#croup
Text

View of an advertising card for D.S. Hallock, advertising Dr. A.C. Hoxsie's Certain Croup Cure. Card depicts a girl holding a cat. Printed on back: "Dr. A.C. Hoxsie's Certain Croup Cure, positive, swift and sure. There is no remedy known that acts with such certain results. It contains no opium, the most delicate infant may take it. For sale by first-class druggists." Stamped on back: "From D.S. Hallock, druggist, cor. Fort & 18th Sts., Detroit, Mich."
Burton Historical Collection, Detroit Public Library
#cat#cats#hallock#hoxsie#croup#vintage#vintage advertising#detroit#detroit history#detroit public library
31 notes
·
View notes
Text
Who knew croup could be so scary? (CW medical emergency)
Last night the family congregated at my sister’s place for Mum’s birthday. Just as dinner was being served, my husband rushed in with my 6yo nephew, who’s had a mild upper respiratory virus for the last couple of days. He said he’d noticed nephew seeming sulky and slinking away down the side of the house after playing in the yard. He asked if he was alright and nephew turned to him with sunken eyes, blue-tinged lips and throat visibly sucking in, and rasped, “I… can’t…. breathe…”. Poor kid had been so freaked out he hadn’t even thought to come find someone - it was just lucky my husband noticed something was off.
My BIL grabbed a spacer and ventolin. My mum sprang into action, bustling nephew down to the shower to get some steam into him. The ambulance was called and within about 5mins (thank God, and amazing response in a semi-rural area) they were on scene, putting adrenaline through a nebuliser for him to breathe.
He was taken to the hospital where nurses and doctors were in the room with him all night. Three times he became similarly affected, needing more adrenaline, as well as hundreds of puffs of ventolin. They even had an emergency paediatric ambulance on standby in case they needed to take him to the Royal Children’s Hospital - called the PIPER unit, they’re able to intubate if necessary.
He was finally stabilised in the wee hours of the morning and has now been discharged.
I’m feeling immensely grateful today that we live in a time and a place where we have access to lifesaving medical care. Grateful to God that it was able to be managed with medications and he didn’t need to be intubated. Grateful that he’s on the mend and back at home. Grateful that my family have the medical knowledge and presence of mind in an emergency to know what to do. Just. Oh so grateful ❤️
3 notes
·
View notes
Text
Croup
Initial treatment consists of administration of dexamethasone via the oral or intramuscular route and administration of nebulized epinephrine to reduce airway edema. Next, you can give heliox (oxygen with helium in it).
3 notes
·
View notes
Text
624
The previous post, though not numbered, is post 623.
Today I’m in an insane amount of pain. A few days ago I complained of a muscle spasm in/on my shoulder blade. Well, today I did the dishes and cleaning and I am now taking a break. Now I can barely move it without pain. I definitely overdid it.
Moving on.
Last night was a bowling night. When I say bowling night I mean it’s a league night for…

