#psychotic disorder nos
Text
Shoutout to those who have had to go through things no one should as kids/adolescents due to their mental illness(es).
BUT ALSO:
Shoutout to those who developed their mental illness(es) after their tween/teen years and had to learn to adjust to life with mental illness.
ADDITIONALLY:
Lots of love to all with mental illness who had to adjust without much or any support from others/those you love(d).
END NOTE:
Mental illness is hard enough on its own, but these conditions can make it so much more difficult.
You’re worthy and deserving of love, support, and respect even if you haven’t been receiving it.
#actually psychotic#actually schizospec#schizospec#schizophrenic spectrum#mad pride#actually schizophrenic#disability pride#schizo spectrum#schizoaffective#brief psychosis#psychosis positivity#psychosis nos#actually schizotypal#schizophreniform#actuallypsychotic#substance induced psychosis#psychosis spectrum#psychotic spectrum#psychotic disorders
158 notes
·
View notes
Text
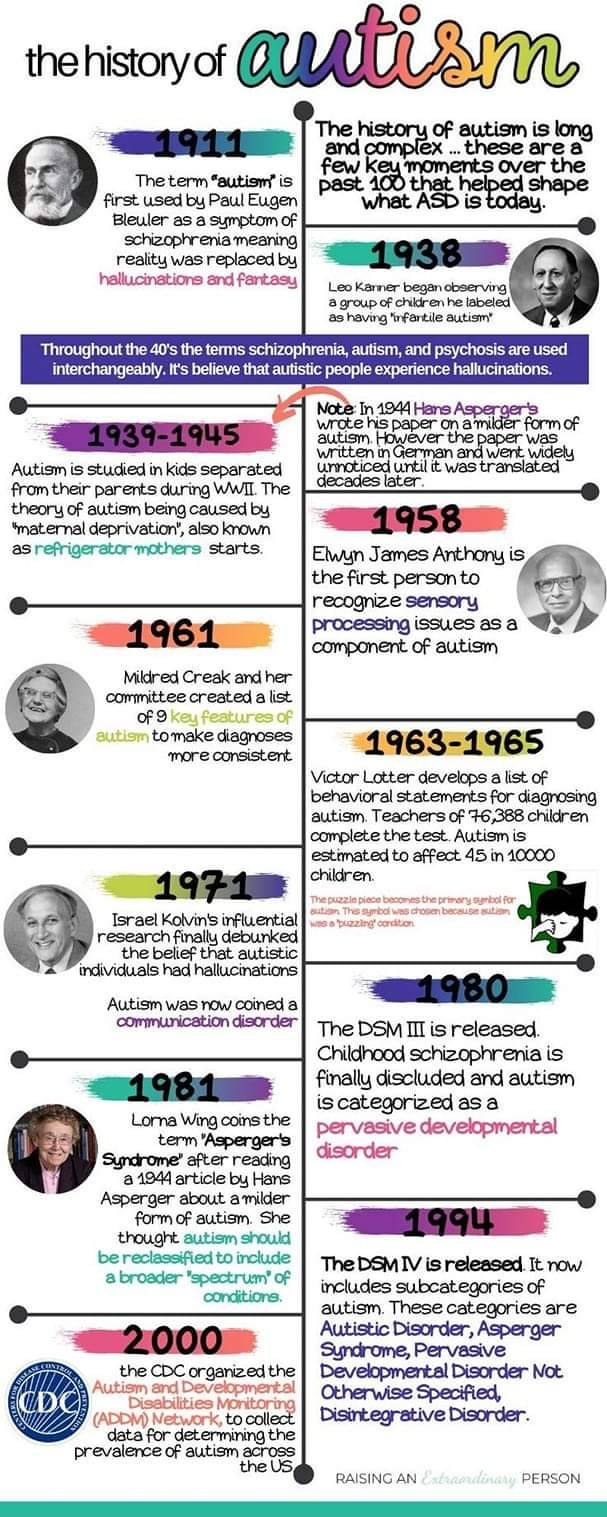
History of Autism
The term autism first was used by psychiatrist Eugen Bleuler in 1908. He used it to describe a schizophrenic patient who had withdrawn into his own world.
Eugen Bleuler coined the word "autism" in 1908 among severely withdrawn schizophrenic patients.
