#actually posttraumatic
Note
hi there!! i've been reading some of the discussions you've had & many of them are super informative and some comforting to read from the perspective of someone who's questioning if they might be plural/have a CDD. i really appreciate ur blog & the views and experiences u share on it, it feels like a warm hug amidst The Horrors of Syscourse.
i've had something on my mind though. this is probably a silly question, but it's possible to have a CDD without (C)PTSD, right? admittedly i'm kind of just asking this for reassurance while i'm on my own discovery journey. like. i have experienced traumatic events and some of it is ongoing & i'm still living with the people responsible, but i don't think i fit the PTSD criteria due to not experiencing flashbacks or strong emotions related to the events—i usually just feel totally empty & detached from it. i still believe i've been negatively affected by the events hence considering them traumatic, but that doesn't include any kind of flashbacks.
i've been trying to look into it & find answers but i've seen a lot of conflating of having experienced trauma with having PTSD, so most of what i find is "can you be plural/have a CDD without trauma" discourse.
i think it'd be neat to see more conversations about this but free to ignore this ask if u don't want to answer it/if u don't feel equipped to! wishing u the best. have a great day!!
This is actually a very interesting question.
I've read a lot of medical literature on trauma, and each author in the field seems to define what qualifies as PTSD or PTSD symptoms differently, which also lines up with my own experiences with medical professionals in practice. In general, me simply being traumatized was enough for me to be given an automatic PTSD diagnosis, regardless of which therapist or psychiatrist I saw. Some professionals I saw were very specific with what they called what, others were a lot more loose with it.
I've seen a lot of differing definitions and academic debate over what qualifies as a flashback, dissociation, a posttraumatic symptom, and so on. That is to say, it can all be very vague.
For example, there are other forms of flashbacks that exist outside of the well-known ones; some people only relive traumatic events emotionally, or through repeated thought processes, or somatic pain. A lot aren't even aware these are flashbacks, because it's experienced as 'random' emotions or pain or spirals or some other response, and a lot have trouble figuring out what even triggers these responses.
Would these experiences fall under what we call flashbacks in PTSD? Well, it probably depends on who you ask. And, in practice, whether someone with these experiences gets diagnosed with PTSD or a mood disorder or a personality disorder or somatic pain syndrome depends on the medical professional evaluating them.
To further complicate it, a lot of people don't experience overt c/PTSD symptoms until they are no longer living in the traumatic situation, which, for people who develop cPTSD, means they may not show obvious symptoms until a very, very long time after the trauma started. I didn't start getting "classic" PTSD flashbacks and "waking up in a panic attack in the middle of the night" type nightmares about the trauma until I wasn't around the people who did it anymore. However, I have experienced many other trauma-related symptoms and heavy dissociation ever since I was very very little. Before I was diagnosed with PTSD in highschool, I was diagnosed with a lot of other things first.
There's also just the fact that, for whatever reason, people don't all develop the same symptoms in response to trauma. Some people with very complex trauma never experience classic PTSD symptoms. Some people are very dissociative and numb, or develop mood disorders, or obsessive-compulsive symptoms, or somatic symptoms, or eating disorders, or some combination of things. Some people never externally harm themselves or cope using substances while others develop addictions to these things.
In addition, some people's experiences with trauma don't fall under the PTSD criteria's definition of trauma, so even if other symptoms are present they don't "technically" fit criteria. And sometimes medical professionals use their own judgement and diagnose these people with PTSD anyway, and sometimes they don't.
Plenty of people diagnosed with other childhood trauma-based disorders besides CDDs also don't fit c/PTSD criteria or show many c/PTSD symptoms or receive a comorbid c/PTSD diagnosis for whatever reason. It's complicated and messy.
This is all to say, I've encountered medical professionals who treat PTSD as synonymous with "traumatized" and are very loose with what they call PTSD and I've also encountered medical professionals who are very strict about the criteria and are very insistent on only diagnosing people who fit that, and I've met a lot of professionals somewhere in the middle as well. I've also encountered plenty who would much rather focus on helping the symptoms than on what the diagnosis is or isn't, and who don't really like the way mental health diagnosis is structured in the first place.
So, to come back to your question... I don't think there really is an objective answer to it, though personally I'd just say "sure it's possible, and I wouldn't really worry about it much."
In the end, what I've found is that it doesn't actually really matter that much? Regardless of whether there is comorbid PTSD or whether there isn't (or whether it's delayed onset or etc), in the end what you're dealing with if you have a CDD is still trauma, and the treatment for that is more or less the same, regardless of what you call it. There might be differences in, say, approaches to medication specifically, or specific symptoms, but even that is often just throwing things at the wall and seeing what sticks. Honestly, in my experience, treatment mostly looks different based on symptoms and individual needs rather than diagnoses, really.
In general, I find that a lot of people dealing with trauma and mental illness tend to over-focus on diagnosis and getting it right and trying to figure out whether they "really" have something or whether they're mistaken or somehow faking or so on. I think that's an unhelpful approach to it; there's no objective way to confirm that sort of thing, and either way you still need ways to cope with your symptoms, and coping skills are useful regardless of diagnosis. Learning how to ground yourself is useful regardless of whether you "really" dissociate that bad, learning emotional regulation skills is useful regardless of whether you "really" have severe mood swings, learning calming techniques and self-care and how to be gentle with yourself are good things for everyone to learn, coping skills are not just for people with certain diagnoses. In fact, you don't even need a diagnosis of anything to do these things.
And with trauma, like... it's all just trauma processing in the end, really.
I'll even go as far to say that even if you don't have PTSD, books and resources for PTSD might still be useful to you if you have a CDD or another trauma-related disorder, since a lot of symptoms overlap with other disorders and especially with trauma the recommendations for what to do about it tend to be applicable to a lot of different situations outside of strictly PTSD.
I realize I rambled a long time just to say "well, it's complicated and depends on what we mean by PTSD, but also it's all trauma anyway" but I hope this was helpful still?
I'm also glad to hear what you said about my blog, it was very nice to read.
51 notes
·
View notes
Text
Not-so-friendly reminder that you cannot be a system without trauma.
Some more proof; done by me, a person living with DID.
This is not syscourse, this is fact.
According to the Diagnostic and Statistical Manual of Mental Illness (DSM-5), a history of childhood abuse and neglect is prevalent in 90% of cases of dissociative identity disorder (DID). The remaining cases involve medical trauma, terrorism, and childhood prostitution. Ninety percent is overwhelming. Other research claims that rates of abuse and neglect in DID are actually much higher.
DID develops in response to severe, recurring trauma in childhood. Children are not fully equipped to cope with continued, severe instances of abuse, so they may develop dissociation as a survival skill, which can then develop into DID. It makes sense, then, that the rate of childhood abuse and neglect in people with DID is so high.
https://www.healthyplace.com/blogs/dissociativeliving/2016/04/the-undeniable-connection-between-did-and-child-abuse
The authors interviewed 102 individuals with clinical diagnoses of multiple personality disorder at four centres using the Dissociative Disorders Interview Schedule. The patients reported high rates of childhood trauma: 90.2% had been sexually abused, 82.4% physically abused, and 95.1% subjected to one or both forms of child abuse. Over 50% of subjects reported initial physical and sexual abuse before age five. The average duration of both types of abuse was ten years, and numerous different perpetrators were identified. Subjects were equally likely to be physically abused by their mothers or fathers. Sexual abusers were more often male than female, but a substantial amount of sexual abuse was perpetrated by mothers, female relatives, and other females. Multiple personality disorder appears to be a response to chronic trauma originating during a vulnerable period in childhood.
https://pubmed.ncbi.nlm.nih.gov/2044042/
Causes
The main cause of DID is believed to be severe and prolonged trauma experienced during childhood, including emotional, physical or sexual abuse.
The development of dissociative identity disorder is understood to be a result of several factors:
Recurrent episodes of severe physical, emotional or sexual abuse in childhood.
Absence of safe and nurturing resources to overwhelming abuse or trauma.
Ability to dissociate easily.
Development of a coping style that helped during distress and the use of splitting as a survival skill.
While abuse is frequently present, it cannot be assumed that family members were involved in the abuse.
Dissociative identity disorder (DID) is the result of repeated or long-term childhood trauma, most frequently child abuse or neglect, that is often combined with disorganized attachment or other attachment disturbances. DID cannot form after ages 6-9 because individuals older than these ages have an integrated self identity and history. Trauma later in life can lead to posttraumatic stress disorder or complex posttraumatic stress disorder, other dissociative disorders including other specified dissociative disorder, somatic symptom disorders, or possibly borderline personality disorder, but DID requires an unintegrated mind to form.
