#coronavirus masks
Text
Source
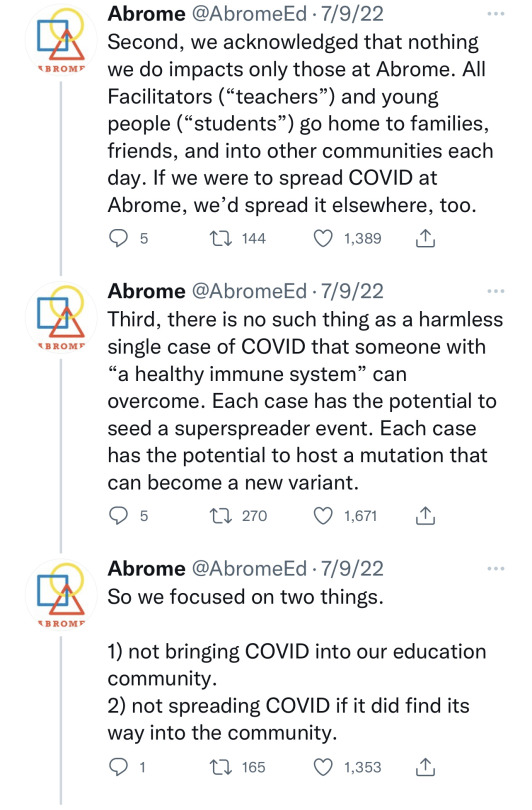
CDC Wastewater Viral Activity Monitoring
BreatheTeq
34K notes
·
View notes
Text
I gotta say the Orwell quotes are getting way less snappy these days.
"the pandemic is over but covid is a leading cause of death" isnt as good of a soundbite as "war is peace freedom is slavery ignorance is strength"
#covid 19#coronavirus#anyways always remember MVV friends#mask ventilate and vaccinate#esp you northern hemisphere ppl going into winter
9K notes
·
View notes
Text

#mask up#covid#covid 19#covid isn't over#pandemic#covid conscious#long covid#covid is airborne#wear a mask#coronavirus
5K notes
·
View notes
Text
Would appreciate reblogs to reach a wider sample size!
13K notes
·
View notes
Link
Covid is still a leading killer, the third-biggest in the US last year behind heart disease and cancer. Unlike with other common causes of death such as smoking and traffic accidents that led to safety laws, though, politicians aren’t pushing for ways to reduce the harm, such as mandated vaccinations or masking in closed spaces.
“The general desire in the world is to move beyond the pandemic and put Covid behind us, but we can’t put our heads in the sand,” said Ziyad Al-Aly, director of the Clinical Epidemiology Center at the Veterans Affairs St. Louis Health Care System in Missouri. “Covid still infects and kills a lot of people. We have the means to reduce that burden.”
[...]
Long Covid, estimated to affect around 10% of infected people, is considered one of the biggest post-pandemic medical challenges. The economic costs are also significant.
In the US, long Covid was estimated to cost around $50 billion a year in lost salaries as of late 2022. In the UK, the Institute for Fiscal Studies last year estimated that about one in 10 people with long Covid have to stop working as a result. The number of people with those symptoms, including brain fog, breathing difficulties and fatigue, are rising even as infections are decreasing.
It’s particularly scary for high-risk people, who’ve had to return to work and public spaces where masks are sparse and the dangers are invisible. A family wedding can still turn into a super-spreader event, and a flight can be catastrophic.
3K notes
·
View notes
Text
You might be forgiven for thinking it’s been a very quiet few months for the Covid-19 pandemic. Besides the rollout of new boosters, the coronavirus has largely slipped out of the headlines. But the virus is on the move. Viral levels in wastewater are similar to what they were during the first two waves of the pandemic. Recent coverage of the so-called Pirola variant, which is acknowledged to have “an alarming number of mutations,” led with the headline “Yes, There’s a New Covid Variant. No, You Shouldn’t Panic.”
Even if you haven’t heard much about the new strain of the coronavirus, being told not to panic might induce déjà vu. In late 2021, as the Omicron variant was making its way to the United States, Anthony Fauci told the public that it was “nothing to panic about” and that “we should not be freaking out.” Ashish Jha, the Biden administration’s former Covid czar, also cautioned against undue alarm over Omicron BA.1, claiming that there was “absolutely no reason to panic.” This is a telling claim, given what was to follow—the six weeks of the Omicron BA.1 wave led to hundreds of thousands of deaths in a matter of weeks, a mortality event unprecedented in the history of the republic.