In 1943 Leo Kanner studied 11 children. The children had difficulties in social situations, adapting to changes in routines, good memory, sensitivity to sound, allergies to food, good intellectual potential, echolalia, and difficulties in spontaneous activity.
In 1944 Hans Asperger, who was a German Nazi, sorted autistic individuals into two categories. He studied one group and had the other group killed. The children he studied were considered "high functioning" and spoke like grownups. He also said that many of the children were clumsy.
In 1952 autism is added to the DSM as a psychiatric disorders diagnosed by a profound emotional disturbance that does not affect cognition and many people with schizophrenia were misdiagnosed.
Bruno Bettelheim studied the effect of three therapy sessions with children who he called autistic. He claimed that the problem in the children was due to coldness of their mothers. He separated the children from their parents. Kanner and Bettelheim both worked towards making hypothesis that showed autistic children had frigid mothers. This is where the term refrigerator mother came from.
Bernard Rimland was a psychologist and parent of a child with autism. He disagreed with Bettelheim. He did not agree that the cause of his son’s autism was due to either his or his wife’s parenting skills.
Autism came to be better known in the 1970’s. The Erica Foundation started education and therapy for psychotic children in the beginning of the 80s. Many parents still confused autism with mental retardation and psychosis.
In 1980 autism was changed in the DSM to be a pervasive developmental disorder seperate from childhood schizophrenia. It defined autism: a lack of interest in people, severe impairments in communication and bizarre responses to the environment, all developing in the first 30 months of life.
It was in 1980’s that Asperger’s work was translated to English and published and came into knowledge. Lorna Wing read it and coinsd the term Asperger's.
In the 1980’s that research on autism gained more traction and it was believed that parenting had no role in someone being Autistic and that there were neurological disturbances and other genetic ailments as the cause.
In 1987 the DSM divided autism into categories based on functioning labels. PPD NOS was used to describe those considered high functioning and autism for those considered low functioning.
Lorna Wing, along with Christopher Gillberg at BNK in Sweden in the 1980’s found the Wing’s triad of disturbed mutual contact, disturbed mutual communication and limited imagination.
In the 1994 the DSM is changed to include Asperger's. With PPD NOS as high functioning, Asperger's in the middle, and Autism for low functioning.
Them Ivar Lovaas studied and furthered behavioural analysis and treatment of children with autism. He developed it to target younger children (less than 5 years of age) and implemented treatment at home and increased the intensity to about 40 hours weekly. This therapy was ABA. This therapy was also modified and used as conversation therapy.
In 2013 the DSM removes Asperger's and PPD NOS and autism is now classified a social communication disorder.
In 2018 the DSM classified Autism as autism spectrum disorder and makes a distinction between autism with and without intellectual disability, and highlights the fact that older individuals and women sometimes mask their autism traits.


#autistic#autistic pride#autism acceptance#autism#audhd#actually audhd#autism acceptence month#asd#autistic adult
13 notes
·
View notes
Text
ฅ^•ﻌ•^ฅ My Writeblr Intro ฅ^•ﻌ•^ฅ
About me:
Hi there, my name is Max, and i don't particularly care what pronouns you refer to me with, as i am genderfluid :3
Brand new to writeblr (unless you count fanfiction) and kinda nervous to post my original works, but also excited! I do tend to read a lot more than i write- my favourite genres are horror, thriller, crime, splatterpunk, urban fantasy, and dystopia :)
i have been posting fanfiction on and off since i was 10 (i'm 19 now), though the majority only stay up for a couple months until i delete the individual post or the entire blog/account from awkwardness of being a very slow poster
I am very open to feedback on my posts, and would enjoy being recommended different things to read, particularly original works or hidden-gem-manga!