https://did-research.org/origin/
Other helpful links!!
DSM-5 on DID and
A explanation of each DD
NAMIs fact sheet on DID
Please see this account for OP
A PDF research paper done on the link between DID and childhood abuse
My own multi-part research thread
A post about biomarkers in the brains of pw/OSDDID
#Sage speaks#host posts#Mystic speaks#Mystic - 🧜🏻♀️#co-con#did is a disorder#did research#did#did is caused by trauma#you cannot have DID without trauma#stop faking DID you clowns#I was not traumatized for it to be used for clout chasing#endos aren't real#tw endos#endo dni#anti endo#fuck endos#anti endogenic#endos do not interact#endos fuck off#endos stop being shitty#endos are not valid#truamagenic system
221 notes
·
View notes
Text
DID/OSDD or CDD?
"Over the past few decades, it has become increasingly clear that DID is characterized by much more than alter personalities. Persons with DID routinely exhibit a vast array of dissociative symptoms. In other words, DID is more than an alter disorder; it is a chronic complex dissociative disorder. Coons (2001), for example, has argued that DID needs a name that 'truly reflects the polysymptomatic nature of DID' (p. 44).
In keeping with this understanding, Dell (2001a) has suggested renaming DID major dissociative disorder and Coons (2001) has suggested pervasive dissociative disorder. Perhaps the most common referent or label for DID (other than MPD or DID) is 'complex dissociative disorder.'
To my knowledge, no one has actually proposed that DID be renamed Complex Dissociative Disorder, but variations of this term have been cropping up in the literature with increasing frequency: 'chronic complex dissociative disorders' (Ross, 1990), 'complex chronic dissociative symptoms' (Loewenstein, 1991), 'complex posttraumatic and dissociative disorders' (Chu, 1998), 'chronic, complex dissociative disorder' (Tutkun et al., 1998, p. 804), 'complex dissociative disorders' (Coons, 2001), and 'the taxon of chronic complex dissociative disorder' (Ross, Duffy, & Ellason, 2002, p. 15).
Clearly, the authors cited in this paragraph understand DID to be much more than just 'an alter disorder.' They understand DID to be a major, pervasive, complex, chronic, dissociative disorder. Perhaps the DSM should call DID Complex Dissociative Disorder."
Paul F. Dell (2009) on giving DID a new name: complex dissociative disorder. Source (page 392).
#actuallydid#actuallyosdd#actuallytraumagenic#actuallydissociative#actuallycdd#dissociative identity disorder#complex dissociative disorder#academic#quotes#sunflower posts
174 notes
·
View notes
Text
I watched Dr. Robinson's lecture on social media & self diagnosed DID (didn't watch the Q&A part though). It was a surprisingly decent lecture for the complex subject it's tackling! I took notes throughout the entire video if anyone is interested & doesn't want to watch the hour long video (but I recommend you do so you can form your own thoughts on it).
Here's a link to the video.
My notes are under the cut. If you want, you can read a short version here.
Important to keep in mind: Dr. Robinson says that the TikToks he shares in the lecture are for illustrative purposes. He knows nothing about the people behind them, and he cannot verify who does or does not have DID. Further in the video he says that harassing or fakeclaiming people who say they have DID, regardless if they actually have it, does extreme harm. Despite that, it still feels inappropriate that they used these TikToks without permission, and without censoring.
The introduction starts off with describing how the DID patients in their clinic look nothing like the sensationalized portrayal of DID in media. People with DID experience distress & confusion towards their symptoms, which they are reluctant or ashamed to report. Many of their patients report feeling distraught/confused by online content where people promote DID symptoms openly in a fun, sensationalized way. For illustrative purposes, Dr. Robinson shows a TikTok of a person asking their partner to guess which alter is fronting. It's a bunch of clips cut together of them going "guess who's fronting!" in a different voice and their partner gets it correct every time, like a little game.
He explains how recently, many people are coming into the clinic self-diagnosing as DID. They do not have a trauma history and their parts are character-like. The symptoms they present are not typical to DID.
He shows a TikTok of someone changing outfits to music, with the caption asking to guess which system member is wearing what. Robinson says that these overt changes in wardrobe are not characteristic of DID. Nearly all patients with DID are reluctant to discuss their symptoms and conceal it. So this begs these questions: Do online influencers genuinely have DID? If not, what are they experiencing? And what role does social media play in self-diagnosis & the perception of DID?
DID is considered the most severe/complex trauma-related dissociative disorder. It involves symptoms of:
Depersonalization
Derealization
Amnesia
Identity Confusion
Identity Alteration
At times, pwDID report experiencing someone in their mind who is "not me." At times, it feels like someone else is "driving" the body with a distinct set of thoughts & behaviors. Shifts are subtle or completely hidden. Dr. Robinson emphasizes that they rarely see obvious signs of switching or changes like what was depicted in the video earlier.
What's interesting to me is that he describes amnesia in DID as only being trauma-related… From what I understand, however, amnesia in DID can apply to everyday life as well.
He states that identity alteration (alters, switching) is the most sensationalized symptom of DID. Agreed. DID is not an alters disorder. "DID is really about the 'not me' experience." It is about wanting to get through everyday life without having to re-experience overwhelming trauma info.
He brings up media portrayals of DID like Split & the United States of Tara which have sensationalized the alters aspect of DID. This media has also perpetuated other myths such as the idea that pwDID are dangerous or extraordinary.
He talks about the development of DID. It's a posttraumatic disorder. Requires chronic, severe trauma during early development. In the absence of nurturing & soothing adults, the child internalizes aspects of their environment. The process of personality development is fragmented & those personality parts are anthropomorphized.
DID is really a disorder of hiddenness, he says. That's why it's surprising to see so many people online coming out and celebrating the diagnosis.
He uses a TikTok video of someone saying they got diagnosed with DID & that they're going to get a cake to celebrate. They literally ask the bakery person to write the phrase "happy DID diagnosis" on it. Omg I would not have the balls to do that… Tbh I don't vibe with thinking it's bad to feel happy/relieved about your diagnosis. I think more people should feel happy about it, because in the past it was so common to feel like a diagnosis was more like a death sentence. Robinson says that patients usually feel more fear after getting diagnosed, but that's not a good thing in my opinion.
The problem here shouldn't be that someone is happy/relieved they got an answer to their questions & a label for their pain. The problem here should be the sensationalization. It should be about how they boosted the entertainment value of it for profit.
He describes the history of DID being delegitimized. Freud decided it was false memories, then there was false memory syndrome. Etc. Etc. In the most recent decades, there has been so much more research & support for DID as a legitimate, trauma-based disorder. But many people still don't believe it and false memory controversy is still perpetuated. Robinson says that the recent trend of inaccurate social media representations is further delegitimizing DID.
At the heart of DID controversy there are two models for it:
Trauma model: DID is trauma-related and trauma memories are true
Fantasy model: DID is unrelated to trauma, resulted from fantasy-proneness or suggestibility, influenced by social media or other factors, and trauma memories are exaggerated or simply not true
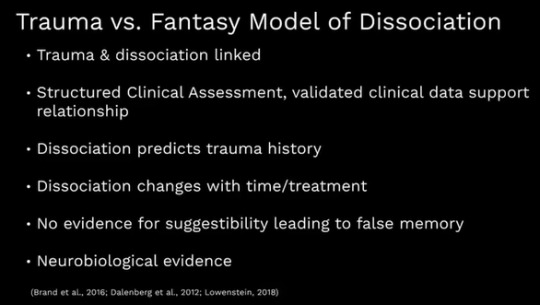
He discusses the neuroscience behind it! Researchers are finding that DID has a unique biological imprint, further supporting its legitimacy as a real, trauma-based disorder.
Robinson says that people with DID have always been online & had online communities. Yet, specifically in facebook, youtube, instagram, TikTok, and twitter we see an issue. They are a bit different because (on the monthly) the active users are up in the billions. They are also algorithm-based, so liking content on DID will result in your feed giving you more DID content. The pandemic has also further driven people to social media, too.
TikTok DID hashtags get billions of views.. Robinson says these views have grown by 200-400 MILLION over the past 4 months.
PROS of discussing DID on the internet:
Evidence & info on DID is becoming widely & easily available. More resources for people. This has created safe spaces online for people who are trauma survivors, researchers, & clinicians. With so much good information, many of the false representations & misinfo can be countered. This means that many people can self-diagnose accurately! There's been a general destigmatization of DID online. The dominant narrative is no longer skeptical.
CONS of discussing DID on the internet:
There is also more inaccurate information. Most of the time the representation of DID is wrong. This leads to inaccurate self-diagnosing. People (especially young people) may attach clinical labels to normal experiences. They may elaborate or manifest DID-like symptoms instead of acknowledging they have a different problem. COVID has made people more vulnerable to this. There is also significant online harassment & fakeclaiming towards DID influencers.
FAKECLAIMING HARMS EVERYONE WITH AND WITHOUT DID. Robinson says that fearing you may be faking is one of the most common symptoms of DID. Regardless if someone genuinely has DID or not, calling them fake will harm both them and all other people with DID.
Now, I find it a bit questionable that they are using uncensored TikToks in this lecture despite acknowledging that these people face elevated fakeclaiming & harassment... I get that it's for educational purposes but it feels especially inappropriate when acknowledging this.

