#mastocytosis
Text
Long post, lots of science but as much plain English as I could. Not proofread. About two conditions in general but also their combined effects on me specifically.
‐‐
In my opinion, anyone diagnosed with fibromyalgia, especially if it is has not been responsive to nerve pain medications, or general "chronic fatigue" should be reevaluated using the ICC for ME/CFS.
Patients should also be evaluated for mast cell disorders (mastocytosis - too many mast cells and MCAS - too sensitive mast cells). If those disorders are present, then patients should be reevaluated for ME/CFS after as much treatment as possible for the mast cell disorder.
The presence of ME/CFS is one of the biggest factors when it comes to quality of life prognosis for the hEDS cluster of disorders (hEDS, POTS, MCD/MCAS, ADHD, and ME/CFS), in my experience. The second largest factor is what mast cell triggers the patient has (like allergies but can be anything including chemicals produced as part of natural body processes).
I have ME/CFS, and one of my mast cell triggers is aerobic activity.
ME/CFS can involve an impaired oxidative metabolic pathway (which makes Krebs cycle not work properly) and impaired energy use (ATP to cellular work), so patients are intolerant to anything that consumes energy - aka being alive. The degree to which energy production is impaired and thus the degree of intolerance to energy use is what determines illness severity, and does make very severe ME/CFS fatal because patients can't produce enough energy for cellular processes and replication, leading to multiple organ failure. Mine is considered mild-moderate. Some people with very mild ME/CFS are able to work, and mild ranges from only minor impact on activities to about 50% reduction in activity. Moderate is mostly housebound.
The changes in energy production is what sets ME/CFS apart from other serious and fatiguing illnesses. Studies in patients with renal disease, pulmonary hypertension, cystic fibrosis, and other such disorders showed that they can exercise to exhaustion on day and then exercise to that same limit the next day. They may have mechanical muscle or joint pain, but they are able to produce the same amount of energy. ME/CFS patients cannot do this.
For some this means they can't produce the same amount of ATP (measured by oxygen consumption at anaerobic threshold), for others it means the same amount of oxygen consumption but being unable to convert that into force. For this first group, this means that their anaerobic threshold is lowered - they switch from aerobic to anaerobic respiration more quickly.
Aerobic respiration produces 36-38 ATP (energy, basically stamina points in a video game) plus water and CO2. Anaerobic respiration produces 2 ATP plus lactic acid. So with the oxygen metabolism impairment, an ME/CFS patient literally cannot produce the same energy as someone doing the same activity with the same rate of respiration with no oxygen metabolism impairment.
But what does having aerobic activity triggered MCAS mean?
All aerobic activity in the muscles causes some mast cell degranulation, which releases histamine and other inflammatory mediators into the bloodstream. This is not necessarily anything anyone would normally consider "exercise." It is any contraction and/or relaxation (change from neutral state) of muscle. While it isn't totally understood (and the exact signal to trigger this mast cell degranulation is unknown) its believed that this process happens to help with vasodilation in the working muscles and to help carry oxygen, sugar, atp, and all those other things muscles need to work and to then heal afterwards.
With mastocytosis or aerobic triggered MCAS, the amount of those released mediators is increased. This can mean mildly more inflammation, or it could be to the point of anaphylaxis. Typically its somewhere in the middle. Mastocytosis is usually stable, but MCAS can become more sensitive - the threshold before there is a problem lowers.
Combining those two together, I have a body that has a low threshold for aerobic activity (higher inflammation than a healthy person for the same activity), poor aerobic ATP production, and a lowered anaerobic threshold (based on symptoms and response to D-ribose supplementation, only way to distinguish between poor oxygen use and poor ATP use is very specialized and largely unavailable testing). Being in an anaerobic state also causes inflammation, which is why a main goal of many workout programs is to /increase/ your anaerobic threshold, something its not clear if ME/CFS patients can do at all.
So what I have is constant inflammation in all of my body that can be worsened by anything.
