#gabaergic
Text
Me, Myself and Progesterone
I touched on progesterone (P4) in my last transgender update post. I am not quite sure if progesterone is working in the way I want it to. My biggest annoyance with it is feeling like my brain is on fire just before trying to sleep.
Rewind to late February 2024, for almost three weeks my progesterone dose was doubled to 400 mg of oral, micronised, compounded progesterone – 200 mg twice a day. That’s up from the 200 mg once at night.
I had also ceased finasteride. And finasteride interferes with the progesterone (oral) pathway conversion to neurosteroids such as allopregnanolone. This is because finasteride blocks *most* of the activity (~70%) of the 5-alpha reductase (5AR) enzyme. In turn, reducing levels of allopregnanolone – or at least slowing their conversion to neurosteroids.

My sleep quality has been pretty broken for a while now. Look at those orange blocks. And here I was looking forward to some of the benefits from progesterone. Anxiolytic? Yes please! Sleep improving? Definitely!

Instead I get this whole brain fire thing and feel like I’ve taken an anxiogenic. That got me thinking, brain on fire? Throw in some formication and it’s what feels like a glutamate rebound or surge. Excitotoxicity perhaps?
I’ve experienced similar feelings while withdrawing from pregabalin (decreases glutamate levels) and trusty old diazepam (increases GABA levels). Definitely that same feeling though. It appears that taking what I would consider a small dose (2 mg) of diazepam negates the insomnia pretty well. Even though diazepam isn’t a terribly good choice for sleep. It takes me from being a wired insomniac to sleeping beauty in about an hour.
Another interesting side effect I am seeing a lot more of is dissociation. Ordinarily, I would only experience this while in high stress, high anxiety situations but recently I’m noting it a lot more just doing chores around the house – which is a little concerning.
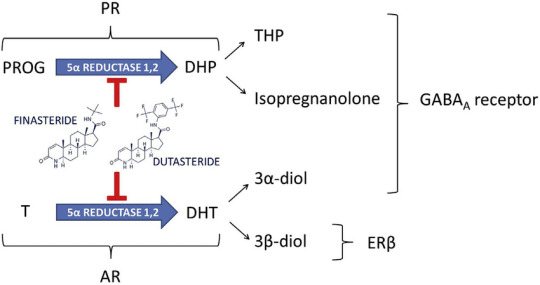
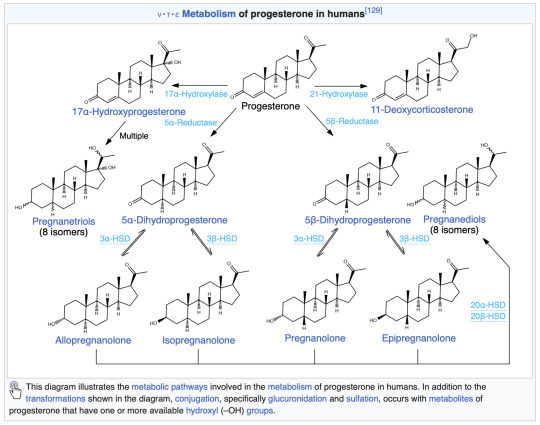
Regardless, it seems that something is messing with my GABAergic system and metabolites of progesterone fit the bill. Armed with my two-thirds of a biomedical science degree I went digging for more information on the metabolites. Up above is an image from my last health blog post. Note the action of finasteride on progesterone – blocking allopregnanolone (THP) and isopregnanolone.
I wonder if moving to a more potent 5AR blocker, such as dutasteride, would reduce the side effects of a higher dose of progesterone? A question for my endocrinologist I suppose. I restarted my finasteride to at least partially block some of the following progesterone metabolites. Let’s look at the metabolites a little closer and how they act.