Indeed, experts have been offering the public advice about how to feel about Covid-19 since January 2020, when New York Times columnist Farhad Manjoo opined, “Panic will hurt us far more than it’ll help.” That same week, Zeke Emanuel—a former health adviser to the Obama administration, latterly an adviser to the Biden administration—said Americans should “stop panicking and being hysterical.… We are having a little too much [sic] histrionics about this.”
This concern about public panic has been a leitmotif of the Covid-19 pandemic, even earning itself a name (“elite panic”) among some scholars. But if there’s one thing we’ve learned, three and a half years into the current crisis, it’s that—contrary to what the movies taught us—pandemics don’t automatically spawn terror-stricken stampedes in the streets. Media and public health coverage have a strong hand in shaping public response and can—under the wrong circumstances—promote indifference, incaution, and even apathy. A very visible example of this was the sharp drop in the number of people masking after the CDC revised its guidelines in 2021, recommending that masking was not necessary for the vaccinated (from 90 percent in May to 53 percent in September).
As that example suggests, emphasizing the message “don’t panic” puts the cart before the horse unless tangible measures are being taken to prevent panic-worthy outcomes. And indeed, these repeated assurances against panic have arguably also preempted a more vigorous and urgent public health response—as well as perversely increasing public acceptance of the risks posed by coronavirus infection and the unchecked transmission of the virus. This “moral calm”—a sort of manufactured consent—impedes risk mitigation by promoting the underestimation of a threat. Soothing public messaging during disasters can often lead to an increased death toll: Tragically, false reassurance contributed to mortality in both the attacks on the World Trade Center and the sinking of the Titanic.
But at a deeper level, this emphasis on public sentiment has contributed to confusion about the meaning of the term “pandemic.” A pandemic is an epidemiological term, and the meaning is quite specific—pandemics are global and unpredictable in their trajectory; endemic diseases are local and predictable. Despite the end of the Public Health Emergency in May, Covid-19 remains a pandemic, by definition. Yet some experts and public figures have uncritically advanced the idea that if the public appears to be tired, bored, or noncompliant with public health measures, then the pandemic must be over.
But pandemics are impervious to ratings; they cannot be canceled or publicly shamed. History is replete with examples of pandemics that blazed for decades, sometimes smoldering for years before flaring up again into catastrophe. The Black Death (1346–1353 AD), the Antonine Plague (165–180 AD), and the Plague of Justinian (541–549 AD), pandemics all, lacked the quick resolution of the 1918 influenza pandemic. A pandemic cannot tell when the news cycle has moved on.
Yet this misperception—that pandemics can be ended by human fiat—has had remarkable staying power during the current crisis. In November 2021, the former Obama administration official Juliette Kayyem claimed that the pandemic response needed to be ended politically, with Americans getting “nudged into the recovery phase” by officials. It is fortunate that Kayyem’s words were not heeded—the Omicron wave arrived in the US just weeks after her article ran—but her basic premise has informed Biden’s pandemic policy ever since.
Perhaps even less responsibly, the physician Steven Phillips has called for “new courageous ‘accept exposure’ policies”—asserting that incautious behavior by Americans would be the true signal of the end of the pandemic. In an essay for Time this January, Phillips wrote: “Here’s my proposed definition: the country will not fully emerge from the Covid-19 pandemic until most people in our diverse nation accept the risk and consequences of exposure to a ubiquitous SARS-CoV-2, the virus that causes Covid-19.”
This claim—that more disease risk and contagion means the end of a disease event—runs contrary to the science. Many have claimed that widespread SARS-CoV-2 infections will lead to increasingly mild disease that poses fewer concerns for an increasingly vaccinated (or previously infected) population. In fact, more disease spread means faster evolution for SARS-CoV-2, and greater risks for public health. As we (A.C. and collaborators) and others have pointed out, rapid evolution creates the risk of novel variants with unpredictable severity. It also threatens the means that we have to prevent and treat Covid-19: monoclonal antibody treatments no longer work, Paxlovid is showing signs of viral resistance, and booster strategy is complicated by viral evolution of resistance to vaccines.