To which we say, "what the fuck? Holy shit. That sucks ass. I'm now amazed you do the amount that you do. Fuck. What can help?"
Medications and supplements to lower the inflammation, avoiding chemical/food/environmental mast cell and inflammatory triggers/treatments to reduce how inflammatory they are, d-ribose supplement to produce ATP on a different pathway, medications to manage the secondary conditions caused by the mcas and inflammation (POTS), resting, and not pushing when my body says stop.
#my og#my life#disability#ME/CFS#MCAS#mast cell activation syndrome#mast cell disorders#mastocytosis#chronic fatigue#chronic illness#chronic fatigue syndrome#myalgic encephalomyelitis#fibromyalgia
4 notes
·
View notes
Text
mast cells united: a summary of my thoughts
overall, I do not like the author. her scientific communication is very weak, her perseverance on naturopathy ranges from grating to outright concerning, and between the two it drastically weakens the overall quality of this book as a resource. there's also some deeply problematic discussion of autism sprinkled in at random. and no glossary at all which seems like a very strange thing to leave out, especially as terms get defined sporadically in the main body (and more often than not, either repeatedly or not at all). the perseverance on naturopathy in particular never seemed to be mentioned when I heard others talking about it, and it was downplayed in the cover blurb as well, so do be aware of that.
however, there are still chunks of this book that are more helpful than the information presented in never bet against occam, the other Big Book Of MCAS. these two books are likely to be most useful in conjunction with one another, with a strong eye for editorializing this one in particular, much like one is strongly suggested to skip certain episodes of classic TV series for the optimal viewing experience.
I would advise reading never bet against occam first, as it rests largely on a number of case studies that are presented in a manner making it much easier to recognize potential symptoms of mcas and bring it to the table for initial consideration. mast cells united is much less narrative in its presentation of potential symptoms aside from the author's experience described in chapter 1 which is gonna be of highly limited recognition especially as the only one, but provides a greater quantity of condensed and accessible information about things like the mast cell itself and supported treatments that is also several years more up to date than occam, making it less useful for raising initial suspicions but more useful as an information resource in the process of diagnosis and treatment.
when reading mast cells united, I strongly advise skipping the following entirely:
chapter 1
in chapter 4, the section starting with the header "MCAS and the RCCX theory" up until the header "the tryptase conundrum"
chapter 5
in chapter 6, the section starting with the header "the big picture approach" through the end of the chapter
in chapter 7, the section starting with the header "autism spectrum disorders" through the end of the chapter
chapter 8
in chapter 9, the section starting at the beginning of the chapter up until the header "mainstream medications for mcas treatment"
chapter 10 (although the section on pregnancy may have some value)
in chapter 12, the section starting with the header "detoxification" up until the header "exercise and MCAS" - the section starting with the header "neuropsychological treatment approaches" up until the header "strategies for emotional healing" - the section starting with the header "joy vs happiness" up until the header "other strategies to restore [PSNS] dominance"
I did not read chapter 11 for personal reasons but it may be useful to others if approached with due caution.
there are other small sections that irritated or bored me, including elements of ableism and patronization, but this removes the majority of the Complete Trash from the pile, leaving you with mostly beneficial information, which will make it an overall more pleasant and useful experience. there are some sections that include discussion of medical neglect, which I have for the most part left in, for though it can be upsetting it is useful.
the author's resource website is still up under the same name as the book, and it looks like she put out another book in 2021 that is much more explicit in the description about its focus on naturopathy, so I'm gonna just assume that of the two probably just get this one, unless you're into it too. and don't worry, of course she also offers a $300 video course about mold! :|
for more detailed (less organized) thoughts, see my other posts as I read under the tag [mast cells united].
#mast cells united#amber walker#mast cells united: a holistic approach to mast cell activation syndrome#mcas#mcad#mast cell activation syndrome#mastocytosis#trying to make this findable :T#long post
2 notes
·
View notes
Text
Has anyone else noticed how very acceptable it is to crap on people with allergies on Tumblr?
