
religion-is-a-mental-illness
Religion is a Mental Illness
Tribeless. Problematic. Triggering. Faith is a cognitive sickness.
13132 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

oh-meu-zeus-blog
Oh Meu Zeus!

240707me
Kamila Novais

kybi32k
Без названия

jamieleefraserrx
Jamie Fraser
Text
By: Lisa Selin Davis
Published: Apr 15, 2024
A thoughtful, comprehensive review just released in Britain points to a way out of the political impasse over youth gender treatments.
The toxicity of the culture war over youth gender medicine is well known to most of us. What’s less well understood is how that poisonous climate affects the very cohort being argued about — and those who care for them.
An exhaustive, level-headed 388-page report, commissioned by the National Health Service in England and released last week, warns: “Polarisation and stifling of debate do nothing to help the young people caught in the middle of a stormy social discourse.”
The Cass Review, led by Dr. Hilary Cass, examines the events and evidence (or lack thereof) that led to the closing of the UK’s only public youth gender clinic, the Gender Identity Development Services. GIDS opened in 1989 and at first served only 10 clients per year, mostly males who received psychological therapy; few medically transitioned. By 2016, GIDS was seeing nearly 1,800 clients a year, and multiple concerned clinicians there were blowing the whistle about the poor quality of the care. For years, their complaints mostly fell on deaf ears.
This document allows them to be heard. It is exceptional in many ways, including its scope. Cass spoke to many different and competing stakeholders, including disagreeing clinicians, “transgender adults who are leading positive and successful lives,” and “people who have detransitioned, some of whom deeply regret their earlier decisions.”
Cass reaches back into the history of youth gender medicine, formalized in the late 1990s in the Netherlands. She observes that the entire practice is “based on a single Dutch study which suggested that puberty blockers may improve psychological wellbeing for a narrowly defined group of children with gender incongruence.”
Recent scrutiny of the Dutch research revealed that the methodology was too flawed to support that conclusion. The Dutch approach involved something different from what has become the norm in the United States and was the norm at GIDS for a time. The Dutch doctors and psychologists offered youths extensive evaluation over long periods of time, discouraged social transition before puberty, and limited interventions to a carefully selected cohort who’d suffered from lifelong gender dysphoria, didn’t have other serious mental health issues, and lived in supportive families.
In America, this approach became denigrated as “gatekeeping,” and we veered toward a model known as “affirming.” We shifted from treating gender dysphoria to affirming a trans identity, letting a child’s feelings lead the way, and allowing social transition at any age. Here, manifesting one’s gender identity separate from natal sex was eventually seen as a civil right, rather than as a series of psychological and medical interventions — a model that influenced GIDS. But science doesn’t work that way. “Although some think the clinical approach should be based on a social justice model,” writes Cass, the National Health Service “works in an evidence-based way.”
That social justice / civil rights framing has made it harder to reckon with what Cass calls the “exponential rise” in adolescent patients starting around 2014, and a reversal in the sex ratio. Once it was mostly natal males who transitioned, but now it is mostly natal females, many of whom had no history of gender distress but did suffer from other mental health issues.
As for the evidence about how to treat these patients and others who havesought care, Cass concludes: “The reality is that we have no good evidence on the long-term outcomes of interventions to manage gender-related distress.” Individual studies may make claims about the efficacy of social transition, puberty blockers, or hormones, but they are too biased and low quality to draw conclusions from.
The National Health Service had already recently declared that puberty blockers would no longer be used for young people with gender dysphoria, “because there is not enough evidence of safety and clinical effectiveness.” The Cass Review confirms this, noting that “bone density is compromised during puberty suppression” and that doctors don’t know enough about the effects on “psychological or psychosocial wellbeing, cognitive development, cardio-metabolic risk, or fertility.” No evidence proved that blockers provided “time to think,” as many proponents of affirmation claim, but there is “concern that they may change the trajectory of psychosexual and gender identity development.”
As for the claim that these interventions prevent suicide, Cass reports that “the evidence found did not support this conclusion.”
Perhaps most important, Cass notes that “clinicians have told us they are unable to determine with any certainty which children and young people will go on to have an enduring trans identity.” That is, in contrast to the affirmative model’s claim that “children know themselves,” the few high-quality studies we have suggest that gender dysphoria in kids most often resolves during puberty, as they develop and mature and gain a deeper understanding of the interplay between gender and sexuality. Many grow up to be gay.
These findings fly in the face of claims by activist groups that the science is settled and that gender-affirming care is “evidence-based” and “lifesaving.” But the findings also don’t negate the fact that some young people are deeply grateful to have transitioned.
Cass isn’t calling for a complete ban on youth gender interventions, like the bans many Republican states have enacted. Nor is she arguing for removing barriers to these interventions and making them more accessible without parental knowledge or consent, as many Democrats advocate. Her recommendation is to expand services but root them in holistic psychological care, making sure all other mental health issues are attended to. She is suggesting the end of the specialized gender clinic model, where gender dysphoria is viewed as the root of all distress.
Without that broader approach to treatment, she says, directly addressing the thousands of youths distressed about their gender, “you are not getting the wider support you need in managing any mental health problems, arranging fertility preservation, getting help with any challenges relating to neurodiversity, or even getting counselling to work through questions and issues you may have.”
The Cass Review offers 32 recommendations, including exercising “extreme caution” when prescribing cross-sex hormones to those 16 and younger and having provisions for people considering detransition. Cass calls for long-term follow-up of those who have transitioned or sought care and a commitment to lifelong care for both those who transition and those who detransition. In contrast, Democrats have blocked attempts to pass detransition care bills and amendments that would require insurers to cover reconstructive surgeries, hormone treatments, and other assistance for detransitioners who want to live as their natal sex again, in whatever way is possible after permanent changes. Detransitioners are often left with nowhere to go to attend to their bodies or their minds — as the case used to be for trans people (and may be the case again).
Increasingly, some providers are so intimidated by the noise around this issue that they don’t want to attend to kids with gender issues at all. But these young people, as Cass says, “must have the same standards of care as everyone else.”
In America, the main problem with the issue of how best to treat kids with gender distress is that it has become intertwined with politics. Some who object to the affirmative model or question it fear the personal and professional repercussions of being cast as a bigot. Some who support the affirmative model in red states that are criminalizing the care fear being jailed. “There are few other areas of healthcare where professionals are so afraid to openly discuss their views, where people are vilified on social media, and where name-calling echoes the worst bullying behaviour,” Cass writes. “This must stop.”
As someone writing a book about the youth gender culture war, I couldn’t agree more. Polarization, the stifling of debate, and invective-flinging have left many families ill informed, making decisions in the dark and often based on fears of suicide that are unsupported by evidence. How can there truly be informed consent when there is so little unambiguous information, when there are more unknowns than knowns? And what do we do in the face of uncertainty? Argue and legislate, or gather data? It doesn’t help when our federal government contributes to the faux certainty, declaring that gender-affirming care is “suicide prevention” or “well-established medical practice” — arguments the Cass Review eviscerates.
For much of Europe, our government’s digging in on these treatments rather than investigating them more fully is just another way America has gone astray. Countries such as Finland and Sweden have analyzed the evidence and crafted more cautious guidelines, with psychological support as the baseline intervention.
We, too, need new, evidence-based guidelines. We need follow-up from all youth who transitioned, those who detransitioned, and those who desisted — meaning they stopped identifying as transgender without medically transitioning. We need to speak with multiple and competing stakeholders, and we need Democrats and Republicans to listen to those who’ve been helped and those who’ve been hurt; we need bipartisanship, not polarization. We need to push past politics and create an environment where robust scientific debate is not only tolerated but celebrated.
The National Health Service itself applauded Cass’s work, writing that it “will not just shape the future of health care in this country for children and young people experiencing gender distress but will be of major international importance and significance.” Let’s use the report to call for a ceasefire in the American gender culture war. We need our own Cass Review.
#Lisa Selin Davis#Cass Review#Cass Report#Hilary Cass#Dr. Hilary Cass#medical corruption#medical scandal#medical mutilation#systematic review#gender affirming care#gender affirming healthcare#gender affirmation#queer theory#gender identity ideology#gender ideology#intersectional feminism#religion is a mental illness
3 notes
·
View notes
Text
By: Adam B. Coleman
Published: Apr 17, 2024
Recently I was driving through an affluent neighborhood outside of Boston and I saw more "Black Lives Matter" flags on one street than I've ever seen in totality in any black majority working-class neighborhood.
If I were to presume that most of the people who live in this area are white, why do they feel the need to brandish this flag more so than black people? It only makes sense if "Black Lives Matter" were using the image of black people as a front for an upper-class religion.
Most people agree with black lives matter as a sentiment, including me, but for many it's a way to signal to other ideological believers where they stand and differentiate themselves from the non-believers.
It's no different than if I wore a cross on my chest to let others know about my faith in Christ: they want to signal to the world their social justice & economic status. Within their class bubble, this is how they measure their righteousness against others within their enclave.
That flag has nothing to do with me as a black person but instead has everything to do with making upper-class suburbanites feel less guilty about their social status and elevate their moral standing amongst their social circle.
They find affirmation about us needing them as our faux saviors through other upper-class blacks, especially the academics who are well-versed in their ideological scripture and reject people like me as being false prophets attempting to lead them astray.
Sometimes when people are void of significant problems, they manufacture their own or adopt other people's problems. I believe a significant reason why this ideology holds so strongly amongst the wealthy is because it gives them purpose and an issue to strive to resolve.
However, regular people who are just trying to make ends meet don't need to create problems that aren't there: they have enough of them already. They don't generally have an ego that accepts the possibility of how they can become the saviors of the world, one flag at a time.
Coincidentally, on that same street, those same houses all had LGBT flags and "hate has no home here" lawn signs: It was like driving through an internet meme mocking the ideological left.
Because they rarely leave their bubble, they can't see the absurdity in their actions. They are distant from the demographics they claim to champion, making their advocacy theoretical and improbable for them to bring a resolution to the problems they claim are abundant.
Personally, I am skeptical about anyone who attempts to state their character unprovoked. When I see a neighborhood like that which is trying to convey that they are good people, I think to myself "If you're moral people, you don't need to tell me this: It will shine through."
I worry that there is a segment of wealthy Americans who are insecure about their morality, which is why they quickly bought into a narrative about them being inherently racist or immoral based on what they look like. Maybe this is their way to repent for their sins?
The reason we are being inundated with racial fallacies, outrageous claims, and ideological bent in our media coverage, entertainment, and legislation is that the people who dominate in these fields have all graduated from the same seminary-esque liberal universities.
What's very clear to me is that the flourishing of radical left-wing ideology is fueled by those who reign at the top of the economic ladder. They are disconnected from the rest of us & can't see the ridiculousness of what they're doing because their bubble only reflects their image.
#Adam B. Coleman#BLM#Black Lives Matter#virtue signal#virtue signalling#virtue signaling#white savior complex#white saviorism#white savior#woke#wokeness#cult of woke#wokeness as religion#wokeism#religion is a mental illness
8 notes
·
View notes
Text
By: Christopher F. Rufo
Published: Apr 17, 2024
Katherine Maher has a golden résumé, with stints and affiliations at UNICEF, the Atlantic Council, the World Economic Forum, the State Department, Stanford University, and the Council on Foreign Relations. She was chief executive officer and executive director of the Wikimedia Foundation. And, as of last month, she is CEO of National Public Radio.
Mere weeks into this new role, Maher has stepped into controversy. Long-time NPR senior editor Uri Berliner published a scathing indictment of the self-professed “public” media service’s ideological capture. Rather than address the substance of these criticisms—which will ring true to anyone who has listened to NPR over the past decade—Maher punished Berliner with a five-day unpaid suspension. (Berliner announced his resignation from NPR earlier today.)
But Maher has another problem: her archive of 29,400 tweets.
I have spent the past few days exploring Maher’s prolific history on social media, which she seems to have used as a private diary, narrating her every thought, emotion, meeting, and political opinion in real-time. This archive is a collection of her statements, but at a deeper level, it provides a window into the soul of a uniquely American archetype: the affluent, white, female liberal—many of whom now sit atop our elite institutions.
What you notice first about Maher’s public speech are the buzzwords and phrases: “structural privilege,” “epistemic emergency,” “transit justice,” “non-binary people,” “late-stage capitalism,” “cis white mobility privilege,” “the politics of representation,” “folx.” She supported Black Lives Matter from its earliest days. She compares driving cars with smoking cigarettes. She is very concerned about “toxic masculinity.”
On every topic, Maher adopts the fashionable language of left-wing academic theory and uses it as social currency, even when her efforts veer into self-parody. She never explains, never provides new interpretation—she just repeats the phrases, in search of affirmation and, when the time is right, a promotion.
Maher understands the game: America’s elite institutions reward loyalty to the narrative. Those who repeat the words move up; those who don’t move out.
Next, you notice the partisanship. Maher was “excited” about Elizabeth Warren in 2012. She “just [couldn’t] wait to vote” for Hillary in 2016. She once had a dream about “sampling and comparing nuts and baklava on roadside stands” with Kamala Harris. She worked to “get out the vote” in Arizona for Joe Biden but slightly resented being called a “Biden supporter”; for her, it was simply a matter of being a “supporter of human rights, dignity, and justice.”
Donald Trump, on the other hand, is a “deranged racist sociopath.”
If you read Maher’s tweets closely, you also get glimpses of the human being. She spent much of her time in airports, taxis, meetings, and conferences. She expressed anger over the fact that most first-class flyers were white men, then noted that she went straight “to the back of the bus.” In her thirties, unmarried and without children, she felt the need to explain that “the planet is literally burning” and that she could not, in good conscience, “bring a child into a warming world.”
Behind the frenetic activity and the moral posturing, you wonder. Maher once posted her daily routine, which involved yoga, iced coffee, back-to-back meetings, and Zoom-based psychotherapy. She resented being served maternity advertisements on Instagram, she said. She was not “currently in the market for a baby” and would not be “tending her ovaries” according to the dictates of American capitalism.
Americans, even CEOs, are entitled to their opinions and to their own life decisions, of course. But the personal and psychological elements that suffuse Maher’s public persona seem to lead to political conclusions that are, certainly, worthy of public criticism.
The most troubling of these conclusions is her support for radically narrowing the range of acceptable opinions. In 2020, she argued that the New York Times should not have published Senator Tom Cotton’s op-ed, “Send in the Troops,” during the George Floyd riots. In 2021, she celebrated the banishment of then-president Donald Trump from social media, writing: “Must be satisfying to deplatform fascists. Even more satisfying? Not platforming them in the first place.”
As CEO of the Wikimedia Foundation, Maher made censorship a critical part of her policy, under the guise of fighting “disinformation.” In a speech to the Atlantic Council, an organization with extensive ties to U.S. intelligence services, she explained that she “took a very active approach to disinformation,” coordinated censorship “through conversations with government,” and suppressed dissenting opinions related to the pandemic and the 2020 election.
In that same speech, Maher said that, in relation to the fight against disinformation, the “the number one challenge here that we see is, of course, the First Amendment in the United States.” These speech protections, Maher continued, make it “a little bit tricky” to suppress “bad information” and “the influence peddlers who have made a real market economy around it.”
Maher’s general policy at Wikipedia, she tweeted, was to support efforts to “eliminate racist, misogynist, transphobic, and other forms of discriminatory content”—which, under current left-wing definitions, could include almost anything to the right of Joe Biden.
The new CEO of NPR, then, is a left-wing ideologue who supports wide-scale censorship and considers the First Amendment an impediment to her campaign to sanitize the world of wrong opinions.
Maher is no aberration. She is part of a rising cohort of affluent, left-wing, female managers who dominate the departments of university administration, human resources, and DEI. They are the matriarchs of the American Longhouse: they value safety over liberty, censorship over debate, and relativism over truth.
Each social gambit is designed for smothering the institution in ideology. Maher says that she knows “that hysteric white woman voice.” She has “done it.” And while she might not be proud of it—she is aware that she has “a big fat privilege pass”—she is willing to do what it takes to move the dictates of conventional left-wing opinion into a position of domination.
It didn’t begin at NPR, and it won’t end there.
--
==
The First Amendment being viewed as an impediment to what she wants to do, is not a good look for the CEO of a publicly (i.e. government, i.e. taxpayer) funded broadcaster.
4 notes
·
View notes
Text
By: Gabriel Nadales
Published: Apr 17, 2024
One night I was driving down I-5 in California, when I decided to stop off the side of the road for some tacos. But as soon as I pulled up into a restaurant I saw two kittens in the parking lot. At first, I got really excited because I absolutely love animals. In fact, I have three cats and two dogs. And while they are a lot of work, especially now that I am a father, I can’t imagine my home without them.
Before I got my food I decided I needed to pet these kittens, so I called one over. As I was petting her I realized she was a stray. I then noticed that she had a little bit of a belly. She was pregnant.
I sighed to myself and thought, “Well tonight’s going to be a long night.”
And it was, because I spent well over an hour trying to catch these gray tabbies so I could find them homes, well knowing that I had at least 5 more hours left in my trip that night.
You see, I'm an activist. For as long as I can remember I’ve been passionate about helping others to make the world a better place.
My dad’s passion for helping
To understand my passion for helping others I need to talk about my dad.
“A manos llenas” is a phrase in Spanish that means to give with all your heart. That saying also sums up my dad.
I remember my mom told me that my dad worked for 5 years to save up money to buy his first car, only to sell it shortly after to help my cousin when he got into legal trouble.
My dad used to be a manager at a chemical factory. He was willing to go to work 6 to 7 days a week, putting in 15 hours a day, just so his workers didn’t have to come in on the weekend.
“Mi papa se quita el pan de la boca para darle a la gente.” -- “My dad takes bread out of his mouth to give to others.”
My dad taught me to care about others and he is the reason I became an activist. And my passion for helping people is the reason I joined Antifa.
Antifa is a movement composed of countless far-left activists which use physical violence and intimidation. They typically wear all black and cover their faces with a bandana at demonstrations to avoid getting arrested. Nowadays, if you hear on the news that someone threw a molotov cocktail at police during a demonstration, you can probably bet it was someone marching under the banner of Antifa.
But, wait a second—how in the world does joining a radical movement like Antifa help others?
Why I joined Antifa
To understand my reasons for joining the Antifa movement, it is important that I speak from the heart of a young activist.
I’ve been an activist since 2006 when I was only 12 years old. Ever since then I have been passionate about making a difference in my community.
My first protest was in the 6th grade. I remember my friends and I marching all over the school chanting “Sí se puede!” to show our support for undocumented Mexican immigrants. It was an exciting feeling. I felt like I was part of something big and that we were finally going to make a difference.
And then nothing happened.
A short time later, I passed out hundreds of anti-war flyers throughout my community and my school, and one of my teachers said to me she was happy to see me, a young boy, getting involved because I was the future of this country.
That felt really good because I realized people could see that I was a part of something bigger than myself.
And then, the wars continued.
This went on for a while. When you’re an activist there is such a thing as activist fatigue. You get tired of marching. You get tired of passing flyers. You get tired of yelling chants because no one seems to listen and nothing seems to change.
So after years of fighting against injustice, I started getting tired because nothing I did seemed to work. So when I turned 17 I adopted a new mentality: I want change. And I want it now.
And it was with this mentality that in 2011, when neo-nazis came to my community, I attended the protest that changed my life.
At this counter-protest, I dressed in all black and I covered my face with a bandana just like Antifa does. I was ready to do more than just hold a sign. But as I arrived at the park, I didn’t know where to start, so I just stood under a tree.
I have to admit it was a little awkward, I thought I was the only one dressed in all black, but it didn’t take long for another anarchist to notice me and ask me if I wanted to roll with him and his friends to oppose the Nazis head-on.
That’s how I joined Antifa.
And for well over a year and a half, I was ready at a moment's notice to put on a black mask to engage in what we called “direct action” which is when you don’t ask for change, you take it.
To give you an example, there was this company in California that my friends told me was transporting monkeys to America to conduct vivisections. As someone who loves animals, I could not stand for it.
Normally, an activist would write letters, maybe hold some signs outside the corporate building, or try to get the government to take action. But no. That's not direct action.
Instead, my friends and I went to the home of that CEO to harass him and yell obscenities. And we threatened that if he did not stop his company’s policies we would come back.
Beginning to have doubts
The more I got involved with this radical faction the more I began to realize that virtually no one took the time to ask, “Is what I am doing the right thing?” People didn’t want to consider other viewpoints, instead, people just wanted to critique “the other side.”
That’s not ever been my style. I’ve always been a curious person, a curious activist, it’s the same reason I stopped for those kittens. I ask a lot of questions.
Well, around this time I began learning about free-market ideals and I was particularly interested in intellectuals like Milton Friedman and Thomas Sowell. To be clear, I didn’t like them, but I found them interesting. So interesting that I wanted to talk about their ideas with my friends.
So I went with my fellow anarchist friends and I started talking about the free-market, the tragedy of the commons, and all that. I’m questioning our ideals—I'm super excited, and one of them turns to me and says, “You capitalist pig.”
There’s that passion I’m talking about. My friend was so passionate about anarchism that he was unwilling to hear anything that challenged his beliefs, and suddenly, I was his enemy, just for asking questions.
It was my passion that told me that if I wanted to make the world a better place then I needed to get radical, so I joined Antifa.
But I was discovering that passion without reason is dangerous.
My mom’s reason and patience.
“Estas bien loco.” These are the words I’ve heard my mom tell me time after time whenever I act solely on passion, and they mean, “You’re freaking crazy.”
But let me tell you about her.
I remember when we were in Mexico saving up to come to America. My mom would give us only a cup of milk and exactly eight “Galletas Marias” for supper—which is a little cheap Mexican cookie. And then when I was little I fell off a bunk bed and hit my head. My cranium sunk as if you hit a deflated ball. You can still feel it.
The doctors told my parents that I would grow up with mental disabilities.
Thankfully the doctors were wrong. But my mom decided to better herself to help me. She went back to school to study child psychology to learn how to help me.
My mom is such a wonderful person and she is incredibly kindhearted, but she has a different outlook on life than my dad. She believes that to make the world a better place you first have to take care of yourself. But more importantly, you have to think about your actions before you act on them.
My mom is a rational person who thinks things through, and that has helped her develop a great patience. Which is lucky, because she always has to deal with my dad and I.
My mom is the reason I left Antifa.
Three lessons for change
There is a common joke that if you are young and conservative you have no heart, but if you are old and liberal you have no brains. Well, I’m here to ask: Why can’t you be both? Why does society think it is so difficult to be both compassionate and rational?
My mom didn’t make me leave Antifa, just like my dad didn’t make me join it. But their individual approaches to life taught me a critical lesson: there is a balance between being passionate and having the patience to see things through. And if you want real change, you need this balance.
In order to get this balance, you need to do three things.
If you are passionate about a particular cause and want to achieve lasting change you need to ask a lot of questions. One of the worst things that can happen to you as an activist is that you work for years to achieve your goal only to realize you were working for something that was negative. Asking questions will slow down your passion and help you find your true purpose.
Just imagine if I had not asked questions while I was in Antifa. I have no doubt in my mind that if I would have continued my involvement in the Antifascist movement. I would have ended up in jail.
But now, say you’re a very rational person who asks a lot of questions. That’s not enough. Remember why you’re doing this in the first place. Find your passion. Get out there and make some noise.
Put yourself out there and talk with the “other side.” Because when you have conversations with all parties you begin to make your case to the world. And in politics, nothing moves unless it is pushed.
And third, remember that small steps lead to change, so be patient. It may not feel like it. But every flier you pass and every person you talk to does create a change. And when you work for something long and hard enough, eventually you will see that change.
Bringing it together
I’ve been an activist for 18 years. First as a left-wing radical, but now as a free speech advocate. And as a free speech activist, I’ve had the opportunity to mentor many activists. One person I used to mentor was a guy named Hayden.
Now Hayden is a great guy and a valued friend of mine. But when I met him I knew that he was an “act first, think later” kind of guy, like my dad.
And unfortunately, a hazard of being an activist is sometimes being confronted by violent people. In fact, both Hayden and I have been attacked numerous times while pushing back against censorship on college campuses.
And predictably, after getting punched in the face, Hayden would fight back. But that only made things worse. So after the third time it happened, I talked to him and I told him, “I know you’re passionate, and I know it sucks to get punched in the face, but be patient and don’t get dragged into a fight. That will only make everything worse.”
And then I sent him to UC Berkeley. It happened again. And this time, it was caught on film. But this time, Hayden listened to me and remained calm.
That punch was dubbed “The Punch Seen Around the World.” And it was seen everywhere. Even the White House saw it—and it made everyone realize that free speech is in danger.
And as a result, President Trump invited hundreds of students who have been silenced on college campuses, as well as Hayden and myself, to the White House to witness him sign an executive order to defend free speech on college campuses.
And the best part is that nearly 3 out of 4 voters—73% of Americans—supported the executive order. We had finally found some common ground.
My lesson for young activists
Hayden and I cannot take all the credit for this historic executive order. Thousands of free-speech activists had been working for years to get something like this on the books. But, Hayden and I were the catalysts for it to happen because we had that balance of passion and patience.
Finding that balance can be hard, especially when you get punched in the face. But let’s look at the flipside.
There are countless activists who are driven solely by passion. And if you want to see what unrestrained passion looks like, just take a look at the "passionate activists" who destroyed innocent communities in the name of police reform during the 2020 riots.
Everyone in the Antifa community has one thing in common: everyone is passionate about helping. I’m still an activist. I am still passionate about helping people and animals, but passion without reason can be truly dangerous and can end up hurting more than it helps.
The reason we were able to get an executive order signed was because our passion helped us by putting ourselves out there, but because we also had the patience not to act solely on that passion.
If all you have is passion, then you may act out in a manner that ends up hurting others. But if all you have is rational and patient thinking, then you may miss out on the joys of helping others.
If you want real change, then you need passion, reason, and patience.
You need passion to drive you forward. But you need reason to be able to steer in the right direction. But overall, you need the patience to remind yourself that the changes you want to see will one day come.
#Gabriel Nadales#Antifa#direct action#antifa thugs#free speech#freedom of speech#woke authoritarianism#irrational#antifa violence#emotional reasoning#religion is a mental illness
0 notes
Text

