#child differentially diagnosed
Note
someone on twitter made a succession incest supercut and i was wondering if you had any thoughts on how articulations of incest shape the roys esp wrt roman. the op of that also remarked on how succession plays into the incestuous dimensions of aristocratic nobility which i thought was interesting.
yeah i wrote a bit about roman and incest specifically here. tl;dr: he has a negative oedipus complex, ie subconscious desire for the father, which is part of the show's overall suggestion that the structure of the family (because it is embedded within the structure of capitalism) inherently creates this type of desire and therefore also enables certain forms of abuse and violence. ie, roman's attraction to father figures, resulting from his unconscious desire for his own father, is not an aberration from the 'typical' functioning of the family, but a heightened expression of the parent-child relationship as it normatively exists. logan's possessiveness over roman's sexual desires and disgust at his body and effeminacy; roman's attraction to women his father finds attractive; the way logan tacitly relies on roman's flirtatiousness when sending him as an emissary to various powerful businessmen; roman's desire for gerri to repeat the sorts of insults his father uses against him in their sexual encounters, and roman eventually firing her when she can't look him in the eye and tell him he's as good as logan was: in all of these we can see how the patriarchal father is a role inherently defined by possession of the wife and children, stymieing the child's sense of identity and ability to differentiate himself from the parent.
in the case of logan and roman, of course, these dynamics are elevated, because this is tv and the writers are using their relationship to draw out the elements of violence and coercion that the father role inherently rests on; also, because logan uses his outrageous wealth and social power as tools against his children, as the other half of the critique here is in pointing out that the capitalist family is an economic arrangement first. logan's children have always existed to be employees, and on a broader level, reproduction is what capitalism uses the family for: it's the site at which a supply of new and able workers is to be ensured. so, the incestuous desires roman has for logan, and the way logan controls him and treats him as a combination of son-daughter-wife, is meant to tease out the way in which these elements are inherently always present in the family. there's no break here between the roys and 'normal' families; there's only a difference of intensity and degree of overtness.
similar analyses can and should be made for the other roy children. shiv and kendall have a patricidal drive that roman does not, and they both desire affection from caroline; roman, on the other hand, identifies with the wife role more, and thus has a degree of conviviality with caroline that shiv and kendall have never had access to. but there are incestuous elements to their relationships with logan as well, partly because in the show's discursive field, killing is always equivalent to fucking is always equivalent to succeeding, and partly through the degree of control and coercion that logan also uses with them. parental possessiveness (eg, the control logan exerts over kendall in s2, or his demands for shiv to perform affection for him publicly) frequently appears continuous with, or as a parallel to, abusive treatment of a spouse; think also of kendall taking on the role of managing logan's pills, or saying he doesn't know what he would be [good] for if not for logan. connor has been discarded much like his mother (presumably for sharing her non-noble bloodline and potentially, in logan's mind, her psychiatric diagnoses).
thus, in all of the relationships between logan and his children, we see how 1) parent-child is inherently a violent and coercive dynamic, and 2) specifically, the nature of the family as a contained sphere of capitalist production means that the child's psychosexual development occurs through the relationships to the parents, which inherently invites some degree of incestuous desire and abuse, and, given certain circumstances, can result in adult children who never move past these stages of development and retain their juvenile incestuous desires and fixations.
the way that the roys talk to one another frequently involves incestuous sub/text and sexually violent threats or metaphors. this accomplishes a few things. first, because their family is part of waystar, the violence that waystar perpetrates (the cruises scandal, the wolf pack, capitalism's broader ab/use of labourers' bodies) trickles down into the family's mode of communication as well. second, although they're not speaking literally when they talk like this, often they are expressing something emotionally true (ie, roman seeing 'getting fucked by dad' as a good thing tells us that roman sees himself as the bottom of the sexual and social hierarchy, that this position makes him vulnerable, and that he does still desire it, which again is because of his attraction to dominant father figures and hypermasculinity). third, again, it's part of how they convey that 'normal' capitalism is violent, 'normal' families are part of capitalist production and therefore also violent, and 'normal' family dynamics are pseudoincestuous (which, obviously, can and does elevate into literal physical incest).
and yes, there is also the incestuous dimension of aristocratic 'breeding' practices, which comes to the fore when matsson jokes that the roys are like the habsburgs, but also like "one of those incestuous family cookouts". in that line, he's playing off the fact that although the roys resemble a medieval or early modern royal dynasty in some ways, they're very much new money, and are insecure about this fact; he's suggesting that they're more like a 'backwater' rural incestuous family than the habsburgs, and that the habsburgs themselves were a bit gross and pathetic for their incestuous bloodline. this fits in with matsson's fixation on biological strength and fitness (his team is specifically young, stacked with olympic hopefuls and fulbright scholars; he flashes his abs to demonstrate his normatively 'correct' body in a business deal; even sending his blood and hair to ebba is specifically an intimidation tactic that doubles as a demonstration of his own strength and uses his body to subordinate his ex-girlfriend; he later calls greg "backwash in the shallow end of the gene pool"; all of this eugenic discourse is of course also contextualised by his racism / white nationalism, as shown in the line about "arabs in france").
but, outside of the context of matsson, i think the critique of the family is a more interesting use of incestuous subtext on succession, honestly. this is where the show actually does have something interesting to say in its typically snarky and satirical way. the family is not just continuous with capitalist production, but is a microcosm of it and a site on which capitalism articulates, and the inherently incestuous elements of the family are thus metonymic of larger structures of violence in capitalism. there is nothing perverse or abnormal about the roys; their abuse of one another, and their incestuous internal dynamics, are the expected outcome of normal capitalist functioning, specifically through the family unit.
115 notes
·
View notes
Text
Headcanons- John Price

Birthday, January 11, 1985
Early Life
Born in Hertfordshire
Only Child, his mother (Mary) had him at 16. He never knew his father
His mother was a barmaid who struggled on and off with substance abuse issues throughout his childhood. His grandmother died before he was born, so he was mostly raised by his Grandfather.
Full name is Jonathan Michael Price Junior, after his maternal Grandfather, not his father.
As a child he only ever went by John to differentiate himself from Johnathan, who was well known as an accomplished hunter in the area. The name stuck into his enlistment, though.
Jonathan was a Captain during WWII, only married once, had three children including his youngest, Mary
Devout Anglican, Price is thus probably the most religious of the 141
Grew up hunting and tracking game on his Grandfather’s property, which he inherited and still owns.
While he specializes in tracking, does and has always preferred fishing to hunting. Mostly because he finds cleaning and gutting fish less annoying and gross than cleaning and gutting game.
Still hunts occasionally.
Has a small collection of antique lures in his office.
Was an alright student throughout school, but he dropped out at 16 to pursue the stability of a military career.
Got married at 19 to a girl from his village, trying to follow in his grandfather’s footsteps, divorced at 22 when he discovered she was cheating while he was deployed
Has an irrational fear that the ex-wife hid a possible child from him
She stopped collecting alimony payments three or so years after the divorce. The ruling was reversed in court. Hasn’t seen her since he was 25.
His greatest regret in life is that he wasn’t around for his grandfather in his final days. He was deployed when Johnathan was diagnosed, and died, from Leukemia.
General
Originally started smoking cigars to try and cut back on his cigarette-smoking habit, did not really work.
Was first gifted his preferred cigars, Maduro, by his first Captain, Captain Macmillan after he gained the rank of Lieutenant.
He has a box of limited edition, 2016 anniversary Maduros he intends on giving Soap once he becomes a Lieutenant to keep the tradition alive.
A pretty good cook; hates baking though. Has a natural talent for throwing flavor profiles together, and he can turn rations into something really special with foraged ingredients in the field.
HATES takeout, HATES eating out, and would much rather make himself a shitty home cooked meal than have anyone else cook for him.
The only exception to this is cafes, he enjoys the occasional pastry + newspaper ambiance when he has downtime.
Actually prefers coffee to tea, but is very particular about his coffee. He also has coffee more frequently in the field so he will opt to make tea when at home/ordering at a cafe
Can pair any meal with a cocktail, even if he has to invent the cocktail himself.
Generally very good when it comes to flavor, except he has the cilantro soap gene. His spice tolerance is mild at best.
Originally grew out his beard to hide/cover rosacea and acne scars
Has since gotten over this insecurity, now just has the beard because he vastly prefers his face with it
Actually has a master's degree in teaching, whenever he gets leave off he takes a couple of classes at a local college
If he is ever forced to retire from the military, he intends on becoming a history teacher
When he’s home, which is very infrequent, he regularly volunteers with his church at various pantries and soup kitchens.
Frequently passed up for promotion because he can, will, and frequently does, bend the rules.
When it comes to reprimanding, he’s the worst out of the bunch. He’s not above screaming and spitting in a private’s face to get them scared shitless.
It’s not because he’s a shitty guy, it’s because he’s seen too many good soldiers die over stupid mistakes to tolerate them.
Likes romcoms and nature documentaries.
The muppet insult originated because he got told he couldn't say "fuckwit" to subordinates and "muppet" has a similar mouth feel to "fuckwit."
Price does not want children or to get married. He is married to his work in a lot of ways, he would have to feel a very very very special way about someone to put them into the danger of his job.
Conversely, Price is absolutely the most likely of the 141 to have a secret family somewhere.
Price’s most toxic trait is that he can justify anything. If he thinks it’s worth the mission, God himself could not sway Price away from it. Genuinely believes he’s doing it for the greater good. If it’s not for the greater good, he's not bothering with it. Price would commit an awful war crime and not blink twice about it if he thought it would further humanity (Oh original timeline Captain Price, you evil-for-the-sake-of-good bastard.)
Talents, special bonds, ETC
Originally took a partial interest in Soap because he reminded Price of a friend he had way back in his private days when he worked alongside Declan O’Conor
She was a sniper from the US
He was given Simon and Gary from her company when they were both sergeants and later sent Gaz to get trained by her to be a sniper.
She now only trains soldiers and is technically retired from active duty because of severe combat injuries.
Considers her something of a guardian angel because her overwatch kept him alive through so much tough shit.
His waterproof and windproof lighter was originally hers, but he used it so frequently that she sort of stopped asking for it back.
To this day, this old friend of his is the only person he lets touch his lighter or light his cigars beside Nikolai. Considers it his good luck charm and is superstitious about it.
Visits her in the US whenever he’s around, and gives her updates on Ghost and Roach when he can.
The relationship is purely platonic, but Simon still gives him shit about “His Girlfriend”
Has the innate ability to “smell when water is about to boil.” Gaz and Soap do not believe him, they think he has a water to heat time table memorized or something. Ghost does not understand it, but he’s seen Price leave water unattended until the very second it's about to boil over too many times to refute his claim
Genuinely believes that Declan O’Conor was KIA, and harbors a lot of guilt over that. In his mind, he was not there to help his friend when he was on a solo mission that killed him. If he ever found out O’Conor was still alive he would be very upset/feel betrayed
Has few close relationships outside of the military, but they include:
Kate Laswell and her wife, he gets along really well with Kate’s wife, to the point that Kate often feels left out when he’s around (again, purely platonic, queer women just love this man)
Nikolai. The two have boned. Are they FWB? Are they soulmates? Are they gay married? No clue, but its the truth.
US friend. Has a standing agreement to marry her should either of them require marital status for something like healthcare
Is the woman he lost the pissing contest to
She calls him “Johnny Cash”
Gaz hates being around them because they act worse like a married couple than Price and Nikolai, which is bad enough.
Their relationship is very reminiscent of Soap and Ghost, where Ghost is Price and the friend is Soap.
Price refuses to introduce her to Soap because Ghost made him promise never to (he knows she’s got hella embarrassing stories about him and fears what energy having the two in the same room would create.)
His cousins. Is not super close with his uncles, but grew up around the same time as their kids so he is pretty close with them. Considers their kids his nieces and nephews.
Specialty!! How he views the mainline 141 boys!
He sees Soap as a protege specifically because he believes he can train him out of his more impulsive habits, in a sort of sick and twisted way, Price knows that Soap will eventually lose his FNG outlook and he wants to be there to direct him out of it when he does-- Just like Macmillan did to him.