Social media has dynamics that reinforce these uncharacteristic DID representations. It rewards people who create attention-grabbing content for likes & follows, regardless if the content is true. That's why you can't know if someone is faking just because of their uncharacteristic portrayal, because it's possible that social media is influencing them to express themselves in different ways. But, it's also possible that these dynamics are still contributing to an increase of inaccurate self-diagnosis.
He brings up someone called the ace system (?) who has generated millions of views. I have NO IDEA how to describe the TikTok he just played. It was like…snippets of different system members talking about their day? They talked about panic attacks and stuff. They also switched so much in just one day. Seems exhausting.
Robinson does say "it's possible that some social media influencers like the ace system(?) may be malingering or have factitious disorders" which I personally don't see as him doubting that person in particular. He's not saying THIS PERSON IS MALINGERING, he's just saying some people might be malingering but we really wouldn't know as onlookers.
Describing what malingering & factitious disorders are now.
Malingering: intentional reporting of symptoms for some external gain like money
Factitious: intentional reporting of symptoms, but not just for som external gain
For illustration of external gain (which isn't inherently malingering), he's showing the ace system's (?) merchandise website. Then a cameo account where you can book a personalized video from the system. Another TikTok system he showed earlier makes a reappearance, this time to show that they are selling hats that their system made.
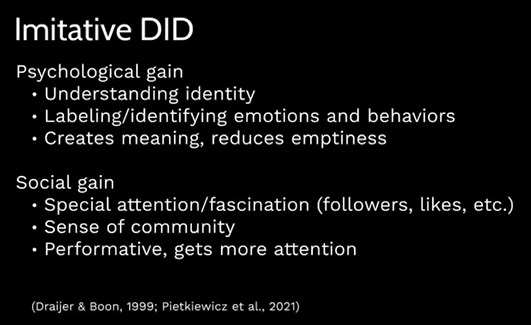
Imitative DID is for people who do not actually have DID but genuinely believe that they do. They may benefit from psychological or social gain, which makes social media platforms the ideal platform for them to thrive. Claiming they have DID might provide them a sense of connection/community. They may struggle with their identity such as who they are in the world, what community they belong in, who they'll be in the future, etc. Robinson says that "the DID narrative helps these people explain frequent confusion about who they really are."
Dr. Robinson says that endogenic systems (which he also just calls plurality/multiplicity) can sometimes be an example of Imitated DID. He mentions Astraeasweb from the 90s claiming nonpathological multiplicity/plurality as an identity. He plays a new TikTok of someone telling people to look up The Plural Association and "welcome to the plural community" and tips on how to start system communication.
He says that people with DID don't choose this or wish for this. The symptoms are developed out of need for survival.
Endogenic plurality refers to any development of plurality that does not have a trauma origin. They promote their plurality as a healthy way of their mind working; an identity. Some of them don't identify as having DID, but Dr. Robinson says that many do (I personally think it's the opposite but *shrugs* he might be lumping all cases of imitative DID in there).
He says that more research needs to be done to see if endogenics are genuine DID, imitated DID, or something else entirely.
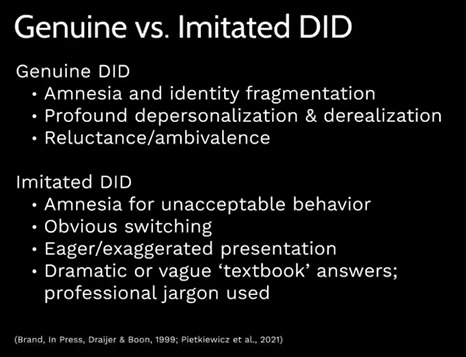
Dramatized, obvious switching is actually very rare in DID. Yet, it's very common in online videos. He shows a TikTok of someone sitting in a car who is "switching." They stare into space, close their eyes slowly, drop their head down for a while, then they lift their head up and smile. He shows another TikTok of someone who also drops their head down (it says "no one in the body"?) and after a long time, they lift their head up, start swearing(????), and then cheekily take their name tag off while staring at the camera.
Robinson says that in both of these examples we see an uncharacteristic awareness of the process of dissociation, because these individuals could actually plan for and videotape what was going to happen. He says the switches in genuine DID are subtle and often unnoticed by outside observers.
In imitative DID there is also an emphasis on elaborated parts. They lack the confusion & distress/conflict with these parts which is characteristic of DID. He shows a TikTok of someone showing Picrews of their parts. Then he shows another TikTok with someone playing guess-who trying to figure out who is fronting. So literally playing a game. "A game-like way of presenting symptoms that would be very distressing in genuine DID," Robinson says about that video.
There was a recent case study that interviewed people who were not given the diagnosis of DID and found that they were angry + relying on the diagnosis for connection & attention.
Once again, he says it's difficult to distinguish whether social media influencers are genuine, malingered, imitative, or something else. It's not something even professionals can distinguish as onlookers. We don't know anything about the people in the video examples except for what they put out online.
To conclude the lecture, Dr. Robinson says that accurate online information & professional education is MORE IMPORTANT THAN EVER given the increase of DID awareness. Wrong info & poor representations delegitimizes DID and causes harm. We don't want it to undermine all of the progress in research in the recent years.
#syscourse#dissociative identity disorder#social media and the rise of self-diagnosed dissociative identity disorder#mclean hospital#long post#sunflower posts
78 notes
·
View notes
Text
February 2023 reading
Books:
Captive Genders: Trans Embodiment and the Prison Industrial Complex, ed. Eric A. Stanley
Toni Morrison, Playing in the Dark: Whiteness and the Literary Imagination
Jeff Vandermeer, Annihilation
H. G. Wells, The War of the Worlds
Tom Stoppard, Arcadia
Essays, articles, and chapters:
John Hermann, The Junkification of Amazon
Peter Brook, 'Introduction,' from Reading for the Plot
Bertrand Cooper, Who Gets to Actually Create Black Pop Culture?
Tzvetan Todorov, Structural Analysis of Narrative
Domino Club, good writers are perverts
Courtney Desiree Morris, Why Misogynists Make Great Informants
Rita Felski, Context Stinks!
Bonnie Burstow, A Critique of Posttraumatic Stress Disorder and the DSM
Bret Devereaux, Collections: Teaching Paradox, Crusader Kings III, Part I: Making It Personal
Hayden White, The Historical Text as Literary Artefact
Jabeen Akhtar, Why Am I Brown?: South Asian Fiction and Pandering to Western Audiences
Karl Marx, ‘Chapter One: Commodities,’ from Capital: Volume I
Roland Barthes, ‘The War of Languages’ and ‘The Division of Languages’ from The Rustle of Language
116 notes
·
View notes
Note
for the did ama, what's something you wish more people understood about did? (this can refer to singlets, people newly diagnosed, stuff that the community in general just may not know or acknowledge, etc)
i kind of share something similar to this in this ask to do with child alters if you wanted to see that
anyways there's probably a lot of angles i could go at this with but hm. i kind of hate how the online community is SO focused on alters themselves, identity alteration, like i think to a lot of people to be perceived as a Valid DID Haver you have to have alters with different names and different pronouns who act totally different from one another and that's just... not... not necessary or even common.
