#medical studies
Text

29.07.2023
Spent most of the day in the library, felt so cozy in such a rainy day. 🍃🌧️
#studyblr#med school#studying#medstudyblr#summer#motivation#med student#library#morning#cozy#medschool library#love rain#rainyday#rainy aesthetic#rainyweather#studygram#medical studies#medschool#medicine#innocent drink#fresh#felt nice#revision
1K notes
·
View notes
Text
honestly you probably shouldn't go into the medical profession if you aren't prepared to treat patients with dignity and respect - even if your job exploits you, even if your bosses suck, even if you're exhausted.
yes, you are allowed to have feelings and be tired. but you have to be willing and able to either admit when you can't do something (and take the consequences), or put how you feel aside and do your job. for the sake of your patient.
you and your job may be harmed by the medical industrial complex's wrongness, but to your patients, you are part of the complex that is also gravely failing them. you have the power to be a force of goodwill and care, or an instrument of oppression.
that is what you're signing up for when you become a medical professional. don't like it? don't become a medical professional.
#softspoonie#medical industry#medical professionals#medical#medical system#medical ableism#medical abuse#medical trauma#disability advocacy#health#health advocacy#ableism#systemic ableism#systemic oppression#nurses#doctors#medical neglect#medblr#medical student#medical studies#medical malpractice
451 notes
·
View notes
Text
لا شئ يُعجبني .. أريد ان أموت 🤦🏻♀️
#mine#vsco#photooftheday#my own stuff#my details#studyblr#moments#study space#study tips#studying#medical studies#study#studyspiration#studystudystudy#studyspo#my stuff#study motivation#study blog#art study#coffeetime#coffeetime☕️
41 notes
·
View notes
Text
“And, of course, the atypical patient is anyone who’s not an anglo white man between the ages 35 to 60”
*Lecturer proceeds to roll eyes*
#medicine#med school#medblr#pharmacology#healtcare#research#data#medical studies#discrimination#pinned
138 notes
·
View notes
Text
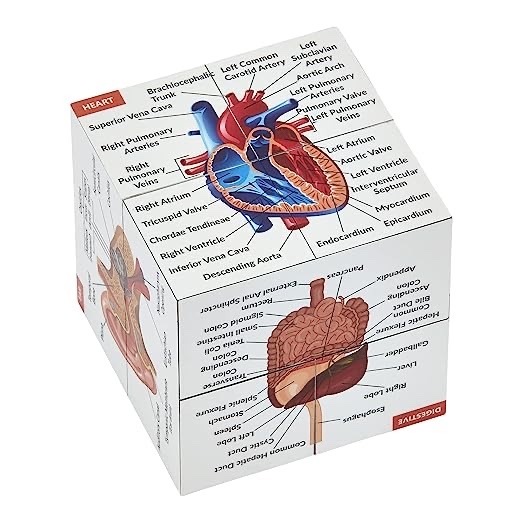
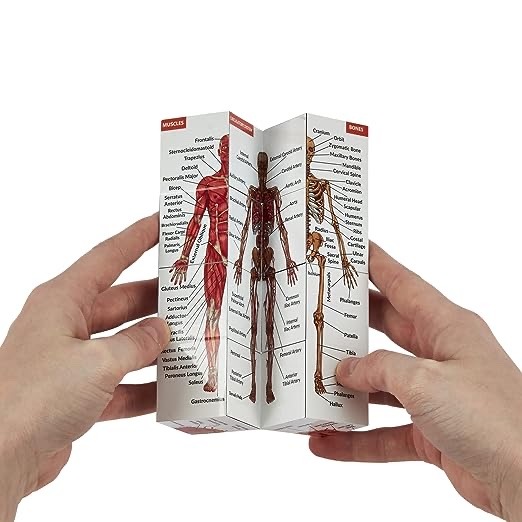
#amazon#amazon favorites#amazon finds#human anatomy#medical stuff#medical shit#medical school#medical studyblr#medical supplies#medical student#medical spa#medical studies#studystudystudy#study studyblr#studyinspo#study space#study aesthetic#study shows#studyabroad#study notes#study session#studyspo#studyblr#bible study#art study#amazon fashion#study stuff
47 notes
·
View notes
Text
Stumbles out of the examination hall covered in blood.