If you remind people that this thing that is completely innocuous to most folks, is deadly to others. Doesn't mean your wrong for enjoying it, just a reminder that people with dangerous allergies do in fact exist.
And they will respond with an eye roll and have a laugh about peak Tumblr nonsense.
I see this from people that would recognize this as unacceptable if allergies were substituted for another disability.
I'm very tired of this societal idea that your allergies are just you being a pain in the ass for the fun of it.

Oh, did the fact that people like me exist ruin your day?! So sorry that my disability has so negatively impacted you.
#allergies#chronic illness#disability#mastocytosis#mcas#mast cell disease#housebound#mast cell activation syndrome#urticaria
16 notes
·
View notes
Link
Understanding Urticaria Pigmentosa: Symptoms, Causes, and Treatment Urticaria Pigmentosa (UP), though rare, is a skin condition that merits attention. This comprehensive guide aims to shed light on UP, offering insights into its symptoms, potential causes, and available treatment options. By the end of this article, you'll have a deeper understanding of this condition and how to manage it effectively. What is Urticaria Pigmentosa? Urticaria Pigmentosa, often abbreviated as UP, is a dermatological condition characterized by the presence of brownish or reddish-brown spots or lesions on the skin. These spots, known as macules, typically appear during infancy or early childhood and may persist throughout a person's life. While UP is considered a benign condition, its impact on skin appearance and potential symptoms can vary significantly from person to person. [caption id="attachment_51820" align="aligncenter" width="532"] urticaria pigmentosa[/caption] Symptoms of Urticaria Pigmentosa The symptoms of Urticaria Pigmentosa can manifest differently in each individual. However, there are several common signs and sensations associated with this condition. Recognizing these symptoms is essential for early diagnosis and effective management Causes and Triggers While the exact cause of Urticaria Pigmentosa is not fully understood, it is generally considered a result of genetic mutations. Specifically, it is associated with mutations in the KIT gene. These genetic changes lead to the abnormal accumulation of mast cells in the skin. When these mast cells are stimulated, they release chemicals that can cause the characteristic skin reactions seen in UP. Diagnosis and Medical Evaluation Diagnosing Urticaria Pigmentosa typically involves a thorough medical evaluation by a dermatologist or a healthcare professional with expertise in skin disorders. The diagnostic process may include: Clinical Examination: A visual examination of the skin to identify characteristic macules and any associated symptoms. Darier's Sign Test: This simple test involves gently stroking a suspected lesion, and if it results in localized itching, swelling, or hives, it's a positive Darier's sign—a strong indicator of Urticaria Pigmentosa. Skin Biopsy: A skin biopsy may be performed to confirm the presence of mast cells in the affected skin tissue. Genetic Testing: Genetic testing may be recommended to identify specific mutations in the KIT gene, providing definitive confirmation. Treatment Options Treatment for Urticaria Pigmentosa aims to alleviate symptoms and improve the quality of life for individuals with this condition. The choice of treatment can vary based on the severity of symptoms and individual needs. Common treatment options include: Topical Corticosteroids: These anti-inflammatory creams or ointments can help reduce itching and skin inflammation. Antihistamines: Oral antihistamines are often prescribed to relieve itching and discomfort. Phototherapy: Controlled exposure to ultraviolet (UV) light can be beneficial in managing symptoms. Avoiding Triggers: Identifying and avoiding triggers that worsen symptoms, such as excessive heat or friction, can be effective. Consultation with a Specialist: For severe