#constitutional medical services
Text
Women won a battle over abortion rights in Montana on Friday, after the state Supreme Court upheld a lower court’s decision that a law banning advanced-practice registered nurses from performing early-stage abortions was unconstitutional.
Montana Supreme Court Judge Laurie McKinnon wrote in the court’s opinion that the “state has failed to meet its burden” showing that advanced-practice registered nurses (APRNs) providing abortion care “present a medically acknowledged, bona fide health risk. The state has failed to present any evidence that demonstrates abortions provided by APRNs include more risk than those provided by physicians and physicians assistants.”
McKinnon continued: “The district court correctly determined that no genuine dispute of material fact exists regarding the safety and efficacy of APRNs providing early abortion care.”
Plaintiffs Hellen Weems, owner of All Families Healthcare in Whitefish, and another woman identified as Jane Doe, are both APRNs. Weems did not respond to a request for comment by press time.
Medication and aspiration are the most common forms of early abortion care. The medications used are mifepristone and misoprostal. An aspiration abortion involves inserting a tube through the cervix into the uterus and using suction to remove uterine contents.
The state argued that while APRNs can perform an abortion, they are not trained to handle complications that may arise.
One of the state's experts, Dr. George Mulcaire-Jones, a family medicine and obstetrics physician in Butte, said the aspiration method involves the removal of tissue from the uterus with instruments, which can cause bleeding, cramping and possible infection. He said that there is an unacceptable risk to women when the abortions are performed without emergency backup policies, such as when APRNs perform the procedures in their offices.
Mulcaire-Jones also said that even medication abortions carry risks, including hemorrhage and bleeding, which could require surgical care beyond what a APRN could provide.
Bolstering Mulcaire-Jones’ views was Dr. Kathi Aultman, an ob-gyn licensed in Florida who serves as a fellow of the American College of Obstetrics and Gynecologists.
“Allowing less qualified practitioners to perform abortions, especially when they cannot handle the serious and life-threatening complications that can occur, creates an unacceptable risk for patients at any location, which expands exponentially in rural area without the necessary facilities and expertise to handle complications,” Aultman said.
One of the plaintiff’s experts, Dr. Suzan Goodman, disagreed.
“Legal abortion is one of the safest medical procedures in the United States. Complication rates of abortion are similar to or lower than other outpatient procedures,” Goodman, a California-licensed family medicine physician with a master's degree in public health, said.
The state Board of Medical Examiners has previously concluded that “medication and aspiration abortion procedures are not significantly different than the procedures, medications and surgeries the nurse practitioners currently perform without significant issues.”
McKinnon ultimately sided with the plaintiffs, citing the Montana Constitution's guarantee of the right of privacy to seek abortion care.
"The state argues that, while APRNs may be able to perform the abortion procedure, they are not capable or qualified to handle the 'unacceptable' risk of complications arising from an abortion. However, the same risk of complications exists in miscarriage care, which the state has not argued presents a threat to public health and safety when performed by APRNs," she wrote.
#us politics#news#courthouse news service#2023#montana#Montana Supreme Court#advanced-practice registered nurses#early-stage abortions#abortions#abortion bans#Judge Laurie McKinnon#aspiration abortions#medication abortions#Montana Constitution#reproductive health#reproductive rights
39 notes
·
View notes
Note
hey you might've been asked this before sorry if so, but have you read or do you have any thoughts on A short history of Trans Misogyny?
I have read it! I have a few thoughts.
I think it's a strong and important work that compiles historical archives into sharp analyses of how "trans misogyny" (using Jules Gill-Peterson's spacing) is not a recent phenomenon but a globalized structure with centuries of history. I also think it's flawed, for reasons I'll get into after a quick summary for those who haven't had the chance to read it yet.
JGP divides the book into three main chapters, the first on the notion of "trans panic". There, she traces how variants of this anxiety with the trans-feminized subject have presented—to deadly effect, for the subject—in such different settings as early colonial India, the colonization of the Americas, the racialized interactions between US soldiers stationed in the Philippines and the local trans women living there, and of course the contemporary United States itself. In every case she analyzes this "panic" as the reaction of the capitalist colonial enterprise to the conceptual threat that the trans-feminized subject poses; we are a destabilizing entity, a gender glitch that undermines the rigid guarantees of the patriarchal order maintaining capitalism. Punishment follows.
The second chapter is my favourite, and considers the relationship between transfeminine life and sex work. I posted a concluding excerpt but the thrust of the chapter is this: that the relegation of so many trans women and trans-feminized people to sex work, while accompanied by the derogation and degradation that is associated with sex work, is not itself the mere result of that degradation inflicted upon the subject. In other words, it is not out of pure helplessness and abjection that so many trans-feminized people are involved in sex work. Rather, sex work is a deliberate and calculated choice made by many trans-feminized people in increasingly service-based economies that present limited, often peripheralized, feminized, and/or reproductive, options for paid labour. Paired with a pretty bit of critical confabulation about the histories of Black trans-feminized people travelling the US in the 19th century, I think this made for great reading.
In her third chapter, JGP narrativizes the 20th century relationship between the "gay" and "trans" movements in north america—scare quoted precisely because the two went hand-in-hand for much of their history. She emphasizes this connection, not merely an embedding of one community within another but the tangled mutualism of experiences and subjectivities that co-constituted one another, though not without tension. Then came the liberal capture of the gay rights movement around the 70s, which brought about the famous clashes between the radicalisms of Silvia Rivera and Marsha P Johnson (neither of whom, JGP notes, ever described themselves as trans women) and the institutions of gay liberalism that desired subsumption into the folds of capital. This is a "remember your history" type of chapter, and well-put.
I think JGP is correct to insist, in her introduction, on the globalizing-in-a-destructive-sense effects of the colonial export of trans womanhood. It is, after all, an identity conceived only mid-century to make sense of the medicalized trans subject; and "gender identity" itself (as JGP describes in Histories of the Transgender Child) is a psychomedical concept conceived to rein in the epistemic instability of trans existence. This is critical to keep in mind! But I also think JGP makes a few mistakes, and one of them has to do with this point.
In her first chapter, under the discussion of trans misogyny in colonial India, JGP of course uses the example of the hijra. Unfortunately, she commits two fundamental errors in her use: she mythologizes, however ambiguously, the "ascetic" lives of hijra prior to the arrival of British colonialism; and she says "it's important to say that hijras were not then—and are not today—transgender". In the first place, the reference to the "ascetism" of hijra life prior to the violence of colonialism is evocative of "third-gender" idealizations of primeval gender subjectivities. To put the problem simply: it's well and good to describe the "ritual" roles of gendered subjects people might try to construe contemporarily as "trans women", the priestesses and oracles and divinities of yore. But it is best not to do so too loftily. Being assigned to a particular form of ritualistic reproductive labour because of one's failure to be a man and inability to perform the primary reproductive labour of womanhood-proper is the very marker of the trans-feminized subject. "Ascetism" here obviates the reality that it wasn't all peachy before (I recommend reading Romancing the Transgender Native on this one). Meanwhile, in the after, it is just wrong that hijra are universally not transgender. Many organize specifically under the banners of transfeminism. It's a shame that JGP insists on keeping the trans-feminized life of hijra so firmly demarcated from what she herself acknowledges is globalized transness.
My second big complaint with the book is JGP's slip into a trap I have complained about many times: the equivocation of transfemininity with femininity (do you see why I'm not fond of being described as "transfem"?). She diagnoses the root of transmisogyny as a reaction to the femininity of trans women and other trans-feminized subjects. In this respect she explicitly subscribes to a form of mujerísima, and of the trans-feminized subject as "the most feminine" and (equivalent, as far as she's concerned) "the most woman". Moreover, she locates transfeminist liberation in a singular embrace of mujerísima as descriptive of trans-feminized subjectivity. As I've discussed previously, I think this is a misdiagnosis. Feminization is, of course, something that is done to people; it is certainly the case that the trans-feminized subject is in this way feminized for perceived gender-failure. This subject may simultaneously embrace feminized ways of being for all sorts of reasons. In both cases I think the feminization follows from, rather than precedes, the trans misogyny and trans-feminization, and there is a fair bit of masculinization as de-gendering at play too, to say nothing of the deliberate embrace of masculinity by "trans-feminized" subjects. Masculinity and femininity are already technologies of gender normalization—they are applied against gender deviation and adapted to by the gender deviant. The deviation happens first, in the failure to adhere to the expectations of gender assignment, and I don't think these expectations can be summarized by either masculinity or femininity alone. I think JGP is effectively describing the experience of many trans-feminized people, but I do not think what she presents can be the universalized locus of trans liberation she seems to want it to be.
Now for a pettier complaint that I've made before, but one that I think surfaces JGP's academic context. In her introduction she says:
In truth, everyone is implicated in and shaped by trans misogyny. There is no one who is purely affected by it to the point of living in a state of total victimization, just as there is no one who lives entirely exempt from its machinations. There is no perfect language to be discovered, or invented, to solve the problem of trans misogyny by labeling its proper perpetrator and victim.
Agreed that "there is no perfect language to be discovered"! But JGP is clearly critical of TMA/TME language here. Strange, then, that less than ten pages later she says this:
this book adds the phrase trans-feminized to describe what happens to groups subjected to trans misogyny though they did not, or still do not, wish to be known as transgender women.
So JGP believes it is coherent to talk about "groups subjected to trans misogyny", which she thinks consists of the union of trans women and what she called "trans-feminized" groups. If this is to be coherent, there must be groups not subjected to trans misogny. So we've come around to transmisogyny-subjected and not transmisogyny-subjected. Look: you cannot effectively theorize about transmisogyny without recognizing that its logic paints a particular target, and you will need to come up with a concise way of making this distinction. But JGP dismissing TMA/TME with skepticism about "perfect language" and immediately coining new language (basically TMS/not TMS) to solve the problem she un-solved by rejecting TMA/TME... it smells of a sloppy attempt to make a rhetorical point rather than theoretical rigour. It's frustrating.
I have other minor gripes, like her artificial separation of "trans women" from "nonbinary people" (cf. countless posts on here lamenting the narrow forms of existence granted TMA people if we want recognition as-such!) or her suggestion that "a politics of overcoming the gender binary" is mutually exclusive from rather than necessarily involved with struggles around "prison abolition, police violence, and sex work". Little things that give me the sense of theoretical tunnel-vision. But I don't think all this compromises the book's strengths as a work of broad historical analysis. I would simply not take every one of its claims as authoritative. Definitely give it a read if you have the chance, especially for the second and third chapters.
#ask answer#jules gill-peterson#(i haven't been asked this before ty for asking <3 🐐)#note that this was mostly off the cuff except what i had taken pictures of bc i left the book in toronto for my mom to read
271 notes
·
View notes
Text
By: Andy L.
Published: Apr 14, 2024
It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Many trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics”, including Andrew Wakefield, has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
-
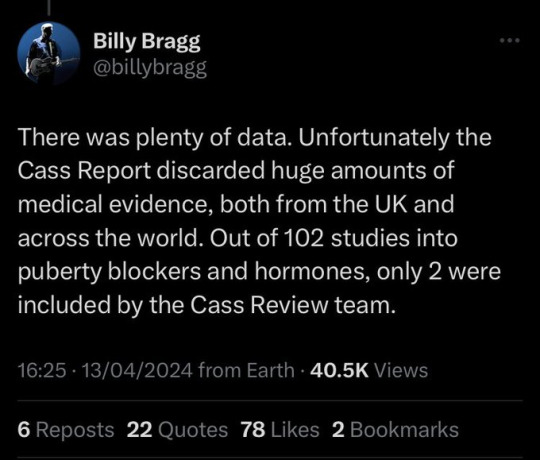
Myth 1: 98% of all studies in this area were ignored
Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
The Review states,
The systematic review on interventions to suppress puberty (Taylor et al: Puberty suppression) provides an update to the NICE review (2020a). It identified 50 studies looking at different aspects of gender-related, psychosocial, physiological and cognitive outcomes of puberty suppression. Quality was assessed on a standardised scale. There was one high quality study, 25 moderate quality studies and 24 low quality studies. The low quality studies were excluded from the synthesis of results.
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.
12 cohort, 9 cross-sectional and 32 pre–post studies were included (n=53). One cohort study was high-quality. Other studies were moderate (n=33) and low-quality (n=19). Synthesis of high and moderate-quality studies showed consistent evidence demonstrating induction of puberty, although with varying feminising/masculinising effects. There was limited evidence regarding gender dysphoria, body satisfaction, psychosocial and cognitive outcomes, and fertility.
Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,
One emerging criticism of the Cass review is that it set the methodological bar too high for research to be included in its analysis and discarded too many studies on the basis of quality. In fact, the reality is different: studies in gender medicine fall woefully short in terms of methodological rigour; the methodological bar for gender medicine studies was set too low, generating research findings that are therefore hard to interpret. The methodological quality of research matters because a drug efficacy study in humans with an inappropriate or no control group is a potential breach of research ethics. Offering treatments without an adequate understanding of benefits and harms is unethical. All of this matters even more when the treatments are not trivial; puberty blockers and hormone therapies are major, life altering interventions. Yet this inconclusive and unacceptable evidence base was used to inform influential clinical guidelines, such as those of the World Professional Association for Transgender Health (WPATH), which themselves were cascaded into the development of subsequent guidelines internationally.
-
Myth 2: Cass recommended no Trans Healthcare for Under 25s
Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
Taking account of all the above issues, a follow-through service continuing up to age 25 would remove the need for transition at this vulnerable time and benefit both this younger population and the adult population. This will have the added benefit in the longer-term of also increasing the capacity of adult provision across the country as more gender services are established.
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
-
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”
Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions

