#mental-health-resources
Text

11K notes
·
View notes
Text

43K notes
·
View notes
Text
Sex and Disability
This Disability Pride Month, check out our series on Sex and Disability! This isn't meant to be a be-all-end-all guide to sex and disability because a) it's not, and b) there just can't ever be such a thing with any guide to sex. This series, much like your entire sexual life, is a work in progress and an endless, ongoing conversation. We hope this can be a good place for you to get started, and something that starts you on the path of good feelings about sex and your disability. Read the introduction above, or skip to one of the sections below:
Taking Your Body for a Ride: Masturbation and Disability
Disabled Sex: Sex for Two (or More)
Consent Is Sexy: Sexual Autonomy and Disability
Sex on the Brain: Sex and Autism, Mental Illness, and Other Cognitive Diversity
Your Body is Not a Sex Object: Devotees and Disability
Wheelchair, Bound? Kink and Disability
I Beg Your Pardon? Dealing with Rude Nondisableds
(Check out the rest of our disability-focused content here)
#disability#consent#sex ed#autism#mental health#mental illness#neurodivergent#disability pride month#resources
2K notes
·
View notes
Text
RPC self-care
We all get worn down by life and often we turn to RP for rejuvenation. But more than once I've seen people on here that find themselves burnt out on the RP community itself. With nearly 20 years of role playing under my belt, I thought I'd share some of my favourite self-care tricks.
Block people. You don't have to explain yourself and 'weird vibes' is a legitimate reason. You deserve to feel safe and unbothered in your hobby space, and RP is based on consent. Just like with any recreational activity, you can withdraw your consent at any time and no is a complete sentence.
Turn off anon. This prevents anonymous harassment and gives you great insight into who to block or report if you get non-anonymous harassment.
Drop threads. I know RP etiquette suggests you need to tell your RP partner when and why, and sure, if they ask politely you can give it a go - just know that a pre-written variant of 'not feeling it' is good enough. In my humble opinion, I think dropping boring or vexing threads is everyone's prerogative and doesn't require explanation. Again, no is a complete sentence.
Talk it out. If you like the thread but things took a turn you didn't like, it's time to bring the RP into the workshop. Something like 'Hey I really like our RP so far but I'm losing my spark, can we talk about course correcting where the plot is going?'
Make clear rules and revise them frequently. I'd also advise against spending said rules excusing or explaining why you don't like or want a certain thing - I cannot stress enough how your preferences are not up for debate.
Get comfy chasing. A lot of RP is about inviting others to play over and over and over. Rejection is a part of it. See if you can't find some element of self-care in it - taking rejection well is a great skill to practice in such a low stake environment.
Notice and celebrate the good stuff, instead of digging holes about the bad. Tell your co-players how great they are. Marvel at all the hard work you put into your muses and graphics. Admire your own blog.
Stop. Take a break. Check in with yourself. Do you actually need to face something in IRL? Do you need to rest? A snickers? A walk? Don't bother with posts á la 'offline for the day' - leave your options open to reduce guilt or shame if you want to poke your head back in.
Happy writing. 🌿
986 notes
·
View notes
Text
Struggling with self-compassion?
Recommended Reading:
Bluth, K. (2017). The Self-Compassion Workbook for Teens: Mindfulness and Compassion Skills to Overcome Self-Criticism and Embrace Who You Are. Oakland, CA: New Harbinger.
Brach, T. (2003) Radical Acceptance: Embracing your life with the heart of a Buddha. New York: Bantam.
Brach, T. (2020). Radical Compassion. NY: Penguin.
Brown, B. (2010). The Gifts of Imperfection. Center City, MN: Hazelden.
Desmond, T. (2015). Self-Compassion in Psychotherapy: Mindfulness-Based Practices for Healing and Transformation. Norton.
Germer, C. K. (2009). The mindful path to self-compassion: Freeing yourself from destructive thoughts and emotions. New York: Guilford Press.
Germer, C. K. & Neff, K. D. (2019). Teaching the Mindful Self-Compassion program: A guide for professionals. New York: Guilford Press.
Gilbert, P. (2009). The compassionate mind. London: Constable.
Hickman, S. (2021). Self-Compassion for Dummies. Hoboken, NJ: John Wiley.
Neff, K. D. & Germer, C. K (2018). The Mindful Self-Compassion workbook: A proven way to accept yourself, find inner strength, and thrive. New York: Guilford Press.
Neff, K. D. (2021). Fierce Self-Compassion: How Women Can Harness Kindness to Speak Up, Claim Their Power, and Thrive. New York: Harper Wave.
Neff, K. D. (2011). Self-Compassion: The proven power of being kind to yourself. New York: William Morrow.
