#cholesteatoma
Text
Okay, just in case anyone is curious, I'll say what is going on with my health under the cut.
Tw: Medical Stuff, mentions of dying
So, I probably have cholesteatoma again. It's not 100% but it's most likely. And, unfortunately, it is in a very VERY bad spot. According to the CT scan, there doesn't seem to be anything between my brain and the inside of my ear. Which means it's likely that that part of my skull has been completely eroded. The barrier was already very small from a previous cholesteatoma, so it COULD just be that it was so small it wouldn't show up.
But the bigger issue, at least in my understanding, is the possible cholesteatoma that is next to my corotid artery. This is the main artery that brings oxygen to the brain. That development is new, so it makes me think it can't just be scar tissue. And it is incredibly dangerous. Both to safely remove the cholesteatoma and for the cholesteatoma to be there.
If I have the surgery, I could die. If I don't have the surgery, I will die. And I'm very scared.
My current doctor cannot perform this surgery. It's beyond his skill set. I have to get a doctor in Vanderbilt to perform this surgery. My doctor's office is reaching out to them to get me in with a neurotologist in Vanderbilt, but that could take up to the week. And I feel a bit like a ticking time bomb.
Anyways, if I make it to Thanksgiving this year, I will certainly have one huge thing to be thankful for!
9 notes
·
View notes
Text
#asl#signlanguage#americansignlanguage#hoh#deafpride#deafcan#tiktokcreator#deafawareness#deaf#deafculture#hearingaids#deaftalent#youtuber#chronicillness#rsd#chiari#access#deafgain#cholesteatoma#tiktok
8 notes
·
View notes
Text
Mastoidectomy: Surgical Treatment for Mastoid Bone and Ear Infections
A mastoidectomy is a surgical procedure performed to remove infected or damaged tissue within the mastoid bone, located behind the ear. This procedure is commonly used to treat chronic ear infections that have spread to the mastoid air cells. Mastoidectomy can alleviate pain, prevent complications, and improve hearing for individuals with severe ear conditions.
Why Mastoidectomy is Needed
Mastoidectomy is typically recommended when other treatments, such as antibiotics or ear drops, fail to effectively treat chronic ear infections or when complications arise. Common indications for mastoidectomy include:
Chronic Otitis Media: Prolonged inflammation and infection of the middle ear can spread to the mastoid bone, leading to a condition known as mastoiditis.
Cholesteatoma: A cholesteatoma is an abnormal skin growth in the middle ear that can erode the mastoid bone, potentially causing hearing loss and other complications.
Abscess Formation: Infected pus can accumulate within the mastoid air cells, forming an abscess that requires surgical drainage.
The Mastoidectomy Procedure
During a mastoidectomy:
Anesthesia: The patient is placed under general anesthesia to ensure they are comfortable and pain-free during the procedure.
Incision: The surgeon makes an incision behind the ear to access the mastoid bone.
Bone Removal: The infected or damaged mastoid bone is carefully removed, creating a cavity.
Drainage and Cleaning: Any infected material, pus, or cholesteatoma is removed from the ear and mastoid area.
Closure: The incision is closed with sutures or staples.
Recovery and Rehabilitation
Recovery from mastoidectomy can vary depending on the extent of the procedure and the individual patient. Patients may experience some pain or discomfort after surgery, which can typically be managed with pain medications. It is essential to keep the surgical site clean and dry during the initial healing period. Patients are advised to follow their surgeon's instructions regarding ear care and follow-up appointments.
Benefits of Mastoidectomy
Mastoidectomy offers several benefits:
Infection Resolution: The procedure effectively removes the source of infection, preventing its spread and reducing the risk of complications.
Preservation of Hearing: In some cases, mastoidectomy can help preserve or improve hearing, especially when cholesteatoma or chronic infection has affected the structures of the ear.
Pain Relief: Patients often experience relief from the pain and discomfort associated with chronic ear infections.
REFERENCE:
TX Hospitals Group, Hyderabad is one of the country’s largest and fastest-growing chains of multi-super specialty hospitals.