View On WordPress
0 notes
Photo

Cough is just indication or outward reflection of an internal. #coughtocancer #coughremedy #cough #coughsyrup #coughandcold #fever #flu #covid_19 #corona #homeopathicdoctor #homeopathiccoughsyrup #homoeopathyforcough #coughcough #croup #chestcongestion #sputum #expectorant https://www.instagram.com/p/Cm4YckmyCR8/?igshid=NGJjMDIxMWI=
#coughtocancer#coughremedy#cough#coughsyrup#coughandcold#fever#flu#covid_19#corona#homeopathicdoctor#homeopathiccoughsyrup#homoeopathyforcough#coughcough#croup#chestcongestion#sputum#expectorant
0 notes
Text
Croup là gì và nó được điều trị như thế nào?
Croup là gì và nó được điều trị như thế nào?
Viêm thanh quản (Croup) là tình trạng viêm nhiễm ở thanh quản và khí quản, chủ yếu gặp ở trẻ nhỏ. Ho khan, tắc nghẽn đường thở ở các mức độ khác nhau và khàn giọng là những triệu chứng xác định.
(more…)
View On WordPress
0 notes
Text
keep overhearing people going on the tirade of their covid war stories. it blows my mind.
going to the ER is now totally normal when you (checks notes) "get the flu"
I guess? That's normal now?
One guy was going, "yeah. Apparently it messed up my thyroid and now im on meds because of the covid..."
WHY ARE YOU SITTING HERE WITHOUT A MASK YOU GOOBER!??
of course, fuking up an essential hormonal producer is just what happens I guess. Getting sentenced to a lifetime of pills or lose your hair is fuking cool.
I really do think covid has this inhibitor that makes people completely oblivious to certain dangers. I wouldn't be shocked if these "covid survivors" went to the store and saw rancid oranges just loaded with fuzzy mold and leaking fluids, and they just go, "omg! oranges!" And buy the lot to eat. There.
And that's probably the inherit evolution advantage covid has found its niche in. Like rabies happens to invoke aquaphobia, which makes the saliva more potent to deliver optimal virus. People who have had covid and took a fun vacation to the ER, are just always going to seek the virus out and contract it, and spread it.
The kids are the worst. Its going through the kid demograph where I live, and I feel so bad for these little babies - they're young, most not having capped 10 yet. But they get that croup cough and it sounds... awful.
And worst of all, there's nothing there that can really be alleviated. With upper respiratory infections, the epithelial cells in the throat and sinus cavity die and shed off. But covid embeds with the vascular tissue, and it sounds like a covid19 infection - the endothelial cells are inflamed, but coughing doesn't loosen or drain the accumulated fluids - because there are none. It's that dry, hacking, smokers cough. And it sounds awful. How are parents okay with their kids getting that sick?
Remember when parents freaked out when their kid got the flu and ran a fever? Now its like "My child is sick. TiMe To gO ShOpPinG!"
What is even going on?
#covid#covid 19#vascular infection#epithelial#endothelial#croup#mers#i mean it when I say these kids sound sick#and then there was a family and they had a baby and the parent had that terrible hacking#either someones a smoker or covid#BOTH OR WHICH ARE BAD FOR BABY#covid will be known as the inhibition disorder
0 notes
Photo

