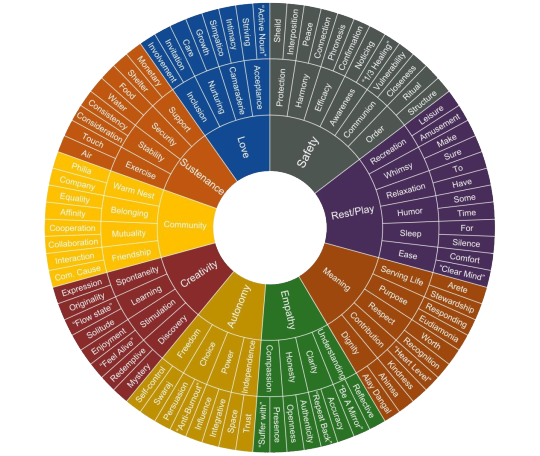
All jokes aside, this thing is changing the way I view my needs.
I hope it changes yours, too.
#needs wheel#feelings wheel#feelings chart#therapy#mental health#mental illness#actually adhd#neurodivergence#neurodivergencies#actually audhd#actually autistic#autism#audhd#autistic#mental health help#help yourself#diy therapy#THAT'S A JOKE
323 notes
·
View notes
Text
This sounds like BS or at the very least the placebo effect, but it was very much a cool thing that happened.
My wife has COVID and with it shortness of breath. We didn't have any albuterol, but we did have another idea!
Knowing that theobromine had been studied as a bronchodilator and found as effective as theophylline, and knowing that cocoa has a lot of theobromine in it, I set out to make a mean cup of bronchodilating hot chocolate.
So the effective dose of theobromine is 10mg/kg, which for my wife is about 900mg. Since cocoa has about 20mg/g of theobromine, about 45g (about 1/2 cup) would do it. We used about 1/3 cup and it... worked amazingly well.
Like so well my wife said it was the best she had ever felt lung-wise. Like, we're thinking she might have asthma because her shortness of breath is better right now with COVID + Chocolate than it is on a totally normal day without COVID.
Definitely talk to your doctor if you're having shortness of breath and don't know why, but if you just wanna make a mean cup of bronchodilating hot chocolate for kicks, the recipe is below:
1 cup water
1/3 cup cocoa powder (or if you want to get really precise, the number of Kg of body weight divided by 2 equals the number of grams of cocoa)
1-2 tablespoon sugar (to taste)
Put the cocoa and sugar in a mug and add about a quarter cup of the water to it and stir into a paste. Add the rest of the water and stir until liquid. Heat in a microwave or on the stove to desired temperature.
Enjoy!
Its not, like, the tastiest hot chocolate ever, but it's not horrible.
205 notes
·
View notes
Text
Feeling better today ❣️💋

#succession#aesthetic#ryan gosling#margot robbie#diy#funny#food#rwby#fashion#health & fitness#cutie w a bootie#beautiful#america#perfect butt#natural body#beuty girl
56 notes
·
View notes
Text

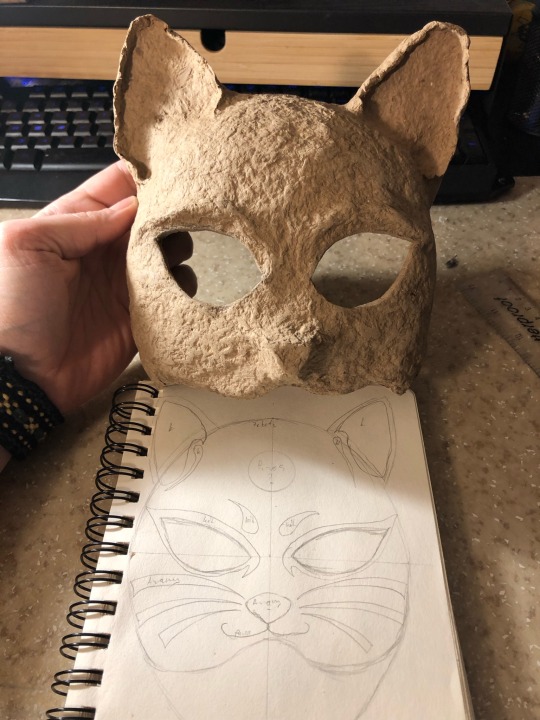
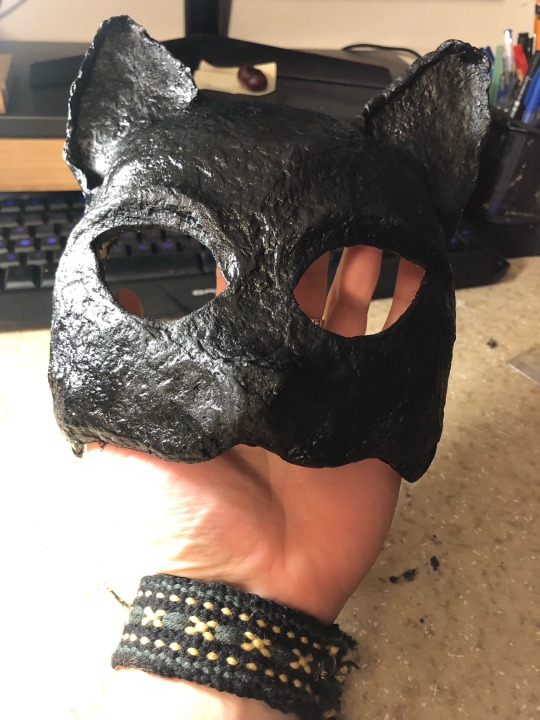