CONTACT : 9089489089
Book an appointment now
0 notes
Text
Semicircular Canal Fistulas and Hearing Loss. Single Surgeon’s Experience by Stefano Dallari*

Abstract
Fistulas of the lateral semicircular canal may occur mainly in cholesteatoma cases, both as consequence of the disease and an excessive or inadvertent drilling of the bone. The risk of significant hearing loss had been stressed, especially in the past. More recent experiences have shown that a careful approach allows to save the pre-operative hearing in the majority of the cases, even when the cholesteatoma matrix is removed from the fistula and the canal is plugged. The author presents his experience in 22 cases collected since year 1989.
Keywords: Labyrinthine Fistula; Hearing Loss; Cholesteatoma
Introduction
Fistulas of the semicircular canals may be primitive or follow an erosive process of the endochondral bone of the labyrinth. A type of primitive/malformation fistula involves the superior canal and may show up as Minor's Syndrome [1]. Also, the posterior semicircular canal may be involved, in rare cases associated with a high-riding jugular bulb and fibrous dysplasia [2]. Secondary fistulas generally follow a middle ear infection, most of the cases a cholesteatoma [3].
An iatrogenic origin should also be taken into account, as a consequence of an excessive drilling during a middle ear surgical procedure [4]. Because of its anatomical location, the lateral semicircular canal is normally involved. As reported in the literature, a fistula of the semicircular canal brings a variable, often high risk of hearing loss until anacusis, due to the damage to the membranous labyrinth [5]. The crucial point is the injury to the endosteum of the canal, while its blue lining is considered safe. When dealing with fistulas due to a bony erosion caused by a cholesteatoma, removal of the matrix may lead to open the endosteum. This is why, especially in the past, for fistulas of more than 2 mm, leaving a piece of matrix in place, over the fistula, used to be advised [6]. It had also been demonstrated that, at a second look operation, most of the time this piece of matrix disappears into normal mucosa.
Conversely, in the more recent literature there have been several suggestions for a careful but complete removal of the matrix, with immediate coverage of the fistula with autologous tissue, even until the obliteration of the canal itself [7,8,9].
The Author’s attitude has always been a careful removal of the pathology and, in regards to the matrix, the decision of completely removing it or leaving a piece over the fistula was based upon the size of the fistula but also the easiness of detaching the matrix from the endosteum. When the detachment seemed to be too difficult, a piece of matrix and/or inflammatory mucosa was left over the fistula itself. The Author’s series was revised mainly in the light of the audiologic outcome and the results will be hereby reported.
Materials and Methods
From 1989 up to December 2019 the Author performed 111 tympanoplasties (TPLs) for cholesteatoma (65 males and 46 females), 39 TPLs for other diseases (28 males and 11 females) and 8 “radical” operations (4 males and 4 females). In 22 cases (15 males and 7 females), a fistula of the lateral semicircular canal was detected (18 cases) or provoked (4 iatrogenic cases). In Table I all these 22 cases are described. Several items have been taken into account: sex, age at operation, ear pathology, year of surgery, pre-operative imaging availability, state of the facial nerve (covered, exposed, pre-operative presence of palsy), state of the semicircular canal, in accordance with the classification of Dornhoffer and Milewski [10], simplified (simple bone erosion with presence of a “blue line”, type I; bony fistula with endosteum exposed and closed, type II or open, type III), type of operation performed, pre-operative hearing (air conduction between 500 and 4000 Hz), post-operative hearing (air conduction between 500 and 4000 Hz) and post-operative bone conduction (0.5,1,2,4 kHz) as compared with the pre-operative one.
Results
The results will be hereby globally analyzed. Furthermore, six cases will be reported and documented, to illustrate the various scenarios. The series consists of 22 patients, 15 males (mean age 52 years) and 7 females (mean age 46 years).
