
mcatmemoranda
MCAT Memoranda
Originally, this blog was for things to be remembered for the MCAT. Then I included EMT training and then medical school; and now residency. Basically, this is where I keep some of the things I am studying or learning so that I can easily look them up when I need to. Search the tags to find stuff!
11160 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs


wendyswhoppers
Wendy's Whoppers

bluepotatorw
Blue Potato

trainfitness
Train Fitness International Limited

furstyphoto
life in Washington.
Text
BRIXADI is bupreborphine injection. Apparently it’s less likely than Sublocade to cause injection site issues. Have a pt on it who complains of pain/a lump at the injection site even days after injection.
3 notes
·
View notes
Text
I didn't get COVID until end of 2022. Then I got it again in January this year. I'm going to get a COVID vaccine tomorrow. I had tried to schedule an appointment to get it at CVS earlier this year, but they didn't have any vaccines available. Now they do. It wasn't that bad. Just annoying. I wonder if they'll start making a yearly combined COVID and flu vaccine. That would be convenient.
0 notes
Text
Have a 22 y/o pt who complained of heart palpitations. Went to ED and had subclinical hypothyroidism and some PACs and ectopic beats in bigemininy and trigeminy. Sent him to cardiology, who recommened: beta blocker, antiarrhythmics, or APC ablation. He decided to start metoprolol XL 25 mg qd and will be getting an echo to rule out structural heart disease.
1 note
·
View note
Text
Fecal calprotectin just tests for inflammation. Can differentiate between IBD and IBS.
1 note
·
View note
Text
I have a pt who has history of hep C that was treated. I checked him for hep C RNA PCR viral load and it came back undetected, which means his treatment worked. This is called "SVR," sustained viral response. So when you do the hep C antibody screen, it still comes up positive, but the viral load (RNA PCR) is undetected, so no further treatment is needed.
1 note
·
View note
Text
Off label tx for plantar warts: Tagamet 800 mg QID x3 weeks
1 note
·
View note
Text

Strokes will spare the forehead, unlike Bell's palsy.
8 notes
·
View notes
Text
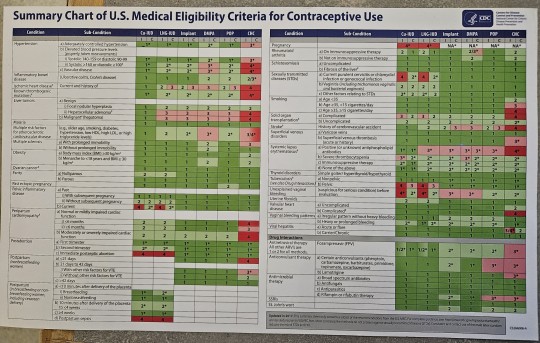