The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1.
Explainer on the Newcastle Ottawa Scale
The Newcastle-Ottawa Scale (NOS) is a tool designed to assess the quality of non-randomized studies, particularly observational studies such as cohort and case-control studies. It provides a structured method for evaluating the risk of bias in these types of studies and has become widely used in systematic reviews and meta-analyses.
The NOS consists of a set of criteria grouped into three main categories: selection of study groups, comparability of groups, and ascertainment of either the exposure or outcome of interest. Each category contains several items, and each item is scored based on predefined criteria. The total score indicates the overall quality of the study, with higher scores indicating lower risk of bias.
This scale is best applied when conducting systematic reviews or meta-analyses that include non-randomized studies. By using the NOS, researchers can objectively assess the quality of each study included in their review, allowing them to weigh the evidence appropriately and draw more reliable conclusions.
One of the strengths of the NOS is its flexibility and simplicity. It provides a standardized framework for evaluating study quality, yet it can be adapted to different study designs and research questions. Additionally, the NOS emphasizes key methodological aspects that are crucial for reducing bias in observational studies, such as appropriate selection of study participants and controlling for confounding factors.
Another advantage of the NOS is its widespread use and acceptance in the research community. Many systematic reviews and meta-analyses rely on the NOS to assess the quality of included studies, making it easier for researchers to compare and interpret findings across different studies.
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
The national infrastructure should be put in place to manage data collection and audit and this should be used to drive continuous quality improvement and research in an active learning environment.
-
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.

Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:
Estimates of the percentage of individuals who embark on a medical pathway and subsequently have regrets or detransition are hard to determine from GDC clinic data alone.
There are several reasons for this:
Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
Gender dysphoria during childhood does not inevitably continue into adulthood. Rather, in follow-up studies of prepubertal children (mainly boys) who were referred to clinics for assessment of gender dysphoria, the dysphoria persisted into adulthood for only 6–23% of children.
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
==
It's not so much "myths and misconceptions" as deliberate misinformation. Genderists are scrambling to prop up their faith-based beliefs the same way homeopaths do. Both are fraudulent.
#Andy L.#Cass Review#Cass Report#Dr. Hilary Cass#Hilary Cass#misinformation#myths#misconceptions#detrans#detransition#gender affirming healthcare#gender affirming care#gender affirmation#affirmation model#medical corruption#medical malpractice#medical scandal#systematic review#religion is a mental illness
245 notes
·
View notes
Text
From the Palestinian Red Crescent's twitter, 13 November 2023:
🔴 Al-Quds Hospital still under intense gunfire.
🔴 The IDF claims to be attacking a "Hamas terrorist" who is firing a rocket-propelled grenade launcher from Al-Quds.
🔴 The main power generator at Al-Amal Hospital stopped working. The hospital is currently relying on a very small generator to supply electricity only to the maternity ward and emergency lighting. Remaining fuel is expected to run out within the next 24 hours.
11:01 AM:
"🚨 The vicinity of Al-Quds Hospital 🏥 is still witnessing intense gunfire, with the presence of Israeli military vehicles. Our staff are trapped with patients and the wounded, without electricity, water, or food. We hope for their safety. 🙏"
1:10 PM, in response to this tweet from @IDF:

[ID: Tweet by Israel Defense Forces (@IDF) at 3:22pm on November 13 reading: "What could these Hamas terrorists possibly be doing with an RPG at the Quds Hospital?" Attached is a 20-second drone video of the hospital with overlaid text reading "Enemy fire from the entrance of the 'Al-Quds' Hospital towards IDF troops: terrorist with RPG launcher."
The PRCS issued a statement reading:
🚨 The Palestine RCS strongly condemns the false claims by the occupying forces about armed individuals launching projectiles from inside Al-Quds Hospital. The PRCS sees these claims as a blatant attempt to incite further targeting and besieging of the hospital, constituting a clear violation of international humanitarian law.
❌ PRCS rejects these baseless allegations, as the published video clearly shows that the armed individuals approached from the street while the occupation tanks were stationed in front of and shielded by the hospital, endangering the lives of medical teams and patients. The PRCS confirms that there are no armed individuals inside the hospital, and no shots have been fired from within. Everyone within the hospital are patients, their families, and the medical staff.
📣 PRCS calls on the international community to intervene immediately to protect its teams besieged inside the hospital, facing imminent danger with each passing moment.
4:22 PM:
"🛑 Today's attempt to evacuate Al-Quds Hospital failed after the IOF decided to return the designated evacuation convoy to the association's branch in Khan Younis, despite receiving prior approval.
"🚨 The decision was rationalized by referring to a security incident in the vicinity, despite the convoy undergoing thorough inspection. It is noteworthy that yesterday, displaced individuals were allowed to exit through a route specified by the occupation forces, under specific and challenging conditions.
"🧑⚕ Our medical teams, patients,and the wounded, along with their companions, remain trapped inside the hospital without food, water, or electricity, and their is 300 person."
4:49 PM:
"🚨 ⚠️ Today, the sole power generator at Al-Amal Hospital, affiliated with the PRCS in Khan Younis, stopped working. This threatens the lives of 90 patients receiving treatment, including 25 in the medical rehabilitation section who now face the risk of death at any moment. Additionally, around 9,000 displaced individuals have sought refuge in the PRCS premises and the hospital.
" 🏥 The hospital is currently relying on a very small generator to supply electricity only to the maternity ward and emergency lighting. It's important to note that the remaining fuel is expected to run out within the next 24 hours.
"🛑 The power generator's failure is impacting the operations of both the PRCS headquarters and Al-Amal Hospital, which includes the emergency operations room for the Gaza Strip. This has resulted in a loss of communication with the operation rooms scattered across the Gaza sector and the cessation of VHF communication services."
350 notes
·
View notes
Text
(CNN) - In new clarifying guidance announced Monday, the Biden Administration said that federal law preempts state abortion bans when emergency care is needed, and that the federal government can penalize institutions or providers that fail to provide necessary abortions to treat medical emergencies.
"Under the law, no matter where you live, women have the right to emergency care — including abortion care," HHS Secretary Xavier Becerra said in a news release Monday. "Today, in no uncertain terms, we are reinforcing that we expect providers to continue offering these services, and that federal law preempts state abortion bans when needed for emergency care."
In more than a dozen states, legal fights are underway over abortion bans and other laws that strictly limit the procedure after the US Supreme Court ended a constitutional right to an abortion on June 24.
In a letter to the nation's health care providers on Monday, Becerra said a federal statute called the Emergency Medical Treatment and Active Labor Act (EMTALA) protects providers' clinical judgement and the actions they take to provide stabilizing treatment to pregnant patients who are experiencing emergency medical conditions, regardless of restrictions in any given state.
EMTALA has been on the books since 1986. It specifically requires all patients get the appropriate medical screening, examination, stabilizing treatment and transfer to an appropriate facility if necessary.
The administration said examples of emergency medical conditions may include, but are not limited to, ectopic pregnancy -- when the fertilized egg grows outside a woman's uterus -- and complications of miscarriages. Stabilizing treatment could include abortion.
Becerra said if a state law bans abortion and does not include an exception for the life and health of the pregnant person, that state law is preempted by the federal statute.
"We heard a lot from physicians that we needed to be clearer on these points because people were still too scared to treat people," a senior adviser with HHS said in a background briefing with the media. The guidance today is "meant to try to provide that reassurance here on the clinical judgment of these physicians and hospitals."
HHS said it will do everything within its authority to ensure patients get the care they need.
The statute applies to emergency departments and other specific clinical settings. Providers also will not have to wait for a patient's condition to worsen to be protected by this statute.
If a hospital is found in violation of this statute, a hospital could lose its Medicare and Medicaid provider agreements and could face civil penalties. An individual physician could also face civil penalties if they are found in violation.
Under the statute HHS may impose a $119,942 fine per violation for hospitals with over 100 beds, $59,973 for hospitals under 100 beds. A physician could face a $119,942 fine per violation.
"We are making enforcement a priority," a senior HHS official said.
A memo from the Centers for Medicare and Medicaid Services said that hospitals should ensure that all staff who may encounter an emergency situation with a pregnant person be aware of the hospital's obligation under EMTALA.
The statute also contains a whistleblower provision that prevents retaliation by the hospital against its employee who refuses to transfer a patient with an emergency medical condition that has not been stabilized by the hospital. A link on the CMS website allows people to file an EMTALA complaint.
The enforcement of EMTALA depends on people making a complaint to the government. An investigation can only follow if a complaint is made.
"Health care must be between a patient and their doctor, not a politician," said Becerra in a news release. "We will continue to leverage all available resources at HHS to make sure women can access the life-saving care they need."
3K notes
·
View notes
Text
Breaking Down Cass Review Myths and Misconceptions: What You Need to Know.
An answer when some tranny or handmaiden disputes the review. (long post with lots of facts!)
Via The Quakometer:
It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Many trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics”, including Andrew Wakefield, has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
Myth 1: 98% of all studies in this area were ignored.

Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation.
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
The Review states,
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.

Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,

Myth 2: Cass recommended no Trans Healthcare for Under 25s.

Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”.

Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions

The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1. Explainer on the Newcastle Ottawa Scale
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.

Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:

Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
#Cass report#the cass report#cass review#the cass review#trans lies#gender critical#tras#medical malpractice#the tide is turning
71 notes
·
View notes
Text
🟢 Hamas:
—
In the name of Allah, the Most Gracious, the Most Merciful
The announcement by the administration of Kamal Adwan Hospital in the Northern Gaza Strip governorate that it is out of service due to the depletion of fuel supplies exacerbates the health and humanitarian situation of our people in the northern part of the Strip. This has led to the martyrdom of many patients due to the lack of medical care and medicine, in addition to the martyrdom of four children in the hospital due to dehydration and malnutrition. This constitutes an international failure to protect humanity from the crimes of the criminal zionist entity that imposes a tight siege on the northern part of the Strip.
The international community and the United Nations are required to take responsibility and fulfill their legal duties by taking all measures to stop this Nazi entity from committing genocide and ethnic cleansing against our Palestinian people in the Gaza Strip, especially in the Gaza and the North governorates, in full view of the entire world.
We also demand all concerned parties, including UN agencies, to urgently act to deliver emergency food supplies to our people in the northern part of the Strip, who are subjected to systematic starvation by the criminal enemy that disregards any humanitarian standards or ethical norms in its comprehensive war against our people.
Islamic Resistance Movement - Hamas
Wednesday: 18 Sha'ban 1445H
Corresponding to: February 28, 2024
[via RNN]
#hamas#palestinian resistance#palestine#free palestine#gaza#free gaza#israel#iof#idf#iof terrorism#war crimes#jerusalem#tel aviv#gaza strip#joe biden#benjamin netanyahu#gaza update#gaza news
54 notes
·
View notes
Text
Detransitioner news
I have been thinking about detransitioners lately and wanted to compile articles I have been seeing. This will be a longer post and reblogged for part II as I hope to copy and paste brief portions of the articles under each headline.
Law firm for detransitioners opens in Dallas

In all of the controversy around gender transition, there is one group that is persistently marginalized by both the right and left.
They are known as detransitioners — people who decide that they want to return to their birth gender, often after receiving years of interventional care, including surgery, to treat their gender dysphoria.
Now, the nation’s first law firm focused solely on representing these patients — many of whom feel abused by a medical system that encouraged their treatment — has opened its doors in Dallas.
It could forever change how hospitals and doctors approach what’s known as gender-affirming care.
Archive link
Fenway Community Health Center in Boston, the largest provider of transgender medicine in New England and one of the leading institutions of its kind in the United States, was named a defendant in a lawsuit filed last month. The plaintiff, a gay man who goes by the alias Shape Shifter, argues that by approving him for hormones and surgeries, Fenway Health subjected him to “gay conversion” practices, in violation of his civil rights. Carlan v. Fenway Community Health Center is the first lawsuit in the United States to argue that “gender-affirming care” can be a form of anti-gay discrimination.
The case underscores an important clinical reality: gender dysphoria has multiple developmental pathways, and many who experience it will turn out to be gay. Even the Endocrine Society concedes that many of the youth who outgrow their dysphoria by adolescence later identify as gay or bisexual. Decades of research confirm as much. Gender clinicians in the U.K. used to have a “dark joke . . . that there would be no gay people left at the rate [the Gender Identity Development Service] was going,” former BBC journalist Hannah Barnes reported. Rather than help young gay people to accept their bodies and their sexuality, what if “gender-affirming” clinicians are putting them on a pathway to irreversible harm?
Due partly to Shape’s lifelong difficulty in accepting himself as gay, his lawyers are not taking the usual approach to detransition litigation. Rather than state a straightforward claim of medical malpractice or fraud, they allege that Fenway Health has violated Section 1557 of the Affordable Care Act (ACA), which bans discrimination “on the basis of sex” in health care. In 2020, the Supreme Court ruled in Bostock v. Clayton County that “discrimination because of . . . sex” includes discrimination based on homosexuality. Citing this and other precedents, Shape’s lawyers argue that federal law affords distinct protections to gay men and lesbians—upon which clinics that operate with a transgender bias are trampling.
Shape grew up in a Muslim country in Eastern Europe that he describes in an interview as “very traditional” and “homophobic.” His parents disapproved of his effeminate demeanor and interests as a child. They wouldn’t let him play with dolls, and his mother, he says, made him do stretches so that he would grow taller and appear more masculine.
At 11, Shape had his first of several sexual encounters with older men. “I was definitely groomed,” he recounts. Shape proceeded to develop a pattern of risky sexual behavior, according to his legal complaint. He told his medical team at Fenway Health about his childhood sexual experiences, calling them “consensual.” The Fenway providers never challenged him on this interpretation, he alleges. They never suggested that he might have experienced sexual trauma or, say, explored how these events might have shaped his feelings of dissociation. (The irony is that Fenway Health describes its model of care as “trauma-informed.”)
Archive link
Ontario detransitioner who had breasts and womb removed sues doctors