He sees Gaz as a soldier because Gaz is already so established in his skillsets that Price sort of thinks "Can't teach an old dog new tricks." He knows that Gaz is damn good at what he does and is not impulsive/explosive enough to make it to where Price has, but there is no one he would rather have under his command. He trusts Gaz's moral judgement the most out of the group and absolutely favors him for it, whether or not he would admit to it.
He sees Ghost as sort of a lateral officer. For better or for worse, Simon Riley is dead, and Price is haunted by his Ghost for that reason. He harbors an immense amount of guilt for not being able to save Simon so he keeps Ghost on a loose leash. Price sees Ghost as sort of a tragic guard dog, too feral and traumatized to be anything more but still fearsome and worthy of love and respect.
70 notes
·
View notes
Text
If you ever wondered why adults with autism often get “missed” and then have such piss poor access to resources after seeking diagnosis, let me present to you search results from UpToDate (a top site for medical professionals to look up clinical information and evidence based treatment guidelines):
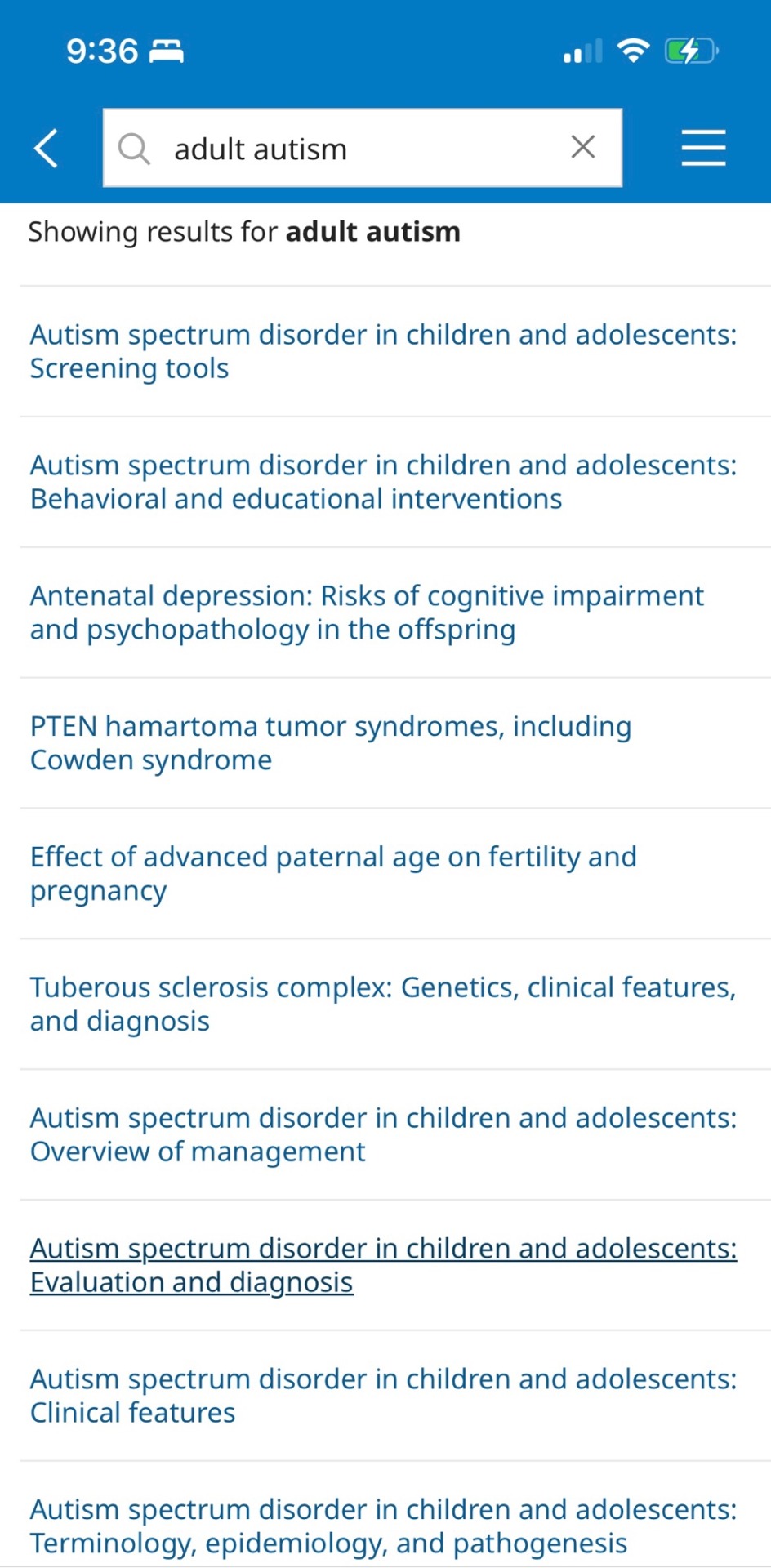
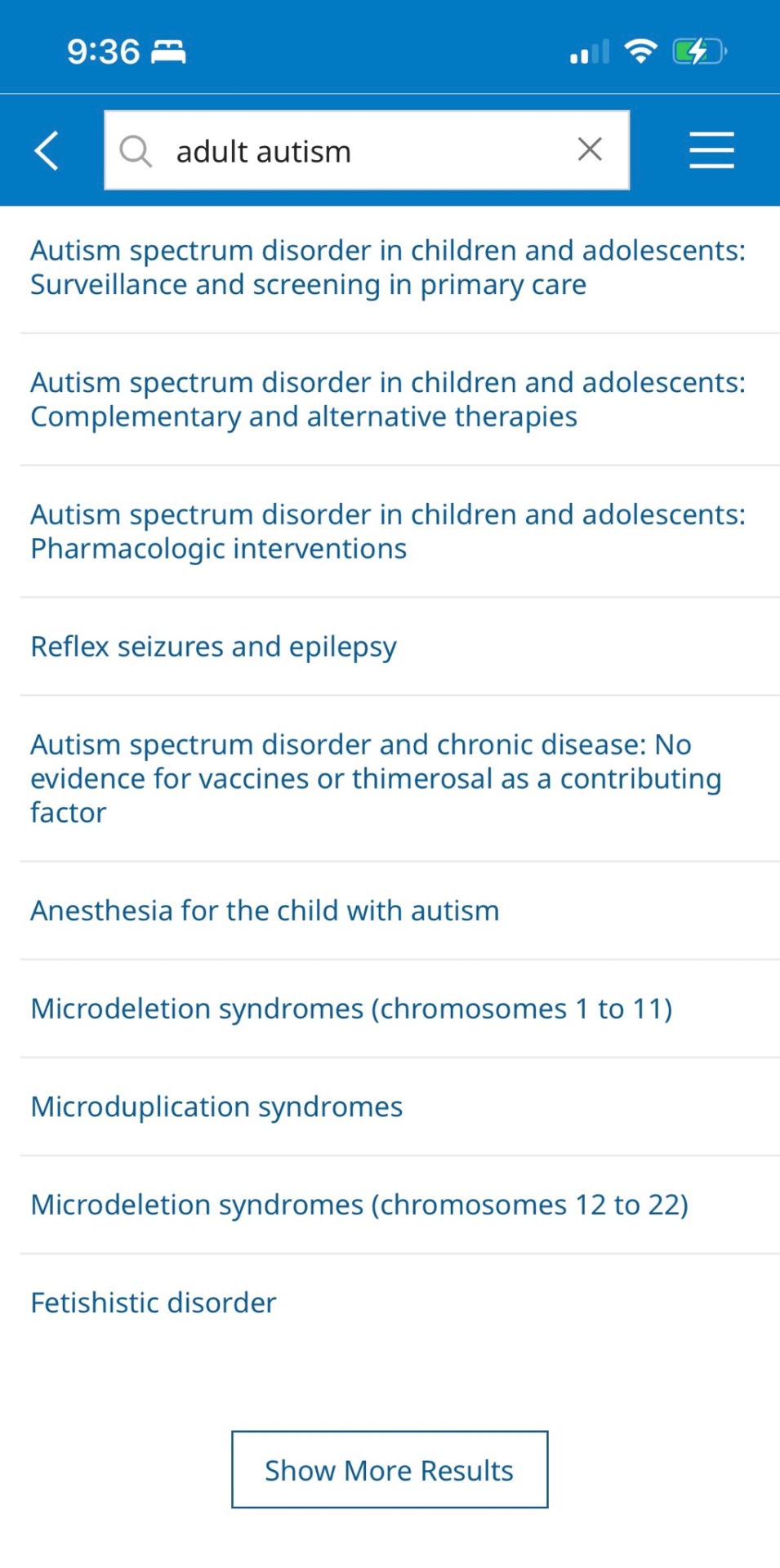
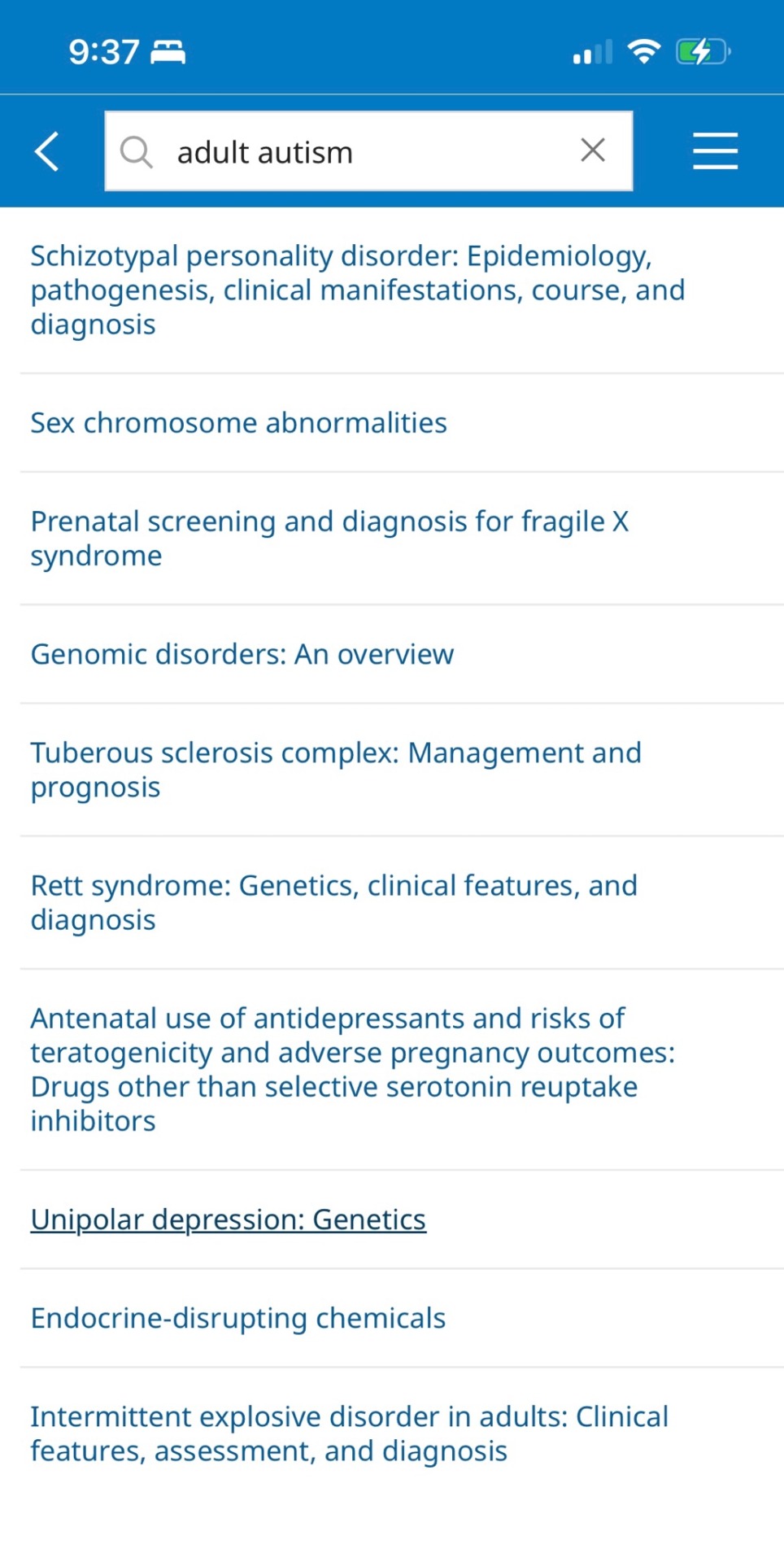
Note how not one of these is specific to adults. Despite the adult search keyword, results are skewed to child and adolescent information, genetic diseases/syndromes, and other psychiatric conditions (may be comorbid, may be differential diagnoses).
