#occipital nerve block
Text
0 notes
Text
Vicodin this, Vicodin that. House needed a) a syringe full of lidocaine to jam into that bitch of a muscle at all times and b) a good old fashioned rhizotomy. As someone who has started managing my migraines with lidocaine, VERY successfully, I am a firm believer that nerve blocks are the shit.
#get a professional to do your greater occipital nerve block#don’t do it at home#you can’t get the angle right#and lidocaine in injectable form isn’t over the counter
160 notes
·
View notes
Text
The Headache That Keeps Marching On
We’re on day 11 of having a headache on the right-hand side of my head. It does not respond to ibuprofen, naproxen, paracetamol, or diclofenac. Just my luck. The only thing that seems to be having any effect is the pregabalin my psychiatrist prescribed.
#headache#day 11#pregabalin#naproxen#paracetamol#diclofenac#ibuprofen#occipital#MRI#nerve block#where is my mind
2 notes
·
View notes
Text
Literally fuck male doctors
How many doctors have I seen this year??? Like 5??? And I just saw the fifth one and I picked a woman on purpose and thank GOD because I’m finally getting some goddamn help. I mean okay to be fair she’s only the second neurologist I saw but the difference between her and the dude is night and day. Basically here’s how it went.
Me to each doctor: hi doctor, I’m having these symptoms and also I have occipital neuralgia and here’s why I think that.
Dick doctor: you are young and healthy and there is nothing wrong with you
Lady doc: yes it appears you actually have migraines and yes you are correct about the occipital neuralgia and you also possibly have glossopharyngeal neuralgia and here are all of the things we are going to do to make you feel better oh and also one of our graduates just moved to Georgia so you might be able to see her when you move
AND YET I SUFFERED
ALL BECAUSE THAT DICK DOCTOR WOULDNT EVEN LISTEN TO ME OR ENTERTAIN THAT I KNEW THE PAIN I WAS FEELING
#we are increasing topamax dosage#and getting a muscle relaxer#and some kind of migraine medicine#and occipital nerve blocks#personal#I’m legit so excited for these occipital nerve blocks#I’ve been waiting for these for MONTHS
1 note
·
View note
Text
Also I'm 99.9% sure my occipital nerve blocks did not work and I that also makes me want to cry.
Holding onto that 0.1% that they start working in the next few days, even though it's been over a month since I've had them done & had relief for an entire week before the pain came back.
#this has never happened#they always work#occipital neuralgia#nerve block#chronic illness#spoonie#invisible illness#chronic pain
1 note
·
View note
Text
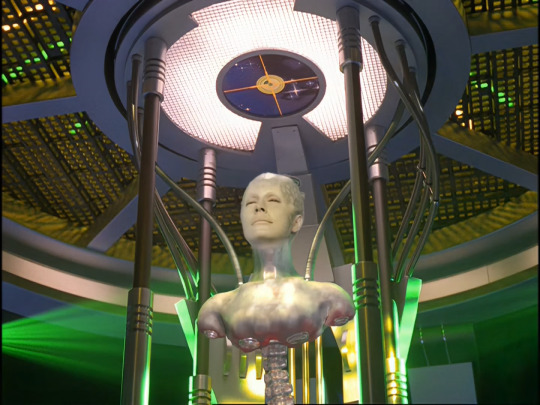
Repeating on a theme on Seven's Borg implants (read here for previous posts)
Because I'm still obsessed with Seven's Borg tech and how much of her is organic. Supposedly EMH took out 82% of Seven's Borg tech and took out many over the years Seven still has a lot of working Borg tech and nanoprobes more than other xB around.
One thing I just noticed from Equinox, part 2 is how we see Seven's ocular implant without the casing:

This is where it makes it so obvious that Seven's head is mostly metal because that is a skin cut out showing what's underneath that skin. Also that there are various lights under there we didn't know about.


Look at how shiny Seven's metallic skull is without skin.

The configuration of Seven's head is mostly just metal.
In this Picard s2 prop - this Borg skull only has a fraction of what Seven has underneath her skin:

Seven's entire cranium is made of metal.
That is why when Narissa bashed Seven's head on the console Seven didn’t lose consciousness and only made Seven a little dizzy, and pissed her off more tbh.
An organic person would've had a concussion and maybe even died.
I wonder if Seven looks like a Terminator beneath the skin.
(This is brought to you by having just rewatched Terminator 1 & 2).
Because as we saw in Imperfections scratch the skin underneath and she seems to have metal exoskeleton as implants.

Speaking of further body horror-- Even when the Borg deadened Seven’s nerve endings, Seven still felt the pain of having her occipital ocular installed:
During or after her procedure, even with all the precautions that the body wouldn't feel a thing, Seven remembered feeling the pain. (It makes me wonder if Unimatrix!Annika felt the pain or it was something she could block out).
A fan theory I subscribe to posited that Seven is a Borg Queen candidate.
This would go a long way explaining why Seven has some form of individual identity and why the Borg Queen has a special interest re: Seven.
Aside from being assimilated at a young age, this would also account for the number of implants in her system.
Even among her own unimatrix, she was the one calling the shots and enforcing the Borg rules.
All the Borg Queens we've seen only have their heads and upper torso.

Seven might have been on her way to a similar fate. Her spine's already reinforced.

