#inpatient medicine
Text
PICU Thoughts
My brain is not wired for this.
Inpatient medicine?
A totally different world.
I'm trying, I really am. But things slip through the cracks. I almost put a patient in benzo withdrawal because my default midazolam order is set to "one time ED" and I signed the order without a second thought.
Luckily my attending noticed that the q6 midazolam order was missing, and caught the mistake in time. But seriously, it's scary.
2 notes
·
View notes
Text
in an even worse way than i thought :3
#:)#my kidneys and maybe other organs are Fucked#gonna be in inpatient for a number of days pumped with iv fluids and high strength medicines#hope they fix me from this so i can stop my organs from dying and go back to rotating things in my mind#in mortal peril and scared out of my mind but i stay silly#now more than ever it is imperative i stay silly
26 notes
·
View notes
Text
"I don't need mnemonics; I have residents for that." - ED attending
#anyhow flecainide is class 1C because i can have fries or something like that i vaguely recalled from first aid#medblr#residency#medicine#emergency medicine#this is what i get when i visit the ED on inpatient months#pgy4
92 notes
·
View notes
Text
i have clinical rotations!!!!
2 notes
·
View notes
Text

took my meds again! surely this will be the time i stick with it and can finally be stably medicated and will actually experience long term benefits of medication for mental illness
#surely this won’t be like every single other time of the past fucking. 6 years or whatever. surely not#surely i have learned my lesson. right. right#meds are one of the things that seem like could actually be substantially beneficial if i ever had to do inpatient but i also think the#nuclear meltdown i would have if i was forced to take medicine would be like. cause lasting damage#soooooo wish i could be normal about taking pills but alas!#orating!
0 notes
Text
FNU
I’d ask my intern if there was anything she wanted me to check during my pre-round visit. My intern usually shrugged; what else could we do besides wait?
FNU used to work for Motorola as an electrical engineer.
Every morning in my pre-rounds, FNU and I would go through the same routine:
I would say good morning.
If she was asleep, she would not respond.
If she was awake, she would writhe and intermittently scream.
I’d listen to her lungs between her screams. I’d check for edema in the pauses between her writhes. We needed to make sure her fluid maintenance was not fluid overload. I once heard a crackle.
FNU had been encephalopathic for ten straight days since admission to the wards.
FNU was forced into early retirement after a company merger.
She decided to become a nurse and volunteer firefighter.
FNU drove from North Carolina to Oklahoma for a tribal celebration and to visit family. She did not feel well at the start of her drive. She visited an emergency room in North Carolina and was treated for a UTI. She visited two more emergency department for the same UTI before becoming confused in ours.
She began volunteering with the American Red Cross.
She wanted to help where help was needed most.
We could not do a lumbar puncture because of agitation. She was sedated, and her first set of CSF studies ruled out anything we could treat. We consulted neuro. We consulted ID. We threw the book at her and waited for any change.
Her identity as a Native American woman was important to her.
She spent time visiting family along the Arizona-Mexico border.
The Mexicans would call her “Indio.”
We started to withdraw irrelevant antibiotics as new CSF studies returned benign. ID wanted a second LP – but for what? How would it change treatment? If LaCrosse was positive, how would it change her current treatment?
FNU had been encephalopathic for twelve straight days since admission to the wards.
She turned to her nurse and asked for a glass of water on day 13.
On day 15, I squatted down next to her bed.
She told me she worked for Motorola as an electrical engineer.
Until a company merger forced her into early retirement.
She wanted to do more.
She wanted to help people.
She started working as a nurse and as a volunteer firefighter.
She started volunteering for the American Red Cross.
She started travelling to natural disaster sites to help with relief.
She wanted to help people where people needed help.
We talked about engineering – and my classmates that majored in engineering.
