#covid-19 treatment
Text
#covid treatment paxlovid#covid-19 treatment#covid treatment drug paxlovid#Covid treatment online#online doctor paxlovid#COVID-19 treatment with Paxlovid
1 note
·
View note
Text
Revolutionary AI-Designed Drug Enters Clinical Trials: Latest News
A groundbreaking new AI-designed drug for COVID-19 has entered Phase I clinical trials, offering hope for an effective treatment against the disease. Stay updated with the latest news on headline horizon.
0 notes
Link
0 notes
Text
are there effective treatments for anosmia?
are there effective treatments for anosmia?
A recent Cochrane review takes stock and concludes that there is not yet enough robust evidence for certain treatments to treat post-Covid anosmia to consider them effective. Nevertheless, there is hope for olfactory training with an ongoing study in Quebec.
L’smellsmell is a primary meaning. It allows us to appreciate pleasant smells and, at the same time, to keep us away from nauseating odors,…

View On WordPress
0 notes
Text
THE COMPLEXITY OF CO-INFECTIONS IN THE ERA OF COVID-19
Around the end of December 2019, Chinese health officials found a cluster of pneumonia in Wuhan, the capital of Hubei province. Shortly later, Chinese scientists discovered a previously unknown beta-coronavirus as the likely cause of the illness. SARS coronavirus 2 (SARS-CoV-2) has been renamed coronavirus disease 2019 (COVID-19). COVID-19, like the 1918 H1N1 influenza pandemic before it, illustrates the catastrophic effect on a vulnerable “naive” population of an emerging zoonotic disease.
WHAT IS COVID-19 DISEASE?
Coronavirus disease (COVID-19) is an infection caused by the SARS-CoV-2 virus.
Case Reports according to the World Health Organization indicate that most patients infected will develop mild to severe respiratory infection but will recover without particular treatment. However, some will become gravely ill and require medical care. People over the age of 65 and those with health problems like heart disease, diabetes, chronic lung disease, or cancer are more likely to get severe covid-19. COVID-19 can cause serious illness and death in people of any age.
When an infected person coughs, sneezes, speaks, sings, or breathes, small liquid particles can be expelled from their mouth or nose and transmit the virus. The size of these particles ranges from large respiratory droplets to minute aerosols.
Researchers have evaluated the size and content characteristics of the SARS-CoV-2 particles. Upon analysis of negative-stained SARS-CoV-2 articles by electron microscopy, researchers have had varying results, but the diameter of the virus has been found to range between 50 nm to 140 nm.
COVID-19 AND EMERGENCE OF CO-INFECTIONS
In a pandemic age, the existing prevalence of Covid-19 guarantees co-infections with a multitude of co-pathogens. Hospitalized patients with Covid-19 and other viral respiratory infections are known to be predisposed to bacterial co-infections for an extended length of time. These co-infections result in a poorer prognosis than each infection alone.
With the SARS-CoV-2 pandemic, there are various subtleties in epidemiology, microorganism, and clinical symptoms. With more focus on therapy and treatment for multidrug resistant viruses, there has been less focus on understanding how these viruses affect other diseases that people may have. With severe or long-lasting viral infections, several pathogens are sure to complicate the clinical presentation, operational condition, diagnostics, and monitoring.
CO-DETECTION OF SARS-COV-2 AND INFLUENZA VIRUS
Since the pandemic, there have been few reports of interactions between influenza and COVID-19. Proper review and meta-analysis reports have revealed the severity of infection in individuals co-infected with influenza and SARS-CoV-2 and the remarkably mild symptoms of co-infected outpatients.
Co-infection with SARS-CoV-2 and influenza virus, coupled with a varied clinical prognosis, offers a more significant threat to public health. It has been shown that having both SARS-CoV-2 and influenza A infections makes the disease more severe. This may be because the two viruses enhance each other’s effects.