But these efforts to manage and direct public feelings are not just more magical thinking; they are specifically intended to promote a return to pre-pandemic patterns of work and consumption. This motive was articulated explicitly in a McKinsey white paper from March 2022, which put forward the invented concept of “economic endemicity”—defined as occurring when “epidemiology substantially decouples from economic activity.” The “Urgency of Normal” movement similarly used an emotional message (that an “urgent return to fully normal life and schooling” is needed to “protect” children) to advocate for the near-total abandonment of disease containment measures. But in the absence of disease control measures, a rebound of economic activity can only lead to a rebound of disease. (This outcome was predicted by a team that was led by one of the authors [A.C.] in the spring of 2021.)
A pandemic is a public health crisis, not a public relations crisis. Conflating the spread of a disease with the way people feel about responding to that spread is deeply illogical—yet a great deal of the Biden administration’s management of Covid-19 has rested on this confusion. Joe Biden amplified this mistaken perspective last September when he noted that the pandemic was “over”—and then backed that claim by stating, “If you notice, no one’s wearing masks. Everybody seems to be in pretty good shape.” The presence or absence of health behaviors reveals little about a threat to health itself, of course—and a decline in mask use has been shaped, in part, by the Biden administration’s waning support for masking.
Separately, long Covid poses an ongoing threat both at an individual and a public health level. If our increasingly relaxed attitude toward public health measures and the relatively unchecked spread of the virus continue, most people will get Covid at least once a year; one in five infections leads to long Covid. Although it’s not talked about a lot, anyone can get long Covid; vaccines reduce this risk, but only modestly. This math gets really ugly.
The situation we are in today was predictable. It was predictable that the virus would rapidly evolve to evade the immune system, that natural immunity would wane quickly and unevenly in the population, that a vaccine-only strategy would not be sufficient to control widespread Covid-19 transmission through herd immunity, and that reopening too quickly would lead to a variant-driven rebound. All of these unfortunate outcomes were predicted in peer-reviewed literature in 2020–21 by a team led by one of the authors (A.C.), even though the soothing public messaging at the time called it very differently.
As should now be very clear, we cannot manifest our way to a good outcome. Concrete interventions are required—including improvements in air quality and other measures aimed at limiting spread in public buildings, more research into vaccine boosting strategy, and investments in next-generation prophylactics and treatments. Rather than damping down panic, public health messaging needs to discuss risks honestly and focus on reducing spread. Despite messages to the contrary, our situation remains unstable, because the virus continues to evolve rapidly, and vaccines alone cannot slow this evolution.
In the early months of the pandemic, many in the media drew parallels between the public’s response to Covid-19 and the well-known “stages of grief”: denial, bargaining, anger, depression, and acceptance. The current situation with Covid-19 calls for solutions, not a grieving process that should be hustled along to the final stage of acceptance.
833 notes
·
View notes
Text
[ID: Tweet by @PlaguePoems dated 2/17/23
“I know an old punk
whose pierced nose
remains hidden
behind the N95 mask
he dutifully wears
and when I ask him
if he still wears it
because his aesthetic
has never cared for norms
he replies that he wears it
because nothing is more punk
than giving a shit
about other people.”]
1K notes
·
View notes
Text

Seen many folks - fully vaxxed + boosted, mind you - posting about coming down with Covid this past week.
NO ONE IS FULLY IMMUNE. STUDIES SHOW EVERY TIME YOU CONTRACT COVID, NO MATTER HOW MILD, IT DOES EXPONENTIAL PERMANENT DAMAGE TO YOUR BODY & IMMUNE SYSTEM.
PLEASE wear a damn mask.
447 notes
·
View notes
Text
“covid is back” my love, it never left. because we are still in a pandemic
#‘put your masks back on’ some of us have been masking the whole time#coronavirus#also tho if you aren’t masking please put your masks back on. im begging you
349 notes
·
View notes
Text

This is another piece of art I made while processing my ongoing anger with how the US specifically, though also many other countries, have completely ignored managing the covid pandemic for the last several years.
This is your reminder: there was a new vaccine released in September of 2023. If you have not had a vaccine since then, you need one.