Hey May 31th anon! (*´▽`*)It’s been another year already! I hope you’re well. Thinking of you! ( ˊᵕˋ )♡.°⑅
#may 31th anon#drawing john is always such a good time for me :)#you little circular angry man#when you are reading this it is actually may 21th for me#I'm scheduling this post because I currently cannot percieve weekdays for some reason#last week I didn't realize it was my grandpa's birthday!! and when I remembered it was already 8pm and I was so sorry#luckly he didn't mind at all#grandma was not angry either she just said remember when you had croup? I can't believe that you went out and had croup#like when I was a physical baby#I did not go out and got croup recently#but I did have a very fun city trip last week!! I went to Münster! c:#I saw MANY baby ducks#and friends you won't believe it#I was window shopping at those fancy little stores#and there was this one expensive furniture and decor store with all those little vases and candles#and in the middle of all of this#proudly on display#was a BBC SHERLOCK HOLMES mug#I cannot describe what I was feeling in this moment#it felt illegal#but it was a very cute mug#it was probably very expensive but I wish I had bought it!!#but my bag was already full of this little fruit snack I had bought earlier#do you know that melon goes bad very quickly if you carry it around Münster for 6 hours in 25 degrees celcius#I did not#(I still ate it)#have a good day friends <3 :)
1K notes
·
View notes
Note
i'm very sorry to say this, but meiri, you are a foul woman for making me (a lonely lesbian) lust for a gender bent version of a canonically male character.....keep going 👍
in a more just world there would be no more male characters and the female characters would be as diverse as them. in a just world a female character would be a 197cm tall bald lying secretive corpse-desecrator who would attack her childhood friend and almost-adopted-sister on sight, spitting in her face that it was she who slept by their mentor's feet like a dog. in a just world a female character would be a vaguely futchy¹ bipolar alcoholic who tries to self-immolate in front of you, participated in a colleague's murder with her sister (or did she?), delirious from guilt, illness and drink (and it NOT being the "sexualized crazywoman" trope. because she'd be worse), whose sister would be protective of her like a rabid dog. in a just world a female character could be a brown-eyed brunette in a tacky snakeskin coat, arrogant, haughty until circumstances beyond her comprehension break her spirit, able and willing to tell someone that if they're that much of a pussy about killing themself she'll fucking help. in a just world a female character could be butcher [as in the cutter of meat.], daughter of butcher, feared for her perceived violence but not more wicked than any other, collecting organs and keeping them in her little pouch.
but it is not a just world. so fine. (rolls up sleeves) i'll do it myself.
¹ the butch-femme scale is not real and therefore "futch" or "futchy" isn't either. however that is a really funny word for a joke
#when i typed ''artemida isidorovna burakh you are a stronger woman than i am. if my lesbian colleague was a brown-eyed brunette#with hairy arms and a little girlstache i would have had to be escorted out of the building#with ropes pushing on my croup like a wild horse'' meant it. as a man he's going to get the pit. as a woman...... she and i could fight#about it first. okay#thank you/you're welcome by the way. they're almost more like OCs at this point i pretend i don't even see it.#they're like. these men's sisters.#actually i have better: i have a hc that all tragedians are women and in my mind i think about tragedians being ''assigned'' a person to#''play'' so. those are the women under the masks......... yes............#rule 63#<- speaking of it. also if you don't want to read me speak about it
32 notes
·
View notes
Text
Cannot be understated how funny Croup eating that statuette is, especially in the audiobook, because he sits there talking about how beautiful it is for ten seconds, with you not knowing what he's getting at until Vandemar goes "are you gonna have it for later or" and "no I'll eat it now" followed by a bunch of crunchy eating noises. The whiplash. Bonus points for Mr V just awkwardly sitting there waiting + asking if it's tasty like he just does not get it but he's supportive. God bless.
65 notes
·
View notes
Text
"Laryngotracheobronchitis? Really? You literally couldn't get any sicker than this."
Whumpee tries to reply but is cut off by loud, hoarse, barking coughs that scrape their throat and chest. When they recover, their voice is a faded whisper.
"The doctor could have just called it croup. You wouldn't have freaked out as much, at least."
"Diagnosis aside, that cough is enough to freak me out anyway. Come. Let's take your poor destroyed lungs home. You really need to be in bed, with tea, cough drops, and a nebulizer."
#listen as someone who has had to deal with croup as an adult too i'm disappointed with how rarely used it is#it's so miserable#i had the last bout around last christmas and it was horrible but i kept thinking how good that would be in sickfics#colds#coughing#caretaking#sicknario
109 notes
·
View notes
Text
Reviewing questions:
Blindness is a potentially devastating complication of sarcoidosis. Ocular sarcoid can develop in up to half of all cases and most commonly presents as anterior uveitis or keratoconjunctivitis. The most serious complication is optic neuritis.