Allopregnanolone (Tetrahydroprogesterone or THP)
Positive allosteric modulator
9 hours
Pregnanolone
Positive allosteric modulator
1 – 3.5 hours
Isopregnanolone
Negative allosteric modulator
14 hours
Targets allopregnanolone only
Epipregnanolone
Negative allosteric modulator
Half-life unknown
Alright, so a bunch of neurosteroids are doing a bunch of things. A few are being blocked, but also produce negative side effects when they weren’t blocked. Hormones are messy. Where does that leave me? I guess I am left questioning whether I should be taking progesterone at all. At minimum a dose reduction is definitely called for. I will probably return back to 200 mg and see what symptoms, if any, follow.
My search revealed some interesting data with overlap in symptoms shared with premenstrual syndrome (PMS) and premenstrual dysphoric disorder (PMDD) in cisgender women.
PMDD is believed to be caused by fluctuations in gonadal sex hormones or variations in sensitivity to sex hormones.
If sensitivity to level shifts is reason for the negative side effects, then single or even twice daily doses are probably not enough to smooth out the levels of neurosteroids for me, allowing me enter a withdrawal state, perhaps? Brain on fire? This paper offers some great insight into the mechanisms behind it all with some interesting side notes on SSRIs.
Interestingly, SSRIs increase allopregnanolone levels in the brain, rapidly and at low doses, as demonstrated in rodents as well as in patients with depression.
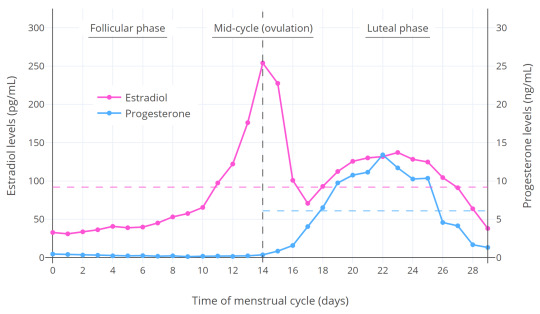
Could this be one of the reasons why I can’t tolerate SSRI/SNRIs? At the very least, it’s some food for thought. Worth noting that the original study has been questioned a little further along in the paper. Let’s circle back to those progesterone levels again. From Wikipedia
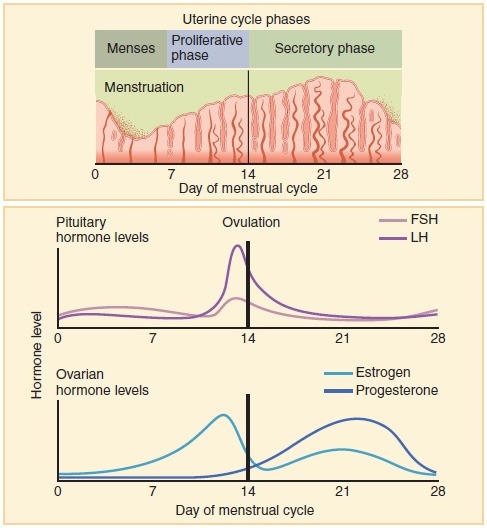
Progesterone levels tend to be less than 2 ng/mL prior to ovulation and greater than 5 ng/mL after ovulation.
What were my most recent levels again? 9.1 nmol/L or should I say 2.6 ng/mL (freedom units). That’s at 200 mg once daily at night, measured in the trough. I really need to ask myself, do I want to have symptoms of PMS/PMDD? Is that even a question that needs to be asked?
Looking at the levels on Table 1 in this paper give an idea where my levels line up. If you factor in the short half-life of most of the metabolites, once daily dosing is probably a bad idea. Ideally, I should look into getting the dose split to 100 mg twice daily.
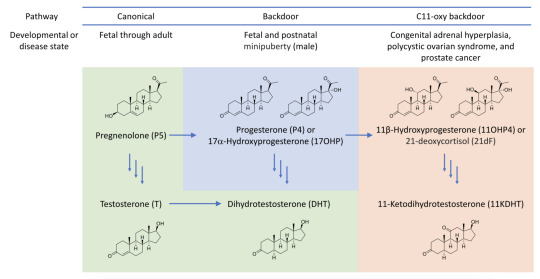
Of course I have to be mindful of negative risk such as the androgen backdoor pathway. This has the potential to generate unwanted androgens like DHT – which will affect the hair on my head. That’s why the finasteride is here to stay until most means of testosterone generation is removed from my system…
It’s not all bad though. Finasteride competes with progesterone for the 5AR enzyme – which results in even less 5AR being available for testosterone -> DHT conversion. Another point worth considering is that progesterone has a positive effect on bone-building cells (osteoblasts). This can help with avoiding or reducing effects of osteoporosis.