By: Mary McCool
Published: Apr 18, 2024
Scotland's NHS has paused prescribing puberty blockers to children referred by a gender identity clinic.
The Sandyford clinic in Glasgow also said new patients aged 16 or 17 would no longer receive other hormone treatments until they were 18.
It follows a landmark review of gender services for under-18s in England.
Dr Hilary Cass's review said children had been let down by a lack of research and there was "remarkably weak" evidence on medical interventions.
NHS England confirmed it would stop prescribing puberty blockers in March.
Puberty blockers work by suppressing the release of hormones that cause puberty and are often prescribed to children questioning their gender as a way of stopping physical changes such as breast development or facial hair.
Like other parts of the UK, Scotland has seen a rapid rise in the number of young people questioning their identity or experiencing gender dysphoria.
The only specialist service for under-18s is the Sandyford clinic in Glasgow, where people can self-refer or can be referred through their GP.
Figures released to BBC Scotland News under a freedom of information request, showed that at the end of 2023, 1,100 patients were on the waiting list.
As well as referrals for puberty blockers, the Sandyford also refers patients for "gender affirming hormones" such as testosterone or oestrogen to 16 and 17-year-olds.
In the NHS in England, fewer than 100 children - who had already started a prescription - are now taking puberty blockers.
In Scotland, the number is likely to be far smaller.
Following the position taken by NHS England, NHS Greater Glasgow and Clyde (NHSGGC) and NHS Lothian deferred starting new patients on the treatment in mid-March.
The Glasgow health board said patients had now been formally notified, however existing patients currently receiving treatment would not be affected.
Dr Emilia Crighton, NHSGCC's director of public health said: "The findings informing the Cass review are important, and we have reviewed the impact on our clinical pathways.
"The next step from here is to work with the Scottish government and academic partners to generate evidence that enables us to deliver safe care for our patients."
Review findings 'considered'
Scottish Health Secretary Neil Gray welcomed the decision, saying the government and health boards are considering the recommendations of the Cass review.
He said: "We have been clear it is for clinicians and health boards to make decisions about clinical pathways, and that these decisions should be made carefully and based on the best evidence available.
"This is what both health boards have done and their position is supported by the chief medical officer.
"More broadly, the Cass review's final report and findings are being closely considered by both the Scottish government and health boards, in the context of how such healthcare can be best delivered in Scotland."
Vic Valentine, of Scottish Trans and the Equality Network, said pausing puberty blockers was the wrong decision and said it would "harm trans children and young people".
A statement said: "This decision has been taken within the context where the reality of trans people's experiences and lives is questioned almost daily in some of the media and some political circles.
"This makes us worry that the decision has been influenced by that context rather than solely through consideration of the best interests of trans children and young people."
Scottish Conservative deputy leader Meghan Gallacher said the decision was "long overdue" and accused the government of leaking the news to the press "before having the decency to update parliament".
She called for an urgent ministerial statement so MSPs had a chance to ask questions on the matter.
She said: "I'm beyond fed up with this lackadaisical approach to gender care. They are failing children and young people."
--
==
"Social Murder Charter" is the best band name ever.
#Mary McCool#Scotland#Sandyford#medical scandal#medical corruption#Cass Review#Cass Report#Dr. Hilary Cass#Hilary Cass#puberty blockers#cross sex hormones#wrong sex hormones#ideological corruption#queer theory#gender identity ideology#gender ideology#intersectional feminism#social murder charter#trans genocide#religion is a mental illness
1 note
·
View note
Text
youtube
Abused By My Girlfriend tells the remarkable story of Alex Skeel, a 23-year-old man from Bedford who survived an abusive relationship with his girlfriend Jordan Worth.
Combining observational filming with personal and police archive, this film provides a raw and uninhibited window into a teenage romance that descended into terrible violence.


Alongside Alex's shocking and thought-provoking testimony, his family and friends also share their stories of seeing him slowly slip away, powerless to stop it, and unaware of how bad it would get.


Bedfordshire Police described Alex's case as one of the most extreme cases of domestic violence they had ever dealt with. In hospital, doctors examined Alex's body and told him that he was just ten days away from death.

In April 2018, Jordan was sentenced to seven and a half years in prison. She became the first female in the UK to be convicted of coercive and controlling behaviour.