An Ontario detransitioning woman who had her breasts and womb removed to change her gender to male is suing medical and health practitioners for failing to consider other treatments during her mental health crisis before ushering her on an irreversible journey she regrets.
Michelle Zacchigna, 34, of Orillia, Ont., north of Toronto, names eight health professionals, including doctors, psychologists, a psychotherapist and a counsellor in a lawsuit filed in Ottawa.
None of the defendants, who work or worked at various clinics and institutions in southern Ontario, responded to requests for comment on the lawsuit prior to deadline. Four of the defendants have filed notices of intent to defend against the suit in Ontario Superior Court, but no statements of defense have been filed. None of the claims have been tested in court.
Zacchigna said she faces an uphill battle in her lawsuit.
“I’ve been under the impression that all medical malpractice suits are challenging. Doctors win the majority of cases in Canada,” she told National Post.
“It’s very much a David vs. Goliath undertaking.”
In her statement of claim filed in court in November, Zacchigna says she had difficulty forming relationships with classmates in elementary school and was often bullied.
By the time she was 11, she engaged in self-harming behaviour, including cutting her arm with a knife. This continued into early adulthood.
When she was 20, she tried to kill herself and she was referred by her family doctor for psychotherapy, where she was treated for social anxiety and clinical depression.
She remained unhappy and depressed, and her mental health decline led to her dropping out of university, according to her claim.
About a year into therapy, she engaged with an online community around gender nonconformity.
“Michelle came to believe that her biological sex of female did not match her true gender identity of male,” her claim says.
“She further came to believe that this mismatch between her biological sex and gender identity was causing her feelings of depression, self-harming behaviour and unease in her body, a mental health condition commonly known as gender dysphoria,” her claim states.
This was the first time Zacchigna felt she was born in the wrong body, and she had not previously identified as male, her claim says.
“However, as a result of what she read on the internet, she became convinced that she was a transgender man, and that once she embraced this new identity, her depression would subside.”
Zacchigna started attending a support group in Toronto for people considering gender transition. A counsellor there told her of opportunities to proceed through a medical transition, her claim says.
Zacchigna was invited to apply for medical intervention in 2010.
The counsellor wrote a recommendation letter outlining a medical history that didn’t fully match her real past, the claim says. The counsellor didn’t recommend any alternatives, or seek confirmation of Zacchigna’s own diagnosis of gender dysphoria.
Her regular therapist also wrote a recommendation for transition treatment, saying Zacchigna was an “ideal candidate for hormone therapy,” even though the therapist had no previous transgender clients, according to the claim.
Part II incoming.
#detrans#detransition#desist#ftm detransition#mtf detransition#LGB#gender critical#gender critical feminism#gender ideology
75 notes
·
View notes
Text
"...a responsibility that does not expire with time".
🟢 Hamas:
—
In the name of Allah, the Most Gracious, the Most Merciful
The Pentagon’s claim that Hamas is using Al-Shifa Hospital for military purposes, without knowing the exact location or time of use, and then the U.S. State Department’s allegation that Hamas is using hospitals and schools as military sites, is a repetition of a blatant false narrative, exposed by the flimsy and ridiculous theatrics of the spokesperson for the occupying army, after their raid on Al-Rantisi and Al-Shifa hospitals, and threatening the safety of patients and medical staff.
The insistence on lying, and ignoring the movement’s and Al-Shifa Hospital’s call to the United Nations and international institutions to form an international committee to inspect the hospitals and schools to confirm the falsehood of the occupation’s narrative, indicates the responsibility of the U.S. administration and its partnership with the occupation in the war crimes and genocide that our people in the Gaza Strip are subjected to, and constitutes a new U.S. cover for the continued aggression on the medical sector to destroy it with the aim of displacing our people.
We would like to remind President Biden and his administration that the occupation bombed most hospitals, cut off their electricity, fuel, and medicine, leading to 26 out of 35 hospitals being out of service, and the occupation also bombed 255 schools, including UNRWA schools housing displaced people under international care and protection, as witnessed by UNRWA and many international organizations.
The indulgence in lying and giving the green light to the occupation to commit more crimes and massacres, holds you politically and legally responsible, a responsibility that does not expire with time.
Islamic Resistance Movement - Hamas
Friday
03 Jumada al-Awwal 1445H
Corresponding to November 17, 2023
#hamas#palestine#resistance#israel is committing genocide#israeli terrorism#israel is a terrorist state#israel#intifada#genocide
59 notes
·
View notes
Text
My own experience as a transsexual parallels the monster’s in this regard. The consciousness shaped by the transsexual body is no more the creation of the science that refigures its flesh than the monster’s mind is the creation of Frankenstein. The agenda that produced hormonal and surgical sex reassignment techniques is no less pretentious, and no more noble, than Frankenstein’s. Heroic doctors still endeavor to triumph over nature. The scientific discourse that produced sex reassignment techniques is inseparable from the pursuit of immortality through the perfection of the body, the fantasy of total mastery through the transcendence of an absolute limit, and the hubristic desire to create life itself. Its genealogy emerges from a metaphysical quest older than modern science, and its cultural politics are aligned with a deeply conservative attempt to stabilize gendered identity in service of the naturalized heterosexual order.
None of this, however, precludes medically constructed transsexual bodies from being viable sites of subjectivity. Nor does it guarantee the compliance of subjects thus embodied with the agenda that resulted in a transsexual means of embodiment. As we rise up from the operating tables of our rebirth, we transsexuals are something more, and something other, than the creatures our makers intended us to be. Though medical techniques for sex reassignment are capable of crafting bodies that satisfy the visual and morphological criteria that generate naturalness as their effect, engaging with those very techniques produces a subjective experience that belies the naturalistic effect biomedical technology can achieve. Transsexual embodiment, like the embodiment of the monster, places its subject in an unassimilable, antagonistic, queer relationship to a Nature in which it must nevertheless exist. (...)
To encounter the transsexual body, to apprehend a transgendered consciousness articulating itself, is to risk a revelation of the constructedness of the natural order. Confronting the implications of this constructedness can summon up all the violation, loss, and separation inflicted by the gendering process that sustains the illusion of naturalness. My transsexual body literalizes this abstract violence. As the bearers of this disquieting news, we transsexuals often suffer for the pain of others, but we do not willingly abide the rage of others directed against us. And we do have something else to say, if you will but listen to the monsters: the possibility of meaningful agency and action exists, even within fields of domination that bring about the universal cultural rape of all flesh. Be forewarned, however, that taking up this task will remake you in the process.
By speaking as a monster in my personal voice, by using the dark, watery images of Romanticism and lapsing occasionally into its brooding cadences and grandiose postures, I employ the same literary techniques Mary Shelley used to elicit sympathy for her scientist’s creation. Like that creature, I assert my worth as a monster in spite of the conditions my monstrosity requires me to face, and redefine a life worth living. I have asked the Miltonic questions Shelley poses in the epigraph of her novel: “Did I request thee, Maker, from my clay to mould me man? Did I solicit thee from darkness to promote me?” With one voice, her monster and I answer “no” without debasing ourselves, for we have done the hard work of constituting ourselves on our own terms, against the natural order. Though we forego the privilege of naturalness, we are not deterred, for we ally ourselves instead with the chaos and blackness from which Nature itself spills forth.
My Words to Victor Frankenstein above the Village of Chamounix: Performing Transgender Rage, Susan Stryker (1994) [pdf]
32 notes
·
View notes
Text
Abortion in South Africa is legal on request during the first 12 weeks of pregnancy, and under certain conditions afterwards. Abortion is provided free at government hospitals and a tele-medical or 'pills by post' service is provided by Marie Stopes South Africa and Abortion Clinic Johannesburg.
In South Africa, a woman of any age can get an abortion on request with no reasons given if she is less than 12 weeks pregnant. If she is between 13 and 20 weeks pregnant, she can get the abortion if (a) her own physical or mental health is at stake, (b) the baby will have severe mental or physical abnormalities, (c) she is pregnant because of incest, (d) she is pregnant because of rape, or (e) she is of the personal opinion that her economic or social situation is sufficient reason for the termination of pregnancy. If she is more than 20 weeks pregnant, she can get the abortion only if her or the fetus' life is in danger or there are likely to be serious birth defects.
A woman under the age of 18 will be advised to consult her parents, but she can decide not to inform or consult them if she so chooses. A woman who is married or in a life-partner relationship will be advised to consult her partner, but she can decide not to inform or consult him/her. An exception is that if the woman is severely mentally ill or has been unconscious for a long time, where consent of a life-partner, parent or legal guardian is required.
