
der-neurodivergente
ich war nie ein mensch
neurodivergent extraterrestrial (wait, that's a pleonasm!) | math/physics/ math. cog. sci. (my special interests) |
he/they - call me superhumanoidAI, or Erik or whatever you would call this (id)entity presented in splinters of this blog.
200 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

mewannafu
Untitled

moonaster
Untitled

highasawizard
feral child
sissycross
greetings

pillowtalk801
Untitled
Text
Today I found a very helpful source of how PTSD might have elevated/altered effects of distress in people on the spectrum (and also probably other people with a neurodivergent neurotype) compared to neurotypical indoviduals. It's also more likely that trauma can correlate with more severity of PTSD symptoms in neurodivergent/ASD individuals due to extra involvement of the neurodivergent nervous system.
And this has serious implications on the treatment for neurodivergent trauma survivors.
The article by Dr. Megan Anna Neff (neurodivergentinsights, neurodivergent therapist):
PTSD vs. AND Autism
(Source: https://neurodivergentinsights.com/misdiagnosis-monday/ptsd-and-autism)
While I have set up this series to distinguish autism from common misdiagnoses, this week’s topic is more complex. You can see from the Venn Diagram there is much overlap among the experiences, sensations, and risks associated with PTSD and autism. Given the high rate of co-occurrence, it is more likely that missed diagnosis happens (vs misdiagnosis), where a person’s PTSD may be accurately diagnosed while their underlying neurotype (autism) remains missed. When they do co-occur this creates some additional complexity in the clinical presentation. I’ll cover these topics as well as provide clinicians will some ideas on how to adapt traditional trauma treatment for the ND in mind.
Misdiagnosis
Given the co-occurrence of Autism and PTSD, it is likely rarely a misdiagnosis (it's likely accurate), but the autism may be missed. PTSD is rarely an inaccurate diagnosis, however when PTSD is used to explain away the autistic traits and experiences it may be considered a "misdiagnosis".
Our field has much to thank for the recent development of trauma-informed care and treatment. I am thankful for the work of Dr. Burke Harris, Bessel Van der Kolk, and countless others in bringing awareness to trauma. I'm thankful for the work done to create trauma-informed spaces as more therapists, educators, and medical providers are working from a trauma-informed lens. And while I fear minimizing these crucial advancements, I believe it's important to consider the potential risk of trauma becoming the new "it" lens from which the mental health field sees everything. I've talked with countless people whose autism was missed because their traits were explained away through the framework of PTSD or c-PTSD. In our enthusiasm to help bring healing around trauma, we (the mental health field) are vulnerable toward making trauma the new "lens" from which everything is understood. The field is at risk of falling into confirmation bias as we quickly reduce all sensory and dysregulation experiences to trauma.
I fell prey to this confirmation bias myself. I have spent much of the last ten years (since becoming a mother (i.e. increased sensory load) in a foggy, disconnected, and dissociated space. As a therapist in training, the only explanation I had for this was trauma. I spent three years in depth therapy, wondering with my therapist if I may have repressed trauma. It turns out it wasn’t trauma; my body was simply responding to being sensory overloaded by disconnecting. It NEVER occurred to me this could be a response to my neurotype/sensory profile. And here lays the problem--too often, clinicians hear dissociation, self-harm, and suicidality and run automatically to trauma without considering the undergirding neurotype. After sharing my story, countless people have reached out to tell me their stories of being in therapy searching for repressed trauma and engaging in trauma treatment with limited results. There are many reasons it can be hard to tease out autism from PTSD; below is a list of overlapping characteristics that can make it difficult to distinguish between the two:
Overlapping Characteristics:
Sensory Sensitivities: The nervous system/amygdala goes on hyper-alert in the aftermath of trauma as a means of trying to protect against future harm. This looks similar to the sensory profile of a hypersensitive autistic.
Increased amygdala activation: Wiring around the amygdala, “safety alarm,” becomes more sensitive after trauma. Research on amygdala and Autistics is mixed, but many of us have more amygdala involvement during certain activities (i.e., eye contact).
Difficulty regulating intense emotions: Associated with brain chemistry (amygdala) and sensory profile, it becomes more difficult to self-soothe and regulate difficult emotions.
Increased risk of substance abuse: Substances can be a powerful method of regulating a hyperactive nervous system. Both groups are at an increased risk of substance abuse disorders.
Self-harm behavior: Elevated within both groups. Self-harm functions to ground, self-soothe, regulate the nervous system.
Dissociation: This is a common trauma response, can also be a response to sensory overload. Common among both groups.
Suicidality: Autistics 3 times more likely to die by suicide. Suicidality is also more common among trauma survivors.
Increased risk of victimization: Trauma survivors are at a higher risk of re-victimization. Similiarly, recent research has demonstrated that autistic women and genderdiverse individuals are more likely to be survivors of violent victimization. Some risk factors include the challenge in social reasoning, missing contextual cues, and tendency to take things literally. In one study, Autistic adults were 7.3 times more likely to endorse having experienced sexual assault from a peer during adolescence (Weiss and Fardella).