Over the whole number of cases, the incidence of fistula is 14 % (22/158). All the cases but one had a middle ear cholesteatoma. The sole non-cholesteatoma case was an iatrogenic one. Thus, the percentage among the cholesteatoma cases is 21/111 (19 %). In 11/22 patients a pre-operative CT had been performed. In all cases but one (case n. 3 of the year 1991), where a complete fistula was present, with endosteum exposed, the exam was positive for fistula. For the three cases with bony erosion (blue-lined canal) caused by the pathology, imaging was not available. In the iatrogenic cases the CT was negative. In regards to the facial nerve, it was exposed in 13/22 cases and closed in the remaining 9/22. In all the four cases where the endosteum was open, the facial nerve was exposed. None of the cases had a pre-operative palsy, neither post-operative. The case n. 22 presented with a facial palsy grade V which was confirmed not to be due to the pathology (adenoma of the middle ear), but to be incidental. The palsy completely recovered after three months.
Coming to the conditions of the semicircular canal, in 4/22 cases (18 %) there was a complete fistula with the endosteum open. The presence of the matrix of the cholesteatoma onto the canal was mentioned in only one of these four cases (case n. 18), where it was removed, in presence of an open endosteum (see description of the case). In 9/22 cases (41 %) the endosteum was exposed, closed. For these cases the operation report did not mention if the fistula was covered by the matrix of the cholesteatoma. Conversely, the presence of the matrix over the canal was reported in further 5/22 cases besides the case n. 18 (see before), for a percentage of 27 % (6/22). It was removed in 3/6 cases, leaving an intact endosteum in two cases and an open one in the case n. 18, and left in situ in 3/5 cases. Finally, in 3 cases (n. 8, 9 and 16), there was a simple erosion of the bone with a blue-lined canal. The ”iatrogenic cases” are 4/22 (18 %): the n. 12 (endosteum exposed, closed, due to excessive drilling); the n. 14 (bone erosion due to the curette-removal of hyperostotic bone over the lateral semicircular canal); the n. 19 (endosteum exposed, closed, due to excessive drilling); the n. 22 (bony fistula with endosteum intact, due to delayed anatomical recognition).
In 14/22 cases (64 %) an open TPL was performed, while a closed TPL was carried out in 5/22 cases (23 %). In the remaining 3/22 cases (14 %) the fistula was detected during a revision of closed TPL which was converted to an open one. Post-operative audiologic data were available for 14/22 patients. Among Figure 1: Case n. 15. The left lateral semicircular canal is absent in his superomedial aspect. The endosteum is exposed and open. A piece of absorbable gelatin is ready to seal the hole. The facial nerve is exposed. these 14 patients there were 3 of the four patients with a fistula with open endosteum. None of them had a worsening of the bone conduction. Only in 1/14 patients with post-operative hearing data, there was a deterioration of the bone conduction curve. It was the case n. 12, iatrogenic, with endosteum exposed, closed. Furthermore, the author does not remember a case of total hearing loss in this group of patients.
(a): Iatrogenic maneuver
(b): The patient was operated on, twelve month later, for the
II stage. The zone of the fistula appeared close with neo-bone
(c): Iatrogenic maneuver
(d): Iatrogenic maneuver
(e): The patient had been operated on for closed TPL I stage in
2013, for intact TM cholesteatoma. At that time the facial nerve
was closed and no lateral scc erosion was present
(f): The patient presented with a right facial paralysis grade V,
not related to the ear pathology. He completely recovered three
months after the operation
(g): Iatrogenic maneuver
Clinical Cases
Case n. 15
(Fig. 1) R.M, male, 69-year-old. Long history of left hearing loss. In September 2005 he suffered for an acute episode of vertigo. The ENT workout confirmed a significant left mixed hearing loss. The CT of the ear showed an opacification of the whole middle ear with erosion of the lateral semicircular canal. He underwent surgery in November 2005 and a huge bony fistula, with endosteum open, was confirmed. The facial nerve was exposed in the tympanic segment and covered by the cholesteatoma matrix. An open TPL was performed and the fistula was cleaned and then repaired with absorbable gelatin+ bone+ fascia. The operation was uneventful, with no vertigo and the 48-hour post-operative bone conduction curve was unchanged. The patient recovered well and was lost to follow-up. Information acquired for this paper says that the patient is still alive and his ear situation is stable with no further problems.