I'm pretty sure one or both of Seven's legs from the knee down are prosthetic legs ala Edward Elric.
(Also there was a VOY writer who seemed keen on blowing up Seven's legs -- the first version of The Raven has Seven becoming a terminator and to stop her the crew apparently needed to blow up her legs, and she had to crawl her way to Janeway—thankfully someone in the writer’s room said “WTF??”, Because WTF???I'm so glad someone went: No, dude).
As possible evidence that one or both of Seven’s legs are prosthetics: when she was unconscious during The Gift we can see there are wires on Seven's left kneecap.
And I don't know if that shin armor is exoplating or if prostheses have replaced her legs.
There's so much about Seven we don't really know about and I really want to know more about her functional Borg components and to settle, once and for all, if by Picard's time, she still needs to regenerate.
I'm on the camp that Seven still needs to regenerate.
/edited
#body horror#body of borg#seven of nine#star trek#star trek voyager#dhawan!master would love the borg too much#the borg collective#star trek picard
47 notes
·
View notes
Text
Neurology appointment was once again a mixed bag. Long story short I actually have occipital neuralgia, not regular migraines, but she didn't actually give me any treatment options and just told me to lose more weight. Full rant under the cut.
But yeah she looked at my CT scan and said she doesn't see any signs that my intracranial hypertension is being caused by my cervical spine alignment compressing anything, which is kinda a bummer bcs thats what I hoped was going on, but alas I guess I will have to continue to pray something gives and we can figure out what's causing it bcs despite being on a very high dose of the medication used to treat the condition for like 4 years and losing 20lbs nothing has gotten better or worse.
Aside from that it does seem like I probably don't actually have generic migraines, I have occipital neuralgia. Which would explain why all of the different migraine medications I'm on have done fuck all to actually help and why my migraine-like symptoms don't 100% line up with typical migraines(no auras, very little sound sensitivity/moderate light sensitivity, they last for days if not weeks, are extremely resistaint to treatment, even when they do respond half the time they just come back within a few days or so, I don't have any noticeable triggers aside from lack of sleep, ect.).
The only problem with that is I can't get another nerve block bcs of the steroid issue, and when I asked her what my other treatment options were she just said "well do it without the steroids then" and didn't let me get a word in edgewise about how my pain doctor said he wouldn't do it without steroids and I know just the lidocaine will wear off within 3-4 hours anyway so how would that help outside of diagnostics(which I no longer need) BUT she did refer me back to my previous pain clinic so I am simply going to ask them to help with this bcs they have a great track record of actually finding alternative treatments for my pain when the usual stuff isn't an option. But still, it's so fucking annoying bcs I did a LOT of research about this once the nerve block worked and there are TONS of other fucking treatments. Just...such bullshit.
Sadly she also told me to lose more weight, bcs she's super convinced me being under 130lbs will magically fix my hypertension despite the fact that I've done my research and about 10-15% of your body mass is the recommended ammount to lose that apparently sends it into remission in almost every case, but I've lost about that much and it didn't do anything at all. So like, idk ma'am I don't think knocking another 3lbs off is going to do jack shit, but whatever I guess.
I'm seeing my primary in a few weeks and at this point I'm demanding a new neurologist. But in the meantime I at least never have to see that fucking pain specialist again and instead can go back to my old one that didn't suck and I'll count that as a win.
12 notes
·
View notes
Text
Villain Or Victim, Chapter 5