When you look at society guidelines related to autism:
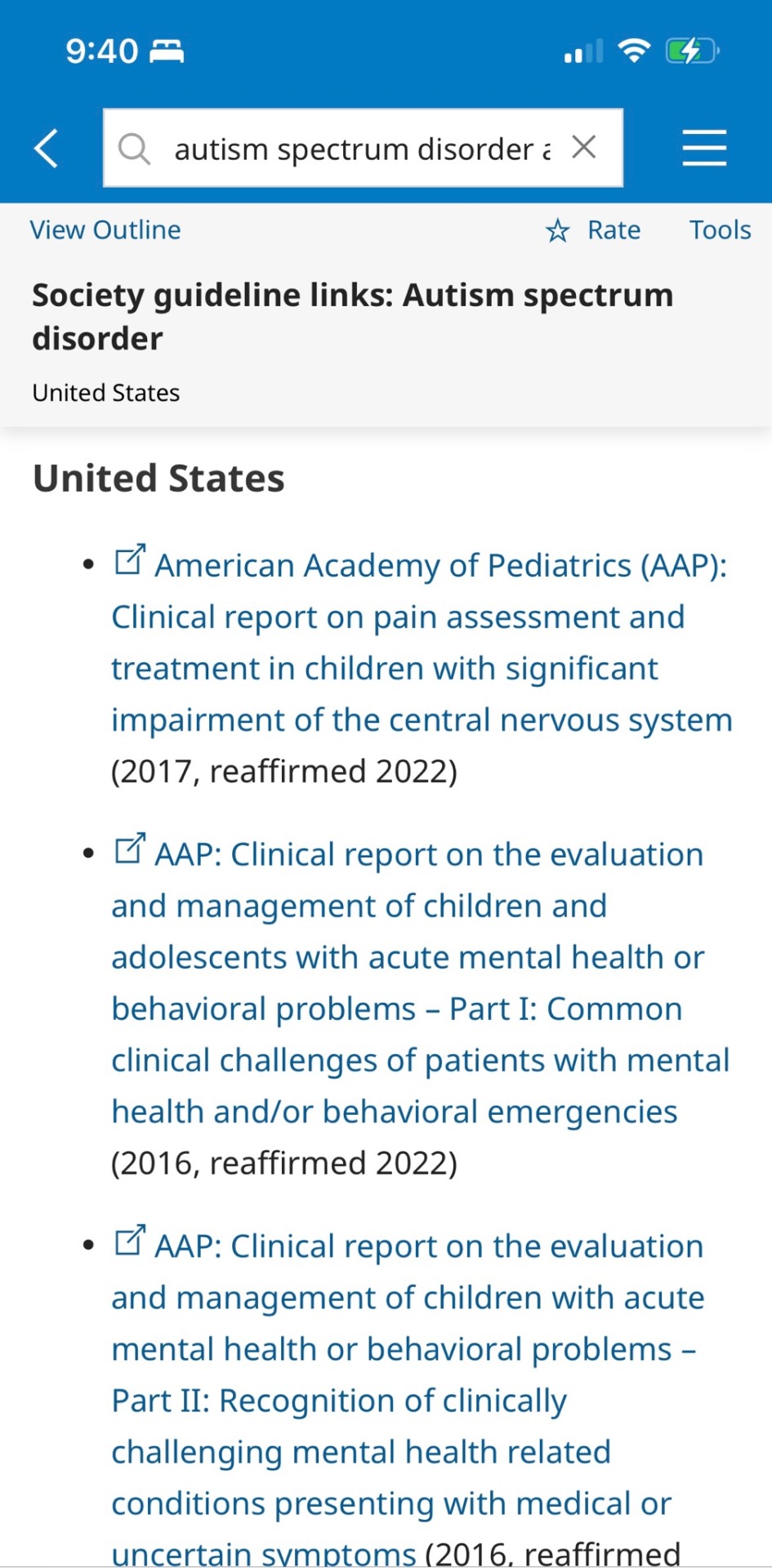
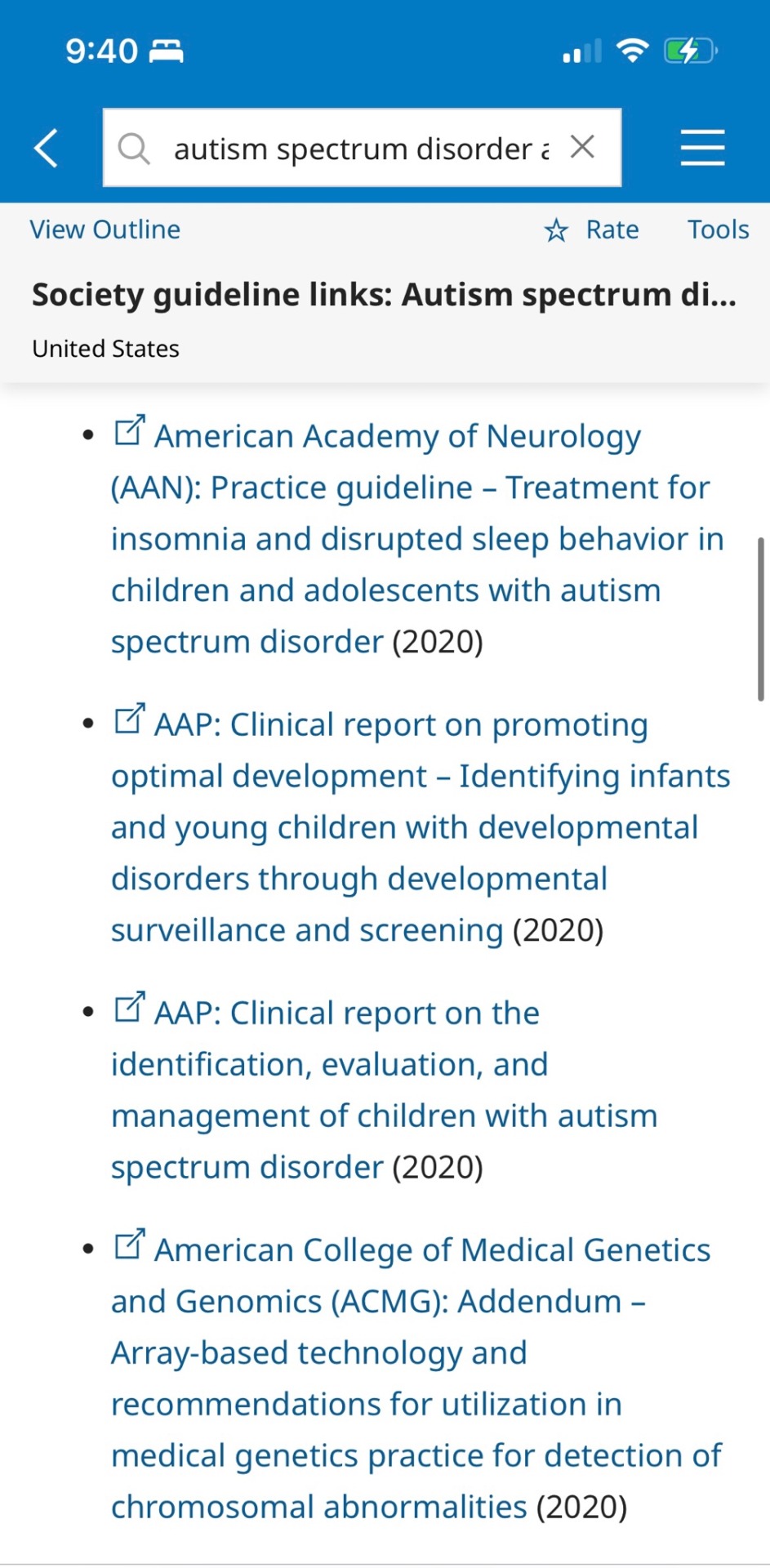
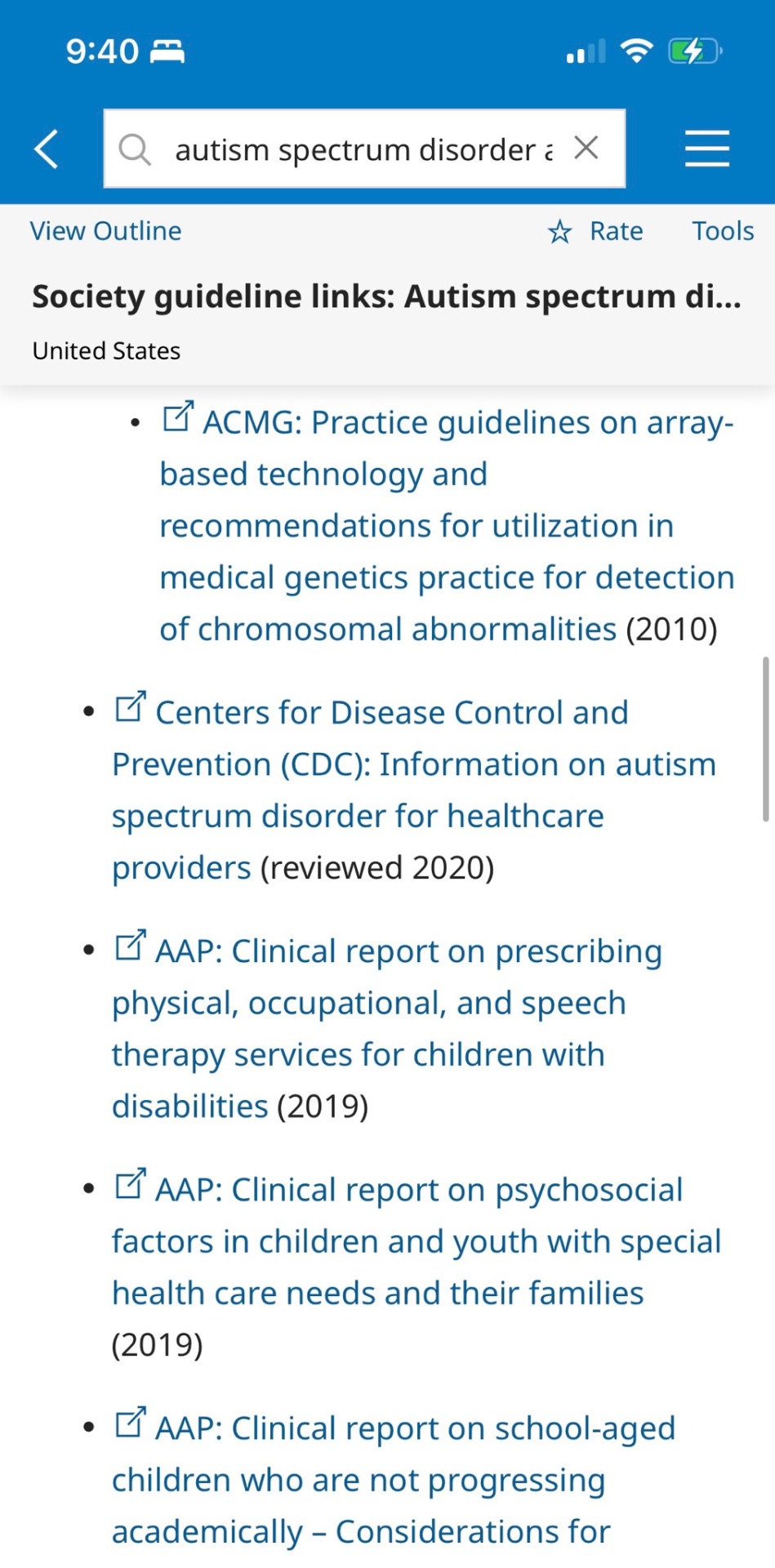
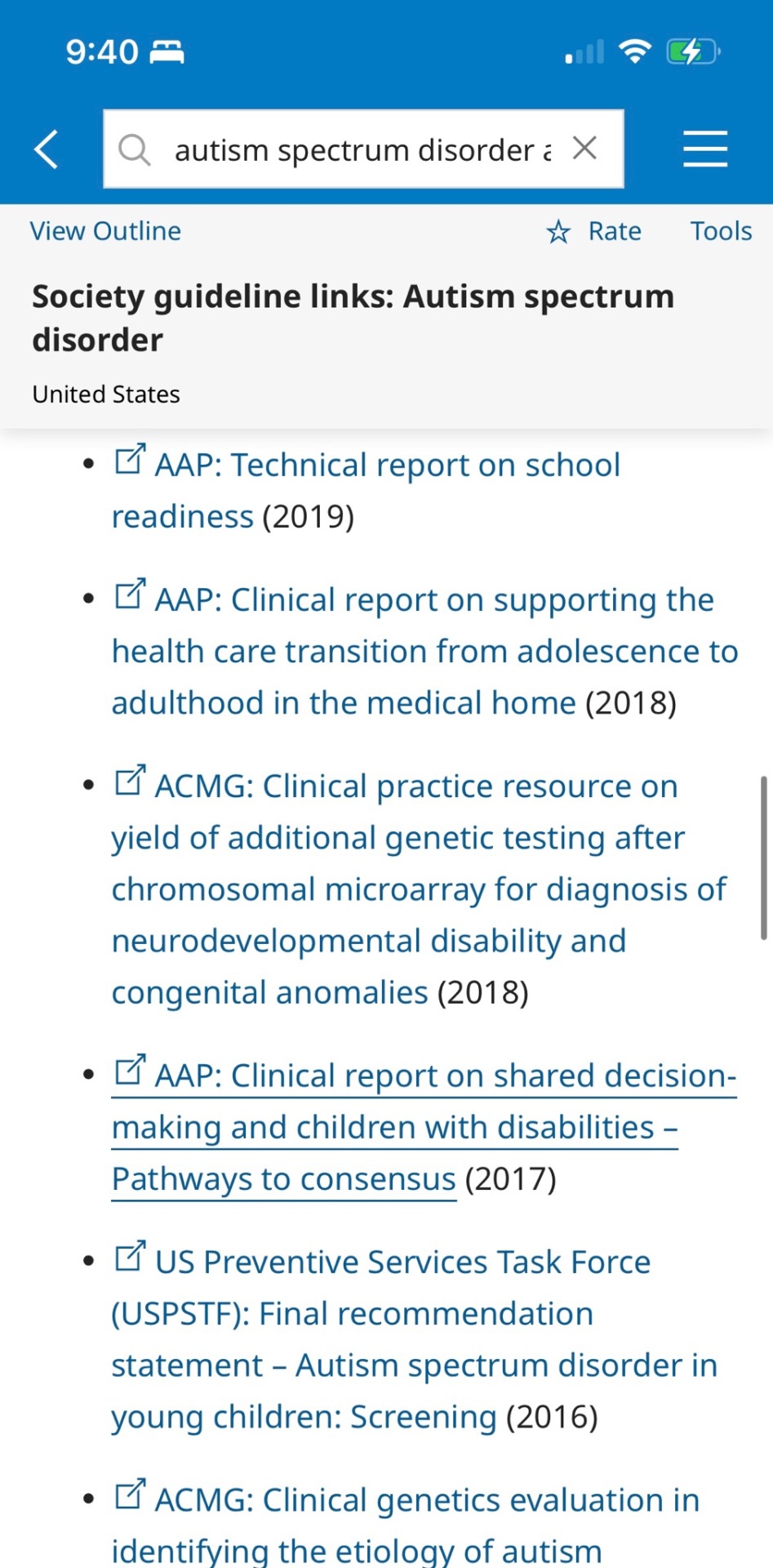
Almost all resources in the US are from the PEDIATRIC association or are primarily related to children. Even that CDC link is really geared towards screening, diagnosing, and treating children. Not older teens, but mainly toddlers and young children. Canada’s resources are all from their pediatric association.
48 notes
·
View notes
Note
oh wow I am so sorry to hear about your daughter having EOE - that sounds really rough. How do you navigate that?
At this point, with a lot of flailing.
It took 3.5 years to even get her properly diagnosed, not through lack of trying-- it's just a hard thing to differentiate, and the specialists that can actually do the test are dealing with a huge number of patients so they're always backed up. We're lucky: we live only an hour from the state children's hospital where they can do the diagnostic procedures, and it has a dedicated EOE specialty clinic that's one of the best in the country. It still takes 2 months to get an appointment as an established patient, and it took even longer to get her in on the initial referral. We're also lucky that she was able to explain to us what she was experiencing in a way that a doctor could take seriously and act on, and we're lucky that her primary care doctor did so.
But generally speaking, things suck spectacularly for pediatric EOE and GERD patients right now, at least in the US. The best medicine for treating it is omeprazole (prilosec), and there was exactly one manufacturer that made it in a suspension that small children could take. Well, that manufacturer decided it wasn't profitable enough, so they quit making it altogether. So now the next best, lansoprazole (prevacid), is on national back order for months because every child that was on the other one is now needing to switch.
So my daughter is currently on the next next best thing, because it was that or nothing, and it's just not working great for her. It keeps her from the worst of the pain, but she's back to not wanting to eat anything but bagels, one specific brand of cereal, and string cheese.
Back when she was officially diagnosed, her doctor gave us the option of going on a super dose of PPI meds, jumping straight to the steroids, or doing a full elimination diet with a nutritionist. For a kid, none of those options are great.
The PPIs reduce absorption of nutrients, which are already few and far between for a growing person with only a few tolerated foods. The steroids may have effects on a growing liver and kidneys, and also make you more prone to fungal infections and upper respiratory illnesses. Both have to be routinely dose-adjusted because the child is growing constantly, but you have to get an official weight/height check at the specialist to do so, which is always backed up. Then the elimination diet is...well, it's hard, to put it mildly, and it takes a really long time because of how delayed the reactions can be. Plus when you already don't like eating and only have a few 'safe foods', it's hard to cut back. Most people with EOE also have more than one trigger, so you have to eliminate a ton of things and hope you get them all, and you can't be on any medication while you're doing it because you have to be able to identify the point at which symptoms get better and then return.
In short, all the options suck.
We eventually decided on trying to get it under control enough with the meds to hopefully expand the foods she was willing to eat, in preparation for doing the elimination diet. It was working. Then the forced medication switch blew that all up. So we're just gonna grit our teeth and go with the elimination diet unless her specialist has another option for us.
But aside from that, it's been a lot of phone tag and appointment waiting, and a lot of readjusting the way we look at food and eating.
For her, whatever she will eat is a win. We've taken pressure off her to try new things. We still offer it, but we don't press if she's not feeling up to it. Reducing stress around the concept of trying new foods is super important, because she's already up against the stress of wondering whether it'll 'get stuck' or feel yucky or make 'the fires' worse.
We've also had to make sure we don't fall into the trap of trying to dictate how much she eats and when. Unless a meal is coming within the half hour, we let her have a snack when she's hungry-- wait too long, and she's in pain. Plus we want her to kind of train herself to respond to those hunger cues because her appetite can get so drastically reduced at times, every instance of her listening to an 'I'm hungry' is a win.
We also had to abandon the idea of the 'perfectly' balanced diet. Proteins are a struggle for her. Leafy greens are a struggle. So are other calcium containing foods like dairy and dairy alternatives. She really only likes carbs, mostly bread and fruit. But it's not like she can help it. Nobody purposefully restricts their diet just to be difficult-- a "picky eater" is someone who is struggling and needs accommodation, not judgement.
So we let her eat what she will eat, and work to find options that can get her the stuff she needs. Protein bars are a big hit with her right now, for example. A better texture than meat, they come in 'treat' flavors, and there are options that don't have all the added sugar that's gonna trigger the acid flareup. We make sure we get enriched flour and bread products so she gets at least some iron. We pick varieties that have added protein and calcium. We get juice with added vitamins and minerals. We stock the pantry with things that cater to her capabilities and needs wherever the two overlap. The goal is nutrition, whatever form that takes and whatever it looks like right now. Getting it "right" will come later. For now, we just need her to be comfortable with food and to learn how to work with her body.
