#JuniperPublishers
Text
Hyperparathyroidism in Pregnant Women: Clinical Issues, Laboratory Findings and Relevant Therapeutic Approachesr - Juniper Publishers

Juniper Publishers- Open Access Journal of Annals of Reviews & Research
Hyperparathyroidism in Pregnant Women: Clinical Issues, Laboratory Findings and Relevant Therapeutic Approachesr - Juniper Publishers
Authored by Rosita Fontes
Abstract
Primary hyperparathyroidism (PHPT) is the most common cause of hypercalcemia in outpatient settings, with an incidence in women of reproductive age of 4.7-6.2 cases per 100,000 persons. When untreated in pregnant women, PHPT can lead to maternal and fetal complications. The authors present a case of a patient with a pre-pregnancy hyperparathyroidism diagnosis: she had worsening symptoms during pregnancy, so was referred for surgery due to failure of clinical treatment to keep the disease under control. Clinical issues, laboratory findings, and relevant therapeutic approaches are discussed.
Keywords: Hyperparathyroidism; Hypercalcemia; Multiple endocrine neoplasia syndrome; mTc-sestamibi scintigraphy; Beta chorionic gonadotropin; Parathyroidectomy; nephrolithiasis; calciuria
Abbreviations: PHPT: Primary Hyperparathyroidism; MEN: Multiple Endocrine Neoplasia Syndrome; BP: Blood Pressure; US: Ultrasound
Introduction
Primary hyperparathyroidism (PHPT) is a disorder that results from hypersecretion of parathyroid hormone (PTH), which is the most common cause of hypercalcemia in the outpatient setting. An analysis published in 2013 showed that the incidence in women of reproductive age, within a racially mixed population, is 4.7-6.2 cases per 100,000 persons [1]. In pregnant women, the disease occurs in 0.5-1.4%, and in 80% it is due to adenoma of the parathyroid glands [2]. When untreated, PHPT can lead to maternal complications such as nephrolithiasis, pancreatitis, and eclampsia, and fetal complications such as low birth weight and neonatal seizure [3-6]. Adequate control of patients who become pregnant with hyperparathyroidism can be a challenge, depending on their clinical symptoms and the laboratory and imaging evaluation. According to the trimester of pregnancy and severity of the disease, the treatment may be either clinical or surgical. The authors present a case of a patient with a pre-pregnancy diagnosis, and a worsening of symptoms during pregnancy; she was referred for surgery due to failure of clinical treatment to keep the disease under control.
Case Presentation
A pregnant 45-year-old woman, Afro-descendant, gravida 3, para 1, presented with a history of recurrent bilateral nephrolithiasis since she was 40 years old. She had a left wrist fracture after falling from height. Her past medical history was notable for low calcium intake, asthma and diabetes mellitus type 2, which was under control with metformin. In her surgical history, she underwent ureteral stent double J, and ectopic pregnancy surgery. She also suffered a lithotripsy for treatment of kidney stones. She presented for consultation for investigation of repetitive renal stones, denying any symptoms compatible with hyperparathyroidism. In her family history, there were no cases of hyperparathyroidism, no multiple endocrine neoplasia syndrome (MEN), or other syndromes associated with hypercalcemia. On physical examination, the patient was overweight (BMI 28.72 kg/m2), blood pressure (BP) was 110/75 mm Hg, bone deformities or fractures were not observed, and renal fist-percussion was negative. There were no other abnormalities found.
At admission, she brought examinations showing parathyroid hormone (PTH) of 390 pg/mL (12-65), total calcium corrected for albumin of 9.5 mg/dL (8.4-10.5), phosphorus of 2.3 mg/dL (2.5-4.5), as well as urinary calciuria in 24hours of 359 mg/day (100-250) and 4.78 mg/kg/day (< 4.0). Thyroid function tests were normal, as well as hemogram and biochemistry assessments. In several tests requested to confirm these results, her serum calcium was high (Table 1), along with maintained high PTH, low phosphate, and high calciuria. The parathyroid glands were not visualized on cervical ultrasound (US), but parathyroid 99mTcsestamibi scintigraphy (MIBI) showed hypercaptation of the tracer after 2 hours in the left lower parathyroid projection area, suggestive of a parathyroid adenoma (Figure 1). Renal US showed bilateral cortical stones, without lithiasis in the pyelocalyceal system. Adequate hydration and furosemide 20 mg/day were prescribed.
The 25-hydroxy vitamin D (VD) was low, 7.1 ng/mL (>30 ng/ mL), and the 1.25-dihydroxy vitamin D (1.25(OH)2D) was 193.9 pg/mL (18-78). She had recently presented with visual turbidity, nausea, headache, asthenia and dizziness, and recurrent renal colic, with an episode of pyelonephritis that was treated with antibiotic therapy. As the patient had a 2-week menstrual delay, a beta chorionic gonadotropin (beta-HCG) test was ordered, and the result was compatible with pregnancy. The gestational age calculated by the date of the last menstrual period was 5 weeks and 2 days. PTH and calcium remained elevated during the first trimester of pregnancy (Table 1). The option at that time, after discussion with the obstetrician, was increased furosemide at 40 mg/day and intensification of hydration. During the second trimester, the calcemia increased even more (Table 1), with the symptoms persisting. At that point, VD replacement was prescribed, and surgery was indicated. Parathyroidectomy was performed at 25 weeks of pregnancy, which was carried out without incident. On the first postoperative day, the patient had no symptoms, and the corrected calcium and PTH were normal (Table 1), although anatomopathological exam confirmed parathyroid adenoma. The pregnancy progressed without intercurrences. At 38 weeks and 2 days, she had an uneventful cesarean delivery. The newborn was healthy, with APGAR 9 at 1 minute and 10 at 5 minutes, 3.990 kg, and 49 cm, with no symptoms or laboratory evidence of hypocalcemia.
Discussion
PHPT is a rare condition in pregnancy [2,7].We present a PHPT case who became pregnant even with a diagnosis of the disease previously confirmed, and then underwent surgery for adequate hypercalcemia control. For the general population, hypercalcemia is defined as total serum calcium above 10.5 mg/ dL (>2.6 mmol/L). In a pregnant patient, the serum albumin falls due to hemodilution and remains low until delivery. Calcium is transferred through the placenta to mineralize the skeleton, and the glomerular filtration rate is increased, culminating with lower total calcium levels. Due to these factors, the upper limit of the reference range for corrected calcium in pregnancy is about 9.5 mg/ dL (2.3 mmol/L) [8,9]. This patient became pregnant at 45-yearsold. In addition to increased calcium and PTH, she presented with low phosphate and elevated 1.25(OH)2D. Most patients with PHPT are older than 50, but the disease is diagnosed during childbearing years in 25% of females [10]. Inappropriately high serum PTH concentration leads to increased renal reabsorption of calcium, phosphaturia, and 1.25(OH)2D synthesis, resulting in hypercalcemia and hypophosphatemia, loss of cortical bone, hypercalciuria, and various sequelae of chronic hypercalcemia [11]. During the course of her pregnancy, the patient presented symptoms of hypercalcemia as the serum calcium increased; such symptoms do not depend on gestational age, as they are the same for non-pregnant women [6,12].
A pregnancy in a patient with hyperparathyroidism may have maternal complications of 67%, and in neonates it would be about 80% [2]. The most frequent maternal complications are hyperemesis and nephrolithiasis; less frequently, preeclampsia and pancreatitis occur [2,6]. Fetal complications may include miscarriage, neonatal seizures, low birth weight for gestational age, and hypocalcemia [3,13]. This patient and her newborn did not present complications, probably because gestation was monitored from the beginning and surgery was performed in the second trimester to control calcemia. In a normal pregnancy, PTH levels are low during the first trimester compared to nonpregnant women and remain normal through the rest of the pregnancy. The relatively low PTH may be due to the suppressive effect of raised 1.25(OH)2D [14]. In this patient with primary hyperparathyroidism, high PTH levels were due to the autonomic secretion of the adenoma, preventing its fall as calcium levels raised. As such, continuous reabsorption of calcium of the bones occurs, as well as an increase of the tubular reabsorption of calcium, including intestinal absorption secondary to 1.25(OH)2D levels [15]. This modifies what physiologically occurs in gestation, when maternal calcium falls by about 10%; the current patient presented calcium within reference values at the beginning of the investigation, which increased progressively. The therapeutic measurements in the first trimester were sufficient to maintain serum calcium at the maximum level of 11.6 mg/dL (2.89 mmol/L); however, in the second trimester, calcium increased to 12.76 mg/dL (3.18 mmol/L). The incidence of pregnancy loss and its relationship to calcium elevation is not entirely known. Fetal loss is seen at all levels of elevated maternal calcium, but it is suggested that calcium levels higher than 11.4 mg/dL (2.85 mmol/L) may increase the risk of adverse events for both mother and fetus [16].
The patient urinary calcium was already high before pregnancy, with previous nephrolitiasis. Characteristic of the gestational period is an increase of calciuria [17]. Despite increased fluid intake, the risk of new kidney stones could be high, especially because she was put on furosemide in order to control hypercalcemia, which was an additional concern in deciding on surgery. This patient had low levels of VD. It has been demonstrated that even in tropical countries, its prevalence in pregnant women may exceed 80% [18,19]. In a normal pregnancy, 1.25(OH)2D may be twice as high compared to non-pregnant women [17]. However, this patient’s 1.25(OH)2D was very high: levels of the transporter 1.25(OH)2D protein, secondary to hyperestrogenism proper to gestation, and an increase in free 1.25(OH)2D production (due to increased activity of 1 alpha hydroxylase stimulated by parathyroid hormone-related protein (PTHrp), estrogen, prolactin, and placental lactogen hormone) are relevant factors that contribute to this issue. In addition, the synthesis of 1.25 (OH) D is increased by the activity of placentary 1 alpha VD hydroxylation [20,21]. In this case, elevated PTH was an additional factor that increased the 1.25(OH)2Dto such high levels. We prescribed VD based on the low levels presented, since the patient would need surgical correction of the hyperparathyroidism, with 1.25 (OH) D returning to normal pregnancy levels (and thereby revealing VD deficiency). There are no specific guidelines for treatment of hyperparathyroidism during pregnancy, as the approach is individualized according to the severity of hypercalcemia, the symptoms presented, a worsening of the clinical condition, and laboratory parameters.
During pregnancy hydration, enhancement and forced diuresis are measures that can avoid severe increases in serum calcium. The medications used for this purpose are class C and D for a pregnant woman, including calcitonin, cinacalcet, and furosemide. Bisphosphonates belong to category D [5,22]. We decided to prescribe a category C drug, with furosemide being the most accessible medication for the patient. However, a 40 mg/ day dose was not sufficient to control hypercalcemia, as she had continued clinical symptoms; thus, we decided not to introduce a new medication, but to refer the patient to surgery in the second trimester. Surgery is avoided in the first trimester due to increased risk of miscarriage, and in the third trimester, due to risk of preterm birth [23]. Although uneventful surgery has been done in the third trimester [24], the second trimester is the ideal time, as it is the period with potentially lower risks for fetal complications [12,25]. The patient underwent surgery, with excision of the left inferior parathyroid at the end of the second trimester: both she and the newborn were free of complications.
Conclusion
Patients with hyperparathyroidism who become pregnant need special attention for the development of clinical symptoms, the monitoring of laboratory parameters, and appropriate therapeutic interventions, given the occurrence of certain events. Since the management of pregnant women with hyperparathyroidism is relatively limited, we present a successful case here, which is aimed at discussing its clinical aspects, expected laboratory changes, and therapeutic possibilities.
To know more about Juniper Publishers please click on: https://juniperpublishers.com/aboutus.php
For more articles in Open Access Journal of Reviews & Research please click on: https://juniperpublishers.com/arr/index.php
To know more about Open Access Journals please click on: https://juniperpublishers.com/journals.php
#reviews research paper#Juniper Publisher Reviews#JuniperPublishers#Hyperparathyroidism#Multiple endocrine neoplasia syndrome#juniper publishers indexing juniper publishers journals
0 notes
Text
Cylinders and Assemblage- Sertoli-Leydig Cell Tumour -Ovary
Sertoli-Leydig cell tumour is an exceptionally discerned, ovarian neoplasm composed of sex cord or Sertoli cells admixed with stromal component expounded by Leydig cells. Sertoli-Leydig cell tumour may occur in association with DICER1 syndrome or emerge as a sporadic phenomenon. Sertoli-Leydig cell tumour manifests as well differentiated, moderately differentiated or intermediate grade and poorly differentiated neoplasms. Additionally, categories such as Sertoli-Leydig cell tumour with heterologous elements or retiform variant of Sertoli-Leydig cell tumour may be expounded. Majority of paediatric Sertoli- Leydig cell tumours are moderately differentiated or poorly differentiated, concur with DICER1 syndrome and frequently display heterologous elements or retiform tumour configuration. Histological categorization of neoplasms with enhanced tumour grade appears challenging [1,2].
Well differentiated tumefaction exhibits distinctive Sertoli cell and Leydig cell components. Moderately differentiated or minimally differentiated neoplasms appear devoid of well-formed Sertoli cell tubules with scant Leydig cells [1,2].
The infrequent, paediatric, preponderantly unilateral ovarian neoplasm is commonly delineated within young females with mean age of tumour emergence at 25 years although postmenopausal women may be implicated. Retiform tumour configuration or germline DICER1 mutations occur in neoplasms occurring in younger females [1,2].
Sertoli-Leydig cell tumour is associated with DICER 1 syndrome which is an exceptional, tumour predisposition syndrome engendered by germline mutations within DICER1, a gene which encodes RNase III enzyme confined to microRNA maturation pathway.
Germline mutation expounds as a truncating mutation which may comprehensively incriminate the gene. Second hit somatic mutation occurs as focused, hotspot missense mutation implicating RNase IIIb domain of DICER [1,2].
Sertoli-Leydig Cell Tumour Exhibits Distinctive Molecular Subtypes as
• DICER1 mutant wherein moderately differentiated or poorly differentiated tumour exemplifies heterologous elements or retiform configuration and incriminates young subjects [1,2].
• FOXL2 c.402C>G (p.Cys134Trp) mutant wherein moderately differentiated or poorly differentiated tumefaction is devoid of retiform component or heterologous elements and incriminates postmenopausal women [1,2].
• DICER1 / FOXL2 wildtype wherein well differentiated neoplasm appears devoid of retiform component or heterologous elements and implicates middle aged women.
• somatic hotspot DICER1 mutations are frequently associated with germline DICER1 mutations [1,2].
• DICER1 mutations commonly appear within moderately differentiated or poorly differentiated neoplasms. In contrast, well differentiated tumours are devoid of DICER1 mutations [1,2].
