#gender affirming surgery
Text
I’m 3 years post phalloplasty and I realized I’ve never really made a post about how things are going. Phalloplasty is a hard surgery to talk about because, bottom line, it’s not part of common conversation to talk about yo dick. That being said I think it’s really important for me to talk about this procedure to help break stigma and misinformation— both inside and outside of trans and non-binary communities.
I had ALT phalloplasty, glansplasty, scrotoplasty, no urethral lengthening (UL) with vaginectomy. This means that tissue from my thigh was used to create my penis, my urethra was not extended or moved (so I don’t stand to pee) and my vagina was closed. I feel like this detail is important because this is one of many variations for this procedure and what I opted for/out of were decisions made according to trade-offs between personal benefit and risk.
I opted out of UL because I do not tolerate catheters well and, due to my very active lifestyle, was not willing to risk longer term catheterization or bladder spasms which would impede my quality of life. This risk, for me, outweighed the benefit of standing to pee.
I opted for ALT knowing that I would likely need debulking (which I didn’t end up needing but opted for anyway out of preference). Debulking is a procedure to make the penis less girthy as ALT phalloplasty is more girthy because of the nature of tissue on the thigh. I chose ALT because, first and foremost, I did not want scarring on my forearm. My ALT scar is covered by clothing most of the time which I appreciate. I also chose ALT because I have skinny forearms, which wasn’t ideal for forearm phalloplasty (RFF).
Vaginectomy, for me, was a no brainer. I have never used or connected with that part of my body so I wanted it gone.
Glansplasty is a procedure to make the glans (head) of the penis and was a short procedure done after my initial stage of surgery. I may get it redone but I’m still undecided on that. Scrotoplasty creates a scrotum, I was ambivalent about this procedure but have grown to more appreciate it over time.
I am considering further surgeries: erectile implant (which creates the ability for the penis to “get hard”) and testicular implants (fills to scrotum with testicle implants). But I’m undecided and want a break from surgery while I finish my degree and focus on work. I’m also considering phalloplasty tattooing to help enhance the contour and coloring to make it appear more like a cis penis.
Whew! Lots of info, right? These are big procedures completed over multiple stages and are very unlike chest surgery, hysterectomy and other surgeries I had completed prior. When I was first considering this surgery I didn’t know there was flexibility in terms of tissue donor site and UL. I waited to have this surgery and am so happy I did because the information I gained from research and consulting with professionals and folks with lived experience was so valuable.
Was surgery hard? Yes. This surgery was the hardest thing I’ve ever been through. I’ve never been so uncomfortable for the first 2 weeks after recovering. I had to re-learn how to walk. I couldn’t sleep. Peeing hurt… but would I do it again? Yes. It was worth it for me but I can’t underscore enough that that doesn’t mean I didn’t have moments where I felt regret while recovering because post op depression is a thing and I was in pain while adjusting to a new body part that was also a healing surgical site… LOTS going on there!
3 years on I feel really at home in my body. Just having a penis is such a comfort to me in ways I didn’t anticipate. I’ve had a feeling my entire life that I was missing a body part and this was it. The quiet gender euphoria of just sitting and feeling my body and for once feeling complete in that is something that’s hard to articulate.
I’m thankfully back to full mobility and got back to full mobility about 3 months post op. I was grateful for this since a long term recovery wasn’t what I wanted. There are still weird twitches, pains and feelings, especially around my donor site (thigh) from time to time but nothing that inhibits me. Just interesting when it happens (usually when weather gets colder?).
What is one thing I would want to go back and tell myself before surgery? Well:
Your penis will feel HEAVY. Like it will fall off. It won’t fall off and your body will adjust to the weight in an area you didn’t have it before. Until then it will feel like you need to hold it at all times.
Hopefully this helps someone as an overview of what an experience with this procedure may look like. Again, my goal is to put information out there and have frank conversations— because it’s these same things that greatly benefitted me in my surgery journey.
Finally— my inbox is open for anyone that has questions. I am in a privileged position to feel safe talking about these things and I feel comfortable doing so. Not everyone does, so please don’t assume that this invitation applies to other folks who have accessed surgery unless they say so.
Thank you for reading :)
#ftm#phalloplasty#surgery#trans#transition#transgender#trans man#trans guy#gender affirming surgery#phallo
4K notes
·
View notes
Text
Context.
Fascist Right Wingers want trauma for all.
1K notes
·
View notes
Text