This has also meant teaching her about nutrition, so we can help her take charge of her body's needs and help us think of ways to meet them. That's hard for a 3 year old, but there's a show called Storybots on Netflix, and they have a great episode on nutrition called "Why can't I eat dessert all the time?" Super accessible for kids, and has a catchy song describing macronutrient categories and why we need lots of different kinds of food, not just one kind. It was a perfect starting point, and we just kept at the explanations. Like when we would eat an apple with breakfast, we'd talk about how it has Vitamin C to help her cells be strong, fiber to help her tummy and intestines work well, and carbohydrates to help her have energy. Every time we try a new food, we talk about what's in it to help her body. That includes things like chips and cake--we're big on the concept of "all food has value, it's just some has more than others, so we eat the most of those."
So now, when she's had a "just bread" day we remind her that her body needs more than just carbs, and we can't get all our protein, fats, vitamins, and minerals from bread, so we should probably have something else too. 9 times out of 10, she'll add something to her request, like some blueberries or carrots. She might not eat a ton of it, but she tries, and that's what counts.
I know this is a mile long and probably way more than you were asking, but it's just one of those things that I have a lot to say about. I could talk all day about accessible eating and nutrition, as well as Going Off on our current medical system in the US, so if anyone has further questions, feel free to reach out.
35 notes
·
View notes
Text
I recently held a word-puzzle contest, and the prize was the chance to ask my therapist one question. @captious-solarian won, and asked
Dear Therapist: You're having a lot of social-ish interactions with your patients outside the bounds of normal therapy. Why do you do this and how do you address ethical concerns with it?
I gave her the question, and her answer is transcribed below the "keep reading". I feel like she's answering a slightly different question than what you intended, but, oh well, you asked, she answered, you get what you get and you don't get upset.
Thank you for the question, captious-solarian. I have been a therapist for over thirty years—actually that's not true, I've been working in the field for over thirty years, and I've been a therapist for over twenty years. The rules of ethics are there to protect clients from the power differential that exists between a therapist and a client. The work that I do is mostly with folks on the Asperger's and autism spectrum, and for them, in order for them to be able to learn skills and adapt to society the way it is, I have found it to be most effective to do that work in the community. Sometimes that involves social interaction that is not typical of therapy. If you would like I'd be happy to send you a copy of the ethical rules for counselors [Editor's note: This document, I believe] and there is nothing ethically wrong with that. When I do social interactions with my clients, I am not inviting them over to hang out with me and be my friend. That would be a dual relationship. I am not engaging in dual relationships, I am engaging in activities that are specifically for the betterment of my clients, and I've found that these strategies and techniques work very effectively. If my client doesn't feel comfortable with these techniques and strategies, they absolutely do not need to participate in them, and I always offer the options for them to just sit in my office and talk.
However, for many of the clients that I work with, sitting in the office and talking is what they've been doing with therapists for their entire lives. For some people that I see who are in their forties, they've been going to therapy — traditional therapy, that abides by the traditional methods — for forty years, since they were diagnosed as children. And they've been stuck. I know what works. So I offer it to my clients because that's where they are, and my goal is to help scaffold them to the next step in their progress and development, wherever that may be for them. So for some of my clients, going out into the community, and engaging in social activities is more therapeutic than sitting in an office and talking. Because they have talked their brains out, and now they need to actually live.
For individuals on the spectrum, they learn social skills and how to function in our disabling society not by simply being told what to do or, technically, usually they're just told what not to do, but nobody ever tells them what to do, and, even when they do, simply being told that does not get them anywhere. They need to be shown. And they need to experience it so they can realize, hey, I actually do want to be social, it's just that nobody's ever shown me how to do it in a way that is satisfying, effective, and — it's scary because any time I try to be social, people reject me. So. What I do is to specifically address that, and I am not going beyond the ethical rules of conduct. I also know that the benefits that my clients are getting, and what their parents see as change in them is so effective that I am not worried that somebody will bring a malpractice suit against me, because, if their child, or if as an adult, they are doing better, they don't care what the technique is. They don't care what my methods are. And these methods are effective. I would be more than happy to answer any follow-up questions that you have [editor's note: lol, not unless you win another contest] and like I would be happy to send you a copy of the rules of ethics for counselors, and you can see that I am breaking any of them.