Asks will be open if anyone wants to chat, and i'll respond as soon as i can- it can be literally anything too, whether someone wants to say hi or discuss moths or video games

Fun Facts:
i am 19 years old, and studying to become a veterinarian
i have a drawing blog and fanfiction blog, both of which i've pretty much abandoned (and feel very guilty about)
i also have a project blog called Belladonna Project V2, which i'm revamping for my biggest project ever
i am genderfluid and asexual
i am autistic and have a psychotic disorder (you can ask questions if you want to, i don't mind)
i adore video games when i'm not reading- my favourites are the entire pokemon franchise, ooblets, paleo pines, world of warcraft and planet zoo!
i have a mini obsession with moths, and also animal genetics/mutations/variants
Current writings:
Series- a vampire and pink cat
the fireberries
ashe has a crush
Daily moth posts
day 1- yellow furry legs
Daily animal posts
day 1- ring tailed vontsira
Blog Yes-es
being tagged in tag games or interactions
asks about literally anything hobby/interest related (mine or yours)
being given recommendations of things to read
discussing ideas and OCs
Blog Nos
transphobia, or homophobia
disgusting topics outside of splatterpunk books that already exist
discrimination of any kind
psychosis-shaming
Thank you for reading if you actually read all of this, and i look forward to sharing my writing with you all!
#introductory post#intro post#blog intro#introduction#introducing myself#writeblr#bookblr#writeblr intro#writing#writers on tumblr#writerscommunity#creative writing#mangablr#max-writes-randoms#masterpost#masterlist
6 notes
·
View notes
Note
why is that schizophrenia should be considered neurodiversity like autism/adhd and not mental illness like psychosis NOS, ocd, bipolar etc? not asking to be rude, just feeling very ignorant about that last post you reblogged oops
Because schizophrenia is more than just a psychotic disorder and actually has a LOT of overlaps with autism. Autism and schizophrenia actually have a shared history and I happen to have both
Psychosis is a small part. It's a brain divergence, hence neurodivergent
#anon#schizophrenia spectrum#autistic schizophrenic#schizo spectrum#actually schizophrenic#actually autistic
6 notes
·
View notes
Text
My mental health?
My therapist says I should talk about my mental health more and I only have like three friends. So I thought I would type it out here. I've had delusions and hallucinations that lasted intensely for a month and while recovering they lasted for a few more months after that. It didn't get better until they upped my dosage of medicine and I still feel like it's not enough sometimes. I don't get the hallucinations any more, but sometimes I get so stuck in my head that it starts to get a little bit delusional.
Some delusions that I've had were as follows:
Believing people were out to get me.
Believing people weren't who they said they were.
Believing that the people that I loved had been replaced with something else.
Believing that the people I loved were trying to cause me harm (i.e. by drugging me).
Believing that people were vampires and there was a hierarchical system.
Believing that the people around me were reincarnations of gods and people from myth.
Believing that the literal devil and angels were walking amongst us.
Believing random strangers were people I knew.
Believing that certain hand signals meant certain things.
Believing that people were talking about me when they really weren't.
Believing that everyone's thoughts were connected in some way, sort of like a fungus.
Now I don't believe those things. I'm taking antipsychotics, anti depressants, and mood stabilizers.
In the hospital I was diagnosed with Bipolar Disorder with Psychotic Features, but since then I've had another diagnosis Bipolar NOS (not otherwise specified). My symptoms don't follow a regular bipolar diagnosis be it bipolar 1, bipolar 2, or Cyclothymia. I have the symptoms, but they don't check all of the boxes.
Really, the only things I need to be working on are my agoraphobia and paranoia.
All of this sounds like a lot and it is something I haven't actually told anyone. I've told my therapist that I've had delusions that people aren't who they were, but I just left it at that. The rest of the stuff sounded too fantastical and I didn't really want to get into it with them. They weren't my first psychologist, but they have been my longest. I have an appointment with them in a few days. I'm hoping it goes well.
I'm better now. Far better than I have been. But sometimes I'm afraid I'll forget things. I usually have a great memory, but when I was having my psychotic episode time became a bit of a blur and reality started to shift. It was hard to keep track of what I was dreaming and what was real. It turned everything into a messy puddle.
Again, I'm better now. I guess if anyone has any questions I'd be happy to answer them. . . I'm not really expecting anyone to read this. It's just something I'm dealing with and I'm hoping if someone reads this they won't feel so alone, because I've felt alone. I felt more alone in those months than I have ever felt in my life.
Au revoir.