Case n. 17
(Fig. 2) G.G., male, 62-year-old. History of left hearing loss. Before referring to us, in the beginning of year 2008, he suffered for recurrent episodes of peripheral vertigo. A CT showed a diffuse involvement of the left middle ear with a probable fistula of the lateral semicircular canal. There was a significant mixed left hearing loss. The patient underwent surgery in April 2008. An erosion of the bony semicircular canal was confirmed. It was covered by the matrix of the cholesteatoma, which covered also the facial nerve, exposed along the whole tympanic segment and second genu. An open TPL was performed, leaving a piece of the cholesteatoma matrix/inflammatory mucosa onto the fistula. The post-operative evolution was good. No worsening of the bone conduction occurred. The patient has been recalled in the occasion of this paper. Under otomicroscopic examination a well done and healthy open TPL cavity was evident, with adequately-sized meatoplasty. There was a mixed hearing loss with the air conduction significantly better than after the operation, while the bone conduction had worsened, with a reduction of the air-bone gap. The patient was extremely satisfied, saying that after the operation he had no more problem, especially no more vertigo episodes nor dizziness. He mildly complained of the earing loss but does not require a hearing aid. He is still working.
Figure 1: Case n. 15. The left lateral semicircular canal is absent in his superomedial aspect. The endosteum is exposed and open. A piece of absorbable gelatin is ready to seal the hole. The facial nerve is exposed.
Figure 2: Case n. 17. Upper row: At the axial (left) and coronal (right) CT view, an erosion of the left lateral semicircular canal is evident. Lower row: A piece of mucosa is left over the semicircular canal bone erosion and also partially over the exposed facial nerve.
Case n. 18
(Fig.3) L.C., male, 62-year-old. Seen in the year 2008 for right chronic otitis media with discharge and evidence of cholesteatoma. The CT confirmed the involvement of the middle ear and showed an evident amputation of the lateral semicircular canal. He had a low-to-medium-grade mixed right hearing loss with a small air-bone gap. The patient was operated on in May 2008. A bony fistula, covered by the cholesteatoma matrix was detected. The matrix was carefully removed and an opening in the endosteum was found. This was immediately sealed with fascia + bone pate. The facial nerve was widely exposed, from the cog to the second genu. An open TPL with an ossicular reconstruction (titanium PORP) was performed. The post-operative outcome was good. The patient had no vertigo and a bone conduction control after 10 days showed no worsening of the curve. The patient recovered well and the hearing level remained as it was pre-operatively. He was strictly followed and ten months later a mastoid recurrence of the cholesteatoma was removed. Over the years the ear has remained stable, with a dry small perforation of the new-TM. As a piece of information, all the patients operated by the Author for open TPL are advised to clean the operated ear, at least twice a week, with a warm boric or boricsalicylic solution [11]. In regards to the hearing, the bone curve was unchanged after seven months following the revision surgery, then started to deteriorate. At the most recent control, in April 2020, the ear is persistently stable but the hearing has worsened to a middle-to-high grade mixed hearing loss.
Figure 3: Case n. 18. Upper row: CT axial view. Middle row: CT coronal view. A wide opening of the right semicircular canal is evident. Inferior row: the superomedial half of the bony right lateral semicircular canal is absent. After careful matrix removal the endosteum is exposed and open.