#Me during my annual exams#student#university#school#exam stress#exams#college#examinations#examination#exam#studying#final exams#studyblr#studystudystudy#exams suck#student life#medical student#medical studies#exams are killing me#academics#students of tumblr#students and student life#i hate exams#relevant#relatable#jokes#humor#lol#lmao yeah#seriously
171 notes
·
View notes
Text


When I entered this college, I became a "chill" kinda student. No planner... No schedule... Just go with the mood kinda studying.
It was okay till now... But hey! University exam is two weeks from now😈
I'll have to reactivate my machine-mode.
My goal for today is to complete the first revision of ABDOMEN (Anatomy) for 30 very important topics.
#study motivation#education#learning#students#studying#classroom#teaching#music#zoomester studyblr challenge#musicians#studyblr#indian studyblr#indian students#medical studies#motivation#motivasyon#inspiration
80 notes
·
View notes
Text












#randomized control trial#clinical trials#parachute use#parachute experiment#anti maskers#mask#medical studies#science#LOL#funny#religion is a mental illness
44 notes
·
View notes
Text
DUCK.
So I have a Ukrainian friend in the same uni but in the 1st year, and he said they have a project to do
"Genetical Tree" or something.
AND THEY HAVE TO KNOW ALL THE NAMES, DISEASES HISTORY, PLACE OF BIRTH AND DEATH ETC
IN ALL THE MEMBERS OF
FIVE
GENERATIONS
AT LEAST
???????PAKDJDJDKXJFJX??????
HOW TO TELL THE PROFESSORS ABOUT RUSSIAN OCCUPATION, NAZIS, HOLODOMOR, DESTRUCTION OF ARCHIVES, ETC???
"My grandpa had an inherited disease. A bullet in the heart. Inherited from nazis. Went right through his negative rezus factor".
"My grandma's disease environmental factors were Holodomor and GULAG. Maybe she had breast cancer. No one knows her real name and surname. No one knows where she was burried either."
At some point, everything you can tell about your ancestors is that they existed.
#medicine#medical student#ukraine#medical studies#genetics#bro my family was lucky because we do know the names of all the 5+ generations but JESUS#we just rely on our memory more than archives
10 notes
·
View notes
Video
Childbirth Is Deadlier for Black Families Even When They’re Rich, Expansive Study Finds
https://www.nytimes.com/interactive/2023/02/12/upshot/child-maternal-mortality-rich-poor.html
In the United States, the richest mothers and their newborns are the most likely to survive the year after childbirth — except when the family is Black, according to a groundbreaking new study of two million California births. The richest Black mothers and their babies are twice as likely to die as the richest white mothers and their babies.
Research has repeatedly shown that Black mothers and babies have the worst childbirth outcomes in the United States. But this study is novel because it’s the first of its size to show how the risks of childbirth vary by both race and parental income, and how Black families, regardless of their socioeconomic status, are disproportionately affected.
“This is a landmark paper, and what it makes really stark is how we are leaving one group of people way behind,” said Atheendar Venkataramani, a University of Pennsylvania economist who studies racial health disparities and was not involved in the research.
The study, published last month by the National Bureau of Economic Research, includes nearly all the infants born to first-time mothers from 2007 to 2016 in California, the state with the most annual births. For the first time, it combines income tax data with birth, death and hospitalization records and demographic data from the Census Bureau and the Social Security Administration, while protecting identities.
That approach also reveals that premature infants born to poor parents are more likely to die than those born into the richest families. Yet there is one group that doesn’t gain the same protection from being rich, the study finds: Black mothers and babies.
Are you a Black parent who recently gave birth? Tell us about it.
“It suggests that the well-documented Black-white gap in infant and maternal health that’s been discussed a lot in recent years is not just explained by differences in economic circumstances,” said Maya Rossin-Slater, an economist studying health policy at Stanford and an author of the study. “It suggests it’s much more structural.”
If anything, the study’s findings understate the dangers of childbirth in much of the United States, a variety of researchers said, because California’s maternal mortality rate has been declining over the last decade, as deaths have gone up in the rest of the country.
Rich Families Have More Premature Babies. But Those Babies Are Less Likely to Die.
Perhaps unexpectedly, babies born to the richest 20 percent of families are the least healthy, the study finds. They are more likely to be born premature and at a low birth weight, two key risk factors for medical complications early in life. This is because their mothers are more likely to be older and to have twins (which are more common with the use of fertility treatments), the researchers found.