#bipolar disorder#mental health issues#mental illness#this is just a record I'm too afraid to write down on paper#its totally fine if its on the internet am i riiiight?#its all fun and games until someone falls into the pit of the void#i can make another post about hallucinations if anyone wants#those were wild and scary and weird#psychotic symptoms#i hope i dont regret this later but i can always delete if i want
3 notes
·
View notes
Text
Introduction
Psychosis NOS (Not Otherwise Specified) refers to a condition where individuals experience symptoms of psychosis that do not meet the criteria for a specific psychotic disorder. It is a significant condition as it can greatly impact an ...
#Mirari #MirariDoctor #MirariColdPlasma #ColdPlasma
0 notes
Note
Barry’s schizophrenia is very poorly written, as someone who was diagnosed as being schizophrenic, I just find he doesn’t even fit the profile of most schizophrenic cases. He is a successful college student, apparently , prior to the comic. Bear in mind the profile of an acute schizophrenic case Involves a very sharp decline in functioning and reasoning skills, the only thing I really see in Barry’s features of schizophrenia is his argumentative and agitated state he typically is in. Maybe his obsession with forcibly grounding himself in reality?
He has no disorganized speech or other negative symptoms that most profiles have, no alogia, hygiene is never commented on, his other symptoms aren’t realistic either (most schizophrenics are either deeply paranoid and delusional in an acute phase of psychosis. or have running dialogue , amongst other auditory hallucinations, visual hallucinations are possible of course but also the way his are written seem very… unrealistic. Most other psychotic people I know (actually diagnosed, not self diagnosed) tend to be excessively paranoid, as am I. I don’t recognize anything that screams psychosis or schizophrenia in this character
The fact that he is autistic also? Yes you can have both it’s just uncommon (most autism cases are hard to distinguish from schizophrenia, these two are notoriously difficult to diagnose in one single person due to the similarities between the disorders, thus most will autistics suffering from schizophrenia symptoms will receive a diagnosis of “psychotic disorder NOS” alongside the autism label)
Also to clarify I’m a fan of the comic and I have nothing against the authors, they seem like decent people but they cannot take criticism at all whatsoever
im not schizophrenic but i am autistic and yeah barrys writing feels really inaccurate to reality based on my experience and the experiences of those close to me, he doesnt show any common autistic traits either besides Really Liking Science, its like they just slap the neurodivergent label on characters they dont wanna acknowledge the faults of
1 note
·
View note
Text
A banda Hierarchical Punishment é considerada um dos nomes mais importantes do Death/Grindcore paulistano e brasileiro, lançou neste domingo (06/11), seu novo lyric vídeo para a faixa “Escape The Fate”.
O lyric video de “Escape The Fate”, foi produzido por Ruy Costa do canal (Motim Underground). A música foi retirada do ótimo disco, “Psychotic Disorders”, disponibilizado em maio de 2021 via Extreme Sound Records, Impaled Records entre outros selos nacionais.
Assista o lyric video em:
https://youtu.be/AtdrYb4s4I8
Sobre o vídeo de “Escape The Fate“:
O vídeo pode ser interpretado como a voz do destino, se dirigindo a todos como um ser onipotente e inescapável. Talvez a mensagem mais clara passada na letra é que não passamos de meras formigas tentando nos esconder de algo muito maior, preparado para selar nossos destinos, não importando o quanto corramos. A agonia que se passa na mente de pessoas atormentadas pela depressão e ansiedade (um assunto muito sério, debatido nos últimos anos, e que deve ser tratado de forma adequada).
Hierarchical Punishment formada atualmente por Arthur Mendes (vocais), Grell (guitarras), Paulo Alexandre (guitarras), Alexandre Martins (Contrabaixo) e Luiz Carlos Louzada (bateria).
Acompanhe todas as novidades do HIERARCHICAL PUNISHMENT:
Site oficial: http://www.hpgrind.com.br/
Instagram: https://www.instagram.com/hierarchical_punishment/
Facebook: https://www.facebook.com/hierarchicalpunishmentband
YouTube: https://www.youtube.com/channel/UCqy-ZFtYTK4vbDo3YmRye-A
Bandcamp: https://hierarchicalpunishment.bandcamp.com/
Spotify: https://open.spotify.com/artist/1qjT2W8hcQ0jScBdfgN7HS?si=xhDzkMlATGybjzakIjtQhg
0 notes
Text
Things I’ve Learned as a Disabled Person
[Text without formatting: “Things I’ve Learned as a Disabled Person]
You did not commit a crime simply by being mentally ill or disabled!