Pollak, S. (2019). Self-Compassion for Parents: Nurture your child by caring for yourself. New York: Guildford Press.
Shapiro, S. (2020). Good Morning I Love You. Boulder, Sounds True.
Silberstein-Tirch, L. (2019) How to Be Nice to Yourself: The Everyday Guide to Self Compassion. San Antonio, TX: Althea Press
CHILDREN’S BOOKS
Beltzner, E. (2019). How to tame the tumbles: The mindful and compassionate way. Ontario: Mosaic Press.
Garcia, G. (2017). Listening with My Heart: A story of kindness and self-compassion. Gabi Garcia Books.
Marlowe, S. (2016). My new best friend. Summerville, MA: Wisdom Publications.
O’Leary, W. (2023). It’s OK: Being kind to yourself when things feel hard. Bala Kids.
Source
#q#mental health#recovery#resources#books#mental health books#reading#mental health reading#self compassion#self care#self love#mod misa#healing
270 notes
·
View notes
Text
in the depths of my mind is an ongoing territorial dispute between debilitating anxiety and hatsune miku
#they be at war#fighting for my attention like its a nonrenewable resource#doc speaks#vocaloid#hatsune miku#mental health
277 notes
·
View notes
Text
When you're vulnerable around the person you trust or love, I hope you aren't embarrassed about it after the fact. I hope you aren't embarrassed about the way you were vulnerable.
When my friends come to me in a vulnerable moment, I know I don't think about the way they look when they cry, or if their breathing is erratic, or how they say what they are saying. I think about the trust that goes into them exposing their heart like that. I think about the love that went into our friendship. Those superficial thoughts won't cross my mind because that isn't what matters. They are what matters. And that's what I mean. It's never embarrassing to look back on those moments because there was nothing but love under that pain.
The culture we live in shames us for being vulnerable. But we cannot be a stoic person all the time. Eventually, we will be vulnerable, and I hope you don't feel shame for that. Your loved ones won't love you less because you're a human person with human feelings. They love you because you're a human person with human feelings.
#mental health#mental health support#mental health advocacy#a friend of mine was vulnerable to me and the only thing i care about is that they EXPRESSED that pain#i don't care what their cry face looks like. that doesn't MATTER. they opened their heart up and we were there to comfort them.#that is what matters. even if we didn't have the resources to help them. they were there in the moment and they weren't okay#and it's OKAY to not be okay
2K notes
·
View notes
Text
WORDS TO USE INSTEAD OF NARCISSIST.
by @scaryinclusive.
presently, narcissist is a word used to define individuals with narcissistic personality disorder. a narcissistic individual is someone exhibiting traits or symptoms of narcissistic personality disorder. due to its widespread use as a derogatory, dehumanising and stigmatising label, despite its original purpose, the use of 'narcissist, narcissism and narcissistic' as an adjective, especially in an insulting, derogatory way, is ableist, sanist and stigmatising.
why should you consider altering your vocabulary and stop using words like 'narcissist' as an adjective — especially a derogatory one? please read this informative post. help the npd community out by opting to utilise less harmful, stigmatising language in your speech and writing! please note: the following words listed are not synonyms with or indicative of npd symptoms or traits. but for the context 'narcissist' is typically socially applied to, they are a beneficial replacement. feel free to reblog.
arrogant. an exaggerated sense of one's own worth or importance. this can come across as overbearing, or socially inappropriate.
selfish. very concentrated on one's own personal profit or pleasure, typically lacking consideration for others.
self-absorbed. preoccupied with one's own interests, feelings or situations.
boastful. excessive pride and self-satisfaction in one's own achievements, possessions or abilities.
braggart. same as above, just a synonym. relating more to bragging than boasting.
conceited. alternative for vain, excessively proud of oneself.
egotistical. excessively conceited or absorbed in oneself. a synonym for self-centred.
haughty. acting superior in an arrogant, disdainful way.
insolent. rude, arrogant, showing a lack of respect.
ostentatious. a pretentious or showy display, an attempt to impress.
overconfident. excessively confident, an excessive certainty in one's abilities.
proud. a deep pleasure or satisfaction gained from one's own achievements, qualities or possessions.
self-confident. trusting in one's abilities, qualities, and judgement.
self-important. an exaggerated sense of one's own value or importance.
superior. an overly high opinion of oneself. synonym for conceited.
vain. excessive high opinion of one's appearance, abilities or worth.
egocentric. thinking only of yourself, without regard for others' feelings or desires.
self-centred. preoccupied with oneself and one's affairs.
self-involved. preoccupied with oneself, not paying attention to anyone else.
smug. an excessive pride in oneself or one's achievements.
pompous. grand, self-important or solemn in a way that is insincere or pretentious.