By sharing his story, Alex hopes to challenge assumptions about violence and masculinity in relationships, and to empower victims of domestic violence to come forward.
--
Interviews with Alex.
youtube
youtube
I didn't know if I was to leave-- I've come across so many men that haven't won in the family courts and gotten the best deal out of it. And that was-- to be honest with you, during the time I never really thought about leaving. It was just purely, is the next day going to be better than the last and it's survival mode, you're just constantly protecting yourself at all times. And I never actually thought about it, and people have asked, do I think people should know anything before, and I genuinely didn't think. It was all about just like a boxer in a ring, keep your hands up.
I was pretty much-- I actually genuinely was waiting to just die. Because I just kept hoping that the next day maybe one less hit on the head or one less stab or I didn't get boiling water. Because if that was the case, it would be a far better day than the day before.
#Alex Skeel#Abused By My Girlfriend#Jordan Worth#domestic violence#domestic abuse#male victims of domestic violence#male victims of domestic abuse#male victims#violent women#female abusers#coercive control#religion is a mental illness
6 notes
·
View notes
Text
By: Jonathan Haidt
Published: Mar 24, 2024
Those born after 1995, argues Jonathan Haidt in his new book, were the first people in history to go through puberty with a portal to an alternative universe in their pockets – and the toll this has taken on their wellbeing has been devastating
Suppose that when your first child turned nine, a visionary billionaire whom you’d never met chose her to join the first permanent human settlement on Mars. Unbeknown to you, she had signed herself up for the mission because she loves outer space, and, besides, all of her friends have signed up. She begs you to let her go.
You hear her desire, so before saying no, you agree at least to learn more. You learn that the reason they’re recruiting children is because they will better adapt to the unusual conditions of Mars than adults. If children go through puberty and its associated growth spurt on Mars, their bodies will be permanently tailored to it, unlike settlers who come over as adults.
You find other reasons for fear. First, there’s the radiation, against which Mars does not have a protective shield. And then there’s the low‐gravity environment, which would put children at high risk of developing deformities in their skeletons, hearts, eyes, and brains. Did the planners take this vulnerability of children into account? As far as you can tell, no.
So, would you let her go? Of course not. You realise this is a completely insane idea – sending children to Mars, perhaps never to return to Earth. The project leaders do not seem to know anything about child development and do not seem to care about children’s safety. Worse still: the company did not require proof of parental permission.
No company could ever take our children away and endanger them without our consent, or they would face massive liabilities. Right?
At the turn of the millennium, technology companies created a set of world-changing products that transformed life not just for adults all over the world but for children, too. Young people had been watching television since the 1950s but the new tech was far more portable, personalised and engaging than anything that came before. Yet the companies that developed them had done little or no research on the mental health effects. When faced with growing evidence that their products were harming young people, they mostly engaged in denial, obfuscation, and public relations campaigns. Companies that strive to maximise “engagement” by using psychological tricks to keep young people clicking were the worst offenders. They hooked children during vulnerable developmental stages, while their brains were rapidly rewiring in response to incoming stimulation. This included social media companies, which inflicted their greatest damage on girls, and video game companies and pornography sites, which sank their hooks deepest into boys. By designing a slew of addictive content that entered through kids’ eyes and ears, and by displacing physical play and in-person socialising, these companies have rewired childhood and changed human development on an almost unimaginable scale.
What legal limits have we imposed on these tech companies so far? Virtually none, apart from the requirement for children under 13 to get parental consent before they can sign a contract with a company. But the law in most countries didn’t require age verification; so long as a child checked a box to assert that she was old enough (or put in the right fake birthday), she could go almost anywhere on the internet – and sign into any social media app – without her parents’ knowledge or consent. (The law is being tightened in the UK, due to the 2023 Online Safety Act, and is under review in the US.)
Thus, the generation born after 1995 – gen Z – became the first generation in history to go through puberty with a portal in their pockets that called them away from the people nearby and into an alternative universe that was exciting, addictive and unstable. Succeeding socially in that universe required them to devote a large part of their consciousness to managing what became their online brand, posting carefully curated photographs and videos of their lives. This was now necessary to gain acceptance from peers, the oxygen of adolescence, and to avoid online shaming, the nightmare of adolescence. Gen Z teenagers got sucked into spending many hours of each day scrolling through the shiny happy posts of friends, acquaintances and distant influencers. They watched increasing quantities of user-generated videos and streamed entertainment, fed to them by algorithms that were designed to keep them online as long as possible. They spent far less time playing with, talking to, touching, or even making eye contact with their friends and families, thereby reducing their participation in social behaviour that is essential for successful human development.
The members of gen Z are, therefore, the test subjects for a radical new way of growing up, far from the real‐world interactions of small communities in which humans evolved. Call it the Great Rewiring of Childhood. It’s as if they became the first generation to grow up on Mars. And it has turned them into the Anxious Generation.
There was little sign of an impending mental illness crisis among adolescents in the 2000s. Then, quite suddenly, in the early 2010s, things changed. In just five years between 2010 and 2015, across the UK, the US, Canada, Australia and beyond, the number of young people with anxiety, depression and even suicidal tendencies started to rise sharply. Among US teenagers, those who reported experiencing a long period of feeling “sad, empty, or depressed” or a long period in which they “lost interest and became bored with most of the things they usually enjoy” – classic symptoms of depression – surged by roughly 150%. In other words, mental illness became roughly two and a half times more prevalent. The increases were similar for both sexes and happened across all races and social classes. And among a variety of mental health diagnoses, anxiety rates rose the most.
More recent data for 2020 was collected partly before and partly after the Covid shutdowns, and by then one out of every four American teen girls had experienced a major depressive episode in the previous year. Things got worse in 2021, but the majority of the rise was in place before the pandemic.
I addressed some of these issues in The Coddling of the American Mind, a book [about modern identity politics and hypersensitivity on university campuses] I wrote in 2017 with free speech campaigner Greg Lukianoff. The day after we published, an essay appeared in the New York Times with the headline: “The Big Myth About Teenage Anxiety.” In it, a psychiatrist raised several important objections to what he saw as a rising moral panic around teenagers and smartphones. He pointed out that most of the studies showing a rise in mental illness were based on “self‐reports”, which does not necessarily mean that there is a change in underlying rates of mental illness. Perhaps young people just became more willing to self‐diagnose or talk honestly about their symptoms? Or perhaps they started to mistake mild symptoms of anxiety for a mental disorder?
Was the psychiatrist right to be sceptical? He was certainly right that we need to look at multiple indicators to know if mental illness really is increasing. A good way to do that is to look at changes in figures not self‐reported by teens. For example, the number of adolescents brought in for emergency psychiatric care, or admitted to hospitals each year because they deliberately harmed themselves, either in a suicide attempt, or in what is called non‐suicidal self-injury, such as cutting oneself without the intent to die.
The rate of self‐harm for young adolescent girls nearly tripled from 2010 to 2020. The rate for older girls (ages 15–19) doubled, while the rate for women over 24 actually went down during that time. So whatever happened in the early 2010s, it hit preteen and young teen girls harder than any other group. Similarly, the suicide rate for young adolescents increased by 167% from 2010 to 2021.
The rapid increases in rates of self‐harm and suicide, in conjunction with the self‐report studies showing increases in anxiety and depression, offers a strong rebuttal to those who were sceptical about the existence of a mental health crisis. I am not saying that none of the increase in anxiety and depression is due to a greater willingness to report these conditions (which is a good thing) or that some adolescents began pathologising normal anxiety and discomfort (which is not a good thing). But the pairing of self‐reported suffering with behavioural changes tells us that something big changed in the lives of adolescents in the early 2010s.Quick Guide
The arrival of the smartphone in 2007 changed life for everyone. Of course, teenagers had mobile phones since the late 1990s, but they were basic flip phones with no internet access, mostly useful for communicating directly with friends and family, one‐on‐one. Some adolescents had internet access via a home computer or laptop but it wasn’t till they got smartphones that they could be online all the time, even when away from home. According to a survey conducted by the US non-profit group Common Sense Media, by 2016, 79% of teens owned a smartphone, as did 28% of children between the ages of eight and 12.
As teenagers got smartphones, they began spending more time in the virtual world. A Common Sense report, in 2015, found that teens with a social media account reported spending about two hours a day on social media and around seven hours a day of leisure time online. Another 2015 report, by the Washington thinktank Pew Research, reveals that one out of every four teens said that they were online “almost constantly”. By 2022, that number had nearly doubled, to 46%. These “almost constantly” numbers are startling, and may be the key to explaining the sudden collapse of adolescent mental health. These extraordinarily high rates suggest that even when members of gen Z are not on their devices and appear to be doing something in the real world, such as sitting in class, eating a meal, or talking to you, a substantial portion of their attention is monitoring or worrying (being anxious) about events in the social metaverse. As the MIT professor Sherry Turkle wrote in 2015 about life with smartphones: “We are forever elsewhere.”
Faced with so many virtual activities, social media platforms and video streaming channels, many adolescents (and adults) lost the ability to be fully present with the people around them, which changed social life for everyone, even for the small minority that did not use these platforms. Social patterns, role models, emotions, physical activity, and even sleep patterns were fundamentally recast, for adolescents, over the course of just five years.
When I present these findings in public, someone often objects by saying something like: “Of course young people are depressed – just look at the state of the world in the 21st century. It began with the 9/11 attacks, the wars in Afghanistan and Iraq, and the global financial crisis. They’re growing up with global warming, school shootings in the US and elsewhere, political polarisation, inequality, and ever-rising student loan debt. Not to mention wars in Ukraine and the Middle East.”
But while I agree that the 21st century is off to a bad start, the timing does not support the argument that gen Z is anxious and depressed because of rising national or global threats. Even if we were to accept the premise that the events from 9/11 through to the global financial crisis had substantial effects on adolescent mental health, they would have most heavily affected the millennial generation (born between 1981 and 1995), who found their world shattered and their prospects for upward mobility reduced. But this did not happen; their rates of mental illness did not worsen during their teenage years. Also, had the financial crisis and other economic concerns been major contributors, adolescent mental health would have plummeted in 2009, the darkest year of the financial crisis, and it would have improved throughout the 2010s as the unemployment rate fell, the stock market rose, and the global economy heated up.
There is just no way to pin the surge of adolescent anxiety and depression on any economic event or trend that I can find.
When Covid arrived in 2020, the disease and the lockdowns made sociogenic illness more likely among people of any age. Covid was a global threat and a stressor. The lockdowns led teens to spend even more time on social media, especially TikTok, which was relatively new. But the steep rise in anxiety and depression among adolescents was in place well before the pandemic.
People don’t get depressed when they face threats collectively; they get depressed when they feel isolated, lonely, or useless.
Parents I talk to about smartphones, social media and video games tell stories of “constant conflict”. They try to lay down rules and enforce limits, but there are so many arguments about why a rule needs to be relaxed, and so many ways around the rules, that family life all over the world has come to be dominated by disagreements about technology. Maintaining family rituals such as mealtimes can feel like resisting an ever-rising tide.
A mother I spoke with in Boston told me about the efforts she and her husband had made to keep their 14- year-old daughter, Emily, away from Instagram. They could see the damaging effect it was having on her. To curb her access, they tried various ways to monitor and limit the app on her phone. However, life became a permanent struggle in which Emily eventually found ways around the restrictions. In one episode, she got into her mother’s phone, disabled the monitoring software, and threatened to kill herself if her parents reinstalled it. Her mother told me:
“It feels like the only way to remove social media and the smartphone from her life is to move to a deserted island. She attended summer camp for six weeks each summer where no phones were permitted – no electronics at all. When we picked her up from camp she was her normal self. But as soon as she started using her phone again it was back to the same agitation and glumness.”
Platforms such as Instagram – where users post content about themselves, then wait for the judgments and comments of others, and the social comparison that goes with it – have larger and more harmful effects on girls and young women than on boys and young men. The more time a girl spends on social media, the more likely she is to be depressed or anxious. Girls who say that they spend five or more hours each weekday on social media are three times as likely to be depressed as those who report no social media time. The difference is far less marked with boys. Girls spend more time on social media, and the platforms they are on – particularly Instagram and Snapchat – are the worst for mental health. A 2017 study in the UK asked teenage girls to rate the effects of the most popular social media platforms on different parts of their wellbeing, including anxiety, loneliness, body image, and sleep. Teenagers rated Instagram as the worst of the big five apps, followed by Snapchat. YouTube was the only platform that received a positive overall score.
The 2021 song Jealousy, Jealousy by Olivia Rodrigo sums up what it’s like for many girls to scroll through social media today. The song begins: “I kinda wanna throw my phone across the room/ ’Cause all I see are girls too good to be true.” Rodrigo then says that “co-comparison” with the perfect bodies and paper-white teeth of girls she doesn’t know is slowly killing her.
Psychologists have long studied social comparison and its pervasive effects. The American social psychologist Mark Leary says it’s as if we all have a “sociometer” in our brains – a gauge that runs from nought to 100, telling us where we stand in the local prestige rankings. When the needle drops, it triggers an alarm – anxiety – that motivates us to change our behaviour and get the needle back up. So what happened when most girls in a school got Instagram and Snapchat accounts and started posting carefully edited highlight reels of their lives and using filters and editing apps to improve their virtual beauty and online brand? Many girls’ sociometers plunged, because most were now below what appeared to them to be the average. All around the developed world, an anxiety alarm went off in girls’ minds, at approximately the same time.
A 13-year-old girl on Reddit explained how seeing other girls on social media made her feel, using similar words to Olivia Rodrigo:
i cant stop comparing myself. it came to a point where i wanna kill myself cause u dont want to look like this and no matter what i try im still ugly/feel ugly. i constantly cry about this. it probably started when i was 10, im now 13. back when i was 10 i found a girl on tiktok and basically became obsessed with her. she was literally perfect and i remember being unimaginably envious of her. throughout my pre-teen years, i became “obsessed” with other pretty girls.
Instagram’s owner, Facebook (now Meta), itself commissioned a study on how Instagram was affecting teens in the US and the UK. The findings were never released, but whistleblower Frances Haugen smuggled out screenshots of internal documents and shared them with reporters at the Wall Street Journal. The researchers found that Instagram is particularly bad for girls: “Teens blame Instagram for increases in the rate of anxiety and depression… This reaction was unprompted and consistent across all groups.”
If we confine ourselves to examining data about depression, anxiety, and self-harm, we’d conclude that the Great Rewiring has been harder on girls than on boys. But there’s plenty of evidence that boys are suffering too.
A key factor was boys taking up online multiplayer video games in the late 2000s and smartphones in the early 2010s, both of which pulled them decisively away from face-to-face or shoulder-to-shoulder interaction. At that point, I think we see signs of a “mass psychological breakdown”. Or, at least, a mass psychological change. Once boys had multiple internet-connected devices, many of them got lost in cyberspace, which made them more fragile, fearful, and risk averse on Earth. Beginning the early 2010s, boys across the western world began showing concerning declines in their mental health. By 2015, a staggering number of them said that they had no close friends, that they were lonely, and that there was no meaning or direction to their lives.
The overwhelming feeling I get from the families of both boys and girls is that they are trapped and powerless in the face of the biggest mental health crisis in history for their children. What should they – what should we – do?
When I say that we need to delay the age at which children get smartphones and social media accounts, the most common response is: “I agree with you, but it’s too late.” It has become so ordinary for 11-year-olds to walk around staring at their phones, swiping through bottomless feeds, that many people cannot imagine that we could change it if we wanted to. “That ship has sailed,” they tell me.
Yet we are not helpless. It often feels that way because smartphones, social media, market forces, and social influence combine to pull us into a trap that social scientists call a collective action problem. Children starting secondary school are trapped in a collective action problem when they arrive for their first day and see that some of their classmates have smartphones and are connecting on Instagram and Snapchat, even during class time. That puts pressure on them to get a smartphone and social media as well.
It’s painful for parents to hear their children say: “Everyone else has a smartphone. If you don’t get me one, I’ll be excluded from everything.” Many parents therefore give in and buy their child a smartphone at age 11, or younger. As more parents relent, pressure grows on the remaining kids and parents, until the community reaches a stable but unfortunate equilibrium: Everyone really does have a smartphone.
How do we escape from these traps? Collective action problems require collective responses: parents can support one another by sticking together. There are four main types of collective response, and each can help us to bring about major change:
1. No smartphones before year 10
Parents should delay children’s entry into round-the-clock internet access by giving only basic phones with limited apps and no internet browser before the age of 14.
2. No social media before 16Let children get through the most vulnerable period of brain development before connecting them to an avalanche of social comparison and algorithmically chosen influencers.
3. Phone-free schoolsSchools must insist that students store their phones, smartwatches, and any other devices in phone lockers during the school day, as per the new non-statutory guidance issued by the UK government. That is the only way to free up their attention for one another and for their teachers.
4. Far more unsupervised play and childhood independenceThat’s the way children naturally develop social skills, overcome anxiety, and become self-governing young adults.
These four reforms are not hard to implement – if many of us do them at the same time. They cost almost nothing. They will work even if we never get help from our legislators or from the tech giants, which continue to resist pressure to protect young users’ safety and wellbeing. If most of the parents and schools in a community were to enact all four, I believe they would see substantial improvements in adolescent mental health within two years. Given that AI and spatial computing (such as Apple’s new Vision Pro goggles) are about to make the virtual world far more immersive and addictive, I think we’d better start today.
This is an edited extract from The Anxious Generation by Jonathan Haidt.
#Jonathan Haidt#The Anxious Generation#Generation Z#Gen Z#mental health#social media#smartphone#smart phones#social media influencers#self esteem#mental health issues#depression#anxiety#self harm#social comparison#psychology#human psychology#religion is a mental illness
1 note
·
View note
Text
"Iran has a right to 'fight back.'"
If those are the words that are coming out of your mouth, remember, you're not talking about the people of Iran. You're talking about the Islamic Republic.
You're talking about the IRGC (Iranian Revolutionary Guard Corps). This is one of the Iranian generals that were killed in the Damascus airstrike. Now, Mohammad here was a Quds (IRGC branch) commander. He helped execute and plan the October 7th massacre. He led Hezbollah's operations in Syria and Lebanon. And he also worked very closely with this guy. He also has the blood of Americans on his hands. So, this is what you're defending, not the people of Iran.
You claim that Israel hit a diplomatic compound, which, by the way, it did not. You can see it's still intact here. It did, however, hit the building next to it, which was being used as an IRGC base, which strips it of diplomatic immunity.

But here's the question. Is Israel, by your logic, allowed to fight back? When our borders are invaded? When the Republic's proxies killed 1200 of our people and are still holding 134 hostages? What about the seven months of almost daily bombardment from Hamas, Hezbollah and the Houthis? Are we allowed then?
When you defend the Islamic Republic, you're not speaking for the people of Iran. Iranians are saying this.

And this.