This is the third mask I made this winter (of the second one I did not take pictures).
This is a neko half-mask I made for a friend. It’s got little bells on it :).
I used papier mache for the mask. I painted it with acrylic paint. For the band I used a japanese technique called kumihimo with super soft merino wool strings.
It’s quite comfy, although it smells of acrylic paint.
This week was an emotional roller coaster for me with awesome highs and some significant lows with plenty of confusion inbetween so it was nice to relax and finish this mask while binging the og Avatar the last airbender. :)
#diy craft#crafting#crafts#neko#mask#japanese#inspiration#relax#gift#art#handmade#kézműves#mental health#cat#macska
57 notes
·
View notes
Text
When I start Testosterone I kept hearing that a side effect of it was having a harder time crying, and although I believe that was true for the boys and men who told me this, it has been the opposite for me.
I cry easier now than I had since I was a little kid. I get emotional easily at emotionally charged things. Happy, sad, inspirational, rage inducing, I feel so much and cry freely a lot.
And I'm happy, I'm so happy I'm feeling things again. I want to feel every emotion so deeply. I want to cry for those who aren't here today and I want to cry to in joy for those becoming themselves. I want to feel angry and inspired and sad and happy, because to feel at all means I am here and I'm connecting.
#testosterone#t#hrt#diy hrt#trans#transgender#gay#queer#mental health#transition#lgbt#bi#lesbian#pan#enby#nonbinary#trans man#trans woman#trans fem#trans masc#genderfluid
90 notes
·
View notes
Text
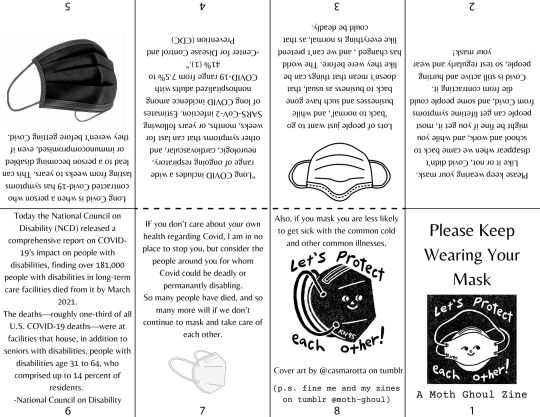
i also posted this in a reblog of the post where i found the cover art- go check them out, @casmarotta
please wear your mask. if you go indoors with other people, wear a mask. people are still dying
#moth's zines#moth ghoul#moth types#zines#zine#diy#punk#diy zine#punk zine#caring is punk rock#covid#long covid#pandemic#covid 19#public health#covid isn't over
84 notes
·
View notes
Text

not enough people talk about the intersections between chronic illness/disability and eating disorders. when i was hospitalized for anorexia i was told all the time “a perfect body is one that works!” but mine didn’t. treatment didn’t account for people like me, but when i thought about it it made total sense. of course you’re more likely to develop a negative relationship with your body when you’re constantly in pain. of course it’s harder to recover when sickness is an important part of your identity. having an invisible disability made me desperately want to be seen as “sick.” now, i can recognize all of these as red flags that i was vulnerable to disordered eating, coupled with preexisting negative feelings surrounding food due to autism. eating disorder treatment programs are hell for an autistic person: forcing you to eat in a neurotypical way, refusing you safe foods and rituals, making you go entirely outside your comfort zone. mental health professionals need to be aware of these risk factors so they can treat disabled people properly.
#punk patches#punk#riotgrrrl#diy#patches#disability#chronic illness#cripple punk#crip punk#recovery#mental health#actually autistic
371 notes
·
View notes
Text
Why Dentistry Is Separate From Medicine
The divide sometimes has devastating consequences.
By Julie Beck

