#attending
Text

Hreinn Fridfinnsson: Attending (1973)
19K notes
·
View notes
Text


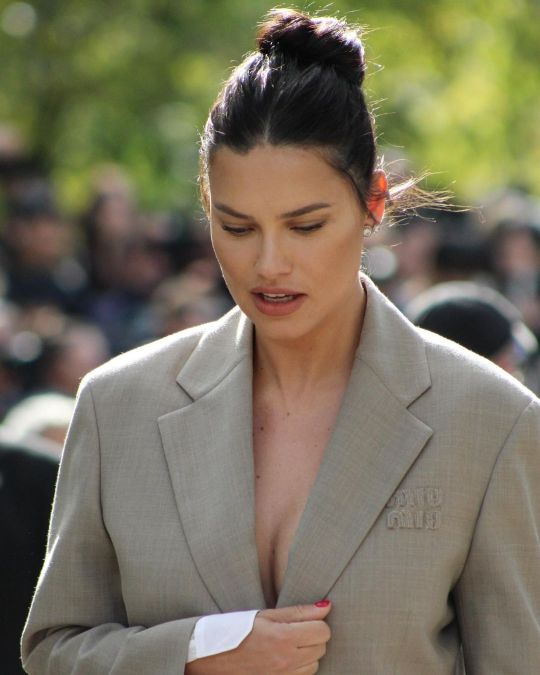
Adriana Lima attending the Miu Miu spring summer 2024 fashion show, PFW, Paris, France, 3/10/23.
#Adriana Lima#miu miu#spring summer#2024#fashion show#attending#pfw#paris#france#goddess#angel#gorgeous#2023
66 notes
·
View notes
Text
"That patient you signed out to me? She coded and died."
The worst type of text you can get in medicine.
These words have been haunting me these past few weeks. They'll pop into my head at the strangest times. I think about that case a lot. About what we could have done differently.
Our attending assured us that whatever had been the cause of death, there was no way we could have caught it. The presentation was just too...atypical.
But I can't help but wonder: what if I'd asked different questions? Or the same questions differently? Would I have gone down the right track? What if she came in a little sooner, would she be okay now? What if my workup had been more broad, would I have stumbled across the diagnosis?
What if... what if...
#medicine#emergency medicine#personal#residency#sign outs#co-residents#attending#medical stories#patient doctor stories
6 notes
·
View notes
Text
On Being an Attending (hey look Ma I made it!)
Somehow, after four years of college, four years of medical school, three years of residency, one year of chief residency, and three long years of fellowship, I have finally made it to this point—I am now an attending!
And I am freaking out.
What I previously thought of as the finish line, I now realize is just the starting line. Yeah, tell that to your 15 years of hard work. But as I sit here on my last day of freedom, ready to start my first real job tomorrow, I have so many conflicting thoughts and emotions.
First off, I took a glorious two-month break between fellowship and starting my job. Everyone recommends taking some kind of break, given this is the first and likely only time you will have a vacation with no clinical or academic obligations. And though I don’t regret this time off, I also feel like I have forgotten every ounce of pediatric cardiology that was previously cemented in my brain over the last three years. I sometimes catch myself in the shower or while I’m brushing, just rehearsing, “Hi, I’m Dr. Misra, it’s so nice to meet you. What brings you guys in today?” as if I have completely forgotten how to talk to patients. I recently google image searched basic echo views to test myself on something I could do in my sleep, just two months ago.
I know I’m being irrational, and I probably felt this way after every small break I had in the different steps of my medical training, but now my medical knowledge counts more than it ever has, and this insecurity is definitely at the forefront. I hope everything is just muscle memory and I’m sure it will come back to me as I get thrown in different clinical situations. But I do worry that the small nuances I knew about subtle echo and EKG findings are now lost to the abyss of my scattered and nervous brain.
As a senior fellow, you feel like you are the top of the highest totem pole. Junior fellows come to you for advice and help, attendings give you independence and back it up with, “well, you’re going to be an attending in a few months so…” and you feel you have earned the right to speak openly with unbridled confidence about your management decisions and clinical reasoning. By this point, you have become an expert at being a trainee—it is, after all, what you have been doing for almost half your time on Earth.
And now, you are placed in an entirely new role with new responsibilities and all that glorious confidence has vanished. You go from feeling like you are at your prime, to all of a sudden feeling like a newborn babe in this field. Right at the cusp of starting, what feels like, the most important step in your career.
This rapid fall from grace brings me to my next anxiety—I don’t want to look or sound stupid. When I interviewed for this job as a third-year fellow, I was confident in what I knew, what I wanted from a career, and just overall felt confident in myself. I currently no longer feel that way, but I want to do myself and my skills justice as the person they hired, and the potential they saw in me. I know I will need to ask for help throughout my career, and am not afraid to do so, but what if I ask stupid questions that I should clearly know the answer to? The need to impress others is deeply ingrained in me from years of medical training, and the fear of looking or sounding dumb has always been a huge motivation to keep learning and getting better. That may be morally incorrect, and I sincerely hope that as I grow and mature my motivation takes on more genuine and pure reasons, but this is the sad reality of medical trainees. And right now, as I start my career as an attending, that external motivation has never been stronger.
And then there’s the weight of your clinical decision making, and the responsibility you have to your patients and team. The buck stops with you now. Yes, you will always have help and resources, but now your decisions matter, you have the final say in what happens with your patients, and that safety net is gone. What you diagnose, and what you miss, is all on you.
The imposter syndrome is real folks. All of a sudden, I’m supposed to teach and speak with confidence about clinical matters I’ve had limited experience with, and have full assurance in what I am doing even though inside I feel like I’m going to pee my pants. People will look to you, as the attending, for answers and next steps, even though you just graduated, and were looking to others just a few months ago. I know I’ve experienced this imposter syndrome when I become a resident, and again as a fellow, but this time it feels profound and with bigger implications.
I’m sure in the beginning I will over-order clinical tests, over diagnose, and be extremely conservative with my treatment plans, for fear of missing something or messing up. I want desperately to just assume that cool confidence I had in clinic as a senior fellow, seamlessly handling a full patient load independently, reading echos and finishing notes on time, feeling great in my own skin, and portraying that put-together doctor that everyone wants for their kid. I know I will get there eventually—it’s in me, it always has been, and I can do it again—but getting there will take time. There will be the clumsiness with the new EMR, the awkwardness with navigating a new team, and learning the flow of a new clinic and my place within it. Compound that with the mental gymnastics of balancing the weight of new responsibilities, and you have the perfect set up for an anxious but eager young attending who just wants to impress everyone and never make any mistakes. It’s like wearing a neon sign that says, “I promise I am a badass, no you didn’t hire the wrong person. Just give me a second, I’ll get there again.”
But wanting to be perfect is unrealistic and I know it. And no one is expecting perfection from me except me. And all of this is just another growing pain in my journey through medicine. And I’m sure all these anxieties are necessary to being a caring doctor who is always willing to do and be better for their patients. I’m sure everyone who has been in this position has felt this way, and all those in the future will feel it too.
I’m nervous as hell, but I’m excited too. This is what I’ve always wanted, and there are so many opportunities and adventures that are in my future. I just have to keep reminding myself that this is the first step of many in my career, and to take time to appreciate everything that has led up to this point. I may never be ready for tomorrow, but whatever comes I will fake it till I make it, and keep pushing.
2 notes
·
View notes
Text
I've decided I really like, as an attendant, when people have dedicated fodder names cuz my brain will register the dragon name faster than the username (usually because fodder names are actual names, and usernames are just a series of letters and numbers when you have dyslexia) and it makes it easier to keep track of things.
I especially like when they are things like "pogworm" and "gaysquidward"
4 notes
·
View notes
Text
Local politics at the new City Hall