She asked me why I wanted to go into medicine.
I told her that medicine was a combination of science and altruism.
She liked that answer.
She told me that I looked “a little Native.”
I told her that I’m Mexican-American.
She told me about her visits to Arizona to see family.
She told me that she would cross the border to shop in Mexico.
She told me that the local Mexicans would call her “Indio”.
She told me about the tribal celebration in Oklahoma.
She started to talk about her home in North Carolina.
On top of a hill – a small mountain.
She didn’t notice any bug bites before she left for Oklahoma.
She tried to visit a friend with COVID, but her friend didn’t let her into the house.
She started feeling unwell a few days before she was set to leave, but she couldn’t cancel.
She needed to bring a ceremonial rifle.
Her identity as a Native American woman was important to her.
She visited an Indian Health Services emergency department.
She was given antibiotics, and she started her drive.
She turned to me on day 15 and told me she wanted to go home.
She was discharged on day 18.
#medicine#internal medicine#inpatient#med school#medical school#med student#medical student#infectious diseases#MS3
1 note
·
View note
Text
Parenting 101: Lakeshore General Hospital Foundation's 5km family walkathon
Parenting 101: Lakeshore General Hospital Foundation’s 5km family walkathon
On Saturday, June 4, Lakeshore General Hospital Foundation is launching a brand-new event – its first Family 5K Walkathon around Centennial Lake in Dollard-des-Ormeaux.
Not only will participants enjoy a nice walk around the lake, but there will also be food, music, and other activities for the kids. People of all ages (and even their dogs!) are welcome to participate in this event. Funds…
View On WordPress
#clinic#demand#inpatient#lakeshore general hospital foundation#Medicine#Mental Health#Unit#walkathon
0 notes
Text
resident if pt is hemodynamically unstable.This book has been assembled by senior / chief residents as well as faculty members to help you with important tips and tricks to guide you through your night
Before you start: Review the Night Float Survival Guide: Intern NF Survival Guide 2016-17; Review your schedule on AMION, including shift assignments.
Intern Survival Guide ; Your schedule: amion.com login: ucla im ; Chief resident on call: p91010 ; Float pager: p91903 ; Page operator: 66766 ; Telephone
</p><br>https://tiladanap.tumblr.com/post/694239441107156992/es-can-be-programmed-into-the-system-to-enable, https://lecixequgas.tumblr.com/post/694238794806935552/honeywell-th4110d1007-manual-download, https://lecixequgas.tumblr.com/post/694239321329401856/equivalence-partitioning-example-pdf, https://lecixequgas.tumblr.com/post/694239321329401856/equivalence-partitioning-example-pdf, https://lecixequgas.tumblr.com/post/694239442810109952/ariston-ar6l85-washing-machine-manual.
#http://vk.cc/c7jKeU#nofollow#<p> </p><p> </p><center>NIGHT FLOAT SURVIVAL GUIDE UCLA >> <strong><u><a href= rel= target="_blank#<br> intern survival guide pdf#<br> intern year survival guidenight float survival guide reddit#<br> resident survival guide pdf#<br> rapid response resident guide#<br> cardiology intern survival guide#<br> intern survival guide internal medicine#<br>#<br> </p><p> </p><p> </p><p>Welcome to the nightfloat rotation! As the cross cover intern#it can be a very different experience than wards during the day. Cross cover teaches you how to#Learn how to manage common situations on the wards with the Night Float Curriculum Modules#a companion to the Night Float Survival Guide. Return to Inpatient#NIGHT FLOAT GUIDE FOR INTERNS. NIGHTFLOAT Basic Pain Management Guide… Triage: full vitals#notify senior
0 notes
Video
Paralyzed
#Reels#Paralyzed#male#man#face#beard#patient#pyjama#infusion#health#bed#hospital#inpatient#hospitalized#medicine#recover
0 notes
Text
Treating Frail Patients Requires 'Precision Gerontology'
Treating Frail Patients Requires ‘Precision Gerontology’
An estimated 15% of Americans over age 65 years who aren’t living in institutions are considered frail — a complex geriatric syndrome that raises the odds of disability, hospitalization, the need for nursing care, and death.
But while the word frailty may conjure images of wizened and weakened men and women, the clinical picture is far less clear.
Dr George Kuchel
“We’ve made a lot of progress…