But even with those early risk factors, these babies are the most likely to survive both their first month and first year of life.
A similar pattern emerged when it came to the health of the parents themselves: Rich and poor mothers were equally likely to have high-risk pregnancies, but the poor mothers were three times as likely to die — even within the same hospitals. Rich women’s pregnancies “are not only the riskiest, but also the most protected,” the paper’s authors wrote.
A pair of charts showing the relationship between a mother’s income and rates of premature births and infant mortality. The first chart shows that as a woman’s income rises, the likelihood of preterm birth rises. The second chart shows that as a woman’s income rises, rates of infant mortality fall.
This finding suggests that the American medical system has the ability to save many of the lives of babies with early health risks, but that those benefits can be out of reach for low-income families.
Resources outside the medical system also play a role. Separate research on children with leukemia, for example, has found that even when treated at the same hospital and using the same protocol, those from high-income families fared better than those from poorer families.
“It’s not just about the medical care that kids are receiving,” said Anna Aizer, a health economist at Brown University. “There are all sorts of other things that go into having healthy babies. If you’re a higher-income mom who can take time off work, who doesn’t have to worry about paying rent, it’s not surprising you’ll be able to manage any health complications better.”
Money Protects White Mothers and Babies. It Doesn’t Protect Black Ones.
The researchers found that maternal mortality rates were just as high among the highest-income Black women as among low-income white women. Infant mortality rates between the two groups were also similar.
Two charts showing the relationship between a mother’s income and rates of infant mortality by race. The first chart shows that as a Black mother’s income increases, the rate of infant mortality generally drops. The same is true in the second chart for white mothers, but at much lower rates than for Black women.
The richest Black women have infant mortality rates at about the same level as the poorest white women.
The babies born to the richest Black women (the top tenth of earners) tended to have more risk factors, including being born premature or underweight, than those born to the richest white mothers — and more than those born to the poorest white mothers. It’s evidence that the harm to Black mothers and their babies, regardless of socioeconomic status, begins before childbirth.
“As a Black infant, you’re starting off with worse health, even those born into these wealthy families,” said Sarah Miller, a health economist at the University of Michigan. She was an author of the study with Professor Rossin-Slater and Petra Persson of Stanford, Kate Kennedy-Moulton of Columbia, Laura Wherry of N.Y.U. and Gloria Aldana of the Census Bureau.
Black mothers and babies had worse outcomes than those who were Hispanic, Asian or white in all the health measures the researchers looked at: whether babies were born early or underweight; whether mothers had birth-related health problems like eclampsia or sepsis; and whether the babies and mothers died. There was not enough data to look at other populations, including Native Americans, but other research has shown that they face adverse outcomes nearing those of Black women and infants in childbirth.
Charts that show the relationship between a mother’s income by group. The groups are Hispanic mothers and Asian mothers. Generally, rates for Hispanic mothers and Asian mothers track more closely with those of white mothers than Black mothers.
Even before the new paper, research found that Black women with the most resources, as measured by education and class mobility, did not benefit during childbirth the way white women did. The new study demonstrates that disparities are not explained by income, age, marital status or country of birth. Rather, by showing that even rich Black mothers and babies have a disproportionately higher risk of death, the data suggests broader forces at play in the lives of Black mothers, Professor Rossin-Slater said.
“It’s not race, it’s racism,” said Tiffany L. Green, an economist focused on public health and obstetrics at the University of Wisconsin-Madison. “The data are quite clear that this isn’t about biology. This is about the environments where we live, where we work, where we play, where we sleep.”
There is clear evidence that Black patients experience racism in health care settings. In childbirth, mothers are treated differently and given different access to interventions. Black infants are more likely to survive if their doctors are Black. The experience of the tennis star Serena Williams — she had a pulmonary embolism after giving birth, yet said health care professionals did not address it at first — drew attention to how not even the most famous and wealthy Black women escape this pattern.
But this data shows how the effects of racism on childbirth start long before people arrive at the hospital, researchers across disciplines say, and continue after they leave. The stress of experiencing racism; air pollution in Black communities; and inequitable access to paid family leave, for example, have all been found to affect the health of mothers and babies.
“Even when it’s not about the direct disrespect that’s going on between the patient and the care provider, there are many ways systemic racism makes its way into the well-being of a pregnant or birthing person,” said Dr. Amanda P. Williams, the clinical innovation adviser at the California Maternal Quality Care Collaborative.
