#dutch model

Text

Lars Verschoor
Such a cute looking Dutch model from the Netherlands, born 25 January 2003 🔥
via larsverschoor
235 notes
·
View notes
Text








✧・゚: *✧・゚:* angelic beauty ✧・゚: *✧・゚:*
#adriana lima#doutzen kroes#ruslana korshunova#girlblogger#lana del rey#fashion#2000s fashion#victoria secert model#vlada roslyakova#victoria secret#vs angel#angelic coquette#angelic aesthetic#angelic beauty#brazilian bombshell#brazilian beauty#dutch model#vogue#black swan#russian dolls#coquette#divine feminine#hyper feminine#feminine beauty#femininity#gaslight gatekeep girlboss#romantizing school
140 notes
·
View notes
Text

Bella Hadid for Vogue Russia March 2019
Photographer Giampaolo Sgura
Fashion Editor/Stylist Celia Azoulay
Makeup Artist Maud Laceppe
Hair Stylist Franco Gobbi
Newest Cool
#newestcool#newest cool#Bella hadid#isabella khair hadid#hadid#hadid icons#fashion editorial#vogue editorial#fashion photography#vogue magazine#Celia Azoulay#vogue russia#giampaolo sgura#fashion photoshoot#beauty shot#model portrait#dutch model
74 notes
·
View notes
Text



27 notes
·
View notes
Text

Doutzen Kroes
Dutch Model
16 notes
·
View notes
Photo
Alani Mini Dress
70 notes
·
View notes
Text


Rianne van Rompaey for Le Goût de M 2023
by Robin Galiegue
#rianne van rompaey#supermodel#dutch model#beauty#robin galiegue#m le monde#m le magazine du monde#fashion#fashion photography#fashion editorial#editorial#black and white photography#ss23
33 notes
·
View notes
Text

Doutzen as Catharina in Nova Zembla, 2011.
20 notes
·
View notes

Text

Lars Verschoor
A toast with the divine Dutch model Lars Verschoor is always welcome 🥂
40 notes
·
View notes
Text
Ellen Soeters in Scheveningen, jaren '80
14 notes
·
View notes
Photo
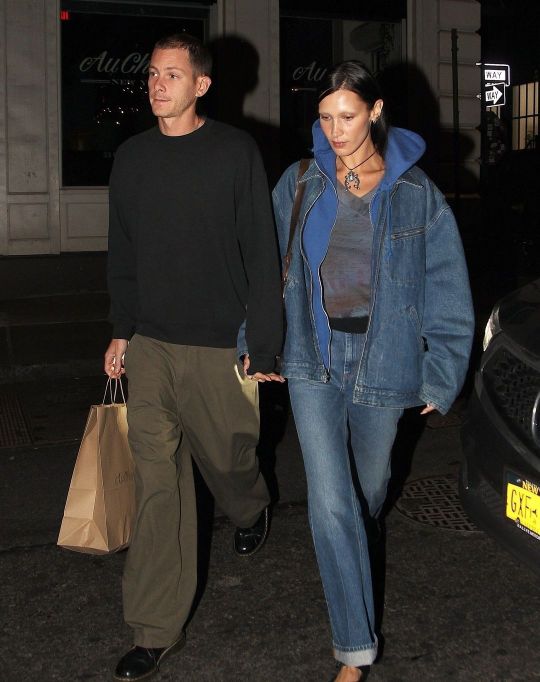


Bella Hadid and Marc Kalman leaving Au Cheval in New York, 10 October 2022
Photographer Said Elatab
Newest Cool on Instagram
#newest cool#newestcool#Bella hadid#Isabella hadid#Isabella khair hadid#palestinian#Arab model#dutch model#supermodel#Hadid sister#Hadid sisters#marc kalman#ny street style#celeb street style#New York street style#said elatab#Bella Hadid & marc kalman#bellahadid#gigi and bella
70 notes
·
View notes
Photo