You are not wasting anyone’s time or energy by simply existing as a mentally ill or disabled individual!
Please surround yourselves with love, support, and positivity whenever you find the opportunity!
You deserve compassion regardless of your symptoms or experiences!
You are not a monster or an abuser for being disabled or mentally ill!
You can and will find people who love and understand you, or at least try to understand to the best of their ability.
You can and will find people who support you, regardless of what that support looks like!
You do not have to need the same types of support as others. As long as you do what is best for you, that’s all that matters.
At the same time, it’s okay to need accommodations, no matter the type!
You can always work towards coexisting with others, and I hope that you will be surrounded by those who do the same for you!
You do not have to stretch yourself thin and overextend yourself to make others happy!
It’s okay to advocate for yourself! And, if you cannot do this because of your mental illness or disability, it’s okay to allow someone with your best interest in mind to advocate for you!
While you don’t need to force it (and it probably helps more not to force it), please hold onto the hope that things will not always be at their worst!
If it helps you and isn’t hurting anyone, it is nothing to be ashamed of!
Finding support is huge! It doesn’t have to be folks in your immediate area, online support is acceptable as well! What matters is that we are uplifting and supporting each other and ourselves.
There are so many things I’ve learned as a disabled person. I hope to learn many more
Please feel free to share what you’ve learned as well, or please share if you found any of this helpful! /not forced
#personality disorder safe#actually psychotic#actually schizospec#actually npd#actually ocpd#actually pocd#intrusive thoughts#actually bpd#cluster b safe#cluster a safe#cluster c safe#schizospec#mad pride#mad punk#schizophrenic spectrum#actually dissociative#actually disabled#schizo spectrum#actually schizophrenic#schizoaffective#disability pride#psychotic spectrum#psychosis nos#substance induced psychosis#postpartum psychosis#bipolar with psychotic features#actually bipolar#mood disorder#actually obsessive#actually neurodivergent
37 notes
·
View notes
Text
So this is probably going to be my favorite way to expand my hand lettering, visual note taking hobby. I’m not the best artist. This will be fun. Let me rustle up all of my drawing/ sketching stuff and just go for it again.
Would you like to see hand drawn notes of Computer Science, Math, Physical Science, and Social Science Concepts?
That might actually help me. Even if they look crap.
#college student#ptsd#chronic illness#stationary wish list#psychotic disorder nos#fibromyalgia#study motivation#studyblr#studyspo#jet pens#stationary#gift set#bundle
0 notes
Text
#college student#psychosis#psychotic disorder nos#trauma#ptsd#survivor#bunny#bunny therapy#emotional support animal
0 notes
Photo
https://neuro.psychiatryonline.org/doi/full/10.1176/appi.neuropsych.11090214
The absence of apparent affective, medical, or neurological conditions increases the possibility that a psychotic disorder could have been present. Schizophrenia is often accompanied by both disorganized behavior and thought processes that interfere with life functioning. In the case of Abraham and in the others that follow, disorganization and cognitive impairments are not apparent. Paranoid schizophrenia (PS), however, is a subtype of schizophrenia that tends to manifest little or no disorganization, has preserved functional affect, and is associated with better occupational and social functioning.
Psychotic disorder, not otherwise specified (PD NOS) is another reasonable diagnostic alternative. PD NOS includes those persons with psychotic symptomatology for which there is inadequate or contradictory information or symptoms that do not meet criteria for any specific psychotic disorder. Abraham’s clinical profile would appear to best resemble that of PS or PD NOS, and perhaps, less likely, an affective disorder-related psychosis. Abraham stands as the earliest case of a possible psychotic disorder in literature.
It’s kind of weird that the father of three major religions suffered from delusions, hallucinations and psychosis.
Wait... no, it’s not.