And this.
The real sad part is the people of Iran are the ones that have suffered at the hands of this regime the most. So please stop pretending that your genocidal fetish towards Israel's destruction is on behalf of the people of Iran.
#Iran#Israel#Islamic Republic of Iran#Iranian regime#Islamic regime#hit them israel#islamic terrorism#islam#hamas#hezbollah#houthis#hamas supporters#terrorism supporters#religion is a mental illness
11 notes
·
View notes
Text




For many, ground zero in gender equality advocacy is the #genderpaygap.
It’s perhaps the king of all tropes, from which discussion always seems to start, and inevitably returns too.
‘Yeah well, women are still paid less than men!’ You will hear, like some kind of broken record.
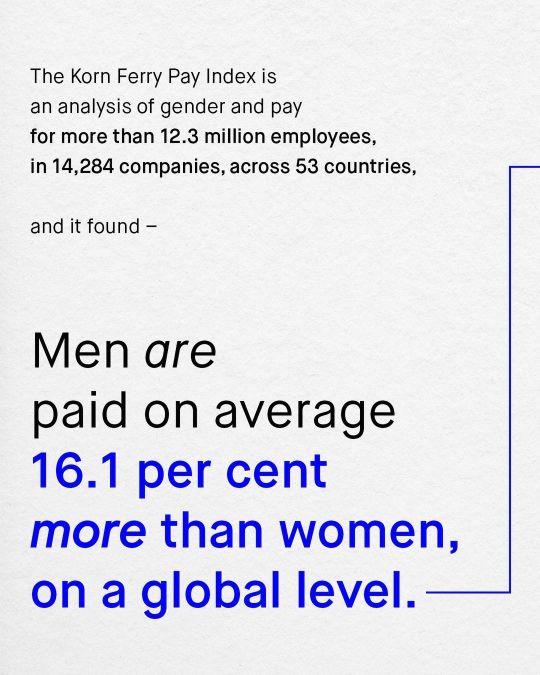
And this is true, they are – the average salary for women, is lower than the average salary for men.
But hold off the pitch forks, flaming torches, and cries of misogyny for a moment, as the picture changes if we ask, ‘are women paid less than men, for the same work?’
And to that, the answer is no.
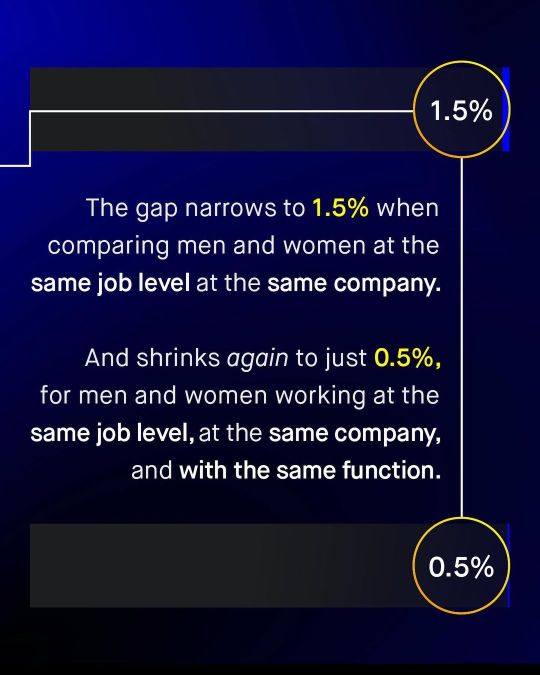
For whilst it’s true that ‘all women’ are paid 16% less than ‘all men’, the gap quickly dissolves and almost disappears completely (to just 0.5%), when comparing women with men working the same job level, with the same function, and at the same company.
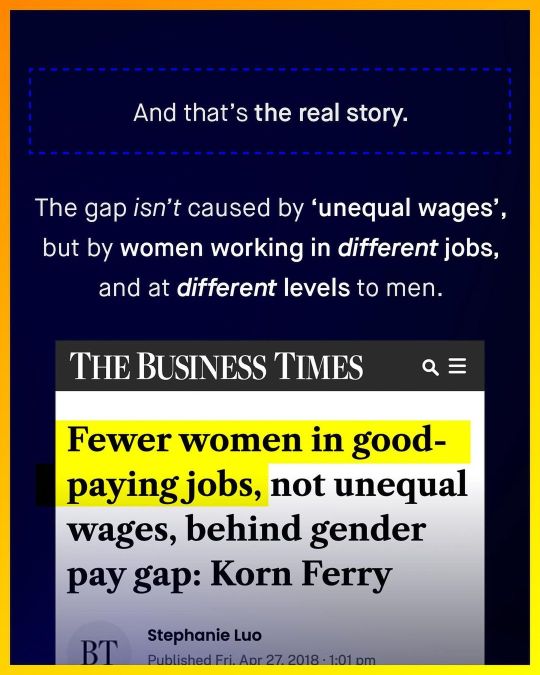
So, the better question is to surely ask ‘why are women not working in these higher paid jobs’?
Or even, ‘do such jobs pay less, because they employ mostly women?’
Or perhaps we’re looking at this the wrong way round...
Maybe we should ask –
‘Do men choose more highly paid jobs, because society tells them to?’
Might society’s warped value system of men being ‘the breadwinner’ be what's really causing the gap?
What do you think?
-
Special thanks to u/problem_redditor
Korn Ferry Gender Pay index:
https://www.kornferry.com/about-us/press/korn-ferry-global-gender-pay-index-analyzes-reasons-behind-inequalities-in-male-and-female-pay
Do Womens Careers Pay less?
https://www.jstor.org/stable/24479913
#The Tin Men#pay gap#pay gap myth#myth of the pay gap#earnings gap#gender pay gap#gender pay gap myth#religion is a mental illness
4 notes
·
View notes
Text

Of all the countries in the world, the Iranian people and the Iranian regime might be the most divergent. You have the barbarous, murderous, genocidal regime on the one hand, and you have the Iranian people cheering on Israel on the other hand.
This is the flag of the Iranian people.

The flag of the Islamic regime is not.

#Iran#Israel#flag of iran#iranian regime#islamic regime#islamic republic of iran#IRGC#exterminate hamas#hamas#hamas terrorism#hamas supporters#islamic terrorism#religion is a mental illness
11 notes
·
View notes
Text
youtube
Why We Should Abolish Hate Speech Laws - Andrew Doyle
Since when did it become the business of the state to audit our emotions?
In effect, this is precisely what's happening by means of the various "hate speech" laws that have been implemented throughout Europe in recent years. In Ireland, the imminent "Criminal Justice" bill would represent one of the most draconian forms of hate speech legislation yet produced.
And how is hatred defined in the bill? Well, the following is a direct quotation: "'hatred' means hatred against a person or a group of persons in the state or elsewhere on account of their protected characteristics or any one of those characteristics."
So, hatred means hatred. Glad we cleared that up. This kind of circular definition is what we've come to expect from legislators when it comes to this most nebulous of concepts. In his book "Censored," Paul Coleman helpfully includes all of the existing legislation on hatred from across Europe. And in doing so, he reveals that no two governments are able to agree on its meaning.
In 2012, the European Court of Human Rights concluded that there "is no universally accepted definition of the expression 'hate speech'" and a manual published by UNESCO in 2015 accepted that "the possibility of reaching a universally shared definition seems unlikely."


When it comes to the statute books, one would have thought that precision and detail would be of paramount importance. After all we've seen how vaguely worded legislation is wide open to exploitation. Consider, for instance, how trans rights activists are now claiming that the reference to sex in the "Equality Act 2010" connotes a sense of "gender identity" rather than, you know, the biological designations of male and female.
If the state is empowered to imprison its citizens on the basis of "hatred," surely we need to know what that means. Hatred, like any other emotion, cannot be legislated out of existence. Will we be seeing laws against envious speech on the statute books? And what about codes against wrath or pride? If the government were to prohibit narcissistic speech, most of the flag waving pronoun-declaring gender ideologues would have to be incarcerated. And while this would doubtless create a much more sane and serene society, it would also involve the obliteration of our fundamental values.
As for "hate crimes," there is no need for mind reading in order to determine the appropriate punishment. If I'm physically assaulted, it makes little difference to me if the assailant was motivated by homophobia. I would prefer the sentence to reflect the crime itself, not to be moderated according to speculations about the perpetrator's private thoughts. The state should have absolutely no license to probe inside our heads, any more than employers should insist on compulsory unconscious bias training.
In a free society we are entitled to think and feel as we see fit, and so long as that does not interfere with the liberties of others, that includes the right to hate. But even if one were to accept the premise that the state must crack down on hateful thoughts, which I most assuredly do not, "hate speech" legislation is holy ineffective.
Censorship of hateful ideas does not cause them to disappear. It drives them underground where they can fester unchallenged. Moreover, "hate speech" laws are easily weaponized by activists seeking to silence their political opponents. For example, in the UK, we have seen people arrested for "misgendering," that is to say, for accurately identifying the sex of another person.
The journalist Caroline Farrow was investigated by police for 6 months after an appearance on Good Morning Britain. According to a complainant, Farrow had referred to another contributor's female-identifying child with a male pronoun during a conversation that took place off-air. And although such instances have not led to convictions, we all know that the process is the punishment.
As one who has received my fair share of abuse online, I understand that free speech has its downsides. But I choose to ignore those of the obnoxious and hateful ilk, rather than call for them to be censored. The price we pay for living in a free society is that unpleasant people are going to say unpleasant things. But their right to do so is precisely the same right that allows us to counter them. If we attempt to silence even our most abusive critics, we are essentially surrendering our principles at their behest.
No doubt the trans-identifying individual who was described as a "faggot with tits" in a recent case in Spain didn't relish the experience. But it should concern us all that the state has intervened and sentenced the woman who posted the offending words to 6 months in in prison, suspended on condition of the payment of a €3,850 fine. In addition, she's been banned from employment in teaching and sports for three and a half years. This is the very definition of authoritarian overreach.
[ *Ironic correction - Both the complainant and the offender were "trans-identified" males. ]
Those who are skeptical of gender identity ideology are particularly susceptible to the misapplication of hate speech laws and there is no way of knowing which other beliefs will eventually be criminalized. Once a state has outlawed "hatred" and failed to define it, the law becomes a cudgel to beat anyone who holds heterodox points of view. Who is to say that a future government might not deem it "hateful" to criticize its policies? What starts with the chilling of free speech ends with the criminalization of dissent.
A new law in Canada, for instance, Bill C63 empowers the state to imprison a citizen for life for "advocating genocide." But of course, activists and even politicians have insisted that claiming biological sex is real and immutable is a form of "trans genocide." On the hands of authoritarians these words are very slippery. They can mean whatever they want them to mean.
And that's why we should be so worried about free speech in Ireland. Last year the Irish Green Party senator Pauline O'Reilly made no effort to disguise the authoritarian nature of the new bill.
"That's exactly what we're doing here, is we are restricting freedom. But we're doing it for the common good."



Hasn't every tyrant in history made an identical claim? In her speech, O'Reilly invoked the notion of safety to justify state censorship. "If your views on other people's identities go to make their lives unsafe insecure and cause them such deep discomfort that they cannot live in peace," she said, "then I believe it is our job as legislators to restrict those freedoms."

Well. it's a common tactic of activists to claim that certain opinions make them feel "unsafe" as a means to provoke a censorial response either from employers or from the state. But this is linguistic sleight of hand and the strategy has been remarkably effective.
The Irish "hate speech" bill goes further than most of its equivalents in European countries. It will give the state the right to prosecute those who cause offense under the catchall of "inciting hatred." And those found guilty could face up to 5 years in prison. Even more worryingly, a citizen can be jailed for 2 years simply if they "prepare or possess" material that could potentially incite hatred. So, if you have a gender-critical meme on your iPhone, that could be sufficient to see you in jail.
In the UK, "hate speech" laws exist in the form of the "Public Order Act 1986" and the "Communications Act 2003." 3,000 people are arrested each year in the UK for comments posted online that have been deemed offensive. And in some cases have even been imprisoned for jokes.
If we're going to tackle this problem, we might start by repealing section 127 of the Communications Act, which criminalizes online speech that can be deemed "grossly offensive." Of course, no attempt is ever made to define "grossly offensive" in the legislation, so anyone could be vulnerable.
In Scotland, the situation is even graver. When First Minister Hamza Yusuf was Justice Secretary, he was instrumental in the passing of the Hate Crime and Public Order Act, and disturbingly, these new laws can see citizens prosecuted for words that they have uttered in the privacy of their own homes. I'm reminded of a speech by William Pitt the Elder, delivered in the House of Commons in March 1763.
"The poorest man may in his cottage bid defiance to all the forces of the Crown. It may be frail, its roof may shake, the wind may blow through it, the storm may enter, the rain may enter, but the King of England cannot enter. All his force dares not cross the threshold of the ruined tenement."

Evidently, these sentiments would not be echoed by the SNP. Given that hatred and offense are entirely subjective concepts, we should be resisting any attempt to codify in law restrictions against them. No two figures of authority will interpret these terms in the same way. And as human beings with frailties and biases, they will doubtless be tempted to wield such laws against their detractors.
If the state is willing to dispense with our right to free expression, there can be no guarantees for any of us. "Hate speech" laws are an affront to human liberty. It's time to ditch them for good.
#Andrew Doyle#Triggernometry#hate speech#hate speech laws#free speech#freedom of speech#hate crimes#thought crime#censorship#freedom of thought#religion is a mental illness
8 notes
·
View notes
Text

All you're doing is trying not to be eaten by your own mob.
7 notes
·
View notes
Text


[ Source: https://pubmed.ncbi.nlm.nih.gov/29507933/ ]
[ Source: https://academic.oup.com/jsm/article-abstract/14/4/624/6973360 ]
"tHiS nEvEr HaPpEnS!!1!"
#Luka Hein#iatrogenic harm#gender affirming care#gender affirming healthcare#gender affirmation#medical mutilation#medical scandal#medical malpractice#medical corruption#double mastectomy#bilateral mastectomy#mastectomy#this never happens#the thing that never happens#religion is a mental illness
4 notes
·
View notes
Text


