#history taking
Text
Explained - History taking
History taking and differential diagnoses
During your secondary assessment, you will begin establishing a patient history. There are two acronyms to help you remember the information to obtain: SAMPLE and OPQRST. SAMPLE questions are focused towards establishing your patient’s medical history and events leading up to the emergency at hand. OPQRST questions are focused on your patient’s current signs, symptoms, and pain level. These questions can help you begin to form a differential diagnosis regarding your patient’s current condition. A differential diagnosis is a working hypothesis of the nature of the current problem. (AMLS, NAEMT.)
SAMPLE will be used in both medical and trauma scenarios, whereas OPQRST only applies to medical scenarios.
SAMPLE
S: Signs and symptoms. Signs are objective- they are what you can see. Symptoms are subjective- they are what your patient is feeling. For example, you arrive on scene for an abdominal pain emergency. Your patient is in the fetal position (a sign) and states that they are having extreme lower abdominal pain (a symptom.)
A: Allergies. Establish if your patient has any medication or environmental allergies. Be sure to ask your patient what occurs when they encounter their specific allergens- do they go into anaphylaxis or is it a simple allergic reaction? Allergy information will help you add to your differential diagnosis. For example, you are tending to a patient with a history of asthma and seasonal allergies. It is the springtime, and your patient has been working outside in their garden for several hours and is now experiencing shortness of breath with wheezing. One could reasonably assume the cause of the current distress is an asthma attack due to prolonged allergen exposure.
M: Medications. Establish what medications your patient currently takes. As well as asking what the patient takes, you will need to know whether they take their medications when they should. This is called medication compliance. You will also need to establish if any of their medications have been recently prescribed, as a new medication may cause unfamiliar side effects for the patient. If you don’t know what a certain medication is, ask the patient what they take it for.
P: Pertinent medical history. Establish your patient’s medical history that could potentially relate to the problem at hand. For example, if your patient is currently experiencing chest pain, it is pertinent to ask about any cardiac or respiratory history. As well, if your patient is experiencing altered mental status, it is pertinent to ask about a history of diabetes, stroke, or behavioral issues. It would not, however, be pertinent to ask about any behavioral issues with a patient experiencing chest pain. It is also pertinent to ask about any recent hospital stays or surgeries.
L: Last oral intake. This refers to the last thing the patient ingested. This includes food, drink, drugs, alcohol, and prescription medications. It is always pertinent to ask when the patient last ate, and whether they have been keeping hydrated. This is especially important for patients experiencing a diabetic crisis. With patients who have recently ingested drugs or alcohol, it is important to ask what, when, and the amount of drugs or alcohol ingested.
E: Events leading up. Establish the conditions in which the patient was in when their current problem began. For example, before the patient began experiencing chest pain, were they exerting themselves? Before having a seizure, was the patient exposed to any bright, flashing lights? You are attempting to establish the potential causes of the patient’s current problem.
OPQRST
O: Onset. Ask your patient when their current symptoms began. What were the conditions surrounding the beginning of this issue? Did it come on suddenly or gradually?
P: Provocation / Palliation. Does anything make the problem worse? (Provocation.) Does anything help to alleviate symptoms of the problem? (Palliation.) These could refer to body positions, medications, activities, temperature therapy, etc. For example, some patients with respiratory difficulties may find it difficult to exert themselves (provocation) and may find leaning forward in a tripod position helps them to breathe more effectively (palliation.)
Q: Quality. Ask the patient to describe to you how their pain feels. Some frequently used descriptors include sharp, dull, stabbing, burning, crushing, throbbing, nauseating, shooting, twisting, and stretching. Remember to ask this as an open-ended question. Document how the patient describes their pain in quotation marks. For example, if your patient is experiencing chest pain, ask, “What does the pain in your chest feel like?” If your patient says, “It feels like something is crushing the center of my chest,” you would document the patient’s quality of pain as “feeling like something is crushing the center of [their] chest.”
R: Radiation. This refers to the localization or distribution of the patient’s pain. In the example above, your patient states that they have crushing pain in the center of their chest. It is pertinent to ask whether the pain stays localized to the center of their chest, or if it moves (radiates) to a different location. Remember that some conditions cause referred pain to another part of the body. This is when the pain is perceived in a location other than the site of the painful stimulus/origin. For example, the spleen is in the upper left side of the abdomen, next to the stomach and behind the left ribs. However, pain from a ruptured spleen can be felt in the left shoulder (Kehr’s sign.)
S: Severity. Ask your patient to rate the pain on a scale of 1-10. A rating of 1 would be minimal pain that is hardly noticeable, whereas a 10 would be pain that is so severe the patient is unable to move; the worst pain they have ever felt in their life. This scale can also be applied to breathing difficulties. A rating of 1 would indicate mild breathing difficulty, whereas a 10 would indicate severe, life-threatening breathing difficulty. To assess a pediatric patient’s pain level, use the Wong-Baker Faces Pain Rating Scale.
T: Time. Establish a timeline of your patient’s current problem, beginning at the onset of their symptoms to when they called 911, then from when they called 911 to your arrival on scene. Determine if they called 911 at the start of their symptoms, or if they called 911 when their symptoms began getting progressively worse/did not improve after a reasonably expected amount of time. Ask your patient whether they have had or were hospitalized for this problem before, and how this current instance compares to the previous.