California Is a Best-Case Scenario. It Still Lags Behind Other Wealthy Parts of the World.
Many parts of the United States have much higher maternal mortality than California, and fewer policies to support families. California was the first state to offer paid family leave. It has one of the most generous public insurance programs for pregnant women. The state has invested in specific programs aimed at reducing maternal deaths and racial disparities in childbirth.
Yet even in this best-case American scenario, mothers and babies fare worse compared with another rich country the researchers examined: Sweden. At every income level, Swedish women have healthier babies. This held true for the highest-income Swedish women and those from disadvantaged populations, including low-income and immigrant mothers.
A pair of charts showing the relationship between birth outcomes in Sweden and California. The first chart shows that Swedish women have heavier babies at every income level. The second chart shows that Swedish women have lower rates of preterm birth than California women at every income level.
Swedish women have heavier babies at every income level ...
... and far lower instances of preterm birth.
In the United States, earning more regularly translates into superior access to the fastest, most expensive health care. But even with that advantage, the richest white Californians in this study still gave birth to less healthy babies than the richest Swedish women. Their newborns were more likely to be premature or underweight. The two groups had roughly equal maternal death rates.
“That finding really does strongly suggest that it’s something about the care model,” said Dr. Neel Shah, chief medical officer of Maven Clinic for women’s and family health and a visiting scientist at Harvard Medical School. “We have the technology, but the model of prenatal care in the United States hasn’t really gotten an update in the last century.”
A chart showing where the U.S. falls on the spectrum of maternal mortality among peer countries. The U.S. is last in a ranking that includes New Zealand, Norway, the Netherlands, Germany, Sweden, Switzerland, Australia, Britain, Canada and France, in that order.
Paper
Sweden, like most European countries, has universal health insurance with low out-of-pocket costs for the patient. Midwives deliver most babies in Sweden and provide most of the prenatal care, which has been linked to lower C-section rates and lower rates of preterm births and low birth weights. It has long paid leaves and subsidized child care.
Like California, Sweden has also started targeted efforts to reduce maternal deaths. When officials there recognized that African immigrants giving birth were dying more frequently, they began piloting a “culture doula” program, with doulas who were immigrants themselves helping pregnant women navigate the country’s health system.
Local maternal health programs could begin to help reduce racial disparities in the United States, too, as could a more diverse medical workforce, research suggests. Nonprofits and universities have experimented with ways to address racism and poverty, with programs like cash transfers for low-income pregnant women and initiatives to improve the environments of Black communities.
By the time a woman is pregnant, Professor Miller said, “it’s almost too late.”
“Health is going to depend on exposures throughout her life, health care she’s received, environmental factors,” she said. “A lot goes on prior to the pregnancy that affects the health of the mother and baby.”
About the data
The researchers collected birth certificate data for all babies born to first-time mothers in California from 2007 to 2016. The final sample included 1.96 million births. They collected hospitalization and death records for babies for one year from the California Department of Health Care Access and Information, as well as hospitalization records for mothers for nine months before the birth and a year after. They collected maternal death records for the same period from a Social Security Administration data set. They provided birth records to the Census Bureau, which assigned anonymous identification codes to access I.R.S. data and determine new parents’ incomes in the two years before the birth. (Infant mortality records were available only until 2012. Maternal mortality data covers a longer period than in government records, which generally include data for six weeks after a birth, and most likely capture some deaths unrelated to childbirth.)
In Sweden, the researchers collected similar health and mortality data from the National Board of Health and Welfare. The final sample included 463,865 births. Analogous maternal morbidity data was unavailable. They linked babies to their parents and collected parents’ demographic and financial data from Statistics Sweden. Sweden has a smaller gap between the highest and lowest earners than the United States.
#tiktok#article#new york times#Healthcare#Health Care#infant mortality#california#reproductive justice#reproductive freedom#reproductive rights#reproductive choice#reproductive health#health news#medical studies
106 notes
·
View notes
Text
01.08.2023
Welcoming August with a ´ Grasse matinée ´.
#studyblr#med school#studying#medstudyblr#summer#motivation#med student#exams#morning#studygram#medical studies#uni student#study tumblr#study motivation#medical students#study blog#undone bed#study in bed#ragdoll cat#cats of tumblr#my cat is cute#my cat#cat#my cat is adorable#cat on tumblr#medecine generale#coffee#morning coffee#self care#caturday
352 notes
·
View notes
Text
Some help for fellow Phlebotomy students!