#abraham#isaac#binding of isaac#the binding of isaac#bible#christianity#judaism#islam#ibrahim#religion#straight outta the bible#bible study#religion is a mental illness
165 notes
·
View notes
Text
oh also i should let u all know that i’m not schizotypal, i have schizoaffective disorder, bipolar type! the doctor at the hospital said that, but he put down “mood disorder nos” and “psychotic disorder nos” because it’s easier to have those on my record than a more stigmatized disorder like schizoaffective disorder
2 notes
·
View notes
Note
i have transient psychotic episodes, that usually last only a day or two. obv this isnt enough to warrant a psychotic disorder dx, so im wondering what other disorders have this sort of thing? ive been dx'd with autism and DID, neither of which are psychotic disorders, so im wondering where this comes from? (obviously youre not professionals and not my therapist so its ok if u cant answer!!) thank u!
Hey there! Transient psychotic episodes are common across many disorders honestly, and it's very much a judgement call whether they're severe enough to warrant a diagnosis of a separate psychotic disorder.
Transient psychosis can be a part of schizotypal, bipolar, depression, borderline, arguably schizoid, arguably severe anxiety, OCD, ptsd, (schizophrenia and schizoaffective), psychosis nos and more..
While they aren't officially linked in the current diagnostic journals, the link between autism and psychotic symptoms is also long-standing.
I hope this helped!
Cat
14 notes
·
View notes
Text
Some complicated thoughts on psychosis and previous diagnoses below the cut
TW: gaslighting, psych ward, psychosis, denial?
We were first diagnosed with psychosis at 15. Over the next several years we were officially treated under mood disorder NOS, but the psychosis was a major feature
At 20, we were diagnosed with schizoaffective disorder, bipolar type. At the time, it was a relief. It was comforting to finally have a name for what was happening instead of just NOS.
We were 28 when our life fell apart and the host was confronted by the existence of other parts before going dormant.
Now, at 30, I've been here for just over two years. My memories of our life before 28 are patchy. I have the outline of our life, the bullet point list with some stories added in for flair, but it's like remembering a book i read long ago.
Sometimes, when i start to think about previous diagnoses, i worry that all of this is just a delusion. I don't actually have dissociated parts, I'm just lost in psychosis.
But were we even psychotic back then? I know one of the major symptoms was threatening voices, but was that just persecutory parts? We ended up in the psych ward twice for psychosis. I know at the time, even with the bad aspects of being hospitalized, it was a relief to be there. It felt safer than being home. I don't know why home wasn't safe, just that the hospital felt safer. Was that because we were psychotic and the hospital helped or was it trauma stuff and we just needed to be out of our house?
Were the boy and the girl who came at night to talk and comfort us actually hallucinations or were they parts showing themselves to the host and helping them calm down before bed?
How can I know when all I can remember is the stories of the hallucinations, not the actual experiences?
And this all more complicated because of the way our diagnoses were used against us. At the Manor, B used our diagnoses to convince others that we were just delusional and that what we said she was doing wasn't real. By the time we escaped, we didn't know what was real anymore.
So i recoil from the idea of being psychotic, but i also fear that I am and that this all just a delusion.
8 notes
·
View notes
Photo

So there’s no copy of Berger’s dissertation easily available.
But . . . he does love to talk about it is faux-expertise, so guess what? We can pretty much see what he said.
Local “biblical” “counselor,” Rick Thomas featured Berger’s new expertise on his site. Here are 20 “facts” to know about ADHD from BJU-trained Doctorate in Pastoral Theology (not chemistry, not pharmacology, not psychology) (bolded words are mine and are either ironic or abusive):
The first official label in 1902 was “a morbid defect in moral control” (MDMC), since childlike behavior was socially viewed as a moral issue and not as a medical problem. Words like “bad” are not used to describe a child’s behavior now. Instead, terms like “maladaptive” are the more popular description of a child’s poor and impairing behavior.
ADHD is best described as a subjective social construct that describes 18 undesirable-impairing-normal-childish behaviors and attempts to frame them as a disorder subjectively.
Every behavior listed in the DSM-5 begins with the word “often” to ensure that even the “symptoms” (the 18 behaviors) of ADHD are subjective and based on a person’s opinion. The acceptance of ADHD by many as objective, though it is entirely subjective, works by psychiatrists propagation of a logical fallacy. The American Psychiatric Association has convinced millions that they are experts on alleged abnormalities (such as ADHD) without ever establishing a standard of normalcy.
Not only is the DSM-5 construct subjective, but there is also no valid or reliable means to measure or diagnose a subjective social construct such as ADHD is. Only a person’s personal judgment based upon their observation or another’s testimony is required. When someone says that they “have ADHD,” they are merely stating that they behave in such a way that causes them or their authorities distress. ADHD equals behavior.