Previous systematic review and meta-analysis has linked influenza viruses, respiratory syncytial virus (RSV), and adenoviruses to COVID-19 patients. Co-infections with bacteria and viruses are more common in mild, moderate, and severe diseases leading to weakened immune systems.
Hypertension, diabetes, chronic renal disease, and heart failure have been linked to increased COVID-19 disease severity in individuals with COVID-19 with weak immune response. Pneumococcus plays a significant role in developing lower respiratory tract infections in children with COVID infection.
In those infected with SARS-CoV-2, there is a strong link between Pneumonia specific to Covid-19 disease (14.4%), cardiovascular disease, hypertension (18.6%), and diabetes (11.9%).
Due to the worldwide nature of the pandemic, even non-viral ailments can co-infect. During flu season, the relationship between influenza viruses and SARS-CoV-2 in co-infection has varied given no proper care guidelines. Fewer than 10% of COVID-19 patients had also been infected with another high-risk respiratory virus.
It has been reported that SARS-CoV-2 infections exacerbate parasite illnesses.
However, intestinal parasite co-infection was linked to COVID-19. SARS-CoV-2 has co-infected several systemic viruses. This co-infection was especially significant in chronic HIV infection when immunosuppression or increased infection susceptibility can make either condition worse. Co-infection with HIV-1 alters T cell responses to SARS-CoV-2, as has co-infection with Mycobacterium TB.
Early-stage COVID-19 illness is linked with frequent bacterial co-infections and severe morbidity and mortality rate.
CO-INFECTION WITH RESPIRATORY PATHOGENS
1.Tuberculosis
There have been instances of COVID-19 co-infection with other respiratory diseases, which may be more prevalent in certain places than others. The initial disease is Tuberculosis (TB). All COVID-19-infected individuals should be screened for tuberculosis, although bigger investigations are required to validate the findings.
Because TB is chronic and COVID is acute, the co-infection may be coincidental, but the high death rate may be larger than for COVID alone.
2.Fungi
Reports have documented cases of coronavirus disease 2019 associated with Pneumocystis Jirovecii Pneumonia, either simultaneously or within a few days of each diagnosis. This presents a diagnostic conundrum, especially in people living with HIV who are not routinely tested for and in those with other fungal infections.
Other evidence suggests viral infections worsen or cause fungal infections. When antimicrobials, corticosteroids, or immunomodulating medications are administered, it is not surprising that COVID-19 is related with opportunistic fungi such as yeast and Aspergillus spp.
3.Measles
As well as the relationship between dengue with SARS-CoV-2 infection in a frontline healthcare worker, measles has also been linked as bacterial co-pathogens to SARS-CoV-2 disease. Due to their immunosuppressive impact, Helminthic co-infection may increase morbidity and mortality among COVID-19 patients.
THE EFFECT OF COVID-19 ON POST-ONSET BACTERIAL INFECTIONS ASSOCIATED WITH COVID-19
Upper respiratory infections caused by viruses are frequently accompanied by an increase in the number of secondary infections like Commensal Bacteria. In viral-induced inflammation, this elevates the risk of middle ear, sinus, and respiratory infections. The frequency of subsequent infections can be anticipated.
Increased hospitalisation, lengthier ICU stays, and death has been associated with comorbidities. Finally, a large body of research case series suggests that viral infections increase patients’ risk of bacterial co-infections.
Early COVID-19 lung infection has a modest rate of authentic co-infections, as currently understood. This disturbance was seen during the COVID-19 outbreak, according to molecular epidemiology. Respiratory, bloodstream and fungal skin infections are common nosocomial diseases. Empiric, powerful, or extended antibiotics enhance nosocomial infection risk.
During the duration of COVID-19, the kind of recommended co-pathogen develops. In the early stages of the condition, respiratory infections are frequent. As the viral illness progresses, nosocomial diseases may become widespread, notwithstanding the varying institutional rate.
Bacterial co-infections rise with patient ageing. Co-infections are more common in patients with greater comorbidities. Gram-negative bacillus infections are linked to longer hospital stays and severe COVID-19.
