#cardiology
Text
What do you do on your day off they asked
Nothing she replied as she turned another page
#doctors of tumblr#medicine#studybuddy#studywithme#studyspo#studygram#cardiology#study studyblr#study#studyblr#bookstore#bookworm#bookishaesthetic#bookaholic#booktok#bookcafe
472 notes
·
View notes
Text

heart from my embalming class
#i didn’t take this image it was just in a powerpoint but i love the heart so much#heart#human heart#cardiology#human anatomy#biology#surgical anatomy
96 notes
·
View notes
Text
So I've discovered something interesting.
I've had a hypothesis for a while now that everyone's heart sounds different because they are different, but I'd always assumed that most heartbeats sound semi-alike and I wouldn't be able to hear all the differences until I had appropriate training. (I'm pre-med.)
Well, yesterday I stumbled upon a YT short of a sound designer who needed to record some heartbeat foley and just used her coworkers (LOL). And not only can you tell the difference right off the bat, but the heartbeat fits the person perfectly. I couldn't tell you why or how, but it just does? Granted, she had really high-res equipment, but apparently, hearts have no interest whatsoever in sounding the same. The generic heartbeat sound we think of is the tip of the iceberg. No one's heart is exactly that. It's so much more.
But yeah, hypothesis officially confirmed. That's awesome.
#premed#hearts#heartbeats#cardiology#medicine#idk it's just really cool to me#it actually made me a bit giddy lol#anatomy is so cool guys
287 notes
·
View notes
Text

-Um, Tae? Is it really necessary for me to wear it?
-Come on, Sae. This whole Phantom Thieves case got you on the edge of your health. You look exhausted. I need to know, if your heart is working correctly. This kind of stress can give you huge problems. You don't want Makoto to give you CPR, right? I need to know if you don't have any Long QTs.
-Ugh, if you say so...
-Besides Sae, you look cute in this one. Imagine, heart is a beautiful part of your body. All the electricity gathered there. Doesn't it make you fell love? *wink wink*
PS: I am dumb. I forgot to give credit to original creator.
Original creator: Tommy AKA Kingdukeee
Source: https://danbooru.donmai.us/posts/4967242
#sae niijima#persona 5#heart#ekg#holter#holter monitor#ecg#ekg test#ecg test#female ekg#female ecg#cardiology
108 notes
·
View notes
Text
Maude Abbott

Dr. Maude Abbott was born in 1868 in St. Andrews East, Quebec. Dr. Abbott graduated from McGill University, but was not allowed to study medicine there because of her gender. She ultimately received her medical degree from Bishop's College in 1894. Dr. Abbott is remembered for her contributions to the field of cardiology. She wrote about roughly 1,000 heart anomalies over the course of twenty years. Dr. Abbott's 1936 Book, Atlas of Congenital Cardiac Disease, paved the way for modern heart surgery. She also served as curator of McGill University's medical museum, where she devised a classification system for uncatalogued medical specimens.
Dr. Maude Abbott died in 1940 at the age of 72.
Image source
#medicine#women in medicine#doctors#science#scientists#women in stem#cardiology#canada#canadian#quebec#women's history
46 notes
·
View notes
Text
“What a stress test is for the heart, pregnancy is for the pancreas.”
About gestational diabetes.
60 notes
·
View notes
Text
Hearts are awesome


Just look at that thing go. Hardworking lil guy, never taking a nap. You go, Glen Coco.
And the coolest part, if you’re reading this, you have this thing inside you.
Yes, I’m studying g cardiac anatomy, why?
39 notes
·
View notes
Text

resting the eyes
95 notes
·
View notes
Text

🥼🩺
#hospital#practice#medicine#med Student#scrubs#july#medicine student#veterinary medicine#vet med student#clinical medicine#laboratory#laboratory medicine#women in medicine#women in science#me#personal stuff#pandora bracelet#cardiology#surgery#surgeon#cardiologist#heart pin#van Gogh heart pin#love#bucharest#romania#brunette girls#brunette girl#beautiful#doctor
73 notes
·
View notes
Text
Ebstein Anomaly of the heart: a 2D echocardiogram in 4 chamber view showing atrialized right ventricle.
Patient was a 20 year old labourer who presented to us with swelling of feet, bluish discoloration of the entire body (cyanosis) and clubbed fingers.
Auscultation revealed an early systolic murmur at tricuspid area and gallop rhythm ( S3 )
Leading cause of Ebstein anomaly is maternal history of lithium intake!
#cardiologist#cardiology#cardiologyexperts#echocardiogram#echocardiography#medicine#medgram#med blog#studyblr#studygram
22 notes
·
View notes
Text