For the following few nights, Loki continued to take Echo out of her cell without anyone else knowing. Aside from Thor, who had given up on telling Loki how bad of an idea it was.
Usually, Loki took her up onto the roof, which seemed to be her favourite place. He did take her for a walk around the grounds too, which she seemed to enjoy.
But tonight, he had something different in mind. After taking her up onto the roof again for a little while, he suggested something else.
‘How would you like to use up some energy in the training field?’ Loki asked her while rubbing her arm. They were sitting close together on the rooftop and he had his arm around her.
‘Would that be ok?’ She asked quietly.
‘Of course. I know you will likely still feel trapped and cooped up. I thought perhaps doing some training of your skills will help, might help you sleep better too.’
Echo had been struggling to sleep well, and she had told Loki that yesterday. It probably was partly due to not doing much during the day, not getting the same exercise like she normally did.
‘That would be great… Thank you, Loki.’ She smiled at him.
Loki took her hand and gave her a gentle squeeze, he led her back down and outside to the field.
He watched from the side as she ran laps around the perimeter first, not quite at her full speed but still an impressive speed none the less. Then she impressed him with some fighting techniques on the robot trainers that Stark had invented. They kept popping up around her but she was able to take them all down with various kicks or punches. She was really agile and light on her feet, which Loki hadn’t noticed previously when they’d been originally fighting her.
He tapped his lip in deep thought while he continued watching her.
‘She has so much potential.’ He hummed quietly to himself.
-
The Avengers were all having their daily meeting to speak about Echo. They got updates from Loki about how she was doing with him, if she was opening up more and if she had told him anymore information that could be useful.
Bruce and Tony would update everyone about their progress in the lab. And there was some…
‘I think, if we can make a serum… a form of nerve block, so to speak, we can perhaps stop her outbursts. We now know the issue is coming from her occipital nerve, so we just need to come up with a solution that will last long enough to block it. Even if we need to administer it monthly, that would be better than nothing.’ Bruce said.
They had been able to work with Echo and she had been letting them run some tests. Including many brain scans to pinpoint where the issue was coming from. She had only been able to allow them to do said tests with Loki’s support though of course.
Though they did need to enrage her on purpose a few times, so they could see her brain in action, which had been relatively easy to do.
‘How long will it take to make this serum?’ Loki queried.
Bruce hummed for a moment in thought. ‘Not sure. It might take a few attempts, but I’d be hopeful within a few weeks we will have the right solution.’
‘I think we can probably do it in about ten days.’ Tony interjected.
‘That soon?’ Loki asked, keeping his tone casual though he was surprised to hear it could be so soon.
‘It shouldn’t be too difficult. We will need to take a few more samples from her, but it will be straight forward enough.’ Tony shrugged.
Loki nodded once. ‘Good.’
He then kept quiet for the rest of the duration of the meeting. He just listened to plans the team came up with, while also forming a plan of his own for Echo. Though he wasn’t going to have as much time now as he had originally thought he would.
Even though he had her trust, he still wasn’t entirely sure how far that trust would go yet.
-
‘Are the team any closer to finding a solution for me?’ Echo asked Loki that night, he was in her cell spending some time with her. He had pulled her onto his lap to cuddle, knowing how much she liked that. Especially when he stroked her hair, it was so soothing for her.
‘Not yet, but they are working hard on it. Between missions they’re in the lab trying to find one.’
‘Do you think it will ever be possible for me to live a normal life? To not have to be caged up constantly?’ She asked.
Loki gently cupped her face and rubbed his thumb against her cheek. ‘You’re not a danger to me, so that’s a big start. It proves it can be done.’
‘I just… want to be normal. I hate being like this, getting angry at nothing.’ She said through gritted teeth, even just thinking and speaking about it made her get worked up.
‘Shh, darling. It’s ok, we will get you there.’ Loki soothed her and she instantly began to calm again. He kissed her forehead, making her heart flutter.
‘Have you been sleeping better now that you’ve been doing some training each night?’ He asked.
‘Yeah, I have. Thank you.’ Echo nodded. ‘Would the others be really angry if they found out? Even though I’ve not done anything wrong, and I’ve always been supervised by you?’
‘They probably would. It’s best we still keep it a secret.’ He winked at her. ‘How would you like to try something a bit different tomorrow night?’
‘What do you have in mind?’ Echo asked curiously.
‘How about going off site for a little bit? There’s a… special little mission I need to do. One that I could do with having your help on.’ Loki said.
‘What… what sort of mission?’ Echo raised an eyebrow.
‘I will fill you in more tomorrow on the way there, if you’re up for going?’
Echo pondered on it for a moment, then nodded. She trusted Loki, so why not? If she could be useful, then surely that was a good thing?
‘Excellent.’ Loki grinned widely and gently kissed her on the lips.
48 notes
·
View notes
Text
September is Chiari Malformation Awareness Month!
Hi yes hello! Since many people probably aren't aware of it, I wanted to bring attention to something we ourselves have called chairi malformation at the start of its awareness month! Its recognized with a purple ribbon usually with a zipper on it (for the zipper scars of those who've had Chiari surgery)
What is Chiari Malformation?
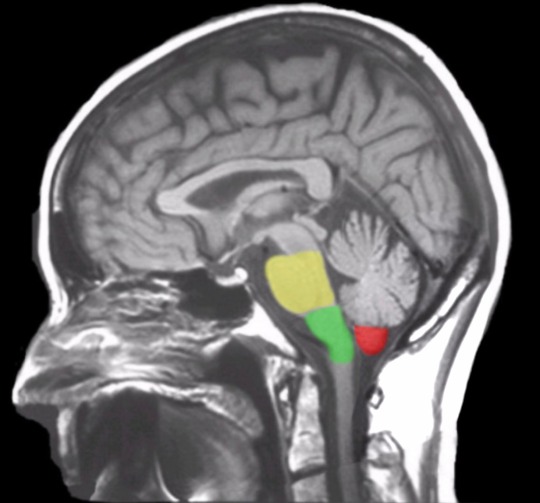
Chiari (key-arr-ee) Malformation is a brain malformation in which the brain is too large, skull is too small, or some combination on the both, causing the cerebellar tonsils (and in some instances the brain stem) to slip through the skull and into the spinal chord.
Chiari is most typically a congenital effect. There are two main types (though they aren't the only ones). The most common of the two us Chiari 1, in which only the cerebellar tonsils are descended through the skull. The second most common, Chiari 2 (also known as Arnold-Chiari malformation) has more tissue herniation in the cerebellar tonsils and even the cerebellum, as well as brain stem herniation as well.
(See Below, the Cerebellar tonsils are marked in red while the brainstem is marked in green and yellow. This is considered a normal MRI)
Chiari malformation is likely to occur in 1 in 1,000 people, making it uncommon but not rare. The statistics are likely to be slightly higher than that for Chiari 1, as many people don't present symptomatically (and many incidents are only found in cases where the person was receiving radiological imaging for other instances such as head injury, so many people are unaware they had Chiari to begin with).
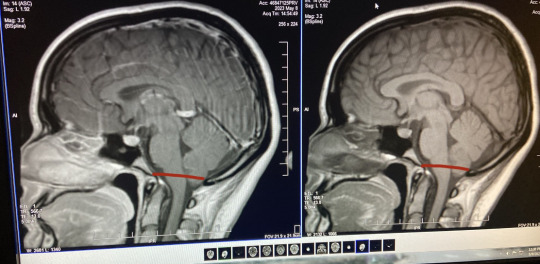
The only way to diagnose Chiari is through radiological imaging (many arguing upright MRI specifically is the only proper way to view the real level pf herniation). Herniation is measured down from the McRae line to the lowest point on the cerebellar tonsils. Depending on the accuracy of the machine (and which imaging tool is used) herniation can appear at different levels at different times. (See below, my first MRI looks markedly less in comparison to my second MRI, which features a roughly drawn on McRae line. In the second image I was noted to have a 7-8mm herniation.)