#American dad#gif#flag#flag waving#town hall#meeting#meet#the smiths#house#attend#attending#politics#local politics
2 notes
·
View notes
Text
my university having the dracula daily guy as a guest speaker is so funny
52K notes
·
View notes
Note
As a doctor, do you have any hygiene tips you think most people could use hearing? Like things people seem to neglect or do wrong that pop up and cause problems? Thanks!
EARS. Earwax is genetically determined. Some people get dry, scant earwax and others get wet, copious earwax. The biggest mistake I see is relying on Q-tips. Every time you stimulate the inside of your ear canal it makes your ears go “oh shit, there’s a threat! I better make more protective wax!” and next thing you know you’ve managed to jam a bunch of wax you told you ears to make back up against your ear drums and you can’t hear as well. Don’t rely on Q-tips. When you’re in the shower, let warm water run in, mush it around by pushing on your tragus (the cartilage flap in front of the canal), and let it drain. Repeat. Blot dry your ears with the edge of a towel or a Kleenex or something afterwards. If you tend to get really stubborn wax, use Debrox drops once or twice a week.
And vaginas. They’re mucus membranes once you get past the labia majora! You wouldn’t soap the inside of your mouth, don’t soap your vagina! It’s a self cleaning oven and if it smells weird GO SEE A MEDICAL PROVIDER because over the counter shit probably isn’t the right answer.
Dandruff isn’t because your scalp is dry. It’s because of a microorganism called malassezia furfur. It eats scalp oils. Dandruff shampoos mostly work pretty well.
Those are the three I can think of off the top of my head. Never use Irish Spring soap! It’s so heavily fragranced it’s a contact dermatitis waiting to happen! I once had a guy develop full body itching and I was JOKING when I said “what, did you just switch to Irish Spring?” and from then until he died he was convinced I was a witch because I was RIGHT.
28K notes
·
View notes
Text
I just wanna say bc I KNOW you're somewhere on tumblr, to the teenage girl who attended Take Your Kid To Work Day at an office building in Ontario, Canada circa 2013 and had a conversation with a middle aged woman in which you showed her your Black Veil Brides fanart and fanfics and ship content and told her about different fanfic tropes including a/b/o verse bc she happened to know who Panic! at The Disco and Fallout Boy were and thus you felt the need to show her your bandblr ship art, that was my fucking mother and I had to clarify all that to her including looking my mother in the eye and trying to explain a/b/o verse without sounding like a lunatic.
It's been 10 years and I still regularly sent evil energies in your direction. Since you'd be probably two years younger than me and thus legally an adult now, please know if this post reaches you it's on sight.
#she cornered me in the car and asked what shipping was and i almost had a fucking heart attack#imagine being like 16 years old and habing to explain knotting to your mother#random emo music girl I'm glad you had fun talking about your Band Guys to my mother#bc i also attended take your kid to work day at that office and i know how boring it was#but christ alive why did you have to fuck me like that?#anyways i hope this post reaches you so at the very least you know i think about you at least once a week#this has been weighing on me for ten years#im almost tempted to blaze this post
60K notes
·
View notes
Photo