Clarifying questions: Clarifying questions are questions not listed in your OPQRST or SAMPLE that you feel could be beneficial for your patient care and documentation, or potentially add to your differential diagnosis.
*Remember to ask these questions in plain language and avoid using medical terminology.*
4 notes
·
View notes
Text
academic bias is so funny because you’ll be reading about the same historical event and one person is like “Despite the troubles that befell his homeland and near constant criticism of the court King Blorbo remained strong in the face of adversity” and the other one is like “after letting his people carry the brunt of his cringefail decisions Blorbo the Shitface refused to listen to any reason and continued to be a warmongering piece of shit. Also he was ugly.”
#historians are out there beefing with ppl who died over 200 years ago. good for them#history#history memes#this isn’t really about anyone in particular#but I did read the most hilariously bitter takes on alexander I#not that it’s hard to poke fun at his vanity and indicisive nature but like. he was just a poor little meow meow#although I have some weird grudges against dead ppl as well *cough* Catherine II *cough*
26K notes
·
View notes
Text
Pediatric history taking
A) Patient details
Name
Age (dob)
Sex
Address
Date of admission
B) Presenting complains
C) History of presenting illness
D) Birth history
Antenatal
Natal
Postnatal
E) Feeding history
F) Immunization history
G) Developmental history
H) Past history
#There's so many subheadings#I'd rather do this on paper tomorrow#So much I missed#Anyway hopefully I'll remember this tomorrow for a test that MIGHT happen#student#study space#study notes#med school#History taking#academia
1 note
·
View note
Text
Assessments explained - History taking
History taking and differential diagnoses
During your secondary assessment, you will begin establishing a patient history. There are two acronyms to help you remember the information to obtain: SAMPLE and OPQRST. SAMPLE questions are focused towards establishing your patient’s medical history and events leading up to the emergency at hand. OPQRST questions are focused on your patient’s current signs, symptoms, and pain level. These questions can help you begin to form a differential diagnosis regarding your patient’s current condition. A differential diagnosis is a working hypothesis of the nature of the current problem. (AMLS, NAEMT.)
SAMPLE will be used in both medical and trauma scenarios, whereas OPQRST only applies to medical scenarios.
SAMPLE
S: Signs and symptoms. Signs are objective- they are what you can see. Symptoms are subjective- they are what your patient is feeling. For example, you arrive on scene for an abdominal pain emergency. Your patient is in the fetal position (a sign) and states that they are having extreme lower abdominal pain (a symptom.)
A: Allergies. Establish if your patient has any medication or environmental allergies. Be sure to ask your patient what occurs when they encounter their specific allergens- do they go into anaphylaxis or is it a simple allergic reaction? Allergy information will help you add to your differential diagnosis. For example, you are tending to a patient with a history of asthma and seasonal allergies. It is the springtime, and your patient has been working outside in their garden for several hours and is now experiencing shortness of breath with wheezing. One could reasonably assume the cause of the current distress is an asthma attack due to prolonged allergen exposure.
M: Medications. Establish what medications your patient currently takes. As well as asking what the patient takes, you will need to know whether they take their medications when they should. This is called medication compliance. You will also need to establish if any of their medications have been recently prescribed, as a new medication may cause unfamiliar side effects for the patient. If you don’t know what a certain medication is, ask the patient what they take it for.
P: Pertinent medical history. Establish your patient’s medical history that could potentially relate to the problem at hand. For example, if your patient is currently experiencing chest pain, it is pertinent to ask about any cardiac or respiratory history. As well, if your patient is experiencing altered mental status, it is pertinent to ask about a history of diabetes, stroke, or behavioral issues. It would not, however, be pertinent to ask about any behavioral issues with a patient experiencing chest pain. It is also pertinent to ask about any recent hospital stays or surgeries.
L: Last oral intake. This refers to the last thing the patient ingested. This includes food, drink, drugs, alcohol, and prescription medications. It is always pertinent to ask when the patient last ate, and whether they have been keeping hydrated. This is especially important for patients experiencing a diabetic crisis. With patients who have recently ingested drugs or alcohol, it is important to ask what, when, and the amount of drugs or alcohol ingested.
E: Events leading up. Establish the conditions in which the patient was in when their current problem began. For example, before the patient began experiencing chest pain, were they exerting themselves? Before having a seizure, was the patient exposed to any bright, flashing lights? You are attempting to establish the potential causes of the patient’s current problem.
OPQRST
O: Onset. Ask your patient when their current symptoms began. What were the conditions surrounding the beginning of this issue? Did it come on suddenly or gradually?
P: Provocation / Palliation. Does anything make the problem worse? (Provocation.) Does anything help to alleviate symptoms of the problem? (Palliation.) These could refer to body positions, medications, activities, temperature therapy, etc. For example, some patients with respiratory difficulties may find it difficult to exert themselves (provocation) and may find leaning forward in a tripod position helps them to breathe more effectively (palliation.)
Q: Quality. Ask the patient to describe to you how their pain feels. Some frequently used descriptors include sharp, dull, stabbing, burning, crushing, throbbing, nauseating, shooting, twisting, and stretching. Remember to ask this as an open-ended question. Document how the patient describes their pain in quotation marks. For example, if your patient is experiencing chest pain, ask, “What does the pain in your chest feel like?” If your patient says, “It feels like something is crushing the center of my chest,” you would document the patient’s quality of pain as “feeling like something is crushing the center of [their] chest.”