A complete ophthalmologic examination at the time of diagnosis is recommended, as asymptomatic disease can result in permanent visual impairment. All patients with sarcoidosis should have a careful history and physical examination to identify other organ involvement before having further testing, including ECG, pulmonary-function testing, and baseline laboratory studies (calcium level, alkaline-phosphatase level, renal-function, and hepatic-function tests) to evaluate the extent of disease.
McConnell's sign is defined as right ventricular free wall akinesis with sparing of the apex. Typically this looks as if the apex of the RV is a trampoline. Echocardiogram shows right ventricular strain and a positive McConnell sign, which is indicative of pulmonary embolism (PE).
All patients who have known or suspected bronchiectasis and who are acutely ill with suspected lower respiratory tract infection should be empirically treated with an antipseudomonal antibiotic, such as cefepime until culture results are available to guide treatment decisions.
Heerfordt’s syndrome (uveoparotid fever) is another collection of clinical findings specific enough to diagnose sarcoidosis without a biopsy. These signs and symptoms include uveitis, parotid gland enlargement, and facial nerve palsy.
Lofgren’s syndrome is a form of acute sarcoidosis. Sarcoidosis is a multisystem disease characterized by the presence of noncaseating granulomas and although classically described in African Americans, it has one of its highest prevalences in the northern European population. Clinical variants exist with certain forms having diagnostic and prognostic value. Lofgren’s syndrome is the combination of erythema nodosum, bilateral hilar adenopathy, migratory polyarthralgias, and fever. This pattern is so consistent that it has 95% diagnostic specificity and allows diagnosis of sarcoidosis without a biopsy. Among European patients, the presence of Lofgren’s syndrome portends to a good prognosis. For mild disease symptomatic treatment with non-steroidal anti-inflammatory agents is reasonable or low dose prednisone may be added.
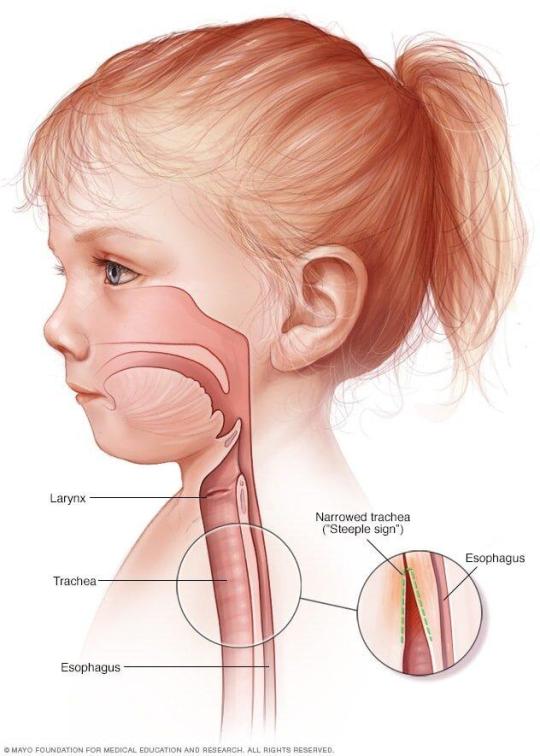
The optimal management of laryngotracheitis (croup) is determined by the severity of disease. There are numerous scoring systems for croup severity, with the Westley croup score being the most validated and most often used. The Westley croup severity scale includes evaluation for the presence of stridor at rest, retractions, and cyanosis as well as assessment of mental status and air entrance. Regardless of any official scoring system, most physicians would consider the presence of retractions and stridor at rest to be indications of moderate to severe disease that requires evaluation in the emergency department. The presence of cyanosis, confusion, depressed mentation, agitation, severe retractions, or absent breath sounds would indicate severe disease and/or the possibility of impending respiratory failure.
Mild cases of croup are treated on an outpatient basis with cool mist therapy and fluid replacement. Moderate cases may require supplemental oxygen, oral or intramuscular corticosteroids, or racemic epinephrine. Severe cases are best treated with hospitalization and racemic epinephrine.
Bottom Line: The most important step in initial management of laryngotracheitis includes nebulized epinephrine (racemic or L-epinephrine) and dexamethasone along with humidified oxygen, fever reduction, and hydration. Epinephrine acts almost immediately, while steroids have a delayed onset of action.
Pneumothorax is defined as a collection of air in the pleural space. The result is pleural separation of the visceral and parietal pleura. Spontaneous pneumothorax lacks an antecedent event (e.g. trauma). There are two types: primary and secondary. Primary spontaneous pneumothorax (PSP) occurs in patients without recognizable underlying lung disease. Secondary spontaneous pneumothorax (SSP) occurs in patients with visible underlying lung disease (e.g. COPD). The most common etiology of PSP is rupture of a subpleural bleb (which are usually not seen on imaging and are undiagnosed). Many cases initially diagnosed as PSP may eventually be diagnosed as SSP after further workup.
Management depends on the size of the pneumothorax. The spectrum of management includes watchful waiting, aspiration, chest tube insertion, and thoracoscopy with pleurodesis or lung resection.
Rhinosinusitis can be defined as either viral/bacterial and if bacterial, as complicated/uncomplicated. Complicated rhinosinusitis implies the extension of disease outside the nasal cavity/sinuses into adjacent structures, such as soft tissues, ophthalmologic tissues, and nervous system.
Current criteria for the presumptive (many of these cases may still be viral) diagnosis of acute bacterial rhinosinusitis (ABRS) include persistent symptoms lasting more than 10 days without any evidence of clinical improvement or a biphasic illness pattern which is also called double worsening, meaning the patient was sick, improved, and then became sicker a second time within a short time frame, usually within a 10 day period. The IDSA guidelines from 2012 also recommend the use of a high fever greater than 39C associated with severe symptoms for 3-4 days as being more consistent with bacterial rhinosinusitis. According to the guidelines by the American Academy of Otolaryngology-Head and Neck Surgery published in 2015, fever itself early in the course of illness is not sensitive or specific enough to warrant treatment based on this vital sign alone, and they do not recommend using this as criteria for the diagnosis of ABRS. They agree with the other criteria used by the IDSA and acknowledge that a "severe" presentation may warrant the use of antibiotics as recommended by the IDSA and the American Academy of Pediatrics which considers more than 3 days of high fever and purulent nasal discharge as a severe presentation of ABRS in children.