*Married life playing in the background
This idea was probably funnier in my head
#sansmaeda#sansmaeda wedding#undertale#danganronpa#nagito komaeda#sans undertale#meme post#I swear there's a reason why not everyone attended in nagito's side#no one wanted to go in the first place#sdr2#fanart#so for the record:#Ibuki DID attend but could't stay put for 5 minutes so she got bored and left#Teruteru is still pretty angry and bitter at Nagito#Hiyoko couldn't care less and thought it was gross#Akane saw no reason to go since her main source of food wouldn't go (Teruteru)#And spoiler alert but Chiaki's fucking dead lmao#she would've gone tho#probably#Also pretend nagito's using really good foundation on his hand cuz I totally forgot about his metal arm
86K notes
·
View notes
Text
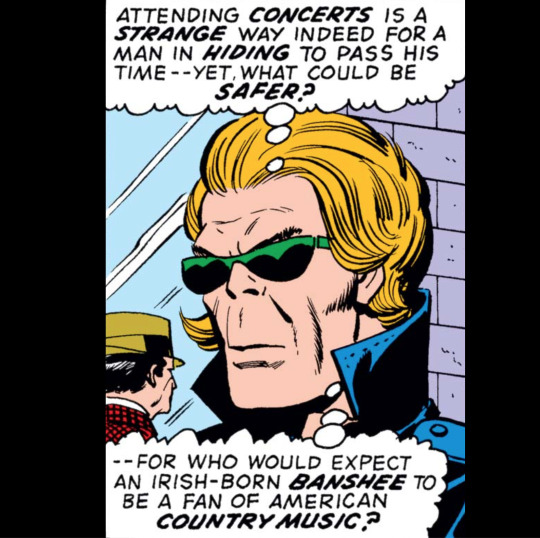
Captain America & Falcon #172
April 1, 1974
#attending concerts#attending#concerts#a strange way#a way#way#in hiding#pass the time#what could be safer#safer#who would expect#a fan#country music#music
0 notes
Text