i keep missing work due to my brain injury + brain cyst + general chronic illness, and i only have 5 months to generate over $10,000 or else i’m going to have to go even further into medical debt!
every single dollar makes a real, genuine difference in my life!
#diary#gender transition#gender affirmation#gender affirming surgery#top surgery#lgbt#lgbtq#lgbtqi#lgbtqia#lgbt+#lgbtq+#lgbtqi+#lgbtqia+#queer#pride#trans pride#queer pride#gender affirmation surgery#ftm#trans ftm#non-binary#nonbinary#enby#ftnb#female to male#female to non-binary#transmasc#transmasculine#trans androgynous#transgender
897 notes
·
View notes
Text

#lgbtqia#lgbtq community#lgbtq#lesbian#sapphic#nonbinary lesbian#nonbinary#queer#lgbt pride#gay girls#harry potter#harry james potter#hp fanart#hp fandom#harry potter fanart#hp fanfic#gender affirming care#gender affirmation#gender affirming surgery#gender affirming healthcare#gender affirming treatment#jk rowling#fuck jkr#jk
604 notes
·
View notes
Text
Not asking about medical complications since that's sort of a different question; this poll is asking about the aesthetic and/or functional results. Obviously a person can have multiple different procedures done with different levels of satisfaction; select any one that applies.
Gender-affirming surgery includes but is not limited to procedures like breast removal, reduction, or augmentation; facial feminization or masculinization; the construction of different genitals; liposuction/body sculpting, etc.
–
We ask your questions so you don’t have to! Submit your questions to have them posted anonymously as polls.
#polls#incognito polls#anonymous#tumblr polls#tumblr users#questions#polls about health#submitted nov 17#polls about the body#polls about lgbtq stuff#lgbtq#trans#transgender#gender affirming care#gender affirming healthcare#gender affirming surgery#trans healthcare#surgery#medical
305 notes
·
View notes
Text
Hey so with the barbie movie coming out mod is once again seeing comments like “I’m nonbinary and wish I could just have flat genitalia like a doll, it would take away my dysphoria”. Mod got a dysphoric culture ask about it like 2 years ago actually and now there are more so:
This is possible.
If your transition goal is to have a complete removal of all your internal and external genitalia, there is a real surgery that people get to do that. It’s called genital nullification.
It’s also called nullectomy or nullo.
It’s not a very new or super complicated surgery. Everything is taken out/taken off and you’re left with just a hole for your urethra (where you urinate out of). The urethra may be moved as part of surgery. If you research the procedure you’ll also probably hear them talk about urethral shortening, because nullification is mostly done on cis men/transfems/nonbinary patients who require a penectomy as part of the surgery.
Now don’t get this for an aesthetic or because you like how dolls look. It takes 6-8 weeks of recovery and is as serious a decision as any other bottom surgery. More info is here and here. This website has some info and pictures (graphic warning) of nullification along with phallus-preserving vaginoplasty, another nonbinary surgery.
Hopefully this helps someone!
#not dysphoric culture#resources#mod talks#nonbinary#gender affirming surgery#trans resources#nonbinary resources#bottom surgery#bottom dysphoria#genitalia tw#tw genitalia mention#transfem#amab nonbinary#lgbtq+
665 notes
·
View notes
Text
If you are a cis ally or a non-medically transitioning trans person or nonbinary person, part of your trans political engagement SHOULD BE KNOWING THE INS AND OUTS OF GENDER AFFIRMING CARE even if you have zero intention of getting any for yourself.
You should know the basics of hrt and informed consent and the basics of surgeries and procedures that trans people want access to. You should know about the laws and bills being passed that make it nearly impossible for people to access these things. And be able to recognize false information and refute it!
And most importantly you should be willing to LISTEN to transitioning people when they describe their experiences with accessing care as well as when they describe the experience and injustices that come with living in a medically transitioned body.
#trans#transsexual#transgender#queer#transition#trans rights#queer liberation#trans pride#hrt#gender affirming care#gender affirming surgery#genderqueer#nonbinary#gender
154 notes
·
View notes
Text