Summary Criteria for the Diagnosis of ABRS
Signs or symptoms of acute rhinosinusitis present for 10 days or more after symptom onset with no improvement
Acute worsening of improving rhinosinusitis within 4-6 days of symptom onset or "double-sickening."
Severe rhinosinusitis: onset of high fever greater than 39C and severe symptoms within 3-4 days of onset
Tx of ABRS: amoxicillin, amoxicillin-clavulanate, doxycycline if PCN allergic, or respiratory fluoroquinolone in kids who can't take doxycycline. I just had a pt in clinic who had bacterial rhinosinusitis and I gave him amoxicillin-clavulanate.
Bottom Line: In patients with ABRS who require antibiotic therapy, the initial therapy of choice is with amoxicillin with or without clavulanate.
One of the feared complications of acute bacterial rhinosinusitis (ABRS) is orbital cellulitis. This infection commonly develops in the setting of ABRS due to the direct extension of bacteria from the sinus cavity into the orbit. Commonly it can project through the roof of the maxillary sinus. Additionally, there can be extension through the adjacent soft tissues. The diagnosis of this condition is clinical and is confirmed with radiographic imaging (CT scan of the sinuses). The presence of pain/difficulty with eye movement, double vision, eye swelling, and erythema should be concerning for orbital infection. The initial imaging test of choice would be with a contrasted CT study of the face and orbits. An MRI could also be performed and has similar accuracy, but is generally slower and more expensive to obtain. Additionally, patients with suspected orbital cellulitis should be evaluated by ophthalmology in the emergency department and started on IV antibiotics with coverage for MRSA (vancomycin generally).
If the sinuses are the suspected source, ampicillin-sulbactam or piperacillin-tazobactam can be added to vancomycin as long as there is no concern for CNS involvement. If the CNS is involved, it should be noted that both ampicillin-sulbactam and piperacillin-tazobactam have relatively poor CNS penetration, and a 3rd generation cephalosporin (ceftriaxone) should be used with the addition of metronidazole for coverage of anaerobic organisms. General guidelines for sepsis and infection should be followed with the physician obtaining the regular laboratories including a complete blood count, metabolic profile, blood cultures, and lactate.
Symptoms of Complicated ABRS:
Proptosis or impaired extraocular movements
Painful eye movements
Diplopia or impaired vision
Periorbital edema or erythema
Cranial nerve palsies
Altered mental status
Neck stiffness/meningeal signs
Papilledema
Complications of ABRS:
Meningitis
Orbital cellulitis
Cavernous sinus thrombosis/thrombophlebitis
Preseptal cellulitis
Ruptured eardrum:
Tympanic membrane perforations are commonly caused by trauma or acute otitis media and are usually noted on otoscopic examination. Perforations with marked hearing loss or other concerning neurologic signs such as nystagmus, ataxia, or vomiting should receive a prompt evaluation by an otolaryngologist. Supportive care only is a perfectly reasonable treatment plan for patients with simple perforations with minimal hearing loss and no neurologic signs. Many perforations will heal spontaneously within 4 weeks and require no intervention.
#sarcoidosis#McConnell#Heerfordts syndrome#Lofgrens syndrome#Lofgren#croup#PTX#sinusitis#rhinosinusitis#ruptured ear drum
3 notes
·
View notes
Text
I want to know so badly what in the name of all that is holy Mr Croup and Mr Vandemar are.
I'm very sure they cannot exist on their own without the other.
The seem human, but they don't have blood, and eat so many fucked up things, and heal too easily, and don't seem to hurt ever.
Their entire purpose seems to be killing. They are probably very, very ancient. They are very bound to their contracts (well, at least by honour). They belong to the Underside but they can move through the Upside just as well.
They are fucked up in so many ways. They are fascinating in so many different way. Peak character design, really, they're terrifying - but what are they??
56 notes
·
View notes
Text

Whippet, now whippet good.
#bark bark bark#border collie#<- i fuckin promise#tried to ask about depth of loin in the conformation border collie group and they didn't even know what I was talking about#Her short croupe and depth of loin give her the impression her spine is curved and she has a bad top line but it's all muscle I promise#Ever
15 notes
·
View notes
Text

Did I tell you guys I made Vi in BG3 and she was running around naked and met Gale and immediately took his underwear. Did you know he likes to wear a cute bra and matching panties? Now you do.
17 notes
·
View notes
Last Seen Blogs

superwedgieboy
Superwedgieboy

gjtothedc-blog
THE TRASHES OF ALL TRASHES


nicksayssummer
And So It Goes

toomanydice
Sydney Does Art Sometimes