Case n. 19
(Fig.4) F.D., female, 47-year-old. She suffered for recurrent right ear discharge since her childhood, with hearing loss. In the year 2011 the situation worsened and the patient saw an ENT specialist who detected the presence of cholesteatoma, requested a middle ear CT and referred her to the author. There was a conductive hearing loss with a substantially normal bone conduction. The patient underwent surgery in February 2012. A posterior-superior bony erosion with granulation tissue and cholesteatoma was detected. The ossicular chain was involved by the cholesteatoma and blocked. The mastoid was contracted and poorly pneumatized. The facial nerve was exposed at the second genu. An open TPL was planned and performed. During the bone-drilling, the endosteum of the lateral semicircular canal was exposed to a grade where the gently pushing on the stapes provoked a bulging of the endosteum itself. The bony erosion was immediately sealed with bone pate and the operation concluded uneventfully. No ossicular reconstruction was performed. The patient had no problem and she has been regularly followed. The hearing remained as it was before the operation. She always refused to undergo a reconstructive/ functional operation. The most recent control was performed in February 2020.
Figure 4: Case n. 19. Upper row. CT, axial view (left) and coronal view (right). The right semicircular canal is covered by bone. Lower row. The excessive drilling has exposed the endosteum of the right lateral semicircular canal. Pressing onto the footplate causes a movement of the endosteum itself.
Case n. 20
(Fig.5) S.G., male, 47-year-old. Referred to the author in February 2012 with an history of recurrent right ear discharge for several years. A previous ENT examination showed an erosion of the scutum with granulation tissue and cholesteatoma. A CT confirmed the involvement of the middle ear and a probable fistula of the lateral semicircular canal. There was a mild conductive right hearing loss. The patient underwent operation in March 2012. There was a huge tympanic-mastoid cholesteatoma. After careful removal of the matrix, a bony erosion of the lateral semicircular canal was detected. The endosteum appeared to be covered by a minimum slice of bone and there was no mechanic transmission when gently pushing onto a mobile stapes. The facial nerve was covered/closed. An open TPL was performed with ossicular reconstruction (titanium PORP). The patient did well and post-operative hearing was improved and grossly normal. The patient was lost to follow-up and recalled for evaluation in June 2020. He reported a good and stable condition of his right ear for the first six post-operative years. In the last two years, instead, he suffered for recurrent inflammations and underwent ENT examinations without significant results. A CT was suggested and performed at the beginning of year 2020. Despite the surgical cavity was filled with crusts and epithelial debris, it seemed to observe a regeneration of the bone over the lateral semicircular canal. The patient was followed by the author and the local situation led to healing. An audiogram performed on August 24, 2020, showed a mild conductive right hearing loss (500 to 4000 Hz: 35,35,50,50), with bone conduction still normal.
Figure 5: Case n. 20. Upper row: CT axial view (left) and coronal view (right). It seems to be a thin bony remnant over the right lateral semicircular canal. Lower row: after careful cholesteatoma matrix removal (left), a bony erosion is evident with nearly exposure of the endosteum (right, white arrow).
Case n. 22
(Fig.6) M.S., male, 22-year-old. In May 2017 the patient had a documented episode of pure conductive hearing loss (50-45 dB from 500 to 4000 Hz) and tinnitus, with a tympanogram type B, which completely recovered within a month after local and general steroid therapy, and was interpreted as serous otitis media. A further control in July 2017 confirmed a normal hearing and a type A tympanogram. In February 2020 the patient was seen at the author’s institution with an acute right facial palsy (grade V, House-Brackman scale). He complained of few symptoms in the ear but a hearing loss. At endoscopic and otomicroscopic examination, a posterior-superior bulging of the tympanic membrane (TM) was observed and an explorative myringotomy was performed which was substantially negative. Both a CT and MRI of the ear were obtained, showing a complete opacification of the middle ear with mastoid inflammation. Besides the suspect of a middle ear inflammation with subsequent irritation of a congenitally dehiscent facial nerve, the hypothesis of a tumor of the facial nerve was also taken into account. An explorative tympano-mastoidectomy was then performed on February 20, 2020. The facial nerve turned out to be closed and the antral-attic mass was histologically diagnosed as “adenoma”. In order to remove this thick and adherent tissue, a posterior tympanotomy was planned. During the drilling, and because of the presence of the pathologic tissue, an excessive thinning of the bone over the lateral semicircular canal was realized only when a complete aperture of the bone had occurred. Fortunately, a thick endosteum was still intact and the bony fistula was immediately sealed with bone pate. In order to completely remove the pathology, the posterior bony wall was temporarily removed, then repositioned and stabilized with bone pate + fibrin glue. A first stage closed TPL was thus accomplished. The patient had mild vertigo for three days. A bone conduction control was performed 4 and 6 days postoperatively and it was as before the operation. The patient was then followed and the last control was at June 2020. The healing was completed with a well oriented and trophic tympanic membrane. A 50-60 dB conductive hearing loss was detected, as normal after first stage TPL. The facial palsy completely recovered. The patient still complains of episodic short spins of unbalance. An MRI control has been planned.