• Sporadic, moderately differentiated or poorly differentiated Sertoli-Leydig cell tumours harbour somatic mutations within hotspot of DICER1 gene. FOXL2 mutation may concur with DICER1 mutations [1,2]. Clinical symptoms of hormonal or androgenic activity are discerned. However, certain representative features may concur or recede, as denominated with characteristic androgenic symptoms or tumour emergence within elderly, peri-menopausal or postmenopausal women. Clinical manifestations as pelvic pain or pelvic tumefaction may be discerned. Ascites or tumour rupture is exceptional [1,2]. Androgenic hormonal symptoms or virilisation is commonly represented as hirsutism, clitoromegaly, breast atrophy, menstrual irregularities or amenorrhea [1,2]. Oestrogenic hormonal manifestations are infrequently observed. Histological subtype and tumour grade are concordant to clinical behaviour [1,2]. Upon gross examination, predominantly unilateral tumefaction may demonstrate a cystic component, foci of heterologous elements or retiform configuration. Poorly differentiated neoplasms exhibit foci of tumour necrosis. Tumour magnitude varies from < 1 centimetre to ~ 35 centimetres with mean diameter of 12 centimetres to 14 centimetres. Characteristically, cut surface is solid and tan to yellow [1,2). Frozen section exemplifies an admixture of Sertoli cell tubules or compressed cellular cords variably intermingled with Leydig cell clusters. Intracytoplasmic Reinke crystals may be delineated [1,2].
• Well differentiated Sertoli-Leydig cell tumour expounds open or compressed Sertoli cell tubules admixed with clusters of Leydig cells accumulated within intervening stroma. Cellular and nuclear atypia or mitotic activity is absent [1,2]. Sertoli cells appear as low, columnar to cuboidal cells with spherical to elliptical nuclei, nuclear grooves and miniature nucleoli. Leydig cells demonstrate abundant, eosinophilic cytoplasm with characteristic Reinke crystals, lipofuscin pigment and spherical nuclei [1,2].
• Moderately differentiated Sertoli-Leydig cell tumour characteristically depicts diffuse or lobulated architecture with alternating hypo-cellular and hyper-cellular areas. Sertoli cells configure compressed tubules, cords or diffuse sheets wherein cells are imbued with hyperchromatic, elliptical or spindle-shaped nuclei. Mild to moderate nuclear atypia and mitotic figures ~ 5 per 10 high power fields are discerned. Exceptionally, miniature clusters of Leydig cells appear commingled with Sertoli cell component. Discernible follicular differentiation may simulate juvenile granulosa cell tumour [1,2].
• Poorly differentiated Sertoli-Leydig cell tumour is constituted of diffuse sheets of immature, sarcomatoid Sertoli cells with configuration of infrequent, indistinct cords. Nuclear atypia is moderate to marked. Mitotic activity is significant with ~ 20 mitoses per 10 high power fields. Undiscernible Leydig cells are represented by few, miniature clusters, characteristically accumulated upon periphery of tumour nodules [1,2].
• Sertoli-Leydig cell tumour with heterologous elements is constituted of epithelial or mesenchymal elements represented within moderately differentiated, poorly differentiated or retiform Sertoli-Leydig cell tumour. Benign, borderline or malignant intestinal or gastric type mucinous epithelium is a common heterologous element. Trabecular or goblet cell carcinoid tumour may arise from heterologous mucinous epithelium. Heterologous mesenchymal elements as cartilage or skeletal muscle are uncommon. Focal differentiation into hepatic parenchyma and elevated serum α-fetoprotein (AFP) levels is infrequent [1,2].
• Retiform variant of Sertoli-Leydig cell tumour demonstrates focal or diffuse retiform pattern with configuration of anastomosing, slit-like, irregular spaces or multi-cystic, sievelike or papillary architecture [1,2].
Sertoli-Leydig cell tumour is immune reactive to general sex cord proteins as inhibin, calretinin, SF1, FOXL2, CD56, WT1, CD99, vimentin, pancytokeratin, Melan A/MART1, CK20, CDX2, AFP, arginase or HepPar1 [3,4]. Sertoli-Leydig cell tumour is immune non-reactive to CK7 or EMA.
Neoplasm is devoid of histochemical staining with reticulin.
Sertoli-Leydig cell tumour requires segregation from neoplasms such as endometrioid adenocarcinoma, adult granulosa cell tumour, fibroma or tubular Krukenberg tumour emerging from metastatic signet ring cell carcinoma. Retiform variant of Sertoli- Leydig cell tumour necessitates distinction from yolk sac tumour or low grade, borderline serous carcinoma ovary. Sertoli-Leydig cell tumour with heterologous elements mandates distinction from carcinosarcoma, teratoma and primary or metastatic ovarian mucinous neoplasms [3,4].
Sertoli-Leydig cell tumour can be assessed with pertinent clinical examination of young women manifesting features such as virilisation with elevated testosterone levels. An ovarian or pelvic tumefaction can be detected upon imaging. Intraoperative frozen section is optimal for cogent tumour evaluation and adoption of relevant surgical procedures. Incriminated subjects depict elevated serum testosterone levels. Sertoli-Leydig cell tumour can be appropriately investigated with imaging of pelvic cavity with techniques as ultrasonography, computerized tomography or magnetic resonance imaging. Upon imaging, a preponderantly solid or solid and cystic adnexal tumefaction is denominated [3,4].
Genetic counselling and assessment of germline DICER1 mutation is recommended [3,4].
Optimally, Sertoli-Leydig cell tumour occurring in young women is treated with fertility sparing surgical techniques. Sertoli-Leydig cell tumour can be appropriately managed with conservative, fertility sparing surgical procedures as unilateral salpingo-oophorectomy. Cogent tumour staging along with or devoid of regional lymph node dissection can be performed in young women exemplifying stage I tumours. Incriminated elderly females, where fertility preservation is unnecessary, can classically be subjected to bilateral salpingo-oophorectomy, total abdominal hysterectomy and comprehensive surgical staging of tumefaction. Platinum based adjuvant chemotherapy is beneficial in treating moderately differentiated or poorly differentiated tumours and neoplasms with heterologous mesenchymal elements, advanced tumour stage or tumour rupture [3,4].
Biological behaviour is contingent to histological subtype and tumour grade. Well differentiated Sertoli-Leydig cell tumours are essentially benign neoplasms whereas ~ 10% of moderately differentiated and ~59% of poorly differentiated tumours demonstrate malignant biological behaviour. Occurrence of heterologous elements, retiform tumour configuration, tumour rupture, tumour dissemination beyond ovary, stage II or advanced stage neoplasms delineate an adverse prognostic outcome. Neoplasms demonstrating germline DICER1 mutations exhibit favourable prognosis, in contrast to tumours with singular somatic DICER1 mutation [3,4].
To Know More About Global Journal of Reproductive Medicine https://juniperpublishers.com/gjorm/index.php
0 notes
Text
Juniper Publishers- Open Access Journal of Case Studies
Ectopic Scar Pregnancy in a 31-year-old Female with Comorbid: A Case Report and Literature Review
Authored by Sanaa Aslam
Introduction
An ectopic pregnancy is the implantation of a pregnancy outside the normal uterine cavity. One in 80 pregnancies are ectopic [1]. Caesarean scar ectopic pregnancy is considered the rarest among ectopic pregnancies. It occurs when the blastocyst implants in a previous Caesarean section scar instead of at the usual site in the uterus. It has an estimated incidence of ~1:1800-2200 pregnancies [2,3]. The overall incidence of this rare form of ectopic pregnancies is increasing worldwide. The current incidence of this type of ectopic pregnancies in women with a previous scar is 6% [4]. The Caesarean section scar can lead to improper healing which makes it more susceptible to implantation. This form of a pregnancy can be life threatening for the mother. In 1978, the first case of a caesarean scar ectopic pregnancy was reported [5]. This form of a pregnancy is usually diagnosed at a gestational age of 5 to 12 weeks [2]. The time interval between the Caesarian section and this type of a pregnancy, on an average, is 6 months to 12 years! [2]. Early diagnosis and recognition of the type of pregnancy can lead to improve in the morbidity and mortality associated with this condition. Prompt treatment leads to fewer complications.
Rationale
No sufficient documentation is available on the incidence and the prevalence of this form of pregnancy in my country, Pakistan. These forms of literature will further set up grounds for research in this area and hopefully lead to more awareness about the condition.
Case Report
My patient, known case of chronic HTN, came to the OPD with complaints of severe vaginal bleeding for one week. She was sent to the labor room for further assessment. Further history revealed that there was mild PV spotting since the onset of this pregnancy on and off. The bleeding would resolve spontaneously in between, and she sought no medical treatment. Over a duration of one week, the bleeding increased in severity and she would have to change pads 2 to 3 times daily. This was also associated with severe lower abdominal pain, dizziness, lethargy and shortness of breath. A night before her arrival at the hospital, the bleeding intensified, and the blood had then started coming in fist sized clots. She rushed to the hospital. Her past obstetric history revealed 4 previous scars due to cephalopelvic disproportion and 2 miscarriages. She also reported use of copper intrauterine device in the last 3 years. She had well controlled HTN and was on oral medication. Her general physical examination revealed transverse scars, pallor and areas of excessive pigmentation. Her abdominal examination revealed scar tenderness.
On admission, her urine R/E was normal. Blood CBC showed Hb at 8.30mg/dL. Her B-HCG was 508.62mIU/mL. Her USG abdomen/pelvis revealed a large, ill-defined lobula. Heterogeneous mass in the lower anterior segment. An MRI of the pelvis was done which showed an enlarged uterus (25 x 90 x 80mm) with an endometrial cavity of 6mm. A large heterogeneous mass with abnormal signal area. A few high signal foci indicative of hemorrhage and a mass in the myometrium effacing the endometrial cavity at the site of the Caesarean section scar. No bladder involvement. Management decided, at the time, was expectant. Orders to watch for bleeding, Inj. Tranexamic acid 11gm IV stat and Inj. Methotrexate 1mg/kg IM stat were given along with serial B-HCG levels. 6 hours into admission, the patient started bleeding profusely with the passage of massive clots. There were no signs of shock. She was transfused 4 units of PRBCs and given further injections of Tranexamic acid. Her bleeding was controlled 3 hours later. She was taken to the Operative room and Uterine Artery Embolization was performed. Hysterectomy was on hold because of the patient’s wish to preserve her fertility.
Discussion
A scar pregnancy is a life-threatening condition. Early recognition of the disease and prompt management can lead to a much better prognosis. These pregnancies have a chance of the development of other morbid conditions like Placenta accreta, placental abruption and other forms of ectopic as well as heterotropic pregnancies.
Patients usually present to the Emergency with painless vaginal bleeding in the first trimester. This bleeding is on and off and can range from mild spotting to the passage of clots associated with heavy bleeding. Proper history and relevant investigations can lead to the diagnosis of ectopic pregnancy and furthermore, scar pregnancies. Initially, a Transvaginal Ultrasound or a color flow Doppler are the modalities of choice. An MRI is performed when the facility is available or in cases when the TVUSS is inconclusive.
Treatment options are many but currently, two major problems exist. The control of bleeding and hemorrhage and the nonviable pregnancy.
For minor bleeding, medical management is sought. Tranexamic acid is an effective agent and is given intravenously as an injectable. IF bleeding is not controlled and blood loss is massive, and the patient is at a risk of hemodynamic instability, consider surgical intervention. Uterine Artery Embolization is now done and is an effective intervention without many complications [6].
For medical management of the pregnancy, systemic methotrexate is given as an injectable according to the body weight of the patient. There has recently been the advent of an ultrasound guided local injection of methotrexate. According to a study published in January 2018 [7], a comparison was made between the efficacy and side effect profile of the local and the systemic methotrexate regimens and it concluded that the local MTX injection treatment may be a better choice for postoperative improvement prognosis and better outcomes than systemic MTX treatment for cesarean section scar pregnancy in combined normal intrauterine pregnancy, in light of adverse effects of MTX on intrauterine pregnancy. The rate of success of local MTX treatment was significantly higher than that of systemic MTX treatment. It was 93.75% vs. 73.33%, respectively (P<0.05>) [7].
Surgical excision of the scar can also be done which will lead to a lower chance of recurrence and can be considered a key management option [8].
Conclusion
With the rise in the number of operative deliveries and diagnostic procedures being performed in the modern world, there has also been a rise in the number of ectopic, and more specifically scar pregnancies. Patients with scar pregnancies are considered high risk. Timely diagnosis and serial monitoring are important to prevent any unwanted events and to protect the life of the mother. Reporting of these rare cases is crucial and further research needs to be done in this field.
To know more about Juniper Publishers please click on: https://juniperpublishers.com/manuscript-guidelines.php
For more articles in Open Access Journal of Case Studies please click on: https://juniperpublishers.com/jojcs/index.php
#JuniperPublishers#juniper publishers journals#Surgical case reports#Emergency Medicine#Critical Care Medicine#Infectious Diseases#Pathology
1 note
·
View note
Text
Quality by Design in Enzyme Catalyzed Reactions-JuniperPublishers
Journal of Chemistry-JuniperPublishers
Abstract
Quality by Design is the new-age path chosen towards achieving the demanding quality standards in pharmaceutical industry. The present paper aims to throw light on Pharmaceutical Quality byDesign (QbD) and how its implementation will help manufacture better quality of Pharmaceuticals. Quality by Design is introduced along with its key elements to help make the understanding process easier. To attain built-in quality is the primary objective of Quality by Design. Finally, it can be said that the quality that is achieved by end product testing is not something that can be guaranteed unlike the quality assurance that can be provided by Quality by Design.
Keywords: Quality by Design (QbD); Quality Target Product Profile; Design Space; Critical Quality Attributes
Go to
Introduction
“Quality Can Be Planned.”-Joseph Juran
The above quote is self-explanatory when it comes to product quality in the pharmaceutical manufacturing industry. Quality by design (QbD) is not very old but a recent inclusion in the pharmaceutical industry. It`s sole objective is to achieve better quality standards that is especially important in the pharmaceutical industry. The QbD approach consists of various components, important ones being risk assessment, assessment and management of the identified risks, design of experiments (DoE), quality target product profile (QTPP), and establishing a control strategy to keep the product within the design space that was created with the QbD study [1]. Out of all the components, a lot of pharmaceutical development studies have incorporated DoE for a more rational approach [2].
The target of analytical QbD approach is to establish a design space (DS) of critical process parameters (CPPs) where the critical quality attributes (CQAs) of the method have been assured to fulfil the desired requirements with a selected probability [3-4].
The principles that are involved in the pharmaceutical development and are relevant to QbD are all described in the ICH guidelines (ICHQ8-11) [5].
Any Pharmaceutical Development Process Typically Covers the Following Sections:
a) Complete portfolio including all the details as well as analysis of the Reference Listed Drug Product
b) Quality Target Product Profile (QTTP) compilation.
c) Figuring out the Critical Quality Attributes (CQA)
d) Complete characterization of API &CMA (Components of Drug product) identification of the API
e) Excipient selection& excipients CMA identification
f) Formulation Development
g) Manufacturing Process Development [6]
Quality Target Product Profile (QTPP) describes the design criteria for the product, and should therefore form the basis for development of the CQAs, CPPs, and control strategy.
Critical Quality Attributes (CQA) – A physical, chemical, biological, or microbiological property or characteristic that should be within an appropriate limit, range, or distribution to ensure the desired product quality (ICH Q8) Critical Process Parameter (CPP) – A process parameter whose variability has an impact on a CQA and therefore should be monitored or controlled to ensure the process produces the desired quality. (ICH Q8) Critical Process Parameters (CPP) identification and their impact analysis is done by conducting a preliminary risk analysis for every process parameter (PP) that is involved in the individual unit operations.