COVID-19 co-infecting bacteria include Mycoplasma pneumonia, Pseudomonas aeruginosa, Haemophilus influenzae, and Chlamydia pneumonia.
UNDERLYING ISSUES OF UNDETECTED CO-INFECTIONS IN COVID-19 PATIENTS
Undiagnosed COVID-19 co-infections can cause greater hospitalisation, several treatment options, and even mortality. During pandemics, clin infect dis can lead to underreporting of additional infections that contribute to disease severity.
Progression of upper and lower respiratory viral infections is widely recognised. They may be asymptomatic or suffer for weeks or months. Viruses are usually gone within 10 days of infection. Inflammatory residual or structural damage caused by a virus can cause prolonged sickness.
This might last a few days or months. Although, permanent airway damage and respiratory infection aren’t the same. Co-infection is possible during acute viral excretion and once illness leftovers are apparent. In such a case, it suggests that two viruses are infected at the same time.
THE MEDICINAL ASPECT – ANTIBIOTIC RESISTANCE
It is crucial to determine if individuals with COVID-19 also have secondary bacterial infections, and if so, if they require antibiotics immediately. This is because antibiotic overuse can lead to the development of drug-resistant bacteria and fungi, which is wished to be prevented.
Antimicrobials may be used as “repurposed medications” to treat the COVID infection itself, even in the absence of co-infection, if antibiotics are frequently used, which is quite prevalent. Antimicrobial resistance can be reduced through social distance, using facemasks and frequent handwashing, isolating sick patients, and sterilising their environment.
56.6 % (965/1705) of hospitalised COVID-19 patients received early empiric antibiotic treatment, but only 3.5 % (59/1705) of hospitalised COVID-19 patients had a proven community-onset bacterial co-infection.
Antibiotic use is a risk factor for co-infection with Clostridioides difficile, and COVID-19 appears to be immune to it.
CONCLUDING REMARKS
Early COVID-19 has a low incidence of new genuine viral co-infections. Reports of significant co-infection rates in current diagnostic procedures must be tempered by limitations. COVID-19 will always be superimposed on existing illnesses, and due to the prevalence of COVID-19, various superimposed disorders will emerge during a SARS-CoV-2 infection.
Opportunistic and nosocomial infections will occur more frequently in patients with severe COVID-19 due to the long-term nature of some illnesses and the regular use of antibiotics and immunomodulatory therapies. More evidence is required, and greater understanding of COVID-19 co-infections will give better direction for successful antimicrobial therapy for SARS-CoV-2 or genuine co-infections.
We provide a variety of INACTIVATED and LIVE ORGANISMS in a variety of forms such as PURIFIED VIRUSES, INACTIVATED CULTURE FLUIDS. Our bacterial strain collection is available as PURIFIED DNA (or NATtrol), designed to meet your research and product development needs.
Visit the Helvetica Health Care Website for more information.
Read More: https://www.h-h-c.com/the-complexity-of-co-infections-in-the-era-of-covid-19/
0 notes
Link
The organization constantly monitors how approved COVID-19 Treatment in Philadelphia is affected by different variants. If the data shows the dose is not effective against the variant, the therapy will no longer be authorized for use at the time.
0 notes
Link
Dr. Nishtha Singh is the best lung specialist in Jaipur and always motivates her patients to adopt a healthy lifestyle.
#lung expert in india#asthma treatment#asthma specialist in jaipur#ASTHMA and COVID-19#Asthma Specialist in Rajasthan#Coronavirus and Asthma#coronavirus#what asthma patients need to know about coronavirus and asthma#How Summer Heat Affects Asthma Patients#COVID-19 vaccine#covid news#covid-19 treatment#covid vaccine#COVID19#covid pandemic#covid third wave#covid-19#covid#asthma#asthma Patients#Summer Heat Affects Asthma Patients
0 notes
Link
After COVID, it is necessary to exercise to keep the lungs healthy. Moreover, you have to take care of some things. To keep the lungs strong, drink plenty of fluids daily and 5 minutes of steam every day. And most importantly, do not make any changes in your lifestyle without the advice of a doctor. In conclusion, you can contact Dr. Virendra Singh at Asthma Bhawan. He has been treating many patients with lung problems for a long time.