Figure 6: Case n. 22. Upper row: CT axial view (left) and coronal view (right). The right lateral semicircular canal is closed. Lower row: the excessive drilling over the right lateral semicircular canal has been recognized when the endosteum was already exposed. Black star: pathologic tissue (adenoma).
Discussion
As easy to understand, erosions of the lateral semicircular canal with exposure of the membranous labyrinth (endosteum) and even rupture of it, happen in the great majority of cases when dealing with a cholesteatoma of the middle ear. An exposed facial nerve is also a common finding and its frequency easy to understand as well.
Significant hearing loss has to be taken into account when dealing with a fistula of the lateral semicircular canal. It may happen also when the post-operative fistula test is negative. This is what reported by Yeho et al. (2004) [4], in the two cases of iatrogenic fistula they could observe. Besides the incomplete reliability of such maneuver, it may also mean that this negativity was caused by a hypofunction of the damaged labyrinth but, finally, also that the auditive (cochlear) partition is more sensible than the vestibular one. Surgically created (iatrogenic) fistulas have been reported to occur in 0.1% of the cases or less, with a good hearing outcome in the majority of such patients [12].
In the author’s series the percentage of iatrogenic fistula is 2.5 % (4/22) and the good hearing outcome is confirmed. It is the author’s opinion that the rate of occurrence is probably higher than reported in the literature, where the Authors generally present such cases without mentioning the number of their whole series [13]. The prevalence of the fistulas of the lateral semicircular canal, instead, in the author’s series, is 14 % (22 cases over 158 patients), which rises to 19 % when considering the sole cholesteatoma cases (21/111). Naderpour et al. (2008) [14] examined series from the year 1978 to the year 2000 and the percentage varies from 2.9% to 21%.
More recently Meyer et al. (2016) [3] report a prevalence of 6 % in their series, with a huge number (16/42) of type I fistulas, that is a simple bone erosion, according to the classification of Dornhoffer and Milewski [10].
The percentage reported by Rosito et al. (2019) [5] is 2.7 %. These authors considered only the type II (endosteum exposed) and III (endosteum exposed and open). In the Author’s series, when considering the sole cases with open endosteum (type III), the percentage is 2.5 % (whole series, 4/158) or to 3.6 % (cholesteatoma cases, 4/111). Adding the type II cases (9/22), the percentage rises to 8.2 % (whole series, 13/158) or 11.7 % (cholesteatoma cases, 13/111). Because the main purpose of this paper was to evaluate the audiological effects caused both by a spontaneous exposure of the membranous labyrinth or by its inadvertent uncovering by excessive bone removal, all the three types of fistula were considered. Indeed, the aim was to test the mechanical and noise effect that an excessive drilling and any manipulation (palpation, suctioning, cleaning), even careful, might cause. In regards to these effects, the results seem to be good. Even though the numbers are small, the sensorineural hearing outcome (bone conduction) was encouraging and a post-operative deterioration was observed in only one case.