Given the significant overlap, it’s easy to see how one may miss the autism in favor of a PTSD diagnosis, especially if a trauma history is present. And, most neurodivergent people do experience trauma, whether it is the big T trauma of victimization or the small t trauma of marginalization, bullying, and discrimination. This brings us to point 2, the intersection of Trauma and Autism:
Understanding the Intersection: Trauma and Autism
Autistics are much more likely to experience PTSD than the general population, especially women, AFAB, BIPOC, trans, and genderqueer autistics. Research shows Autistic women have a double vulnerability—more vulnerable toward victimization and more vulnerable toward developing PTSD following a traumatic event. Autistic women are 1.5 times more likely to be victimized than their neurotypical peers. In addition to being more vulnerable to victimization, we are also more vulnerable to develop PTSD following a traumatic experience. There are various theories about why this is: more active amygdala’s, inflexible nervous systems, more difficulty regulating emotions, and our tendency to take in the sensory experience with more intensity. In fact, Rumball et al. (2020) found that we develop PTSD at higher rates even when criteria A is not met (for non-clinicians, that essentially means a less intense trauma).
Here are a few sobering facts about the intersection of autism and trauma:
💙 Rumball et al. (2020) study found that approximately 60% of autistics reported probably PTSD in their lifetime (compare this to 4.5% of the general population) (Rumball, 2020).
💙 Haruvi-Lamdan et al., 2020 study found that 32% of their Autistic participants had probable PTSD compared to 4% of non-autistic population
💙 Fenning et al, 2019 research demonstrated that autistic children had more reactive nervous systems. This aligns with similar research that has identified the autistic nervous system to be less flexible (Thapa and Alvares, 2019). Less flexible nervous systems have a more difficulty time coping with acute stressors and may contribute to increased hyperactivation of the nervous system following trauma.
💙 Neurodivergent (ADHD/Autism) neurobiology is more vulnerable and reactive: (Beauchaine et al., 2013)
💙 We are more vulnerable to social victimization and marginalization. In the Haruvi-Lamdan et al., 2020 females with autism (but not males) reported more negative life events, particularly social events than typical adults.
💙 Our sensory profiles mean many of us absorb sensory experiences with more intensity. The memories and sensations thus code in our minds and bodies with more intensity.
This double vulnerability is rarely talked about as a part of Autistic Awareness or within the clinical literature on trauma. The lack of awareness around this is unfortunate as any good trauma treatment must consider the neurotype that is undergirding the experience of trauma. Unfortunately, few clinicians are trained in how to do ND affirming trauma work. It’s to that topic we now turn….
Neurodivergent Trauma Treatment
As the above statistics show, ASD/PTSD co-occur at unfathomable rates. When ASD is missed, the trauma treatment is negatively impacted. It is critical to treat autistics trauma with a neurodivergent adapted approach. Just like our pathway to trauma is not the neurotypical pathway, neither can our treatment be the same as neurotypical treatment.
Don’t Skip the Basics: Grounding and relaxation strategies are the foundational blocks of any good trauma treatment. It’s necessary that the person have tools and practices that help them to re-anchor when the trauma hijacks their body. Because our nervous systems are less flexible than a neurotypical, it is harder for us to get back to baseline once triggered. If progress feels slow, that is okay; again, it takes us more work to get back after our nervous system has been hijacked.
Consider Somatic Therapies: We need more attention to our sensory profile (grounding, bodywork, encouraging natural forms of movement, etc.). Our sensory system is likely in intense overdrive. Our bodies are already a difficult place for many of us to occupy; trauma is like throwing gasoline on top of a sensitive sensory system. Somatic experiencing and other body-based approaches to trauma should be considered. However, given the intensity of the body experience, autonomy and empowerment for the client to move at their pace must be considered.
Adapt Exposure Therapy (If Used): Exposure therapy is often treated as the gold standard for PTSD treatment. However, this can be quite dysregulating for the Neurodivergent person if not adapted. If used, it is critical it is adapted & client-led. Please don’t flood your autistic clients. Sensory experiences outside of our control are dysregulating; we must control the sensory experience. Proper attention to pacing and recovery is essential. Initial treatment must focus on increasing interoception and regulation skills before working through exposure.
Be cautious of CBT: CBT is aimed at confronting unhelpful beliefs about the world and self. The clinician must realize that these “maladaptive schemas” were not just developed in the trauma but also derived from years of being marginalized by society (often on an unconscious level). Thus, it is possible that attempting to reframe some of these negative beliefs will have a rebound effect of increasing shame and confidence in beliefs. The insistence of reframing may also result in loss of trust in the therapeutic relationship.
#neurodivergent#ptsd#cptsd#trauma#trauma survivor#autism#asd#complex trauma#actually autistic#neurodivergent struggles#actually neurodivergent#nervous system#adhd#neuroatypical#spectrum people#peer support#mental health#important#trauma treatment#autism spectrum#neurodiversity#neurodivergence
38 notes
·
View notes
Text
Everyone is like "We support autistic people!", but once an autist shows one of their less socially-acceptable traits they are like "Oh, a perfect victim for our collective bullying!"
#hypocrisy#neurodivergent struggles#autism#aspergers#neurodivergent#sick society#hypocrites#bullying
61 notes
·
View notes
Text
Me and my body in a nutshell:
Me: *relaxing*
My body, out of nowhere: *stomach cramps*