Day 5!, when you can finally fill out your fav blouse without stuffing a bra! I'm so happy right now. They are the perfect size for me!
For those of you who have been asking. I got 470cc implants. No big but not small. I wanted a natural size proportionate to my body. I gave my surgeon a ton of leeway on that. He went 55cc more than I thought I wanted. I feel he picked a perfect size for me! I couldn't be happier 🥰🥰🥰
#trans surgery#transgender surgery#gender affirming surgery#transgender#trans#transisbeautiful#trans pride#transgirl#mtf hrt#mtf#girlslikeus#maletofemale#transformation#mtf hormones#trans mtf#actually mtf#mtf positivity#transwomen#transition#actually trans#mtf trans#trans feminine#trans girl#trans is beautiful#this is what trans looks like#trans is sexy#trans positivity#tgirls are better#tgirlsdoitbetter🌈#cute tgirl
623 notes
·
View notes
Text
"everyone goes through puberty, its a natural process that needs to occur."
if you say this shit when it comes to trans kids getting the gender affirming care that they need, then you do not understand how traumatic puberty can be for some transgender people. like why do you want trans kids to suffer? you all say GAC has "permanent changes" but so does puberty. like now i'm getting a surgery which yall deem "mutilation," BECAUSE i was forced to go through a female puberty. it also wasn't just the stereotypical "this is puberty and im a bit uncomfortable because my body is changing." no, i literally wanted to die because i was going through a female puberty. growing breasts made me want to remove myself from this planet.
#ftm#trans#transgender#queer#gay#transsexual#trans man#lgbt#trans male#ftm mlm#surgery#top surgery#gender affirming surgery#gender affirming care is life saving#gender affirming care
240 notes
·
View notes
Text