Symptoms
Chiari is marked by a number of symptoms and commorbidities, even moreso depending on the type you have. Symptoms can occur at any level of herniation. Some people with Chiari can have a 3mm descent and have debilitating symptoms, while some may have a 15 mm descent and be completely asymptomatic. The most common of these is occipital headaches & migraines, ranging from mild to severe, but many more are possible. These range from...
Balance Issues
Dizziness & Vertigo
Neck & Shoulder Pain
Difficulty Swallowing
Sore Throat
Sleep Apnea
Nausea & Vomitting
Tinnitus & Hearing Loss
Blurred Vision, Visual Snow, & Vision Loss
Muscle Weakness
Numbness or Pins & Needles (Caused by Nerve Damage)
Poor Motor Skills
Fatigue
Cognitive Difficulties (including but not limited to Brain Fog, Memory Problems, Confusion, & Difficulty Speaking)
Insomnia
Photophobia/Light Sensitivity
Syncope, Fainting, & Drop Attacks
Seizures
Dysautonomia
Since the cerebellar tonsils block the opening to the base of the skull, Chiari can halt the proper flow of CSF (Cerebral Spinal Fluid) between the brain and the spinal chord. Because of this, Syringomylia (cysts filled with CSF formed on the spine called Syrinxs) is considered common with Chiari. Other common disorders with Chiari are Scoliosis, EDS & Cervicocranial Instability, POTS, Tethered Spinal Chord Syndrome, Spina bifida, & Hydrocephalus.
So What's the Solution?
Well, the only known solution for Chiari as of right now is surgery. This surgery is called posterior fossa decompression-- in which a small portion of the base of the skull is removed from the Chiari patient to relieve pressure and give more room for the brain. The surgeon can then do for sone patients a duraplasty, in which the dura (or opening of the brain) is cut open and a patch of tissue is sewed into the incision to make the dura bigger and give even more room for the brain. Surgery can also be done as a preventative measure against syrinxes for those without them. In the case the patient also has a syrinx, more surgical procedure can be done to drain the cyst. In patients with EDS, special procedures must be made to avoid surgical complications and making things worse.
Surgery is not guaranteed to completely alleviate symptoms, but typically helps with some. However, due to large misunderstanding and disagreement on proper diagnostic traits of Chiari from doctors (most typically neurologists and neurosurgeons) many may be denied surgery for a number of years, and Chiari Diagnosis can take on an average of 4 years to officially receive.
Some go years experiencing symptoms and having "low lying cerebellar tonsils" (or similar language, such as incidental tonsillar ectopia) noted on their radiology reports without doctors officially recognizing it as Chiari. In this time many are misdiagnosed with other disorders such as chronic headaches, multiple sclerosis, fibromyalgia, and more before finally finding a doctor who will listen. Many will brush off the radiological findings as just a difference in your brain being formed at birth before admitting the symptoms can be due to Chiari. It can take years of your own patient advocacy before someone finally listens.
This is why awareness to it is so important, in hopes of reaching other people and doctors and forming a stronger understanding of the condition from information found by experts on it and those with Chiari themselves. With more awareness comes more accessibility to treatment and surgery so those who are symptomatic can hopefully find some relief. So this month send a little love & luck to those with Chiari!