#covdi-19#covid-19 treatment#covid vaccine#covid-19 third wave#covid news#Covid-19 XE variant#long covid#covid pandemic#COVID-19#Covid-19 XE Variant Symptoms#COVID-19 XE Variant Symptoms and Precautions#How does COVID-19 XE Variant outbreak affect Asthma Patients?#covid_19#asthma#asthma treatment#Asthma Patients#lung cancer#interstitial lung disease#Best Pulmonologist in Jaipur | Lung Specialist and Chest Doctor in Rajasthan India#How to Keep Your Lungs Healthy During Covid-19 XE Variants#Dr. Virendra Singh#Lungs Healthy During Covid-19
0 notes
Text
Hello! I'm here to bring you your breaking medical news from Twitter!
(No lie: I'm sure it depends who you're following, but I get really clear and specific COVID-19 info there.)
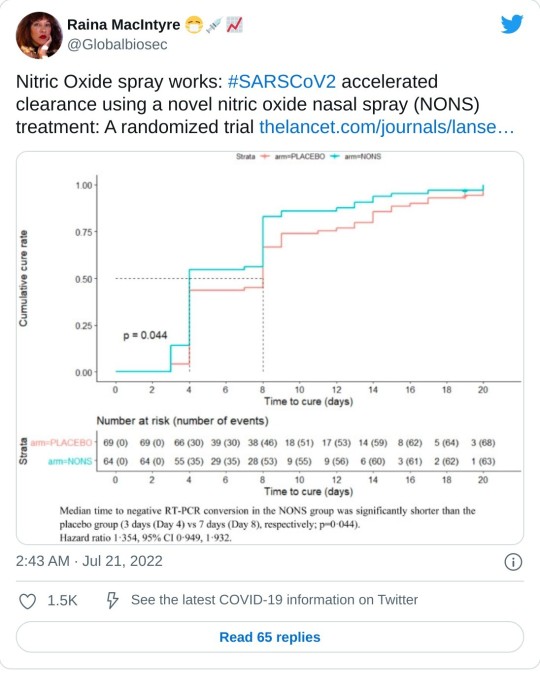
In this peer-reviewed, randomized, double-blind, multicentre, parallel group, placebo-controlled phase III clinical trial (which you KNOW I read through before sharing!), people with COVID-19 tested negative much sooner when using nitric oxide nasal spray.
It reduced the virus in their noses, which makes it less contagious AND means the patients get less sick.
(It specifically mentioned symptoms ending sooner, and it looked like a fair number of people on placebo were still having symptoms after 2½ weeks. I really hope that means it will significantly reduce the risk of long COVID, but of course it'll take months to find out for sure.)
And it apparently works on all (or just lots?) of airborne viruses.
More trials are apparently on the way, but you can buy these sprays over the counter - at least online.
464 notes
·
View notes
Text
CME program on Long Covid I watched today explicitly called out medical gaslighting and mentioned that long covid patients were “victims” that needed support and validation of their symptoms and experiences.
9 notes
·
View notes
Text
#Paxlovid prescription#what medicine to take for covid#covid treatment paxlovid#what otc medicine to take for covid#covid-19 treatment#Online doctor for covid treatment#covid treatment drug paxlovid#Covid treatment online#online doctor paxlovid
1 note
·
View note
Text
The Weather
A study in Clinical Infectious Diseases reported “that the risk of developing symptomatic illness within 14 days was 5 times greater when contacts were exposed to an asymptomatic [COVID]-positive child in their household.” Nearly 11% of household contacts developed symptoms within 14 days of exposure. The study also found, during a 3-month follow-up, that 6 out of 77 asymptomatic children developed Long COVID. The likelihood of developing symptoms from asymptomatic exposure is higher than we might expect. Continue to spread awareness of asymptomatic spread and advocate for increased infection control measures at your local schools.