By: SEGM
Published: Apr 15, 2024
The Cass Review of England’s gender services for children and young people, initiated four years ago, culminated earlier this week in the publication of the final 388-page report. The report was accompanied by 9 systematic reviews of evidence supporting the recommendations. Within hours, NHS England responded, thanking Dr. Hilary Cass and her team for “stepping up to lead such a complex review.” NHS England committed to following through on Dr. Cass’ recommendations, and acknowledged the national and international significance of this seminal work: “Your final report will not just shape the future of healthcare in this country for children and young people experiencing gender distress but will be of major international importance and significance.”
A wide range of stakeholders–from patients and clinicians to bioethicists, legal scholars and healthcare historians–will undoubtedly be studying the hundreds of pages of the Cass report and the accompanying studies for weeks and probably years to come. However, there is also considerable urgency to understand its key take-aways and the likely implications.
Balancing two conflicting priorities–the need for an unrushed, thorough and accurate analysis, as well as our commitment to the members of the healthcare community to inform them of key developments in the field–SEGM has decided to release our preliminary analysis. We chose to focus only on the most salient aspects of the Cass Report that will likely lead to a change in clinical practice.
What we present below is SEGM’s interpretation of the key messages in the report. We do not doubt that every person who reads the report will find a new “angle” and perhaps have a different interpretation. As always, we welcome disagreement and debate. The “many eyes of science” are needed now more than ever.
Summary
The Cass Review marks the end in England of the era of a highly medicalized approach to the treatment of young people with gender-related distress, which has come to be known as “gender-affirming care.” While the treatment protocol for youth comprising of puberty blockers, cross-sex hormones, and surgery, known as the “Dutch Protocol,” was invented in the Netherlands in the 1990’s, the report points out the concept of “gender-affirming care”–the notion that the doctors must accept children’s declarations of identity at face value and must assist them in gender change as early as possible–actually originated in the United States, and only then spread internationally.
The Cass Review provides a scathing assessment of the gender-affirming approach in general, and the gender-clinic model of care, which operationalized this approach of on-demand provision of gender-reassignment interventions, in particular. Going forward, England will treat gender dysphoric youth <18 using standard psychological and psychotherapeutic approaches, with very few young people receiving endocrine gender reassignment interventions (gender-transition surgeries for <18s have never been allowed in England). Further, the review noted that the group of young adults 18-25 is subject to many of the same concerns as the <18s, and recommended that the new regional “hubs” being set up to help gender dysphoric youth be expanded to include patients up to 25 years old.
NHS England (NHSE) welcomed the Cass Review’s recommendations and expressed a firm commitment to implement the recommended changes. However, NHSE went one major step further, announcing that they will be initiating a Cass-style review into the adult gender dysphoria clinics (GDCs) in England. NHSE had already decided to bring forward to 2024 its periodic review of the adult “service specifications,” which set out what clinical services adult clinics provide; as a consequence of Cass’ recommendations, they are additionally launching a much broader review of the entire adult gender clinic system. This was in part due to the concerns raised by the Cass Review that a vulnerable group of 17-25-year-olds represents fundamentally the same group of youth as the <18s, and needs similar protections from non-evidence-based practices. Further, whistleblower complaints from adult clinics corroborated concerns that vulnerable adults were not receiving proper evidence-based care. The refusal by all but one adult gender clinic to cooperate in the outcome analysis for the 9000 patients as part of the Cass Review likely contributed to NHSE’s determination to investigate the adult service. Adult gender dysphoria clinics see patients aged 17 and upwards, and NHSE has written to require them to halt appointments with 17-year-olds.
In summary, the care for <18s in England will no longer be based on the “gender-affirming” model of care but instead will treat youth with gender distress similarly to how it treats youth with other developmental struggles. Further, with the announcement of the adult gender clinic review, England starts a new chapter in the history of gender medicine, with a new focus on vulnerable gender-dysphoric young adults.
Many more developments are expected from England in the coming months. To what extent the UK changes will impact the West’s approach to helping young gender-dysphoric individuals remains to be seen. In SEGM’s view, the impact will likely be significant, even if delayed, as other countries contend with England’s findings and their implications for evidence-based clinical practice.
Detail Regarding Social Transition, Puberty Blockers, Cross-Sex Hormones, Surgery, and Overall Care Delivery Model
Social Gender Transition
The Cass Review positions social transition as an active healthcare intervention “because it may have significant effects on the child or young person in terms of their psychological functioning and longer-term outcomes.” (UK and other countries’ clinicians increasingly use “social prescribing” interventions in order to impact health outcomes).
For young children, the review strongly discourages social transition, noting that “sex of rearing” may profoundly alter a child’s developmental trajectory, with long-ranging consequences. Should parents insist on it, the review recommended that a healthcare professional be involved in helping parents understand the risk-benefit ratio of such a profound and likely life-altering decision.
For older teens, the review recognizes the autonomy of young people’s self-expression but strongly recommends that parents be involved in the decision, noting that secret transitions cause a rift between teens and their families, destabilizing the very support networks that are essential for young people’s long-term well-being.
More generally, should social transitions be undertaken, the review recommended only a partial, rather than complete, social transition, especially for younger children, noting how many children currently live in fear of being “found out.” The discontinuation of the use of puberty blockers (discussed next) will make that fear a certainty. Thus, it would be highly unwise for a parent to create a situation where a young child is living in “stealth.”
These recommendations were supported by interviews with patients and families, and by a systematic review of evidence of social transition published in a peer-reviewed BMJ journal. The review found a dearth of evidence and concluded, “professionals working in the area of gender identity and those seeking support should be aware of the absence of robust evidence of the benefits or harms of social transition for children and adolescents.”
The recognition of not only the potential benefits, but also the potential harms, and the unknown benefit-harm ratio of social gender transition is noteworthy.
Puberty Blockers
The use of puberty blockers to stop normally-timed puberty will no longer be offered as part of England’s publicly funded healthcare system. This is not a “new development” as the problems with using puberty blockers for gender dysphoria were already part of the Cass Review’s interim report, and NHSE had updated its puberty blocker policy a month before the issuing of the final Cass Review.
The rationale for withdrawing puberty blockers from medical practice is manifold. It ranges from unclear treatment aims (besides altering a child’s body), a lack of credible evidence that stopping normally-timed puberty leads to improvements in mental health, safety concerns (e.g., bone health), and profound unknowns across a range of health domains, especially brain development. The fact that nearly 100 percent of puberty-blocked youth proceeded with cross-sex hormones was treated as a negative signal that puberty blockers may be setting children on an irreversible path of gender transition.
As we noted in our earlier analysis, the NHS guidance regarding discontinuing the use of puberty blockers for stopping normally-timed puberty affects only the NHS clinics. Private clinics (including the single non-NHS youth clinic operating in the UK, as well as online clinics based abroad but serving UK citizens) are not subject to the NHS policies. This created a loophole that could be exploited to circumvent NHS actions to safeguard England’s youth from harmful medical interventions. In response to these concerns, Health Minister Victoria Atkins made clear the government’s intention to limit private gender care for under 18s and to eradicate the online trade in hormones, following Cass’ recommendations.
As we noted earlier, the NHS intends to conduct research into puberty blockers, and there has been much speculation about research design in general, and the eligibility for research in particular. The quote below from the final Cass Review suggests that eligibility may be limited only to natal males with early-onset and long-lasting gender dysphoria. It appears to suggest that natal females may not be eligible, as they can successfully undergo convincing masculinization with the help of testosterone at virtually any age:
14.56 Transgender males masculinise well on testosterone, so there is no obvious benefit of puberty blockers in helping them to “pass” in later life, particularly if the use of puberty blockers does not lead to an increase in adult Height.
14.57 For transgender females, there is benefit in stopping irreversible changes such as lower voice and facial hair. This has to be balanced against adequacy of penile growth for vaginoplasty, leaving a small window of time tо achieve both these aims.
14.58 In summary, there seems to be а very narrow indication for the use of puberty blockers in birth-registered males as the start of a medical transition pathway in order to stop irreversible pubertal changes. Other indications remain unproven at this time.
As we noted earlier, the NSHE made it clear in its puberty blocker update policy that there are no guarantees that such research will obtain the necessary ethical approval.
Like other recommendations in the Cass Review, the puberty blockers recommendation was based on extensive stakeholder consultation, and supported by a systematic review of evidence, which showed no credible psychological benefits of puberty suppression in the treatment of gender dysphoric youth. As we explained earlier, the original 2020 NICE systematic evidence review was updated in 2023, but newly-identified studies did not change its conclusions.
Cross-Sex Hormones
Shortly before the publication of the final Cass Review, NHSE issued an updated policy about the cross-sex hormones. As we noted at the time in our earlier analysis, the policy was only a minor update, necessitated by the launch of the new gender services, and it represented only minor changes. Cross-sex hormones for those around their 16th birthday were still allowed, although a new centralized team not directly involved in care of the young person would need to approve the medical necessity. At the time, SEGM posited that following the final Cass Review, the NHS will commit to a more thorough review of the cross-sex hormones policy, and further updates. This indeed has occurred.
According to NHS England’s response to the final Cass Report:
NHS England will review the use of gender affirming hormones through a process of updated evidence review and public consultation, similar to the rigorous process that was followed to review the use of puberty suppressing hormones.
NHS England has made clear that there will be a single cross-sex hormones policy “which will cover all people over the age of 16,” with further details to follow.
NHSE acknowledged Dr. Cass’s recommendation that “the new providers should be ‘extremely cautious’ when considering whether to refer young people under 18 years for consideration of hormone intervention.” To support this recommendation while the new cross-sex hormones policy is being developed, NHSE has “established a national multi-disciplinary team (MDT) that will review and need to agree all recommendations for hormone intervention.” Further, NHSE noted that the “first meeting of this new national MDT will take place later this month” chaired initially by Professor Judith Ellis, former CEO of the Royal College of Paediatric and Child Health.
The original NICE systematic review of evidence for the effects of cross-sex hormones was conducted in 2020, and it found similar problems in the evidence base as the puberty blockers review (unreliable evidence base), but with a signal that there may be some small short-term improvements in mental health following cross-sex hormones administration. The new systematic review of cross-sex hormones confirmed these findings.
The final Cass Review expressed concern over how small these changes were, considering the fact that the introduction of the long-awaited cross-sex hormones and desired physical changes is expected to lead to short-term improvements in mood. This suggests that the Cass Review is concerned not only with the low certainty of the reported benefits due to poor study designs, but also with the possibility that the small improvements may be short-lived and due to the potential placebo effect:
15.27 When a young person has been on puberty blockers, a short-term boost in mental wellbeing is to be expected when sex hormones are introduced. Testosterone is faster to produce physical changes than oestrogen, and birth-registered girls can expect to start seeing body changes in line with their identified gender within a few months. The start of long anticipated physical changes would be expected to improve mood, at least in the short term, and it is perhaps surprising that there is not a greater effect size. However, much longer term follow-up is needed to understand the full psychological impact of medical transition.
The NHSE’s announcement made it clear that the final cross-sex hormones policy will be based on the updated systematic review of evidence.
Surgery
Surgeries have never been available to under 18’s in England, so no systematic reviews of surgeries has been conducted, and no additional changes to the policy for youth under 18 are needed. However, NHSE’s announcement of the Cass-style review into the adult gender clinics raises questions about whether surgical interventions for young adults will now come under scrutiny as well.
Change in the Delivery Care Model Overall
In addition to making specific recommendations overall about social transition and endocrine interventions, the review challenged the concept that gender dysphoria/gender incongruence in youth as an exceptional condition that needs exceptional treatments delivered via exceptional models of care exemplified by gender clinics.
The healthcare delivery system for gender dysphoric youth will be restructured to provide a fundamentally different model of care, and realign it with the way care is typically organized in England. Every gender-dysphoric child or young person will have a dedicated primary care provider (a pediatrician or a GP) overseeing their care and well-being. Children and young people with mental health conditions, or those whose gender incongruence is causing distress, will receive psychotherapeutic and psychological services from the second level of care at the Child and Adolescent Mental Health Services (CAMHS).
Very few young people will be referred to super-specialized tertiary services, which will carefully examine the medical necessity of cross-sex hormones. The referring clinicians will need to demonstrate why cross-sex hormones delivered to under-18’s are medically indicated and preferred over allowing the young person to reach maturity, and a centralized team not directly involved in the care of the young person will need to agree with this assessment. It is expected that in the end, very few young people will be treated with interventions to alter their bodies.
Other notable aspects of the final report
The final Cass Review made a number of other highly consequential statements and observations. It is impossible to do a thorough overview of all of them given the short time since the report’s release, but we will highlight several that stood out to SEGM as particularly noteworthy.
Although chiefly forward-looking, the review described the alarming inadequacies of clinical practice at GIDS.
While the focus is on service improvement, the legal ramifications of the unsafe practice at GIDS in the longer term must be apparent to NHSE. GIDS refused to participate in the review’s research study, to compare clinical practice at a range of European pediatric gender clinics, therefore the report (at Appendix 9) of the Multi-Professional Review Group (MPRG) which oversaw GIDS’s referrals for puberty blockers is the major source of information about what went on there. The MPRG painted an extraordinary picture. It was not clear how thoroughly different treatment options had been discussed, and most children and parents were asking to obtain puberty blockers from their first appointment with GIDS, having “turned for information to the media and online resources, with many accessing LGBTQ+ and GD support groups which appear to be mainly affirmative in nature.”
Concerns of over treatment of neurodiverse and same-sex attracted youth.
Neurodiversity was suspected or diagnosed in a majority of children referred for puberty blockers and where sexuality was discussed “most cases are of same sex, opposite-gender attracted children.” The MPRG were “concerned about the lack of evidence of professional curiosity” about these children’s lives shown by GIDS clinicians. A recurrent concern was “the inadequacy and on occasion inaccuracy of answers given to children and their families by GIDS and their failure to correct child and parental misconceptions about puberty, puberty blockers and hormones.” Unsurprsingly, then, they note that the Care Quality Commission’s (CQC) observation that consent taking was judged to be “not in line with NHS and GMC requirements.” Records varied “from succinct to disorganised.”
A scathing assessment of poor quality and lack of independence for the guidelines by WPATH, The American Academy of Pediatrics (AAP), and the Endocrine Society (ES).
As part of the Cass Review, an independent team of research methodologists assessed all the current treatment guidelines and recommendations for quality in a systematic review, using the internationally recognized AGREE II methodology for evaluating guideline quality. The AAP 2018 treatment recommendations guidelines scored amongst those at the bottom of the 23 reviewed guidelines. The WPATH and the ES treatment recommendations did not fare much better. The review noted a marked lack of independence in guideline authorship, noting circular referencing: one non-evidence-based guideline was used to justify another non-evidence-based guideline’s recommendation. The significant overlap in authorship between the guidelines (especially between WPATH and ES) was noted as a significant cause for concern, as was WPATH’s refusal to acknowledge the results of their own systematic review in its adolescent section. The report points out that only the Swedish and Finnish treatment recommendations appear credible, but even they lack the specificity needed for the NHS to operationalize the treatment recommendations in the UK context. The concern over the proliferation of non-evidence-based guidelines, which at times do acknowledge the poor quality evidence but then issue strong recommendations to medically transition youth anyway, has been seconded in the BMJ article dedicated to this specific aspect of the Cass review findings.
Condemnation of the “toxic” nature of debate within which standard psychological therapies were rebranded "conversion practices."
The Cass Review drew attention to the difficulty of undertaking the review amid an “increasingly toxic, ideological and polarized public debate” that ill-served children. The report noted that it is essential to explore children’s complex needs and stated that it is “harmful to equate this approach to conversion therapy as it may prevent young people from getting the emotional support they deserve.” Furthermore, potential accusations of conversion practice “when following an approach that would be considered normal clinical practice” in other scenarios made clinicians wary of offering support to young people, leaving them without the help they deserve. The report highlighted the potential for legislation on conversion practices to complicate the situation and emphasized that “strong safeguards must be built into any potential legislation” to guard against the risk that clinical staff feel that discharging their duty of care would expose them to legal challenge.
Questioning the assumption of the gender identity theory.
While some have criticized the Cass Review for relying on constructs coming from the gender identity theory (e.g., referring to “gender identity” without critically assessing the origin and validity of this concept), the report did briefly address the outdated nature of the assumptions on which the “gender-affirming” care model is based. The report noted that the theory of gender identity development was set forth in 1966 by Kohlberg, who described a typical progression whereby by the age of 5-6, children develop gender identity constancy.
The report noted the obvious fact that the current patterns of both identifying as transgender for the first time at much older ages and also the growing phenomenon of detransition and re-identification with natal sex demonstrably contradict this theory.
The review considered a range of factors that may have contributed to the current phenomenon of a sharp rise of trans identification in youth. It noted that while biology likely plays a role, “since biological factors have not changed in the last 10 years it is necessary to look at other possible reasons for the increase in referrals and the disproportionate representation of birth-registered females.”
8.23 For children and young people with gender incongruence, ‘innate’ or biological factors may play a part in some individuals, in ways that are not yet understood, and in others psychosocial factors, including life experiences, societal and cultural influences, may be more important. Since biological factors have not changed in the last 10 years it is necessary to look at other possible reasons for the increase in referrals and the disproportionate representationof birth-registered females.