By: SEGM
Published: Aug 13, 2023
Near-zero regret” findings among adults suffer from a critical risk of bias and have low applicability to youth
Recent research published in JAMA Surgery evaluated satisfaction and regret among individuals who had undergone chest masculinizing mastectomy at the University of Michigan hospital. The average patient age at the time of mastectomy was 27 years; no patients who were under age 18 were allowed to participate in the study.
The participants reported high levels of satisfaction and low levels of regret at an average of 3.6 years following mastectomy. The study authors lauded the “overwhelmingly low levels of regret following gender-affirming surgery,” and framed their findings as in conflict with the “increasing legislative interest in regulating gender-affirming surgery,” referring to current legislative attempts to restrict or ban “gender-affirming” procedures for minors. Another group of authors provided an invited commentary on the paper, reinforcing the view held by the study authors, and asserting the presence of a “double standard:” “gender-affirming” mastectomies have come under undue scrutiny by states’ legislators, while other surgical procedures with higher regret rates do not appear to concern legislative bodies.
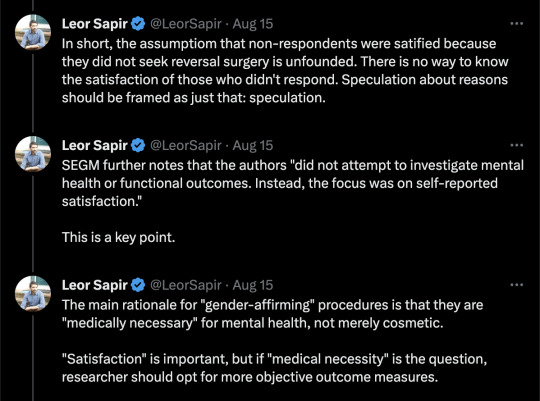
The study suffers from serious methodological limitations, which render the findings of high levels of long-term satisfaction with mastectomy among adults at a "critical risk of bias"—the lowest rating according to the Risk of Bias (ROBINS-I) analysis. ROBINS-I is used to assess non-randomized studies for methodological bias. The "critical risk of bias" rating signals that the results reported by the study may substantially deviate from the truth. The results also suffer from low applicability to the central issue the study and the invited commentary sought to address, which was whether legislative attempts to regulate “gender-affirming” surgeries are warranted in minors. Unfortunately, these highly questionable findings are misrepresented as certain and highly positive by both the study authors and the invited commentators, several of whom have significant conflicts of interest.
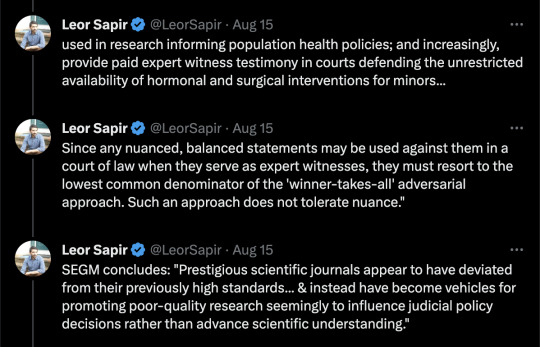
Below, we provide a detailed explanation of the key methodological issues in the study which render its claims untrustworthy and not applicable to the patient population at the center of the debate: youth undergoing gender reassignment. We also comment on the alarming trend: several prestigious scientific journals appear to have deviated from their previously high standards for scholarly work and instead have become vehicles for promoting poor-quality research, seemingly to influence judicial policy decisions rather than advance scientific understanding. We conclude with recommendations about how journal editors can restore the integrity of scientific debate and raise the bar on the quality of published studies in the field of gender medicine.
[ For in-depth analysis, see: https://segm.org/long-term-regret-satisfaction-mastectomy-critical-appraisal ]
SEGM Take-Aways
Although this study reports extremely high rates of satisfaction and low regret, the timeframe in which these outcomes were assessed is insufficient—just 3.6 years post-mastectomy on average. The sample is also highly skewed: 50% of the participants had mastectomies in the last 3.6 of the 30 years. This skewing of the length of time since surgery is expected, given the sharp rise in the number of people (especially adolescents and young adults) identifying as transgender and undergoing chest masculinization mastectomy. It is also a short time in which to assess regret, particularly since one quarter of study participants were younger than age 23 at time of surgery and the median age of first birth in the US is 30 years.
The conclusion of high satisfaction/low regret suffers from a critical risk of bias due to the high non-participation rate, important differences between participants and non-participants, and lack of control group. Problematically, the authors misuse the (critically-biased) results from adults to argue against regulations for irreversible body alternations for minors and do so with a decidedly politicized spin.
The only intellectually honest commentary is that we do not have good knowledge of the likely rates of detransition and regret following chest masculinization mastectomy, nor do we know how many people experience regret but remain transitioned. There is an urgent need for quality research in this area. Previously, detransition and regret rates were considered to be low: they may have indeed been low due to the much more rigorous screenings, or the results may have been biased by the notoriously high dropout rates that plague “regret” research. Regardless, there is now growing evidence of much higher rates of medical detransition.
A recent study from a comprehensive U.S. dataset with no loss to follow-up revealed a 36% medical detransition rate among females within just 4 years of starting hormonal transition. At least two recent studies suggest that average time to regret among recently-transitioned females is about 3-5 years, but there is a wide range. Much less is known about detransition among those who undergo surgery. A growing number of detransitioners now express regret associated with the loss of breastfeeding ability, with one case study detailing breastfeeding grief experienced some 15 years post-mastectomy.
The study and invited commentary exemplify three problematic trends that plague studies emerging from the gender clinics: problematic conflicts of interest of the authors; leveraging scientific journals to disguise politically-motivated pieces as quality research; and a conflicted stance by the gender medicine establishment on surgery for minors. We expand on each briefly below.
Conflicts of interest of study authors and commentators
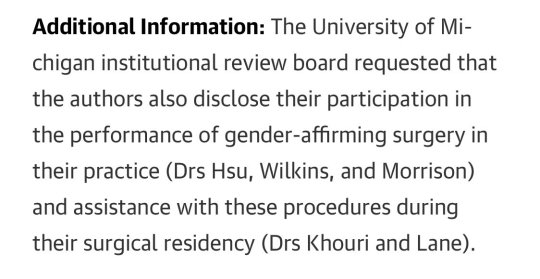