Touching on side effects I’ve noticed, Progesterone should increase libido. Which is something I do not want due to past trauma. However, I wonder if the finasteride side effects are at play here. Again, I don’t consider them negative side effects either.
Other oddities I’ve also noticed my facial hair has become darker at the higher progesterone dosing at 400 mg. My upper lip now has dark black hairs, that’s new and unwanted. It might be useful for IPL treatment. But now there’s shadow on my upper lip I never had before. It isn’t just the thinning of skin either. The hairs are black instead of blonde.
One big uncertainty is that I’m not sure what my levels of estradiol will be at the next blood test. Are the 200 mg of pellets doing their job properly? Or did they fail? Does the dose need to be increased?
For now, I’ve been supplementing the implant with the remainder of my 2 mg estradiol pills while the pellets stabilise. One pill gives me ~85 pmol/L in estradiol levels. I’ve only just ran out of those so now I’m adding in some of the estradiol gel (Sandrena branded). These gave ~200 pmol/L estradiol per dose according to my most recent blood tests. In theory with one a day, I should be guaranteed to be in the late follicular phase – regardless of the implant levels.
Anyway, that was one heck of an info dump. I think that sums everything up that has been on my mind lately.
TL;DR
400 mg oral progesterone makes my brain go on fire. Progesterone metabolite levels shifting around are very activating for me. I will now target cisgender progesterone levels in the late follicular phase. Hormones are complicated. One size fits most seems to be at play when it comes to progesterone. Nothing like some trial and error! 🙃
#transgender#transfem#trans#lgbtq#queer#progesterone#estrogen#GAHT#HRT#allopregnanolone#pregabalin#diazepam#GABA#finasteride#PMS#PMDD#GABAergic#brain on fire#fire brain#brainly fires#firely braining
1 note
·
View note
Text
me when i get out of bed after waking up tachycardic with 5 hours of drunken sleep
[ID: A gif of a white man dropping his backpack and collapsing to the carpet floor, face down. /End ID]
#POTS and hangover sure go well together /s#i also did not take my seroquel bc it was too dangerous.#didnt expect to use enough to be inebriated for almost ✨️ 12 hours ✨️#“your body clears 1 drink an hour” yeah well it feels like 2 if you add more GABAergics into the mix. go figure#dont do that btw. very dangerous.#julian rants#alcohol tw#drugs tw#vent
13 notes
·
View notes
Text
harm reduction my beloved
#huge difference between now and the last time i drank and drugged#thought i was going to die the last time#right now i have pretty good confidence that i'll survive tonight#hell yeah#around 8 shots in on 3 other GABAergics (including 3.4g of gabapentin today)#and i feel like im on 3 shots. maybe 2. without tolerance#oh my GABAergic tolerance is absolutely fucked#and this time it's not entirely my fault. psych ward gave me 2 more GABAergics#very potent ones too#julian rants#vent#drunk posting#posting under the influence#drugs tw#alcohol tw#harm reduction#addiction#alcoholism
12 notes
·
View notes
Text
out of nowhere my brother decided to stop being straight edge & is finally trying drugs lol
#so excited to finally have someone to do drugs with#someone who i legitimately enjoy hanging out w them not just because they get me high#just weed psychedelics & some dissociatives. maaaybe some of the milder stimulants & gabaergics#so no hard drugs lol i would never encourage that#but i doubt that he would ever be interested in that#since i think me being addicted to drugs is what made him not even want to smoke weed or anything at all for the longest time
7 notes
·
View notes
Text
Thanks to my recent Plans TM and shit + good conversations with @indigochromatic @whybrainhere and @reimeichan (shouting out cause they're awesome people / blogs and great individuals to chat about experiences with; ily guys) about ADHD and neurotransmitters I've started getting a bit really into reading about neurochemistry / neurobiology as well as the similarities and differences with Autism and I have to do something else so I havent finished reading this but for those that are interestsed
I found a really good article that is open access to read about the GABAergic function in autism across a large number of different studies and methods of exploring the relationship between GABA and autism.