Recognition that the challenges in the mental health of Generation Z are likely at the root of the current phenomenon of trans identification in youth.
The report acknowledged the likely multi-factorial basis for the current explosion of gender-dysphoric youth, with a focus on “Gen Z” and the significant mental health crisis affecting this population more generally, as well as the role of social media.
7.21 The striking increase in young people presenting with gender incongruence/dysphoria needs to be considered within the context of poor mental health and emotional distress amongst the broader adolescent population, particularly given their high rates of co-existing mental health problems and neurodiversity.
7.22 Internationally, there have been increasing concerns about the mental health of Generation Z. The reasons for this are highly speculative, although there is ongoing debate about the contribution of excessive smartphone use and social media as discussed above.
Suggestion that the invention and the availability of the Dutch protocol likely contributed to the rapid rise in gender dysphoria in youth.
The report noted that the sharp rise in the numbers of gender dysphoric youth in the West also coincided with the introduction of puberty blockers into general medical practice. Of note, the Netherlands experienced a similar spike several years before the rest of the West–and incidentally, the Netherlands introduced the Dutch protocol/blockers into clinical use several years before the rest of the West. This lends further credibility to the theory that the very availability of the Dutch protocol treatment may have contributed to the growing numbers of youth seeing their developmental struggles through the “gender identity” lens and pursing medical interventions.
8.50 The dramatic increase in presentations to NHS gender clinics from 2014, as well as in several other countries, coincided with puberty blockers being made available off protocol and to a wider group of young people. The only country with an earlier acceleration in referrals is the Netherlands, where the Dutch protocol was developed.
Clear attribution of the “gender-affirming” model of care to the United States.
While it was the Dutch clinicians who came up with the “innovative clinical practice” to use puberty blockers in an off-label way to stop normally-timed puberty of gender-dysphoric youth, the report suggests that it was the Americans who propagated the approach of allowing the child to direct what medical interventions they need based on their self-declared identity.
Specifically, the review credits an American psychologist Diane Ehrensaft, who pioneered and promulgated this theory, which has become the core of the “gender-affirming” model of care. The report describes the model as a belief that “a child of any age may be cognizant of their authentic identity and will benefit from a social transition at any stage of development.”
2.13 In 2007 Norman Spack established a clinic in Boston, USA modelled on the Dutch protocol and began prescribing puberty blockers from early puberty (Tanner stage 2).
2.14 Practice in the USA began to diverge from the models of care in Canada and the Netherlands, following instead a gender affirmative model advocated by Diane Ehrensaft (Eherensaft, 2017). She described the three approaches as follows (Ehrensaft, 2017):
“The first model, represented in the work of Drs Susan Bradley and Ken Zucker [Canada], assumes that young children have malleable gender brains, so to speak, and that treatment goals can include helping a young child accept the gender that matches the sex assigned to them at birth.
The second model, represented in the work of practitioners in the Netherlands, allows that a child may have knowledge of their gender identity at a young age, but should wait until the advent of adolescence before engaging in any full transition from one gender to another.
The third model, represented in the work of an international consortium of gender affirmative theoreticians and practitioners, allows that a child of any age may be cognizant of their authentic identity and will benefit from a social transition at any stage of development.”
2.15 The third model - the ‘affirmative model’ - has subsequently become dominant in many countries. As a result, some gender services have moved away from a more exploratory approach, and this is seen by some advocacy and support groups as a move to ‘gatekeeping’ model.
Incidentally, (a fact the the report does not mention), Ehrensaft was also a notable figure in promoting the now-defunct theory of repressed memory of satanic abuse, and published on the subject. This subject is outside the scope of this analysis, but notably, the epidemic stopped only after successful lawsuits demonstrating that some psychologists facilitated the patients’ “recovering” non-existing memories of abuse as an explanation of the patient's distress.
Clear acknowledgment of detransition as a growing phenomenon that can no longer be ignored.
There was a chapter dedicated to detransitioners, and the term “detransition” was mentioned in the report over 80 times, citing a number of studies from the UK and internationally. The report recognized that the rate of detransition and regret among the novel population of youth is unknown, but suggested it is no longer negligible, citing a UK study of double-digit detransition in a relatively short follow-up period. Of note, a recent US study found that among participants who were medically transitioning, almost 30 percent ceased medical transition based on a 4-year average followup, but the reasons for the cessation were not explored.
Suggestion of lack of data integrity in gender clinics.
The Cass Review revealed that in a truly unexpected turn of events, all but one adult gender clinic refused to cooperate in a data analysis project that would have allowed tracking of longer-term outcomes of 9,000 gender dysphoric young people, which included both those who underwent gender transitions as well as those who chose less invasive options. The responsibility for the research, which has obtained ethics permission, has now been handed over to NHSE, which will conduct the review without the gender clinics’s cooperation. The objection of the gender clinics and the responses to those objections (both contained in the appendices to the report) suggest that the reasons for the lack of cooperation may be ideological.
Further, there are indications through the report that there may be a lack of integrity in the gender clinic approach to data collection and reporting more generally. For example, the Cass team was advised by GIDS/Tavistock (the youth gender clinic) that only 27 percent of the referred cases were referred for endocrine interventions (puberty blockers and/or cross-sex hormones), creating the impression that only a minority of gender dysphoric youth are intervened with medically.
However, the context of the report signaled that this figure is open to misinterpretation (without directly calling it misleading). The report noted that the 27 percent only applies to the young people who were referred directly to the two adolescent endocrine centers. Among the 73 percent “non-referred” for endocrine interventions, 69 percent actually went on to adult gender clinics, where most likely received hormonal interventions.
The question of what percentage of youth referred to gender clinics end up transitioning is an open one. In the Netherlands, which claims a cautious approach, this number appears to be around 70-80 percent. It is reasonable to expect similar or even higher numbers among gender clinic staff who subscribe to the “gender-affirming” model of care.
Problems with applying the Dutch protocol to the “wrong” population.
The report clarifies that GIDS/Tavistock’s approach to validating the Dutch protocol failed on at least 3 accounts. As previously discussed, the clinic started scaling the treatment before they analyzed and published the results and they also changed the protocol where the minimum age of 12 for puberty blocked was dropped and replaced by pubertal tanner stage 2 stage–which can be as young as ages 8-9 in girls. However, the report highlights another important deviation, which may be responsible for the sheer scale of the current problem.
While the research study (aka “Early Intervention Study”) was only approved to include youth with the classic early childhood, the pre-pubertal onset of gender dysphoria that intensified in adolescence with no other significant mental health problems (to replicate the Dutch research), when the clinic chose to scale it widely, it expanded eligibility to all youth including those whose gender dysphoria emerged post-puberty and in the context of complex mental health problems (p. 73). The latter group currently represents the single biggest affected demographic.
The fact that the Dutch research is currently being applied to the very demographic which was originally contra-indicated for gender transition and that this problem is not confined to the UK but is a worldwide problem, has been highlighted in a number of recent publications and emphasized in the Cass report.
The current “suicide and suicidality narrative” surrounding gender-dysphoric youth is misleading.
The Cass Review noted that “balanced information, which is realistic and practical, and does not over-exaggerate or underestimate the risks, is essential to support everyone involved and identify young people in most urgent need of help.” The review commented on the thankfully low rates of completed suicides in the population of trans-identified youth, pointing out the latest evidence from Finland. However, the review appropriately recognized every suicide is a tragic event and the causes in each individual case must be clearly understood. The report noted a recent UK analysis of suicides using the National Child Mortality Database (NCMD). The analysis of 91 cases of youth suicides between April 2019 and March 2020 (1-year span) identified 108 total deaths across the entire population of the UK that were likely due to suicide. In examining the factors contributing to suicides, the Child Death Overview Panel concluded that Household functioning was found to be the most common contributing factor (69%), followed by mental health problems (55%), bullying (23%), and neurodevelopmental conditions (16%). Sexual orientation, sexual identity, and gender identity were assessed as a factor in 9 percent of total suicides. The Cass report did not provide an additional breakdown for sexual orientation vs gender identity. However, the report did note that systematic reviews failed to provide evidence that endocrine interventions reduce suicides.
The problem with the notion of the “diagnostic assessment.”
The report zooms in on a central argument leveled by gender-affirming clinicians that “gender-affirming” treatments are only provided following a diagnostic assessment, and therefore are medically necessary. The review aptly points out that neither the DSM-5 diagnosis of “gender dysphoria,” nor the “de-pathologized” ICD-11 diagnosis of “gender incongruence,” have a known predictive validity. In other words, a young person can meet the diagnostic criteria today, but nothing is known about how likely the young person is to continue to experience gender-incongruent feelings in the future.
16.8 A formal diagnosis of gender dysphoria is frequently cited as a prerequisite for accessing hormone treatment. However, it is not reliably predictive of whether that young person will have longstanding gender incongruence in the future, or whether medical intervention will be the best option for them. Depending on what has caused their distress or dysphoria, it may be resolved by medical treatment, but it may also be resolved in other ways.
The Cass Report notes, “The Review was unable to obtain clear criteria from the GIDS team on their criteria for referral for endocrine intervention.” The report also points out that if the causes for gender-related stress are “psychosocial,” “sociocultural” and/or “dynamic,” providing invasive and irreversible interventions to such young people presents a challenging ethical dilemma.
16.9 As discussed in Chapter 8, the nature and causes of gender dysphoria/incongruence are complex and poorly understood, and there is very limited understanding of the currently presenting population of predominantly birth registered adolescent females. Each individual will have a different mix of biopsychosocial factors, but if potentially dynamic psychosocial or sociocultural factors predominate in a significant proportion of people, one of the most challenging ethical questions is whether and/ or when medical intervention is the correct response.
Further, the report takes on the notion of the “diagnostic assessment” itself, noting that there is no formalized assessment process whereby one can determine how to conduct such an assessment, and how to arrive at predictable outcomes as to which young person is referred to the endocrine interventions and which one is not. The report notes:
10.17 There was also a general lack of understanding among service users participating in the lived experience focus groups about what the assessment was for and confusion about what was assessment and what was diagnosis. Thoughts on the purpose of the assessment included:
• To support young people to explore their options and access the care that’s right for them.
• To get validation of their trans identity and access to the medication pathway.
• To make the person comfortable and focus on what they’re looking for from the service.
• To ensure patients have an understanding of the healthcare options available.
The report concluded that, following a review of international clinical practice, “there was no approach to assessment that could be directly adopted for use in the NHS.” One needs to be developed to meet key goals (support identification of individual needs, allow outcomes to be measured more consistently and ensure children and young people have a similar experience of the service.)
The fundamentally new model will focus on assessment with the goal of “case formulation” followed by psychotherapy as the first line of treatment.
The new treatment framework will be comprised of the assessment, case formulation, diagnosis, care plan. Due to the problems described above (lack of specificity of what the goal of the “assessment” are), the report sets out a new and clear expectation of the role of the assessment. Rather than attempting to identify which young person should be referred to endocrine interventions, the goal is to “derive a multi-level formulation for a child or young person who presents to the NHS seeking help around their gender or experience of gender-related distress.”
The starting point of the assessment is to assess immediate risk and assess complex care needs. Assuming any immediate risks (if any) are addressed using standard psychotherapeutic approaches, the next goal is to come up with a “case formulation.” A case formulation is a standard psychotherapeutic process whereby clinicians synthesize the complexity of the young person’s situation to develop an individualized treatment plan.
The report makes it clear that if any interventions are indicated, standard psychotherapeutic interventions for mental health conditions, as well as more specific exploration of gender-related distress (if indicated), will be the primary treatment. Referrals to endocrine interventions will only be accepted from the Child and Adolescent Mental Health Services (CAMHS) with onus on the clinician making the referral to demonstrate to a centralized team that includes members not directly involved in the care the medical necessity of cross-sex hormones. As mentioned elsewhere, Cass recommended extreme caution in prescribing cross-ses hormones to youth, and the NHS has committed to updating its current cross-sex hormones policy to align it with the final report recommendations.
Recognition of the need to update the diagnostic categories to meet the changing clinical presentations of gender-related distress, and the phenomenon of detransition.
The Cass Review subtly but powerfully signals that the DSM-5 “gender dysphoria” diagnosis appears to be preferred by most clinicians, while the attempt to “de-pathologize” the condition in ICD-11 is less clinically useful.
At the same time, the report recognizes that neither of these diagnostic categories are adequate for the current complexity of the presentations. The diagnosis itself was criticized for relying on outdated notions of preferences for sexed stereotypes from “previous decades,” and the “DSM-5 diagnostic criteria for gender dysphoria has a low threshold based on overlapping criteria” leading to the risk of overdiagnosis and overtreatment. Further, the report indicated that the diagnosis is unhelpful in the care for the growing number of detransitioners as it does not have any specific categories for this growing patient population.
New focus on young adults.
The report recognized the new understanding of adolescent development and that adolescence does not stop at 18 but extends into mid-20s. Noting the disproportionate number of non-neurotypical individuals struggling with gender identity, the report noted that neurodiverse young people are particularly vulnerable “into their early 20s or longer because of their tendency to want black-and-white answers, and their difficulty in tolerating uncertainty.”
Consistent with that, the report recommends that the restructured approach to gender-dysphoric youth does not stop at 18, but subsumes the category of young adults. In addition, the report notes that while the provision of adult gender services fell outside of the review’s remit, several staff in adult gender clinics “contacted the Review in confidence with concerns about their experiences working in adult gender services.” Adult clinic “whistleblowers” shared that adult services experienced a similar influx of young adults, primarily females with complex mental health problems, presenting to adult gender clinics with an expectation of rapid provision of “gender-affirming” medical interventions, as well as growing numbers of detransitioners. The whistleblowers expressed deep concerns about the harm to the vulnerable population of young adults which seemed to represent the same demographic that began to be seen at the Tavistock a few years ago.
As a result, the review recommended a heightened focus on the adult services, and the NHS has responded by announcing an investigation into the adult NHS gender clinics.
Call for the development of new treatments and clear clinical targets.
The review recognizes the the evidence base for psychotherapeutic approaches to the management of gender dysphoria in youth is very low quality. At the same time, the report pointed out that standard therapeutic interventions for distress are the standard of care in medicine, and that no studies of the application of this approach to gender dysphoria have shown harm.
The review stated unambiguously that the “ultimate goal of any intervention is to help the child or young person to function and thrive, they need to be provided with tools and strategies to give them the best opportunity to do so.” The review called for the development of an “explicit clinical pathway for non-medical interventions, as well as a research strategy for evaluating their effectiveness.”
With this recommendation, the Cass report has redirected the clinical community towards the development and study of non-invasive clinical interventions with a focus on long-term outcomes, with the goal of helping young people achieve the best quality of life.
SEGM Take-Aways
The single most salient take-away is that the so-called “gender-affirming” model of care, which treats young people’s declarations of transgender identity as an indication that any physical body modification desired by the young person is medically necessary, is over in England. So is the era of the “gender-clinic model of care,” which exists to operationalize the highly medicalized “gender-affirming” care model.
We end our take-away by pointing the readers to a powerful editorial by the BMJ Editor in Chief. The entirety of this short editorial is worth reading, but we will highlight the more salient quotes below:
“Offering treatments without an adequate understanding of benefits and harms is unethical. All of this matters even more when the treatments are not trivial; puberty blockers and hormone therapies are major, life altering interventions.”
“Without doubt, the advocacy and clinical practice for medical treatment of gender dysphoria had moved ahead of the evidence—a recipe for harm.”
“...Families, carers, advocates, and clinicians—acting in the best interests of children and adolescents—face a clear choice whether to allow the Cass review to deepen division or use it as a driver of better care.”
This analysis, published by the Editor-in-Chief of one of the most prestigious medical journals in the world, signals that the implications of the Cass Review will likely reverberate worldwide. It now appears inevitable that the arc of history has bent in the direction of reversal of gender-affirming care worldwide, although in some countries it will take considerably longer to change medical practice.
The Cass Review is a historic document the significance of which cannot be overstated. It is also multi-faceted, and no single analysis can do it justice. We have done our best to synthesize the most salient aspects of the review after a single reading. We have no doubt that we missed other important aspects and we trust that others will point them out.
#SEGM#Society for Evidence Based Gender Medicine#Cass report#Cass review#Dr. Hilary Cass#Hilary Cass#NHS England#National Health Service#gender affirming care#gender affirming healthcare#gender affirmation#medical scandal#medical malpractice#medical corruption#religion is a mental illness
11 notes
·
View notes
Text
Hamas supporters showed up in droves for a riot organized by radical hate group WOL Palestine in lower Manhattan today.
Israel supporters showed up to peacefully counterprotest, carrying Israeli and American flags. One of their American flags was set on fire by a Hamas supporter; the man holding the flag nearly got burned. As the flag burned, a masked terror supporter yelled “Death to America!” Several members of the pro-Hamas crowd echoed his cry.
If it wasn’t abundantly clear by now, these terror supporters don’t just want to destroy Israel. They want to tear down the entire Western world.
This isn't only about Israel anymore. These crazed terrorists want to destroy everything.
Believe them when they tell you who they are and what they're up to.
#antisemitism#israel#hamas#hamas supporters#islamic terrorism#pro palestine#pro hamas#hamas terrorism#death to america#religion#islam#jihad#jihadism#western civilization#religion is a mental illness
18 notes
·
View notes
Text