Satisfactory hearing results seem also to confirm that a careful manipulation and removal of the cholesteatoma matrix is a significantly safe maneuver, as it is in regards to an exposed facial nerve. None of the author’s patients with an exposed facial nerve, in fact, developed a post-operative palsy. The author has no experience of the complete obliteration of the semicircular canal, which too seems to be a safe maneuver in regards to hearing preservation
Conclusion
When dealing with a middle ear cholesteatoma, the possibility of finding a fistula of the lateral semicircular canal, as well as an exposed facial nerve, has always to be kept in careful account. This was mandatory when imaging was not routinely obtained and before the CT era. Nonetheless, even though high quality CTs allow an easier detection of the bony erosions, attention must constantly be paid as well. In regards to how to manage the fistula, the ongoing experience has validated the strategy of a careful removal and an immediate seal of an eventual open endosteum, with biologic means. Also, a complete obliteration of the canal has proved to be safe. As reported in the literature and also in the author’s experience such a careful attitude reduces the risk of sensorineural hearing loss to a minimum. Furthermore, in the author’s opinion, the choice of leaving a piece of matrix on top of a wide bony erosion, which appears to be soft at a careful palpation, is still an advisable option (mandatory in the case of the only hearing ear), trusting in its mucosal transformation, as seen during second look operations.
Acknowledgment
The author wishes to thank Massimo Giuliano Bonetti, MD (Neuroradiology Unit, Department of Radiology, “A. Murri” Hospital, Fermo, Italy) for his valuable help in the choice of.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-cr-id-00145/
https://ijclinmedcasereports.com/pdf/IJCMCR-CR-00145.pdf
0 notes
Text
A cholesteatoma (koleszteatóma) vagy gyöngydaganat a középfül krónikus, gennyes gyulladása, amelyet a hallójáratból származó sarjadzó laphám (egy szövetfajta) összegyűlése okoz. Ez a jóindulatú daganat kizárólag műtéttel gyógyítható. A betegek kis részénél azonban a műtét nem lehetséges.
Nálam sem. Szoknom kell a gondolatot.
7 notes
·
View notes
Text
How a Tinnitus Specialist Perth Can Help
Earwax build-up, middle ear infections and structural abnormalities can all cause conductive hearing loss. These issues can be addressed through medical or surgical intervention and hearing aids. However, you should seek guidance from a Perthbased hearing specialist for personalised recommendations.
Most tinnitus cases are fully treatable. If your tinnitus is caused by another health issue, treating that condition should also take care of the tinnitus.
Conductive hearing loss
Conductive hearing loss is when a tinnitus specialist perth in the outer or middle ears prevents sound from travelling efficiently through them to the inner ear or the cochlea. It can also occur when fluid build-up in the middle ear impedes sound from passing through the ear canal, ear drum or the tiny bones of the middle ear (the malleus, incus and stapes).

Unlike sensorineural hearing loss, which can be permanent, many conductive conditions are treatable and often resolve with medication, a visit to an ENT specialist or surgical treatment. For example, ear wax removal, a middle ear infection and cholesteatoma are all conditions that can be treated with surgery and medical management.
In most cases, a full and thorough hearing assessment will be conducted in our clinic to determine the cause of your conductive hearing loss. This will include an audiogram and may also require additional diagnostic tests including CT or MRI scans. These will identify the severity of your conductive hearing loss and the best option for you to move forward.
Earwax
Despite the odd texture and smell, earwax (also known as cerumen) plays an important role in keeping the ears healthy. It is a natural product made by glands in the ear canal that combine secretions from sweat and sebaceous glands with dead skin cells.
These lubricate and protect the skin inside the ear canal, and help ward off infection. However, too much earwax can cause problems, such as itching or blockage. In addition, earwax can clog the eardrum, causing hearing loss.
Unfortunately, people’s good intentions to clean their ears often result in a build-up of earwax. For example, using cotton swabs to “clean” the ears actually stimulates the body’s production of more earwax, which then builds up and creates the blockage the person was trying to prevent. In some cases, a doctor may recommend the use of ear drops to soften earwax so it can come out on its own. However, it is never a good idea to try home remedies like ear candling or sticking anything foreign into the ear.
Middle ear infections
Most kids get at least one middle ear infection (otitis media) by the time they’re 3 years old. This happens when viruses or bacteria infect the fluid behind the eardrum. Your child may have a sore throat, cough, runny nose, or fever when this happens. Sometimes sticky fluid stays in the middle ear after the infection clears up. It can prevent your child from hearing well and can cause problems with eating and sleeping. Talk to your doctor if your child has persistent problems with their ears.