Doctors are doctors, and dentists are dentists, and never the twain shall meet. Whether you have health insurance is one thing, whether you have dental insurance is another. Your doctor doesn’t ask you if you’re flossing, and your dentist doesn’t ask you if you’re exercising. In America, we treat the mouth separately from the rest of the body, a bizarre situation that Mary Otto explores in her new book, Teeth: The Story of Beauty, Inequality, and the Struggle for Oral Health in America.
Specializing in one part of the body isn’t what’s weird—it would be one thing if dentists were like dermatologists or cardiologists. The weird thing is that oral care is divorced from medicine’s education system, physician networks, medical records, and payment systems, so that a dentist is not just a special kind of doctor, but another profession entirely.
But the body didn’t sign on for this arrangement, and teeth don’t know that they’re supposed to keep their problems confined to the mouth. This separation leads to real consequences: Dental insurance is often even harder to get than health insurance (which is not known for being a cakewalk), and dental problems left untreated worsen, and sometimes kill. Anchoring Otto’s book is the story of Deamonte Driver, a 12-year-old boy from Maryland who died from an untreated tooth infection that spread to his brain. His family did not have dental benefits, and he ended up being rushed to the hospital for emergency brain surgery, which wasn’t enough to save him.
I spoke with Otto about how the dentistry/medicine divide came to be, why it’s stuck around, and what its consequences have been. A lightly edited and condensed transcript of our conversation is below.
Julie Beck: Let’s go back to the origin of how dentistry and medicine became separate in the first place. It’s something we take for granted now, right? But it’s actually really weird. Was there ever a time when dental care was integrated with medical care?
Mary Otto: It stayed generally separate. Taking care of the teeth became kind of a trade. In the barber-surgeon days, dentist skills were among one of the many personal services that barber surgeons provided, like leeching and cupping and tooth extractions. They approached it as a mechanical challenge, to repair and extract teeth. Barber surgery was practiced in the very early part of our country's history. And Paul Revere was a denturist—he was a jeweler and he made dentures too.
But the dental profession really became a profession in 1840 in Baltimore. That was when the first dental college in the world was opened, I found out, and that was thanks to the efforts of a couple of dentists who were kind of self-trained. Their names were Chapin Harris and Horace Hayden. They approached the physicians at the college of medicine at the University of Maryland in Baltimore with the idea of adding dental instruction to the medical course there, because they really believed that dentistry was more than a mechanical challenge, that it deserved status as a profession, and a course of study, and licensing, and peer-reviewed scientific consideration. But the physicians, the story goes, rejected their proposal and said the subject of dentistry was of little consequence.
That event is remembered as the “historic rebuff.” It's still talked about sometimes, not a lot, but it’s seen as a symbolic event and it’s continued to define the relationships between medical and dental education and medical and dental healthcare systems in funny ways. Dentists still drill and fill teeth and physicians still look at the body from the tonsils south. Medical and dental education is still provided separately almost everywhere in this country and our two systems have grown up to provide care separately, too.
Beck: It seems like since the historic rebuff, dentists have really wanted to stay separate. Why is that, do you think?
Otto: People have raised questions about the system over the years, and they’ve called for reforms periodically. Nearly a century ago, in the 1920s, this biological chemist named William Gies was a kind of prophet. He visited every dental school in the country and in Canada for the Carnegie Foundation, for this big report, and he called for dentistry to be considered an essential part of the healthcare system. He said: “Dentistry can no longer be accepted as mere tooth technology.” He wanted oral health and overall health to be integrated into the same system, but organized dentistry fought to keep dental schools separate. [Dentists] emerged as defenders of the professional autonomy and professional independence of the private practice system that we have here. David Satcher, the [former] surgeon general, he kind of said the same thing when he issued this “Oral Health in America” report in 2000. He said we must recognize that oral health and general health are inseparable. And that too, was a kind of challenge. And it seems like things are changing, but very slowly.
Beck: So you think the reason they wanted to stay separate was really just a matter of professional independence?
Otto: Yeah. It’s a marketplace issue. It’s a formidable thing, professional autonomy.
Beck: It’s interesting to hear this separation traced back to one moment because it has shaped so many things—insurance, access to care, all these things. Can you give an overview of what the effects have been of carving dentistry out of medicine?