Since ADHD is subjective and entirely fluid, it is regularly impossible to win or lose an argument about ADHD. Making matters worse, people label many children under the subcategory of ADHD entitled as “Not Otherwise Specified (NOS),” which determines that children do not even need to meet the subjective listed criteria in the DSM-5 for a diagnosis of ADHD. Children need to be misbehaving in a way that a clinician feels it impairs or distresses the child or his family. This subjectivity regularly leads to clinicians overlooking authentic objective problems that the child may have.
Not all of the 18 behaviors listed as supposed symptoms of ADHD are moral in nature. Some actions, such as “often forgets things of importance,” are normal childlike (and adult-like) amoral behaviors. Others, such as “often gets out of his seat when expected to remain seated” is direct disobedience and not hyperactivity as it is listed in the DSM-5. Because ADHD is subjective, some kids who are diagnosed as having the construct are not sleeping well at night, whereas others are rebellious at heart. It is not fair, therefore, to make blanket statements about the spiritual condition of all children who have been stigmatized with the ADHD label or suggest that ADHD is just a parenting problem. In some cases, that is true, but in other cases—because ADHD is so subjective—a child could have a physical sickness that has been undiagnosed (e.g., ASD).
ADHD does not describe an inability to pay attention; the construct describes a problem of misplaced or immature interest/values. The child labeled can play video games for hours at a time without losing focus. The problem is not an inability to pay attention, but rather, it is a problem of misplaced attention. Attention is naturally a reflection of a person’s values/desires.
The construct of ADHD assumes that healthy children have self-control rather than needing to be taught self-control and trained by the Holy Spirit. The default position of all children is to be like a city without walls that is open to destruction. Only by learning self-control can a child be successful.
Hyperactivity is another name for high energy, which exposes another subjective aspect of the syndrome: “normal” energy levels do not exist from which to suggest a standard let alone to discern alleged deviances. When a person becomes a parent, individuals view his high energy as an asset not as a determinant like when he was a child. Who doesn’t want higher levels of energy? The most successful people in professional sports, in academia, and commerce are often the most energetic. High energy is only viewed as a disorder or impairment when it disrupts an academic setting, causes distress, or hinders success. But such is the result of a lack of self-control and not a problem of high energy.
Unlike the construct of ADHD, when a child has a genuine physical impairment that hinders giving attention (e.g., ASD), he does not selectively offer attention (e.g., the child labeled as ADHD can memorize lines from his favorite movies but not math formulas). In ASD, attentional problems can be observed in all aspects of life and not just those that are not of interest to the child.
ADHD depends on the perspective that “normal children” inherently offer their attention to their authority in a productive way and that children naturally know how and to what to give their attention. These vital lessons are not inherent to the child, and a cursory overview of the book of Proverbs reveals that teaching a child how to pay attention correctly and to what to give his attention are priority number one for the parent/sage.
Research/statistics regularly reveal that many children who are labeled and stigmatized as having ADHD struggle with dyslexia, reading comprehension, are enduring familial problems at home (e.g., divorce, neglect, and abuse), and are sometimes autistic (they have a misdiagnosis of ADHD). They act out further because they are misunderstood, hurting, stigmatized with a psychiatric label that categorizes them as abnormal, and have lost motivation thinking that no hope exists for them.
If ADHD were a valid physical disease with biological markers and an objective etiology, the child could grow out of it according to the DSM-5. The construct of ADHD is listed as a “neurodevelopmental disorder” in the DSM-5, which means that children are merely developing slower than their peers. This type of child was once called a “late-bloomer,” but now late-bloomers are looked at as disordered or degenerated children. If children are late bloomers, they can and will mature with loving direction and the learning of self-control. Through repetition and maturity in desires and pursuits, a child’s brain will conform to the patterns of thinking and behaving he or an authority establishes in his life. When you view a child as normal, this process is called education. When a child is considered disordered, abnormal, or neurologically damaged, this same process is called neuroplasticity. The answer is the same.