self-serving. having concern for oneself and oneself only.
sycophant. someone who is too eager to praise or obey someone in order to gain an advantage.
complacent. smug or uncritical satisfaction with oneself or one's achievements.
vainglorious. overlay vain, excessively proud of oneself.
obnoxious. extremely unpleasant.
egoistic. relating to egoism, preoccupied with oneself, synonymous with self-centred.
callous. showing or having an insensitive or cruel disregard for others.
cruel. wilfully or deliberately causing pain / suffering to others, potentially with no remorse.
abusive / emotionally abusive. extremely offensive or insulting. a form of interaction wherein the abuser is psychologically controlling, manipulating or harming you.
manipulative. exercising control or influence over another individual or situation. can be intentional but equally can be subconscious.
self-righteous. a certainty, especially an unfounded one, that one is totally correct or morally superior.
unsympathetic. not expressing, showing or feeling sympathy towards others or a situation.
toxic. poisonous, very harmful or unpleasant in a way that is pervasive or insidious.
insidious. the proceeding of something in a gradual, subtle way, but with extremely harmful effects.
malignant. very dangerous or harmful.
#mental health awareness#writing resources#actuallynpd#npd safe#rp resources#resources.#writing resources.#npd related.#will probably do one for like... aspd and psychotic or smth#as someone who has removed a bunch of words from my vocab#it's not impossible and if you really want to care about everyone you make the effort
311 notes
·
View notes
Text
spotify playlists i made that i love:
for instantly inducing sadness and depression
for losing sight of what love means to you
for feeling present in the current moment
for deep-rooted loneliness
for the pure excitement of having a crush
for sleeping
for the person who left and would ruin you if they ever came back
for a love that rages like a fire
for your pride & prejudice hand flex moment
for feeling dreamy
for your radiohead fix
for crying while still bopping along
for drinking warm spiced milk on a rainy day
for feeling like you're an indie coming of age film
for the nostalgic emo phase
for feeling wretched
for when you're walking the streets of a new city by yourself
for daydreaming about moving to new york city with your best friends
for bangerz only
for wearing bold lipstick
for your bollywood fix
for allowing yourself to change
for feeling like you're floating on your back in a swimming pool at night in an indie movie
for your gracie abrams fix
for when you don't recognize yourself
for my desi diaspora kids
for my desi diaspora kids pt 2
for traveling and being present
for feeling like a smashed vase, or for smashing vases
for the jungle
for your james blake fix
for managing the aux cord
for feeling like the color orange, or perhaps the fruit. either one
for late night car rides surrounded by the open sky
for seeing the end of the world but smiling ridiculously
for your ridiculous bestie
for dying of love
for gradually falling into sleep
for your joji fix
for watching bright orange sunsets while hating yourself
for feeling the first warmth of summer hit you
for feeling like the weird kid in class again
for learning to live without the heartache it gives you
for playing breath of the wild
for realizing that romantic love will not be the thing that heals you
for whispering secrets to your best friend
for the kids who grew up on the internet
for love, or the lack thereof
for when you want to move to a new city but something is keeping you where you are
for your morning walk
for sitting in a field of marigolds
for beat drops that make you go feral
for traveling to see your best friends
for not allowing yourself to feel ridiculous anymore
for feeling like a perpetually open wound
for risk-taking
for your coke studio pakistan fix
for waiting for better days
for haunting
for being afraid that this is all there is
for texting them to get home safe
for falling in love in the summertime
for your hallmark movie main character moment
for your slowcore fix
for studying
for eating heartshaped jam cookies
for an espresso shot of joy
for feeling like an empty well that has nothing left to give
for love-filled days
for your ariana grande fix
for web-weaving
for your commute
for losing grip of your dreams
for setting this whole year on fire
for feeling like a pakistani uncle drinking chai on the porch
for isolation
for kicking anxiety in the face
#havent made one of these in a while hi#sound#journal#playlists#masterlist#spotify#music#self care#concept playlist#love#romance#mental health#positivity#playlist#spotify playlist#spotify playlists#resources
6K notes
·
View notes
Text




bonus:

Emotional Support Bestie comes along to first therapy appointment
#It doesnt work out because it would go like#Therapist: what's your earliest bad memory?#Fuyuhiko: if I told you I'd have to kill you.#But he tried it out and thats something <3#1st step as head of the yakuza: mental health resources on the payroll#A job for the Ultimate Counselor?#Super danganronpa 2#Danganronpa 2#super danganronpa goodbye despair#danganronpa summer camp#Fuyuhiko kuzuryu#Hajime hinata#Kuzuhina#2 of my closest friends are listed as my emergency contacts/ next of kin or whatever which is <3 to me
2K notes
·
View notes
Text
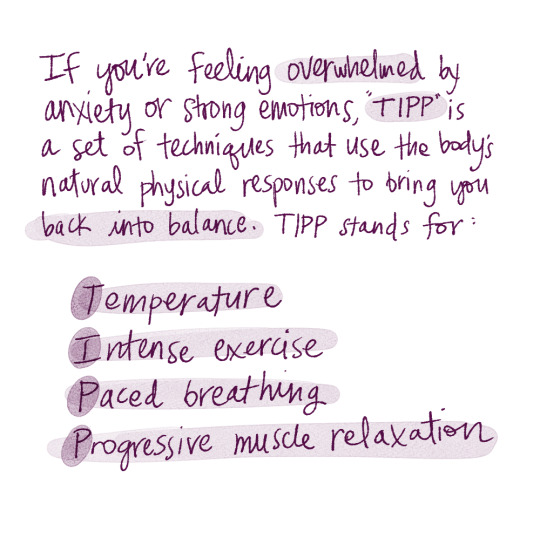
I was talking to my therapist about some anxiety symptoms --- "In my mind, I know I'm going to be perfectly okay, but my body doesn't listen and reacts anyway" --- and she recommended TIPP as strategies to keep in my toolbox of dealing with distress in the moment. I really appreciate having more than one option to try in moments of overwhelm!