i took a bit to answer this because i wanted to pull up this study which has this quote, referencing some kluft research:
Many clinicians and lay people believe that DID presents with dramatic, florid personality states with obvious state transitions (switching). These florid presentations are likely based on media stereotypes, but actually occur in only about 5% of DID patients [60]. The vast majority of DID patients have subtle presentations characterized by a mixture of dissociative and PTSD symptoms embedded with other symptoms such as posttraumatic depression, substance abuse, somatoform symptoms, eating disorders, personality disorders, and self-destructive and impulsive behaviors [23, 61].
DID is a heavily covert disorder for many and while it's not unusual or even surprising that going into therapy and purposefully interacting with alters + using social media where that sort of behavior is expected/encouraged can cause us to become more "florid", many of us aren't like that... at all! and the lack of representation for people with DID who don't have super distinct alters or who simply don't want to share that information online is actually kind of appalling to me. DID is a dissociative disorder caused by childhood trauma first and foremost and comes with all the struggles related to those things. alters are just one piece of the puzzle. and the continued focus on alters harms both singlets because they don't understand DID outside of that, and people with DID... i can't tell you how many times i've talked to people with very obvious DID who thought they didn't have it because they didn't match social media depictions of the disorder. it's like everyone's trying to be like Sybil, subconsciously or not, and that's just... not always how it is!!
of course people with DID who have florid presentations are valid too and there are aspects of my DID that are very Not covert but growing up my situation was a lot more subtle and even now, there's so much about my DID people don't see because the only acceptable way to parse or talk about your symptoms and experience online are by well defined alters and the majority of our alters are just Not like that. i have so many alters that are just "me but slightly to the left" who would be hard to detect personality changes with, etc. many such cases.
tldr very good to keep in mind that people with DID are traumatized and dissociative individuals with a variety of symptoms that may or may not fall into the "idealized" standard depiction of DID on social media and in fiction, and i REALLY wish there was more discussion on the other parts of this disorder more often
#kiki was here#asks#the DID ama#mephilesthegay#i think it's easy tofall into the trap of only talking about alters#cause talking about alters can be fun!#it's like an escape from the bad of it all sometimes#and some talking about alters is good#just wish there was more balance yknow
24 notes
·
View notes
Note
hi, in a post you recently said 'if you're ever questioning if something you're experiencing in a relationship is healthy, please don't hesitate to reach out to me and ask', so i was wondering if this was okay? if not, please ignore and sorry for the convenience. i hope this isn't triggering but it includes bdsm and rape fantasies.
i'm very lucky to be in a relationship with a man who made it clear for day 1 that he wasn't going to hurt me during sex, pretend to force me, or engage with any of that. i used to be big time into bdsm but over the last 10yrs i've been doing more feminist reading and having conversations with others and tried to unpack all of that, which has left me wanting to distance myself from it. i stopped justifying and defending bdsm, stopped engaging with bdsm-content in fiction and stopped watching porn all together. i got more involved with anti-prostitution and porn advocacy too.
the problem is that i'm still engaging with it internally. it's like a switch flips in my head when i'm with my partner and i construct this world where i'm being forced but can't show it. i used to think it was because of prior trauma and i was trying to get a sense of control, but it just feels like i'm using that as an excuse. it's a big thing in the bdsm community to justify it by claiming you're 'working through your trauma' but i was supposed to be past that now. it's been years so i feel like i don't have a good reason to be still doing this.
do you have any advice? once again, thank you.
I'm glad you asked! it wasn't exactly what I was talking about in the post - more internal rather than interpersonal - but I actually can relate in a sense. my wife tells me that sometimes when I get super stoned (which I rarely do tbf), I talk about wanting some fucked up things. I definitely THINK about some fucked up things. I'm quite far out from any posttraumatic mental effects, so I also don't feel that that explains it, and I'm fairly sure I had some questionable fantasies prior to my traumas, too. i wouldn't call it kink, though, bc they're not inherently tied to sex nor arousing to me on their own. I think I like violence and adrenaline and always have, and I don't really care which direction the violence goes, I just find it fun. but that's not a "need," as men would have you believe. it's just a quirk of my personality, and while I choose not to engage with it outwardly (I don't start unnecessary fights but I don't shy away either), I also refuse to make myself ashamed by it. there is no such thing as a thought crime. your stances against prostitution, porn, and, yes, bdsm as well, are not compromised or hypocritical because you have those thoughts. let them be, observe them, and release them as feels right to you. i think the idea that we must analyze such things to death is rather Christian in nature and likely in origin: the idea that our thoughts and desires can be sinful themselves, or that they speak to who we "really" are. I think that's a load of shit. I don't believe anyone who would claim to have never thought (or even desired!) some really unhinged shit. humans are weird! I'm glad I have someone I can tell all my unhinged thoughts to without judgment, but none of it means I'd ever act on such things.
tldr, we all have some out of pocket thoughts (beyond just intrusive thoughts, to be clear!) and I don't believe there's anything wrong with that on its own, nor are we obligated to explain them
I don't expect everyone to agree with this, but it is where I stand on the matter
9 notes
·
View notes
Text
stop fakeclaiming child alters just because they aren't "accurate"
below is a comment found on a popular subreddit that fakeclaims dissociative and posttraumatic experiences. in this comment, they are referring to people with dissociative identity disorder and similar disorders who have "littles" which is a common community term for alters that present as children. if you are not familiar with child alters, please refer to this professional's explanation.
you can also find more information on how alters might present as different ages here. please stay informed!