Need for QbD in Pharmaceutical Industry [7,8]:
a) To integratepatient needs, quality requirements and scientific knowledge all in one design while the pharmaceutical product is still under developmentand further extending to the manufacturing process.
b) To have a better understanding about the impact of raw materials and process parameters on the quality of the final product. This is especially important for biopharmaceutical products since raw materials like cell culture media can be the risk for variability, effecting important factors likecellular viability, cell growth and specific productivity.
c) To collaborate closely with rest of the industries and the regulators and successfully keep up with the regulatory reviews
d) To maintain harmonization in all the regions so that a single CMC submission worldwide is all that is needed.
e) To encourage continuous quality improvement for the benefit of patients.
f) To enable better product design that will have less problems while manufacturing, thus facilitating more efficiency in the manufacturing process.
g) To make post-approval changes easier since it will be contained within a pre-defined design space, thus resulting in regulatory flexibility.
Every production process in a pharmaceutical industry to implement certain control strategies with the ultimate goal of a robust process. A robust process is the gateway to high product quality at the end of the day [9]. Process variability stands as a hurdle to process robustness, and this originates from lack of control on the process parameters. Thus, QbD steps-in to avoidbatch to batch variability in pharmaceutical products [10].
The net outcome of the detailed QbD study (applied in any product) is the segregation of process parameters with respect to their criticality and the finalization of a proven acceptable range (PAR) for every operation. The knowledge that is gained post the QbD evaluation encompasses every minute detail of the operational process as well as the product in general, and lead to the defining of a Design Space. This way, the impact that the manufacturing process might have with regard to the variability of the CQAs becomes apparent, which helps in strategizing testing, quality and monitoring of batches [11].
Process Evaluation: Linking Process Parameters to Quality Attributes
It is important to carefully evaluate the process completely before applying QbD to it. The better knowledge you have of the process, the more effective your QbD will be. Moreover, process characterization is required to specify the proven acceptable ranges (PAR) for critical process parameters (CPPs). In the traditional approach that is implemented in biopharmaceutical production, existing empirical process knowledge is used on a daily basis. However, this approach leads tolaborious and time consuming post approval changes during process adaptation and any new technology implementation that may have become necessary for raising the efficiency of the process. Also, the effects aprocess scale-up can have on the quality of the final product cannot be predicted when using the empirical process development.
This can increase costs and also can cause difficulty in implementing any changes in the set manufacturing process. Thus was born a way to achieve deeper understanding of processes which would lead to greater flexibility and freedom to effect changes. The concept of operation under a pre-defined design space gave this flexibility. Design space is nothing but a concept that is a part of the “Quality by Design” (QbD) paradigm. Now, manufacturers are to follow a science-based process development than their empirical counterpart.
The QbD Concept is Best Explained in this Flowchart Below
Define a Quality Target Product Profile (QTPP) for product performance
⇩
Identify its Critical Quality Attributes (CQAs)
⇩
Create experimental design (DoE)
⇩
Analysis done to understand the impact of Critical Process Parameters (CPP) on CQAs
⇩
Identify and control the sources of variability.
Process characterization sets the ball rolling in any process development, which employs a sound risk assessment rating the various critical process parameters according to their importance [12-14].
Downstream Processing in Biotransformation
Downstream processes of biopharmaceutical industry essentially include the following steps:
a) Harvesting
b) Isolation
c) Purification
Various unit operations that constitute any biopharmaceutical process follow a designed sequence to form an integrated process [15]. Thus, any change in any one of the one-unit operation can affect the functioning of the subsequent unit operations. This is the reason why interaction effects between participating parameters across unit operations should also be taken into account during the process development. Interactions are said to happen when setting of a parameter will show effect on the response of another parameter. Due to this dependence between the parameters, the combined effects of any two parameters hailing from different unit operations cannot be predicted from their individual effects. Regulatory authorities demand inclusion of interactions of parameters within the QbD approach during any process optimization [16]
Example: Downstream processing of 1, 3-propanediol
Process: Fermentation
Fermentation broth that uses flocculation, reactive extraction, and distillation was studied. Flocculation of soluble protein as well as cellular debris that were present in the broth was carried out by using optimal concentrations of chitosan (150 ppm) and polyacrylamide (70 ppm). It was seen that the soluble protein that was present in the broth decreased to 0.06 g L-1. Recovery ratio (supernatant liquor: broth was found to be greater than 99% (Figure 1) [17,18].
The above flowchart shows a typical fermentation process broken down in steps. Glycerol fermentation process is taken as example for the illustration [19].
Go to
Case Study for API
API product development from the very nascent stages require a lot of planning when implementing QbD at every stage. Whether it is two-step process or a multi-step process, each and every operation and parameter needs to be scrutinized before creating a relevant design space. Brainstorming every possible roadblock that might threaten the quality of the final pharma product is what will help design a top-quality process. A futuristic vision is important in the initial steps of QbD planning. The most important part is to pay sufficient attention to detail lest critical aspects might be missed. This is best done by sitting with the entire development team and taking every minor detail into account. Given below is a case study for a API intermediate development process with the help of QbD that highlights the important steps as to how to go about implementing it from the very beginning of your research. QbD is done best, when it is implemented from the very nascent stage of product development.
Quality Target Product Profile
When making your QTPP, make sure you list down everything from your vendor details to target costing. This step basically asks you to think of every aspect of your product and make a comprehensive profile of it. The specification of quality must be highlighted here with all the challenging impurities that might threaten your quality. Everything from stability testing requirements to raw material quality [20] is encompassed in this stage of QbD.
CQA Determination
Given below are some typical CQA parameters that are considered in most of the enzymatic methods of API intermediate preparations.
a) Purity
b) Chiral purity
c) Enzyme residue
d) Assay
e) Appearance
f) Residual Solvent
g) Yield
h) Polymorphic forms
i) Moisture content
j) Melting point (Table 1)
Initial Risk Assessment
The risk assessment can be done in various ways and is the customizable step in QbD. This part calls for a group-discussion or a team meeting where everyone can list down all possible risks related to the project in discussion and grade each one in the list with the amount of risk that it poses. The simplest module suggests you number them 1, 2, 3 with the increasing or decreasing order of the risk threat. A more complicated and detailed risk assessment requires linking of CQAs and CPAs to highlight the risk of their interdependence (Figure 2) [21].
Post risk assessment, comes the control strategies to be followed to tackle the possible risks that are probable. The control strategies are for you to think and execute to achieve your target quality specifications.
Design of Experiment
This is a valuable tool for channelizing your experimental work, to move ahead in a systematic manner. Design of experiments can be of several types: comparative, screening, response surface modeling, and regression modeling [1].
Comparative Experiments: The aim of this study is simple, i.e., picking best out of two options. The selection can be done by the comparison data generated, which is the average of the sample of data.
Screening Experiments: If you want to zero-in on key factors affecting a response, screening experiments would be the best bet. For this, list down concise list of factors that might have critical effects on response that you desire. This model serves as preliminary analysis during development studies.
Response Surface Modeling: Once you have identified the critical factors that affect your desired response, response surface modeling comes handy to identify a target and/or minimize or maximize a response.
Regression Modeling: This is used to estimate the dependence of a response variable on the process inputs.
A step by step guide is given for the DoE step of the QbD process (Figure 3).
Response columns were filled post experimentation as per the design creation (Figure 4).
Factorial Design Analysis Done as Given Under
Analysis Done First for One of the Responses, “Yield”: (Table 2)
P-Values Were Checked for Significance and Higher P-Value Term Eliminated First to Create a Reduced Model:
(Table 3) (Figures 5 & 6)
Observation
From the above graph, significant interaction between the two terms can be inferred.
Analysis Done for the Response “Diacid”: (Table 4)
P-values Checked for Significance and Higher P-Value Term Eliminated First to Create a Reduced Model: (Table 5) (Figure 7)
Observation
From the above graph, significant interaction between the two terms can be inferred.
Response Optimizer Was Used to Optimize Both The Terms With Respective to The Given Responses- Yield and Diacid: (Table 6) (Figure 8)
The optimized parameters predicted for maximum yield and minimum impurity (of di-acid) was found to be 8pH and 37C.
Go to
Case Study 2
As mentioned before, regression analysis is another important tool that can be used to study existing data. This means that if you have done some experiments (without designing them beforehand), you can quickly run a regression analysis of the collected data to derive a relationship between CPPs and the reaction results.
A lot of times, when one follows the one-factor-at-a-time optimization process, by the time any CPP is optimized, a lot of data stands generated. Instead of just tabulating the data and wasting time manually making sense out of them, regression analysis can come to your rescue. As always, graphical data representation seems much easier to understand and also saves your valuable time.
The effect of pH was studied [22] separately in the preparation of deoxynojirimycin base (stage III). The reaction involved N-formyl amino sorbitol, water, oxygen and whole cells of Gluconobacter oxydans DSM2003. Later involvement of sodium hydroxide and sodium borohydride gave rise to deoxynojirimycin. Further work-up and 2-methoxy ethanol facilitated crystallization yielded Deoxynojirimycin base. In this experiment, pH of the reaction was changed to find out its role during the reaction and a regression analysis was run using Minitab to study this affect.
Observations recorded showed that reaction did not occur at pH2 and at pH8, the reaction did not reach completion. The optimum pH range between 4 to 6 showed certain effect on yield and purity. The significance of pH variation during the reaction was thus established as described below (Graphs 1-3):
When null hypothesis p-test was carried out, no significant effect of pH was to be found on product purity, impurity1 and impurity2, but its significant influence was seen in minimizing impurity3.
Furthermore, large-scale batches conducted were statistically analyzed as well to achieve better understanding of the influence of list of parameters on the output obtained. The following parameters were studied during the stage III reaction described above:
a) pH, RPM and Oxygen cylinders consumed during the course of the reaction.
Their effect on the output and reaction completion time was studied. It was seen that only RPM showed statistically significant effect on the reaction completion time and rest of the factors did not contribute to any significant effect on the output or reaction completion time.
During biotransformation process, i.e. during oxidation of N-formyl using Gluconobacter oxydans DSM2003 whole cell, three main unknown impurities peaks were observed in HPLC chromatogram while reaction monitoring. This process is capable of removing these three impurities during down streaming, work up & isolation to the levels mentioned below:
a) Impurity 1 (has defined RRT on HPLC chromatogram) not more than 3%
b) Impurity 2 (any other unknown impurity) not more than 1%
c) Impurity 3 (has defined RRT on HPLC chromatogram) not more than 10 %
Since higher level of impurities affect the yield of the process, efforts were carried out to study the factors which can reduce the formation of process impurities.
Go to
Conclusion
The concept of Quality by Design (QbD) is highly reliable when it comes to achieving foolproof quality of your product. This is a modern tool that is going viral in Pharmaceutical industry especially because this industry demands high quality standards and tolerates no compromise when it comes to the quality. Breaking down QbD, it essentially comes down to identifying the critical parameters of the process and assigning a particular design space for every single critical attribute. Thus, QbD can be considered as an intelligent approach to quality that yields robust processes. QbD also ensures that there is continuous improvement in the process during the entire lifecycle of a Pharmaceutical product [23].
Go to
Acknowledgement
Our group would like to thank the Department of Scientific and Industrial Research India, Dr. Hari Babu (COO Mylan), Sanjeev Sethi (Chief Scientific Office Mylan Inc); Dr. Abhijit Deshmukh (Head of Global OSD Scientific Affairs); Dr. Yasir Rawjee {Head - Global API}, Dr. Sureshbabu Jayachandra (Head of Chemical Research); Dr. Suryanarayana Mulukutla (Head Analytical Dept MLL API R & D) as well as analytical development team of Mylan Laboratories Limited for their encouragement and support. We would also like to thank Dr. Narahari Ambati (AGC- India IP) & his Intellectual property team for their support.
To know more about Journal of chemistry,
Click here:
https://juniperpublishers.com/omcij/index.php
To know more about juniper Publishers,
click here:
https://juniperpublishers.com/index.php
#Juniper Publishers group#Juniper Publishers#JuniperPublishers#Juniper Publisher Reviews#Juniper Publishers Indexing Sites List#organic chemistry#inorganic chemistry#Open access Journal of chemistry#chemistry journal#chemistry#open access journals
3 notes
·
View notes
Text
Qualitative Approach to Understanding Barriers to Delivering Difficult News in Sub Saharan Africa- Juniper Publishers

Dear Editor,
Communication, especially delivery of difficult news (DDN), remains a key part of clinical practice. Despite its importance, many medical providers lack the skill and ability to effectively DDN to their patients. Due to lack of data specific to sub-Saharan Africa and to help us develop an appropriate training tool for this geographical area, we sought to explore what challenges and barriers residents at our institution faced when they deliver difficult news to their patients.
Methodology
A qualitative approach using thematic analysis was adopted and a self-administered open ended survey was administered amongst residents currently doing their Masters in Medicine at the Aga Khan University Hospital in Nairobi and Dar es Salaam. The survey was emailed to all the residents within the two campuses using the REDCap software. Two independent researchers identified recurring themes and categorized barriers into either: physician, cultural or institutional. All residents provided written informed consent prior to participation in this study.
Results
A total of 105 residents participated in the survey (response rate 70%). The most frequent physician barriers identified were lack of training opportunities and time to DDN. More than fifty percent of the residents stated that cultural diversity, gender role-play and discussing dying as a taboo subject were the most common cultural barriers. Approximately 4 out of 10 residents faced institutional barriers such as lack of time due to busy schedules especially when on call, lack of private spaces to hold these conversations and limited mentorship/guidance by the faculty when having difficult conversations with patients.
Discussion
Physician barriers: Only 42.1% of the residents in our study had received any formal training in DDN. A study conducted in Nigeria looking at breaking bad news among nurses and physicians showed that only 21% of the respondents had formal training to do so [1]. Similarly, minimal formal training in conducting complex discussions were reported by health care providers in a Tanzanian health care facility [2]. In addition, our resident expressed lack of mentorship and support from faculty members in delivering difficult news to their patients.
Cultural barriers: Our residents felt that the diversity of cultures at our institutions greatly influenced the DDN to their patients, especially if different than their own. Similarly, Periyakoil and colleagues also found that many physicians struggle with end of life conversations especially in patients with a different ethnicity than their own [3]. Female residents at our institution were not taken seriously and struggled with delivery of difficult news compared to their male counterparts. Residents expressed that a majority of patients preferred a male relative be present during DDN. In addition, extended family members, rather than the female spouse, were involved in the decision making process. Our residents also expressed that talking about dying was often seen as taboo for many patients and their families. Further studies are needed to better understand how specific cultures affects effective communication especially in sub-Saharan Africa.
Institutional barriers: Similar to other studies, our residents reported a lack of adequate space and privacy when DDN to patients [2]. Opportunities supported by the institution to train and enhance communication skills were scarce. Similar to other studies, time constraint due to other clinical duties was also reported as a significant barrier [4].
Conclusion
Our study helps shed light on the barriers and challenges our residents face within our institution in delivering difficult news to their patients. This study will help us design and implement effective strategies, unique to sub-Saharan Africa, to better train our resident in DDN to their patients.