Threadless, Redbubble
#covid#covid 19#covid isn't over#long covid#covid19#coronavirus#pandemic#wear a mask#mask#mask up#get vaccinated#angry
134 notes
·
View notes
Text
Most of you are going as this for Halloween. And it doesn't even require a costume.
https://www.reddit.com/r/HermanCainAward/
#COVID #COVIDisNotOver #COVIDisAirborne #COVID19 #eugenics #ableism
#happy halloweeeeeeen#halloween#long covid#covid19#covid 19#covid isn't over#covid#coronavirus#corona virus#health#occupationalhealthandsafety#plaguecore#plague mask#plague doctor#a plague tale#plaguetober#plague#viruses#virus#infectious diseases#infection#eugenics#eugenicist#ausgov#politas#auspol#tasgov#taspol#australia#fuck neoliberals
203 notes
·
View notes
Text
Reducing the covid isolation period to 1 day - a single day- when an infection can be contagious for up to 21 days is... unbelievably cruel.
#chena.txt#like if this doesn't tell you how little these public health guidelines are about protecting people#and are actually about preserving companies bottom lines...#they're willing to let so many people die or get permanently disabled#working people to an early grave#but giving us more pto? free tests/masks? impossible#ridiculous#covid#covid 19#coronavirus
119 notes
·
View notes
Text



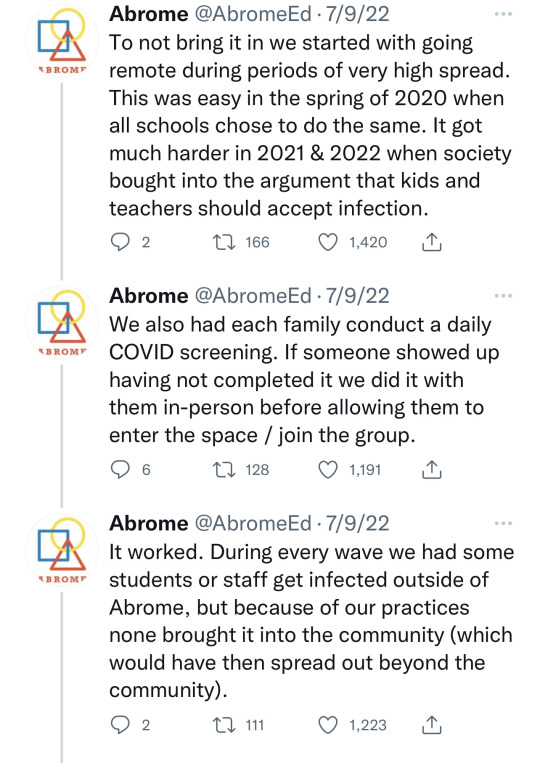
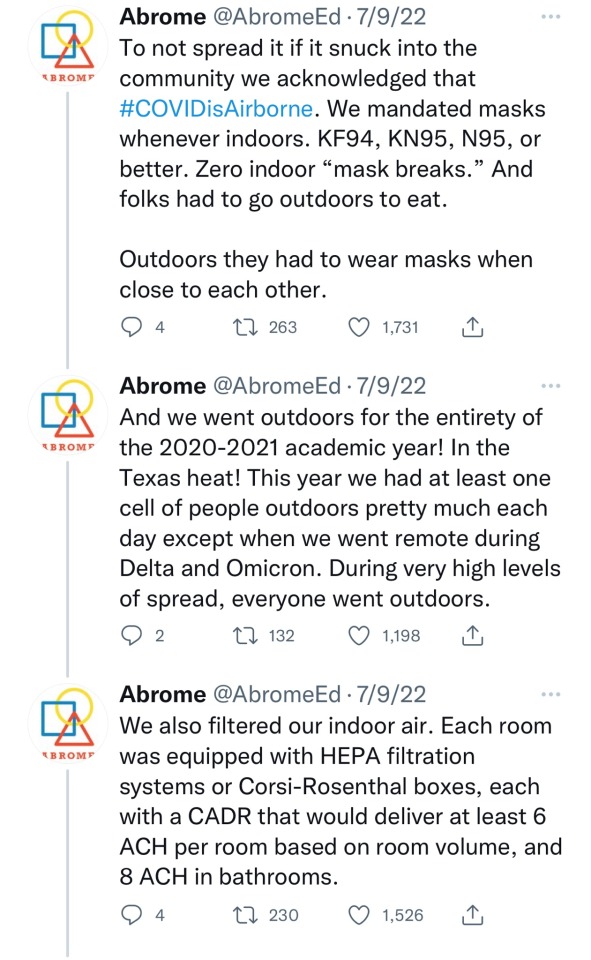


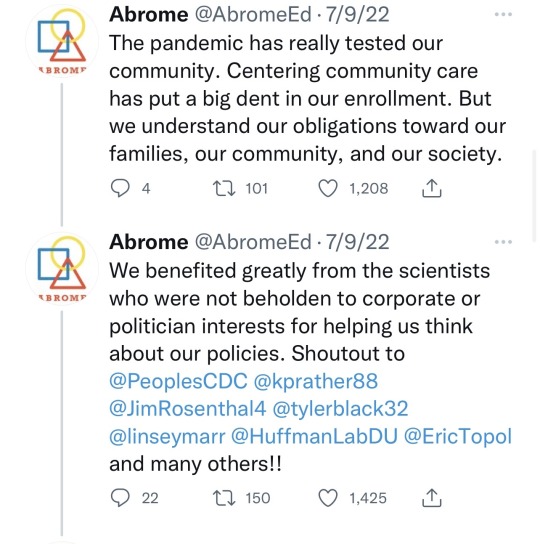
Very impressive. Wearing face masks is still important, and this school seems to get that.
We might be tired of Coronavirus, but it’s not tired of us. The pandemic is not over.
👉🏿 https://threadreaderapp.com/thread/1545758673242411009.html
2K notes
·
View notes
Text
#mask up#covid#covid 19#covid isn't over#pandemic#covid conscious#covid is airborne#wear a mask#coronavirus#funny
519 notes
·
View notes
Text

#disability justice#COVID#COVID safety#covid isnt over#COVID19#Long COVID#wear a mask#able bodied#ableism#eugenics#coronavirus#fuck ableism#anti ableism#wear a fucking mask
388 notes
·
View notes
Link
At the start, masks helped flatten the curve to protect our hospital systems, and since, masks have helped make public spaces and essential services more open and accessible to everyone. Many studies show that masks work, and they work best when everyone wears a high-quality one to protect each other. Masks are magnificent.