Otto: One of the most dramatic examples is that more than a million people a year go to emergency rooms with dental problems. Not like they’ve had a car accident, but like a toothache or some kind of problem you could treat in a dental office. It costs the system more than a billion dollars a year for these visits. And the patients very seldom get the kind of dental care they need for their underlying dental problems because dentists don’t work in emergency rooms very often. The patient gets maybe a prescription for an antibiotic and a pain medicine and is told to go visit his or her dentist. But a lot of these patients don’t have dentists. So there’s this dramatic reminder here that your oral health is part of your overall health, that drives you to the emergency room but you get to this gap where there’s no care.
There’s also the fact that our medical records and our dental records are kept separately. Dentistry has treatment codes, but it doesn’t really have a commonly accepted diagnostic code language which makes it hard to integrate medical and dental records and harder to do research on the commonalities between oral health and overall health.
One dental researcher said at a meeting I was at, “Back in the days of the bubonic plague, medicine captured why people die. We don’t capture why teeth die.” There’s this gap in the way we understand oral diseases and the way we approach tooth decay. We still approach it like it’s a surgical problem that needs to be fixed, rather than a disease that needs to be prevented and treated. And we see tooth decay through a moral lens, almost. We judge people who have oral disease as moral failures, rather than people who are suffering from a disease.
Beck: Insurance is all separated out as well, and a lot of times it’s optional. How, politically, did dental care come to be seen as optional?
Otto: There were discussions all through the 20th century, periodically, about this subject. Organized dentistry, like organized medicine, fought nationalized health care on a lot of fronts and testified against the practicality of extending benefits to everyone in the country. And all the healthcare programs that we’ve come up with as a nation have on some level or another left oral health out, or given it sort of an auxiliary status as a fringe benefit. Private insurance has also treated it that way.
Beck: It’s interesting, on one hand, dental care is treated as “optional,” but on the other hand, as you note in the book, there’s this social pressure to have perfect teeth, especially in America, especially among the rich. And so there’s a lot of money to be made in cosmetic dentistry. Do you think that social pressure to have perfect teeth is kind of exacerbating the inequality?
Otto: I think on some level it must. We do put so much emphasis on perfect smiles and there is a lot of money to be made in that field. One dentist I talked to as I was working on this project said “Nobody wants to do the low-end stuff anymore.” Of course there is a lot more money to be made with some of these really high-end procedures. But on the other hand there’s this vast need for just basic basic care. A third of the country faces barriers in getting just the most routine preventive and restorative procedures that can keep people healthy.“There’s this kind of feast and famine aspect to dental care that’s striking.”
Beck: I wonder if the value put on that perfect Hollywood smile is in part because so many people don’t have access to dental care, so perfect teeth are a very clear way of signaling your wealth. More clear than if everyone had access to good care and had decent teeth.
Otto: It could be. It’s very interesting. This whole “perfect American smile” did have its origins in Depression-era Hollywood. Filmed movies were still pretty new at that point. There was this young dentist named Charles Pincus who had this dental office that opened on Hollywood and Vine and he went to the movies too. And he saw these movie actors who didn’t have perfect teeth up on the silver screen, like James Dean, who actually grew up on a farm and had dentures, and Judy Garland, and Shirley Temple. He started working with the studios. He created these little snap-on veneers for Shirley Temple so we never saw her lose her baby teeth. Over all the years she had a perfect little set of pearly whites.
But you’re right, there’s this kind of feast and famine aspect to this that’s striking. They call the [top] front six teeth “The Social Six,” and the perfect set of veneers for these front six teeth are not just a status symbol here in this country—they’re sought around the world as a marker of success.
Beck: I guess partially because of this market for cosmetic dentistry, dentists tend to cluster in rich areas, and there are often shortages in rural areas or poorer areas. But at the same time, you write about a lot of instances where dentists were really resistant to allowing anyone else to provide that preventive care, like training hygienists to do cleanings in schools. Why is that so controversial?
Otto: There’s been a long history of that and it really came home to me with some of the stories I heard, like the story of Tammi Byrd, this dental hygienist in South Carolina. There’s about a quarter million children living in the rural areas of the state who weren’t getting care, and she and some other dental hygienists fought to get the law changed so they could go out and see children without being first examined by a dentist. The dental association just fought back, they got an emergency regulation passed to stop her from doing her work and finally the Federal Trade Commission came in and took her case and won it for her, in the interest of getting economical preventive care to all these children who lacked it.