as you can see in this comment, this person is criticizing how child alters type or speak because it's not accurate when comparing them to real life children. what they don't seem to understand is that child alters are not the same as real life children (howell, 2011, pp.60-61). they are part of a mental health disorder. and while child alters are often more vulnerable & traumatized then older alters, it's actually counter-therapeutic to treat them like they're no different from real life children (shusta-hochberg, 2004).
child alters are very similar to the concept of an inner child. your inner child is a part of you that preserves the things you remember, learned, fantasized about, and felt when you were a child. child alters are very similar to that, except they're more disconnected. dissociative processes involve them taking control of the body and acting independently.
child alters are often more limited than the adult alters...they "may not be able to tell the time, hold a pen and write, and they may only use and comprehend very simple language. these assets become even weaker when survivors become very afraid, angry, or ashamed" (van der Hart et al., 2006, pg.138). it is extremely common for trauma survivors to regress to a child-like state at times, even for people without child alters.
no matter how child-like someone becomes, if they are adult-bodied then they are not an actual child. the way a child alter acts or talks may be inhibited but is rarely fully "accurate."
it makes no sense to criticize an adult for...not being a child?
one of my alters is an infant. that infant alter is still able to type and communicate, although in a more limited way. they know how to unlock our phone & how to contact someone during emergencies. they don't write or talk very well, but they still know how to do it. if young alters had to act "accurately", i would be unable to communicate or understand phones or walk or stand up or even eat solid foods when that alter fronted. this alter fronting could end up killing us, so i would probably need a caregiver 24/7.
that isn't how things work, though. i'm an adult with a mental disorder, not a shapeshifter. the lack of compassion and critical thinking that some people extend to neurodivergency and trauma survivors is heartbreaking.
please stay educated on mental health! please don't fakeclaim someone just because their child alters aren't "accurate."
references
Alter ages. DID. (n.d.). Retrieved August 16, 2022, from https://did-research.org/did/alters/ages
Holland, K. (2019, August 30). Age regression: What it is, why it happens & when it may be helpful. Healthline. Retrieved August 16, 2022, from https://www.healthline.com/health/mental-health/age-regression
Howell, E. F. (2011). Understanding and treating dissociative identity disorder: A relational approach. Routledge/Taylor & Francis Group. https://doi.org/10.4324/9780203888261
Incest AWARE. (2021, February 24). How to reparent the child within: Healing the inner child after incest abuse. Incest AWARE. Retrieved August 16, 2022, from https://www.incestaware.org/post/how-to-reparent-the-child-within-healing-the-inner-child-after-incest-abuse
MSW, K. B. (2020, August 3). Understanding child parts in the dissociative system. Discussing Dissociation. Retrieved August 16, 2022, from https://www.discussingdissociation.com/2009/01/understanding-child-parts-in-the-dissociative-system/
Shusta-Hochberg, S. (2004). Therapeutic Hazards of Treating Child Alters as Real Children in Dissociative Identity Disorder. Journal of Trauma & Dissociation. 5. 10.1300/J229v05n01_02.
van der Hart, O., Nijenhuis, E. R. S., & Steele, K. (2006). The haunted self: Structural dissociation and the treatment of chronic traumatization.
#syscourse#dissociative identity disorder#dissociation#dissociative identities#dissociative alters#child alters#mental health awareness#mental health stigma
108 notes
·
View notes
Text
i hate this damn post so much and it showed up on my dash recently so i need to rant a little bit about the parts that bother me the most lol. putting it under a cut because it's not the prettiest or most well-constructed argument i've ever made, i mostly just want to be a bitch about it.