The Constitution does not explicitly mention abortion, but two sections of the Bill of Rights mention reproductive rights. Section 12(2)(a) states that, "Everyone has the right to bodily and psychological integrity, which includes the right ... to make decisions concerning reproduction," while section 27(1)(a) states "Everyone has the right to have access to ... health care services, including reproductive health care." In the case of Christian Lawyers Association v Minister of Health an anti-abortion organisation challenged the validity of the Choice on Termination of Pregnancy Act on the basis that it violated the right to life in section 11 of the Bill of Rights; the Transvaal Provincial Division of the High Court dismissed their argument, ruling that constitutional rights only apply to born people and not to fetuses.
Health workers are under no obligation to perform or take active part in an abortion if they do not wish to; however, they are obligated by law to assist if it is required to save the life of the patient, even if the emergency is related to an abortion. A health worker who is approached by a woman for an abortion may decline if they choose to do so, but are obligated by law to inform the woman of her rights and refer her to another health worker or facility where she can get the abortion.
1K notes
·
View notes
Text
Queer Charecters in One Peice.
The queer community lives and dies but those who remain in sight. What constitutes this sight? From top down, it's Activism. Advocating for yourself, those around you and those you will never see. Community, advocating for yourself and those around you. Then there is seeing yourself as something worthy of protecting, worthy of expression. Worthy to speak in your own defense. That was an exceedingly pretentious opening for a post regarding one piece and its themes but I do believe that it's a good flat layer in which we can build our understanding of the importance of seeing Militant Queer characters.
To be militant means to be combative and aggressive in support of a political or social cause, often in favor of extreme and confrontational methods. It is often shown to be a negative state of being. Survivors of the rise of JpegTubers angrily waving their stick puppet around yapping yelping and parking because a lesbian was miffed that she was only socially acceptable as a tab on someone's browser may sit this explanation out, please enjoy the cookies, pizza and soda left outside of the seminar hall, don't bitch about them being store brand tho.
We still see this bastardization of what it means to be militant in shows and movies, Milquetoast hand wringing writers eager to join the laughs at the straw men they crafted with dyed hair and pronouns waved about to pantomime the faux outrage they believe comes with being militant. “Ah yes, those Snowflakes will most certainly care that I'm placing this Sticker on the back of my truck~! Mmmm, their outrage, delightful, tasty, a Special Little treat for a Special Little Man~ WAIT NO, BIG MAN, BIG MAN, BEHOLD THE BALLS ON MY TRUCK, A SIGN THAT MY OWN BALLS ARE JUST AS SWOLLEN AND ENGORGED, A BEACON OF MASCULINITY THAT ANY MEDICAL PRACTITIONER WILL WEEP AT!” What was I talking about…?
Oh yeah if i ask you to come up with a list of characters that follow this little diddy. A well meaning, white suburbanite, oft well to do who is overly vocale on social issues much to the detriment to their own social circles. Switching the tracks, a young black woman with a protective hairstyle or Big afro. Maybe a green jacket in most weathers.Attends rallies and goes about abusing bullhorns via shouting about black issues, often alienating her from her own friend group or creating discord between them because she may have white friends that are rather Perturbed by her rhetoric. The second may be played to attempt a positive characterization but it still comes from the same hay bale.
This character comes from a shift in public perception that the Advocates words must be genial and pleasant if it is to make the mark. That their struggles must be made palatable and consumable to the larger audience if they are to be accepted. Of course this is a larger load of shit then the streets of london prior to the advent of public plumbing.
Yes this is the Malcom x vs Martin luther bullshit again, a million smarter authors have penned this shit enough time for the squids to beg for a bit reprieve and I promise i'm not going to go over it to much as I have nothing clever to say on it aside from a brief summary of pop cultural digestion and acidic markings.
Martin Luther is seen as the Soft Figure, the Proper advocate. The one that will go to a place and make a heart warming street and march and hope the police will beat them a little bit softer or hope the towns water pressure isnt as bad (an unforgivable assertion by the by, those marches were massively disruptive, you cant march that many people down a large street and not have it be in some way fucking disrubtive.) This gets turned into someone like Professor X, one who balks at his own power and helps humanity in hopes of appealing to the shared empathy of all. This is contrasted to Malcolm X, the black panther movement, the Threat of violence in service to a social cause. The Scary Other. This is morphed to magneto, the one who demands mutant acceptance now but is revealed to be a mutant supremacist. Song Meet Dance.
Now what the fuck does all of this have to do with one piece? Simple. It is the story of the Militant Other.
But do I hear someone say, it's a shounen manga that's filled with gratuitous fighting! Of course we're going to see those labeled as the “other” being militant! Well I must simply retort that you are trespassing, please leave im vary scared, im holding a sword and quivering in place, my fucking teeth are chattering, get out please, you can have a bottle of water on your way out but take no more I beg of thee.
The story of one piece is about characters that are othered at birth, made others by circumstance and society or choosing to embrace their otherness and becoming militant. Who shall we look at first? The main character?! Oh you treat me so well, what a delight~!
Now Luffy and his story isn't inherently tied to him being queer but it sets up a very clear arc path for other queer characters that we will see later on in this post. If you are not aware, luffy is almost violently asexual, by violent i mean in that way that if I was an obnoxious power scaler i could easily list it as a power feat. please note the episode when he first met boa hancock, a woman drawn to be sexually attractive with the explicit power of turning people who find her cute or attractive into stone. Luffy gets hit with this and just ignores it. Fuck you it counts and I like it… ok im sorry, i dont know how you reacted to that information, that was so rude of me, im so sorry, please sit down, you can have another water bottle ontop of the courtesy failed robbery water bottle you recived. Please try to remain hydrated.
Funny aside, Luffy is Himself. He is always Himself. There is no situation in which he can act as anything other than himself in all situations the self that he embodies is indelible. He understands this about himself thus surrounds himself with people that are able to not change the self but help the self become more with the promise of the same happening to those around him.
He is also astoundingly passionate in what he believes in, he is passionate about the causes of his friends, he is passionate about the causes of people he finds to be good. This passion often shows itself as Extreme, Violent and one may even say Confrontational. Of course some may not consider punching someone directly in the face multiple times as confrontational but apply your better judgment to this matter as you consider it.
Luffy is a militant activist. When he supports a cause, it's mostly for its ideological aspects. He believes that people should be free in the most basic of terms, they should be free to travel, grow, eat, laugh. Anything that hinders that is a direct insult to Luffy's ongoing system of thought and means you are going to be punched or ignored.
Lets keep going down the line to see who else fits in this theme, shall we? No? What the fuck man? I gave you two water bottles, and they're like…Good water bottles, they don't even have those squiggly walls, they're like… smooth plastic square bottles.
Well I'm going with or without you, starting with my beloved Bon clay. We meet bon prior to the start of the alabasta arc, fished out of the water by the straw hat crew in which he gives his express thanks, here we are given a stark humanization. We get to see him eagerly match pace with the energy of the crew, eagerly feeding into their jokes, showing off his powers, laughing with them.
A side note. Laughing has always been made a huge deal in one piece, whether it's the other characters' starkly unique laughs or most arcs ending off with the crew and cast laughing. It's a show of celebration, that you are in a joyous mood, that you are Happy. I wonder if that's important to any narrative theme… anyways
I think this is all astoundingly important because they show bon clay as a fun weirdo who is in love with the self they have become before they are shown as a part of the villains crew. It establishes that they are more than their narrative born role as a minor antagonist, they are a complex human that is capable of complex thoughts and ideology. Show cased by the end of the arc, the exact moment that i fell in love with them, like really fucking hard. I'm talking about running into senpai, bread in mouth. My hearts going doki doki, doctors are flipping shit trying to label it as heart arrhythmia but oh no it's not you P.H.Dick it's the power of love burning like a goddamn cyclone smashing into a oil refinery, that explosion isn't disrupting the wind flow but it is sucking up those flames like a really well thought out sexual innuendo that your super duper impressed by and think is really funny and want to congratulate me on for making such a cool sexual joke.
They sacrifices himself in order to allow the straw hats to escape from alabasta. Ending their appearance with a heartfelt farewell to the crew that they have fought with only a day ago, that he was willing to kill on orders a day ago. Leaving them with the words
“One may stray from the path of a man, one may stray from the path of a woman, but we never stray from the path of a human.”