cases, consultation with an allergist or immunologist may be necessary to explore advanced treatment options. Living with Urticaria Pigmentosa Living with Urticaria Pigmentosa requires proactive management and lifestyle adjustments. Here are some tips for individuals with UP: Skin Care: Adopt a gentle skincare routine to minimize irritation. Temperature Control: Avoid overheating or extreme cold, as temperature changes can trigger symptoms. Allergen Avoidance: Identify and avoid allergens or irritants that may exacerbate symptoms. Regular Follow-ups: Maintain regular appointments with your dermatologist or specialist to monitor your condition and treatment effectiveness. Support Groups: Consider joining support groups or communities to connect with others facing similar challenges. Research and Advancements Ongoing research and advancements in the field of dermatology and genetics continue to expand our understanding of Urticaria Pigmentosa. Here are some notable areas of progress: Genetic Studies: Researchers are delving deeper into the genetic mutations associated with UP, paving the way for potential targeted therapies. Immunotherapy: Promising research explores the use of immunotherapy to regulate mast cell activity and mitigate symptoms. Clinical Trials: Participation in clinical trials may offer access to cutting-edge treatments and contribute to advancing UP research. Coping and Support Living with Urticaria Pigmentosa can be challenging, but with the right support and coping strategies, individuals can lead fulfilling lives: Education: Understanding your condition and its triggers is empowering. Emotional Well-being: Seek emotional support from friends, family, or support groups. Advocacy: Advocate for yourself by communicating openly with healthcare providers about your needs and concerns. Positive Lifestyle: Embrace a positive lifestyle by focusing on activities and interests that bring joy and fulfillment. Frequently Asked Questions (FAQs) related to Urticaria Pigmentosa: Q: What is Urticaria Pigmentosa (UP)? A: Urticaria Pigmentosa is a rare skin condition characterized by brownish or reddish-brown skin spots or lesions. Q: What causes Urticaria Pigmentosa? A: UP is primarily caused by genetic mutations, specifically mutations in the KIT gene, leading to mast cell accumulation in the skin. Q: Are there any known triggers for Urticaria Pigmentosa symptoms? A: Symptoms of UP can be triggered by factors such as heat, friction, and emotional stress. Q: Is Urticaria Pigmentosa contagious? A: No, UP is not contagious; it is a non-infectious skin condition. Q: Can Urticaria Pigmentosa be cured? A: UP is a chronic condition, and while it can be managed, there is no known cure. Treatment aims to alleviate symptoms. Q: How is Urticaria Pigmentosa diagnosed? A: Diagnosis typically involves a visual examination by a dermatologist, the Darier's sign test, skin biopsy, and genetic testing. Q: Are there any complications associated with Urticaria Pigmentosa? A: In some cases, UP may lead to systemic mastocytosis, a more severe condition. Regular medical monitoring is essential. Q: Can Urticaria Pigmentosa be passed down through generations? A: UP can have a genetic component, and there may be a familial predisposition, but not everyone with a family history will develop the condition. Q: What treatment options are available for Urticaria Pigmentosa? A: Treatment may include topical corticosteroids, antihistamines, phototherapy, and allergen avoidance, depending on the severity of symptoms. Q: Is there ongoing research into Urticaria Pigmentosa? A: Yes, research into UP and related conditions continues, with a focus on genetic studies, immunotherapy, and clinical trials for potential treatments. Conclusion In conclusion, Urticaria Pigmentosa is a unique dermatological condition characterized by skin lesions, itching, and mast cell accumulation. While it poses challenges, proper diagnosis and management can significantly improve the quality of life for those affected.