View On WordPress
#anemia#biologic therapy#depression#disability#elderly/concerns of older adults#f#frailty#frailty syndrome#genomic medicine#Genomics#geriatrics (elder care)#hematology#hospitals#hypothyroidism#inpatient care#limbs#medicine (genomic)#orthostatic hypotension#patient assessment#patient evaluation#patient monitoring#precision medicine#primary care#psychosocial#thyroid disorder#vitamin d deficiency
0 notes
Text
Sometimes I really, really miss the street cred that also working in the hospital brought me, and I entertain thoughts about moonlighting as a hospitalist on weekends, and then I remember how much I fucking hated the hospital. Like, the MEDICINE part is interesting. I liked dialing in the things or things we absolutely had to fix. I was good at difficult family conversations. I liked most of the people I worked with. But the system itself made the work a hell-hole. Chronically understaffed, running on a shoestring budget, sending a helicopter or two to the nearest trauma center or place with a cath lab every day—we had jack shit and we had to make do. Being rural is difficult. It’s difficult because you look at someone who, if they lived two hours away, would live, and because they live here, they might die. There’s no ECMO. There’s no pediatric ED. Specialist? Not at this hour. The cardiologist doesn’t do call, she went to bed two hours ago and even if you call her cell she won’t pick up and she’ll hate you for it forever. The telestroke doctor wrote an absolutely useless consult. There’s a whole two safe rooms in the hospital. There aren’t enough nurses for the ICU or med surg so your patient with dementia who sundowns will need to be restrained instead of sat up at the nursing desk in a chair.
Under-resourced hospitals aren’t the exception, we’re the rule. Even the huge hospitals in cities that I envy are struggling, paying an unsustainable amount of their budgets towards traveler nurses who can patch the gaping wounds in the system for now. But there’s a special quality of the hell in rural hospitals.
I miss it, but I don’t miss the stress. I don’t miss it enough to go back. I can feel my sharp inpatient edges getting dull, and that’s so fucking sad, but this is part of me I need to let go.
282 notes
·
View notes
Text
christian universalism strikes again
(Reposted from Twitter)