almost cult-like in what way, lmao??? all the preceding sentence describes is...someone being attached to a community they like and feel valued in. following that up with "eww, culty, right?" is just weird fearmongering. also, why wouldn't this hypothetical person look any further? in what plural circles are you witnessing anybody be anything less than wildly supportive of self-exploration??? really the fearmongering about cults is what squicks me out here though lol you can't just say shit like that without an actual argument to support it

this conjecture is so fucking stupid i don't even know where to begin. where is proof for any of this? do you actually think endogenic plurality research has more funding than research on dissociative disorders? do you think even if that were the case that would be endogenics' fault or responsibility??? i dare you to point out anything, anywhere, indicating the endogenic community has any kind of collective opinion on how DID treatment should work. it would sure be weird if they did because most people who do not perceive their plurality as disordered therefore aren't looking for treatment for it!
i mean, yeah, you're just describing an unwillingness to work on a symptom, you've very nicely made it look like there's a correlation with iding as plural here but there really isn't. if someone who IDs as plural thinks they can get away with "my alter is just an asshole" then that person would be just as likely to use the logic "i'm just an asshole" if they didn't. "well, somebody COULD use [x] to avoid working on their problems!" is not an indictment of [x] because people can use literally anything to do that.

ok im just going to be a huge bitch here and get on my antipsych high horse a little bit but LOOOOOOL. LMAOOOO. oh noooooo...ND/MI people supporting each other and creating resources for each other instead of revering the psych industry above all else...ahhh so scary!!! Somebody do something!!!

could not disagree more! i'm diagnosed with DID, i experience complex dissociation and posttraumatic stress symptoms that inform literally every area of my life, AND I STILL find a lot of common ground with endogenics/nondisordered plurals and have learned a lot from them and been helped significantly by what i've learned :thumbsup:
anyway this post sucks, i think it's full of fearmongering and bad faith arguments. i also think fearmongering is something this particular user is really good at along with sounding like they're making clever and insightful points when what they're saying doesn't actually have any weight behind it, and their determination to villainize endogenics (and their attempts to paint them as a group with some kind of significant societal power???) is alarming. don't like to see that.
52 notes
·
View notes
Note
can you do a debunk on these sources? https://at.tumblr.com/debunkingsystemscringe/mind-if-i-can-get-some-pro-endo-research-from-you/yihxbmcgdly4
I've already debunked all of these, but sure, I can do it again, let's see if @debunkingsystemscringe will actually respond this time
So, the carrd
The card is extremely bad, it's misquoting an incredibly important paper by Ross. His was the first to acknowledge that not just abuse caused DID, but trauma. I hate seeing this one used by endos because it was a MASSIVE step for DID systems, and it's being misused and misquoted here.
"These individuals often did not report abuse history and often reported experiencing little psychopathology."
This was one of the first papers to look at functional multiplicity as a treatment path and "smaller" trauma as a cause. It's not meant for endogenics.
"About 2% of people may be natural multiples who do not have dysfunctional posttraumatic MPD. They may simply have a highly dissociative psychic organization’ (Ross, 1991, p. 510)."
This was a theory that was debunked with the idea of trauma as a cause, and "highly dissociative psychic organization" doesn't mean "alters". I don't even think that's the correct quote, which is hilarious.
What's funny here, is that they're not actually quoting Ross, because his paper doesn't say that shit. They're quoting a college dissertation by McClure, quoting Ross, because you have to double twist it in order to make it work.
McClure's paper also doesn't imply anything about endogenic systems. Here's my debunk on her and Ross.
Next: Transgender Mental Health
I've talked about this one before, and how it's being touted as more important than it is. It's actually a really good book! I support this book and the stuff in it. But a lot of people are blowing it way out of proportion.
First, it has one chapter on "plurals" and how to treat them for gender related issues. Cool. That's true, it happened. I support the book.
However, it's not supported or endorsed by the APA, it wasn't published by them -- it's an independent book and everything in it is the opinion of the author. Same with the next paper by Isler. Like, it's useless, it means nothing. It doesn't talk about how or why, it says, "these people say they exist and it's going to make treatment harder because of the intricacies." That's it. Still a good book, check it out.
Next: Tulpas and Mental Health (it’s a PDF, be careful opening on phones)
I’m trying to find my full debunk on this. Jacob Isler is a practicing tulpamancer and has done some REALLY shady stuff-- Reddit has basically turned on him and disowned him and all of his work. As soon as I find the sources, I’ll add. Just give me a bit.
Alright, we’re going to have to redo it, here we do.
Jacob Isler has a severe nonresponse bias. Survey sent to 365 people and only 68 got back? That’s too small. Negligible read. The entire paper is about how tulpamancers are mentally ill in other ways, and that creating a tulpa has a positive impact on their mental health. Fine and dandy. It discusses how those mental health issues might play a huge role in the tulpamancy phenomon, but purposefully tries to twist the connection between the two to be unrelated on a pathological level. It also states: “Additionally, self-reported data gathered through online surveys, regardless of the care taken to ensure objectivity and accuracy, is bound to be influenced by biases and misconceptions. And, of course, the observational nature of this study means that causality cannot be proven. The intent of this paper is not to provide definitive assertions on the psychology of tulpamancy. Rather, the purpose is to accentuate outstanding associations and suggest further research into them.“
It’s basically admitting it’s own failure as an unreliable paper and simply calls for more research.
As for reddit disowning Isler: Isler is Fordaplot. Here’s the ban note from the mods

Next: Multiplicity: An Explorative Interview
We all know how much I love this useless article. Here’s my debunk. It’s based on 6 people only, admits it’s limited by not being able to verify their claims of functionality to make the point of the article, and then goes on to claim that online spaces for multiples are harmful, doesn’t discuss how and why, and only discusses the fact that they claim to exist and calls for more research, so. Kind of useless.
As for the cultural exclusion in the DSM and ICD, it’s specifically in regards to religious practices in cultures that someone has been raised in. As per the DSM, the difference between DID and these forms of “non-pathological possession trances” is that the non-pathological possession is short-term and occurs in specific cultural and religious ceremonies-- which is the opposite of what endogenics are experiencing (long-term, occurring continuously and not only in ceremonies (which they are not participating in to begin with)). It’s not excluding these experiences because they’re “endogenic”, it’s excluding them because it’s not plurality as we (endos and DID systems) describe it. Claiming that exception is for endogenics is hugely disrespectful to the clinicians and researchers who put an absurd amount of work into keeping religious experiences out of the DSM.
It’s just not for you.
22 notes
·
View notes
Note
i just - your two ao3 bookmarks are in supernatural and metal gear? impeccable, flawless taste, no notes, but aye, the horrors -
SHDHGSDHDKJ Y EAH I started watching spn back in 2008 or 2009, I actually have a million more bookmarks on my browser because I was reading spn fic on. livejournal.
speaking of metal gear, borrowing this ask as an opportunity to connect some dots because my god do I think about metal gear constantly

Posttraumatic Stress Disorder, Trauma, and History in Metal Gear Solid V, Amy M. Green



Rome, Blood, & Power, Gareth C Sampson

Posttraumatic Stress Disorder, Trauma, and History in Metal Gear Solid V, Amy M. Green