#chiari#chiari malformation#chiari awareness#neurological disability#disabled#disability#disability awareness
24 notes
·
View notes
Text
for my migraines I have to get these steroid injections called nerve blocks, and it's mixed with local anaesthetic to reduce pain while the steroids get working. but they do this to the greater occipital nerves, which are around the base of the skull/top of the neck and supplies sensation to a pretty large portion of the head. so for like, 2 days I just cannot feel the back of my head at all unless I poke it. just had my second one and it has not become any less weird yet
7 notes
·
View notes
Text
Rural Family Medicine Is Great And Exhausting
Today, I saw 21 patients, I prescribed medication for an abortion, I started a patient on hospice, I placed on IUD, I started a transgender patient on anti-androgens, I saw someone with a one in a million genetic disease, I comforted a queer person who just lost their spouse to cancer, I adjusted psychiatric meds for a schizophrenic patient with profound paranoia who is tremendously kind. I saw two employees of my clinic. I saw a doctor's spouse.
Every day is different. I do IUD insertions, Nexplanon insertions, colposcopies, skin biopsies, cyst removals, toenail removals, greater occipital nerve blocks, shoulder and knee injections. I treat blood pressure and diabetes and atrial fibrillation and congestive heart failure, like all generalists do. I treat things specialists would see in the city because we have a tiny handful of specialists. I could work in the hospital again if I wanted to. I could go back to delivering babies if I wanted to. I see pediatric patients, I see patients over 100 years old. I see psychiatric patients who simply do not have access to a psychiatrist because there are never more than five of them to serve an area of 70,000 people, scattered across our geography. I diagnose cancers and rheumatologic diseases. I am forced, on a daily basis, to become a better version of myself--more aware of the system I work in, more underlying medical knowledge.
I love my work. It takes most of me. I don't have kids, and I'm glad, because I wouldn't be able to work like this and I love my work. I don't regret the choices that I've made that led me here.
I'm turning thirty-nine this year. I worked in so many different jobs, took so many different classes, volunteered and read and wrote and experimented with who I was and who I wanted to be. You have time. You can become the version of yourself that can make you happy. There is no single endpoint, no moment when you get to stop and go, that's it, I'll just calcify in place now. You are a human. You are meant to keep moving and changing and growing. That scared the shit out of me when I was younger and came from a deeply unstable home and all I wanted was peace. I wanted to be able to rest. But you can't stagnate and call it peace.
My life has worth beyond what it's worth to me. That's what I wanted. I wanted the bliss of service. I wanted to be of service. And in my own way, in my own time, on my own terms, I am.
163 notes
·
View notes
Text
I've been gone the longest these past months, and I'm once again apologizing for the absence. Life hasn't been good. I've barely been functional. Not two months ago, I buried my aunt who passed in January. Still don't think I've really accepted it fully. Then, in early June, an uncle died due to Covid and complications. And then my dad had to put down his dog, who I was also quite close with, because of sudden and severe health issue.
And I won't go into much detail, but my health has worsened. In some ways, things have improved by getting accurate diagnoses, but then other issues just pop up. In March, my OB/GYN found endometriosis on the outside of my rectum (other lesions and problems were found but have been managab). I'm so thankful for her because the endometrial-like tissue did not present in the normal way (cigarette-like burns) but instead like thin, white veiny tissue. Most doctors probably would have ignored it, but she cut it out and had it biopsied just in case. And she was right.
And literally a week after the laparoscopy, I had a gastric emptying scan. After, my GI diagnosed me with Gastroparesis and also lumped on Post-Cholecystectomy Syndrome as well. Treatment has sucked. I've lost an unhealthy amount of weight in a small time. The most basic nutritional needs are getting harder to meet.
During this, dealt with months of horrible pain in my head. Felt like liquid cement leaking into the back of my skull and pressing into my brain. Went to the ER in early June because the pain was coming on so quickly and so severely I was considering suicide. After imaging, they found my left occipital nerve showed a higher thickening and hyperintensity. So turned out to be Occipital Neuralgia and treatment has been long. Not responding to nerve blocks that well, so we're still trying.
Also, turns out I have Myasthenia Gravis. Started treatment and there's been some improvement. For over a month I could barely do anything: couldn't use my laptop and struggled to us my phone, couldn't read or write or color, couldn't do puzzles or even open my own water bottle after the seal was broken. Literally just stuck watching TV and it took a toll on my mental health. The double vision, dysphagia, and hand weakness has gotten a bit better as I can now at least do some things, but I'm still very limited.
Sorry for the absence. And sorry for any rambling. Haven't really talked to anyone lately, so life's been lonely.
40 notes
·
View notes
Text
i am not dead!
however i now have occipital and temporal neuralgia after my accident which means i get to enjoy stabbing/goring/burning sensations all over my scalp, forehead, and around my right eye at random intervals throughout the day, sadly due to the healthcare system where i live there are no options for treatment until 6 months from now since treatment might paralyze the nerves or something. at this point who knows!
but basically my head is apparently much worse off than i initially thought and i am living in 40 minutes blocks of activity -> laying down in a dark and quiet room with no brain stimulation -> 40 minutes of activity -> no stimulation etc etc. so sadly idk when i can be back but i felt bad leaving on a note of "i hit my head but i'm fine!!" *doesn't post for 5 months* lest ye all think the opps got me. the opps didn't get me!!!!!