mayvisuals_
#Adriana Lima#instagram#miu miu#spring summer#2024#fashion show#attending#pfw#paris#france#goddess#angel#gorgeous#2023
22 notes
·
View notes
Text
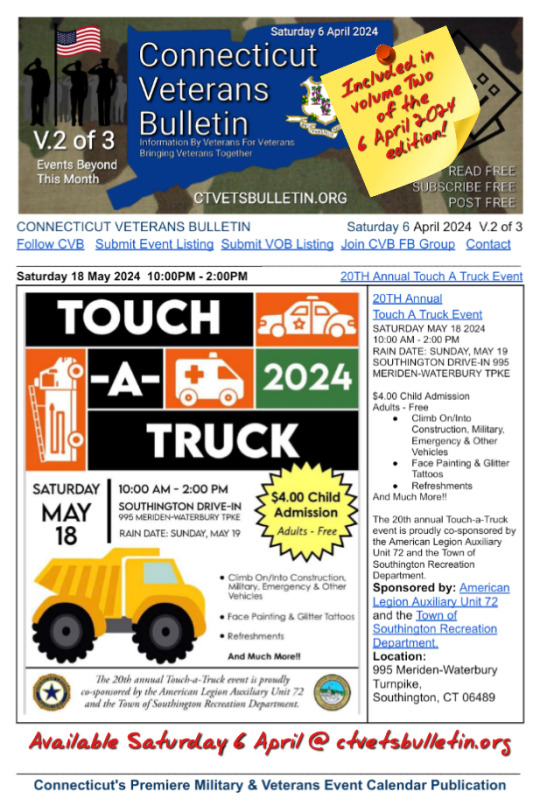
A sampling of Over 200 Veterans Events Included in the 6 April 2024 edition of CVB's Weekly Connecticut Veterans Calendar Publication.
Thursday 4 April 2024 7:00AM
Available at ctveteransbulletin.org Saturday 6 April 2024
The following events are new additions to the CVB Connecticut Veterans Calendar Publication this week.
VFW Post 1523 Saturday Breakfast
VFW Post 1523 Saturday Breakfast
SATURDAY MORNING
9 AM TO 11 AM
APRIL 6TH, 2024
BREAKFAST INCLUDES
SCRAMBLED EGGS
SAUSAGE
BACON
HOMEFRIES
TOAST
PANCACKES
JUICE…
View On WordPress
#ctvetsbulletin#10004#20th Annual Touch A Truck Event#American Legion Auxiliary Unit 19#American Legion Post 10 Veteran&039;s Service Day#American Legion Comedy Night#Annual RF&G Veterans Committee Picnic/BBQ#attending#Blessing of the Bikes In The Memory of Fallen Veterans#Breakfast buffet at the Morgan-Weir American Legion Post 27#Events for veterans in Connecticut#Veterans event calendar#VETERANS OF FOREIGN WARS JEWETT CITY CONNECTICUT POST 10004#VFW Post & Aux 1523 Present Stone County Band#VFW Post 1523 Saturday Breakfast#VFW Post 1523 Sunday Monster Meat Raffle
0 notes
Text
President Tatar: “The isolation imposed on Turkish Cypriots should be lifted”
TRNC President Ersin Tatar attended the 2nd. Global Destination Exchange Forum in the German capital Berlin.
Continue reading President Tatar: “The isolation imposed on Turkish Cypriots should be lifted”

View On WordPress
#2nd. Global Destination Exchange Forum#Attending#Berlin#Briefing#Cyprus 2 state solution#Frankfurter Allgemeine newspaper.#German capital#TRNC President Ersin Tatar
0 notes
Text


first set of fnaf ruin fanart guys we are back
#fnaf ruin spoilers#oh please dont take this joke seriously btw#cw strong language#fnaf ruin#fnaf sb dlc#fnaf sb ruin#fnaf security breach#fnaf sb#eclipse ruin#dca#fnaf daycare attendant#eclipse fnaf#moon fnaf#sun fnaf#moondrop#sundrop#fnaf#five nights at freddy's#fnaf fanart#fnaf sb cassie#roxanne wolf
38K notes
·
View notes
Text
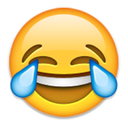
FNAF movie Mike fights Moon at the Pizzaplex..
#myart#chloesimagination#comic#mike schmidt#fnaf moon#moondrop#fnaf daycare attendant#fnaf#fnaf movie#security breach#fnaf fanart#five nights at freddy's#what a crazy fight that was.. does moon win or lose here? both?#moon is baffled bamboozled even flabbergasted#my man wasn’t prepared for someone to be that happy to sleep#didn’t even get to use his magic on him#Mike just took himself out slept on command#officially Mike likes moon just cause he’s an excuse to eepy
9K notes
·
View notes
Last Seen Blogs

aivantheshadow
Moonchild

elibooy
I want to die.

saltylikecrait
Salty Like Crait

orangesalamander-but-studying
helianthus
funny-relatable
True To You And True To Your Heart