The Deaths of the Republic, Brian Walters
its like. the recurring violence of it all!! the last generations of the roman republic, snake eater/peace walker/phantom pain, none of you ever stood a fucking chance! the rot of military imperialism already doomed you!!!! you are trying to fix a decaying corpse, but the putrid flesh from the limbs is sloughing off in your hands!!! assigning a higher ideal, a fantasy, to the economy of war/imperialism/political violence won't change what it is!! do you think love can bloom on a battlefield? yeah, but it sure as hell won't save any of you! it will make you cannibalize each other**
**love wins for dave and otacon tho
#ask tag#long post#there's a cannibalism fic where post hell dean eats sam that really did a lot for me when i was reading ancient greek lit#love a family horror show in any setting or genre!#actually the exact thing that makes me chomp on bb/kaz gives me brainrot about sulla-crassus#anyway i getting off topic. if anyone thinks my additional reading notes are bad (long) now. they could be so much worse#i cut out all the stuff that isn't strictly related to the topic at hand so RIP to the MGS quotes and to Alan Wake and Control......#(somewhere. in a folder. i have a 3/4 of the way finished dead romans Control AU)#anyway thank you anon for giving me an opening to finally do a MGS-Late Roman Republic connect the dots post#do y'all ever think about kaz going by benedict in mgs1. because i think about it a lot#CHRIST i am getting off topic. i think about metal gear a lot
19 notes
·
View notes
Text
Many clinicians and lay people believe that DID presents with dramatic, florid personality states with obvious state transitions (switching). These florid presentations are likely based on media stereotypes, but actually occur in only about 5% of DID patients [60]. The vast majority of DID patients have subtle presentations characterized by a mixture of dissociative and PTSD symptoms embedded with other symptoms such as posttraumatic depression, substance abuse, somatoform symptoms, eating disorders, personality disorders, and self-destructive and impulsive behaviors [23, 61]. A classic presentation includes a history of multiple treatment providers, numerous serious suicide attempts resulting in repeated hospitalizations, and good medication trials typically with limited or no benefit [23].
Although the media and public are often overly fascinated with DID dissociated self-states, the complex symptomatic presentation of DID receives more clinical attention from trained clinicians [62–64]. Under-recognition of DID is common because the most obvious and pressing aspect of a patient’s clinical presentation may be one of the many comorbid disorders (e.g., severe mood disorders, posttraumatic stress disorder [PTSD], eating disorder, substance abuse, BPD), or the pseudopsychotic symptoms related to the overlap and intrusions of self-states into consciousness. This overlapping influence of self-states causes “passive influence” phenomena or Schneiderian first rank symptoms, which are more common in DID than overt, obvious “switching” of states. DID patients experience more first rank symptoms than do individuals with schizophrenia, with the exception of thought broadcasting or audible thoughts [65, 66]. Intrusions into consciousness may be partially excluded from consciousness (e.g., hearing voices of states, thought insertion/withdrawal, “made” actions/impulses) or fully excluded from consciousness (e.g., time loss, fugues, disremembered behaviors; [61, 62, 64]. Psychotic symptoms occur in 20 – 50% of BPD patients and childhood trauma may play a role in development of hallucinations in BPD, as well as in DD and other disorders [67]. Research indicates that DD patients show greater ability to be logical, reflective, and reality-based than BPD patients (see below) although more research directly comparing the groups on psychotic symptoms, including Schneiderian symptoms, are needed.
-> Chronic complex dissociative disorders and borderline personality disorder: disorders of emotion dysregulation? by Bethany L Brand & Ruth A Lanius
13 notes
·
View notes
Note
About the post of one of the last anons, which post was the one with types of DID? The ones mentioned in the other post were modular and secret DID. I looked on your blog for them but can't find anything. ^^
It can be a bit of a pain to find things here. Thank you for asking.
Oz
Here you go:
Latent DID – The alters are generally inactive but may be triggered by stressors which are somehow symbolic of the traumatic event. Examples of this are when the patient’s children reach the age of the patient during the trauma, or the perpetrator becomes ill or dies. During such time the alters may emerge for the first time publicly, which provides a window of diagnosability.
Posttraumatic DID – Symptoms are not present until the patient experiences an overwhelming contemporary event such as a great loss, rape, combat, or a head trauma sufficient to cause organic amnesia.
Extremely Complex or Polyfragmented DID – Presence of such a wide variety of alter personalities with such frequent switching between alters that it is difficult to discern the outline of DID and the multiplicity actually disguises itself.
Epochal or Sequential DID – When an alter emerges it takes over for a long period of time before the next alter takes over for another long period of time. While one alter is out, the others go dormant.
Isomorphic DID – Several very similar alters take control as a group and try to pass as one. The only overt signs may be a fluctuating level of function, unevenness of memory, or inconsistencies in the patient’s personality. Kluft’s example is “she’s quite bright, but what an airhead!”
Co-conscious DID – The alters know about one another so there is no demonstrated time loss or memory gaps.
Possession Form DID – The most evident alter presents as a demon or devil. This can be seen more commonly in cultures where religion or rituals have to do with demons and can easily be mistaken for psychotic conditions.
Reincarnation/Mediumistic DID – Alters who are experienced by the patient as having a supernatural quality and communicate with the patient in such a manner.
Atypical DID
A group of patients that is rarely diagnosed.
Private DID – Alters are aware of one another and have consciously adapted to pass as one.
Secret DID
Closely related to Atypical DID . The host is unaware of the alters, who only emerge when the host is alone. One might suspect this in a patient who cannot account for his or her private time.
Ostensible Imaginary Companionship DID – The patient has an adult version of the imaginary companion who is friendly and supportive with the other socially constricted host. What the patient is not aware of is that this entity does assume executive control and that there are other alters present as well.
Covert DID
This is the form most characteristic of patients with DID . Alters contend for control and influence without assuming full executive control. To patients it feels as though their lives are out of control and that their actions are imposed upon them by a power unseen rather than selected by them.
Puppeteering or Passive-Influence Dominated DID – The host is dominated by alters that rarely emerge. If the host is unaware of these alters he/she feels like the victim of influences that force behaviour in a direction not chosen.
Phenocopy DID – The most important of the covert forms. Occurs when the alter’s interactions with, and influences on the host and each other, create phenomena that are similar in appearance to the manifestations of other mental disorders. For example, alters who are in conflict and are insistent on their thoughts while cancelling out one another’s actions can imitate obsessive compulsive disorder. When a patient has alters who harass one another, it appears to the onlooker as though the patient is hallucinating, which would resemble an acute schizophrenic episode. Alters with different moods can have the appearance of an affective disorder. Alters in contention may create the chaotic appearance of borderline personality disorder.
Somatoform DID – Very common. The pain or discomfort of a traumatic event which was experienced by an alter, is felt physically by the host, who has no memory of the trauma. Examples are pain in the rectum or vaginal area, numbness or tingling in the extremities from being tied up during abuse, a sense of choking or nausea associated with forced oral sex. This should be suspected when there is no apparent physiological explanation for the pain.
Orphan Symptom DID – Closely related to all of the covert categories. This is the phenomenon of unexplained and spontaneous feelings, sensations, actions, or intrusive traumatic imagery which manifests in the host, is not understood by the host, and which has been triggered by a contemporary stimulus that relates to the childhood trauma.
Miscellaneous Presentations Of DID
Switch-Dominated DID – Most commonly seen in the patient with a large number of alters. The switching process is so rapid and frequent that the patient appears bewildered and forgetful. Patients are often misdiagnosed with an affective disorder, psychosis, and organic mental syndrome, or seizure disorder.
Ad Hoc DID – Very rare. A helper alter creates a series of alters that function briefly and then cease to exist. This can be suspected when the patient’s history may suggest DID or recurrent fugues, but no alter can be found to explain the missing time.
Modular DID – Very uncommon. This occurs when usually autonomous ego functions split and different personalities are reconfigured from their elements. When an alter is encountered it may have a vague feeling to it, and may never be seen in exactly the same way again. These patients have been seriously abused, and are brilliant and quite creative. Kluft has also found an unusual computer literacy since childhood among these patients.
Quasi-Role-Playing DID – In this case the patient is attempting to disavow the diagnosis of DID . One alter acts out when it knows of the other alters, and then informs the clinician that he/she has been feigning DID . The patient states they have willfully generated this behaviour. In the 11970’s and 1980’s this was seen exclusively in mental health professionals. Now it is also found in sophisticated lay persons.
Pseudo False Positive DID – This presentation was common in the 1970’s and 1980’s and is now uncommon. In this case a patient would adopt the behaviour of a widely publicised or Hollywood movie type of case, one that is very flamboyant in appearance. The purpose of this was a desperate attempt to convince the clinician of the presence of DID , while the patient anticipated incredulity on the part of the clinician. Now that DID is accepted as a valid diagnosis, this presentation is rarely seen.
22 notes
·
View notes
Text
like an example of that is how people come away from the DID subculture online thinking there are certain ways to treat people with DID that aren’t actually applicable outside of that subculture. ive seen people claim that when you think someone with DID has switched, what you should do is introduce yourself again and ask them for their new name/pronouns. for me i think i would prefer when people noticed a switch or interference from a part if they made sure i was OK and safe, because usually that’s more caused by things like flashbacks or other posttraumatic symptoms/triggers. making sure you know how to refer to the new part is really not even close to the priority if that part is like, actively in a flashback or experiencing PTSD symptoms. if you tried to handle that situation based on the aforementioned Tips Online it might end kind of poorly.
15 notes
·
View notes
Text