The significant conflicts of interest of the gender clinicians who study and report on the outcomes of “gender-affirming” interventions cannot be overlooked. These clinicians are conflicted financially, since their practices specialize in “gender-affirming” interventions, as well as intellectually. While conflicts of interest among experts are common, such experts should still attempt to be balanced in their discussions and should acknowledge and reflect on their conflicts of interest.
The interpretations of the data in the study is neither rigorous nor balanced, and both the study and the invited commentary have a decidedly political spin. Further, the invited politicized commentary does not disclose that at least one of the authors is a key expert witness opposing states’ efforts to regulate “gender-affirming” surgeries for minors. This role alone precludes the ability to provide a balanced commentary.
There is a fundamental problem with research emerging from gender clinic settings. The same clinicians provide gender-transitioning treatments to individual patients in their practice; serve as primary investigators and custodians of data used in research informing population health policies; and increasingly, provide paid expert witness testimony in courts defending the unrestricted availability of hormonal and surgical interventions for minors.
As a result, such clinicians cannot express nuanced perspectives. Since any balanced statements may be used against them in a court of law when they serve as expert witnesses, they must resort to the lowest common denominator of the "winner-takes-all" adversarial approach. Such an approach does not tolerate nuance. Unfortunately, this approach contributes to the erosion of the quality of the published work in the arena of gender medicine and accelerates loss of trust about the integrity of the scientific process.
Misuse of scientific publications to promote politically-motivated articles disguised as scientific research
That prestigious medical journals now serve as platforms for promoting misleading, politically motivated research that aims to apply a veneer of misplaced confidence in highly invasive, irreversible treatment should worry everyone committed to evidence-based medicine and the integrity of science. Moreover, it impairs our ability to accurately assess and improve the long-term health outcomes of the rapidly growing numbers of gender-diverse and gender-distressed youths.
This is not the first time that a JAMA has been used as a platform for positioning advocacy for “gender-affirming” care as scientific research. In 2022, JAMA Pediatrics published a study that assessed bodily happiness in a group of subjects aged 14-24 three months after chest masculinization mastectomy. Despite the very short follow up and dropout rate of 13%, the authors argued that their findings supported the premise that there was no evidence to suggest that young age should delay surgery. They also asserted that their research would help dispel the misconception that such surgeries are experimental. The editorial commissioned to bolster the authors claims was descriptively titled, “Top surgery in adolescents and young adults-effective and medically necessary.”
Another troubling trend is the misuse of statistical tools to reframe research findings that contradict the author's own position. For example, a well-known study that claimed that access to puberty blockers reduce the risk of suicide disregarded the fact that individuals reporting use of puberty blockers use had twice as many recent serious suicide attempts as their peers who did not use puberty blockers. Like the finding cited above, the doubling of suicide attempts was not statistically significant due to a small underpowered sample—but the magnitude of the effect was striking and should have tempered the authors’ enthusiastic conclusion that puberty blockers prevent suicides. Another recent gender clinic study, widely and positively covered by major media outlets, claimed that puberty blockers and cross-sex hormones led to plummeting rate of depression—even though the rate of depression among youth taking those medications remained demonstrably unchanged. More information about problems with research originating from gender clinics is detailed in this recent analysis.
Gender medicine’s stance on pediatric surgery
More generally, the gender medicine establishment is in a curious state of internal conflict about its stance on “gender-affirming” surgeries for minors. On the one hand, it has become common for advocates of “gender-affirmation” of minors to insist that surgeries for minors are not performed and anyone who suggests otherwise is spreading “scientific misinformation” and “science denialism.” On the other hand, gender clinicians publish mastectomy outcomes for minors in major medical journals, and laud surgeries for minors as “effective and medically necessary.” It is not uncommon for these opposing claims to be made by the same group of researchers and clinicians, as they test various arguments, searching for the "angle" that is most likely to convince judges and juries--and public at large--that scrutiny of the practice of pediatric transitions, which is increasingly occurring in European countries, is not warranted in the United States.
Notably, none of the European countries that are enacting severe restrictions on the use of puberty blockers or cross-sex hormones for minors have ever allowed surgeries for youth under 18. That the U.S. gender affirmation professionals continue to fight regulation of these problematic procedures speaks volumes about how far the U.S. healthcare has drifted when it comes to "gender affirmation" of minors.
Final thoughts
While it is challenging to determine how best to reduce the temperature of the highly politicized nature of the debate in gender medicine, the editors of scientific journals can begin to restore balance by recognizing how far the field has drifted from the standards of quality scientific research, and begin to expand their circle of peer-reviewers to those with diverse views. Inviting those concerned with the state of gender medicine (and not just the practices’ advocates) into the peer-review and commentary process is the first essential step to improve the quality of research published in the field of gender medicine.
--