FUCK THATS A REALLY GOOD LINE, anyways we see him again later in impel down in one of the hell layers, with even the scorching heat and arid air unable to squash his eccentric personality like the god damn wonder they are. Dancing in the depths of hell they soon hear that luffy has broken in and rush lower through the layers to meet up with them, Eager to join up and fight with him.
Again, we are seeing behavior Vary similar to luffy, that actions which serve their passions are to be taken always. A passion for friendship, loyalty, all of that. The willingness to serve time in a massive human rights violation of a prison…ok thats a little vague, thats most prisons… Anyways we do get to see more of bon clay's belief system as we meet both our next queer character and our next militant character.
Ivankov. They to me are the true exemplification of all three levels of advocacy in service to a group of peoples existence. At the most basic level, ivankov cannot hide who they are, it's impossible, I mean look at her! He has powers that can increase the size of their face, they wear makeup so thick it can be peeled off, they are Violently of the self.

For their community, we have the new kama queendom, she has created a paradise in the depths of super hell jail to protect those around her. Even outside of the jail he has done much of the same by creating the okama queendom, the island outside of government control in which men and women flock in order to be able to express their true selves. Notably, despite ivenkovs ability to turn men into women, many of them do not make use of this power. They are free to express themselves without the expectation of fitting into that role visually. That's the community aspect to me.
Then we get the more militant activism, ivenkovs role as a member of the revolutionary army. The way he provides an outpost in the middle of the grand line, his funding through his miracle medical work, his willingness to fight for those she will never ever see.
And there are more, we see other queer characters in the revolutionary army, and they have yet to be shown in any sort of negative light. Their militant activism, their willingness to fight and rally others to fight for a cause is shown to be positive.
The desire to fight for a cause throughout one piece is shown to be an overall positive cause, all forms of it. Whether it's through the more peaceful methods such as otohime or through violence and confrontation such as Fisher tiger.
So to reiterate because this is getting hella long, I love One Piece because it allows its queer characters to fight for what they believe in, in any way that they desire. That queer characters are allowed to be weird, they are allowed to be evil, they are ugly, beautiful, powerful, anything and everything!
Thank you for reading.
33 notes
·
View notes
Text
From the article:
A Florida House panel has approved legislation to preemptively set potency caps on recreational marijuana ahead of a potential vote on a legalization initiative on the November ballot.
The legislation, which would prohibit dispensary sales of adult-use cannabis flower with a potency of greater than 30 percent THC, cleared the House Health and Human Services Committee on a 14-6 vote on Thursday.
All other cannabis products would be limited to 60 percent THC under the legislation, and it would mandate a serving size on edible products of 10 milligrams THC or less, with the total amount per package no more than 200 mg.
Before voting on the bill, the committee adopted an amendment to limit cannabis vape cartridges to a size of one gram. The amendment also removes a sunset provision in current law that would repeal the current medical cannabis program law six months after a marijuana constitutional amendment, such as the one that may be on the November ballot, is adopted.
17 notes
·
View notes
Text
President Biden and Vice President Kamala Harris on Monday announced new steps to support access to abortion, highlighting an issue that has galvanized voters in the year since the Supreme Court struck down Roe v. Wade.
Ms. Harris will travel to Wisconsin on Monday morning as she begins a national tour focused on preserving access to reproductive health care, as Mr. Biden brings together a task force on reproductive health care in Washington.
Both events are designed to call attention to the 51st anniversary of Roe v. Wade, the landmark Supreme Court ruling that established a constitutional right to abortion, and to announce new steps that Mr. Biden’s administration has taken to help Americans get contraceptives and abortions under an emergency care law.
“Even as Americans — from Ohio to Kentucky to Michigan to Kansas to California — have resoundingly rejected attempts to limit reproductive freedom, Republican elected officials continue to push for a national ban and devastating new restrictions across the country,” Mr. Biden said in a statement. “On this day and every day, Vice President Harris and I are fighting to protect women’s reproductive freedom.”
In Washington, the Department of Health and Human Services will issue guidance for patients experiencing pregnancy-related emergencies to better understand their rights to care under the Emergency Medical Treatment and Labor Act, known as EMTALA.
The law requires hospital emergency rooms to provide medically necessary care, including abortions, in urgent circumstances. The department will also provide “training materials for health care providers and establish a dedicated team of experts” to support hospitals around the country, according to a fact sheet distributed by the administration.
19 notes
·
View notes
Text
I’m not sure how reliably I’ll be able to keep up with it, but I’ve been wanting to start posting weekly or monthly Good News compilations, with a focus on ecology but also some health and human rights type stuff. I’ll try to keep the sources recent (like from within the last week or month, whichever it happens to be), but sometimes original dates are hard to find. Also, all credit for images and written material can be found at the source linked; I don’t claim credit for anything but curating.
Anyway, here’s some good news from the first week of March!
1. Mexican Wolf Population Grows for Eighth Consecutive Year