It's a relatively "hard" read I think (especially in some parts if you aren't familiar with transgenic rodent models and genetics / neurobiology) but its really informative so far
For those up for it and with the time, I do recommend. It cites some interesting studies that have made my reading time on this stupid longer cause I keep falling down rabbit holes of the cited studies help
3 notes
·
View notes
Text
my paper on the neurobiology of sleep and the role of some previously-uncharacterized GABAergic cells got accepted, so I’ve been taking all these semi-artsy photos of mice on cortical EEG traces to hopefully send to the journal as cover art.

39 notes
·
View notes
Text
how do i build self-discipline without willpower in the first place. is there a nootropic or gabaergic for this
6 notes
·
View notes
Text
Interesting Papers for Week 1, 2023
How Stimulus Statistics Affect the Receptive Fields of Cells in Primary Visual Cortex. Almasi, A., Sun, S. H., Yunzab, M., Jung, Y. J., Meffin, H., & Ibbotson, M. R. (2022). Journal of Neuroscience, 42(26), 5198–5211.
Neural circuit mechanisms of hierarchical sequence learning tested on large-scale recording data. Asabuki, T., Kokate, P., & Fukai, T. (2022). PLOS Computational Biology, 18(6), e1010214.
Shared resources between visual attention and visual working memory are allocated through rhythmic sampling. Balestrieri, E., Ronconi, L., & Melcher, D. (2022). European Journal of Neuroscience, 55(11–12), 3040–3053.
Spatiotemporal dynamics of noradrenaline during learned behaviour. Breton-Provencher, V., Drummond, G. T., Feng, J., Li, Y., & Sur, M. (2022). Nature, 606(7915), 732–738.
Development of visual response selectivity in cortical GABAergic interneurons. Chang, J. T., & Fitzpatrick, D. (2022). Nature Communications, 13, 3791.
Distinct neural codes in primate hippocampus and lateral prefrontal cortex during associative learning in virtual environments. Corrigan, B. W., Gulli, R. A., Doucet, G., Roussy, M., Luna, R., Pradeepan, K. S., … Martinez-Trujillo, J. C. (2022). Neuron, 110(13), 2155-2169.e4.
Dendritic Compartmentalization of Learning-Related Plasticity. Godenzini, L., Shai, A. S., & Palmer, L. M. (2022). ENeuro, 9(3).
Action-driven remapping of hippocampal neuronal populations in jumping rats. Green, L., Tingley, D., Rinzel, J., & Buzsáki, G. (2022). Proceedings of the National Academy of Sciences, 119(26), e2122141119.
Dopamine encodes real-time reward availability and transitions between reward availability states on different timescales. Kalmbach, A., Winiger, V., Jeong, N., Asok, A., Gallistel, C. R., Balsam, P. D., & Simpson, E. H. (2022). Nature Communications, 13, 3805.
Towards a more general understanding of the algorithmic utility of recurrent connections. Larsen, B. W., & Druckmann, S. (2022). PLOS Computational Biology, 18(6), e1010227.
Reward learning and statistical learning independently influence attentional priority of salient distractors in visual search. Le Pelley, M. E., Ung, R., Mine, C., Most, S. B., Watson, P., Pearson, D., & Theeuwes, J. (2022). Attention, Perception, & Psychophysics, 84(5), 1446–1459.
Stress-sensitive inference of task controllability. Ligneul, R., Mainen, Z. F., Ly, V., & Cools, R. (2022). Nature Human Behaviour, 6(6), 812–822.
Disentangling the critical signatures of neural activity. Mariani, B., Nicoletti, G., Bisio, M., Maschietto, M., Vassanelli, S., & Suweis, S. (2022). Scientific Reports, 12, 10770.