Hello!! I'm new to tumblr, I'm a young artist just putting my stuff out there, so here's an oil painting I did a couple months ago. This was a gift for a cardiovascular surgeon, she's very special to me and was very happy with the painting. I hope you like it too<3
#art#artwork#artists on tumblr#my art#original art#oil on canvas#oil painting#painting#human anatomy#anatomy#cardiology#anatomy art#medical art#<3#drawing#hand drawn
34 notes
·
View notes
Text
Embark on a journey with Jennifer Carlquist, PA-C, and course director of The Urgent Care EKG Course as she shares 12 essential insights for navigating through EKGs in the urgent care setting.
1. When a patient has an irregular rhythm, it is important to look closely for P waves. If they are the same shape and distance from the QRS complex, you could be dealing with sinus arrythmia. This is usually caused by breathing.
2. If you have a patient with palpitations, you may find a clue to the cause by asking the patient when the palpitations happen. Often, palpitations only occur when the patient is about to go to sleep which could be caused by anxiety, although this is a diagnosis of exclusion.
3. When you have a patient with tachycardia, make sure you can explain why. Pulmonary embolus can cause tachycardia and will not always be associated with an s1q3t3.
4. If you have a very short PR interval, the first thing you should look for is a delta wave. This is what you will see with Wolff-Parkinson-White syndrome, which can be fixed with an ablation.
5. If a patient has experienced a recent stressful event such as the death of a spouse and has new onset heart failure, consider Takotsubo cardiomyopathy. This can present a myriad of EKG findings, including STEMI.
6. PVCs are not always benign. They can lead to heart failure if there are enough of them.
7. There is always a reason for sinus tachycardia, while supraventricular tachycardia (SVT) comes on suddenly for no good reason. It’s hard sometimes to tell the difference between the two, but when you start to sort through the history, that’s where it really starts to make sense. Sinus tachycardia will have volume loss, fever, anemia, or anxiety, while SVT patients will usually have none of those. The exception would be if a patient has anxiety after they started feeling the SVT, which is a whole different story.
8. When interviewing a patient about their palpitations, it is always helpful to ask if they have anxiety as well. If they do, ask them which came first: the palpitations or the anxiety. If the anxiety came first, then it is most likely anxiety causing the palpitations, although this would be a diagnosis of exclusion. If the patient feels palpitations and then anxiety comes on, that’s more likely arrhythmia based.
9. It is impossible to diagnose Takotsubo cardiomyopathy from an EKG alone. There are many different presentations of the condition, including STEMI, nonspecific STT-wave changes, T wave, and inversions that are symmetric. If you have a patient with a classic story that involves recent major stress in their life, then absolutely consider this diagnosis. It can be seen during their angiogram, where it will look like apical ballooning, and they will have a reduced ejection fraction.
10. ST-segment elevation can be very minimal and still deadly. It is important when you are screening for ST elevation to look closely at the TP segment. This is the most isoelectric line, and this is where you should draw your line to see if there’s any elevation or depression. As little as 1 mm can be significant for STEMI in the inferior leaves, so it really does matter here. Get serial ECGs.
11. When looking at the intervals at the top of the EKG, one of the most important numbers to look at is the QTC. The QTC should be <460 ms to be normal in women and <450 ms in men. If it is longer than that, consider adjusting the patient’s QT-prolonging medication. We do not usually see Torsades de Pointes until they get >500 ms, but it’s still a good idea to minimize risk by getting the patient off any QT prolongers you can.
12. Torsades de Pointes is lethal and most likely stems from a prolonged QT. Unlike in VT, the treatment is magnesium, but prevention is always the key. Amiodarone can also prolong the QT and can be proarrhythmic, so you may have to choose a different drug in some cases.
This course is ideal for PAs and NPs practicing in urgent care. Whether you’re new to practice or have many years of experience, you’re sure to learn practical, evidence-based tips you can use on your next shift. You can sharpen your EKG interpretation skills, improve your accuracy, become more proficient, and boost your clinical confidence with The Urgent Care EKG Course.
Visit https://www.ebmedicine.net/ekg to learn more.
Even more content:
Check out one of our latest reels (less than one minute!) by Jennifer Carlquist, the course director.
18 notes
·
View notes
Text
Some volume and mass measurements