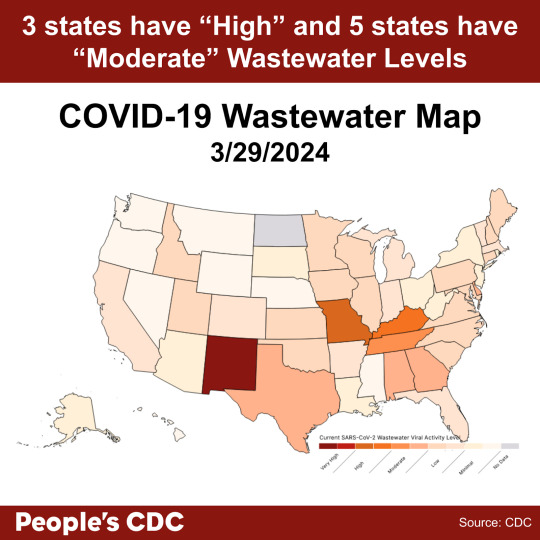
COVID wastewater levels are decreasing. As of 3/29/24, New Mexico is “Very High,” Arkansas and Kentucky are “High,” and the rest of the states are “Moderate” to “Low” levels of SARS-CoV-2 detected in wastewater.
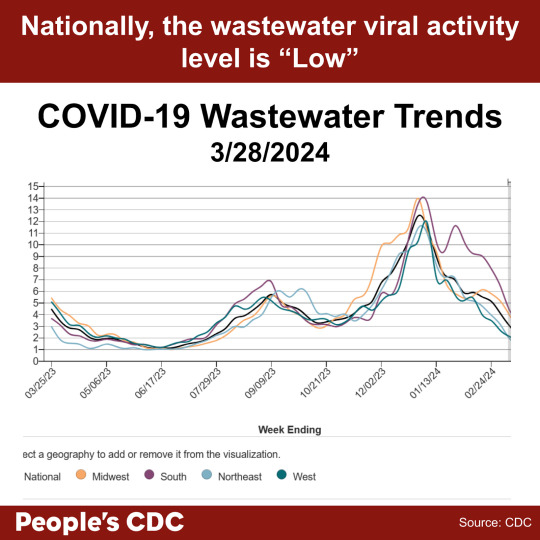
Wastewater levels continue to show a downward trend in the provisional data (gray shaded area) in all regions. The national wastewater levels are overall indicated as “Low.” While lower wastewater levels indicate decreased spread, it is important to continue to take precautions against infection. Holidays and spring breaks may bring people in closer proximity, so be sure to wear a mask to protect yourself and your community.
Wins
As we work to take more actions against the removal of vital public health measures, we remind you that you can still watch the recording of the People’s CDC press conference from March 13 and read the press release here. We would also like to remind you of the pre-proof of the People’s CDC External Review in the American Journal of Preventive Medicine Focus. The publication highlights the shortcomings of the CDC’s approach to public health and recommends a more equitable pandemic response.
News sources have published articles about the frustrations of people who continue to take COVID precautions. Time Magazine published an article presenting “both sides,” highlighting protest from people working with the CDC and concern from citizens and experts alike. While we are glad to see our voices be published in popular media, we are also saddened that “returning to normal” under economic and political pressure is so valued.
Treatments
Invyvid has received an FDA emergency use authorization for Pemgarda, a pre-exposure prophylaxis (PrEP) for people with immunocompromising conditions. Pemgarda is approved for people 12 and older with moderate to severe immunocompromise who are less likely to produce an adequate immune response to COVID vaccination alone. According to a press release from Invyvid, Pemgarda will release to market “imminently.”