#what's worse is my scar has faded so i LOOK like 95% normal but i am just having the craziest time every day#for example as i'm typing this it feels like someone is STABBING my scalp! and if i touch my head it feels spongey somehow#yesterday i was also convinced my skull was caving in and i could “feel” it as i ran my hands over my head. (:#thankfully my skull remains mostly intact <3 for now <3
8 notes
·
View notes
Text
So I had a procedure today at the hospital- occipital nerve blocks in my neck to try and stop my chronic migraines that don’t respond to anything (:
ANYWAY no one he wants to hear about that but basically it was REALLY trash and is one of the most painful and uncomfortable things I’ve ever experienced (and I’ve broken bones/ dislocated limbs and live with chronic pain)
The procedure also makes you feel SUPER weird like dizzy, lightheaded, vertigo, nausea, and as my nurse put it “really yucky”
I’m recovering rn and probably will for a few days and I HATE resting… I’m struggling to really do anything rn even sit up and eat but I have such a strong urge to write a drabble and inflict this shit on a character…
7 notes
·
View notes
Text
Migraine isn’t a Headache Part Six: make it stop
We looked at medication and treatment for acute attacks of migraines. Things that you can do to treat the pain when you're having it.
This is also probably the first line of help you'll get from a GP or pharmacist or whoever you approach for help.
Some people have success with acute treatments. Maybe the migraine was a one-off, or is a rare occurrence, maybe it was just really responsive to acute meds.
Some people have migraines that don't respond to acute meds, or don't respond well enough to be considered effective treatment.
When you get to this stage, you need to start looking at stopping the migraines before they start, instead of constantly taking acute meds that a) don't work and b) can cause rebound headaches and other problems.
It sucks, because you want to reach for the painkillers when you have pain, but doing so is not sustainable.
Getting into preventative meds ties in a lot with how you go about getting a diagnosis, but I'm going to try to speak about the meds and complimentary treatments AROUND being under a neurologist. On that note, GPs are rarely going to work with you on preventative meds.
There are a few they can prescribe, but you'll probably get better treatment under a neurologist or headache specialist. Sorry.
GPs are useless.
Sorry, bit of my bias there, but I don't use GP's unless I need a referral or quick acute treatment, and EVEN THEN.
It's worth noting as well that you'll usually only get to this stage if your migraines have become chronic, that is:
for over 3 months
you've had 15 headache days a month minimum
of which 8 have migraine features
Some of the treatments aren't indicated for episodic migraines.
((As previously mentioned, this definition might be changing to take into account the impact migraines are having on your life, and not a somewhat arbitrary number; fingers crossed this happens soon))
My list of attempted treatments includes:
amitriptyline (this is one the GP might prescribe for you) (also prescribed for abdominal discomfort and major depressive disorder, although it's fallen out of favour due to increased risk of fatality in overdose)
propranalol (and this) - beta blocker
flunarizine (calcium channel blocker, used to treat high blood pressure and certain heart conditions)
lamotrigine (usually prescribed for epilepsy and bipolar disorder)
topiramate (usually prescribed for seizures)
candesartan (usually prescribed for hypertension)
pregabalin (usually prescribed for seizures and anxiety)
gabapentin (usually prescribed as an anticonvulsant and for nerve pain)
Botox injections
greater occipital nerve blocks
Magnesium/CoenzymeQ10/Vitamin B trio
Aimovig (erenumab, CGRP injection, one of the first migraine-only treatments)
Ajovy (fremanezumab, another CGRP injection, one of the first migraine-only treatments)
sTMS machine (single pulse transcranial magnetic stimulation)
Vyepti (eptinezumab-jjmr IV infusion, another CGRP drug)
I don't think I've had EVERY drug available for migraine prophylaxis, but judging by the increasingly surrendering tone of the letters from my neurologist, I'm just about there.
As you can see, apart from the last CGRP drugs, almost every drug listed is used off licence for migraines, and none of them were developed to treat migraine at all.
You can group most of these drugs into treatment for blood pressure, epilepsy and mental health issues.
The idea that migraines are mainly caused by blood pressure has kind of aged out with advances in research, but the fact remains that some medication that acts on blood pressure still helps migraines.
I think, bearing in mind that a migraine is a neurological storm, that it makes sense that meds that act on activity in the brain (mental health meds/epilepsy meds) can help migraine. Makes logical sense, right?
The usual procedure for taking these medications for migraine (at least in the UK) is to titrate up to the correct dose, and then (assuming you tolerate it and don't get floored by adverse reactions or the side effects) remain on that dose for 3 months before concluding if the medication is successful or not.
If you're seeing some improvement but not a lot, they might keep you on it for longer, or increase the dose.
Otherwise, 3 months and no improvement means you move onto the next drug and/or treatment.
A lot of these drugs have some really heavy side effects. I've experienced worsened tremors, awful dizziness, change in sense of taste, changes in appetite, terrible brain fog.
For migraineurs it comes down to a balancing act.
How bad are the side effects vs how much is this med helping my migraines, and which of the two am I best able to handle.
Maybe you can manage dizziness or not being able to drink Coke anymore over the migraines.
Maybe the awful tremors and inability to think clearly is worse than bearing with the migraines.
This is usually something you discuss with your specialist.
Just saying again, some of these meds are a little hardcore. Don't try treating your own migraines on your own with these meds if you can get your hands on them somehow. Apart from the side effects, the dose if really important too.