Finally went through the tedium of measuring masses and volumes. Annoyingly I did part of it wrong and only calculated RV total mass, instead of volumes, but i got the LV numbers at least.
My LV mass is 300g without papillary muscles. This puts my LVMi at 158g/m^2. For comparison, normal is 121g and 62g/m^2.
My LVEDV is 340ml and LVESV 154ml, so my stroke volume is 186ml. Normal is 103ml. Also fun side note, my heart empty (LVESV) is holding about the average amount of blood a regular person's heart holds when full. Makes sense with my earlier recording which put my chamber diameter in systole at 46mm or so, which is a fairly average wideness for most folks in diastole.
Anyway big heart is big. My total heart volume was 1009ml. My heart is holding in the volume of a 1 liter bottle.
47 notes
·
View notes
Text
Cardioverted someone today and I felt like a god. Pressing a button, stopping his heart then seeing it restart in the correct rhythm has got to be one of the coolest things I've done. Medicine is fricking awesome
301 notes
·
View notes
Text



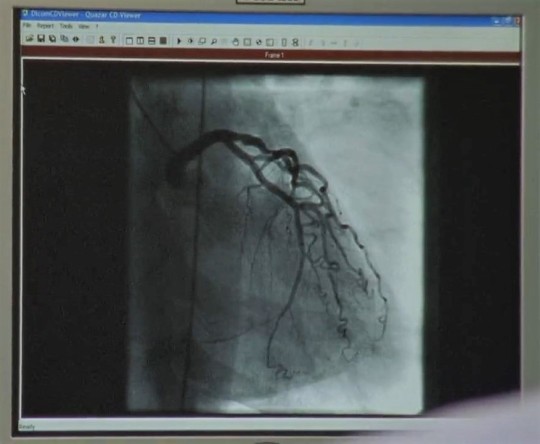
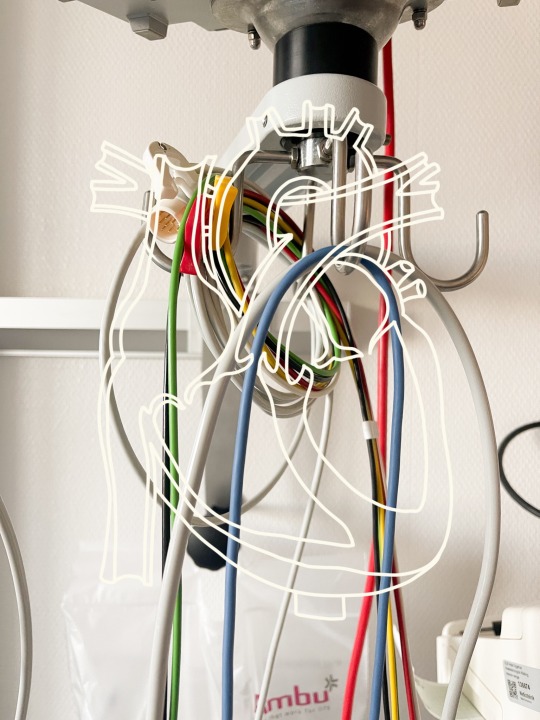
Bergdoktor s1 ep6 - cardiac catheterization
#female heartbeat#female patient#herz#heart#herzschlag#cardiophilia#heartbeat#cardiology#hospital#bouffant cap#electrodes
49 notes
·
View notes


Last Seen Blogs

hereformcdonaldshonestly
☽Mack's Writing☾

golden-jeon-jungkook
bts jung kook

council-of-tords
The Council of Tords stand ready

arteella
The Drawing Board