5 notes
·
View notes
Text
Featuring "Imitate 'til you make it."
3 notes
·
View notes
Text
So

I thought this was a funny joke but
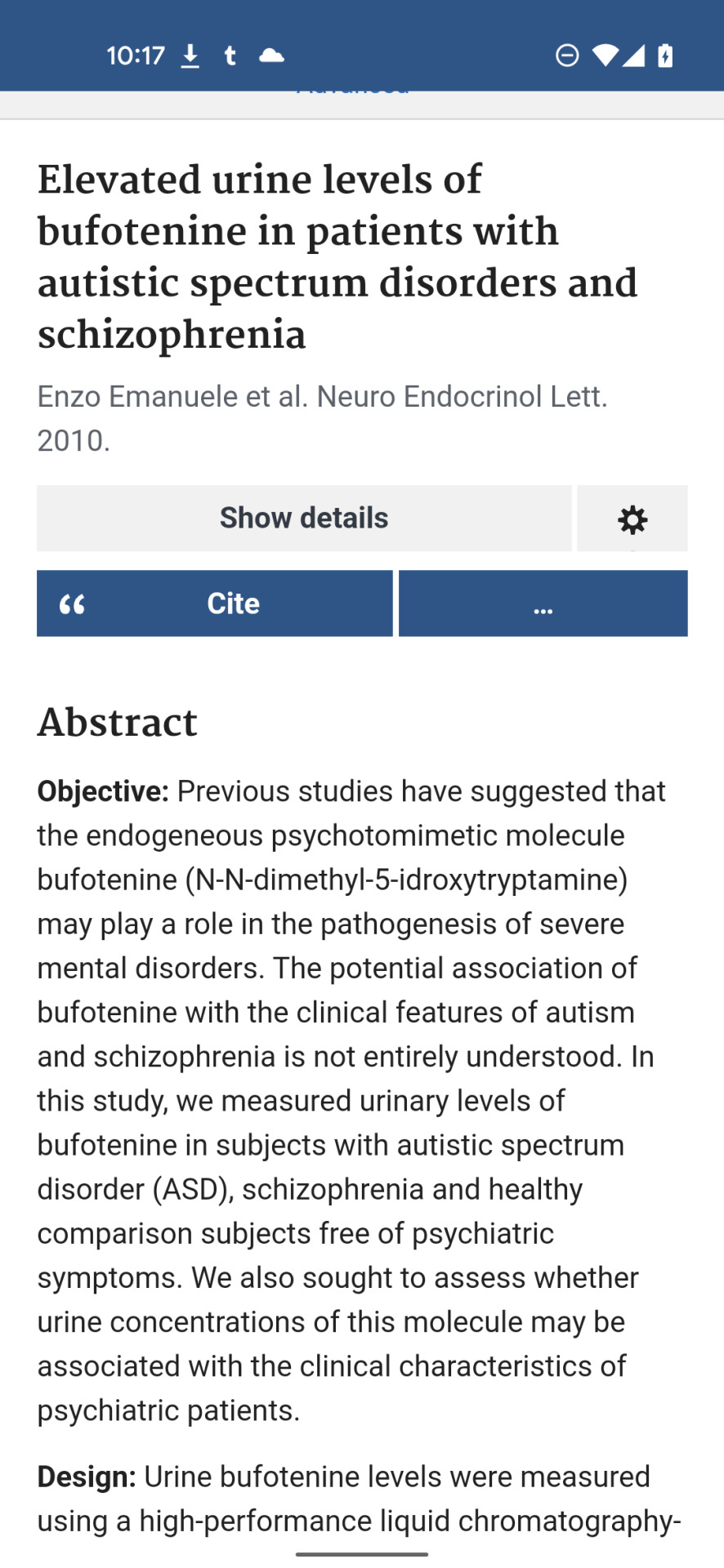

????????
147 notes
·
View notes
Text
Thank you for this insight! Makes a lot of sense actually, as my "routine" is really what you desribe!
One of my main routines is needing 6-8 hours at least each day to listen to music while daydreaming and thinking.
I think we need to rework the whole “needing routine as an autistic person” thing because for the majority of allistic people, “routine” looks something like:
-wake up at 6am
-shower at 6:15am
-eat breakfast at 6:30am
-do important outings at 7am
-come home at 3pm
and so on..
And that is nothing like what I and many other autistic people experience (though it is what some experience).
Routine can be more accurately described as needing to do things in order to feel comfortable.
For example, I have no set time I wake up, I have no set time I do anything. But when I do wake up, I need to do my morning tasks in a specific order or I’ll struggle to function.
I get out of bed, turn on my lamp, switch my computer on, go to the bathroom, make my bed, get dressed, and sit down at my desk. That’s what a routine looks like to me.
If I’m cooking, I need to do things in a certain order or the food will be “wrong” (this could possibly be down to ARFID, but that is also comorbid with autism.)
There are other things like this. I guess you could call them mini routines. They aren’t a typical routine you’d see in a neurotypical or even someone who’s allistic.
For the longest time, I thought this was a symptom of autism I did not have at all but I do.
Just because a symptom doesn’t present in a neurotypical way, doesn’t mean it’s not there.