--

==
The activists are predictably - and consistent with the superficiality of their own ideology - upset that anyone should look below the surface. It seems to be more troubling that anyone would notice the shoddiness of the research, than that the research is shoddy.
If this is supposed to be "healthcare," you would think that they would want the best healthcare, and be more alarmed at the misrepresentations of the study, than by people finding those misrepresentations.
Could it be that this is ideological rather than medical? 🤔
The conflicts of interest and funding sources alone are remarkable.
#Leor Sapir#SEGM#Society for Evidence Based Gender Medicine#double mastectomy#top surgery#gender affirming mastectomy#ideological corruption#ideological capture#medical malpractice#conflict of interest#sarcastic font#medical scandal#medical corruption#gender ideology#genderwang#queer theory#gender affirming care#gender affirming surgery#gender affirming healthcare#medical mutilation#sex trait modification#religion is a mental illness
276 notes
·
View notes
Text

"A trio of health care bills enshrining access in Colorado to abortion and gender-affirming procedures and medications became law Friday [April 14th] as the Democrat-led state tries to make itself a safe haven for its neighbors, whose Republican leaders are restricting care.
The main goal of the legislation signed by Democratic Gov. Jared Polis is to ensure people in surrounding states and beyond can go to Colorado to have an abortion, begin puberty blockers or receive gender-affirming surgery without fear of prosecution. Bordering states of Wyoming and Oklahoma have passed abortion bans, and Utah has severely restricted transgender care for minors...
The governor’s office was packed with lawmakers, advocates and health care providers, many of them women, for a ceremony with a celebratory feel that resembled a rally at times with loud applause and call-and-response chants.
“We see you and in Colorado, we’ve got your back,” Democratic state Sen. Julie Gonzales said during the ceremony.
With the new laws, Colorado joins Illinois as a progressive peninsula offering reproductive rights to residents of conservative states on three sides. Illinois abortion clinics now serve people living in a 1,800-mile (2,900-kilometer) stretch of 11 Southern states that have largely banned abortion...
Colorado’s southern neighbor, New Mexico, is also controlled by Democrats and signed a similar abortion protection bill earlier this year. It legally shields those who seek abortions or gender-affirming care, and those who provide the treatments, from interstate investigations...
Polis added the first layer of abortion protection a year ago, signing an executive order that bars state agencies from cooperating with out-of-state investigations regarding reproductive healthcare. One of the bills he signed Friday codifies that order into law. Like the New Mexico law, it blocks court summons, subpoenas and search warrants from states that decide to prosecute someone for having an abortion.
Colorado’s abortion law extends the protections to transgender patients dodging restrictions in their own states. Gender-affirming health care has been available for decades, but some states have recently barred minors from accessing it, even with parental consent. Hospitals in some of those states say gender-affirming surgeries are rarely recommended for minors anyway. Puberty blockers are more common.
Also on Friday, Polis signed a measure that outlaws “deceptive practices” by anti-abortion centers, which are known to market themselves as abortion clinics but don’t actually offer the procedure. Instead, they attempt to convince patients to not terminate their pregnancies. The bill also prohibits sites from offering what’s called an abortion pill reversal — and unproven practice to reverse a medical abortion...
A third bill signed Friday requires large employers to offer coverage for the total cost of an abortion, with an exception for those who object on religious grounds. It exempts public employees because Colorado’s constitution forbids the use of public funds for abortions."
-via AP News, 4/14/23
#colorado#new mexico#abortion#abortion access#pro choice#gender affirming care#gender affirming surgery#puberty blockers#illinois#united states#us politics#reproductive rights#safe haven#jared polis#democrats#good news#hope
594 notes
·
View notes
Text
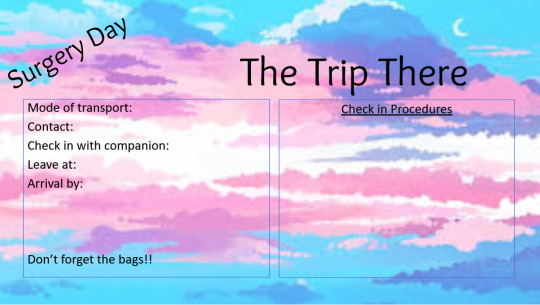
Top Surgery Planner!
Hey all, this is a link to the editable top surgery (removal) planning binder I created for my top surgery this past summer. It features 13 pages of content such as the ones shown below.
All medical content was reviewed by my surgeon for my surgery. It can and should be verified with your surgeon and edited as appropriate for your own.