Transcription below:
If you're feeling overwhelmed by anxiety or other strong emotions, TIPP is a set of techniques that use the body's natural physical responses to bring you back into balance.
TIPP stands for
temperature
intense exercise
paced breathing
progressive muscle relaxation
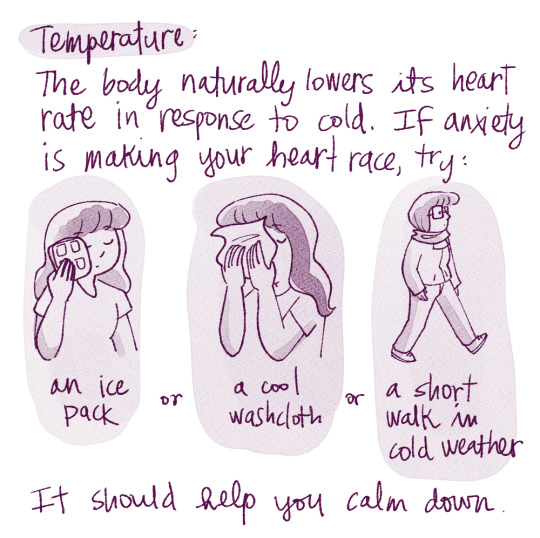
Temperature:
The body naturally lowers its heart rate in response to cold. If anxiety is making your heart race, try an ice pack, a cool washcloth, or a walk outside in cool weather, and it should help you calm down.
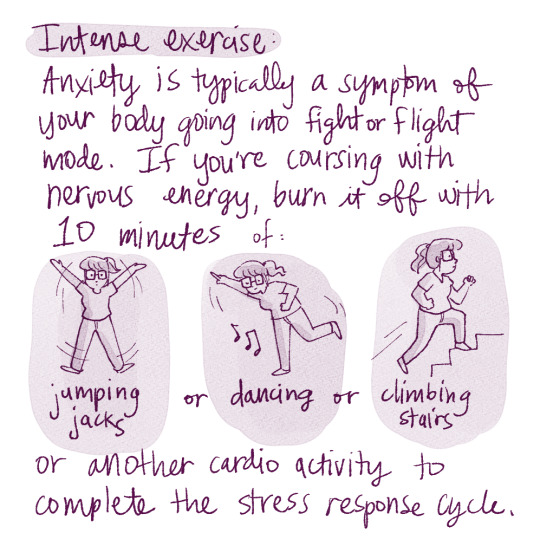
Intense exercise:
Anxiety is typically a symptom of your body going into fight/flight mode. If your body is coursing with nervous energy, burn it off with 10 minutes of jumping jacks, dancing, climbing stairs, or another cardio activity to complete the stress response cycle.