#brown_skin_spots#Brown_Spots_on_Skin#Dariers_Sign#Dermatological_Condition#Genetic_Mutations#Mast_Cell_Accumulation#Mast_Cell_Disorder#Mastocytosis#Reddish_Brown_Lesions#Skin_Disorder#Skin_Lesions#Urticaria_Pigmentosa_Symptoms
0 notes
Photo

A #dayinthelife of a #spoonie: Festive #stpatricksday with the 'rents. I can't stress how good it is to get out of the apartment, especially to spend some time with #family . Cabbage, potatoes and carrots didn't know what hit 'em. Then my #gastroparesis didn't know what hit it. 😶 . . Rockin my @moetheband #moedown themed "Vote Rex" (@rex_a_vision ) shirt and sequinned suspenders. Yes, it's my only green shirt lol. #symptoms #dysautonomia #pots #irish #primaryimmunedeficiency #mastocytosis #mastcellactivationsyndrome #dreads #raredisease #spoonielife #dreadlocks #systemicmastocytosis #ehlersdanlossyndrome #research #cure #chronicillness #curvygirl @rarediseasedayofficial @rare @rareis___ @rarediseasedayus #invisibleillness @medtronic @chronicillnesshumor (at Lake Ronkonkoma, New York) https://www.instagram.com/p/Cp84e_fN6Rs/?igshid=NGJjMDIxMWI=
#dayinthelife#spoonie#stpatricksday#family#gastroparesis#moedown#symptoms#dysautonomia#pots#irish#primaryimmunedeficiency#mastocytosis#mastcellactivationsyndrome#dreads#raredisease#spoonielife#dreadlocks#systemicmastocytosis#ehlersdanlossyndrome#research#cure#chronicillness#curvygirl#invisibleillness
0 notes
Text

#kirby#daily kirby#my art#digital#hal laboratory#nintendo#biopsy results got logged automatically#so I know it's not mastocytosis which means it's mcas#which is the 'less serious' disorder but not the outcome we wanted.#cuz I already got 4 immunology referrals rejected last year.#so I have no idea how much longer it will be before I actually get some friggin treatment.#(I am somewhat medicated but it's clearly not enough and I haven't gotten actual meant-to-help-now changes in 2 years.)#it's a friggin time of it my dudes.
117 notes
·
View notes
Text
.
#I'm having a weird influx of feelings because I'm watching a person I care about find out in real time#that they have systemic mastocytosis#an aggressive auto-immune disorder that can destroy a person's tissues in anywhere from 2 to 16 years#they're MY age#and in a committed relationship with a kid#I dunno how to feel but weird and sad
4 notes
·
View notes
Note
Hi! Sorry to bother you with this - I checked your FAQ and MCAS tag and if the answers are there already I apologize for missing them! But I was wondering if you have a masterpost or similar with basic info on MCAS (what it is, how to figure out if you have it, what to do...) anyway thank you for posting so much about this, I'm learning a lot ^^
Hello! I don't have a list because if I started typing one out, I'd never stop. The Healthline article about it, however, is fairly comprehensive for the basics.
One thing the article doesn't list is that MCAS can also be a source of deep, deep tissue pain (sometimes I swear it's coming from my bones). Some recent research has linked unstable mast cells to fibromyalgia, which is why you'll often find a lot of anecdotal stories online about the two being co-morbid. MCAS can also be more likely in people with EDS or hypermobility spectrum disorder and can sometimes also be a source of dysautonomia. (Honestly, it's a bit chicken vs egg sometimes.)
They may have updated their criteria since the last time I checked, but the American Academy of Allergy and Asthma & Immunology used to list anaphylaxis as a requirement for diagnosis, but that is not true.
Many people experience MCAS without ever going into full anaphylactic shock.
They also used to stipulate that diagnosis was based on elevated tryptase tests, which is not accurate for MCAS. The tryptase tests are meant for diagnosing mastocytosis, which is like the big cousin disorder of MCAS. Most knowledgeable MCAS doctors now diagnose based on a history of symptoms and response to elevated doses of h1 and h2 antihistamines, as well as other mast cell stabilizers.
TMS for a cure has a lot more info, as well as a patient resource portal that includes a list of physicians, support groups, and ER protocols.
I'd highly rec having a read-through at some point.
Hope that helps!
248 notes
·
View notes
Text

Screaming into the void
Reaction from exposure to scented laundry products from the neighbors across the street
Tide and Downy products
#chronic illness#disability#mastocytosis#mcas#allergies#mast cell reaction to fragranced laundy products#mast cell disease#mast cell activation syndrome#perfume#personal safety#accomodations#disability accommodations#disability access#scents#scented products#tide#Tide laundry#Downy#Downy laundry#Unilever#housebound#spoon theory#spoonie#out of spoons#comorbid conditions#eds#actually disabled
7 notes
·
View notes
Text
What is Idiopathic Mast Cell Activation Syndrome?