R: Radiation. This refers to the localization or distribution of the patient’s pain. In the example above, your patient states that they have crushing pain in the center of their chest. It is pertinent to ask whether the pain stays localized to the center of their chest, or if it moves (radiates) to a different location. Remember that some conditions cause referred pain to another part of the body. This is when the pain is perceived in a location other than the site of the painful stimulus/origin. For example, the spleen is in the upper left side of the abdomen, next to the stomach and behind the left ribs. However, pain from a ruptured spleen can be felt in the left shoulder (Kehr’s sign.)
S: Severity. Ask your patient to rate the pain on ascale of 1-10. A rating of 1 would be minimal pain that is hardly noticeable, whereas a 10 would be pain that is so severe the patient is unable to move; the worst pain they have ever felt in their life. This scale can also be applied to breathing difficulties. A rating of 1 would indicate mild breathing difficulty, whereas a 10 would indicate severe, life-threatening breathing difficulty. To assess a pediatric patient’s pain level, use the Wong-Baker Faces Pain Rating Scale.
T: Time. Establish a timeline of your patient’s current problem, beginning at the onset of their symptoms to when they called 911, then from when they called 911 to your arrival on scene. Determine if they called 911 at the start of their symptoms, or if they called 911 when their symptoms began getting progressively worse/did not improve after a reasonably expected amount of time. Ask your patient whether they have had or were hospitalized for this problem before, and how this current instance compares to the previous.
Clarifying questions: Clarifying questions are questions not listed in your OPQRST or SAMPLE that you feel could be beneficial for your patient care and documentation, or potentially add to your differential diagnosis.
*Remember to ask these questions in plain language and avoid using medical terminology.*
0 notes
Text
There's a version of the "don't go grocery shopping while hungry" rule specifically for writers where you should never under any circumstances be allowed to touch your draft within 3 hours of reading a really good story. Because sometimes when you read something great your head goes "fuck this is so much better than my stuff I should make that more like THIS instead!" Look at me. That's the devil talking and you should close the document NOW.
#you will make superficial edits that do not gell well with the rest of your work#and won't actually capture what you thought was so good about that story#close the doc. sit down. think about it for a while. inspiration is fine. getting a 'eureka' moment from another story is fine#but if you find yourself comparing your work one to one with someone else's and taking any differences to be flaws on your part then STOP#you will never write good stuff by trying to make it look less like you wrote it#writing#writing advice#guess who just had to go into her google doc history and undo a bunch of panic-induced edits#because she read a fic about the same characters she's writing for?#meeee. they aged badly within just a few hours of hindsight. learn from my mistakes#self-hatred is not a good motivation for creation#fic writing
9K notes
·
View notes
Text
Y'all, saying that cartomancy is a "closed Romani practice" is like saying money lending is a "closed Jewish practice." Cartomancy was a practice that Romani people were forced into due to discrimination.
Ettellia said he learned tarot from Romani people who brought tarot from Egypt. He was lying to make tarot sound more exotic. Europe was in the middle of egyptomania. There is literally no historical evidence that this supposed origin is even slightly true. Europe has had cartomancy since the Roman Empire.
Around the time that tarot divination was being invented, tarocci decks were fairly new. If there was a "traditional romani cartomancy" method, (which even Romani oral histories do not support) it almost definitely would have been based on the massively more popular Belgian-Genoese pattern deck, not the tarocci deck.
#please stop taking the golden dawn at their word when it comes to esoteric history#they are not a reliable source#sometimes i feel like some of y'all dont actually give a fuck about romani history its just words to you
9K notes
·
View notes
Text
going through my old journals as part of therapy homework and i'm reading a section written in the emotional wreckage of a full-on breakdown when i get hit with this line:
There is never a satisfying answer to ‘Why didn’t they love me?’
like wow babe. good fucking point
#like you were on the ground biting the carpet and dry sobbing while you wrote that and still. good fucking point#not a shitpost#cptsd#and it's true. there's never a satisfying answer#the truth is i know why i wasn't loved#i analyzed my parent's traumas and abuse to death. i understand why i alienated and was alienated from my siblings#i know why my mom was too overwhelmed to be capable of nurturing#i know why my dad vanished into addiction and avoidance#the details of our cycles of trauma and cptsd and family history i have a phd in all of it#i understood perfectly. i spent years studying and now i knew the answer#and guess what? IT WAS NOT SATISFYING!!!#because they still didn't love me! and i still couldn't change that!#it was still a completely unsatisfying state of affairs!#so like. when the people who are supposed to love you...don't.#when the people who are supposed to take care of you...fail to#you can look for answers and reasons and explanations#but that's not actually going to FIX your situation.#and it's probably not within your ability TO fix the situation. (and definitely not your job)#because you don't need answers--you need a new situation#*inserts Just Walk Out. You Can Leave!!! (Running Skeleton) Meme*#and yes. walking out isn't always possible.#but for you i hope it will be one day soon. and i hope you build the courage to take that leap.#stepping away from the people who failed to love you...it feels like being untethered but also like being lighter than air#new and scary. immensely relieving. the future opens up. empty but empty like a canvas. blindingly bright until your eyes adjust#like climbing out of a pit you called home and for the first time realizing how bright the light of day can truly be#when you aren't just getting glimpses from the bottom of a hole
9K notes
·
View notes
Text
GUYS THEYRE MAKING AN OFFICIAL CROSSOVER COMIC. THIS IS NOT A FUCKING DRILL.