Pre-exposure prophylaxis is commonly used for folks at high risk for exposure to HIV. As access to PrEP for HIV has been instrumental in keeping people safe, we hope that PrEP for COVID will be a useful tool for our community members with immune compromise. We also urge you to continue to wear high-quality masks and take other precautions to protect those most vulnerable.
Long COVID
People Magazine recently published an article highlighting an essay by Ziyad Al-Aly, physician and clinical epidemiologist, that pools data from several studies showing that COVID infection has lasting impacts on brain health. The review points out several impacts to cognitive functioning, including memory loss, spatial reasoning, and planning. Additionally, imaging studies have shown significant impact to brain tissue from inflammation, among other processes. The publication may be validating to those who experience lower cognitive function following COVID infection, including brain fog and memory dysfunction.
Take Action
We know that taking precautions–including masking, testing, and improving air quality–helps prevent the spread of airborne viral infection. Introducing more stringent precautions slowed outbreaks in the hematology ward of a hospital. The CDC recently released tips to improve ventilation. Help us urge the CDC to take other measures, including reinstating isolation periods.
Additionally, the home Test to Treat program is ending in April 2024. The program provides un-or-underinsured adults with free COVID and flu tests. If a participant in the program tests positive, they can also receive free healthcare via telehealth services. Join us to help save the program that helps so many at-risk people!
#op#covid#covid19#covid-19#covid 19#pcdc#people's cdc#long covid#covid pandemic#covid news#covid conscious#covid isn't over#pandemic#sars cov 2#coronavirus pandemic#coronavirus#sars-cov-2#cdc#prep#hiv#covid treatment#prep for covid#prep for covid-19#immunocompromised#disability#medical#uspol#img#links#described in alt text
2 notes
·
View notes
Link
A brand-new scientific study compared hundreds of hospitalized recipients of hydroxychloroquine (and azithromycin) with thousands of controls who received standard hospital care. Source This study was carefully done, peer-reviewed, and published in a prestigious journal. It looked at very sick, hospitalized patients with COVID-19 and tried to see if hydroxychloroquine, given with or without the antibiotic azithromycin, would help save lives. The authors selected matching controls to account for any possible confounding effects. We conducted a retrospective analysis to compare the 28-day mortality rate in 352 patients treated with hydroxychloroquine with or without azithromycin (HCQ-group) in our hospital with a contemporary control group of 3533 patients receiving standard of care from the Belgian … Continue reading →
5 notes
·
View notes
Photo

www.drsheetusingh.com
0 notes
Text
Covid 19 wasn't enough
Covid 19 wasn't enough so besides the train derailments contaminating water, factories burning down they now invented a fungal that is not curable by antibiotics or any kind of medication.
The fungal is called Candida auris or C. Auris. They are saying it is a yeast type of fungus that is spreading through health care facilities.
Apparently it was only in 3 states back in 2016 but has spread to 20-27 states in 2022 but now is in 30 states.
Why are they just now sharing this? Why are they just now talking about it now that the Covid has died down and no longer causing a panic?
This is probably to lead to another panic and pandemic as if the train derailments, the factories burning down and everything else going on in the world is not enough.
#covid 19#pandemic#coronavirus#covid#covid pandemic#train derailment#fungal infection#fungal treatment#bacterial#infection#bacteria#Candida auris#conspiracy#conspiracy theorist#conspiracy thinking#conspiracy thriller#conspiracy theorist keith#government control#conspiracy theory
7 notes
·
View notes
Link
Antibodies are proteids the body produces when a disease happens; they connect to a virus and support eliminating it. A monoclonal antibody is an antibody generated by cloning a selective white blood cells. Antibodies can be monoclonal or polyclonal, It is procured from a one cell clone which is a single B cell clone.
0 notes
Last Seen Blogs

danihsr
Untitled

mouth-dreams
Gardenhome, as told by Mouth Dreams

angelyne
Big Boys Sharp Knives

sobarrigudos
quero coroas e gordos...

nar-kotiki
hate u