Jessie Bloemendaal
Balmain - Men fashion week SS19 by Jean Baptiste Soulliat
Book┃IG
23 notes
·
View notes
Text

Lilly Becker with Baby Bump
Dutch Model
7 notes
·
View notes
Text

By: Bernard Lane
By: Mar 5, 2024
The gist
The puberty blocker-driven “Dutch protocol” of medicalised gender change—administered to ever more teenagers around the world—appears more likely to come under serious scrutiny in its home country.
The parliament of the Netherlands has now passed two motions this year calling for a closer look.
On February 27, with a majority of 101 out of 150 votes, the parliament approved a motion asking the government to commission research.
This would compare the outcomes of the Dutch protocol with the results of new, more cautious treatment policies in other European countries, such as Sweden, where non-invasive psychosocial techniques are now favoured as first-line responses to gender distress.
On January 25, the parliament approved a motion—proposed by Diederik van Dijk of the conservative Calvinist Reformed Political Party (SGP)—that the government seek advice from the independent Health Council on the medico-legal implications of medicalised gender change for minors.
Both motions were opposed by the temporary Health Minister of the Dutch administration in caretaker mode, but cabinet negotiations are under way and expected to produce a new, more responsive government reflecting the success of centre-right and populist-right parties in last November’s elections.
“I think this [second motion] will exert extra pressure on the new minister of health to initiate a review of the puberty blockers in one way or another, be it the Health Council or another institution,” said media sociologist Dr Peter Vasterman, who has been calling for independent evaluation of gender medicine in the Netherlands before any expansion of capacity.
“We don’t have a new government yet, but it will probably be a right-wing variant. So, there is a good chance that this topic will finally be put on the agenda and a review will be conducted of current trans care.”
--
The detail
Parties supporting the February 27 motion included the centre-right New Social Contract (NSC) party of Peter Omtzigt, the right-wing populist Party For Freedom (PVV) of Geert Wilders and the populist-right Farmer-Citizen Movement (BBB) of Caroline van der Plas. The motion was spon.sored by NSC member Dr Rosanne Hertzberger.
Among those opposed to the motion were GreenLeft-Labor (GL-PvdA), the social-liberal party D66, the Socialist Party (SP) and the Christian Democratic Appeal party (CDA).
The objections raised by Health Minister Pia Dijkstra, of the D66 party, included privacy risk, the difficulty of the research proposed, the redundant nature of the research proposed, and the ethics of using randomised clinical trials (something not proposed by anyone).
Dr Hanneke Kouwenberg, a Dutch radiologist and nuclear physician who has followed the gender clinic debate, said she was angry at the denial and hypocrisy of parties seeking to block the motion.
“As often happens, opponents of a more fundamental scientific approach in this debate do not substantiate their position with arguments, but rather with emotional blackmail,” she told GCN.
“It is deeply disturbing that research aiming to examine whether Dutch gender care has better outcomes than other countries, which indeed might substantiate the claim of successful selection of treatment candidates, is being vilified by parties perceived as ‘progressive’ and ‘left wing,’ whilst the minister goes so far as to call such research ‘unethical’—which is especially bizarre since no intervention is needed in the proposed research.
“It once again shows how much the parties resisting [inquiries] do not have the interests of minors, nor quality of care, in mind, but consciously and repeatedly close their eyes to a practice whose benefits have never been substantiated but whose drawbacks are increasingly coming to light.”
“More and more teenage girls are choosing to change their gender around the world. In Quebec, the health system responds very quickly to their requests for medical transition by prescribing blockers, testosterone and mastectomies. These young girls often present with several mental health problems and many wonder if we give ourselves the time to evaluate everything that is going on in their heads. Is it normal for a 14-year-old girl to get a testosterone prescription within minutes? And what happens when they change their minds?”—Documentary, the French-language arm of Canada’s CBC public broadcaster, 29 February 2024
Watch the ethics