In the UK, if you've failed at least three preventative treatments, and have been managed for medication overuse headaches, you can try botox.
BOTOX
The reason botox works for migraines isn't well known, but doctors think it blocks pain transmitters in your brain.
Botox, or botulinum toxin, is a nerve toxin that paralyses muscles.
It's used for cosmetics treatments, but also medically for hemifacial spasm, cervical dystonia, cerebral palsy, bladder pain, lower back pain, neuropathic pain and stroke.
When used for migraine, it's delivered in a series of 31 to 39 small injections, mostly around the forehead, but also on the temples and at the base of the skull.
If you've ever had acupuncture, the needles are a lot like that. I thought they'd hurt more than they did. They were just little stings, not even as bad as plucking an eyebrow hair. Of course, everyone's different with different pain thresholds (especially if you're oversensitised migraine pain leaves you with allodynia) but it's truly not that bad.
You get three sessions 12 weeks apart, just like taking the meds, and if you've had improvement you can continue. If you don't, its on to the next med or treatment.
It feels weird when it settles in. Your forehead tends to freeze, so you can raise your eyebrows and have no lines there. This might unsettle some people, but it does wear off over time.
Side effects include neck pain, muscular weakness and a drooping eyelid, but these improve as the botox wears off. I had a little neck pain, but nothing else. One of them in my forehead bled only a little, none of the rest did.
You can have an allergic reaction, but they will keep you in the treatment or waiting room for some time after your first treatment to check that.
Getting botox for migraine sounds worse than the experience is, but it is about 75% successful for reducing migraine.
Not for meeee
GREATER OCCIPITAL NERVE BLOCKS (GONB)
If your migraines have been resistant to drug treatments and botox, your specialist might decide to try GONB. This is usually a treatment for cluster headache or headaches that originate from pain in the neck, so it may not be applicable to your specific situation.
This treatment involves injecting an anesthetic and a steroid (not always both) into the back of your head/top of your neck around the greater occipital nerve (GON).
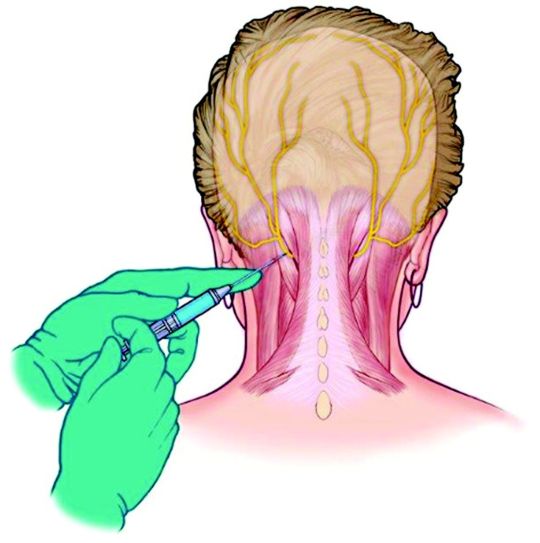
The GON runs from the top of the spine to the scalp, and feeds into an area of the brainstem called the trigeminal nucleus.
A nerve block reduces traffic in this nerve, so reduces the amplification of pain and other sensory information that might be overloading this area.
In simple terms, the nerve block stops the pain signals going into the nerves that make you feel the headache.
A lot of people have had success with this treatment, but I'm not one of them.
I don't want to scare anyone!
The reaction I had is (apparently) pretty rare.
After the neurologist injected the first lot of lidocaine into one side of my head, then the other, I almost immediately felt dizzy and sick.
He let me lay down for a moment, but I felt that I was going to puke, so I had to get up. What followed was tunnel vision, greying out, nearly full syncope (fainting) and then vomiting.
I was having a reaction to the lidocaine, which suddenly made my nausea and faintness when I had my lumbar punction (spinal tap) make sense.
I wasn't able to get to the stage where I had the steroid injection, and whatever there was of the anesthetic after my body tried to purge it made no change to my migraines.
I can't speak for the efficacy of the GONB because my body failed it, but if it's offered, I'd encourage you to try it. Apparently it has helped a lot of people.
CGRPs
After trying 3 meds, then botox, then the GONB and failing all of them, I was put on the next med to see if I'd respond to any of them.
You don't need to have exhausted every pill before trying injection treatments.
You can also mix and match treatments, especially a pill or a CGRP with botox.
With the knowledge that you spend a minimum of 3 months per med (and assuming you don't come off it immediately due to adverse reactions) you can only go through 4 meds in one year. It takes two years on this schedule to go through the meds I've worked through, not including the botox and GONB, and the extra time taken to titrate to the correct dose.
Finding a medication that works to prevent your migraines is a long and exhausting process.
Thankfully, recent research into migraine has come out with the biggest breakthrough in migraine management, I'm going to say ever, because we now have the first medication created directly for the prevention of migraines.
CGRP stands for Calcitonin Gene-Related Peptide
It's a chemical involved in transmitting pain signals through the nervous system – and it’s also associated with the triggering of migraine attacks (among others).
CGRP medications are actually ANTI-CGRP drugs, designed to stop the action of the chemical.
The ones currently available in the UK fall into two groups.
Aimovig (erenumab) that works by binding to the receptor.
Ajoy (fremanezumab), Emgality (galcanezumab) and Vyepti (eptinezumab) which bind to the protein.
Because of that, if you don't have success with Aimovig, try one of the others (and vice versa) as you might see some improvement.
These are adminstered by self-injection (although the first one will be done under nurse supervision) every month with something like an epipen that's injected into your thigh.
The injections hurt me and ached afterwards, but I had no other side effects than that.
I actually had one migraine day where my pain was a 3, which hadn't happened since I started having migraines, but unfortunately, NHS guidelines state that you need to have a reduction in pain days or a significiant reduction in pain in order to stay on them, so I was taken off.
We've just had Vyepti (eptinezumab-jjmr) approved for some people with migraine in the UK.
Vyepti is a CGRP administered via IV infusion over 30 minutes at a clinic, and it's still such a new drug that they're still collecting information on side effects, etc.