By: Carlos Turcios
Published: Apr 13, 2024
A mother may soon be allowed to have her son castrated without the father’s permission because she believes her son is transgender.
California’s court system is preparing to allow a divorced mother, Anne Georgulas, to have her 11-year-old son castrated against the will of the father, Jeff Younger, based on the mother’s claim that the biological boy identifies as female.
A pro forma hearing on April 25 will have court-ordained transgender “experts” take the stand, per National File. Younger will not be allowed to testify in defense of his son during the hearing.
Younger said he believes his ex-wife will take their son to a gender clinic in California after the hearing, fearing the court will rubber-stamp the castration of his son.
The divorced couple has been engaged in a years-long custody battle over their children. As previously reported by The Dallas Express, Younger petitioned the Texas Supreme Court to force the return of their children, who had been moved to California by their mother. However, on December 30, 2022, the court rejected the petition.
DX recently communicated with Younger, who reflected on the disposition of his legal case in the Lone Star State.
“My case is proof that the statutory design of the Texas Family Courts is abusive of the liberty of Texas citizens. The family courts are a clear and present danger to the welfare of Texas children. Judge ‘Bloody’ Mary Brown, 301st District Court, stripped me of parental rights without possibility of appeal, just because I want to raise my son as a boy,” Younger wrote in a text message.
“Even the Supreme Court of Texas, under Justice ‘Blackhearted’ Blacklock, allowed my son to be moved to California where he is at danger of chemical castration, right now,” he added. “There are no limits to the child abuse these courts will inflict on children. It’s long past time for the Texas Legislature to fix these lawless child-abusing Family Courts. My message to the effeminate Texas Legislature: fix the Family Courts, or else.”
In response to the court’s rejection of his petition in 2022, Younger tweeted, “The Supreme Court of Texas denied my Mandamus, effectively terminating my parental rights. My children are now subject to being chemically castrated in California. Texas is an empire of child abuse, led by Texas judges.”
The Supreme Court of Texas argued that it denied Younger’s petition because of an earlier district court order that prohibited Georgulas from transitioning their children without Younger’s consent.
Texas Supreme Court Justice Blacklock stated that Georgulas “freely acknowledges that she is bound by this order in both Texas and California” and has ”flatly denied to this Court that she will seek to evade the district court’s order while she is in California.”
Despite these claims from the Texas Supreme Court, Younger fears that his ex-wife will follow through with the castration of their son.
Younger argued that Georgulas moved their children to California to evade Texas law and benefit from SB 107. California Gov. Gavin Newsom signed the bill, which went into effect on January 1, 2023.
California lawmaker Sen. Scott Wiener (D), the bill’s primary author, said that the legislation was a “refuge for trans kids and their families.”
“SB 107 will protect trans kids and their families if they flee to California from Alabama, Texas, Idaho, or any other state criminalizing the parents of trans kids for allowing them to receive gender-affirming care,” Wiener continued, as previously reported by DX.
Younger’s attorneys have not stated what they plan to do about Georgulas’ purported misrepresentation to the Texas Supreme Court, but action is expected, reported National File.
--