ISSUE 13 OF SATURDAY MORNING ADVENTURES DROPPING IN JUNE.
updates below the cut —>
UPDATE #1:
Hiya! since this is blowing up just thought i’d stick this on here. I got this info from a YT community post from teddygamingreview, a smaller channel knee deep in the comics side of the tmnt franchise that i’ve been following for a while. From what i understand this is just teaser/promo material so there’s not a whole lot of other info out yet. Thats all, cowa-fuckin-bunga dudes
UPDATE #2:
TEDDYGAMING REVIEWS CAME IN CLUTCH ONCE AGAIN WITH A BREAKDOWN VIDEO
(Most important new info takeaway that wasn’t already laid out in the previous post, in case you don’t got time to watch right now: the issue after this has some villains from the 2012 series on the cover art, implying that whatever multiverse crossover shenanigans are going on might bleed into he next issue, at least to some extent?)
youtube
UPDATE #3:
THIS ONES TOO BIG SO I MADE A SEPARATE POST FOR IT, LINK HERE:
#source: teddygamingreview#HOLY FUCKING SHIT#THIS IS A MOMENT IN HISTORY#TAKE A PICTURE#tmnt#tmnt 2003#2k3 tmnt#tmnt 2012#tmnt idw#mirage tmnt#tmnt 1987#rottmnt#rise of the teenage mutant ninja turtles#teenage mutant ninja turtles#tmnt crossover#thoughts from the pit#Youtube
6K notes
·
View notes
Text