6K notes
·
View notes
Text

16 notes
·
View notes
Text

This is my brain adapting to compensate the ADHD.
21 notes
·
View notes
Text

2 notes
·
View notes
Text

It is okay to go at your pace.
103 notes
·
View notes
Text
sometimes, when someone does a silly joke, and i respond to it sincerely, it is because i did not get the joke, and sometimes its because i am actually doing a joke myself. i like to call this "the autist's double bluff"
57K notes
·
View notes
Text
Being a multiply neurodivergent writer is like jumping from one association to another, and each side note either creates a new project or accounts to an already existent project, in semi-irregular cycles.
#multiply neurodivergent#fusing hyperfixations with special interest#lost in thought networks#aspergers#adhd#special interest#writer#neurodivergent writer#writer problems#associations#hyperfocus#hyperfixation
56 notes
·
View notes
Text
Digging deeper into the special interest/ getting a new special interest:
*me, to my special interest:* "Are you ready to get dissected by my mind?"
0 notes
Text
I can only really perceive and process body sensations, feelings and emotions if I link them with associations: The analogy enables me to "translate the feelings into a processable language" because I can't do anything with the raw data.
#aspergers#relatable content#autism#alienation#sensory processing disorder#sensory processing issues#emotions#incomprehensible emotions#associations#analogies#analogy
4 notes
·
View notes
Text
Every day of having aspergers be like:

#autism#aspergers#autism memes#aspergers memes#rejection#neurodivergent struggles#from the life of a neurodivergent
39 notes
·
View notes
Text
39K notes
·
View notes