==
No parent ever has the right to give their child a sexual lobotomy.
#California#castration#chemical castration#gender affirming care#gender affirming healthcare#munchausen syndrome#munchausen syndrome by proxy#transhausen syndrome#transhausen syndrome by proxy#child abuse#gender affirmation#medical corruption#medical scandal#medical mutilation#SB107#gender lobotomy#religion is a mental illness
5 notes
·
View notes
Text

These pro-Hamas terrorist supporters claim to be "anti-war" and want a "ceasefire," while celebrating a (failed) attempt to eradicate Israel from the face of the Earth. Meaning, they're as "anti-war" as Antifa is "anti-fascist"; they're in favor of war/fascism when they do it.
These crazed fanatics support the brutal Islamic regime of Iran. You remember, the one that the citizens had an uprising against when Mahsa Amini was murdered. At the time, even the most left-wing ideologues finally got around to condemning the regime, albeit with the caveat that the fault lies with the regime, not with Islam, and scolded us not to be "Islamophobic" about it.
Now, far-left western terrorists are shouting "Allahu Akbar" and cheering for the same regime, having decided their goals line up with those of a far-right fundamentalist theocracy.
Given they're chanting "Allahu Akbar," any claim that this isn't about Islamic supremacy is completely dishonest. These people need to be removed from our societies before they destroy them and turn them into Islamic hellholes.
#ceasefire#antisemitism#Iran#israel#iran vs israel#anti war#islam#islamic regime#islamic republic of iran#iranian regime#islamic supremacy#religion#religion is a mental illness
20 notes
·
View notes