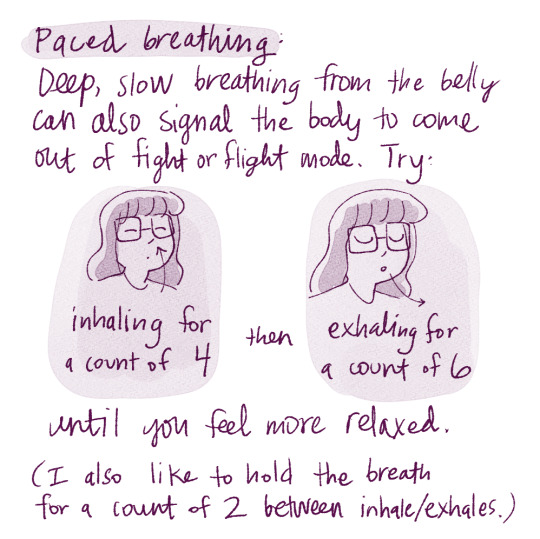
Paced breathing:
Deep, slow breathing from the belly can also help signal the body to come out of fight/flight mode. Try inhaling for a count of four and exhaling for a count of six until you feel more relaxed. (I like to hold the breath for a count of two between each inhale and exhale.)
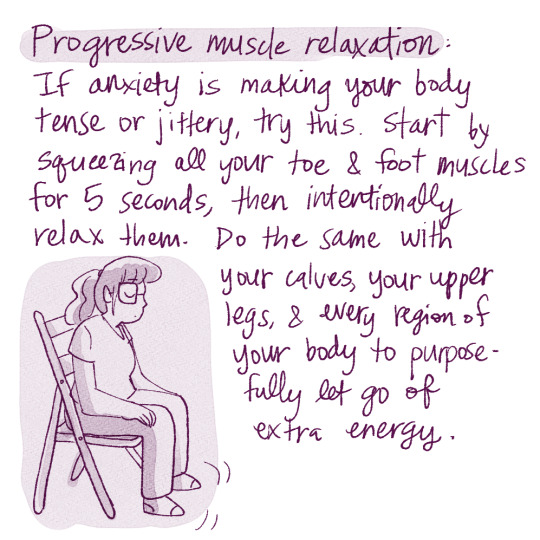
Progressive muscle relaxation:
If anxiety makes your body tense up, try this. Start by squeezing the muscles in your toes and feet for five seconds, and then intentionally relax them. Move up to the calves, up your legs, and every region of your body to purposefully let go of extra energy.
When you're feeling overwhelmed, try one or more of these to see what works for you.
#self-care sunday#self-care#anxiety#anxiety relief#managing anxiety#dbt#tipp#mental health#mental health resources#stress
8K notes
·
View notes
Text
As a Gévaudan Lycan, June’s design is supposed to give off an unknowable and melancholy energy.
Gévaudan Lycans are mimics, and their emotions alter their form, especially if they have little to no control of themselves when they shift.

The way June was changed into a lycan and her experience during first shift were extremely traumatic, and over time, her lycan form reflected her feelings of loss and self-loathing. She fronts as this charming and confident woman, while holding back her deeper emotions that eventually leached into the form that reflects her true self.



Fear, sadness, loss, and rage all mixed into this one entity she cannot control. Once a month, she's forced into facing all of those emotions, reliving that trauma again and again for nearly 30 years.
#so when people say they like her design#it makes me so so happy#I put lot of thought into it#as I really wanted to reflect a top very near and dear to my heart#which is the lack of access and resources for black women (especially queer black women) for mental health#there's this kind of cultural thing#where your hairstylist is also your therapist#and June’s design and lore is a reference to that culture#all these hardworking women in the community who will just be TALKING about their experiences at hair salons#it's cathartic but also like#it happens because of how little professional help is available and accessible for the community#anyway June is a big sad cryptid werewolf and needs to not be sad :[#she can still be a big cryptid werewolf but she needs lycantherapy#june kingston#strawberry moon
406 notes
·
View notes
Text
before people start posting shit like ‘euphoria needs to be cancelled now’ please remember that this is the death of a human being you’re talking about, so don’t reduce his life or passing to the role he played in a TV show. that’s not what this should be about or the discussion that needs to be had.
#angus cloud#like i get the perspective i do#but the first thing we need to be talking about is mental health and mental health resources#the top comments under the post announcing his death were about fezco and not angus himself#which just feels off and somewhat wrong to me#anyway. i hope he rests in peace
467 notes
·
View notes
Text

having lyrics addressing how mental health is just completely dismissed coupled with all that religious imagery in the staging hits incredibly hard when the cultural mindset in serbia is one of "mental illness isnt real you just need to go to church"
#eurovision#in corpore sano#when i told one of my closest friends about my autism diagnosis her response was#'autism doesnt exist in serbia because we tell ppl to go to church and god helps fix their psyche'#and that 'in the west its different because they dont trust god'#if you have a problem that isnt physical it just means u arent believing in god hard enough#and with how few mental health resources are even available faith kinda does become the only solution#like i shit on england a lot but as an autistic person with adhd and anxiety im SO GLAD i only lived in belgrade for a few years#quasigh
8K notes
·
View notes
Text
CALLING ALL PPL WHO STRUGGLE TO KEEP A CALENDAR!