I've had my first dose (they're given every 3 months) and while I didn't see a reduction in pain days, I saw maybe a slight reduction in pain, but more than that, my brain fog and pain cloudiness really cleared up, at least for the first month and a half that the effect lasted.
I was actually present in my body for once, instead of half-checked out, even if I was still in pain.
I don't know what the review will bring, but I hope they let me stay on it.
In the US, they've also got a new group of drugs called -gepants (Ubrogepant, Atogepant and Rimegepant for now) which are being used preventatively, but also like triptans, acutely.
Like the injections, they also work on the CGRP receptors by blocking their effect.
I don't know very much about them, but they're also some of the first drugs made specifically for migraine, and there's a lot of excitement about them.
They're safer than triptans for people with heart issues to take, and they DON'T CAUSE REBOUND HEADACHES!
This is huge in the world of migraine treatment, as there are no other acute treatments that do this.
NON MEDICINAL
A large chunk of preventative non-medicinal treatments for migraine involve making lifestyle changes (I know)
The migraine brain is oversensitive and overreactive creature, and ANYTHING can push it into a tantrum. Weather changes, temperature changes, lights, sounds, smells, so many things that we can't control in our environment.
Our migraine brains love routine, and even though it's annoying and removes some chunk of flexibility in our lives, it annoyingly does help.
Sleep routines are helpful, as much as you can fit yourself into one. Setting sleep and wake alarms with x amount of hours in between (7 or 8?) and then sticking to them rigidly means that you'll be getting up when you're still sleepy and going to bed when you're not, but your body will eventually fall into a rhythm and you'll find yourself sleeping and waking at those times automatically.
Issues: daytime naps are no good for sleep routines, and sometimes you just HAVE to sleep when a migraine hits. What if you want to stay up on the weekend? It's difficult, but keeping to a schedule as much as possible is better than leaving it in the wind.
Eating regularly, small meals often is the best. I'm not going to spend a lot of time on this because diet is a huge and sensitive subject, and comorbidities can make this even more difficult, but as far as migraines on their own are concerned, they like the body to be kept as stable as possible, which means a level blood sugar level, etc, and avoiding hunger.
Exercise? I know, I'm not going there, apart from, gentle stretches for your neck, maybe your back, can help. Even if neck problems have nothing to do with your migraines, you're going to end up all crunched up and tense from being in constant pain. Look at stretches for post-operative, for the elderly, for anything you can do in bed. It doesn't have to be high impact or intense, just something you can do now and again to keep your muscles loose.
H~y~d~r~a~t~i~o~n. I'd say use a pretty bottle, but honestly, using whatever will make it easier for you to fill and keep drinking from is better than something that fits your aesthetic. You can always decorate a plastic bottle, or use a favourite glass.
Apart from all those irritating things that abled people always recommend (yoga anyone?) there are also non-drug but prescribed treatments.
One category is DEVICES
I've only tried the sTMS device, so I'll address that first.
sTMS stands for single pulse transcranial magnetic stimulation
You press the button to charge the thing. When it beeps you place the bean-shaped device at the back of your head so it cradles your skull, and then press both buttons at the same time.
There's a ka-chonk, and a sensation like someone's smacked you in the back of the head a little, which is actually the small magnetic pulse.
It works by generating mild electrical currents in the brain that are supposed to disrupt the brain activity linked to your migraines. You can use it acutely, but also daily (2 or 3 times a day, 1 or more than 1 pulse at a time) to prevent migraines.
The machine didn't do anything for me, and made my scalp feel a little sore, although that doesn't appear to be common.
You may also have heard of the Cefaly, a device otherwise called a 'external trigeminal nerve stimulator'
There's that trigeminal nerve again, running around the side of your face and your eye, playing up and causing pain.
You place an electrode on your forehead, and the Cefaly generates micro-impulses to stimulate the trigeminal nerve's nerve endings.
Be aware that the efficacy of the Cefaly device is debated, but it does help some people.
ACUPUNCTURE has been used to help migraine
I had many courses via my GP (the only good one I had) who was trained in acupuncture and went above and beyond to give me as many treatments as possible. I think I had 12. I felt something from them, but they didn't have any effect on my migraines.
Finally, not a drug per se, but VITAMIN SUPPLEMENTS
The best are a trio as follows:
Riboflavin 400mg once daily
Co-enzyme Q10 100mg three times a day
and Magnesium (there are two/three types and the doses are different)
Citrate 600mg OD
Tricylicate 250mg twice a day
or Phosphate 400mg once daily
There is also therapy that is prescribed for management of migraine, not so much prevention as just giving you tools to learn to live with being in pain.
I haven't gotten to that stage yet, and have mixed feelings about it.
Some people have said it's helped, some said it hasn't.
It -feels- a lot like being told 'we can't do anything to help you, you just have to deal with being in pain now'
I haven't tried it, I probably will end up doing so, and maybe I can write a little about it then. For now, I can see why it could be useful, but it does feel a little bit like being abandoned.
And that's all I've got for preventative treatments.
I don't know when I'll be able to start writing about my diagnosis journey, but that should be the next part.
please excuse any typos!
i hope this is still helpful for some people.
#migraine isn't a headache#migraine#disability pride month#migraine awareness#chronic pain#spoonies#headache#preventative meds#migraine medication#migraine treatment
8 notes
·
View notes
Last Seen Blogs

lamartine1
sweetheart

marti-kudo
M a r t i n a

sangraweeparnthep
Sangrawee Parnthep

package-svg
Package-Svg

clockworkorange90
İsimsiz