To read more articles in
Journal of Surgery
Please Click on:
https://juniperpublishers.com/oajs/index.php
For More
Open Access Journals
in
Juniper Publishers
Click on:
https://juniperpublishers.com/journals.php
#plastic surgery#surgery journals#JuniperPublishers#openacessjournals#Cardiac Surgery Orthopedic Surgery
0 notes
Text
Modified Starch and Its Potentials as Excipient in Pharmaceutical formulations

Authored by Khalid Garba Mohammed
Despite its vast commercial value, native starch has some inherent weaknesses when it comes to pharmaceutical application, to mention few include; poor compressibility, low flow ability values and often drug/excipient compatibility problems. In this review, some potentials of modified starch with particular emphasis on their improved functionalities and applicability in pharmaceutical formulations were discussed. Basic requirements for pharmaceutical excipients and various modification methods for starch i.e chemical modification, physical and biotechnological methods were highlighted.Pharmaceutical applications of modified starches as tablet super disintegrant, sustained/controlled release polymer, plasma volume expanders and as directly compressible excipient in tablet formulations have been cited.
To Read More.. PHP in Novel Approaches in Drug Designing & Development in Juniper Publishers
1 note
·
View note
Text
Prevention of the Development of Diabetes by Early Intervention-JuniperPublishers
Abstract
The current research, a retrospective study on early stage intervention on the development of diabetes is based on a concept discussed in 2011 by Ralph A De Fronzo and Muhammad Abdul-Ghani in a publication by American Diabetes Association.
The Research comprises of early recognition of the patients at the stage of developing IGT and initiation of treatments with oral hypoglycaemic agents in order to reach a normal HbA1C. The overall number of patients in practice were 5000. And those with IGT were 26. The research was started 7 years ago and has resulted in these patients reaching a HbA1C of 5.2. The target of treatment was maintaining lower than 5.2.
Metformin has been mostly effective in patients reaching the target value. However, in rare cases Gliclazide was needed. In one Case Acto's and Insulin treatment was essential for a female patient with Polycystic Ovarian Syndrome. The current success has resulted in preventing further complications from diabetes.
In earlier years clinical were advised to start oral hypoglycaemic agents, once the patients had shown a HbA1C of 7.5. However, the evidences have shown that by this stage many complications from diabetes would have occurred.
Keywords: Oral hypoglycaemic agents; Pre-Diabetics; Metformin
Introduction
There has been a dilemma among clinicians as to when to initiate the oral hypoglycaemic agents (OHA) following non pharmacological approaches e.g. diet, exercise and weight loss. Earlier understand was that the medications can be started after the patient had reached a HbA1C value of 7.5. Current Canadian Guideline are HbA1C of 6.1 being in normal range and those with HbA1C of 6.2-6.5 are considered "Pre-Diabetics" or with IGT. As explained in the article by De Fronzo, et al. [1]. Initiation of treatment with appropriate OHA prevents the development of a full blown diabetes. If the clinicians wait until the patient reaches the HbA1C of 7.5, many complications from diabetes already are existing. My experience dates back to approximately 10 years when a patient of mine with HbA1C of 6.9 was started on metformin and subsequently switched to Gliclazide for effective prevention.
Past Investigations
De Fronzo, et al. [1] had established a link between insulin resistance, diabetes, obesity, hypertension, dyslipidaemia and ASSCVD in 1991. Cusi in collaboration with De Fronzo reviewed the metabolic effects of metformin in 1998 [2].
Subsequently, UKPDS Group had focussed on the intensive glucose control with sulfonylurea or insulin and the risk of complications in the patients with Type 2 diabetes in 1998 [3,4]. Later, UKPDS group advanced their research to metformin use with similar objectives. Turner, et al. [5] in 1999 investigated the role of diet, sulfonylurea, metformin or insulin treatment in patients with Type 2 diabetes in conjunction with UKPDS [4,5].
Knowler, et al. [6] in 2002 emphasized on the reduction in the incidence of Type 2 DM with life-style interventions. Abdul-Ghani in 2006 studied the risk of progression to DM by establishing a relationship between post-load plasma glucose and fasting plasma glucose [7]. Holman, et al. [8] reviewed a 10 year follow-up study with intensive glucose control in Type 2 DM. Eriksson, et al. [9] in 2008 emphasized on the significance of diet and exercise in the prevention of Type 2 diabetes. Lastly, Vendetti, et al. [10] in 2008 investigated the role of lifestyle interventions and weight loss.
Method
My current study of diabetes prevention is based on identification of PRE-DIABETICS among a population of 5000 patients. These patients with HbA1C of more than 6.2 were given a starting does of Metformin of 250mg after their evening meal. There was an equal proportion males and females. A total number of 29 patients were identified in the "pre-diabetics" group. They were offered counselling for the diet, lifestyle interventions and followed by lab investigation after one month. If there was no change in HbA1C the patient was offered Gliclazide 15mg with their evening meal and lab monitoring was continued. The patient identified 10 years ago has a history of sinus arrhythmia and suffers from hypercholesterolemia. He has been maintaining a normal HbA1C like other 28 patients with a low dose of OHA and controlled heart disease. It was commonly observed that one to two months of OHA was sufficient for the patient to reach HbA1C of 6.2 or less, provided the treatment was continued. This approach showed the prevention of further complications from diabetes e.g. hyperlipidemia or renal dysfunction.
The likely contribution factors to IGT indentified were family history, obesity, pancreatitis, alcoholism, gestational diabetes or viral diseases. The age of onset was observe between 40 and 50 years.
Results
The results of the retrospective study are listed in the enclosed Table 1.
Conclusion
Early prevention of patients from developing diabetes was achieved by commencing treatment with either Metformin or Gliclazide. Two of my patients observed having a normal HbA1C in the absence of and OHA after a short term initial medical management while others maintained a normal HbA1C with a small dose of OHA with continuation. The patients have been free of any other co-morbidities e.g. CKD or CVD.
To know more about Journal of Urology
Click on: https://juniperpublishers.com/jojun/index.php
To Read more about JuniperPublishers
Click on: https://juniperpublishers.com/index.php
#Juniper Publishers#Juniper Publishers Review#Juniper Publishers LLC#JuniperPublishers#urology#kidney#kidney disease#Nephrology#Open access journal of Urology#open access journals
0 notes
Text
Journal of Gerontology and Geriatric Medicine-JuniperPublishers

Mini Review
Resiliency is the ability to bounce back from a physical or emotional problem. An emerging public health concept is that attenuation of the aging process with improved resiliency will extend healthy lifespan. By slowing the rate of aging a health dividend is expected whereby the human population will manifest fewer chronic conditions or delay the onset and duration of chronic disabilities that consume over 90 percent of health care costs. In this conceptual framework the European Union has set a public health goal of extending current average life expectancy of the population by a modest 2 years [1-5].
This effort comes at a time when several countries are experiencing a continuous and steady improvement in life expectancy while others, such as the United States, show the opposite trend, likely due to the obesity and opioids epidemics. Thus far, the most convincing anti - aging approaches have been caloric restriction and increased physical activity, but neither of these interventions work uniformly and their alleged global impact often differ between genders. Accordingly, investigators look to oral supplements that improve bioenergetics and metabolism while reducing so -called inflammation. Additional anti - aging approaches include senilities that expunge senescent cells and rejuvenation strategies that employ stem cells. All these approaches attest to the likelihood that no approach alone will achieve healthy lifespan and optimize cognitive, musculoskeletal, cardiovascular and metabolic functions throughout the human lifespan [6-8].
One marker of successful health span interventions is the ability to strengthen resiliency. In essence, human resiliency is the ability to confront a biological or psychological perturbation and return to normal functionality sometime after the disturbance. Figure 1 presents a theoretical graph of how people with high and low resiliency might recover after an acute illness such as community acquired pneumonia. Current health outcomes data suggest at least 5 trajectories of recovery after an acute illness, ranging from rapid recovery to no recovery at all. In the elderly population, the consequence of hospitalization can result in roughly one of three outcomes they return to prehospitalization function, they improve their pre-hospitalization function, or they permanently lose a percentage of their pre - hospitalization function. A few clinical studies suggest that the window for recovery is approximately 60 days, thereafter little gains in recovery are made. Conceptually, the rate of recovery post - hospitalization could be a strong marker of resiliency. In a similar fashion, physiologic recovery from maximal exercise may be a surrogate marker of resiliency. Loss of physiologic reserves and homeostasis with age impair resiliency and one concept is that people with the largest homeostatic reserve early in life maintain their adaptation to stress for a longer period of time than those with lower homeostatic reserve [9]. Stress resistance in the long live mouse models give credence to this concept of "more is better" in terms of robust early life resiliency. Given that rates of human aging exhibit a bell shaped curve, a key question is whether those who rapidly age can be transformed to normal aging as manifest by improved resiliency.
Physical activity has long been associated with improved resiliency, especially against cardiovascular disease risk. Recent evidence suggests that the intensity and duration of exercise is proportional to the cardiovascular risk reduction. In many ways, intermittent exercise resembles the concept of hormesis whereby periodic stressors improve overall resilience. Exercise reverses telomere shortening, improves oxidant stress responsively, strengthens bioenergetics, optimizesproteostasis, and reverses age - dependent loss of insulin sensitivity. Given the general benefits of exercise, emerging studies are examining the potential benefit of physical activity during acute illnesses to expedite post - hospitalization recovery processes.
In addition to exercise, nutritional interventions may enhance resiliency with aging. High dose berry extracts and other food products appear to have anti-oxidant properties. Some common spices such as turmeric have clear anti-inflammatory properties and are used as bio-equivalents to salicylate in clinical conditions such as inflammatory bowel disease. Caloric restriction has a mixed review on its efficacy as a promoter of resiliency in aging. On one hand, caloric restriction appears to improve cellular response to stress, oxidation, and inflammation. But on the other hand, long term caloric restriction has been linked to poor immunologic responses perhaps as a consequence of NK and T cell suppression. Additionally, caloric restriction appears to suppress wound healing and recent human studies suggest that it accelerates osteopenia. Collectively, these observations suggest that longevity extension alone does not necessarily confer higher levels of resiliency. Whether combination caloric restriction and exercise provide synergistic effects on longevity and resiliency has not been substantiated, and in animal studies the combination has adverse effects [10].
The impact of Methuselah compounds on age - dependent changes in resiliency are variable, despite their ability to extend longevity. Rapamycin, a macrolide originally derived from Easter Isle bacteria, inhibits the mTOR signaling pathway that has been associated with the rate of aging. Similar to observations with caloric restriction, rapamycin improves stress resistance at the cellular level, but its immunosuppressive effects may not protect elderly from acute infections. Additionally, the molecular response to stress appears to be inhibited when the mTOR pathway is attenuated, thus raising concerns that rapamycin may further reduce an age - dependent decline in cytoprotective response or proteostasis. Metoformin, another longevity compound which interferes with AMPK activation, may interfere with acute cellular stress responses. As metformin therapy for human aging enters a randomized controlled trial, it will be useful to monitor its effect on resiliency as participants experience hospitalizations from acute infections, strokes and other ischemic and metabolic insults.
Other conceptual approaches to enhance resiliency in aging include removal of senescent cells and stem cell therapy. The idea of "senilities" is to reduce senescent associated secretory phenotypes (SASP) that accelerate aging through secretion of adverse cytokines and non - youthful intercellular products. The cell growth inhibitor and heat shock stimulator, quercetin has been reported as a senolytic in combination with a tyrosine kinase inhibitor. This and other efforts to reduce SASP appear to improve different physiologic functions in rodents, but no evidence exists whether resiliency against infection or acute insults also improves. The impact of stem cell therapy on age- dependent loss of resiliency is less certain, however, gradual loss of organ vitality is thought to be due to changes in the stem cell pool due to epigenetic drift, environmental issues, and somatic mutations. Old donor stem cells can be rejuvenated by plasma from young donor animals (parabiosis) thus suggesting that one approach to improve tissue resiliency is to "transfuse" old donors with a stem cell concoction. Another thought is to suppress age - dependent stimulants of stem cell mutagenesis such as oxidant injury and inflammation, thus preserving a more functional pool of stem cells as we age.
Conclusion
In summary, interventions to extend lifespan do not necessarily improve resiliency, and efforts to create healthy lifespan must take both outcomes into consideration for successful aging. Lifestyle issues, such as robust exercise and Mediterranean - like diets are the most potent stimulants of resiliency, and it remains to be seen whether adjuvants such as Methuselah drugs, senolytics or stem cell therapy, either alone or in combination, optimize healthy lifespan.
To read more articles in Journal of Gerontology & Geriatric Medicine
Please Click on: https://juniperpublishers.com/oajggm/index.php
For more Open Access Journals in Juniper Publishers
Click on: https://juniperpublishers.com/journals.php
0 notes
Text
Juniper Publishers- Journal of Physical Fitness, Medicine & Treatment in Sports (JPFMTS)

Research Article
Corruption in Football of World in 21st Century
*Corresponding author: M Dousti, Department of Sports, Assistant Professor, University of Mazandara, Iran; Email: [email protected]
How to cite this article: M Dousti, A Tahery, Abolfazl darvishi. Corruption in Football of World in 21st Century. J Phy Fit Treatment & Sports. 2018; 2(2): 555582 DOI: 10.19080/JPFMTS.2018.02.555582
Abstract
This article analyses the corruption in football of world in 21st century. In view of the many sporting events that take place every day throughout the world, the number of proven cases of corruption in sport can be put into perspective, even if the considerable percentage of unknown cases are taken into account. The purpose of this research was the study of corruption in football of world. For this purpose is used the documents, books, articles and websites has been associated with the corruption in football of world. The results show that Europe’s football is as advanced as it is more common corruption. The based on this results Football players and officials alike are made fully aware of their obligations under the anti-corruption rules, including their duty to report improper approaches, however trivial they may seem.
Keywords: Corruption; Football; Gambling; Bribers
Introduction
Corruption in sport is nothing new. The first documented case of corruption in international sport is attributed to the athlete Eupolos of Thessalia who successfully bribed three of his competitors in the first combat tournament at the Olympic Games of 388 BC, among them the reigning Olympic champion Phormion of Halikarnassos [1]. Integrity in sport is crucial to its success and to the enjoyment of participants and spectators. Sport is a global activity providing entertainment and enjoyment to an international audience who watch with intense passion. There are isolated occasions where the players involved have been tempted to cheat to gain an advantage over fellow competitors [2]. One of the most widely publicized cases of judging bias occurred during the 2002 Olympic Winter Games in the pair figure skating competition. The Canadian pair was said to have skated a flawless performance, and were expected to win gold before the scores for their program were revealed.
Most accusations of corruption in sport should not be taken too seriously. When athletes lose, they tend to look everywhere else for the blame rather than at themselves. Dishonest wheeling and dealings of their opponents, such as corruption and doping, may also be readily cited as an excuse. When fans see their team lose, the accusation of rigging always quickly arises [3].
corruption in sport is understood as behavior by athletes who refrain from achieving the levels of performance normally required in the sport in question to win the competition and instead intentionally permit others to win, or behavior by sporting officials who consciously perform their allocated tasks in a manner at variance with the objectives and moral values of the relevant club, association, competitive sports in general and/ or society at large.