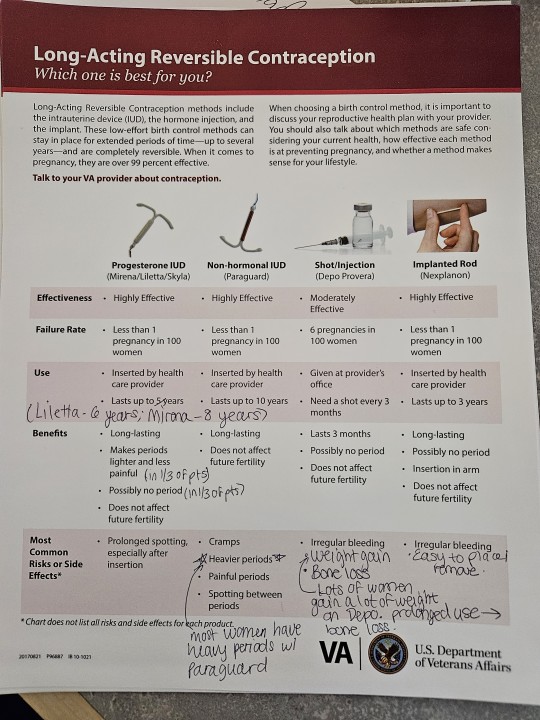
Will have to zoom in close to see this!
2 notes
·
View notes
Text
Liraglutide (Saxenda) dosing: Start 0.6 mg daily for 1 week. If tolerated, increase to 1.2 mg daily for 1 week. Increase by 0.6 mg a day per week (i.e., 1.8 mg per day on week 3, then 2.4 mg a day on week 4, then 3 mg a day on week 5). Maximum dosing is 3 mg daily. Discontinue if weight loss less than 4% after 16 weeks or if 3 mg daily is not tolerated.
1 note
·
View note
Text
Semaglutide can be used to treat alcohol use disorder.
4 notes
·
View notes
Text
The Rotterdam 2003 criteria are the most widely used diagnostic criteria for PCOS, endorsed by multiple national and international professional societies. These criteria require the presence of two out of the following three features: oligomenorrhea, hyperandrogenism, and the presence of polycystic ovaries on ultrasonography. When the first two of these criteria are clearly met, ultrasonography to establish the presence of polycystic ovaries is not required.
1 note
·
View note
Text
Hormone therapy is not required for all transgender patients, but those who receive treatment generally report improved quality of life, higher self-esteem, and decreased anxiety. Feminizing and masculinizing hormone therapies, including the use of estrogen and/or androgen therapies such as testosterone, are partially irreversible. Thus, it is important to make a reasonable, educated decision and use informed consent prior to treatment. Patients who receive masculinizing therapy are at increased risk for erythrocytosis and those who receive feminizing hormone therapy often experience reduced muscle mass and fat redistribution
1 note
·
View note
Text
I have a pt in clinic who I diagnosed with C. diff. According to UpToDate, the treatment for an initial infection is fidaxomicin (200 mg bid x10 days).
Regimen selection – For patients with an initial episode of nonsevere CDI, appropriate treatment regimens include either oral fidaxomicin or oral vancomycin; we favor fidaxomicin over vancomycin given a small benefit with respect to recurrence rates, in accordance with 2021 Infectious Diseases Society of America (IDSA) guidelines
2 notes
·
View notes
Text
Methylnaltrexone (Relistor) is used to prevent opioid-induced constipation in pts on chronic opioids.
1 note
·
View note
Text
I just answered a question the other day about a pt who was on an anticoagulant and whether he needed to be bridged prior to a procedure.
Now I have a pt who is on warfarin for AFib and who will be going for a psoas abscess draiange. So I'm holding his warfarin. He needs to be bridged based on his CHADSVASc score being 2, meaning high risk for thromboembolism. From UpToDate:
Atrial fibrillation (to prevent stroke and systemic embolism): Note: When admitted for short-term hospitalization (eg, admission for a procedure or surgery), ambulatory patients taking an oral anticoagulant and not at high risk of immediate thromboembolism typically do not require bridging anticoagulation. Patients at high risk of thromboembolism (eg, recent cardioversion, high CHA2DS2-VASc score, prior cardioembolic stroke, current intracardiac thrombus) may be considered for bridging with a parenteral anticoagulant (see Transitioning between anticoagulants below).
Transitioning between anticoagulants: Note: This provides general guidance on transitioning between anticoagulants; also refer to local protocol for additional detail.
Transitioning from another anticoagulant to IV heparin:
Transitioning from a therapeutic dose of SUBQ low-molecular-weight heparin or SUBQ fondaparinux to a therapeutic dose of IV heparin: Start IV heparin without a bolus dose (infusion rate depends on the indication) 1 to 2 hours before the next dose of low-molecular-weight heparin (LMWH) or fondaparinux would have been due (Ref).
Transitioning from warfarin to a therapeutic dose of IV heparin: Stop warfarin and, when INR is as close as possible to the lower end of the targeted INR range, start IV heparin without a bolus dose (infusion rate depends on the indication) (Ref).
Transitioning from a direct-acting oral anticoagulant to a therapeutic dose of IV heparin: Stop direct-acting oral anticoagulant (DOAC) and, when the next DOAC dose would have been due, start IV heparin without a bolus dose (infusion rate depends on the indication) (Ref).
Transitioning from IV heparin to another anticoagulant:
Transitioning from a therapeutic dose of IV heparin to therapeutic SUBQ low-molecular-weight heparin or SUBQ fondaparinux: Stop IV heparin and within 1 hour start SUBQ LMWH or SUBQ fondaparinux. Note: If aPTT is not within therapeutic range at the time heparin is stopped, consult local protocol (Ref).