I would appreciate this being shared as I think it’s a helpful resource for planning and preparing
594 notes
·
View notes
Text

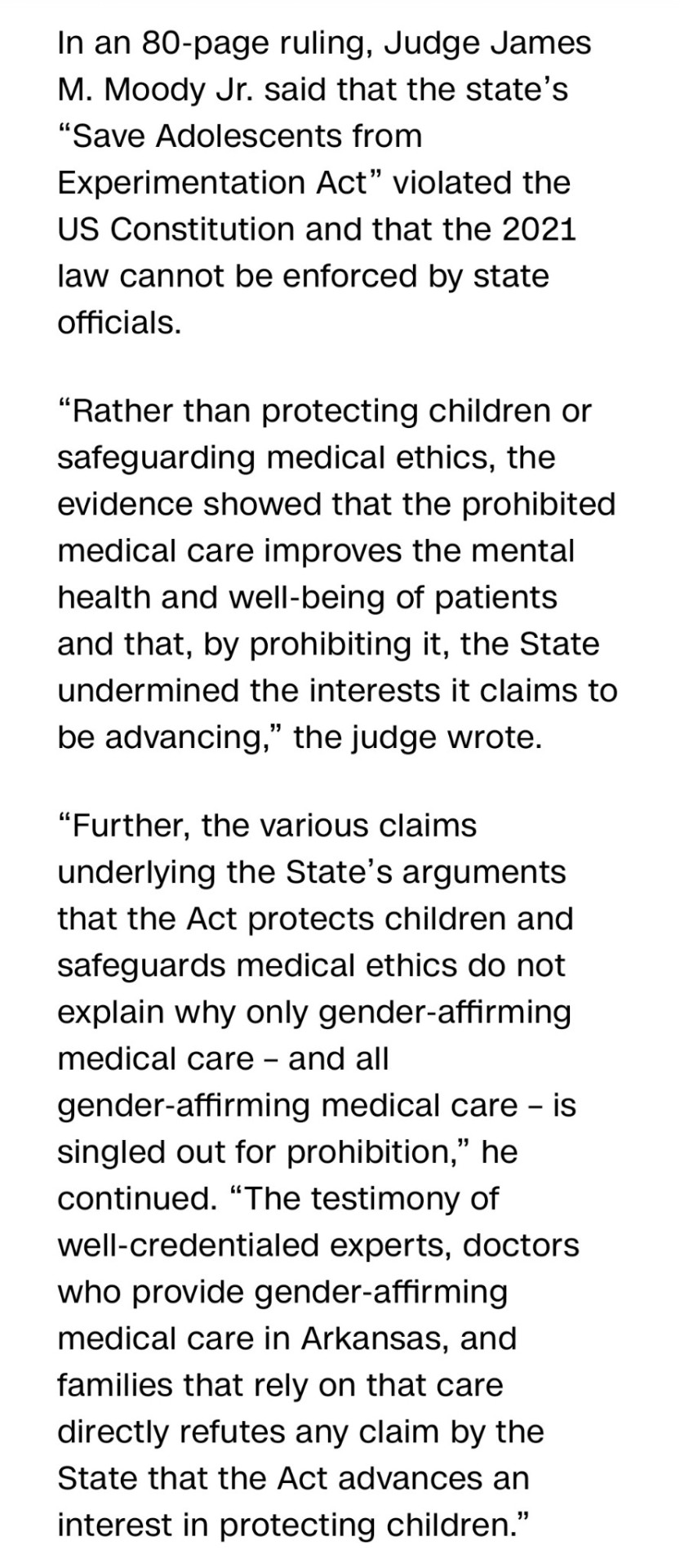
Federal judge rules Republicans are fascist assholes. The goals of conservative politics are increased trauma and suicide for children.
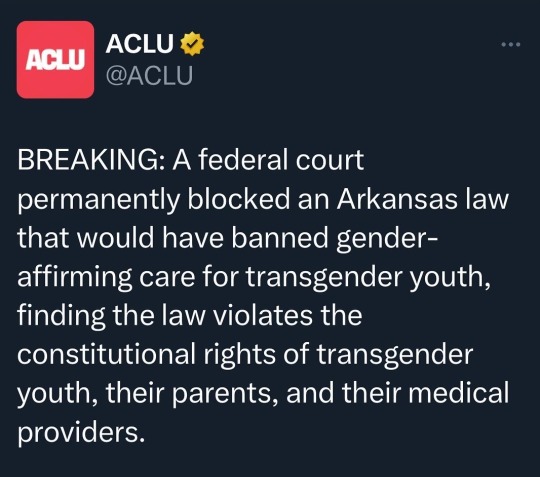
Categorical bans on gender affirming care are unconstitutional.
574 notes
·
View notes
Text
Those who perform "gender-affirming surgery" on MINORS is no better than a paedophile or s groomer.
I know that it is sometimes used to treat intersex people (which should certainly remain an important exception to this rule) however that's rare. Most of them are not done for that reason.
These scumbags should be thrown in prison for the rest of their lives.
#lgbtqiia+#lgbtq#lgbtq community#lgbtqia#lgbt pride#lgb drop the t#lgb alliance#trans men#transition#transsexual#transgender#trans man#transfem#gender affirming surgery#gender euphoria#conservative#conservatism#conservativism#conservation#transgirl
65 notes
·
View notes
Text