Idiopathic Mast cell activation syndrome (MCAS) is one of several mast cell disorders. MCAS occurs when there are a normal number of mast cells in a person's body but they over-release mast cell mediators causing random allergic reactions in multiple systems of the body. MCAS is incredibly common being present in an estimated 17% of the population.
Symptoms
MCAS symptoms are incredibly varied and always occur in multiple systems of the body. Anaphylaxis is common.
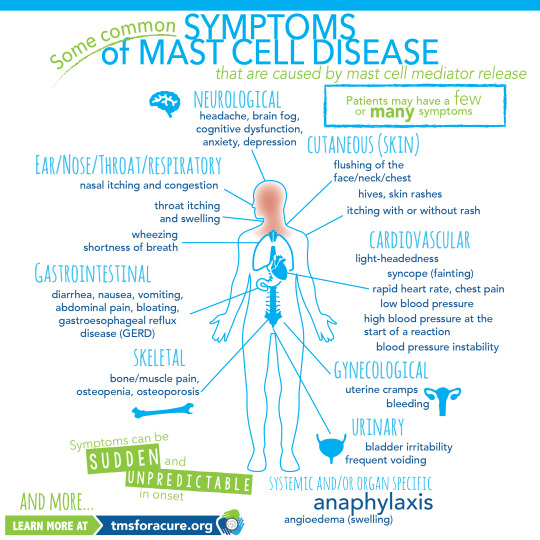
[ID: A graphic labeled "Some common symptoms of Mast Cell Disease" A graphic of a person standing in the center with multiple organs visible is shown. Around the person are lines pointing to specific areas of the body labeled with the body system and symptoms. Clockwise these read "Neurological headache, brain fog, cognitive dysfunction, anxiety, depression Cutaneous (Skin) flushing of the face/neck/chest, hives, skin rashes, itching with or without rash Cardiovascular light-heartedness, syncope (fainting), rapid heart rate, chest pain, low blood pressure, high blood pressure at the start of a reaction, blood pressure instability Gynecological uterine cramps, bleeding Urinary bladder irritability, frequent voiding Systemic and/or organ specific Anaphylaxis angioedema (swelling) Skeletal bone/muscle pain, osteopenia, osteoporosis Gastrointestinal diarrhea, nausea, vomiting, abdominal pain, bloating, gastroesophageal reflux disease (GERD) Ear/Nose/Throat/Respiratory nasal itching and congestion, throat itching and swelling, wheezing, shortness of breath and more" In the bottom left corner "Symptoms can be sudden and unpredictable in onset learn more at tmsforacure.org"]
MCAS symptoms are specifically not allergies. the reactions may look like allergies but the two are not the same and MCAS is not a condition meaning "many allergies" While MCAS can have some consistent triggers one of the defining features of the disease is that reactions are random and happen unpredictably.
Anaphylactic shock is not a requirement for diagnosis.
Diagnosis
MCAS is diagnosed by an immunologist. It is in part a diagnosis of exclusion and requires ruling out both allergies and systemic mastocytosis as well as other conditions such as certain types of tumors.
Diagnostic criteria for MCAS is debated. Some immunologists follow the symptom-based diagnosis approach in which case the diagnostic criteria are:
Recurring and severe anaphylactic-like episodes that involve more than one organ system
and
Positive response to mast cell stabilizing or mediator medications anaphylaxis-type symptoms
Others follow diagnostic criteria based on laboratory findings. In this case the diagnostic criteria are:
Episodic symptoms consistent with mast cell mediator release affecting two or more organ systems evidenced as follows:
Skin: urticaria, angioedema, flushing
Gastrointestinal: nausea, vomiting, diarrhea, abdominal cramping
Cardiovascular: hypotensive syncope or near syncope, tachycardia
Respiratory: wheezing
Naso-ocular: conjunctival injection, pruritus, nasal stuffiness
and
A decrease in the frequency or severity; or resolution of symptoms with anti-mediator therapy: H1 and H2 histamine receptor antagonists, anti-leukotriene medications (cysLT receptor blockers or 5-LO inhibitor), or mast cell stabilizers (cromolyn sodium)
and
Evidence of an elevation in a validated urinary or serum marker of mast cell activation: Documentation of elevation of the marker above the patient’s baseline during a symptomatic period on at least two occasions; or if baseline tryptase levels are persistently >15ng, documentation of elevation of the tryptase above baseline on one occasion. Total serum tryptase is recommended as the markers of choice; less specific (also from basophils) 24 hour urine histamine metabolites, or 11-beta-prostaglandin F2.
and
Primary (clonal) and secondary disorders of mast cell activation ruled out.