Set against the background that corruption affects a broad spectrum of sports and that the corruption phenomenon is virulent in every country. Corruption is understood as the use of a position by its occupant in such a way as to fulfill the tasks required of the occupant by the employing institution in a manner consciously different to the objectives of that institution. Such activity results from a desire for advantages for the occupant of the position (or, if that occupant is acting as principal agent, for acquaintances, relatives, associated organizations or parties) from the person or institution benefiting from the actions [4].
In sport, corruption may take the form of behavior by athletes who refrain from achieving the levels of performance normally required in the sport in question to win the competition and instead intentionally permit others to win, or behavior by sporting officials who consciously perform their allocated tasks in a manner at variance with the objectives and moral values of the relevant club, association, competitive sports in general and/ or society at large.
Types of corruption in sport including: Competition results (“competition corruption”), whereby the provider and the recipient of the bribes can be: athletes only; sporting officials and other non-athletes, e.g., referees, only (sometimes without the knowledge of the athletes involved); athletes and officials.
As well as: non-competition-focused decisions by sporting bodies and sports officials (referred to henceforth as “management corruption”), and in particular regarding: host venues for important competitions; allocation of rights (for example for televised transmission); nomination for positions (including honorary positions); commissioning constructions works for sports arenas and other venues.
Although there are parallels both between the causes of corruption and other forms of illicit behavior in sports such as doping as well as between their potential solutions, it is nonetheless still useful to separate the phenomena. The concept of corruption is interpreted differently from nation to nation (and from continent to continent); various types and forms exist, which need to be analyzed in different ways [5,6].
In connection with the allocation of the rights for the TV marketing of the 2002 and 2006 football World Cup Championships, allegations have also surfaced concerning the payment of bribes to association officials. So far however these allegations have had no legal consequences.
The cases discussed here, in which corruption in sports is used to attain certain positions (honorary or otherwise), influence the allocation of television or other rights, or acquire construction contracts, represent “innovations”, which until recently were considered unthinkable. It seems possible that all the areas of activity relating to sport will in future be affected by corruption, in as much as this has not happened already. For this reason alone the categorization of corruption given above can have no claim to completeness.
As for the extent of corruption in sport, it must firstly be mentioned that the extent of corruption depends heavily on the definition adopted that, as we have shown above, is in itself a problematic question. Secondly, it must also be assumed that the known cases merely represent the tip of the iceberg.
In industrialized countries such as Germany, 5% at most of corruption cases are brought to light. The problem of corruption in sport is a particularly great one, going beyond the dimensions of corruption in other areas of human endeavor. In spite of all the problems associated with quantification in ascertaining the extent of non-sporting corruption [7,8].
In view of the many sporting events that take place every day throughout the world, the number of proven cases of corruption in sport can be put into perspective, even if the considerable percentage of unknown cases are taken into account. Even the extent of corruption at the IOC discovered in the late 1990s can be relative. Following intensive internal investigations, just fewer than 10% of the members of the IOC were either cautioned or punished (within the space of one year).
The reduction of the degree of discretionary leeway would also be an efficient anti-corruption measure for other sporting disciplines. In football for example, which has often been associated with corruption on the part of referees, a number of steps towards making referee decisions more objective are conceivable, including electronic registering of balls going out of play, 3D location systems and enabling instant correction of referee decisions via video review [9].
Stricter controls (that is heightened likelihood of discovery and prosecution) and increased penalties could serve to influence the decision calculations of the potentially corrupt in the direction of honest behavior.
The connection between system of control and degree of punishment on the one hand and corruption on the other is however more complex than may first appear. Success in combating corruption depends on the practical measures taken. Iran Football betting has become a business. Government is the custodian of football in our country and all its works from the competitions to get all the other administrative procedures, and the only thing is that people do is play football and watch it!
Despite the large number of studies on corruption in sport [10-25], study about corruption in sport in Iran especially in football has received little attention. In the current atmosphere of sport in Iran, especially football, to fight the corruption in the sport is admirable, and certainly people in sport and football would welcome this, because a significant portion of the layers of corruption in football in Iran has been accumulated. So, powerful and influential network of corruption that exists in football that does not solve short-term programs.
The findings of this research can help the football managers and policy makers to planning for controlling and prevention of corruption and also for building a football full of health.
Methodology
The purpose of this research was the study of corruption in football of Iran and world. Qualitative research is a method of inquiry employed in many different academic disciplines, traditionally in the social sciences. Qualitative researchers aim to gather an in-depth understanding of human behavior and the reasons that govern such behavior. The qualitative method investigates the why and how of decision making, not just what, where, when. Hence, smaller but focused samples are more often needed than large samples. The process of this research are includes the qualitative research with study of articles and documents.
Finding and Results
The results show that apart from the a few some obvious corruptions in football of Iran there are no others records for the corruption (Table 1). Because of the high incidence of corruption in Italian football, the table of corruption in football of Italy have presented separately. As show that in Table 2, the most popular corruption in the Italy's top professional football leagues occur at 2006. As show that in Table 3, Europe's football is as advanced as it is more common corruption. As can be seen in Table 4, there is corruption in the football world. Asian countries have the highest share.
Discussion and Conclusion
Corruption is a major problem for the sporting authorities to deal with the emerging discourse about corruption in football cannot be understood without drawing stronger connections to the media discourse on broader societal corruption.
Corruption has a major affect on those that keep professional sport functioning spectators, television and sponsors. For example in the 2006 Italian football scandal involved Italy's top professional football leagues, Serie A and Serie B. The scandal was uncovered in May 2006 by Italian police, implicating league champions Juventus, and other major teams including AC Milan, Fiorentina, Lazio, and Reggina when a number of telephone interceptions showed a thick network of relations between team managers and referee organizations. Juventus were the champions of Serie A at the time. The teams have been accused of rigging games by selecting favorable referees.
Corruption puts spectators off attending events, watching them on television and sponsors from giving them the money they need for competitions.
In view of the many of football competitions that take place every day throughout the world, the number of proven cases of corruption in football can be put into perspective, even if the considerable percentage of unknown cases are taken into account.
The categories of corruption on football are concerned, two tendencies. Firstly, at least within the cases of competition corruption that have come to light, competition judges and other officials are becoming involved in corruption more frequently whilst, in contrast to previous eras, athletes and trainers are less often directly involved. Secondly a tendency towards an increased number of cases of management corruption in football can also be observed.
In order to finance bribes of a sufficient amount for decision makers, the bribers must expect sufficiently high economic rents from the victory they have purchased. Only those types of sport are affected by corruption that is able to generate considerable sources of income of football. In order for economic rents of this kind to be established in the long term (and for corruption not to be a merely temporary phenomenon), limitations to competition need to be in place.
As far as the role of discretionary margins for corruption is concerned, simple, transparent and easily understandable decisions are at a low risk of corruption. On the other hand, decisions in which abuses of freedom of decision can quickly be discovered are also hardly at risk from corruption. Thus the creation of a high degree of transparency is of considerable importance in combating corruption. This can be achieved, for example, by the detailed documentation of decision-making processes, the monitoring of executive and administrative bodies by a number of staff members or by the creation of internal auditing departments to monitor staff.
Increasing controls and introducing tougher penalties. In addition to the exclusion from sporting activities already practiced by most sports associations, the effectiveness of higher fines ought to be tested.
The Officials of football federation in Iran must be trying to various initiatives to help remedy the problems associated with corruption. Football Players must be educated and aware of the threats to the integrity of football, along with education and awareness of the rules and regulations against betting, gambling, and performance enhancing drugs. A crucial aspect of addressing the threats to integrity in football is an effective education and awareness program for all players, players' support staff, officials and other relevant persons. Players and all those connected with football must understand the nature of the threats and the penalties if caught, as well as the need to act responsibly in enhancing the integrity of football. A strong message must be delivered that each player, official, and coach has a role to play in maintaining and enhancing the integrity of football.
Football players and officials alike are made fully aware of their obligations under the anti-corruption rules, including their duty to report improper approaches, however trivial they may seem. This is vital not only to ensure that incidents of attempted match fixing are properly investigated and dealt with by the relevant authorities, but also to ensure that the public perception of the "integrity of football" is maintained so far as possible. With regard to the process of effective education, sporting governing bodies, anti-corruption units and players" and officials" associations all have a key role to play. Put simply, where there is a comprehensive knowledge and understanding of the relevant rules, there can be little or no excuse for failing to comply.
In order to be able to provide a meaningful analysis of anticorruption measures in football, reference should first of all be made to the economic causes. These indicate that corruption arises when for both the potential briber and the potential recipient of the bribes this is seen, within a rational calculation, to be a dominant, net utility increasing strategy as set against other, legitimate behavioral alternatives.
For more Journals in Juniper Publishers please click on https://juniperpublishers.com/index.php
For more articles in Journal of Physical Fitness, Medicine & Treatment in Sports please click on https://juniperpublishers.com/jpfmts/index.php
#juniper publishers#Juniper Publishers Review#Juniper Publishers in USA#JuniperPublishers Publons#JuniperPublishers
0 notes
Text
Juniper Publishers- Open Access Journal of Otolaryngology
Research Article
The Prevalence of Otolaryngologist’s Practice Location In Relation To: Birth State, Medical Residency, and Medical School
Shane Griffith1* and Anton Power2
1Department of Otolaryngology and Facial Plastic Surgery, Lake Erie College of Osteopathic Medicine, USA
2Department of Otolaryngology and Facial Plastic Surgery, University of New England College of Osteopathic Medicine, USA
Submission: March 11, 2016; Published: March 18, 2016
*Corresponding author: Shane Griffith, Department of Otolaryngology and Facial Plastic Surgery, Lake Erie College of Osteopathic Medicine, ENT Specialists of Northwestern Pennsylvania
Objective: This workforce study examines the geographic distribution of practicing otolaryngologists in relation to the residency, medical school and state of birth from which these physicians came.
Study Design: Descriptive cross sectional study.
Subjects and Methods: Using the American Medical Association (AMA) master physician file, current otolaryngologist practice locations were analyzed for the distance from previous medical training sites and birth state.
Results: Of the 6648 otolaryngologists for which practice location, training locations, and birth state could be obtained, approximately 25.7% and 30.7% practice within 100 miles of their graduating medical school and residency, respectively. 31.6% of otolaryngologists currently practice within the same state as birth. These rates were variable by state with New Jersey, New York, and California residents having higher than national average rates of regional retention.
Conclusion: Approximately 1/3 of otolaryngologists practice within regions of previous medical training. While future studies are needed to determine causal relationships, by acknowledging these current trends we can adapt future graduate training decisions to support the geographic diversification of otolaryngologists.
Introduction
Each year the approximately 300 graduating otolaryngology residents and fellows must decide where to practice. This decision has vast implications from an individual, family, community, business, and population perspective. As the demand for physician’s increases, understanding which factors contribute to a physician’s location of practice is important. While pragmatic factors such as malpractice cost, tort reform, and incentive pay play a role [1], so do other factors related to personal background and even location of training during medical school [2].Particularly, graduating otolaryngology residents rank geographic location as the second most important factor (after time available for family) in the choice of practice setting [3].
The vast majority of physician specialties in demand are primary care practitioners (general internists, family physicians, and psychiatrists). Likewise, the literature regarding training location’s impact on practice location is dominated by primary care specialties. There is, however, still a great demand for employment within the Otolaryngology specialty. According to recruiting agencies like Merritt Hawkins, Otolaryngology is ranked 17 in the top 20 most sought after specialties by employers in 2011 – 2012 [4].
A recent study by Johnson et al. quantified the distribution of residents in the Otolaryngology specialty relative to where they went to medical schools. They found that a strong proportion of current residents in the South and Midwestern regions attended residency programs affiliated with their medical schools.10 However; the factor that ultimately affects the physician shortage in specific areas of the United States is where these physicians will ultimately establish their practice following the completion of their education. Furthermore, little research has been done to identify motivations for the current group Otolaryngologists to establish a practice in a specific region. We aimed to assess the geographic distribution of current otolaryngology physician practices in relation to the residency, medical school, and state of birth from which these physicians came.
Methods
Using the American Medical Association (AMA) Physician Master file a data set of active otolaryngologists was collected. Since the goal of the study was to provide a current snapshot in time, only active practicing physicians were included. Residents, current fellows, teaching (non clinical) physicians, and research (non clinical) physicians were excluded so that only confirmed office based or hospital based otolaryngologists in the United States were included. The otolaryngology sub specialties that met these criteria were also included within the data set. Furthermore, since the AMA physician master file is based on reporting, only those with confirmed practice location addresses (rather than home addresses) were included within the data set.
Fagan et al. [5] found that 56% of Family Physicians practice within 100 miles of their residency program. According to the National Bureau of Economic Research calculation of hospital competition, community hospitals can expect patients living within 35 miles to seek care at their facility and tertiary care/teaching centers can expect patients living within 100 miles [6]. This may suggest 100 miles as a reasonable cut off for competitiveness between otolaryngology centers [6].
Using the same radius as a model, we too chose to elucidate whether otolaryngology physicians practiced within 100 miles of their residency or medical school program. The public address listed for each medical school and residency was compared to the city center of each physician practice. Google Maps was utilized to calculate road travel distances and the data was recorded for each physician in a binary fashion. The data was also used to determine the percentage of otolaryngologists that are currently practicing within the same state of birth.
Results
Excluding residents, teaching physicians, and research physicians yielded a data set of 9,045 active otolaryngologists but only 6,648 had a confirmed active practice location (rather than home location) on file. This sample was representative of practices in all 50 states in addition to the District of Columbia and Guam. The data set was consistent with prior workforce analyses and contained 13.7% females and 86.3% males [7].
The 6,648 otolaryngologists included graduates from 348 different medical schools; of these, 213 were foreign medical schools, 130 United States allopathic institutions, and 15 osteopathic institutions. After excluding international graduates a sample size of 5,901 otolaryngologists remained. Results revealed that 1,519 or 25.7% currently practice within 100 miles of their medical school (Table 1). Figure 1 demonstrates the state variability and one can see that New York, New Jersey, Delaware, and Louisiana have higher than national average rates of otolaryngologists currently practicing within 100 miles of their medical school.
The sample was representative of Otolaryngology ACGME, AOA, and military accredited residencies. Of the 6,648 otolaryngologists only 5,922 had medical residency information provided in such a manner that the location could be verified. Of these 5,922 otolaryngologists, 1,821 or 30.7% currently practice within 100 miles of their postgraduate training (Table 1). Figure 2 represents the percentage of otolaryngologists that currently practice within 100 miles of their residency demarcated by state. New York, New Jersey, and Illinois have the highest rates of otolaryngologists living within 100 miles of their postgraduate residency training.
The sample was representative of otolaryngologists born in all 50 states, Guam, the District of Columbia, Puerto Rico and the Virgin Islands. Out of 6,648 Otolaryngologists, state of birth was provided for 5,192 of them. Of these 5,192 otolaryngologists, 1,641 or 31.6% currently practice within their state of birth (Table 1). Louisiana and New York are the two states with the highest retention of physicians based on state of birth (Figure 3).
Discussion
It is not uncommon to hear anecdotal claims that physicians practice in locations surrounding their training institutions. Additionally, previous studies have found that 51% of all physicians work within the state of their residency [5]. Specifically, 56% of Family Physicians practice within 100 miles of their residency program [5]. While otolaryngologists may not currently be in demand to the extent that primary care specialties are, understanding trends and factors that influence practice locations are important to the future of the specialty.