But, yeah, there’s this marketplace issue. Private organized dentistry protects the marketplace for care and the power of private practitioners to provide it but that leaves a lot of people out. Stories like the battle of this dental hygienist in South Carolina, or the battle that’s going on over these midlevel providers called dental therapists in a number of states, really illustrate how fiercely that terrain is protected.
Organized dentistry continues to say the current supply of dentists can meet the need, that if the system paid more for the care, more providers would locate in these poorer areas. That we Americans need to value our care more and go out and find care more aggressively. They see the fault as being with society at large.
Beck: This opposition to hygienists stepping up and filling that role, does that have anything to do with the fact that hygienists are mostly women? You quoted some old-timey dentists who were like, “Ah yes, the best assistant for a dentist is a woman because she won’t be ambitious and take over our patients." And it kind of sounds like that attitude is still around in some ways.
Otto: You could say that there might be a sense of that still. There’s certainly a deep sense among the powers of organized dentistry that only dentists are qualified to do the lion’s share of dentistry.
Beck: Are there other plans proposed to fill the gap in dental care, if not letting the hygienists or the dental therapists do it? Is there another plan that would be more pleasing to dentists?
Otto: They have their own alternative model. It's kind of a health navigator who connects people with existing dentists, a community-health-worker type of model. [The navigator] helps divert people from ERs into existing dental offices, helps people make dental appointments, educates them about maintaining oral health, and taking care of their children. But it’s guiding people to existing dentists, rather than expanding the dental workforce.
Beck: And if they don’t have insurance then it’s not going to help very much?
Otto: It’s not as helpful. Unless there’s a philanthropy or some kind of group that’s raising money to pay for the care.
Beck: The separation between dental and medical care is pretty entrenched at this point. Do you think it can be overcome, that it should be overcome, that the two could be integrated a little more? What might that look like, do you think it would help?
Otto: Something that was talked about in the medical world during the work going into the Patient Protection and Affordable Care Act was the “Triple Aim”: bending the cost curve toward prevention, expanding care more broadly and more cheaply, and [creating] a better quality of care. It’s something that needs to be discussed in the oral health world too, and I think it’s being discussed more.
Beck: Do you think it would be like a parallel reform in dentistry or would it be more integrating them back together somewhat?
Otto: It seems like it’s going to have to involve both. There’s been work being done in this area, there’ve been efforts to put dental hygienists into these federally qualified health centers that are part of our public-health safety net, which serve poor rural communities. It seems like it’s capturing an increasing amount of attention from state lawmakers, governors, and public health officials who are interested in bringing costs down for all kinds of health care and seeing that these things show promise. They're saying we’re spending too much on emergency rooms, we're spending too much on hospitalization for these preventable problems, so there are cost incentives to get more preventive and timely routine restorative care to people.
Beck: Trying to undo some of the damage of the historic rebuff.
Otto: Yeah, isn’t it funny?
this is from The Atlantic...interview is from like seven years ago, though, so no guilt about bringing it out from the paywall.
0 notes
Text
#funny#lol#haha#humor#meme#memes#art#draw#drawing#artists on tumblr#landscape#paradise#nature#adventure#introverts#mental health#asmr#spirograph#satisfying#spiroart#spirography#diy#relaxing
21 notes
·
View notes
Text
free dance only now ;)
enjoy more if you subscribe to my FREE page😘
#aesthetic#animals#anime and manga#architecture#art#autos#beauty#black stories#books & libraries#business#celebrities#comics#computer science#design#DIY#education#fashion#food#funny#health & fitness#history#home & lifestyle#illustration#kpop#movies#museums#music#nature#nonprofit#photography
35 notes
·
View notes
Text

#80s#80s aesthetic#90s#90s aesthetic#art#autos#design#diy#health & fitness#clothes#70s film#70s music#70s fashion#that 70s show#70s#80s horror#80s retro#80s movies#80s music#90s movies#90s horror#90s cartoons#80s interior#90s music#90s supermodels#90s fashion#80s alternative#90s alternative
455 notes
·
View notes
Text

21 notes
·
View notes
Text
Recipes
Recently my wife and I have been offering our cooking/recipe creation skills on reddit to anyone who has a very limited diet due to food allergies/intolerances/MCAS, GI issues, or any other problem that limits a diet to very few foods.
If you're someone who might benefit from this, send your safe foods to our inbox and we'll post a couple recipes!
You can absolutely do this on anon if you are more comfortable. I can also make meal shake or tube feed recipes.
Note that we are not nutritionists, we just like a good challenge and helping people eat their best.
75 notes
·
View notes
Last Seen Blogs

icecoolmountain
IceCool Mountain Art Studio

mega-pussy-bushes
Mega Hairy Pussy Bushes

estamosseparados-blog
Separa2

everysoorphan
Orphan's Progress Report

newsbydkoding
Dkoding Official