IT WAS ERIC AFTER ALL!!!! I'm so glad we got to meet him (before Vil snaps him away with those Infinity Gauntlets) (can't wait to see what happens when we get the matching Infinity Tiara to go with them, there will be no survivors)
(sorry to be so slow/rough lately, just got a lot of stuff on the ol' brain at the moment! alas, if only I could spend all my time drawing incredibly stupid characters I mean I do but)
#art#twisted wonderland#twisted wonderland spoilers#tapis rouge#i know these are not my best but by god i needed to draw ~daddo venue~#he is a treat! can't wait for him to yell at us for screwing up a shoot or whatever the last-minute disaster will be#i am SO HAPPY it turned out to be about movies after all! ...i mean sort of anyway#i'll take what i can get (and i do enjoy twst trying to be all cute about snow whAHEM i mean beautiful queen) (i see you there twst)#(also to be fair it actually wasn't poisoned in historial-revisionism-twstland so i think we can trust this apple. a+ acting eric)#anyway we are still. very solidly in the 'stand around and talk about the wallpaper for three hours' part of the event.#but HEY we got to meet eric! i was not really expecting it to be him so i am VERY pleased#also god help me i did think the shopping montage as portrayed by a rhythmic where they literally SKIP down the street was hilarious#there's a lot of Choices that were made in this event and that was a good one
3K notes
·
View notes
Note
the brightly coloured skinny jeans that Teens wore in the late '00s and early '10s were meant to denote where you stood in gang hierarchy. salmon was the highest rank and meant you had killed someone.
I think the funniest part of this is that, if you'd floated this idea at the time, at least some parents would have believed you.
18K notes
·
View notes
Text
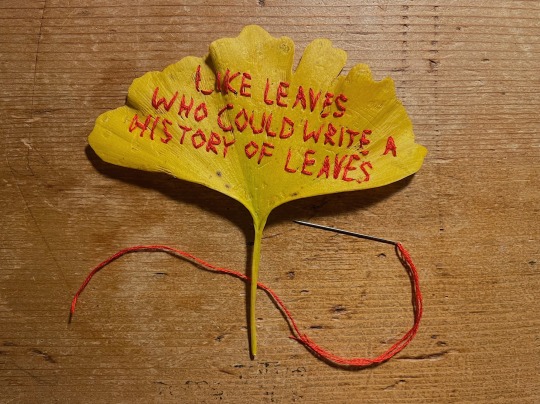
The wind blows their ghosts to the ground
line (loosely a translation of iliad 6.146-9) from memorial by alice oswald, embroidered onto a ginkgo leaf i found on the ground
#desk lamp lighting because it is dark and i Would take a photo tomorrow but i am Sure it will shrivel overnight#and it's in red for iliad book 3 reasons :-)#oh embroidery as somewhere in between the ideas of historical memory as presence and historical memory as a series of puncture wounds#we're really in it now!!!!!!#like leaves who could write a history of leaves#trees instead of gravestones#embroidery#alice oswald#iliad#beeps
4K notes
·
View notes
Text
they want to talk about mental illness and acceptance and how everyone is a little ocd it's cute and quirky and their "intrusive thoughts" are about cutting their hair off and you say yours are about taking a razorblade to your eye and they say ew can you not and everyone is a little adhd sometimes! except if you're late it's a personality flaw and it's because you are careless and cruel (and someone else with adhd mentions they can be on time, so why can't you?) and it's not an eating disorder if it's girl dinner! it's not mania if it's girl math! what do you mean you blew all of your savings on nonrefundable plane tickets for a plane you didn't even end up taking. what do you mean that you are afraid of eating. get over it. they roll their little lips up into a sneer. can you not, like, trauma dump?
they love it on them they like to wear pieces of your suffering like jewels so that it hangs off their tongue in rapiers. they are allowed to arm-chair diagnose and cherrypick their poisons but you can't ever miss too many showers because that's, like, "fuckken gross?" so anyone mean is a narcissist. so anyone with visual tics is clearly faking it and is so cringe. but they get to scream and hit customer service employees because well, i got overwhelmed.