Performance enhancing drugs (psychostimulants; e.g., Ritalin and Adderall) that are framed as medicines do not fix an alleged malfunction or balance out neurochemicals. Instead, these powerfully addictive drugs attack the nervous system to produce their effects. Behavioral changes due to the impact of powerful psychostimulants do not prove that ADHD is a valid construct; The results reveal that the drug action of psychostimulants is to stimulate and thus to enhance performance. This reality is why psychostimulants are forbidden in most competitive sports.
Whether labeled or not, taking psychostimulants will enhance a person’s academic and athletic performance, which is why they are one of the most widely abused prescription drugs in America and regularly referred to as “Kiddie Cocaine.”
Psychostimulants regularly cause insomnia, which is known to atrophy the prefrontal lobes and cause attentional problems. Sadly, the child’s alleged problem that these drugs are marketed to correct is to heal the prefrontal lobes where ADHD is supposed to one day be found. The evidence shows, however, that a large portion of children started on psychostimulants end up addicted to the prescribed drugs’ illicit counterparts (e.g., cocaine and meth) later in life. There is also mounting evidence that keeping children on an artificial high produced by psychostimulants causes them to be diagnosed as depressed, psychotic, and manic later in life. These drugs are not healing agents but neurodegenerative drugs. One must ask why a neurodegenerative drug that blocks the healthy function of the nervous system is being given to children who allegedly have a neurodevelopmental problem.
No medical degree, knowledge of biology, or classes in neuroscience are required to diagnose ADHD, as it is a matter of recognizing behavior according to the APA’s standard rather than discovering a disease. This fact exists because there is no physical cause to the construct of ADHD; “No biological marker is diagnostic for ADHD” (DSM-5, 61). Parents, school counselors, behavioral therapists, and teachers—those without medical degrees—typically diagnose ADHD within social contexts, exposing ADHD to be a social construct and not a valid biological disorder. Teachers usually diagnose ADHD according to the child’s behavior (often on a behavioral scale and according to their perspective) and regularly initiate encouraging parents to have their children checked out.
More than not, children labeled as ADHD will become defiant toward their authority and labeled as having ODD. This kind of person is precisely the pattern of the biblical fool that Proverbs warns. When the simpleton becomes a natural fool, he is headed toward becoming a scorner. Oppositional Defiant Disorder (ODD) does not describe a disease, but the natural digression of a child being told he only has to listen to himself and is not responsible for his actions.
Many of the behaviors listed as alleged symptoms in the secular construct of ADHD are in Proverbs as being ordinary foolishness. Scripture understands that poor behavior is the expected activity of the natural fool: “Like a dog that returns to his vomit is a fool who repeats his folly” (Proverbs 26:11). According to Scripture, fools should be expected to repeat their bad behavior.
To deny the secular construct of ADHD as legitimate is not to deny that a child has behavioral problems. Instead, it is to reject the secular attempt to reframe human nature apart from God’s wisdom, and in the process, it is to establish God’s Word as the proper authority and provide hope for these precious children and their families. Proverbs 20:11 exposes that all approaches to a child’s behavior require a presuppositional moral system: “Even a child makes himself known by his acts, by whether his conduct is pure and upright.” People have the freedom to choose which authority to place their faith in discerning children’s behavior. Nonetheless, everyone is judging or diagnosing children by a moral system that evaluates their behavior. ADHD represents the most popular secular moral system currently available.
The summary of Berger’s dissertation, then, is this: I, an untrained person, don’t understand the chemistry or neurology or psychology behind the ADHD diagnosis; therefore, it doesn’t exist. But Proverbs does.
And like a good BJU-trained “pastor,” Berger ends with a sales pitch:
For more information on the construct of ADHD and to see supporting evidence, please purchase my book, The Truth about ADHD, and you may chat with me here.
That’s BJU in a nutshell: Cast stones at something you don’t understand, tout your faux-expertise, and sell your wares.
Is there any difference among BJU, Scientology, or the latest MLM?
#Bob Jones University#Daniel R. Berger II#Biblical Counseling#History of ADHD#TellTheTruth#Moral Problem#BJUisNOTSafe
1 note
·
View note
Last Seen Blogs

sunny-and-moonlight
🌙☀️💫


pa-rou
Parou

reactionimagesdaily
Daily Reaction Images

parallel67979
CAEL2104 YingJun Li