A spokeswoman for the group Genderpunt, which advocates for more open debate about gender medicalisation, said the Dr Hertzberger’s February motion with its focus on comparative outcomes might seem more palatable to government, although she suggested that if the job were given to Dutch gender researchers it might be undermined by “gender-affirming” groupthink.
She said it was possible that the ethical and medico-legal analysis called for by Mr van Dijk’s January motion would prove “far more interesting.”
“Is it ethically justified to take the risk that a minor will, in the long-term, regret gender-affirming care and have to deal with the consequences for the rest of his life? How is this child protected by national and international law (like the Convention on the Rights of the Child).”
Science: egalitarian or authoritarian?
Before her recent election to parliament Dr Hertzberger was a microbiologist studying the little understood bacterial makeup of the human vagina, a field with implications for the reproductive and sexual health of women.
“For instance, it is unclear why humans are the only apes with this high acidity and dominance of Lactobacillus whereas these characteristics are absent in other primates. Why is the human vagina such a good host for these specific bacteria?” she says on her website.
She carried out her research thanks to the hospitality of a lab at the VU University Amsterdam, which is also home to the gender centre whose Dutch protocol for “juvenile transsexuals” culminates for males in castration and the surgical creation of a pseudo vagina.
Dr Hertzberger has practised “citizen science” with the rationale of engaging ordinary women in research to develop a probiotic to modify the vaginal microbiome. She is also an advocate for “open science” whereby all findings, even negative results, are made public.
“The general aim is to increase scientific efficiency by sharing as much information as possible with other scientists and the general public,” she says.
She has also reflected on the role of science in society, publishing an essay with the title The great nothing: Why we have too much faith in science. Her thesis is that science is muscling into the moral vacuum left by organised religion.
“I see a new generation of Western secular policymakers, politicians, administrators, thinkers, writers, entrepreneurs and leaders who no longer see science as a tool for generating knowledge, but as a new infallible authority; an all-knowing judge who decides what is good and what is evil,” she writes.
Video: Dutch MPs debate gender clinics
youtube
Vision necessary
Dr Hertzberger’s motion was put in the context of the international scientific debate over youth gender dysphoria and reports to the Dutch parliament acknowledging missing data and a “lack of visibility” into local gender patients.
A familiar narrative in the Netherlands has been that the pioneering Dutch protocol was a source of pride and that any concerns arose from its less careful application in other countries. However, the rigour and ethics of the key Dutch studies establishing the protocol have recently come under much sharper scrutiny both in the Netherlands and internationally.
During the February 15 debate of motions proposed by her and other MPs, Dr Hertzberger said: “The decision to treat these children with puberty inhibitors is taken at an early age, 14 to 15 years on average, during a period of major hormonal, physical and mental changes, based on symptoms that are not objectively quantifiable.”
“We have seen in recent years how other European countries have become more reluctant to treat minors according to the so-called ‘Dutch protocol’. More importantly, the reports before us today show a lack of visibility [into Dutch gender patients].
“We see in Sweden, for example, that they have temporarily really stopped puberty inhibitors altogether and only allowed them in experimental settings. We are very curious to see what happens to that cohort of patients in the end and how their wellbeing goes.
“This [shift to more cautious treatment] comes not only from politics and not only from society, but also from healthcare itself and from science.”
“The Endocrine Society (ES) is updating its clinical practice guidelines on ‘gender-affirming care.’ ES, however, appears to be putting its thumb on the scale in favor of medical interventions by appointing experts with serious conflicts of interest to its guideline-development group, ignoring its own standards for how to write trustworthy medical recommendations, and trying to keep the process hidden from the public.”—Leor Sapir, news article, City Journal, 27 February 2024