Thank you so much for your question, and I really really enjoyed being able to answer it fully, because I know that [REDACTED], whatever his screen name is, enjoys posting things that I say because they are not typical. I also know that he doesn't give any context, because he likes to freak people out. So, I very much appreciate your question, and I would be happy to speak with you further if you want to. [editor's note: again, not happening] And I can explain more or I can tell you about the way that I work. And I have been doing this, like I said, for twenty years, I have never ever had to advertise. I've never requested for a referral. And I have been full with waiting lists because of the way I do things. Nobody else does it this way. Not because they don't care, but because they don't think outside the box. And, because, maybe they don't care that much. Maybe they just see their clients as clients. I see them as human beings, and I meet them where they're at, and if where they're at is that they need to experience positive social interactions in order to want to take the next steps in their lives, then that's what I do.
My view of therapy, if you would like to look at my website [editor's note: I am not linking you to her fucking website] is that my job is not to fix anyone. My job is to meet someone where they're at, figure out where they want to go, and help them get there, or coach them to get there. Sometimes that means showing them experiences that they've never had before, or ones that have not been satisfying; sometimes that means just standing and waiting for them to be ready to go to the next step; sometimes it means giving them a little push, or a kick in the ass, if they are not ready, or if they don't think they're ready but they actually are. I actually think I'm a fantastic therapist (and I'm not just saying that to be conceited, I've just seen results over and over and over again) and parents usually think that I am some kind of miracle worker. Which I'm not. I am just somebody who treats my clients as human beings, meets them where they're at and tries to hold their hand as they're going to the next phase of their life. Once again, thank for your question, and thank you for giving me the opportunity to answer it.
19 notes
·
View notes
Text
History of Situational Mutism
have made a post on this before, so have taken some parts of that. but this is more comprehensive. aka long post like looong⚠️
summary:
aphasia voluntaria -> elective mutism (voluntary, refusal, oppositional) -> DSM IV = inability (failure, rather than refusal, to speak).
differential diagnoses: DSM-III = developmental disorders -> IV and IV-TR = speech abnormalities and social anxiety disorder -> DSM-V = communication disorders, social anxiety and psychotic disorders like schizophrenia and autism spectrum disorders.
2013 DSM-V changed it from Childhood disorder to anxiety disorder. it also removes reference to trauma as a possible cause.
DSM IV-TR said SM had slightly more females than males. DSM-V says SM has equal gender distribution.
People thought DSM-V would subsume SM into SAD, but it didn’t due to the uncertainty around the relationship between SM and SAD.
It has since been recognised unofficially as ‘situational’. but this is not enough because ‘mutism’ also ignores how SM can affect all communication.
“It was back in 1877 that a German physician called Adolph Kussmaul used the term ‘aphasia voluntaria’ to describe children who ‘refused’ to speak though they could speak normally. Kussmaul used the term after he reported three clinical cases with similar symptoms (Jainer, Quasim, & Davis, 2001). In 1934, a child psychologist from Switzerland called Mortis Tramer used the term ‘elective mutism’ for the first time to describe ‘a fascinating group of children, whose talking is confined to familiar situations’ (Kolvin, Trowell, Le Couteur, Baharaki, & Morgan, 1997). Going by both the terms, it can be seen that the understanding was of a voluntary act of refusing to speak, which would mean it was an oppositional behavior (Noelle, 2017).
The same understanding is reflected in the diagnostic criteria given by the earlier versions of the Diagnostic and Statistical Manual (DSM). The third editions of the Diagnostic and Statistical Manual (DSM-III and DSM-III-R) explained elective mutism in terms of ‘refusal to speak’. This was changed in the fourth edition of DSM, where it was recognized as an inability to speak (Noelle, 2107). The diagnostic criteria given in DSM-III (APA, 1980) talks of ‘continuous refusal to speak in almost all social settings’, while the diagnostic criteria given in DSM-III-R (APA, 1987) updated it to ‘persistent refusal to speak in one or more social settings’. In contrast, after the publication of DSM-IV in 1994, the diagnostic criterion read ‘failure to speak in specific social situations’.
There are other differences between the elective mutism as described in the third editions (DSM-III and DSM-III-R) of the Diagnostic and Statistical Manuals (APA, 1980, 1987) and the selective mutism as described in the subsequent editions, i.e., DSM-IV (APA, 1994), DSM-IV-TR (APA, 2000) and DSM 5 (APA, 2013). Some instances would be the predisposing factors and differential diagnosis.
According to both the third editions of the DSM (APA, 1980; 1987), maternal overprotection, speech disorders, mental retardation and trauma were possible predisposing factors for the onset of selective mutism. These factors were, however, removed in the subsequent editions of the DSM (DSM-IV, DSM-IV-TR & DSM-5). Similarly, the third editions stated that the ‘refusal’ to speak could be differentially diagnosed as developmental disorders, while the later editions (DSM-IV & DSM-IV-TR) list speech abnormalities and social anxiety disorder as differential diagnosis for selective mutism. DSM-5 (APA, 2013) lists a differential diagnosis of communication disorders, social anxiety and psychotic disorders like schizophrenia and autism spectrum disorders.” Source: ‘selective mutism - understanding and management’ by Charu Kriti 🌹🌹
in 2013 the DSM-5 moved SM from the childhood disorders category to the anxiety disorders category. The DSM-5 also drops the reference to trauma as a possible cause of SM, and indicates that SM has equal gender distribution, whereas the DSM-4-TR had indicated slightly more females than males.
People thought the DSM-5 would subsume SM into SAD, but this didn’t happen due to the uncertainty surrounding the relationship between the two disorders. (high comorbidity, some argue SM is an extreme version of SAD; some argue SAD causes SM; others argue vice versa).
people with SM have since recognised it as ‘situational mutism’ to avoid the misunderstanding that sm is ‘selective’ or a choice not to speak; and they consider it an inability to speak in certain situations (people, places, settings). but this name is still not enough in my opinion, because it still focuses on what is considered the biggest problem for OTHER people, rather than for the person. sm is not just mutism (inability to speak); it affects all forms of communication. source: ‘Selective mutism in adults: an exploratory study’ by Carl Sutton. pp 18-19
maybe a better name is communication anxiety disorder or something like that. but then again, it is still not fully accepted as an anxiety disorder; only in official definitions.
33 notes
·
View notes
Text
Anon wrote: Hello mbti-notes, 28F ENFP here. I have written to you a few times, one of them about my relationship with my 27M INTJ boyfriend and the other about my childhood trauma regarding my ENTJ mother and how it was keeping me from pursuing my art career.
I have been on the road of Fi development and lately I have started to develop Te. Some major life events happened since the last time I wrote to you; I had gotten diagnosed with ADHD after suspecting having it for years; then, my younger cousins got diagnosed with level one autism (Formerly known as Aspergers), and after my mother conversed with their mothers, we reached the conclusion I and other members of the family are also autistic and ADHD, since I displayed symptoms of both as a child.
With this new knowledge, I have been making all the changes necessary to accommodate myself and do the best I can and pull my own weight. I am almost finishing University, and my boyfriend (he’s pretty much my husband at this point) started his doctorate and is now an art teacher at our local arts University. (those issues I had written to you prior were resolved and we have been very happy together and supportive of each other since).
I have been slowly tearing down my perfectionistic tendencies; I am no longer unhappy about my work or extremely self-critic to the point I put myself down. I have gained confidence and trust in myself and handling problems, crafting solutions, planning (even if short-term) and improvising. I have been re-enganging my Ne in a healthy manner, focusing on my projects and progress instead of being scattered and wanting to do everything and anything.
Despite that, and all the growth I have done already, I feel that I have an unsurnamable mountain of obstacles to pass through. Over the last year, I have realized just how little my ISTP, probably autistic and bipolar father and ENTJ, probably ADHD mother completely failed to prepare me for life. I was emotionally neglected, made a scapegoat for their problems, made to pick up after myself because of my autism and ADHD being seen as failures of character instead of disabilities.
They saw I was intelligent, and rationalized it as “not needing help”; then, when my problems with executive disfunction and organization started flaring up due to their neglect, they yelled and blamed it on me, worsening the situation. I grew up with no understanding of boundaries; I wasn’t allowed to advocate for myself and everytime I tried I was yelled at; I wasn’t allowed to discover myself and my identity properly so I clinged to my special interests like a moth to a flame; I was shamed for my way of functioning and that impeded me of developing proper knowledge of myself and what I needed.
I now notice my social differences, my trouble dealing with and regulating emotions (and why I put off dealing with them), and my lack of social skills and differentiating levels of relationships. I feel angry that the time I needed to be using to deal with these issues, during adolescence and early adulthood, was taken away by autistic burnout, depression, and dealing with a disfunctional family who had no idea how to care for me and never tried to, and spent pursuing bad relationships, hyperfixations and changing interests, all the while not being able to put effort into what I really wanted because of the shame and judgement they placed on me.
I have been trying my best to pick up the slack, but it’s hard. I can see now how I was unjustly punished for my differences my whole life. I finally understand now why people get upset with me with things like being unable to regulate tone or asking clarifying questions (when I’m just trying to understand them).
I have accepted myself; I know my difficultities now and I know what I have to do to regulate myself, but I still can’t stop feeling angry at this injustice. I do my best to be proactive and helpful in the communities I join and make friends, but people will turn on me the moment I do something impulsive like vent to chat about my parents doing something rude to me that day (which happens regularly). The bridges I put effort into building get destroyed in minutes, and I feel like all my progress is undone.
Family is a tricky issue for people, I get it. There are different times and places to say things, I get it. But It still happens. I know the way to fix it would be to leave, but due to the housing crisis, inflation and my expenses of trying to finish my degree, I can’t move out of this place and still currently live with them. Rent is unnafordable, my boyfriend is going through his degree and busy, and I’m already at capacity fully comitting myself to art and doing the best job I can with chores and house stuff.
I know my parents have issues and I try my best do understand and be empathethic, but they aren't doing anything to get better or to resolve them. My dad is on disability and unemployment aid right now, he does minimal chores and watches TV and sleeps all day. My mother is a pre-school teacher and constantly overworks herself because that's how she learned to get through life.
A few months ago, my mom almost ended her marriage because in her words, she developed a "platonic crush" for another man. It was a huge fight, and one they tried to drag me into. When they're not having outright fights, they act lovey-dovey; but they soon have another nasty fight, and the cycle goes on.
My dad is extremely misoginistic, judgemental, and cynical. Everytime he tries to engage me in conversation, I act uniteresting so he leaves me alone. I am uncapable of building a relationship with them after all they did to me.
I just can’t stop feeling I got dealt a sh*tty hand in life and there is nothing I can do about it. I realize this is Si grip talking, but this enviroment completely kills all my optimist, motivation and will to move foward in life, and I’ve been doing this dance for way too long and just want it to end once and for all so I can keep progressing. I know I’ve already come a long way, but I can’t stop feeling it still isn’t enough, and I’m afraid that feeling won’t ever go away. So I turn to you for guidance on what to do.
Currently I am sitting on a few unfinished projects (a comic and animation) that will be my portfolio só I can start working while I finish my degree. My parents are paying for the remainder of it (honestly, the least they could do after the horrible lifetime they gave me) but I plan to start paying for it myself as soon as I get some work. I guess what I'm trying to get at is that I'm doing everything to try and make things better, but I feel like they never will, and I don't know how to deal with that.
----------------------
Whenever people tell me about how they're making progress, even trying to develop lower functions, but also suffering from inferior grip, the alarm bells go off in my head, because it usually indicates some form of troublesome denial. In terms of type development, inferior grip is one of the most serious signs that something is not right psychologically.
I never want to poopoo on people's efforts to improve. I definitely believe that you've been putting forth your best efforts. However, if the outcome is inferior grip, it means there's a problem with your approach or method.
The way that you're stuck in blaming your parents for your misfortunes is not just a sign of Si grip, but also Te loop. If you're suffering from Te loop, it means Fi development hasn't progressed to the point where you are ready for Te development. Being a lower function, trying to develop Te when you're not ready is only going to exacerbate Te loop and eventually lead you into Si grip.