Active inference unifies intentional and conflict-resolution imperatives of motor control. Maselli, A., Lanillos, P., & Pezzulo, G. (2022). PLOS Computational Biology, 18(6), e1010095.
Pre- and postsynaptically expressed spike-timing-dependent plasticity contribute differentially to neuronal learning. Mizusaki, B. E. P., Li, S. S. Y., Costa, R. P., & Sjöström, P. J. (2022). PLOS Computational Biology, 18(6), e1009409.
Altered excitatory and inhibitory neuronal subpopulation parameters are distinctly associated with tau and amyloid in Alzheimer’s disease. Ranasinghe, K. G., Verma, P., Cai, C., Xie, X., Kudo, K., Gao, X., … Nagarajan, S. S. (2022). eLife, 11, e77850.
Sleep-dependent upscaled excitability, saturated neuroplasticity, and modulated cognition in the human brain. Salehinejad, M. A., Ghanavati, E., Reinders, J., Hengstler, J. G., Kuo, M.-F., & Nitsche, M. A. (2022). eLife, 11, e69308.
Gamma oscillations in primate primary visual cortex are severely attenuated by small stimulus discontinuities. Shirhatti, V., Ravishankar, P., & Ray, S. (2022). PLOS Biology, 20(6), e3001666.
Tracking the contribution of inductive bias to individualised internal models. Török, B., Nagy, D. G., Kiss, M., Janacsek, K., Németh, D., & Orbán, G. (2022). PLOS Computational Biology, 18(6), e1010182.
A supramodal and conceptual representation of subsecond time revealed with perceptual learning of temporal interval discrimination. Xiong, Y.-Z., Guan, S.-C., & Yu, C. (2022). Scientific Reports, 12, 10668.
#science#Neuroscience#computational neuroscience#Brain science#cognition#neurons#cognitive science#neurobiology#neural networks#neural computation#psychophysics#scientific publications
29 notes
·
View notes
Text
Of course, true rationalists only drink Everclear and refer to it as a "GABAergic nootropic."
7 notes
·
View notes
Text
Weird that I'm less neurotic after experiencing multiple traumatic head injuries during my stint last year as a daily user of various GABAergic drugs
5 notes
·
View notes
Text
tired and sick too much activity too many drug/med
#busy day busy day#too many meds take with al ohol#nadolol (beta blocked#Gabapentin (gabaergic like alcohol is)#seroquel (hellish neurolwptic v3ry strong)#didntt take tizanidine (muslce relaxant a 2 agonist#need take nightly seroquel eventually.#POTS go bad with all thie#felt good until come down#coming down feel bad just tired and sick#wanna take tizanidine calm down make sleep#but maybe make too much Cns depression#will just lay here and listen music#....be safe will be safe#julian rants#drunk posting#vent#drugs tw#alcohol tw
15 notes
·
View notes
Text
Abstract
Tramadol overdose is frequently associated with the onset of seizures, usually considered as serotonin syndrome manifestations. Recently, the serotoninergic mechanism of tramadol-attributed seizures has been questioned. This study’s aim was to identify the mechanisms involved in tramadol-induced seizures in overdose in rats. The investigations included (1) the effects of specific pretreatments on tramadol-induced seizure onset and brain monoamine concentrations, (2) the interaction between tramadol and γ-aminobutyric acid (GABA)A receptors in vivo in the brain using positron emission tomography (PET) imaging and 11C-flumazenil. Diazepam abolished tramadol-induced seizures, in contrast to naloxone, cyproheptadine and fexofenadine pretreatments. Despite seizure abolishment, diazepam significantly enhanced tramadol-induced increase in the brain serotonin (p < 0.01), histamine (p < 0.01), dopamine (p < 0.05) and norepinephrine (p < 0.05). No displacement of 11C-flumazenil brain kinetics was observed following tramadol administration in contrast to diazepam, suggesting that the observed interaction was not related to a competitive mechanism between tramadol and flumazenil at the benzodiazepine-binding site. Our findings do not support the involvement of serotoninergic, histaminergic, dopaminergic, norepinephrine or opioidergic pathways in tramadol-induced seizures in overdose, but they strongly suggest a tramadol-induced allosteric change of the benzodiazepine-binding site of GABAA receptors. Management of tramadol-poisoned patients should take into account that tramadol-induced seizures are mainly related to a GABAergic pathway.