you keep seeing these posts about how people pleasers are "inherently manipulative" and how it's totally unfair behavior. but you are a people pleaser, you have an ingrained fawn response. in the comments, you have typed and deleted the words just because it is technically true does not make it an empathetic or kind reading of the reaction about one million times. it is technically accurate, after all. you think of catholic guilt, how sometimes you feel bad when doing a good deed because the sense of pride you get from acting kind - that pride is a sin. the word "manipulation" is not without bias or stigma attached to it. many people with the fawn response are direct victims of someone who was malignantly manipulative. calling the victims manipulative too is an unfair and unkind reading of the situation. it would be better and more empathetic to say it is safety-seeking or connection-seeking behavior. yes, it can be toxic. no, in general it is not intended to be toxic. there is no reason to make mentally ill people feel worse for what we undergo.
you type why is everyone so quick to turn on someone showing clear signs of trauma but you already know the fucking answer, so what's the point of bothering. you kind of hate those this is what anxiety looks like! infographics because at this point you're so good at white-knuckling through a severe panic attack that people just think you're stoic. even people who know the situation sometimes comment you just don't seem depressed. and you're not a 9 year old white kid so there's no way you're on the spectrum, you're not obsessed with trains and you were never a good mathematician. okay then.
mental illness is trending. in 2012 tumblr said don't romanticize our symptoms but to be fair tiktok didn't exist yet. there's these series of videos where someone pretends to be "the most boring person on earth" and is just being a normal fucking person, which makes your skin crawl, because that probably means you are boring. your friend reads aloud a profile from tinder - no depressed bitches i fucking hate that mental illness crap. your father says that medication never actually works.
you still haven't told your grandmother that you're in therapy. despite everything (and the fact it's helping): you just don't want her to see you differently.
#writeblr#warm up#to be clear let me state again: i think you should id however you fucking want if it helps you seek peace#but there is a HUGE difference between being like '.... im undiagnosed but i think i might be X'#and a person who is like ''omg my intrusive thoughts made me buy a birkin!!!''#babe mine made me throw up bc they disgusted me so much <3#mine made me hurt myself evenly. even when i wanted to stop. i have had to put my hand on the stove MULTIPLE TIMES#and again i'd rather have 10000 people get help for something they don't need help for#than have 1 kid NOT get help#but there has GOTTTTT to be a middle ground here#bc at this point it isn't ''raising awareness''#it's . fucking misinformation. and ''what this picture says about you!!!!!''#& yes! im mostly talkin about ppl who are actually disgusted and offended by signs of mental illness#but use it to defend THEIR actions#like babe you hate when kids start yelling in the walmart? but you YOuRSELF can yell?#you are depressed so it's fine you were cruel to your spouse?#but if your spouse spends too much time in bed she's a lazy fuck?#your partner needs to do everything for you bc of your history in trauma? but when SHE has needs she's being clingy and gross?#HUGE difference here between whom i think most of my followers are btw. like#all it takes is fucking anyyyy empathy or kindness . like.#anyway it's hard to explain im hoping we all know the person im talking about lol
6K notes
·
View notes
Text
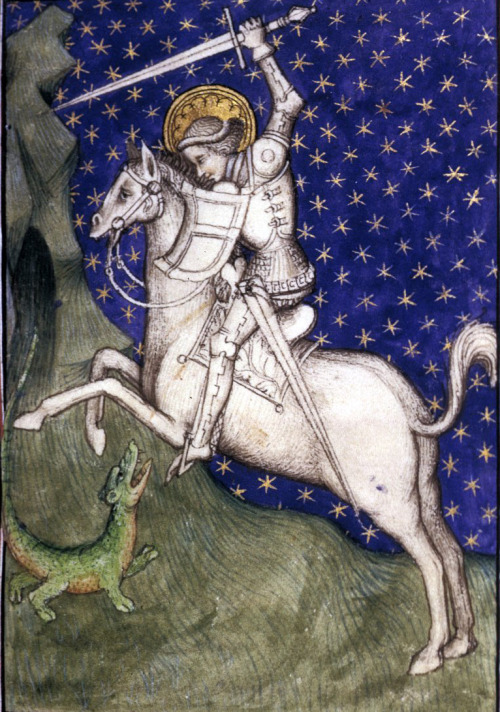
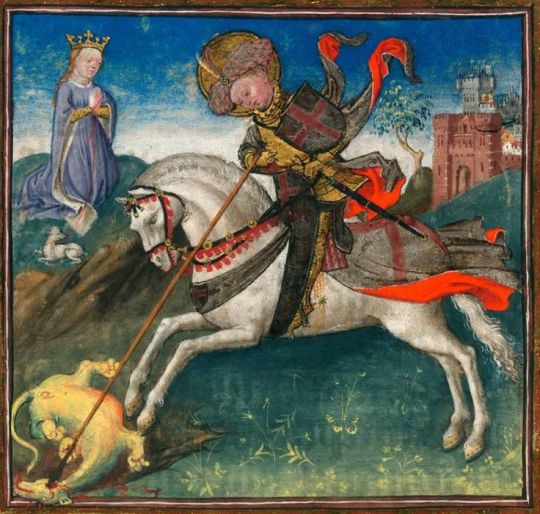
Ever see a depiction of St. George and the Dragon? It's pretty fair to say if you've seen one, you've seen them all: Georgie on a horse stabbing a flailing dragon creature, princess piously kneeling in the background, vague landscape alluding to the homeland of the artist's patron.
The most varied part is the dragons. No one had a real definition for the thing, it seemed. For your pleasure and entertainment, I have ranked some medieval depictions based on how impressive George's feat seems once you see the dragon.