This is the saying that helps me remember the order of draw for venipuncture:
Yellow (blood cultures)
Light (PT, PTT, Coagulation)
Stop (Chemistry testing)
Green (Any plasma test except plasma cells)
Light (Blood group, Carbon Monoxide levels, CBC)
Go (Glucose, Lactic acid, Blood alcohol levels)
And then these are the tubes and their functions!
Yellow tube:
Blood cultures
Invert 8-10x
Light blue tube:
PT
PTT
Coagulation studies.
Always draw two.
Invert 3-4x
Red, tiger, or gold tubes:
Chemistry testing
Electrolyte panel:
Bicarbonate, carbon dioxide, chloride, potassium, sodium
Basic metabolic panels:
Electrolyte panel, BUN, creatinine, glucose, calcium
Drug monitoring:
Digoxin, vancomycin, aminoglycosides, phenobarbital, phenytoin, valproic acid, methotrexate, lithium, theophylline
Comprehensive metabolic panel
Basic metabolic panel, hepatic function panel
Hepatic function panel
ALT, AST, Bilirubin, albumin, total proteins
Total cholesterol
HDL, LDL
Lipid panel
HDL, LDL, TG
Thyroid profile
T3, T4, TSH
Individual tests
Folic acid, Vitamin B12, HIV, hCG
Invert 5-6x
------------------------------------------------------------------------------
Capillary/Dermal Tubes:
Pink tube:
Blood bank studies
Rh typing
Pearl/white tube:
bDNA
Keep on ice.
Royal blue with purple or red stripe:
Toxicology
Heavy metal testing
Chain of custody.
Tan, royal blue (no stripe), or lavender:
Lead levels
Royal blue (plain):
Trace metal analysis.
Sodium Heparin
Pale yellow:
Compatibility for transplant
DNA & Paternity testing.
Chain of custody
ACD
Capillary/Dermal Tubes END
------------------------------------------------------------------------------
Dark or light green tubes:
Any plasma test EXCEPT plasma cells
C reactive protein for inflammation
Immunoglobin A measures antibodies and tests for autoimmune diseases
Liver enzymes
Bone marrow disorders
Serum HCG
Gets spun!
Lithium heparin
Sodium heparin (Dark green)
Ammonium Heparin
Invert 8-10x
Lavender tubes:
Blood group (ABO)
Carbon monoxide levels
CBC
Hemoglobin
Hematocrit
RBC
WBC
WBC w/ diff.
Platelets
Hemoglobin A1c
Rh typing
Sickle cell anemia
ANY blood cells
EDTA
Invert 8-10 times
Gray tubes:
Glucose
Glucose fasting and tolerance testing
Lactic acid
Do NOT use tourniquet
Patient does NOT need to make a fist
Blood alcohol levels:
DO NOT USE alcohol-based antiseptic
USE Chlorhexidine as an antiseptic.
Potassium Oxalate
Sodium Fluoride
Invert 8-10 times
Feel free to let me know if you have any questions, or if I missed something!! This is straight from my notebook, so it's highly likely that I missed something!
Have a wonderful day and stay safe!!
#phlebotomy#medical studies#studyblr#medical student#medical studyblr#medical stuff#order of draw#venipuncture
85 notes
·
View notes
Text


تمر أيام ثقيلة على روحِ الإنسان، يَصعب عليهِ قول كلمة واحدة، يرى كل أبواب الدُنيا مُغلقة أمامه، لا يعرف الوِجهة التي يُريدها، حتى يقول:
﴿رَبِّ اشْرَحْ لِي صَدْرِي، وَيَسِّرْ لِي أَمْر، وَاحْلُلْ عُقْدَةً مِّن لِّسَانِي، يَفْقَهُوا قَوْلِي، وَاجْعَل لِّي وَزِيرًا مِّنْ أَهْلِي﴾
تهون على المرء شدائدهِ، إنّه لطيف يقضي الهموم بقدرتهِ.