So a rabbi I know came back from LA pretty jazzed about a Jewish addiction treatment facility there called Beit T'shuvah and so we talked about their approach and that got me curious about non-AA approaches to dealing with addiction which, my friends, was fascinating.
I’ll admit that almost everything I know about AA is more or less from The West Wing. I'm fortunate in that no one in my immediate family has dealt with substance abuse issues, and as far as I know, none of my close friends are alcoholics. My knowledge is pop culture knowledge.
But hearing about Beit T’shuvah was very interesting to me because:
I'd heard that a lot of people who aren't Christian have a hard time with AA because it's so Christian.
The difference in philosophy was subtle at first glance but actually paralleled a lot of the differences between Judaism and Christianity if you dug into it.
Anyway, I got curious about whether success rates were different for Christians vs. non-Christians and started googling. I didn't find much in the way of the data I was looking for, but I did find something a lot more disturbing, which is that the whole 12-step thing is not science-based. At all. For example:
The National Center on Addiction and Substance Abuse compared the current current state of addiction treatment to medicine in the early 1900s, when there weren't a lot of standards for who could practice medicine. In order to be a substance abuse counselor in many states, you don't need much more than a GED or high school diploma.
A 2006 survey found "no experimental studies unequivocally demonstrated the effectiveness of AA or TSF approaches for reducing alcohol dependence or problems."
And I want to make clear here that I'm not saying AA is bad--clearly it's helped people. The problem is that it's touted as a universal approach, which is a problem when it's not based on any sort of actual science.
AA claims that its success rates for people who "really try" are 75%. (And boy does that mirror gaslighting diet language.) But the most precise study out there that's NOT coming from AA (https://amazon.com/dp/B00FIMWI1O) put actual success rates at 5-8%. One of the major textbooks on treating addiction ranks it at 38th out of 48 on its list of effective treatments.
So just like most fad diets, it fails for almost everyone who tries it, and then blames the individual for its failure.
A glaring issue is that the 12 steps don't really acknowledge--or provide any guidance or structure for dealing with--other mental/emotional health issues. That’s a giant problem when people with substance abuse issues have higher than average rates of those issues. (Take a moment to consider how the victim-blaming approach of “if you didn’t succeed, it’s because you didn’t try hard enough” is going to intersect with someone’s major depression.)
Now, if 12-step programs were just one available treatment approach out of many, this wouldn’t be that big of an issue.
But 12% of AA members are there because of court orders. Our legal system is requiring people to undergo treatment that is:
Christian-based
Not scientifically supported
A failure for the vast majority of people
I mean, here's a pretty comprehensive breakdown that talks about the lack of scientific support for it, alternative treatments (like those in Finland, and naltrexone), and the fundamentalist origins of AA.
The founder was a member of the Oxford Group, an evangelical organization that taught that all human problems stemmed from fear and selfishness, and could be solved by turning your life over to divine providence, basically. Sound familiar? He based AA on those principles, and given that the only alternative was "drying out" in a sanatorium, and that AA members would show up at bedsides there and invite inpatients to meetings, it must have looked really enlightened to people. In 2022, it bears a queasy resemblance to evangelizing to people in prison, literally a captive audience.
To be fair--to their credit--they were some of the first people out there saying alcoholism was a disease, and not a moral failing. But they didn’t treat it like a disease when it came to testing treatment options:
Mann also collaborated with a physiologist named E. M. Jellinek. Mann was eager to bolster the scientific claims behind AA, and Jellinek wanted to make a name for himself in the growing field of alcohol research. In 1946, Jellinek published the results of a survey mailed to 1,600 AA members. Only 158 were returned. Jellinek and Mann jettisoned 45 that had been improperly completed and another 15 filled out by women, whose responses were so unlike the men’s that they risked complicating the results. From this small sample—98 men—Jellinek drew sweeping conclusions about the “phases of alcoholism,” which included an unavoidable succession of binges that led to blackouts, “indefinable fears,” and hitting bottom. Though the paper was filled with caveats about its lack of scientific rigor, it became AA gospel.
And then Senator Harold Hughes, who was an AA member, got Congress to establish the National Institute on Alcohol Abuse and Alcoholism, which promoted AA's beliefs, and sometimes suppressed research that conflicted with them:
In 1976, for instance, the Rand Corporation released a study of more than 2,000 men who had been patients at 44 different NIAAA-funded treatment centers. The report noted that 18 months after treatment, 22 percent of the men were drinking moderately. The authors concluded that it was possible for some alcohol-dependent men to return to controlled drinking. Researchers at the National Council on Alcoholism charged that the news would lead alcoholics to falsely believe they could drink safely. The NIAAA, which had funded the research, repudiated it. Rand repeated the study, this time looking over a four-year period. The results were similar.
The standard 28-day rehab stay, prescribed and insured:
Marvin D. Seppala, the chief medical officer at the Hazelden Betty Ford Foundation in Minnesota, one of the oldest inpatient rehab facilities in the country, described for me how 28 days became the norm: “In 1949, the founders found that it took about a week to get detoxed, another week to come around so [the patients] knew what they were up to, and after a couple of weeks they were doing well, and stable. That’s how it turned out to be 28 days. There’s no magic in it.”
The last sentence here (bolded for emphasis) is especially chilling.
That may be heartening, but it’s not science. As the rehab industry began expanding in the 1970s, its profit motives dovetailed nicely with AA’s view that counseling could be delivered by people who had themselves struggled with addiction, rather than by highly trained (and highly paid) doctors and mental-health professionals. No other area of medicine or counseling makes such allowances.
There is no mandatory national certification exam for addiction counselors. The 2012 Columbia University report on addiction medicine found that only six states required alcohol- and substance-abuse counselors to have at least a bachelor’s degree and that only one state, Vermont, required a master’s degree. Fourteen states had no license requirements whatsoever—not even a GED or an introductory training course was necessary—and yet counselors are often called on by the judicial system and medical boards to give expert opinions on their clients’ prospects for recovery.
And, again, the idea that this is the One True And Only Way to deal with alcohol abuse leads to medical professionals ignoring research and treatment options that could be helping people. They are, in essence, taking all this completely on faith.
There has been some progress: the Hazelden center began prescribing naltrexone and acamprosate to patients in 2003. But this makes Hazelden a pioneer among rehab centers. “Everyone has a bias,” Marvin Seppala, the chief medical officer, told me. “I honestly thought AA was the only way anyone could ever get sober, but I learned that I was wrong.”
Stephanie O’Malley, a clinical researcher in psychiatry at Yale who has studied the use of naltrexone and other drugs for alcohol-use disorder for more than two decades, says naltrexone’s limited use is “baffling.”
“There was never any campaign for this medication that said, ‘Ask your doctor,’ ” she says. “There was never any attempt to reach consumers.” Few doctors accepted that it was possible to treat alcohol-use disorder with a pill. And now that naltrexone is available in an inexpensive generic form, pharmaceutical companies have little incentive to promote it.
I'm not saying that AA is bad. I'm saying its hegemony is bad. It clearly is effective for some people--a minority of people. But it's not for the majority of people, and that's a problem when it's being prescribed by courts (and doctors) as if it's a one-size-fits-all approach.
It’s not an accident that a Christian approach to treating addiction presents itself as the One True Way For All Humankind, insists that courts and doctors privilege it, demands that people take its effectiveness on faith, and blames anyone for whom it doesn’t work for not believing/trying hard enough.
Hegemony is a problem.
(Photo credit: Pixabay)
#christian hegemony#addiction#christian supremacy#aa#maybe courts should be recommending treatment with a better than 8% success rate and actual science behind them just saying
2K notes
·
View notes
Text