I used to keep a bullet journal years ago but I completely fell off it once COVID began. Since then, I have had no calendar to keep my life together.
As someone with ADHD, a calendar would help me stay sane, but every time I tried to get back into it, no matter what I tried, it never stuck. Therefore, my life was a mess.
But while reading a Webtoon (called "30 Minutes With You" if you're interested, it's really wholesome) the main character does daily doodles in her pocket calendar, and then it clicked.
I've been doing daily little doodles in my pocket calendar and I've generally kept up for two months now! Overall, it's been really fun AND has kept me more put together!
Here is an example:
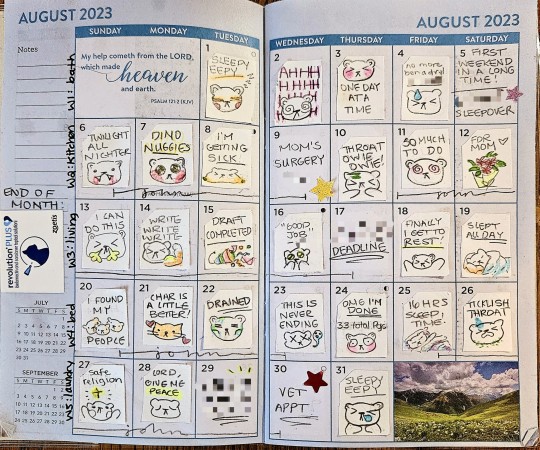
You can get a pocket calendar from Dollar Tree for $1.25 (if you're in the US and Canada)! I use blank office labels cut into the right size as the white squares I draw on just because it looks better.
This has also really helped my memory, because once stuff happens my brain forgets it immediately. It really makes me feel like my life is fuller and it's been easier to look back and see how far I've come!
Hope it helps! 💛
#pocket calendar doodles#actuallyadhd#adult adhd#actually adhd#adhd problems#adhd#neurodivergent#executive dysfunction#forgetfulness#brain fog#mental health#memory problems#memory#accomodations#resources#calendar#bullet journal#bujo#i know its not a bujo but its an alternative for ppl who struggle to keep one!#if the blurring out text is not a great safeguard PLS LET ME KNOW 😘 im not knowledgeable about that stuff#mine
264 notes
·
View notes
Text
Writing Mental Health With Compassion
I've gotten a few questions regarding depicting characters with mental health challenges and conditions and I wanted to expand a little more on how to depict these characters with compassion for the real communities represented by these characters.
A little about this guide: this is, as always, coming from a place of love and respect for the writing community and the groups affected by this topic at large. I'm also not coming at this from the outside, I have certain mental illnesses that affect my daily life. With that, I'll say that my perspective may be biased, and as with all writing advice, you should think critically about what is being told to you and how.
So let's get started!
Research
I'm sure we're all tired of hearing the phrase "do your research," but unfortunately it is incredibly important advice. I have a guide that touches on how to do research here, if you need a place to get started.
When researching a mental health condition that we do not experience, we need to do so critically, and most importantly, compassionately. While your characters are not people, they are assigned traits that real people do have, and so your depiction of these traits can have an impact on people who face these conditions themselves.
I've found that reddit is a decent resource for finding threads of people talking about their personal experiences with certain illnesses. For example, bipolar disorder has several subreddits that have very open and candid discussions about bipolar, how it impacts lives, and small things that people who don't have bipolar don't tend to think about.
It's important to note that these spaces are not for you. They are spaces for people to talk about their experiences in a place without judgment or fear or stigma. These are not places for people to give out writing advice. Do NOT flood subreddits for people seeking support with questions that may make others feel like an object to be studied. It's not cool or fair to them for writers to enter their space and start asking questions when they're focused on getting support. Be courteous of the people around you.
Diagnosis
I have the belief that for most stories, a diagnosis for your characters is unnecessary. I have a few reasons for thinking this way.
Firstly, mental health diagnoses are important for treatment, but they're also a giant sign written across your medical documents that says, “I'm crazy!” Doctors may try to remain unbiased when they see mental health diagnoses, but anybody with a diagnosis can say that doctors rarely succeed. This translates to a lot of people never getting diagnoses, never seeking treatment, or refusing to talk about their diagnosis if they do have one.
Secondly, I've seen posts discuss “therapy speak” in fiction, and this is one of those instances where a diagnosis and extensive research may make you vulnerable to it. People don't tend to discuss their diagnoses freely and they certainly don't tend to attribute their behaviors as symptoms.
Finally, this puts you, the writer, into a position where you treat your characters less like people and story devices and more like a list of symptoms and behavioral quirks. First and foremost, your characters serve your story. If they don't feel like people then your characters may fall flat. When it comes to mental illness in characters, the people aspect is the most important part. Mentally ill people are people, not symptoms.