These are not all proposed diagnostic criteria as the subject is heavily debated. Generally, a laboratory-confirmed MCAS diagnosis is considered more legitimate.
Treatment
MCAS is a very treatable condition. Generally treatment follows a path from antihistamines -> mast cell mediators -> biologics.
Epipens are given to MCAS patients with a history of anaphylaxis.
Antihistamines are divided into 2 categories: H1 antagonists and H2 antagonists. These categories are determined based on the histamine receptor each one targets.
H1 antagonists mostly deal with systemic and cutaneous symptoms. H1 antagonists are also further divided into first and second generation antihistamines. first generation antihistamines include diphenhydramine (Benadryl) and Hydroxyzine. These tend to cause drowsiness. With second generation H1 antagonists cause fewer side effects and include drugs like loratadine (Claritin) and cetirizine (Zyrtec)
H2 antagonists primarily affect the gastrointestinal tract and include medications like famotidine (pepcid)
Typically when treating MCAS a person will be put on both a second generation H1 antagonist and an H2 antagonist.
When antihistamines do not treat symptoms well enough the next step is a mast cell mediator. The most common mast cell mediator is cromolyn sodium which is available by prescription only. (this is technically available OTC but it is at 1/50th the dose used for MCAS) Mast cell mediators work by preventing the degranulation of mast cells in the first place.
When both antihistamines and mast cell mediators are insufficient someone with MCAS might be prescribed a biologic such as Xolair to treat their remaining symptoms.
Sources:
American Academy of Allergy, Asthma, and Immunology
Mast Cell Hope
Mast Cell Activation Syndrome: Proposed Diagnostic Criteria
#mast cell activation syndrome#mcas#mast cell disease#mast cell activation disorder#mcad#chronic illness#chronically ill#physical disability#physically disabled
47 notes
·
View notes
Text
@nomnomlexy, @endreal, @gelfling-gxrl, @quannaix, @cryptheks, and then @endreal again, have all tagged me to post a selfie at various intervals over the past few months and I just honestly have not been feeling my me to the point where I've been comfortable putting up a selfie in that entire timeframe, but on the weekend I went Spot Spotting for International Mastocytosis & Mast Cell Diseases Awareness Day 2023 and I did take a few selfies over the course of the night so here is just all of them.






22 notes
·
View notes
Text
Mega post
Please share
World Health Network global
Protect Their Future (Grassroots org of parents & pediatricians advocating for protection for ALL children)
linktr.ee/laughterinlight_sciencelibrary
PeoplesCDC.org
longcovidlearning.org
covidresearch.net
#ME Action Network
Long COVID with ME
Long Covid Advocacy Ireland
Dysautonomia International
DecodeME the ME/CFS Study (The world's largest study ever into #MEcfs.Take part today (UK, 16+) #pwME [email protected] - 0800 196 8664 #DecodeMEStudy #pwME #MillionsMissing)
Dysautonomia Society (💜We aim to increase global awareness of Dysautonomia. Join us!)