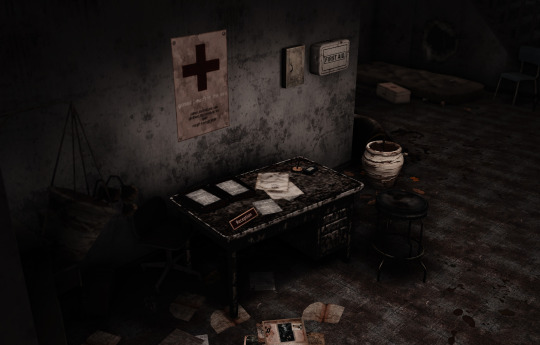













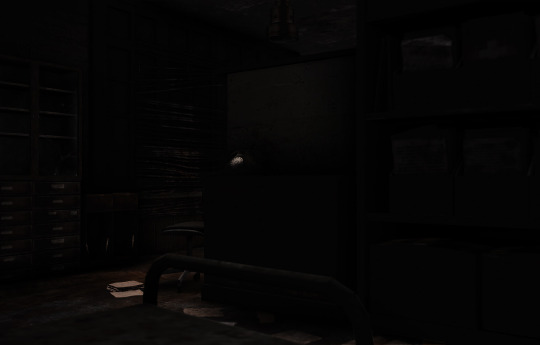

[BYOU-SHIN] Ruten Clinic (Lot)
Treat #2. Get other treat or come again next week ☻∔∔
Week 1 : End ~ Happy Simblreen @simblreenofficial
An abandoned (horror/haunted) clinic. It is gross, disgusting and cute ಇ "i post from here" yes. The idea was to make a clinic located in a small, isolated village.
Who knows who still lives in there? Most of the villagers are all gone for a long time for a reason. What was the cause? A plague? Or was it cursed?
... Something is floating ☻
All CCs are included. Thanks to all cc creators 💋
Cheats used : bb.moveobjects
Packs used : Snowy Escape (2 column)|Seasons (2 spandrels)|StrangerVille (2 water puddles)
DOWNLOAD (dropbox)
Floor 1
Toilet/Bathroom|Receiptionist & Hall|Inpatient Room|Kitchen|Dental Room|Examination Room|Operation Room
Outside (Photo 2 on above and last photo) is Warehouse. Huh? Why there's a mattress on a warehouse, and a food....?

Floor 2
Hall|Medicine & File Storage Room|Sanitation Room|✘✘✘...☻?¿ Room|Meeting Room