Paolo Uccello, 1456
This is a terrifying beast. The hell is that. Uccello was one of the first experimenters with perspective, so the thing also looks surreal, like it's taking place on Mars, or a Windows 95 screensaver. I would not want to fight that, I would not want to be tied to that. (Sometimes the princess is tied to the dragon for some reason.) 10/10
Horse thoughts: Maybe if I look at the ground it will be gone when I look up

Unknown artist, c. 1505
This is a rare change of form for the dragon; it's the only one I've seen actually flying (or at least falling with style). It doesn't look particularly deterred by the spear through its throat, either. Also, George looks appropriately nervous. On the other hand, it hasn't got teeth, it seems to be fuzzy rather than having scaly armor, and George is bolstered by his army of Henry VII and his children, most of whom definitely didn't actually die in infancy. Still, wouldn't want to fight it, wouldn't want my pet sheep near it. (Sometimes the princess has a pet sheep for some reason.) 9/10
Horse thoughts: I am so glad I wore my mightiest feather helmet for this

Raphael, 1505
We are coming to Dragons With Problems. This guy looks about comparable in size to George, and does have wings, but doesn't seem to be using these things to his advantage (and has he only got one wing?) And how does he deal with the neck? He does have a comically small head, but holding it up with such a twisty neck seems complicated at best. But most egregiously, he is doing the shitty superheroine pose where he is somehow simultaneously showcasing his chest and his butt, with its unnecessarily defined butthole (more on this later) (regrettably). 8/10 bc it's Raphael
Horse thoughts: AM I THE BESTEST BOI? AM I DOING SUCH A GOOD JOB? WE R DRAGON SLAYING BUDDIEZ