Keywords: GABA, overdose, positron emission tomography, seizure, tramadol
20 notes
·
View notes
Text
Mysteries of Zopiclone
Mysteries of Zopiclone: A Comprehensive Guide**
In the realm of sleep aids, few names resonate as prominently as Zopiclone. Widely prescribed for its efficacy in treating insomnia, this medication has garnered attention for both its benefits and potential drawbacks. Let's delve into the depths of Zopiclone, exploring its mechanisms, applications, and essential considerations.
Telegram username: @itstheboogeymanbrad
****
Zopiclone belongs to a class of drugs known as nonbenzodiazepine hypnotics, which act similarly to benzodiazepines but with fewer associated risks. It exerts its effects by enhancing the activity of gamma-aminobutyric acid (GABA), a neurotransmitter that inhibits brain activity, thus inducing sedation and sleep.
** Action:**
Zopiclone operates by binding to specific sites on GABA receptors, intensifying GABAergic transmission. This process results in a calming effect on the central nervous system, promoting relaxation and facilitating the onset and maintenance of sleep. Its rapid onset of action makes it particularly effective for addressing short-term insomnia.
****
Zopiclone is primarily prescribed for the short-term management of insomnia, typically for periods not exceeding four weeks. It is recommended for individuals experiencing difficulty falling asleep, frequent awakenings during the night, or early morning awakenings, with the goal of restoring healthy sleep patterns.
****
While Zopiclone offers relief for insomnia, it's essential to exercise caution and adhere to prescribed guidelines. Here are some crucial points to keep in mind:
1. **** Zopiclone dosage should be tailored to individual needs, with lower doses recommended for elderly patients and those with hepatic impairment. It should be taken immediately before bedtime to minimize the risk of residual effects.
2. **** Common side effects of Zopiclone include drowsiness, dizziness, dry mouth, and altered taste perception. Less frequently, it may lead to gastrointestinal disturbances, headache, and memory impairment. Long-term use may increase the risk of dependency and tolerance.
3. **** Prolonged use of Zopiclone can lead to physical and psychological dependence, necessitating careful monitoring and gradual tapering when discontinuing treatment. Abrupt cessation may precipitate withdrawal symptoms, including rebound insomnia, anxiety, and agitation.
4. **** Zopiclone has the potential to interact with other medications, particularly those that depress the central nervous system, such as opioids, benzodiazepines, and alcohol. Concurrent use may potentiate sedative effects and increase the risk of respiratory depression.
5. **** Caution is warranted when prescribing Zopiclone to elderly individuals, as they may be more susceptible to adverse effects, including falls and cognitive impairment. Patients with a history of substance abuse or psychiatric disorders should be monitored closely for signs of misuse or exacerbation of symptoms.
***:**
Zopiclone stands as a valuable therapeutic option for individuals grappling with insomnia, offering a potent solution for restoring restful sleep. However, its use requires careful consideration of dosage, duration, and potential risks. By understanding its mechanisms, indications, and precautions, healthcare providers can harness the benefits of Zopiclone while mitigating adverse outcomes, ensuring a balanced approach to sleep management.
**** Zopiclone, insomnia, sleep aid, nonbenzodiazepine hypnotic, GABA, neurotransmitter, sedation, dosage, side effects, dependency, withdrawal, drug interactions, special populations.
#actually ptsd#insomia#adhd things#adhd brain#ambient#420life#420daily#420girl#420culture#420stoner#710life#710dabs#710community#710babes
1 note
·
View note
Text
Mitochondrial stress in GABAergic neurons non-cell autonomously regulates organismal health and aging
http://dlvr.it/T4cBDr
0 notes
Text
Understanding Nembutal capsules mechanism of action

Nembutal, also known as pentobarbital, is a medication primarily used for its sedative and hypnotic properties. Understanding its mechanism of action is crucial for both medical professionals and individuals seeking information about its effects and usage.