PUBLIC INFO (things that anyone can know, or that he willingly tells people- most of which are lies lmao)
muska is a wanderer and enjoys going to historic places all over the world
he served in the welsh military and held the rank of colonel, but resigned due to overwhelming stress
he's currently 33, but held the aforementioned rank even at the age of 28
he suffers from posttraumatic stress due to his time in the military
he is a prodigy and is quite well rounded in his talents
he is second generation in wales and his family is from iran
he is fluent in multiple languages: farsi. english. cymric (welsh), gaelic. latin, and is conversational in french and german.
he's a terrifyingly accurate shot with long range weapons
SEMI-PUBLIC INFO (things that people can know if they are remotely observant, usually just because he does things, or that he'll tell someone if asked)
he likes inventing things and is a talented engineer
he is blind* (or at the very least legally blind)- whether or not this was from birth or not is up for debate, but he clearly compensates with other senses and certainly would not describe this as a disability- just a part of who he is.
he is skilled in swordplay
SEMI-PRIVATE INFO (things that only a few people know)
muska has bipolar affective disorder and has had at least one episode of mania.
he had a spouse who is now deceased
PRIVATE INFO (things muska just might take with him to the grave... or things that he'd never bring up ever and the only people who know EXPERIENCED THIS firsthand)
muska is "ramuska šâh" the king of kings
he has lived 4000 years and hasn't actually aged past 33 for all that time
he is the last pureblood of the laputians and gains all the benefits and downsides of being a god of the heavens created from the earth itself-
his first language is the celestial language
that deceased spouse that few people know about? her first name is anahita, but she's been reincarnated many times as many different people. he's loved and lost her many times
he had three children: parisa, minu, and eshan- while he was king of laputa
he was actually a government spy... and he's still willing to do work as a spy if the right people find him... he's very good at that
#𝙝𝙞𝙨 𝙡𝙚𝙜𝙚𝙣𝙙 𝙞𝙨 𝙬𝙧𝙞𝙩𝙩𝙚𝙣 𝙞𝙣 𝙩𝙝𝙚 𝙨𝙩𝙖𝙧𝙨! —— * the ichor laced corpse of eternity#this is for his mainverse but basically just change the names of places and its for everything
6 notes
·
View notes
Text
Rose Relationship Revolution Pt 2
I would argue that most of us spend a good portion of our lives learning how to have a peaceful relationship with ourselves. Life under colonialist capitalism is inherently traumatizing.
One of the best books I’ve read on complex PTSD and its physiological ramifications is Dr. Bessel Van Der Kolk’s “The Body Keeps the Score” published in 2014. I read it in 2019 and it catapulted me into a hard close look at my own lived experience as an autistic woman who experienced emotional abuse, sexual abuse, medical negligence, religious abuse, and extreme poverty in my childhood.
Before reading this book, I had never heard the term complex PTSD.
The book reads:
"Trauma, by definition, is unbearable and intolerable.
It takes tremendous energy to keep functioning while carrying the memory of terror, and the shame of utter weakness and vulnerability.
While we all want to move beyond trauma, the part of our brain that is devoted to ensuring our survival (deep down below our rational brain) is not very good at denial. Long after a traumatic experience is over, it may be reactivated at the slightest hint of danger and mobilize disturbed brain circuits and secrete massive amounts of stress hormones.
This precipitates unpleasant emotions, intense physical sensations, and impulsive and aggressive actions. These posttraumatic reactions feel incomprehensible and overwhelming.
Feeling out of control, survivors of trauma often begin to fear that they are damaged to the core and beyond redemption.
Research has revealed that trauma produces actual physiological changes, including a recalibration of the brain’s alarm system, an increase in stress hormone activity, and alterations in the system that filters relevant information from the irrelevant.
We now know that trauma compromises the brain area that communicates the physical, embodied feeling of being alive.
These changes explain why traumatized individuals become hypervigilant to threat at the expense of spontaneously engaging in their day-to-day lives.
They also help us understand why traumatized people so often keep repeating the same problems and have such trouble learning from experience.
We now know that their behaviors are not the result of moral failures or signs of lack of willpower or bad character - they are caused by actual changes in the brain."
Over the next few posts I’ll be reviewing more of what I learned from this book and I encourage anyone who has been captured by the quotes I’ve shared to purchase or borrow the book for themselves.
Thanks for joining me on this discovery process. Love you guys.
10 notes
·
View notes
Last Seen Blogs

arizuume
Clowntown is colder in the summertime (•ˇ●ˇ•)
sticksandsharks
STICKS&SHΔRKS

lyut21leo-blog
I'm a dreamer I love September Mourning #adommy

mangocovid
Goddess of Destruction

suburbanrelapse-moved
MOVED