Those are my top three reasons for believing that most characters will never need a specific diagnosis. You will likely never need to depict the difference between bipolar and borderline because the story itself does not need that distinction or to reveal a diagnosis at all. I feel that having a diagnosis in mind for a character has more pitfalls than advantages.
How does treatment work?
Treating mental health conditions may appear in your story. There are a number of ways treatments affect daily life and understanding the levels of care and what those levels treat will help you depict the appropriate settings for your characters.
The levels of care range from minimally restrictive and minimal care to intensive in-patient care in a secure hospital setting.
Regular or semi-regular therapy is considered outpatient care. This is generally the least restrictive. Your characters may or may not also take medications, in which case they may also see a psychiatrist to prescribe those medications. There is a difference between therapists, psychiatrists, and psychologists. Therapists do not prescribe medications, psychiatrists prescribe medications after an evaluation, and psychologists will (sometimes) do both. (I'm US, so this may work differently depending where you are. You should always research the specific setting of your story.) Generally, a person with a mental illness or mental health condition will see both an outpatient therapist and an outpatient psychiatrist for their general continuing care.
Therapists will see their patients anywhere from once in a while as-needed to twice weekly. Psychiatrists will see new patients every few weeks until they report stabilizing results, and then they will move to maintenance check-ins every 90-ish days.
If the patient reports severe symptoms, or worsening symptoms, they will be moved up to more intensive care, also known as IOP (Intensive Outpatient Program). This is usually a group-therapy setting for between 3-7 hours per day between 3-5 days a week. The group-therapy is led by a Licensed Professional Counselor (LPC) or Licensed Professional Social Worker (LPSW). Groups are structured sessions with multiple patients teaching coping mechanisms and focusing on treatment adjustment. IOP’s tend to expect patients to see their own outpatient psychiatrist, but I've encountered programs that have their own in-house psychiatrists.
If the patient still worsens, or is otherwise needing more intensive care, they'll move up to PHP (Partial Hospitalization Program). This can look different per facility, but I've seen them to be more intensive in hours and content than IOP. They also usually have in-house psychiatrists doing diagnostic psychological evaluations. It's very possible for characters with “mild” symptoms to go long periods of time, even most of their lives, without having had a diagnosis. PHP’s tend to need a diagnosis so that they can address specific concerns and help educate the patient on their condition and how it may manifest.
Next step up is residential care. Residential care is a boarding hospital setting. Patients live in the hospital and focus entirely on treatment. Individual programs may differ in what's allowed in, how much contact the patients are allowed to have, and what the treatment focus is. Residential programs are often utilized for addiction recovery. Good residential programs will care about the basis for the addiction, such as underlying mental health issues that the patient may be self-medicating for. Your character may come away with a diagnosis, or they may not. Residential programs aren't exclusively for addictions though, and can be useful for severe behavioral concerns in teenagers or any number of other concerns a patient may have that manifest chronically but do not require intensive inpatient restriction.
Inpatient hospital stays are the highest level of care, and this tends to be what people are talking about when they tell jokes about “grippy socks.” These programs are inside the hospital and patients are highly restricted on what they can and cannot have, they cannot leave unless approved by the hospital staff (the hospital's psychiatrist tends to have the final say), and contact with the outside world is highly regulated. During the days, there are group therapy sessions and activities structured very carefully to maintain routine. Staff will regulate patient hygiene, food and sleep routines, and alone time.
Inpatient hospital programs are controversial among people with mental illness and mental health concerns. I find that they have use, but they are also not an easy or first step to take when dealing with a mental health condition. Patients are not allowed sharp objects, metal objects, shoelaces, cutlery, and pens or pencils. Visitors are not allowed to bring these items in, staff are not allowed these items either. This is for the safety of the patients. Typically, if someone is involuntarily admitted into the inpatient hospital program, it is due to an authority (the hospital staff) deeming the patient as a danger to themselves or others. Whether they came in of their own will (voluntary) or not does not matter in how the program operates. Everyone is treated the same. If someone is an active danger to themselves, then they may be on 24-hour suicide watch. They are not allowed to have any time alone. No, not even for the bathroom, or while sleeping, or during group sessions.
Inpatient Hospital Programs
This is a place of high curiosity for those who have never been admitted into inpatient care, so I'd like to explain a little more in detail how these programs work, why they're controversial, but how they can be useful in certain situations. I do have personal experience in this area, but as always, your mileage may vary.