Geographic location was the second most cited factor for choosing a practice location among graduating otolaryngology residents. Moreover, geographic location appears to become more important as residents transition from intern to graduates as their willingness to move family decreases [3]. Given the importance of geographic location to graduating otolaryngology residents it was our hypothesis that the rate of otolaryngologists practicing in areas surrounding their training would comparable to that of family practice physicians.
The national rate of otolaryngologists practicing within 100 miles of their medical school (25.7%) and residency (30.7%) is lower than that of the general physician population. Training location is certainly not the only influence on practice location decisions. Low award cap areas for malpractice appear to attract surgeons and malpractice premiums have a statistically significant impact on geographic location of practice for all surgeons [1]. This may contribute to otolaryngology geographic retention rates being lower than that of the general physician population.
According to the U.S Census Bureau 58.8% of Americans are currently livings in their state of birth [8]. For the otolaryngology population 31.6% currently practice in the same state of birth. The rate of otolaryngologists practicing within their same state of birth is reduced from the general population. A possible explanation for these findings could be the competitiveness and decreased number of residency spots for otolaryngology in comparison to other specialties. Moreover, the amount of otolaryngologists needed per community is lower than that of family practice and markets may become more easily saturated with otolaryngologists. This may require otolaryngologists to travel to places with higher demand.
The outcome data of this study is variable by state. Naturally, states like Idaho, Montana, Alaska, and Wyoming without otolaryngology residencies or medical schools have non-existent training trends of geographic retention. As one may expect, states with numerous medical schools and residencies like New York ad California had higher than national average rates of 100 mile retention. This demonstrates that although current residents are more likely to attend residency programs affiliated with their medical school in such areas as the South and Midwest [9], they will overwhelmingly flock to regions with higher population density such as California and New York. By using 100 miles as an inclusive criterion, we were also able to demonstrate the interesting case of New Jersey; approximately 60% of its otolaryngology population is currently practicing within 100 miles of their graduating residency and medical school, despite much less state training institutions. This is likely a result of the surrounding New York City metropolitan area.
While the sample used was nearly representative of all states of residence, otolaryngology residencies, US medical schools, and a male to female ratio consistent with other published demographic data [10] there were limitations to this descriptive cross sectional study. Although strict inclusion criteria were followed, since the AMA physician master file is a self-report measure, data may not demonstrate “desired” practice locations for all physicians. While those pursuing fellowship and residency were excluded, some may be pursuing other academic endeavors post-residency. This information was not included in the master file. Thus, there may be a bias towards physicians appearing to move to more centralized medical centers.
While other factors likely contribute, recognizing that approximately 25-31% of otolaryngologists practice within 100 miles of their medical training may help residency graduates or migrating otolaryngologists further decide on competitive practice locations. The strategic distribution of otolaryngologists may become more important as it has been previously proposed that there is a moderate oversupply of 3.16 otolaryngologists to 100,000 population [10].
Conclusion
This study demonstrates that nearly 1 out of 3 otolaryngologists practice within the same state of birth or within 100 miles of their training institution. If current trends continue, an otolaryngology residency program may expect approximately 1 out of 3 of their graduates to practice within 100 miles at some time. These rates are variable by state and region. Moreover, geographic population distribution and other factors likely contribute and further studies are needed to elucidate the specific causal relationships of these factors.
Given the rising concern over physician shortages today and in the near future, this study demonstrates that some residency programs and medical schools are more successful than others at retaining their physician graduates. Using this data as a guide for future study into incentives programs and public policy will allow regions, states, and other localities to better understand what motivates physicians to practice in certain areas. Further study is needed to assess whether demographics such as race, gender, age, and other factors affect location of practice.
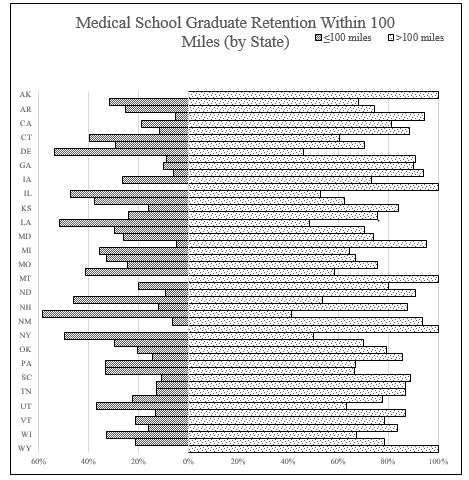
Figure 1: Percentage of Otolaryngologists by state who are currently practicing within 100 miles of their graduating medical school.
For more information click on regarding Global Journal of Otolaryngology
https://juniperpublishers.com/gjo/GJO.MS.ID.555560.php
For more open access journals click on Juniper Publishers
https://juniperpublishers.com/
#juniper publishers#JuniperPublishers#Juniper Publishers Review#Juniper Publishers Publons#Juniper Publishers in usa
0 notes
Text
Juniper Publishers (0000-0003-1007-1243) - ORCID | Connecting

Juniper publishers have been established with the aim of spreading quality scientific information to the research community throughout the universe. We, as Open Access publishers, strive to offer the best in class online science publications. Open Access process eliminates the barriers associated with the older publication models, thus matching up with the rapidity of the twenty-first century. Our main areas of interest lie in the fields of science, engineering and other related areas. Juniper Publishers is a platform for professors and researchers who aspire to give out quality information based on their research and expertise, in an attempt to aid scholars/researchers in their field of interest with the latest information.
To Read More about Juniper Publishers (0000-0003-1007-1243) - ORCID | Connecting
Click on: https://orcid.org/0000-0003-1007-1243
To Know More about Juniper Publishers click on: https://juniperpublishers.com/
For More Open Access Journals in Juniper Publishers Click on: https://juniperpublishers.com/journals.php
#Open Access Publishers#Juniper publishers e-books#Juniper Audio Articles#Juniperpublishers#Juniper publishers e-pub
0 notes
Text
Why Adolescents with E - Wings Sarcoma Being Reluctant to Amputation? A Study under the Phenomenological View
This study aimed to understand the implications and feelings associated during preoperative stage, with the process of amputation. Several perspectives through review of literature has allowed the knowledge to understand the phenomenon. In this study, the testimonies of 12 adolescents of male and female at preoperative stage of amputation, suffering with E-wings Sarcoma inclusive of upper and lower limb were analyzed. The interview of the adolescents, shown various perspectives through statements, by these sharing moments understood the concept from the perception of those who is experiencing it.
To read more...Full Text in Annals of Reviews & Research in JuniperPublishers
1 note
·
View note
Text
Juniper publishers (Juniper_Publish) on Pinterest

Juniper publishers have been established with the aim of spreading quality scientific information to the research community throughout the universe. We, as Open Access publishers, strive to offer the best in class online science publications. Open Access process eliminates the barriers associated with the older publication models, thus matching up with the rapidity of the twenty-first century. Our main areas of interest lie in the fields of science, engineering and other related areas. Juniper Publishers is a platform for professors and researchers who aspire to give out quality information based on their research and expertise, in an attempt to aid scholars/researchers in their field of interest with the latest information.
To Read More about Juniper publishers (Juniper_Publish) on Pinterest
Click on https://in.pinterest.com/Juniper_Publish/
To Know More about Juniper Publishers click on: https://juniperpublishers.com/
For More Open Access Journals in Juniper Publishers Click on: https://juniperpublishers.com/journals.php
0 notes
Text
Juniper Publishers- Open Access Journal of Case Studies
Treatment if Pericarditis in an HIV-Infected Patient in a Regional Hospital in Thies (Senegal)
Authored by Bammo M
Summary
Pericarditis is a common and serious cardiovascular disease during HIV infection. In sub-Saharan Africa, tuberculosis is the most common etiology; however, other infectious causes of pericarditis pose a problem of diagnosis and treatment. We report the case of a patient living with HIV 1 for 3 years without ARV treatment who developed a purulent pericarditis treated at regional hospital of Thiès.
We highlight the diagnostic difficulties of this condition in the decentralized zone and the means of treatment of this pathology, fatal if it is not treated early.
Keywords: Purulent pericarditis; HIV infection; Diagnostic difficulties
Introduction
HIV seroprevalence in the Thiès region is 0.3% in 2017. The treatment of PLWAs has been decentralized to the regions and health districts since 2013 with free antiretroviral treatment [1].
a) The immunodepression induced by this virus is at the origin of several affections and/or opportunistic infections responsible for morbidity and mortality, among which cardiac involvement with histological lesions in 60% of cases and clinical expression in 30% of cases.
b) The involvement of the pericardium occupies an important part among these cardiac attacks.
c) The etiological factors of pericarditis vary with the course and magnitude of HIV-induced immune deficiency.
Various causes of pericarditis have been reported in the literature but pericarditis of unidentified (idiopathic) cause can reach 45% of cases [2]. We report the case of an HIV-infected patient who developed a purulent greenish pericarditis of unknown etiology. The objective of this case presentation is to highlight the diagnostic difficulties of this condition in a decentralized environment.
Observation
Mr. Y N is a 26-year-old man, who has sex with a well-known man (MSM), single without children, from the city of Thiès. He presented himself in consultation at the hospital of Thiès October 10, 2016 for a quintessential cough with a notion of hemoptysis of low abundance not objectified. A retrosternal thoracic pain rhythmized by the breathing and a dyspnea with orthopnea type evolving since 15days and exacerbated for a few hours. He also complains of a progressive weight loss of 24kilos in 3years.
For only antecedent, this patient was diagnosed infected with HIV 1, asymptomatic, after a voluntary screening 3 years ago without treatment because He cannot be found. At admission, the patient had a fever at 38.3°C, an impairment of general condition, he was sleepy and cachectic weight 42 kg with BMI: 12.8Kg/m2.
Clinical examination revealed NYA grade 4 dyspnea, tachycardia at 108beats/min and arterial hypotension (BP 100/50mmHg). The heart sounds were muffled. Pericardial friction was not perceptible. There was no paradoxical pulse. Crackling rattles were heard on auscultation at the two pulmonary bases
The rest of the examination found diffuse prurigo and oropharyngeal candidiasis.
The electrocardiogram revealed, in addition to sinus tachycardia, a peripheral low voltage with probable right ventricular hypertrophy, while the chest X-ray showed cardiomegaly and bilateral low-grade pleural effusions.
Complementing the exploration, transthoracic echocardiography confirmed the presence of a pericardial effusion of great abundance without fibrin network. The exploratory puncture aims to produce a purulent yellow-greenish liquid. A percutaneous drainage under xiphoidal under local anesthesia was performed, allowing the evacuation of two liters of greenish-yellow pus free with good tolerance without complications.
The biology revealed an inflammatory syndrome with a CRP of 61.76mg/l and an accelerated sedimentation rate at the first and second hours. There was; microcytic hypochromic anemia at 5.5g/dl, 78.7% neutrophil polynucleosis. Cytobacteriological examination of the pericardial fluid identified 65% of lymphocytes, gram-negative bacilli, but the culture on solid medium was negative. GeneXpert MTB/RIF performed on sputum and pericardial fluid was negative.
As treatment, the patient received an intravenous administration of Ceftriaxone at a rate of 100mg/kg/day; Metronidazole 30mg/kg/day. It was temporarily (3 days) associated with gentamicin (3mg/kg/day) and Prednisone 20mg/day for 5 days. He had also received Furosemide Injection: 40mg/day, Captopril 25mg daily; Enoxaparin 0.4 per day; DLlysine acetylsalicylate 100mg/day. The evolution was marked on day 6 of treatment by a disappearance of cough and dyspnea as well as apyrexia (37°4).
Cardiac echocardiography on day 14 showed a poor pericardial effusion plate insufficient for surgical drainage. The patient was put on antiretroviral therapy and on cotrimoxazole prophylaxis.
The patient was seen six months after discharge in cardiology for signs of late complication; it was stable, with a weight gain of 12kg. Moreover, the M6 ultrasonography showed a quasi-total regression of the pericardial effusion with a slight thickening of the pericardium.
Discussion
This case of purulent pericarditis is singular by its clinical presentation in a PvVIH lost sight of 3 years
Many HIV-infected patients have cardiac involvement [3]. The prevalence of pericardial lesions is regularly reported in all African clinical series: nearly 28% in the Democratic Republic of Congo (DRC) and 35.3% in Congo Brazzaville [2]. In Senegal, already in 1984, D. SOW et al reported a prevalence of purulent pericarditis of 11% in pediatric hospitalized children [4]. I. Thiam found 2.5% of cases of tuberculosis pericarditis with microscopic discovery [5]. Ngouala G. in a study conducted in a decentralized area (Louga) found 3.7% of pediatric cases of tuberculous pericarditis [6].
Pericarditis remains however a serious and rare entity which is almost always fatal because of a late management. The presence of clinical signs and paraclinical examinations allow rapid diagnosis in order to start early treatment [7]. This patient had advanced dyspnea, febrile chest pain on a febrile deterioration of the general condition that had been evolving for 15 days, and effusions indicating delayed diagnosis [3].
The dominant functional symptomatology in the literature is dyspnea of effort and deterioration of the general state. This finding has been made in Africa by several authors [3,8]. Fever is also a reason for frequent consultation. For Cohen, the presence of fever and dyspnea is suggestive of purulent pericarditis or myocarditis [8].
The deafening of heart sounds and tachycardia were the stethoacoustic signs present in our patient and most found in the Niakara and Pio studies, which reported respectively 43.7% and 47.5% of cases [4,8].
The low rate of pericardial friction reported in the literature may be related to the abundance of pericardial effusion [8,9]. He was not present with our patient. Acute pericarditis can be caused by a wide variety of etiologies, which can be infectious or non-infectious [10].
Possible causes include connective tissue disorders, malignancies, radiation, heart lesions, uremia, and infections (including viral, bacterial, and fungal etiologies) [10,11]. In the majority of cases (45 to 80%), infectious pericarditis is of viral origin [11,12].
Bacterial pericarditis is a rare cause of acute pericarditis in the era of modern antibiotics with an incidence of less than 1% [13,14]. The most common living microorganisms involved are Streptococcus sp, Staphylococcus sp, Haemophilus sp and Mycobacterium tuberculosis [15,16].
Pericarditis in a seropositive person, living in Africa in addition, should first look for a tuberculous etiology [3,5,6]. It occurs most often in the early stage of infection, but can also occur in the AIDS stage [3].
No primary infectious focus was found in our patient; the etiological investigation was difficult in our working conditions in the decentralized zone because of the absence of a performing microbiological laboratory, however the favorable evolution under probabilistic antibiotherapy with broad spectrum allowed us to retain the hypothesis of a cause non-specific bacterial.
Predisposing conditions for bacterial pericarditis are immunosuppression, malignant tumors, pre-existing pericardial effusion, alcoholism, uremia, thoracic trauma, cardiac and thoracic surgery, and the insertion or use of catheters for drain the pericardial fluid [15]. This case of pericarditis occurred on HIV-related immunosuppression. The Niakara study in Ouagadougou had a seroprevalence of HIV of 47% out of 79 cases followed for 75 months from 1993 to 1999, reinforcing the work that established a correlation between HIV infection and pericarditis especially in Black Africa [3]. During HIV infection, the occurrence of pericarditis with pericardial effusion is common.