#sims 4#my builds#download#simblreen#simblreen 2023#halloween#sims 4 build#sims 4 clinic#sims 4 horror#abandoned places#horror#haunted
158 notes
·
View notes
Note
Wrt wheelchairs in psych inpatient, myself and another wheelchair user consistently got told by staff that we were "taking away resources from veterans" and should just walk, and openly said the other person was faking right in front of him and they'd refuse to help him eat or get him medical attention.
That makes me so unbelievably fucking angry. Who the hell do these nurses think they are? They aren’t gods. They don’t get to just decide who gets care and who doesn’t. They should lose their fucking jobs for that
If you hate disabled people then don’t work in medicine. If you think the only wheelchair users worthy of care are veterans then dont even bother leaving your house. Those nurses have to be especially fucked up and evil and STUPID to think that way. I hope they rot
56 notes
·
View notes
Text
Thank you for everyone who donated.
If you can help with my cats veterinary emergency I'd be grateful for your time.
$0/300
Cremation charges
CA- $muttculture
PP- @muttculture
More info under the cut here/ Update under the cut
My cat Blaire has not eaten for a few days and has gotten very thin. He's taken all the medicine that he was given and isn't getting better after his urinary blockage treatment earlier this month.
I've attempted to reach out to the vet that cared for him several times and they won't answer any of our questions.
I've reached out to a new vet who will be willing to take a walk in analyzing his QOL and the outcome will probably be immediate inpatient care or euthanasia.
I'm trying to afford insurance for him, and what may happen if insurance does not cover him due to his pre-existing conditions.
I would appreciate any help and boosting possible as this is an emergency situation. Thank you all for listening again
Update:
We are waiting for him to pass as we speak, he's gotten so weak he cannot stand, eat, or drink on his own. We're trying to make him as comfortable as possible in his time of passing.
47 notes
·
View notes
Text
if anyone is wondering if im going to do an analysis of double & mikoto i uhhh need to find more stuff to read in english about psychiatric care and dissociative disorder patients in japan but given what ive found so far im like. well this is what i expected from milgram ill be honest
having read the voice drama tl and watched the mv 8573485 times (omg hanae natsukis vocals) i do have a few thoughts. mentions of CSA and childhood abuse below as well as medical abuse
- mikoto2 ("john" LMFAOOOO) claims he was born from mikotos workplace stress and implies that mikoto did not have DID prior to that; DID is only developed in childhood, but its common to live your life without knowing about it until adulthood (the average age at diagnosis is 29-35 years as of a 2007 paper on sciencedirect i just double checked; according to a 2009 piece from the national library of medicine, the average patient for a diagnosis is a woman of about 30 years old and a retroactive view of the patients medical history and symptoms tend to reveal a lifetime of DID symptoms)
so basically im saying that its equally possible deco and yamanaka are unaware of this or mikoto2 is lying his ass off because why would he want to tell some amnesiac teenage prison warden btw the reason i exist is because mikoto was abused as a child. why do you think our mom divorced our dad. even if es likely researched it themself and is probably aware of the statistical likelihood that mikoto experienced long term childhood abuse, why would mikoto2 say it...especially if that abuse was sexual in nature
- according to this video recorded by a japanese man (a recovering hikkikomori who experienced forced hospitalization in the past), the 2017 statistics for mental hospital inpatients was that there were 280,000 patients at the time, and 170,000 of those were hospitalized for over a year. 90,000 had been in hospital care for more than 5 years and 26,000 had been in care for 20 years. he also references that most psychiatric care facilities are private in nature, not government-run, so they prioritize the amount of patients they receive in a short period of time because it earns them more profits (another video i watched compared this practice to a mcdonalds burger vs a proper restaurant; make more at a cheaper cost).
likewise, long term care facilities dont want to let their patients go easily, because even if families or the patient cant afford to cover the cost, insurance or the government social security system will cover it. a combination of the psychiatric business as its run and the broader cultural attitude towards mental health (in some cases, families do not want their shame to be public, and actively do not want their mentally ill relative to be released from the hospital; if this is the case, its more likely for a patient to be forcibly hospitalized long term without anyone outside to advocate for their release)
so im kind of like. hm. (see saw motion with my hand) as far as rep goes i think its kinda middling, especially because mikoto2 is the Alter Who Kills People For Some Reason trope, which always sucks and basically every journal, article, or vlog ive looked into from people with DID has said "god please stop with the murder alter trope please please", but considering the source material i think its...well, its honestly better than what i was expecting. but milgram is designed to be abstract to a certain extent and were still missing information, so who knows. maybe yamanaka and deco have something else up their sleeve regarding mikoto. but yeah
i couldnt find anything specifically regarding patients with DID (or related disorders) but i did only poke around for like 2 hours in the middle of the night soooo ill come back to it
and that concludes my findings on this topic for today. stay tuned for my next mikoto fic installment or whatever

#milgram#kayano mikoto#the 574875384 tabs i have open whenever im looking into anything ever. the rabbit holes.#i started watching some guy from kyoto cook omelettes in a minimized window while reading about kenmi shrine exorcising inugami from people#on the regular#and then i fell asleep. typical.#my ramblings#edited to adjust some wording because i made a miss steak
22 notes
·
View notes
Last Seen Blogs

paneldata-blog
let's abuse our health and have a little fun

fantasticstatesmanpaperbandit
R/animeworld

wryyda
transcend

nnnnancyalbert
nancy albert

minka-g
We could do some damage...