I won't deny that the people around you every day have a big influence over you. As a Feeler, their moods can easily affect yours. When that happens, the best thing to do is to draw up boundaries, to try to shield yourself from those negative influences as much as possible. However, what you've done is the opposite.
You've been drawn into the negative influence through blaming them, fighting back (mentally), judging them for their flaws, indulging pointless "what if" scenarios about your past, etc. In short, you have been swallowed up by the negativity partly because you didn't do enough to protect yourself from it. This is related to Fi development because Fi should inform you about what is needed for self-protection.
Now, since you find yourself in a hopeless place and can't accept the feelings of helplessness, the recourse is Te loop. You wish to actively "correct" everything that you perceive is "wrong". However, this is a futile endeavor. Why? Because those things are not for you to correct. You have overstepped/violated boundaries by wanting to solve problems that aren't your responsibility. This only serves to entangle you in them.
You mom and dad's flaws, your mom and dad's relationship, are none of your business, but you are all up in there. Even if they try to involve you, as an adult, you have the power to refuse. Because you care about them, it's hard for you to refuse, but refuse you must. That's what it means to draw healthy boundaries.
Yes, it's tragic to have been deprived as a child. One thing you realize more and more deeply as you get older (especially if you have children of your own) is that parents are human, their knowledge is limited, and people can only do the best they can based on what they know. Many, many people are ignorant about psychological issues because they have had no opportunity to learn about them. What's worse, sometimes what they have learned is misinformation or outdated information based on what was being taught when they were growing up.
I say this not to excuse the bad things that parents do, but to foster empathy for the fact that people can't do better when they don't know better. You are the same. You didn't think to change your behavior or didn't know how to do it in the right way until you learned about ADHD. You live, you learn.
Empathy for others starts with empathy for oneself. Instead of pitying yourself or being angry about your past, healthy Fi should prompt you to express empathy for your struggles today. There aren't enough signs that you possess this depth of empathy, which indicates Fi development has a long way to go yet. It's hard to feel empathy when you're in the thick of negativity, but that's the time when it's most important to practice it.
An important part of having empathy for yourself, aka self-compassion, is allowing yourself to move at a realistic pace in life, a pace that takes your challenges into fair consideration, rather than always trying to live up to unreasonable ideals. Feeling "not good enough" and being afraid of that feeling never going away is directly related to Fi development and lack of self-acceptance. You must accept the truth of yourself and the facts of your situation before you can move forward in a meaningful way.
Also, if you find yourself speaking inappropriately or not giving enough consideration to social context when your feelings get too big, it means you haven't done enough to set up a good social support system and create more appropriate opportunities to explore your personal issues. Expecting parents or colleagues to give you support that they are not capable of giving is basically wasting energy barking up the wrong tree. In other words, don't look for love in all the wrong places. This is related to Fi development in terms of doing what it takes to care well for your well-being.
You are well into adulthood. At some point, it has to be fully your responsibility to craft the life you want. By continuing to blame your parents for not living up to your ideals, you are the one keeping yourself tied to past unhappiness, rather than moving forward. It is a choice you make.
I always say that forgiveness isn't about other people. Forgiveness is something you do for yourself. It's not good for you to live in a state of resentment, anger, or hate. It's not good to keep revisiting and rehashing such emotions on an endless loop. Therefore, you have to learn to forgive the mistakes of the past so that you can have the emotional stability necessary to focus on improving your life today and into the future.
Forgiving your parents for being the imperfect human beings that they are is difficult but necessary, not for their sake, but for yours. You can set yourself free from the past at any time through learning how to be more accepting, empathetic, and forgiving, which is very much tied to Fi development. This would be a healthy way of lifting yourself out of Si grip and mending your mental health.
#enfp#auxiliary fi#te loop#si grip#boundaries#self compassion#empathy#forgiveness#blame#anger#resentment#ask
12 notes
·
View notes
Text
I'm nervous to share this but I need to get better at it. In March this year my therapist diagnosed me with OSDD - otherwise specified dissociative disorder - or one of the variations under the umbrella of what used to be called multiple personality disorder. I didn't know my undiagnosed autism in early childhood could become something this advanced, and I can never find out what trauma exactly caused it because 1) that's the nature of the disorder and 2) my parents who homeschooled/abused me will never help me remember. My best guess is CSA that they tried to cover up and it should bother me more to share that but despite having been a walking billboard of the symptoms at times I don't recall the trauma itself whatsoever so whatever, just the rituals I used to do to try to get out of any more of it happening I guess. Telling my therapist that as a child I stopped bathing for days at a time and don't remember when it started and to this day I'm still mysteriously horrified of the shower tipped her off to my dissociation being highly abnormal
"DID is a dissociative trauma disorder in which a survivor has undergone longterm, repeated trauma in early childhood. This trauma, combined with other factors, results in a rather dramatic interruption of psychological development -- particularly as it pertains to identity. Through a process known as dissociation, this thwarted development results in "differentiated self-states" (also known as alters/parts) who may each think, act, and feel considerably different from one another. These parts of the mind - who may have their own name, age and personality - are able to take executive control of the body, leaving the survivor without any awareness for the time they were gone. These amnesic gaps in memory can be for just a few moments, a few days, or even entire chunks of one's childhood. The alters in a DID mind exist to help the survivor cope with deeply painful and unconscionable trauma, holding it outside their awareness to the best of their ability. However, often once the survivor begins to find safety and/or enter adulthood, this once supremely creative and protective mechanism can turn into a maladaptive trait causing real life consequences."
I'm not sure if I count as fully DID because of my likely low end alter count, which I'll explain, and because how my amnesia works. I want to say I am because I don't remember anything before the age of 7 and didn't know until recently that not everyone forgets early childhood that hard, lately everything before age 13 is on its way out too and I'm gathering that the degree of my short and long term memory loss are pretty severe during times of stress, but I don't currently have blackouts or alters who keep each other out of consciousness to "take over" and are damned to keep secrets from each other, so I don't know. It feels more like they just filter themselves through me, like we're all living the same life but just deal with it and feel about it different ways.
They've written a lot of notes/journals to me over the years, so as an adult as long as I check those I usually remember what they do and feel generally and don't ever wake up like "where the fuck am I," but in the past I mistook them for fictional characters or "intrusive inner monologue" that conflicted with "me," because I didn't know what this was. With more therapy and introspection I've figured that 20+ years ago I once had alters who I can't remember anymore who took a lot of memory away whenever it was they "left"/I no longer needed them.
Turns out even if I hadn't decided to formally learn creative writing I would've been coming up with other people in my head to cope anyway. Kinda puts a damper on the last decade I've spent as a writer or so I thought. Similar to the ablutophobia I don't recall when exactly I started coming up with and illustrating stories, just that I seemed to be able to and I needed to do it as much as possible.
Without prodding off the top of my head I only have two clear memories of being 7, I don't know when they are and they aren't reels of continuous moments more than they are snapshots of just having been there, but I can still see what the rooms looked like when I was in them: 1) playing Pokemon Yellow in my bedroom for the first time and 2) sitting down at the brick computer in my parents' bedroom to write my first word document story.
I say my alter count is likely to be low (but I can't be sure until I get a therapist who specializes in this disorder, mine only does in autism) because I, the host of this blog and normally my brain/body, used to feel like a singlet (someone without DID) and was long unaware of what this disorder was besides the name of it, so we didn't have a naming or recognition method for alters for 20+ years. The way its portrayed in media and online I see a lot of systems with drastically individualized members, but a lot of mine are just "me but with certain emotions dialed up" "me slightly to the left or right" "me at 13" "me when I've suddenly forgotten x important thing again"
Like the autism this is definitely one of those things I needed to know about myself decades sooner, but unlike the autism which I was #bornwith this feels like something I need to apologize for, despite not having the language or knowledge to express how it felt and despite not remembering why I started doing it.
If I'd been able to always express myself as a "we," if I'd known, I wouldn't have hidden this from people, so that I can get better. Whether that be through "final fusion" (all alters becoming one) or "functional multiplicity" (less alters becoming as few as possible) I plan on healing as much as possible despite no longer being able to recover all the pieces of my puzzle
9 notes
·
View notes
Note
Can we get four headcanons about Helena Sinclair?
Realistic
Helga Sinclair wants her children to be educated and have a solid start of life; she taught them a lot of things, and finds textbooks for them.
You know, history books about dictatorships, failed and thriving civilizations, the Art of War, guerilla war tactics, how to mix your own Molotov in few easy steps...
Helena decided she likes psychology and psychiatry. She doesn't differentiate between rhose as long as it teaches her neat tricks to manipulate people. Or allows her to figure out what the fuck is wrong with the majority of Isle people.
Yes, she explained what narcissism is to Mother Gothel. Fortunately for Helena, Gothel was teaching a class (which was originally about Yzma, but that lasted about two minutes before Mother Gothel started talking about her favourite topic. Herself.) Consequently, Mother Gothel didn't hear a word of what Helena said.
One of her favourite hobbies is saying „Hmm mommy//daddy issues,“ every time she thinks someone is being annoying.
Unrelated, but she is a pretty good runner.
Unrealistic but funny
She's an OC, there is no such thing as unrealistic.
Once she lent her gun to CJ.
Wait, yeah, it is unrealistic: in the regard that she survived after Harriet and Harry learned she gave a gun to CJ.
Also Uma and Sammy Smee and Anthony Tremaine.
There is a reason the Hooks aren't allowed guns, okay?!
Freddie though it was funny though and offered her an azyl.
Heartbreaking
She is jealous of CJ Hook.
You see, Helga Sinclair saw tiny gremlin child CJ Hook (way more feral and willing to do pretty much anything for attention and out of spite) and thought „Wow. This baby can fit so much chaos.“
So she decided to basically adopt CJ as an "auntie" and teach her even more ways to create chaos. Also how to get away with murder.
Helga Sinclair has lot of enemies on the Isle and in Auradon. And she is absolutely encouraging CJ to, ehm, get creative. (It's fine. Murder is a bonding activity.)
But yeah, Helena can get jealous of the attention CJ recieves from her mom. She also spent way too much time thinking about why she feels that way and she hates her conclusions, thank you for asking.
Canon is a suggestion ✨
Upon leaving the Isle, she took one (1) look at Ben & Audrey and began "diagnosing" them.
The words "Daddy//mommy issues" were said.
It was mostly an excuse to rant about King Beast anyway.
Also, she is one of the very few people that seeks out the company of both Hooks and Hearts. Anthony Tremaine thinks she is absolutely insane for that.
He had told her so one time.
She looked around the room, in which were his cousins or maybe Ginny or anyone really, pointed a finger straight at his chest, and said: „Saviour complex.“
He shut up.
16 notes
·
View notes
Text
Oh the way those PANS/PANDAS parents talk about their children’s illness get my hackles fucking raised. It’s like every “autism mom” I’ve ever heard talk. I’m not even writing off the idea that there may be cases in which an infection leads to an autoimmune response that causes neurological mental health changes in children. I can totally conceive of that being a thing we don’t totally understand yet. But the way these people approach it…. God. I know it’s got to be terrifying for parents if their kid suddenly develops OCD, ED, and/or tourette’s symptoms, but the scientific data is so severely lacking, and the language these parents use to talk about those experiences is. Very specific.
The proposed biological indicators for PANS are often present in people without the disorder, without any of the related symptoms. The current proposed diagnostic criteria is extremely generalized and doesn’t very rigorously provide ways to rule out differential diagnoses.
The proposed treatments of long term antibiotics and steroid usage can have dangerous side effects and extreme consequences.
But there are thousands of parents online who will insist it’s 100% real, it’s an epidemic, and they’ll use their numbers to attack anyone online who disagrees with them. Some of these kids may have symptoms that did genuinely arise because of an autoimmune response linked to infection. I wouldn’t write it off. Further scientific study is clearly needed. But it’s also just as likely to me that there are parents out there that just refuse to accept that their kid could be mentally ill for no single curable reason.
I say this as someone who, themselves, developed severe mental illness as a very young child. It’s possible your kid just does have trauma, just does have ocd, just does have depression, just does have tourettes. But these parents see their kids “suddenly” present symptoms and insist on correlating it with extremely common childhood infections. And then manage to find some medical professional somewhere who will actually agree to put their kid on long term antibiotics, and insist their kid’s mental illness just totally went away afterward!