The mechanisms are multiple; pericarditis may be related to viral infection by HIV or other viruses, bacterial or fungal superinfection in an immunocompromised patient or the presence of Kaposi’s lymphoma or sarcoma [3,10,15]. Laboratory assessment may reveal systemic inflammation with leukocytosis and elevated CRP and SV [15]. The chest X-ray usually shows cardiomegaly with an abnormal heart shape. Pulmonary infiltrates, pleural effusion and mediastinal enlargement may also be present [15,16].
The ECG often makes it possible to evoke the diagnosis, especially in its acute form by the Holtzman stages. The signs that we observed at the ECG have no specificity as demonstrated by a piece of literature [9].
In our case, none of the paraclinical examinations were directed to the diagnosis of pericarditis. Echocardiography remains the first-line imaging examination for the diagnosis of pericardial effusion by specifying abundance and location. The abundance of the effusions facilitates the ultrasonography diagnosis of these pericarditis [3,9], as was the case in our patient; he had significant pericardial effusion without cardiac tamponade.
The treatment is based on probabilistic antibiotherapy in the absence of bacteriological data of pericardial fluid and / or blood culture. Surgical drainage is often necessary [8,9]; it allowed our patient to evacuate two liters of greenish yellow pus without complications. Even under treatment, the rate of complications and deaths remains high, with a lethality rate close to 40% secondary to tamponade, pericardial constriction or sepsis [15- 17].
Conclusion
Although rare, purulent pericarditis usually responds to probabilistic treatment provided that a tuberculosis etiology is eliminated even in a health facility with limited means. Early recognition and rapid intervention are essential to the success of the treatment whose etiological research is confronted with daily technical difficulties in a decentralized environment.
For more articles in Open Access Journal of Case Studies please click on: https://juniperpublishers.com/jojcs/index.php
#JuniperPublishers#Juniper Publishers Contact#Gastrointestinal Surgery#Infectious Diseases#Obstetrics and Gynaecology#Ophthalmology
1 note
·
View note
Text
Synthesis and Characterization of Low-Cost Activated Carbons for Pollutants Removal from Automotive Emissions-JuniperPublishers
Journal of Chemistry-JuniperPublishers
Abstract
Air purification is one of the most widely known environmental applications of activated carbons. In order to guarantee the successful removal of contaminants and pollutants on activated carbons, the development of new adsorbents has been increasing in the last few years. This paper presents a systematic study for cleaning vehicles emissions of CO, SO2, NO2 and H2S using the process of physical adsorption on novel adsorbents obtained from tropical biomasses. Use of this simple method is a valuable alternative to meet emission standards in Developing Countries. It is known that the agricultural wastes studied here are a feasible alternative for granular activated carbons preparation for pollutants removal during engines operation, approaching its efficiency to the commercial Catalytic Converters.
Keywords: Combustion gases purification; Activated carbons; Adsorption and adsorbents; Pollutants removal
Go to
Introduction
“Quality Can Be Planned.”-Joseph Juran
Wastes cannot be introduced to the environment in unlimited amounts, especially in case of air pollutants. Different measures have been taken to limit the pollution emission. These are e.g.: the elimination of technological processes generating a lot of waste, introduction of new technologies which minimize the contamination, etc. If it is not possible to reduce the emissions, the waste gas must be purified [1,2]. Nowadays, the economic conditions of Developing Countries don’t allow that all individuals own a new automotive. It is necessary to develop alternatives to reduce the negative environmental impact associated with obsolete engines operation. The best way to address it is by reducing certain exhaust gas components during fuel combustion. The answer therefore is to look at vehicles as an integral whole to identify which solutions would be more feasible. Taking this holistic approach to vehicle improvement as a basis, three main exhaust emission control strategies can be defined:
a.Reduction of fuel consumption;
b.Exhaust gas treatment, and
c.Performance monitoring.
From these three alternatives the second one is currently the more effective for air quality improvement. The main gas treatment currently used is the Catalytic Converter, typically comprises of an expensive porous ceramic substrate with large surface area [3]. Unfortunately some users in Central America and the Caribbe an Countries tend to remove the Catalytic Converter from the vehicles to get better power loads. Over the last decade, the study of combustion gas treatment has been focused on more sophisticated Catalytic Converters. Consequently, the study of other alternatives for exhaust gas purification is important. There are a few methods to purify harmful combustion gases such as physical adsorption [4,5], chemical absorption [6], catalytic methods, etc. [7,8]. It is necessary then to select a suitable method to purify harmful gas for Developing Countries. Besides, standards for vehicles become more mandatory day to day. The more feasible alternative would be the development of customized activated carbons filters for the betterment of the environment. This can be accomplished by reducing the emissions that contribute to smog and acid rains [9].
Activated carbons can be obtained from different precursors, with benefits to the environment [10-12]. Due to its chemical composition, forest biomasses are valuable sources in the synthesis of adsorbents materials. Several examples of activated carbons preparation can be found in the open literature [13,14]. They have been used among others in the purification of pollutants gases such as carbon dioxide, sulfur dioxide, hydrogen sulfide, nitrogen oxides and mercury [15-17]. Taking into account this background, the main objectives of this work can be summarized as follows:
I.Study the feasibility of some agricultural wastes as raw material for activated carbons production with high specific surface area, high mechanical resistance and wide availability.
II. Definition of the best experimental conditions for “chemical activation” with H3PO4 such as “physical activation” with steam water for each precursor.
III. Study of the elimination of pollutant gases in vehicles engines with filters of the adsorbents produced.
IV. Proposal of a methodology for filters evaluation in the removal of undesirable pollutants (CO, SO2, NO2 and H2S) during engines operation.
The practical aspects addressed in this research cover the broad spectrum of applications for air cleaning. Better engines performances can be obtained with an adsorption technique of activated carbons, through an extremely economic method.
Go to
Materials and Methods
The raw materials selected for the study are presented in Tables 1-3.
Preparation of Activated Carbons
The starting raw materials were cut up in small pieces and next subjected to pyrolysis. This process was carried out in a tubular reactor in nitrogen atmosphere. The samples were heated (10 °C/ min) from room temperature to the final pyrolysis temperature of 500. In the final pyrolysis temperature, samples were kept for 60 minutes and then cooled down. The solid products of pyrolysis were next subjected to physical activation [18]. In the case of chemical activation the raw materials were the original precursors which were overnight impregnated into H3PO4 and later submitted to pyrolysis into a stainless steel reactor of 30cm of length per 3cm of diameter. Once the reactor reached the desired temperature the samples were kept at the final temperature according to the experimental conditions of the specific experiment. The activated products then cooled down and washed with enough water till get a neutral pH. Finally, the products were dry at 120°C and then stored [19]. Two different processes were used for the synthesis of the activated carbons from the chars previously obtained by pyrolysis. [18,19]. The experimental conditions used were:
Factorial experimental designs 32 were executed to evaluate the simultaneous influence of the activation conditions on the final product features [14,20]. Following the details for both synthesis processes:
Key properties of the activated carbons prepared were analyzed:
a. Raw material availability;
b. High specific surface area;
c. High mechanical resistance;
d. High adsorption speed.
Characterization of the Raw Materials and Synthetized Activated Carbons
Elemental Analysis: The amount of elements (carbon, hydrogen, nitrogen and oxygen) in the raw materials was determined by an Elemental Analyzer by flash combustion. The samples were firstly dried in an oven at 110°C before the measurement was carried out. The materials was burned at a temperature of 1000°C in flowing oxygen for C, H and N analysis in the analyzer. The CO2, H2O and NOx combustion gases were passed through a reduction tube with helium as the carrier gas to convert the NOx nitrogen oxides into N2 and bind the free oxygen. The CO2 and H2O were measured by selective IR detector. After corresponding absorption of these gases, the content of the remaining nitrogen was determined by thermal conductivity detection. The oxygen was calculated by the difference of carbon, hydrogen and nitrogen.
Apparent Density Measurement: Apparent Density is a measure of the mass per unit volume of a material. It is also called Bulk Density and provides a measure of the “fluffiness” of a material in its natural form. In this work the Standard ASTM D1895 was used. According to this standard the materials are poured into a cylinder of known volume (e.g. 100 mL pipettes) and later weight. Apparent density was calculated as the mass of material divided by the volume occupied into the cylinder [21].
Specific Surface Area Measurement: In order to examine the structure of the synthetized materials, the measurement of the specific surface area of the activated carbons was carried out by gas adsorption isotherms using a Sorptometer applying BET Model. All samples were degassed at 200°C prior to N2 adsorption measurements. Specific surface area was determined by a multipoint BET method using the adsorption data in the relative pressure range: 0.05-0.3 [22,23].
Mechanical Resistance Measurement: The mechanical resistance of the obtained activated carbons was measured through a simple method. A know mass of the granular material was impacted by six glass balls into a semispherical container of stainless steel. The percentage relation between the fragmented mass retained in a 0.5mm mesh and the initial mass is used to estimate the mechanical resistance [24].
Adsorption Speed Evaluation: The adsorption speed was determined by Arrhenius Equation:
where: dX/dt is speed of the adsorption process studied; α is the residual concentration of the adsorbed; and k'ads the apparent kinetic constant of the adsorption process that can be determined by:
Applying logarithm to (Equation 2) brings the possibility to change an exponential equation into a linear dependence, see below:
Plotting ln k'ads vs 1 the activation energy (EA) and the preexponential factor (k0) of the adsorption process studied can be calculated. In the Results discussion ads k'ads will be refers as K for practical reasons.
Designing Process of Activated Carbon Filters
Figure 1 illustrates the process of activated carbon units customized assembling. These filters are very useful to study pollutant gases elimination in automotive engines with the adsorbents produced [25]. The samples, in the form of granules of 2-5 mm in diameter, were packed into a steel column (length 300 mm and internal diameter 90 mm). The gas was passed through the bed of the adsorbent at 0.50 L/min. The concentration of CO, SO2, NO2 and H2S were monitored using a Gas Chromatograph Equipment with standard TCD detector. The concentrations were calculated by integration of the area above the curves.
Pollutants Monitoring at Laboratory Scale
There is no known method available in the open literature which is capable of simultaneously determining all components of combustion gas evaluated here [2]. So the method developed in this work in an innovative alternative for Developing Countries. In order to determine the suitability of the obtained adsorbents in the elimination of CO, SO2, NO2 and H2S, the pollutants removal rate was determined. Figure 2 show a schematic diagram of the customized laboratory system for pollutants monitoring. The system includes, among others:
a. 6 cylinder automotive engine;
b. Activated carbon filter;
c. Exhaust gas analyzer device (Gas Chromatograph);
d. Computer system for data acquisition and recording, etc.
Gas Monitoring System: A standard gas chromatography was used with the following specs:
i. Detector: TCD;
ii. Carrier: Helium;
iii. Column: Porapak Q and Molecular Sieve 5A;
iv. Oven Temperature: 100°C;
v. Sample volume: 1 ml;
vi. Carrier Flow: 25 ml/min;
vii. Detector Temperature: 120°C
Under the described chromatographic conditions, the four gases could be easily separated and quantified [25,26].
The methodology used starting with the preparation of the calibration gas sample by injecting known volumes of each of the four pure gases (CO, SO2, NO2 and H2S) and balance nitrogen into adequate Gas Sampling Bag through the bag’s rubber septum. One mL of the calibration gas mixture and the combustion gases were analyzed by a GC system. Randomly measures of combustion gases before and after the purification process were made on a similar manner in order to evaluate the removal rate of the undesirable pollutants.
Go to
Results and Discussion
Composition and Physical Properties of Raw Materials and Synthetized Products
Table 4 brings a summary of the chemical composition (elemental analysis), such as some physical properties of the 5 precursors studied. Elemental nitrogen, carbon and hydrogen were determined from the elemental analyzer by flash combustion while oxygen was determined by the difference of these three elements. Table 4 shows that the largest amount of element in the raw materials was carbon (except for Corncob which had smaller amount of carbon than oxygen), followed by oxygen, and the smallest amount was nitrogen. The lower content of carbon for Corncob can be attributed to a higher content of volatiles in the structure, translated into a high porosity for the raw material. All precursors do not contain sulfur in their structure, which is very favorable from the ecological and technological points of view.
dap: apparent density; dr: real density; P: porosity
The activation process increases carbon amount (~20- 40%) after modification. On the contrary, there was a reduction in the oxygen content (~20-30%) after physical and chemical modifications. There will be also a reduction of hydrogen amount. The amount of nitrogen was so small for all materials. In Table 4 it can be observed that the initial porosity of all material, except corncobs, have lower values, below 0.5, it makes these materials adequate for activated carbons preparation through chemical or physical activation. The best products synthetized by each process will be reported in Tables 5 & 6.
S: specific surface; K: apparent kinetic constant of the adsorption process; Y: yield; Mr: mechanical resistance; dap: apparent density.
S: specific surface; K: apparent kinetic constant of the adsorption process; Y: yield; Mr: mechanical resistance; dap: apparent density.
Activated carbon from Central American Mahogany was the more reactive material with a significant porosity development (S = 847 m2/g). Should be noted also that Activated carbon from Mamey Zapote was the best adsorbent (S=940m2/g) and also have the higher mechanical resistance, yield and apparent density, very important for filters durability, but it’s the less available material. Finally it’s necessary to remark that Common Corncobs, a widely available agricultural by-product in Central American Countries, showed the worst results for all adsorbents properties; it can be attributable to the higher porosity of the initial raw material (P = 0.79%).
Table 6 show that activated carbon from Central American Mahogany was again the more reactive material but registered now the higher yield and adsorbent area (S = 832 m2/g). Furthermore, Activated carbon from Mamey Zapote was the second better adsorbent (S = 805 m2/g) and again have the higher mechanical resistance and apparent density. One more time activated carbon from Common Corncobs was the worst adsorbent (S = 470 m2/g). This fact is a consequence of poorly porous structure development during the activation process. Further analysis of the data from Tables 5 & 6 indicates that irrespectively of the variant used, the process of activation leads to further changes in the structure of carbonaceous material. The activated carbons synthetized from different materials studied here differ significantly mainly in the specific surface area development. The adsorbents differ not only in the surface properties but also in their texture and morphology that depend first of all on the variant of activation and the pyrolysis conditions of the initial material. Figure 3 illustrates the differences in specific surface development with both methods and the same materials.
In Figure 3, it can clearly be observed that larger specific surface area developments were achieved with physical activation processes. Those products were the better adsorbents to remove the undesirable pollutants. It also confirms that the factorial experimental designs used are the most suitable to optimize the conditions for activated carbon preparation. Textural parameters significantly affect the adsorption properties of the samples studied. [5] This observation suggests that the functional groups of the surface also have considerable influence on the abilities for combustion gases removal. All adsorbents studied had a rapid decrease in CO, SO2, NO2 and H2S concentration after gases interacted with the corresponding filters. High intensity of these harmful gas reductions at ambient conditions can be the reason for much better adsorption on higher surface area products. This explains the lower efficiency of gases removal by chemically activated carbons. The chemical activation process has the additional disadvantage of the required product washing after preparation which inevitably aggregates additional costs.