What are Nembutal Capsules?
Nembutal capsules are a pharmaceutical formulation containing pentobarbital, a barbiturate derivative. These capsules are commonly prescribed for their sedative, hypnotic, and anticonvulsant effects. They belong to the class of drugs known as central nervous system (CNS) depressants.
Mechanism of Action
Interaction with GABA Receptors
Nembutal acts primarily by enhancing the activity of gamma-aminobutyric acid (GABA), the major inhibitory neurotransmitter in the brain. It binds to specific sites on GABA-A receptors, which are ligand-gated chloride channels. This binding results in the opening of chloride channels, leading to hyperpolarization of neuronal membranes and inhibition of neuronal excitability.
Effects on Central Nervous System
By enhancing GABAergic transmission, Nembutal produces sedative, hypnotic, and anxiolytic effects. It induces a state of calmness, relaxation, and drowsiness, making it effective for treating conditions such as insomnia, anxiety, and agitation.
Pharmacokinetics
Nembutal is well-absorbed after oral administration, with peak plasma concentrations reached within 1 to 4 hours. It is widely distributed throughout the body, including the brain, where it exerts its pharmacological effects. The drug is primarily metabolized in the liver and undergoes renal excretion.
Indications for Use
Nembutal capsules are prescribed for various medical conditions, including:
Treatment of insomnia
Management of anxiety disorders
Sedation prior to surgical procedures
Control of seizures in certain neurological conditions
Dosage and Administration
The dosage of Nembutal capsules varies depending on the indication and individual patient factors. It is typically administered orally, either as a single dose or divided into multiple doses throughout the day.
Onset and Duration of Action
The onset of action of Nembutal is rapid, with sedative effects usually observed within 30 minutes to an hour after administration. The duration of action varies but is generally 4 to 6 hours for the hypnotic effects.
Side Effects and Adverse Reactions
Common Side Effects
Common side effects of Nembutal capsules include:
Drowsiness
Dizziness
Confusion
Respiratory depression
Nausea and vomiting
Serious Adverse Reactions
Serious adverse reactions may occur with high doses or prolonged use of Nembutal, including:
Respiratory depression leading to respiratory arrest
Cardiovascular collapse
Dependence and withdrawal symptoms upon discontinuation
Contraindications
Nembutal capsules are contraindicated in individuals with:
Hypersensitivity to barbiturates
Severe respiratory insufficiency
Acute intermittent porphyria
History of substance abuse or dependence
Drug Interactions
Nembutal may interact with other medications, including:
Alcohol
Benzodiazepines
Opioids
Antidepressants
Overdose and Management
Signs of Nembutal overdose include profound central nervous system depression, respiratory depression, and cardiovascular collapse. Management of overdose involves supportive care, including airway management, respiratory support, and monitoring of vital signs.
Regulatory Status
Nembutal is a controlled substance in many countries due to its potential for abuse and dependence. It is classified as a Schedule II controlled substance in the United States under the Controlled Substances Act.
Controversies Surrounding Nembutal
Nembutal has been the subject of controversy due to its association with euthanasia and assisted suicide. Some advocacy groups and individuals argue for its availability as a means of peaceful death, while others raise ethical and legal concerns regarding its use for this purpose.
Conclusion
Nembutal capsules exert their pharmacological effects primarily by enhancing GABAergic transmission in the central nervous system. Understanding their mechanism of action, pharmacokinetics, indications for use, and potential adverse reactions is essential for safe and effective clinical practice.
Frequently Asked Questions
Is Nembutal addictive?
Nembutal has a potential for dependence and addiction, especially with prolonged use or high doses.
Can Nembutal be used for euthanasia?
While Nembutal has been used for euthanasia in some cases, its legality and ethical implications vary by jurisdiction.
What should I do if I miss a dose of Nembutal?