And like. Sorry. But there’s no way for me to hear that and not be reminded of the parents who think red dye makes ADHD worse. Or the parents who think their children’s autism is caused by intestinal parasites, and insist that since they started making their kid drink a bleach solution they bought online their autism has “improved.” The science is inconclusive, everywhere you look there’s confirmation bias, and also.
Every time I hear parents talk about this, not one of them mentions how their child felt about their experience. It’s always “they developed all these tics and compulsions, they wouldn’t eat, they were paranoid, they became suicidal, it was SO scary and hard for me!” and it’s like. As someone who was once a very mentally ill child. Why do every single one of you fail to address this. They seem more concerned about how “scary” it is and how “different” their child has become than their child’s own internal experience of suffering.
#also the idea that autoimmune response -> causes neurological symptoms#and then said symptoms just…. go away after ‘treatment’#sorry. what.#some symptom secession makes sense.#bc of the immune issue has been resolved then so has any inflammation#but here’s the thing about how those conditions work:#if the damage is that extensive that it is causing sudden onset of extreme symptoms#then PERMANENT damage has been done. it is not just going to go away.#the symptoms may get better with treatment yes. but the breadth of new neurological issues are not just going to spontaneously resolve#I mean we see this w sydenham’s chorea. which is literally an example of this proposed mechanism happening#also sorry but when I developed severe depression at age 8 yeah it WAS scary. for ME#Christ. I cannot imagine if my parents had started insisting my new obsessive compulsive symptoms and lethargy and sadness was bc I’d had#fucking strep throat a few weeks before#child abuse mention tw
3 notes
·
View notes
Note
Hello! Not a request but a question. I hope I won’t make you uncomfortable, sorry— but you could please explain to me what systems are? Or sending some links explaining? I have saw it sometimes but never could understand it well… I just want to get informed since some of my moots are and I want to support and learn more about them.
No worries, this doesn't make me uncomfortable at all, and I'm glad you asked!
First things first, every system or person with DID is different with different experiences. I'll be describing some of my own here, but just know it could always be different for others. The best way to support someone is to ask them questions, see what their experiences are like, and try and educate yourself outside of that as well!
Anyone feel free to correct me on anything I got wrong! DID is still seen in a horrible light where I live, which is hard for me, but I've been trying my best to learn
DID/dissociative identity disorder is usually caused by traumatic events in childhood, where the child proceeds to try and distance themselves from this trauma by dissociating, or pushing the events and memories onto another self, thus creating a fragmented sense of identity. This usually causes amnesia as well, due to repressing memories
A system is a body that has dissociative identity disorder/other specified dissociative disorder. There's usually a "host", the core of the body, and "alters", other personalities who diverge from the host
"Fronting" is a term usually used to describe which alter is in control of the body's actions at the time, or most present in the moment. Not all people with DID have such distinct compartilzations, though. Sometimes multiple alters might be fronting, sometimes you might not know at all. Remember that DID is a dissociate disorder!
Alters have a wide range depending on person to person- sometimes they have different interests, names, genders, ages and the like, and sometimes they're a lot more foggy and unspecific than that. People can have even up to 100 alters, or just the one. For me, it's only me and my alter Blaze! He's only chosen a name for himself pretty recently, though.
Remember to ask, if they're comfortable with it, more about alters and their differences. And, again if they're comfortable with it, who's fronting right now so you can differentiate between them. It's a nice way to show you respect their identities and that you care!
Here are some links that go a little more in-depth about the symptoms of DID!
Link 1 ☆ Link 2 ☆ CARRD made by someone w DID!
I talk a bit more about my own experiences with DID down below, but you can skip this bit >.> TW: mentions of childhood sexual abuse past this point
While I am not medically diagnosed with DID, I've had 3 therapists say I have a dissociative disorder and it's highly likely to be DID/OSDD, but since a medical diagnosis like that would literally wreck my life in this backwards ass country lol I don't want it on any of my records [same thing with autism! I was asked to get a formal diagnosis but my mother literally refused]
I formed my alter Blaze due to repeated sexual abuse at school from a teacher, and grooming from an older woman. Blaze was there to help me manage my emotions, and take over when I was too overwhelmed to even speak let alone move or function properly. I know I speak about it in a fairly casual and friendly manner on here, but DID has heavily affected my life. There's things neither me or Blaze can remember, and it scares us. There's days where I feel so far away from my body and I shut down completely because I don't feel like I really exist in the physical world. There's days where I or Blaze look in the mirror and we can't see ourselves, and it's very distressing.
I've been getting much more comfortable talking about it online! The community is very loving and open, and it's helped me and Blaze feel more comfortable. Nobody irl knows this part of me, despite the fact our mom notices the changes in behaviour sometimes, so it's nice having somewhere to talk about it
Me and Blaze been trying to manage our symptoms and relationship better! Things are much much better than they were in the past, especially now that we're far away from our past sexual harassors.
I think that's about it! I hope this helped at least somewhat, and feel free to ask more questions if you've got any! ☆
8 notes
·
View notes
Note
Hey, I totally understand you might not want to answer this so please don’t feel pressured to! But I was wondering how you found out you have fibromyalgia? Is it something you’ve known since you were a child, or did you recognise the symptoms later in life and go to a doctor? I’m asking because I think I might have some sort of condition, if not fibro then maybe some kind of arthritis. I get a lot of the symptoms, but I don’t know if it’s just a normal amount. I do get joint pain, and even though it gets worse sometimes, most of the time it’s not unbearable. And also other symptoms like fatigue and brain fog etc, but they could be linked to a lot of things in my life. Obviously I know you can’t diagnose me or anything over an ask, but do you have any advice on how to tell what level of pain is more than expected for someone without a condition? Like I said at the start, please don’t feel like you need to answer this, feel free to ignore/delete it.
Honestly other people who have it talking about it clued me in a lot. I really don’t know how long I’ve had it but it got really bad and unbearable for me after a pretty bad head injury I had last fall. That’s a big way it can get started theoretically (nobody really knows anything about this for sure) and hoooo boy did it for me. So I’ve really only been actively aware of this for I’d say 4ish months? When I think back though I’ve had most of these symptoms for years, like since college
So a lot of googling around and talking to the right people and doctors (though I still have to get my ass up to a specialist for a ✨formal✨ diagnosis despite being p much confirmed already but I’m like literally why I have doctor anxiety and half of doctors think it’s fake and there’s nothing to be done about it anyway rip, the medical system in this country isn’t uh the best for that kind of shit) bada bing bada boom there we go
Some tips maybe I guess
If you are always/often in pain that’s not normal. It seems obvious but I had to actually have someone tell me that after putting up with it for so long. Also if you have fibro/chronic pain you’re likely to have a higher pain tolerance than others, for clear reasons
If a doctor tells you you don’t have it then maybe you don’t but also so many of them like don’t believe in fibro so I’d always get a second opinion
Track/pay attention to symptoms and when/how they get better or worse. A lot of times fibro pain gets better with exercise so you can differentiate it from like. Injuries or being out of shape. Also for me I’m always gonna have more pain after eating a lot of sugar.
Also fibro pain often affects muscles vs joints and isn’t necessarily limited to like one body part. For me I have several places it likes to be and it kind of just moves around. Also there are some areas more commonly affected than others
A lot of info can be found by googling! Symptoms and treatment!
A lot of symptoms for me are just stuff I’ve learned to live with but I often have “normal” days just from paying attention to diet, exercise (cycling), and taking glucosamine daily. I also have some mobility aids for days I need them but the more I exercise the less often that is
Obviously doctors can suck, but it’s definitely useful to get an opinion if you have the option
I hope any of this random rambling is helpful!!
2 notes
·
View notes
Note
hey i cant remember your DID blog, im sorry, idm if you answer over there if you tag me.
to start with, i have professionally diagnosed DID and have been dx'd 3 separate times, and i have something i guess i want validation for?
since i was itty bitty i was reading greek mythology, like children's versions (i could read very early - "gifted" kid) at 3-5 and it has always very much been a huge running theme in my life, well i have a lot of religious greek alters.
it makes sense that.. reading about these figures, watching movies like disneys Hercules and stuff especially while experiencing consistent trauma that i would develop these alters with my brain viewing them as powerful and comforting?
and as an adult i have developed a bit of spirituality with them, a deeply, deeply personal relationship and devotion to deific alters formed to protect and care for me
i recently had a whole issue with a friend who told me my perception of the gods were "wrong" and that they could communicate with them for me. that the gods could only visit one person at a time. and it fucked me up so bad even though i knew they were wrong. they traumatized my whole system
because the things i communicate with aren't just the gods, they dont even claim to be the real gods nor speak for them, just "real to the andromeda system". no one can communicate with my version of them because they are *alters* and my perception is based in trauma and my needs at the time of formation
i feel fakey and i generally avoid even mentioning the religious alters to therapists because i dont want to come across as attention seeking. my experience is valid right?
in terms of clarsenses.. maybe thats a part of it too? idk but these guys are inherently different from say. the spirit of the trees. idk its complicated, they can front and care for me and have a place in my headspace. i notice i get some gifts like i asked hermes to help us get the car we wanted since ours is breaking, and we're getting an even better version. i dont understand fully, i just know my experience is different and deeply personal and relevant to my trauma and DID.
last thing; i do have other alters unrelated to the greek pantheon that interact with them in the headspace. ones that are more "normal" i guess like child alters and trauma holders/persecuters and regular protectors (many of the greek ones are protecters/caregivers/managers. a small few hold trauma - like Hera holds the trauma i witnessed my mom go thru and she is a caregiver. some front. some are internal.)
i guess im seeking an explanation from someone in a similar position? in terms of being spiritual with a dissociative disorder. especially considering i do feel like i receive gifts from them in the real world
im just confused about myself and experiences which feel incredibly complex. it feels like my experiences go hand in hand with each other!
I'll say what I always say in these situations:
It's not a question of "valid" or "invalid," it's a question of what something is. Our feelings are always valid, but that has nothing to do with whether we're accurately interpreting them or not. Discernment is what's important, and as frustrating as it is, no one can really do that work other than you.
I can't even offer much in the way of perspective, to be honest. Despite the fact you and I are in similar positions, my experiences with dissociation and clairsenses are totally different. None of my alters take the form of deities, for one thing, but I've also never had trouble differentiating my alters from deities.
My advice would be to just give it time. Spiritual exploration is full of heavy lifting, and it's something we just work our way through over the course of time.
(Also my brain blog is @prefrontal-bastard, if you ever have questions in the future.)
24 notes
·
View notes
Text
A Resource on DID/OSDD and Glossary of Terms, with Neither a Pro or Anti Endo Stance
Since we as a DID system saw a lot of carrds that were made by anti endos, and clouded by syscourse, we decided we'd make our own DID/OSDD resource for singlets to learn about DID/OSDD or newly discovered DID/OSDD systems to learn more about how they work and find terms that describe them and their alters. This resource also goes into self diagnosis and tips for living with DID/OSDD. All with a neutral view on endogenic systems and syscourse. Helpful for those who are just learning about DID/OSDD and want to get to the point or those who are sensitive to syscourse.
‧͙⁺˚*・༓☾ DID/OSDD Resource ☽༓・*˚⁺‧͙
by the 80s Rewinders System
Hello, and welcome to the DID/OSDD Resource! This has everything a singlet who is just starting to learn about DID/OSDD or a newly discovered system needs to know.
So first, a system, although its sometimes called a collective, is a collective term for a person with DID or Other Specified Dissociative Disorder 1b (also known as OSDD 1b.) Other specified dissociative disorder 1a can be considered a system, but theyre usually called medians. Now for a glossary of terms on DID/OSDD.
Glossary:
DID- dissociative identity disorder. This develops when a child under 6-8 is frequently exposed to traumatic events and it feels inescapable, so they dissociate. This stops the ego states everyone is born with from integrating into one whole identity, memory and consciousness. The ability to dissociate easily is needed along with trauma to develop any dissociative disorder.