Gas Monitoring System
The calibrating gas analysis through the regression equations obtained from triplicate analysis of the gas mixtures at identical concentrations, revealed excellent agreement with the known concentrations. The pollutants monitoring system and analytical method used were effective for the simultaneous analyses of the four toxic combustion gases. Figure 4 shows two examples of 2 chromatograms obtained during the analysis of combustion gases purified with activated carbons from Mamey Zapote physically activated. In this figure it can clearly be observed the significant difference before and after gases interaction with adsorbents that can remove large amount of these undesirable gases with the associated environmental benefits.
The analyses of combustion gases revealed moderate concentrations of H2S and CO but very high concentrations of SO2 and NO2. The most effective adsorbent to remove these gases were the physically activated ones. At the present state of knowledge we can only speculate about the reasons for such poor results obtained from the chemically activated samples. Most probably the reason is the presence of a large number of acidic groups on their surface, in contrast to the physically activated samples, that probably have more basic functional groups present on the surface of the samples. Other chemicals present in the combustion atmospheres did not appear to interfere with the analyses. The chromatographic peaks were well separated and defined and the gases were present in amounts that could be easily determined. An excellent precision with relative standard deviations significantly below 2% were achieved in all gas monitoring analysis. The speed, sensitivity and selectivity of the used method make it suitable for analyzing combustion gas mixture of the four gases studied. Table 7 shows the overall average values of pollutants removal with activated carbons (A.C.) during automotive engines combustion.
In Table 7 it can clearly be observed that SO2 and NO2 amounts monitored are remarkable higher than the average limit values for 24 h. The good news is that the activated carbons studied can efficiently remove about 80% of pollutants in exhaust gases from automotive engines with the added value that the harmful gases concentration goes below the limit values. Figure 5 show the correlation between pollutants removal rate and specific surface area of activated carbons during automotive engines operation. In Figure 5 it can be clearly be observed that higher activated carbons specific surface area translated into higher pollutants removal rates that could be estimated by the equation 4 with a correlation coefficient R2 = 0.995:
A proper choice of the parameters of chemical and physical activation such as temperature, activation time, activates agent, etc., permits getting universal adsorbents showing very good adsorption properties towards such pollutants as SO2, CO, NO2 and H2S, however more studies are needed.
Go to
Conclusion
Agricultural wastes studied here are a feasible alternative for the synthesis of activated carbons for pollutants removal during automotive engines operation. The main features that make these products feasible for the diminishing of automotive engines emission are their high adsorption capacity, approaching its efficiency to the commercial Catalytic Converters such as the cheaper costs and its renewability. Based on these results the granular activated carbons studied, produced in large amounts, are fully exploitable for combustion gases treatment. The complex composition of the flue gas with SO2, CO, NO2 and H2S can be successfully analyzed with good compound separation and repeatability. The method used in this investigation would be also be suitable for combustion toxicology researches and could possibly be easily modified to analyze these gases when they are liberated from biological sources [27].
Go to
Acknowledgement
The author wishes to acknowledge Maria Andrea Camerucci and Ana Lia Cavalieri from Mar del Plata University, Argentina, they provided a crucial help in the experiments of this work.
To know more about Journal of chemistry,
Click here:
https://juniperpublishers.com/omcij/index.php
To know more about juniper Publishers,
click here:
https://juniperpublishers.com/index.php
#Juniper Publishers Indexing Sites List#Juniper Publishers group#JuniperPublishers#Juniper Publisher Reviews#Juniper Publishers#organic chemistry#chemistry journal#Open access Journal of chemistry#inorganic chemistry#chemistry#open access journals
2 notes
·
View notes
Text
The Clinical Outcomes Regarding to Tumor-Infıltrating Lymphocytes in the Breast Cancer Patients Treated with Neoadjuvant Chemotherapy- Juniper Publishers

In breast cancer great endeavors are going on to find new markers in determining the prognosis. In addition to well-known prognostic factors such as tumour size, grade, nodal status, molecular subtype, proliferation index, gene-expression based recurrence score, recently there is increasing evidence that tumor-infiltrating lymphocytes (TILs) are of important role as an immune biomarker in breast carcinoma [1-3]. TILs might be a reflection of host immune response which plays an important role in cancer control and patient’s clinical outcome. TILs are mononuclear immune cells that infiltrate tumour tissue and mainly comprised of cytotoxic (CD8+) T cells as well as macrophages, helper (CD4+) T cells, B cells, and NK cells [4,5]. There are two types of TILs: Stromal TILs (sTILs) are defined as the percentage of tumour stromal field in which lymphocytes are located without direct connection to tumour cells. In contrast, intratumoural TILs reflect immune cells within the tumour cells. Stromal TILs are commonly detected in H&E stained sections by light microscopy, and consist the majority of TILs in breast cancer [1]. Its assessment is the most reproducible parameter by pathologists. Moreover, lymphocytes-predominant breast cancer (LPBC) is defined as those cancer with TILs occupies at least 50 % to 60 % of the stroma [4].
The clinical importance and amount of TILs appear to vary significantly among different subtypes of breast cancer [2,6]. TILs are more common in triple-negative breast cancer (TNBC) and HER2-overexpressing breast cancer, with LPBC frequency of 15-25 % in these groups. Contrary, luminal tumour is the least immune infiltrated breast cancer subtype [3,6,7]. Large series suggest that tumour with higher TILs levels are associated with improvement of prognosis by longer survival rates and with reduction of locoregional recurrences [8,9]. This positive prognostic effect is especially striking on TNBC and HER2 positive patient populations [6,10]. In addition to prognostic value of TILs, trials also indicate the predictive role of TILs in response to neoadjuvant chemotherapy [11,12]. The aim of this study was to determine the association between TILs level and other clinicopathological parameters and to explore the prognostic and predictive roles of TILs in our breast cancer patients treated with neoadjuvant therapy.
Materials and Methods
The study was conducted to determine the association of TILs value with the clinical outcomes at neoadjuvant settings. Breast cancer patients treated after neoadjuvant chemotherapy at Bakırköy Sadi Konuk Training and Research Hospital from July 2011 to January 2016 were included in this study. All were followed up in our hospital. Patient’s demographic information, characteristics, outcomes and follow-up were obtained from hospital records. The study protocol was approved by the ethics committee of our institute (No:2017/09-20). Neoadjuvant therapy were taxane and anthracycline-based protocol, adding transtuzumab in the HER2 positive subtypes. Surgical treatment was decided as to treatment response. Radiotherapy and endocrine therapy were given in accordance with institutinal guidelines. Inoperable patients following neoadjuvant therapy were excluded of this study. The patients were categorized according to molecular subtypes as triple negative (TN), HER2 positive and luminal type. All patients in each subtypes were distributed into two groups according to TILs, with 10 % of cut-off value. In order to determine TILs value all patients’ paraffin sections stained hematoxilyn and eosin (H&E) from core biopsies were retrospectively assessed by an experienced pathologist (S.A.), blinded of clinical information. Briefly, all mononuclear cells (including lymphocytes and plasma cells) in the stromal compartment within the borders of invasive tumour were evaluated and reported as a percentage value. pCR was defined as ypT0/Tis ypN0.
We analysed associations of TILs with other clinicopathological factors such as menopausal status, tumour molecular type, ypTNM classification, histology, grade, lymphovascular and perineural invasion. In order to evaluate the predictive role of TILs, we investigated pathological responses to neoadjuvant therapy in high and low TILs groups of each subpopulation. To determine the prognostic role of TILs we recorded the patients’ locoregional recurrence and systemic metastasis in all groups and detected overall survival and disease free survivals. Statistical analysis was carried out using NCSS 11 package program. For categorical variables the frequency and percentage values were calculated and for continuous variables, average and standard derivation values were calculated. Standard distribution sort of variables was made with Kolmogorov-Smirnov test. Student t test was used in the comparison of two groups and single direction variance analysis was used in the comparison of more than two groups for variables exhibiting standard distribution. Disease-free survival (DFS) and overall survival (OS) were obtained using Kaplan-Meier survival analysis. The relations between categorical variables were examined with Chi square test, Fisher exact probability test and Fisher-Freeman-Halton test. P<0,05 was accepted as statistically significant.
Results
The study consisted of 89 breast cancer patients who underwent neoadjuvant chemotherapy. The mean follow-up duration of all patients was 33,8 (15-84) months. According to molecular subtypes, 39 patients had luminal tumour, and 25 patients each triple negative and HER2 positive.
TILs values in all groups and its relation with other clinicopathological factors
The mean TILs values were 10.8%, 15.4%, 6% in TN, HER2 positive and luminal groups, respectively. Among the patients of high TILs levels, HER 2 positive group was the most frequent molecular subtype (50 %), followed by triple negatives (32%) (Table 1). Sixty percent of patients with TILs less than 10 % had luminal tumour. There was statistically significant relationship between TILs value and both molecular type of tumour (p=0.0001) and presence of lymphovascular invasion (p=0.048). No association was detected between TILs and other variables such as menopausal status, ypTNM classification, histology, grade, and perineural invasion (Table 2).
TILs and prognosis
No association was seen in any subtypes between TILs levels and presence of either locoregional recurrence or systemic metastasis (Table 3). Neither OS nor DFS were significantly different between high and low TILs groups in both TN and HER2 positive groups. Because there was no death in luminal group, we could not detected survival analyses in this subtype.
Predictive role of TILs
In the neoadjuvant setting, no interaction was found between TILs level and complete pathological response according to each subtypes (Table 4). But, there was non-significantly better pathological response rates in high TILs group of HER2 (+) population.
Discussion
The constant interaction between tumour and host immunity influences patient’s outcome. Innate and adaptive immune response in the tumour milieu require functional cytotoxic T-cells in order to achieve efficent tumour elimination [1]. The impact of TILs on the prognosis and treatment prediction suggests its importance on the reflection of individual immunity [13]. Various studies of TN and HER2 (+) breast cancer have pointed consistent results that the increased TILs value the patients have, the better OS and DFS in the adjuvant setting [6,14]. Moreover, the highest TILs also show the highest expression of T-cell checkpoint receptors which found on T cells [1]. Antitumour immunity is enhanced by monoclonal antibodies against checkpoint inhibitors. In addition to standard therapeutic options, immunotherapy in breast cancer is a new and promising implication especially in selected patient population. Therefore, TILs evaluation may be accepted as a biomarker for immunotherapeutics in patients with breast cancer at near future.
In the light of these rapidly evolving field, in 2014 international TILs working group has recommended TILs evaluation as a immune parameter along with standard histopathological practise to facilitate its use in research setting and clinical trials [4]. They reported TILs measurement as a percentage of stromal TILs on a continuous scale by visual assessment of H&E-stained sections of primary tumour specimens similar to any other quantitative histological biomarker. Several studies have evaluated lymphocyte subtypes by using immunohistochemical analysis, yet added value of immunohistochemistry on to TILs evaluation remains to be demonstrated [4,15]. Moreover, digital image analysis of TILs can provide more exact measurement and eliminate inter-pathologists differences in TILs assessment [13]. Visual measurement of TILs is prefered at many trials like our study [4,6]. Because this route is stated as rapid, easly available, less expensive and adequate tool in TILs assessment. There is no established threshold for high TILs. Various studies used different cut-off values [7,9,16,17]. Moreover, 50-60 % of TILs value for lymphocytes-predominant breast cancer had been arbitrarly chosen [17]. In this study, ROC Curve was applied for the estimation of pathological response of TILs values, but a significant breakpoint could not be found (unreported data). Therefore, we accepted 10 % of TILs level as a cut-off value similar to many studies [6,18].
In our study, we investigated the relation of TILs value with other clinicopathological parameters and its impact on patients with all molecular subtypes of breast carcinoma who were operable following neoadjuvant treatment. The positive relation of higher quantities of TILs and both negative steroid receptor status and presence of HER2 positivity is striking in the literature like in our study [6]. Also LPBC is commonly found in HER2 positive and triple negative subtypes [4,19]. Similarly, in our study HER2 positive group was the main molecular subtype (50%) that harbours the high percentage of TILs. But, interestingly unique patient with LPBC was seen in our series. In this study, patients with luminal type breast cancer had lower TILs value, with the median of 6%. Similar to litreture, no significant prognostic role of TILs was found in patients of our luminal group [1]. According to the trial by Huszno [7] higher grades of TILs were present more frequently in younger patients than older women (47% vs. 24%). Moreover, higher TILs levels was appeared to be associated with higher histological grades. On the other hand, TILs value also was significantly correlated with lymphovascular invasion in our study.
The positive association between TILs levels and favourable clinical outcomes was based on Sistrunk’s cohort trial at 1922 [20]. Eastern Cooperative Oncology Group’s phase III trials showed that each 10 % increase in TILs levels significantly predicted better DFS and OS in TNBC with a median follow-up of over 10 years [21]. A recent meta-analysis of twenty-five trials including more than twenty thousands patients confirmed the survival benefit of TILs in TN and HER2 positive breast cancer patients [18]. Moreover, according to secondary analysis of the NeoALTTO trial reported by Salgado [17] patients with high TILs levels at baseline had better outcomes for event free survival independent of whether they achieved pCR in the neoadjuvant phase. The association between higher levels of TILs and decreased distant recurrence rates in TN breast cancer was found in FinHER trial [22].
Contrary to obvious results as to prognostic impact of higher TILs levels on the adjuvant and neoadjuvant settings, we could not detected any significant relationship between TILs and survival analysis. Another issue related to TILs is its utility in prediction of adjuvant and neoadjuvant therapy response [6]. At the adjuvant setting, the association between higher levels of TILs and increased transtuzumab benefit in HER2 (+) subtype was detected in phase III trial including 1010 early stage BC patients [22]. Positive correlation between TILs levels and pCR rates was prominent in HER2 (+) tumours. According to the study of Carbognin [12] pCR rates were increased by nearly 30 % in the presence of TILs reported as LPBC. Another trial has also indicated that the level of TILs greater than 5% was associated with higher pCR rates [17]. Although we could not detected significant correlation between TILs value and pCR in our study, there were non-significantly higher pCR rates in HER2 (+) group. The minority of our patient population explains the limited power of the statistical analysis.
Conclusion
Host immunity controls cancer and influences patient’s outcome. How can a host enhance anti-tumor immune response and which biomarker provides better treatment approach are the main questions. Although which level of TILs should be used to determine optimal treatment strategy for breast cancer patients has not been certain yet, many trials indicate that TILs is of prognostic effect in long-term disease control and predictive effect of a better local response to treatment. But, further resaerchs are warrented before the utility of TILs as an immune biomarker for routine clinical practise of breast cancer patients.
To read more articles in
Journal of Surgery
Please Click on:
https://juniperpublishers.com/oajs/index.php
For More
Open Access Journals
in
Juniper Publishers
Click on:
https://juniperpublishers.com/journals.php
#plastic surgery#surgery journals#JuniperPublishers#openacessjournals#Cardiac Surgery Orthopedic Surgery
0 notes
Last Seen Blogs

shespoeme
d.

audriwrites
AUDRIWRITES

idealuk
I don't negotiate with idiots.

datante
Datante's Inferno

ashesofangst
Jailbird is Singing High