#muslim#muslim life#minimalist photography#minimalism#minimalstyle#todoist#today on tumblr#to do list#study notes#studentlife#study biology#study space#medical studies#my own stuff#study tips#studying#studyblr#studyspiration#mineblr#mine ❤️
18 notes
·
View notes
Text
#memes#meme#medical school#medicine#funny#medschool memes#medical student#medschool funny#humor#dank memes#medschool meme#medschool#medical studies#medstudent meme#medstudent problems#medical school funny#medical school meme#hospital memes#hospital meme#healthcare memes#healthcare meme
58 notes
·
View notes
Text
Story time!
Several years ago the Brazilian government did an extensive study on the health of its older citizens.
My eightysomething grandma participated in the study, and when I called her to say hi she started telling me about it. Her description of things went something like this:
When they were testing for senility and cognitive ability the nurse held up a ball and asked me what shape it was. And I was like "It's a sphere." and they were like "I would have accepted 'a circle' but that works too." And I was like "But it's NOT a circle, it's a sphere. Circles are two-dimensional and this is 3D. Get it right."
#my grandma#lol#brazil#health study#medical studies#brazilian government#the real life of me#i mean she's not wrong
8 notes
·
View notes
Text
How Adult Male Circumcision Improves Sexual Health

Adult male circumcision, the surgical removal of the foreskin from the penis, has been practiced for centuries for various reasons, including religious, cultural, and medical purposes. Beyond its traditional significance, research has increasingly highlighted the potential benefits of adult male circumcision for sexual health. In this article, we’ll explore the evidence-backed ways in which adult male circumcision can enhance sexual health and well-being.
Reduced Risk of Sexually Transmitted Infections (STIs):
One of the most compelling reasons cited for adult male circumcision is its role in reducing the risk of sexually transmitted infections (STIs), including HIV. Numerous studies have demonstrated that circumcised men are at lower risk of acquiring HIV, herpes simplex virus (HSV), human papillomavirus (HPV), and other STIs compared to uncircumcised men. This is believed to be due to the decreased surface area and moist environment under the foreskin, which can facilitate the transmission and replication of pathogens.
Lower Risk of Penile Cancer:

Adult male circumcision has also been associated with a reduced risk of penile cancer, a rare but serious condition that affects the tissues of the penis. The removal of the foreskin eliminates the moist and bacteria-prone environment that may contribute to the development of penile cancer. While penile cancer is relatively rare, circumcision offers a preventive measure that can lower the risk of this disease.
Improved Hygiene:
The removal of the foreskin through adult male circumcision simplifies genital hygiene and may reduce the risk of certain infections and irritations. Without the foreskin, it’s easier to clean the penis, as there are no folds or creases where bacteria and debris can accumulate. This improved hygiene can contribute to overall genital health and comfort, reducing the likelihood of unpleasant odors or infections.
Enhanced Sexual Satisfaction:
Some studies suggest that adult male circumcision may lead to increased sexual satisfaction and pleasure for both men and their partners. This is thought to be related to changes in penile sensitivity and sensation following circumcision. While individual experiences may vary, some men report heightened sexual sensitivity and improved erectile function after undergoing circumcision, which can positively impact sexual satisfaction and intimacy.
Reduction in Foreskin-Related Issues:
Uncircumcised men may experience foreskin-related issues such as phimosis (tight foreskin), paraphimosis (inability to retract the foreskin), or recurrent infections. Adult male circumcision can alleviate these problems by removing the foreskin entirely, eliminating the need for ongoing treatment or management of foreskin-related conditions. This can lead to improved genital comfort and function, enhancing overall sexual health and well-being.
Psychological Benefits:
In addition to the physical benefits, adult male circumcision may have psychological benefits for some individuals. For men who choose circumcision for personal or cultural reasons, undergoing the procedure can bring a sense of empowerment, confidence, and cultural identity. Feeling more comfortable and confident in one’s body can positively influence sexual self-esteem and relationships.
Conclusion:
Adult male circumcision offers several potential benefits for sexual health, including reduced risk of STIs, lower risk of penile cancer, improved hygiene, enhanced sexual satisfaction, resolution of foreskin-related issues, and psychological well-being. However, it’s important to note that circumcision is a personal decision, and individual experiences and preferences may vary. Before considering circumcision, it’s essential to consult with a healthcare provider to discuss the potential risks, benefits, and implications of the procedure. Ultimately, the decision to undergo adult male circumcision should be informed by careful consideration of one’s health, cultural beliefs, and personal preferences.
2 notes
·
View notes
Last Seen Blogs