OSDD- other specified dissociative disorder. there are a few subtypes but the subtypes that cause a system to develop are OSDD 1a and OSDD 1b. OSDD 1 is diagnosed when a person fits most of the criteria for DID except one of these: distinct alters or amnesia.
OSDD 1a- the identity is more faceted and the facets don't have their own identity; they are not differentiated. There is amnesia between them but they feel more like different sides of the same person than different people inside the person's head. Amnesia without distinct alters is cited as the reason for an OSDD 1a diagnosis.
OSDD 1b- there are distinct alters, but little to no amnesia between them. Amnesia of trauma and emotional amnesia still occur. Distinct alters without amnesia is cited as the reason for an OSDD 1b diagnosis.
Dissociation- a disconnection from identity, memory, thoughts, the body and surroundings. The forms of dissociation are depersonalization, derealization, dissociative amnesia, identity confusion and identity alteration. People with DID experience all forms of dissociation to some extent, and people with OSDD experience most of them to some extent.
Depersonalization- feeling like you're watching yourself inside or outside your body, losing control over your body as if you were being controlled and are mechanical, detached from your surroundings or like you're going through the motions of life with little conscious effort.
Derealization- the feeling people, objects, and/or the world might not be real, feeling dreamlike, or like you might not be real.
Dissociative amnesia- forgetting trauma, seconds, hours, minutes, weeks, months to even years of good or neutral memories, forgetting what you thought recently, forgetting your recent actions, or partially remembering things you should remember fully.
Identity confusion- not knowing who you really are, what you really like, having wildly different opinions on the same thing, things that are usually static in people changing quickly back and forth in you like your values and beliefs. Basically what it sounds like; you don't know who are supposed to be or what you truly like because of unstable sense of identity.
Identity alteration- the alters in DID/OSDD. Identity alteration can range from facets in OSDD 1a to distinct alters with their own autobiographical memory and amnesia in DID.
Zoning out- a common form of dissociation everyone experiences at least rarely. For people with dissociative disorders, zoning out is a moderate to almost daily occurrence. Zoning out is usually not considered pathological dissociation.
Median- feeling in between being a system and being a singlet. The alters are usually facets and not distinct from each other.
Singlet- a person without DID/OSDD. The ego states integrated into one identity, memory and consciousness in a singlet. This doesn't mean they can't be traumatized even in childhood. Not everyone who is traumatized as a child, even repetitive, develops DID/OSDD. Singlets can and often do have childhood trauma; it just didn't make them a system.
Now that we've got the general terms out of the way, its time for alter roles.
Host- in DID, the alter that fronts the most often. Host does not mean original or core; the theory of structural dissociation disproves the original/core theory. Alters are parts of one whole who developed independently, not split from a whole. The host can have trauma they remember contrary to popular belief. In most systems, the host changes a few times throughout the years but doesn't have to change more than once. Some hosts were always host since the system developed.
Protector- there are different types of protector alters. Physical, sexual, emotional, and internal, but mixed or all purpose protectors exist. They protect the body and/or the host during abuse or situations its seen as necessary.
Persecutor- an alter that harms the body, other alters, makes contact with abusers and usually does all of this to protect the system in a misguided way.
Comforter/Soother- an alter who comforts other alters. Usually during times of abuse, stress or flashbacks.
Caretaker- an alter that looks out after littles or other alters internally and/or helps take care of the body.
Gatekeeper- an alter that is like a manager; they can create or lower dissociative barriers, control which alters communicate and are aware of each other to some extent, put alters into dormancy and most famously bring different alters to front.
The following aren't alter roles, just types:
Little- an alter under 13.
Middle- alters aged 13-18.
Big- Alters aged 18 and over.
Ageless- alters who don't feel like they have an age.
Age Slider- an alter who changes between different ages.
Brainmade- an alter created entirely by the brain; it is not influenced by outside sources like friends or book characters.
Introject- an alter from another source outside of the body. This alter is not their source and is the brain's representation and idea of what that source is like. Introjects include fictives and factives.
Fictives- an introject alter from a fictional source.
Factives- an introject alter of another person. The stereotype is most factives are of abusers; this is absolutely not true. Factives can be of positive people like friends, family, or celebrities. They can also be of abusers but not all the time at all.
Tips for Newly Discovered Systems:
Call out for your alters in your head by asking "Is there anyone in here? " and waiting for an answer. When they tell you their names and information about themselves, write it or use Simply Plural or PluralKit to log it, log switches, and communicate.
Don't ask your alters about the trauma. If you know some of it, don't tell an alter that doesn't know it.
Don't share your diagnosis or system with anyone you don't trust and if you share it online, keep your legal identity and face offline. Be anonymous of sorts.
Tips for Singlets:
Don't use terms like multiple personality disorder, multiple personalities, split personality, or crazy to describe DID/OSDD or anyone who has it.
Don't watch media on DID/OSDD because none of it is correct and its all made by singlets glorifying or dramatizing the disorder for views and money. Namely Split, Sybil, and The Three Faces of Eve.
Don't get your information from media, including books, movies, TikTok or Reddit. Only trust scientific studies on DID/OSDD, medical journals and peoples documented lived experiences with DID/OSDD.
We hope this resource helps! Feel free to share it and bookmark it.
#dissociative identity disorder#actually dissociative#other specified dissociative disorder#osddid#dissociation
4 notes
·
View notes
Text
Okay so I have just gone down QUITE the rabbit hole today because as it turns out my migraine was not a migraine, it was a postural headache, and it turns out I was diagnosed with postural syncope as a child, and the fact that somehow posture/position is so consistently relevant to my symptoms I figured that might mean something and hoooooo boy does it.
So now I'm 19 symptoms deep for the differential diagnosis of things that cause both postural syncope and postural headaches and basically it.....doesn't look good. I'm trying not to think too hard about some of the worst options, but even the "good" ones don't have great outcomes for me
So. That's going to be a fun time for my new primary when I go in for a yearly physical and just drop a massive stack of symptoms related to total autoimmune/autonomic failure on their lap. Hope that doesn't fuck up my HRT plans!
27 notes
·
View notes
Text
Sadistic Personality Disorder (SaPD)
Note: You cannot be diagnosed with this disorder, as it's not in any diagnostic manual; you would be diagnosed with Other Specified Personality Disorder instead.
Criteria from the DSM-III-R (1987):
A. A pervasive pattern of cruel, demeaning, and aggressive behavior, beginning by early adulthood, as indicated by the repeated occurrence of at least four of the following:
has used physical cruelty or violence for the purpose of establishing dominance in a relationship (not merely to achieve some noninterpersonal goal, such as striking someone in order to rob them);
humiliates or demeans people in the presence of others;
has treated or disciplined someone under their control unusually harshly, e.g., a child, student, prisoner, or patient;
is amused by, or takes pleasure in, the psychological or physical suffering of others (including animals);
has lied for the purpose of harming or inflicting pain on others (not merely to achieve some other goal);
gets other people to do what they want by frightening them (through intimidation or even terror);
restricts the autonomy of people with whom they have a close relationship, e.g., will not let spouse leave the house unaccompanied or permit teen-age daughter to attend social functions;
is fascinated by violence, weapons, martial arts, injury, or torture
B. The behavior in A has not been directed toward only one person (e.g., spouse, one child) and has not been solely for the purpose of sexual arousal (as in Sexual Sadism).
Millon's subtypes:
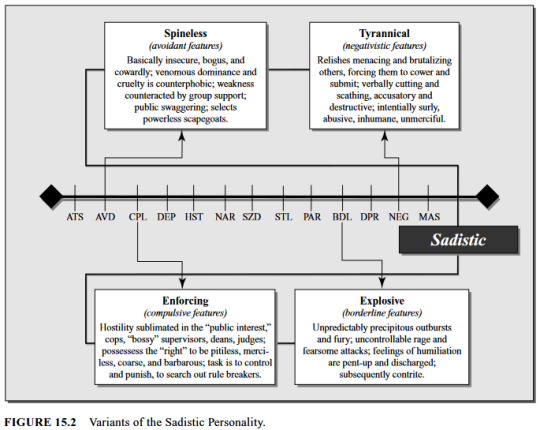
(Millon, ed.).
About SaPD
SaPD is similar to antisocial, negativistic / passive-aggressive, paranoid, and narcissistic PDs. It's part of what Millon & Bloom term the "Aggressive Personality Patterns", along with AsPD, NPD, & Negativistic / Passive-Aggressive PD.
Differential diagnoses include anxiety disorders, mood disorders, substance abuse, AsPD, psychotic disorders (especially with paranoid & persecutory features), and coercive sexual sadism disorder.
The most common PD comorbidities with SaPD are AsPD (36.45%), Negativistic / Passive-Aggressive PD (24.04%), & NPD (14.09%). The least common was OCPD (0.77%). Less than 1 percent (0.31%) had only ("pure") SaPD [less than those who had comorbid OCPD] (Millon & Bloom).
Millon defines it on a spectrum from assertive -> negativistic (Millon Personality Group); or alternatively from assertive [personality type] -> denigrating [style] -> sadistic [disorder] (Millon).
In the DSM-III-R it was described as being “characterized by pervasive cruel, demeaning, humiliating, and aggressive behavior directed toward others, along with a basic lack of empathy and respect for others" (Coolidge & Segal).
Millon also calls it "Aggressive Personality Disorder" (Millon & Bloom).
People with this disorder "might engage in risky behavior undaunted by danger, and [they] might be forward and inhibiting to others. This kind of person is often described as strongly opinionated, closed-minded, unbending, energetic, hardheaded, competitive, and malicious. [They] might be cold-blooded and detached from awareness of the impact of [their] own actions. Sexual energy might lead to imprudent and unseemly behavior" (Millon & Bloom).
People with SaPD are "socially aggressive and seek to dominate those around them", and "are likely to identify vulnerabilities in [people] and exploit them, producing strong fearful or painful emotional responses" (Millon & Bloom).
Not everyone with SaPD is violent, and some inflict pain by other non-physical means; "[t]he person may inflict pain or suffering by lying; for example, a woman may call her former husband and lie to him about their son's having been seriously hurt" (DSM-II-R).
"People with this disorder rarely experience depression, and their reaction to feeling abandoned is usually anger" (DSM-III-R).
SaPD is often caused by childhood trauma, especially domestic abuse (DSM-III-R). The underlying reason for symptoms is often pain avoidance; "[a]lthough sadistic individuals do seem to acquire a perverse pleasure in inflicting pain on others, the underlying motivation seems to be in their own pain avoidance by inflicting overwhelming pain on others before it can be done to them" (Millon & Bloom).
"... sadists may think of themselves as energetic, assertive, and realistic. What is dominating and callous to others is competitive and not overly sentimental to the sadist" (Millon, ed.).
SaPD only ever appeared in the appendix of the DSM-III-R, and if a person met criteria for this PD they were diagnosed with PDNOS (Coolidge & Segal).
"... it was dropped because of scientific concerns, such as the relatively low prevalence rate of the disorder in many settings. However, there were also political reasons. Physically abusive, sadistic personalities are most often male, and it was felt that any such diagnosis might have the paradoxical effect of legally excusing cruel behavior” (Millon, ed.).
References
Coolidge, Frederick L., & Segal, Daniel L., ‘Evolution of Personality Disorder Diagnoses in the Diagnostic and Statistical Manual of Mental Disorders’, Clinical Psychology Review, 1998, vol. 18, no. 5, pp. 585-599.
Millon, Theodore, & Bloom, Caryl, The Millon Inventories, 2008.
Millon, Theodore, Disorders of Personality, 2011.
Millon, Theodore, ed., Personality Disorders in Modern Life, 2004.
'Assertive / Sadistic Personality', Millon Personality Group, 2015, https://www.millonpersonality.com/theory/diagnostic-taxonomy/sadistic.htm.
#sadistic personality disorder#personality disorders#pd info#other specified personality disorder#ospd#dogpost#long post#described#described in alt text#dsm-iii-r#dsm iii r#dsm iii#dsm-iii
12 notes
·
View notes
Last Seen Blogs

coffee-creamer-doodles
*Rouge Simp*

tomc4t
F-14 Tomcat
corruptedtm-blog
INACTIVE. FIND ME @BUTTERFLYBURNED

millersheating
Miller's Heating

futureofscience-vn
Science Blog