When admitting, hospital staff are the final say. Not the police. The police hold some sway, but most often, if someone is brought in by the police, they are likely to be admitted. They are only involuntarily admitted when the situation demands: the staff have determined the person to be an imminent danger to themselves or others. This is obviously subjective, and can easily be abused. A good program with decent staff will do everything they can to convince the patient to admit voluntarily if they feel it is necessary, but ultimately if the patient declines and the staff don't feel they can make the clinical argument that admittance is necessary, the patient is free to leave. It should be noted that doctors and clinicians have to worry about possibly losing their licenses to practice. They don't want to fuck around with involuntary admittance if they don't have to, and they don't want potentially dangerous people to walk away.
Once admitted, the patient will have to remove their clothing and put on a set of hospital scrubs. These are mostly made of paper, and most often do not have pockets, but I have seen sets that do have pockets (very handy, tbh). They are not allowed to take anything into the hospital wing except disability-required devices such as glasses, hearing aids, mobility aids, etc. Most programs will require removing piercings, but not all of them, in my experience.
The nurses will also do a physical examination, where they will make note of any open wounds, major scars, tattoos, and other skin abrasions that may be relevant.
The patient will then be led to their bed, where they will receive any approved clothing items from outside, a copy of their patient rights, and a copy of the floor code of conduct and rules, a schedule, and any other administrative information necessary for the program to run efficiently and legally.
Group sessions include group-therapy, activities, coping skills, anger management, anxiety management, and for some reason, karaoke. There is a lot of coloring involved, but only with crayons. A good program will focus heavily on skills and therapeutic activities. Bad programs will phone it in and focus on karaoke and activities. Most hospitals will have a chaplain, and some will include a religious group session. I've never attended these, so I can't speak for them.
Unspoken rules are the hidden pieces of the inpatient programs that patients tend to find out during their first visit. There is no leaving the program until the doctor agrees to it. The doctor will only agree to it if they deem you ready to leave, and you are only ready to leave if you have been compliant to treatment and have seen positive results in the most dangerous symptoms (homicidal or suicidal ideations). Noncompliance can look like: refusing your prescribed medications (which you have the right to do at any time for any reason. That does not mean that there won't be consequences. This is a particularly controversial point.), refusing to attend groups (chapel is not included in this point, but that doesn't mean it's actually discounted. Another controversial point.), violent or disruptive outbursts such as yelling or throwing things, and refusing to sleep or eat at the approved and appointed times. All of this may sound like the hospital is restricting your rights beyond reason, but I've seen the use, and I've seen the abuse. Medications are sometimes necessary, and often patients seriously prefer having medication. Groups are important to a person's treatment, and refusing to go can be a sign of noncompliance or worsening symptoms. If someone is too depressed or anxious to go to group, then they're probably not ready to leave the hospital where the structure is gone and they must self-regulate their treatment. Violent or disruptive outbursts tend to be a sign of worsening symptoms in general, but even the best of us lose our tempers from time to time when put into a highly stressful situation like an inpatient hospital stay. The hospital is supposed to be a place of healing, for many it is. But for many more, it is a place of systematic abuse and restriction.
Discharge processes can be long and arduous and INCREDIBLY stressful for the patient. Oftentimes, they won't know their discharge date until the day of, or perhaps the day before. Though the date can change at any time. The discharge process requires the supervising psychiatrist to meet with the treatment team and then the patient to determine if the patient had progressed enough to be safely discharged. Discharge also requires a set outpatient plan in place, such as a therapy appointment within a week, a psychiatrist visit, or admittance into a lower level of care. This is where social workers are involved. Patients are not allowed access to cell phones or the internet. They cannot make their own appointments with their outpatient care providers without a phone number and phone access. Some floors will have phone access for this reason, others will insist the social worker arrange appointments and discharge plans. Social workers are often incredibly overworked, with several patients on their caseload.
The patient cannot be discharged until the social worker has coordinated the discharge plan to the doctor's approval. Most often, unfortunately, the patient rarely receives regular communication regarding the progress of their discharge. I've been discharged with as much as a day's notice to two hours notice.
Part 2 Coming Soon
This guide got longer than expected! Out of respect for my followers dashboard, I will be cutting it here and adding a Part 2 later on.
If you find that there are more specific questions you'd like answered, or topics you'd like covered, send an ask or reply to this post with what you'd like to see in Part 2.
– Indy
#writing advice#writing tips#writing resources#writeblr#amwriting#asktheprose#ask the prose#writing mental health#mental health#writing with compassion#writing mental illness#writing compassionately
121 notes
·
View notes
Last Seen Blogs

akiyoyamashita
Akiyo Yamashita Illustration
ldbrilliant
Brilliant

bribgitte
Æncrée ⚓

inaztogata
🎄InazTogata🎄

balicipisi
Nevi Şahsına Münhasır