Transitioning from a therapeutic dose of IV heparin to warfarin: Start warfarin and continue IV heparin until INR is within therapeutic range (Dager 2018; Hull 2022a). Note: Overlap IV heparin with warfarin until INR is ≥2 for at least 2 measurements taken ~24 hours apart (duration of overlap is ~5 days) (Ref).
Transitioning from a therapeutic dose of IV heparin to a direct-acting oral anticoagulant: Start DOAC when the heparin infusion is stopped (consult local protocol if the aPTT is above the target range) (Ref).
So I'm gonna hold warfarin and check his INR. Day team can start the heparin.
2 notes
·
View notes
Text
Doing review questions.
Hyperkalemia is a known side effect of ACE inhibitors and angiotensin receptor blockers such as olmesartan. The risk of hyperkalemia is increased with chronic kidney disease, diabetes mellitus, moderately severe to severe heart failure, NSAID use, and older adults. Chlorthalidone and hydrochlorothiazide can cause hypokalemia.
In men who are diagnosed with hypogonadism with symptoms of testosterone deficiency and unequivocally
and consistently low serum testosterone concentrations, further evaluation with FSH and LH levels is
advised as the initial workup to distinguish between primary and secondary hypogonadism. If secondary
hypogonadism is indicated by low or inappropriately normal FSH and LH levels, prolactin and serum iron
levels and measurement of total iron binding capacity are recommended to determine secondary causes of
hypogonadism, with possible further evaluation to include other pituitary hormone levels and MRI of the
pituitary. If primary hypogonadism is found, karyotyping may be indicated for Klinefelter’s syndrome.
Daily use of polyethylene
glycol (PEG) solution has been found to be more effective than lactulose, senna, or magnesium hydroxide
in head-to-head studies. Evidence does not support the use of fiber supplements in the treatment of
functional constipation. No adverse effects were reported with PEG therapy at any dosing regimen.
Low-dose regimens of PEG are 0.3 g/kg/day and high-dose regimens are up to 1.0–1.5 g/kg/day.
Ref: Tabbers MM, DiLorenzo C, Berger MY, et al: Evaluation and treatment of functional constipation in infants and children:
Evidence-based recommendations from ESPGHAN and NASPGHAN. J Pediatr Gastroenterol Nutr 2014;58(2):258-274.
2) Gordon M, MacDonald JK, Parker CE, et al: Osmotic and stimulant laxatives for the management of childhood
constipation. Cochrane Database Syst Rev 2016;(8):CD009118. 3) Lauters R, Saguil A: Laxatives for the management of
childhood constipation. Am Fam Physician 2017;96(7):433-434
Primary hyperaldosteronism should be suspected as a cause for hypertension if a patient has a spontaneously low potassium level or persistent hypertension despite the use of three or more antihypertensive medications, including a diuretic. This can be evaluated by checking a serum renin activity level and a serum aldosterone concentration and determining the aldosterone/renin ratio. Primary hyperaldosteronism typically presents with a very low serum renin activity level and an elevated serum aldosterone concentration. A 24-hour urine collection for 5-hydroxyindoleacetic acid (5-HIAA) would be used to evaluate for a neuroendocrine tumor, which can present as chronic flushing and diarrhea. Cortisol levels can be checked if Cushing syndrome is suspected. Hypertension can be present in Cushing syndrome, but it is typically associated with other signs such as obesity and an elevated blood glucose level due to insulin resistance.
Psychogenic tremor is characterized by an abrupt onset, spontaneous remission, changing characteristics,
and extinction with distraction. Cerebellar tremor is an intention tremor with ipsilateral involvement on
the side of the lesion. Neurologic testing will reveal past-pointing on finger-to-nose testing. CT or MRI
of the head is the diagnostic test of choice. Parkinsonian tremor is noted at rest, is asymmetric, and
decreases with voluntary movement. Bradykinesia, rigidity, and postural instability are generally noted.
For atypical presentations a single-photon emission CT or positron emission tomography may help with
the diagnosis. One of the treatment options is carbidopa/levodopa.
Patients who have essential tremor have symmetric, fine tremors that may involve the hands, wrists, head,
voice, or lower extremities. This may improve with ingestion of small amounts of alcohol. There is no
specific diagnostic test but the tremor is treated with propranolol or primidone. Enhanced physiologic
tremor is a postural tremor of low amplitude exacerbated by medication. There is usually a history of
caffeine use or anxiety.
Ref: Crawford P, Zimmerman EE: Tremor: Sorting through the differential diagnosis. Am Fam Physician 2018;97(3):180-186.
I got 100% on the first quiz! :)
2 notes
·
View notes