““In total, 99 pups carefully selected for their genetic value have been placed in 40 wild dens since 2016, and some of these fosters have produced litters of their own. While recovery is in the future, examining the last decade of data certainly provides optimism that recovery will be achieved.””
2. “Remarkable achievement:” Victoria solar farm reaches full power ahead of schedule

“The 130MW Glenrowan solar farm in Victoria has knocked out another milestone, reaching full power and completing final grid connection testing just months after achieving first generation in late November.”
3. UTEP scientists capture first known photographs of tropical bird long thought lost

“The yellow-crested helmetshrike is a rare bird species endemic to Africa that had been listed as “lost” by the American Bird Conservancy when it hadn’t been seen in nearly two decades. Until now.”
4. France Protects Abortion as a 'Guaranteed Freedom' in Constitution
“[A]t a special congress in Versailles, France’s parliament voted by an overwhelming majority to add the freedom to have an abortion to the country’s constitution. Though abortion has been legal in France since 1975, the historic move aims to establish a safeguard in the face of global attacks on abortion access and sexual and reproductive health rights.”
5. [Fish & Wildlife] Service Approves Conservation Agreement for Six Aquatic Species in the Trinity River Basin
“Besides conserving the six species in the CCAA, activities implemented in this agreement will also improve the water quality and natural flows of rivers for the benefit of rural and urban communities dependent on these water sources.”
6. Reforestation offset the effects of global warming in the southeastern United States

“In America’s southeast, except for most of Florida and Virginia, “temperatures have flatlined, or even cooled,” due to reforestation, even as most of the world has grown warmer, reports The Guardian.”
7. Places across the U.S. are testing no-strings cash as part of the social safety net
“Cash aid without conditions was considered a radical idea before the pandemic. But early results from a program in Stockton, Calif., showed promise. Then interest exploded after it became clear how much COVID stimulus checks and emergency rental payments had helped people. The U.S. Census Bureau found that an expanded child tax credit cut child poverty in half.”
8. The Road to Recovery for the Florida Golden Aster: Why We Should Care

“After a five-year review conducted in 2009 recommended reclassifying the species to threatened, the Florida golden aster was proposed for removal from the Federal List of Endangered and Threatened Plants due to recovery in June 2021, indicating the threats to the species had been reduced or eliminated.”
9. A smart molecule beats the mutation behind most pancreatic cancer
“Researchers have designed a candidate drug that could help make pancreatic cancer, which is almost always fatal, a treatable, perhaps even curable, condition.”
10. Nurses’ union at Austin’s Ascension Seton Medical Center ratifies historic first contract

“The contract, which NNOC said in a news release was “overwhelmingly” voted through by the union, includes provisions the union believes will improve patient care and retention of nurses.”
This and future editions will also be going up on my new Ko-fi, where you can support my art and get doodled phone wallpapers! EDIT: Actually, I can't find any indication that curating links like this is allowed on Ko-fi, so to play it safe I'll stick to just posting here on Tumblr. BUT, you can still support me over on Ko-fi if you want to see my Good News compilations continue!
#hopepunk#good news#wolf#wolves#mexican wolf#conservation#solar#solar power#birds#abortion#healthcare#abortion rights#reproductive rights#reproductive health#fish and wildlife#turtles#alligator snapping turtle#snapping turtle#river#reforestation#global warming#climate change#climate solutions#poverty#social safety net#flowers#endangered species#cancer#science#union
15 notes
·
View notes
Last Seen Blogs

jeseniahockaday-blog
Couple Of review Ripoffs And How You Can Refrain From

gay-trier-rlp
Unbetitelt

baeksthighs
Inactive

briebdraw
briebdraw
valentaes
arson