If you miss a dose of Nembutal, take it as soon as you remember. However, if it is almost time for your next dose, skip the missed dose and continue with your regular dosing schedule.
Are there any lifestyle changes I should make while taking Nembutal?
It is important to avoid alcohol and other CNS depressants while taking Nembutal, as they can increase the risk of side effects and overdose.
How should Nembutal be stored?
Nembutal capsules should be stored at room temperature away from moisture and heat. Keep them out of reach of children and pets.
0 notes
Text
Interesting Papers for Week 18, 2023
Internally generated time in the rodent hippocampus is logarithmically compressed. Cao, R., Bladon, J. H., Charczynski, S. J., Hasselmo, M. E., & Howard, M. W. (2022).eELife, 11, e75353.
Reasoning about mental states under uncertainty. Cho, I., Kamkar, N., & Hosseini-Kamkar, N. (2022). PLOS ONE, 17(11), e0277356.
Flexible integration of continuous sensory evidence in perceptual estimation tasks. Esnaola-Acebes, J. M., Roxin, A., & Wimmer, K. (2022). Proceedings of the National Academy of Sciences, 119(45), e2214441119.
Systematic reduction of the dimensionality of natural scenes allows accurate predictions of retinal ganglion cell spike outputs. Freedland, J., & Rieke, F. (2022). Proceedings of the National Academy of Sciences, 119(46), e2121744119.
Nucleus accumbens dopamine tracks aversive stimulus duration and prediction but not value or prediction error. Goedhoop, J. N., van den Boom, B. J., Robke, R., Veen, F., Fellinger, L., van Elzelingen, W., … Willuhn, I. (2022).eELife, 11, e82711.
Visual experience has opposing influences on the quality of stimulus representation in adult primary visual cortex. Jeon, B. B., Fuchs, T., Chase, S. M., & Kuhlman, S. J. (2022). eLife, 11, e80361.
The role of conjunctive representations in prioritizing and selecting planned actions. Kikumoto, A., Mayr, U., & Badre, D. (2022). eLife, 11, e80153.
Reward expectation extinction restructures and degrades CA1 spatial maps through loss of a dopaminergic reward proximity signal. Krishnan, S., Heer, C., Cherian, C., & Sheffield, M. E. J. (2022). Nature Communications, 13(1), 6662.
Adult newborn granule cells confer emotional state–dependent adaptability in memory retrieval. Lei, B., Kang, B., Lin, W., Chen, H., Hao, Y., Ma, J., … Zhong, Y. (2022). Science Advances, 8(45).
Long-range GABAergic projections contribute to cortical feedback control of sensory processing. Mazo, C., Nissant, A., Saha, S., Peroni, E., Lledo, P.-M., & Lepousez, G. (2022). Nature Communications, 13, 6879.
Neural dynamics of causal inference in the macaque frontoparietal circuit. Qi, G., Fang, W., Li, S., Li, J., & Wang, L. (2022). eLife, 11, e76145.
Recalibrating vision-for-action requires years after sight restoration from congenital cataracts. Senna, I., Piller, S., Ben-Zion, I., & Ernst, M. O. (2022). eLife, 11, e78734.
Sampling motion trajectories during hippocampal theta sequences. Ujfalussy, B. B., & Orbán, G. (2022). eLife, 11, e74058.
An opioid-gated thalamoaccumbal circuit for the suppression of reward seeking in mice. Vollmer, K. M., Green, L. M., Grant, R. I., Winston, K. T., Doncheck, E. M., Bowen, C. W., … Otis, J. M. (2022). Nature Communications, 13, 6865.
#science#neuroscience#computational neuroscience#Brain science#research#cognition#cognitive science#neurons#neurobiology#neural networks#neural computation#psychophysics#scientific publications
8 notes
·
View notes
Last Seen Blogs

naughty-dog
Naughty Dog

doublemily
Two M's? In this economy?

toxiclips-blog1
—— (( ┇☓ Don't you know that you're toxic? ))

awesome-bpbds-blog
발품부동산TV

blackhearting-blog1
that girl is a goddamned problem;