Yet, three years into the pandemic, we still see conflicting stories in the news about masks on a daily basis. The latest culprit powering the confounding headlines is a new scientific review published in Cochrane. The paper analyzes many different studies that assess how physical measures – including masks – fare against respiratory viruses.
The analysis is flawed because it compares apples to oranges. The paper mixes together studies that were conducted in different environments with different transmission risks. It also combines studies where masks were worn part of the time with studies where masks are worn all the time. And it blends studies that looked at Covid-19 with studies that looked at influenza.
If apples work and oranges don’t, but your analysis mixes them together, you may come to the false conclusion that apples don’t work. Out of the 78 papers analyzed in the review, only two actually studied masking during the Covid-19 pandemic. And both of those found that masks did protect wearers from Covid-19. But these studies are drowned out by the greater number of studies on influenza included, where the benefit of masking is harder to detect because it’s a far less contagious virus than Covid-19.
[...]
The mischaracterization of the Cochrane review by its authors and like-minded supporters is deliberate. Those with vested interests are sowing doubt about the science of Covid-19 protections by using the same disinformation playbook that tobacco companies, the fossil fuel industry and the anti-vax movement have used in the past.
The overselling of the Cochrane study is a classic example of cherry-picking, where biased groups highlight a subset of data that support their position, while ignoring the larger pool of evidence that disagrees with them. Many direct studies in labs show that high-quality masks significantly reduce the number of viral particles mask-wearers inhale and emit, but these are intentionally omitted in the arguments of anti-maskers.
These disinformation tactics are successfully quashing public health policies. Policymakers are susceptible to bad faith arguments about masks because they are beholden to short-term corporate interests. Masks are a visible symbol that the pandemic is ongoing, and politicians fear that these reminders stop people from consuming. It’s easy to lie to those who want to believe.
451 notes
·
View notes
Last Seen Blogs