The Beauchamp Hours, c. 1401
We had a spirited debate about this one at work. Again, the dragon has gotten smaller, and this one hasn't got even one wing. He's basically a crocodile. So the debate became: would you want to fight a crocodile if you had a horse and a pointy stick? Would the horse trample the animal, who can't get on its hind legs, or freak out and throw its rider? Would the pointy stick be enough to pierce the croc's thick hide? In this case, George seems to be controlling his horse and putting his pointy stick in the dragon's weak spot, so we can be impressed by his skill and strategy. However, his hat is dumb. 7/10
Horse thoughts: Dehhhh

Book of Hours, c. 1480
Here we have the same kind of croco-dragon, but George's focus on his strategy has gone out the window. He's flailing around, not even looking at his target, he's about to lose his pointy stick, he hasn't got a hand on the reins, and his sword seems to only be poking the invisible dragon over his shoulder. All he's got going for him is that his hat is slightly less dumb. 6/10
Horse thoughts: Yay, new friend! Come play with me, new fr- what is happening
Final dragons put behind this Read More for your safety:

Rogier van der Weyden, c. 1432
I'm thinking this guy is at least semi-aquatic. Webbed feet, wings that seem more like fins, bipedal but top-heavy, jaws that seem more for scooping than biting. Maybe she's crawled up here from the nearby body of water to lay her eggs, and this is all a big misunderstanding. Moreover, George's dagged sleeves seem entirely impractical for the situation. 5/10
Horse thoughts: i got my hed stuk in a jar and now it is this way forever

Unknown artist, c. 15th century
I hate this. I hate everything about it. Why has it got human eyes and teeth. Why is its nose melting. Why has it got a dick on its face and balls under its chin. The fin/wings are back but they look even more useless. Also, George is shifty as hell, schlumped over in his saddle with his bowler hat thing over his eyes. The baby dragon at the bottom eating some hapless would-be rescuer is kind of metal. 4/10 at least the thing is gonna die
Horse thoughts: I Have Smoked So Much Crack

Book of Hours, c. 1450
Remember what I said about the buttholes? First, sorry. Second, yeah, we're back to that. I'll admit this one is less about the danger from the dragon itself than the very specific choices the artist has made. They didn't need to do that. It's a lizard. They don't even have. And it's like they had an orifice budget and they skipped an exit wound for the spear to focus. Elsewhere. It's so detailed. And George had an even dumber hat. 2/10 take it away
Horse thoughts: I Have Smoked So Much Weed
Book of Hours, c. 1415
This is just bullying. There isn't even a princess. That is clearly an infant. Look at that smug look on George's face as he swings his sword that's bigger than the whole little guy. This is the equivalent of when DJT Jr. hunted those sleeping endangered sheep. 1/10
Horse thoughts: ....yikes
And this is the previous one, but now the baby dragon is cute. He's chubby. He's got toe beans. He's Puff the Magic Dragon. His eyes have already gone white, implying that George is just kicking its corpse around for funsies. What's the difference between the dragon and the lamb in the background? That the dragon is dead, like our innocence. This George is truly deserving of the dumbest hat of all. 0/10 plus one more butthole for the road
Horse thoughts: Perhaps it is we who are the buttholes.
#art history#nonsense#hot takes#I am doing a St. George painting and have been wading through reference material#manuscript#fuck me I didn't notice van der Weyden managed to sneak a butthole in his too#the definitive list#when knighthood was in flower
7K notes
·
View notes
Text
"Israel is more LGBTQ friendly than Palestine."
Let's say, that hypothetically, Israel is the most LGBTQ-friendly country on the entire planet. I STILL would be against them committing genocide. What they have done to Gaza is horrific and we should be talking about a ceasefire to prevent more innocent people from dying. But nah, people would rather shift the conversation over to something that's completely unrelated away from the war crimes the IDF is committing.
As a queer person who has lived in Texas and Mississippi her whole life, it has always disgusted me how gleeful some of you "progressives" act when something horrific happens to places you deem "conservative." Do you people not understand that every place has diversity, every place has LGBTQ people? People deserve to live full and happy and safe lives regardless of where they were born. There is nothing in the world that could ever justify the mass killings of innocent people.
#free palestine#free gaza#something like this shouldn't need to be said#also fuck the people who argue that Palestinians can just leave#how braindead do you need to be to have that take#i'm begging you to read a history book
3K notes
·
View notes
Text
[mc is reading a devildom textbook that is on human world history]
mc: .......
satan: ... you look troubled
mc: yeah cause it's all wrong
satan: what do you mean?
mc: well, first of all it says the earth is flat
#why did it take me so long to come up with an outrageously wrong history fact#uh#im literally studying the cold war rn#yeah#wo hoo#obey me crack#obey me shall we date#obey me shitpost#obey me incorrect quotes#obey me#obey me mc#obey me satan
1K notes
·
View notes
Text

falin and thistle are like this to me
#my art#falin touden#thistle#dungeon meshi#delicious in dungeon#falin has a history of taking care of children + marcille mistook thistle for a child#so obvious conclusion is that the falin side of faligon sees thistle as a child
1K notes
·
View notes
Last Seen Blogs

rare2o1
UNDERPSYCHO

kopphie
Kopphie

debbiecolon
A Lot Like Awesome

queensarrow
a city of heroes
thelastofhope
lasthope