so this is just something i just now realized by looking through my health records - apparently, as part of the whole process of my hysterectomy, i was diagnosed with "dual role transvestism"??? even though that's clearly untrue when you look up the term? like i have been on T for over 6 years and i pass completely as cis and literally the hysto itself was a gender affirming surgery. my surgeon told me, even, that the reason on file for the surgery would be gender dysphoria. why on earth would i be diagnosed with basically "part time crossdresser" wergfbdwe
my best guess is that someone just straight up misclicked or something bc it makes no sense lol but has anyone else ever had this happen to them??
58 notes
·
View notes
Text
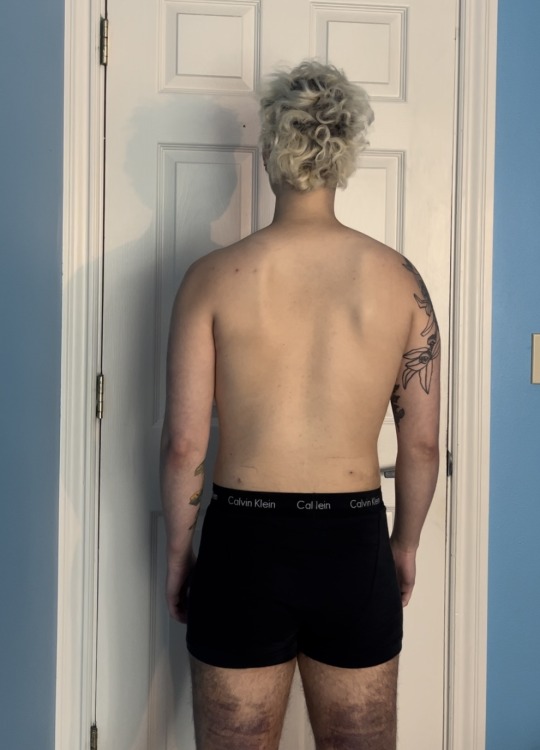
2 weeks post-op body masculinization surgery.





#trans man#ftm#trans guy#transgender#transmasculine#gender affirming care#gender affirming surgery#gender euphoria#trans joy#nonbinary
297 notes
·
View notes
Last Seen Blogs

janesamsposts
Sem título

northernyogurt
finn macauley

yourkaitouniverse
アニメ・ゲームを100%楽しむ方法

mybreastfeeding02
Untitled

lady-hinatsuru-academy-official
Hinatsuru