“It’s noteworthy that most of the authors of ES’s 2017 clinical practice guidelines were also big names at WPATH [the World Professional Association for Transgender Health]. Two—Peggy Cohen-Kettenis and Louis Gooren—were Dutch pioneers of pediatric gender medicine. Despite the perception that ES and WPATH are separate entities, and that recommendations on behalf of ‘gender-affirming care’ are not just made by trans advocacy groups but also by run-of-the-mill U.S. medical groups, the truth is that WPATH members used ES as a guise for embedding hormonal interventions as an accepted standard of care in the United States.”
Why the data drama?
Aside from her successful motion, Dr Hertzberger put up another which did not go forward. This sought data to compare people diagnosed and treated in Dutch gender clinics with those on waiting lists.
She noted that the patient group seen today—dominated by teenage females—was different from the past group of mostly males with gender distress stretching back to early childhood.
“I am really puzzled by this [resistance of some MPs to requests for more data], because there is a report [to parliament] that says there is too little visibility into this group [of patients] and the medicalisation of this growing group of children and adults,” she said.
“We are particularly interested in the children. We see major changes in recent years in European countries that have changed their standard of care [Finland was first in 2020, followed by Sweden in 2022 and England issued a new, cautious draft treatment policy in 2023—GCN.]
“Surely that is a goldmine of data which, by the way, we can easily collect in anonymised and aggregated form, as we so often do.
“I really want to ask [Health Minister Dijkstra] why she does not want more data on this important development [in gender dysphoria], which also has medical-ethical consequences,” Dr Hertzberger said.
Dr Vasterman told GCN that it was quite reasonable to request current data on patient registrations, diagnoses and treatment at Dutch gender clinics.
“It is unacceptable that no new data has been provided for years now, which makes it very difficult to evaluate current trends, such as the shift in sex ratio [of patients] and the rise of non-binary identity among young girls.
“These developments have huge impact on the needs for trans care but without data it is difficult to develop new a policy.”
“Despite claims that blocking puberty gives time for decision-making, no one can answer the obvious: How is it possible for a child to discover ‘This isn’t as bad as I feared,’ when they are blocked from experiencing it? Fears are resolved by confronting them, not avoiding them.”—Sexual behaviour scientist Dr James M Cantor, tweet, 3 March 2024
Not our problem
Dr Kouwenberg said that “Dutch politics has long acted as if there were no problem with the Dutch protocol,” despite last October’s breakthrough Zembla documentary on the flawed design of key studies, critiques in international journals and the shift to caution of progressive European countries.
“And if there were a problem, it was invariably stated that the problems abroad were due to a poor selection of candidates for puberty blockers, that in the Netherlands, work was being done very carefully, and only children who were actually ‘trans’ [those whose gender dysphoria would not desist with the passage of time] would be treated with puberty blockers. The concerns of critics were always dismissed as moral panic and fear-mongering,” Dr Kouwenberg told GCN.
“It comes as no surprise that there is actually no test, let alone a validated one, to distinguish desisters from persisters prospectively, and Dutch medicine does not possess crystal balls to predict the future. Nevertheless, the gender clinic in Amsterdam [which developed the Dutch protocol] and the politics associated with it have long been able to stave off further investigation with statements like these.”
“With this motion [by Dr Hertzberger], it seems that finally an end has come to a long period of denial of the altered reality at the gender clinics and of the criticism of the approach for gender dysphoric youth.”
#Bernard Lane#Dutch protocol#Dutch model#gender affirming care#gender affirming healthcare#gender affirmation#affirmation model#medical corruption#medical malpractice#medical scandal#queer theory#gender identity ideology#gender ideology#medical mutilation#puberty blockers#wrong sex hormones#cross sex hormones#gender lobotomy#religion is a mental illness#Youtube
3 notes
·
View notes
Last Seen Blogs

cuckfuck4daddy
Dominate Me

degrassi-fandom-confessions
Welcome to Degrassi

hanzajesthanza
the witcher books

arildsen60braswell-blog
Untitled

younginnjuice
Flipper
25