Mast Cell Disease Society (Transforming lives of patients and families while finding a cure for #mastcelldisease since 1995. #Mastocytosis #MCAS #HereditaryAlphaTryptasemia #raredisease)
Mast Cell Action (We exist to promote progress in the awareness, diagnosis and treatment of Mast Cell Activation Syndrome and to provide support to people affected by MCAS)
Awareness for POTsies (POTS, Chronic Illness, & Mental Health Support. Compassion, Awareness, Education, Empowerment)
linktr.ee/longcovidlife
linktr.ee/longcovidfam (Long Covid Families)
Long Covid Kids (UK, Ireland)
Clinically Vulnerable Families
Abrome (Self-Directed Education community)
Long COVID Physio
NotRecovered.org (Support for chronically ill)
Covid Persistente México Comunidad Solidaria
Long Covid Latin America (Twitter & Instagram) & André Saravia (Twitter & Instagram)
Long Covid Chile (Instagram, Twitter & YouTube)
Linktr.ee/wearebodypolitic (Support for chronically ill)
Linktr.ee/patientled (Patient led research)
Long Covid Advocacy
RTHM.com (RTHM Health, biotechnology research. Transforming care for complex illnesses starting with long covid).
Linktr.ee/covidisntover (Virtual hangout)
CovidSafeDentists.ca
CovidConsciousTherapists.com
Covid Safe Cuties (dating) Twitter & Instagram
CovidMeetUps.com (Covid safe networking & listings)
Linktr.ee/PenGwenWithLC (Project in progress for long haulers)
Bheecollective.org (Send letters to White House)
International Long Covid Awareness
MandateMasksUS.org
PandemicAidNetworks.org (Organizing and info hub)
High Impact Strategies (S4HI builds the power of chronically-ill & disabled people, our groups & networks. #NothingAboutUsWithoutUs #PandemicsAreChronic)
Birch Health (Twitter & Instagram (Infographs and amplifying stories of black, indigenous and racialized peoples)
The Chronic Collaboration
Linktr.ee/equiinstitute
CoalitionForCovidJustice.com
Long Covid Justice
Linktr.ee/Project_N95 (PPE)
Linktr.ee/DonateAMask (PPE)
Clean Air Crew (Airborne pandemic tips and tools)
Clean Air Stars (Helping businesses protect their customers from viruses like SARS-CoV-2)
Aaron Collins (@/masknerd) Twitter & YouTube "Goal is to test and evaluate the best masks out there."
Breathe Safe Air (Everything that you need to know about air pollution. Respirators, masks, air purifiers, monitors and more)
Clean Air Club (Ensuring accessible and cleaner air for Chicago artists and venues. ☁️ a new project by @/nora_barnacles)
*List updated periodically*
You are not alone
Your life has inherent worth
Sars CoV-2 and long covid are real
The pandemic is not over
#Covid-19#covid 19#sars cov 2#covid#long covid#long haul covid#The Pandemic#pandemic#public health#Resources#Info#Information#Mega Post#Please share#Feel free to share!#Feel free to reblog and add more#Especially resources in other languages and countries
24 notes
·
View notes
Text

#kirby#daily kirby#my art#digital#hal laboratory#nintendo#I don't think I mentioned at the time because it was in the middle of kirb2k#but I had an appointment with a hematologist last week#they confirmed the culprit behind my chronic illness is definitely my mast cells#but I need to get a bone marrow biopsy next month to find out#if it's actually not-technically-autoimmune (mcas)#or if it's actually not-technically-cancer (mastocytosis)#which is actually good news cuz 1 someone finally confirmed my nearly 6 year old hypothesis instead of just agreeing (or disagreeing)#and 2 if it *is* mastocytosis they're gonna start medicating me A Lot more aggressively :)#which I need! I've been sick for right about 8 years now but it's gotten rapidly worse in the past 1-1.5 years#so clearly I'm badly under-medicated#(since I've been on all the same meds for 2 years except for my own emergency intervention.)#(I mean technically I've been chronically ill my whole life it just wasn't disabling until early 2016)#anyway I'm so tired I feel like a ragdoll half the time! sure hope I get adequate medication in a couple months!
86 notes
·
View notes
Last Seen Blogs

shashin-nikki
Shashin Nikki

ithegirl
Untitled

ndcdebtrelief
National Debt Counsellors

punkyneuronerd
Is that neurodivergence??

shantisweetz-blog
Shanti