Your ear, nose, and throat (ENT) doctor can diagnose middle ear infections with a physical exam and a test called tympanometry. During this test, the doctor blows puffs of air into your ear to see how the eardrum moves. When the eardrum is filled with fluid, it doesn’t move as easily. Your doctor might also order a blood test to check for certain types of bacteria. They might also use a computer tomography (CT) scan or a specialized instrument called a ctympanometer to measure how the eardrum responds to changes in air pressure.
Hearing aids
If you find that your ear works is getting in the way of your daily life, it might be time to consider hearing aids. Our team have fitted tens of thousands of patients with hearing aids who are able to live their lives again with confidence and ease.
Tinnitus is a sound that is often described as ringing, buzzing or humming in the ears and head. It can be continuous, come and go, vary in pitch, and be located in one or both ears. It can cause problems such as annoyance, stress, fatigue, sleep disturbance and loss of concentration.
To diagnose tinnitus, your doctor will review your symptoms and perform a physical exam. He may also order an audiometry test and an imaging technique, such as a CT scan. In addition, your doctor might want to draw blood for lab tests to check for underlying conditions, such as anemia or thyroid issues. He might also recommend that you avoid certain medications if they might be the source of your tinnitus.
0 notes
Text
Looking for a Top-Rated ENT Surgeon?

Finding the right doctor for your ENT (ear, nose, and throat) needs is crucial. If you're in Delhi and searching for an experienced and qualified ENT surgeon, look no further than Dr. Nayeem Ahmad Siddiqui at DIYOS Hospital.
About DIYOS Hospital
DIYOS Hospital is a leading healthcare facility in Delhi, known for providing personalized care and advanced ENT services. Their team of highly skilled doctors utilizes the latest technology to deliver exceptional patient outcomes.
Dr. Nayeem Ahmad Siddiqui: Your Trusted ENT Specialist
Dr. Siddiqui is a senior ENT consultant at DIYOS Hospital with over 19 years of experience. He is a highly regarded ENT surgeon known for his expertise in various procedures, including:
Micro-ear surgery: This minimally invasive technique treats a range of ear conditions, such as chronic otitis media, cholesteatoma, and tympanoplasty.
Nose surgery (Rhinoplasty): This surgery can address functional issues affecting breathing or improve the cosmetic appearance of the nose.
Throat surgery: Dr. Siddiqui performs various throat surgeries, including tonsillectomy, adenoidectomy, and thyroidectomy.
What Conditions Does Dr. Siddiqui Treat?
Dr. Siddiqui offers comprehensive ENT care, treating a wide range of conditions, including:
Sinus problems, such as sinusitis and nasal polyps
Ear infections
Hearing loss
Allergies
Thyroid disorders
Sleep apnea
Snoring
Personalized Care at DIYOS Hospital
At DIYOS Hospital, Dr. Siddiqui and his team prioritize personalized care. They take the time to understand your individual needs and concerns before recommending the most suitable treatment plan. Whether you require medication, minimally invasive procedures, or surgery, Dr. Siddiqui will guide you through every step of the process.
Advanced ENT Services
DIYOS Hospital is equipped with advanced diagnostic and treatment technologies, allowing Dr. Siddiqui to provide the most effective care for his patients.
Considering ENT Treatment?
If you're experiencing any ENT-related issues, scheduling a consultation with Dr. Nayeem Ahmad Siddiqui at DIYOS Hospital is a great first step. Dr. Siddiqui's expertise, combined with DIYOS Hospital's commitment to personalized care and advanced technology, can ensure you receive the best possible treatment for your condition.
Don't hesitate to schedule an appointment with Dr. Nayeem Ahmad Siddiqui today to discuss your ENT concerns and explore treatment options. Also, If you want to learn more about ENT Hospital in Safdarjung Enclave please visit the website.
0 notes
Text
Cholesteatoma Treatment in Kolkata
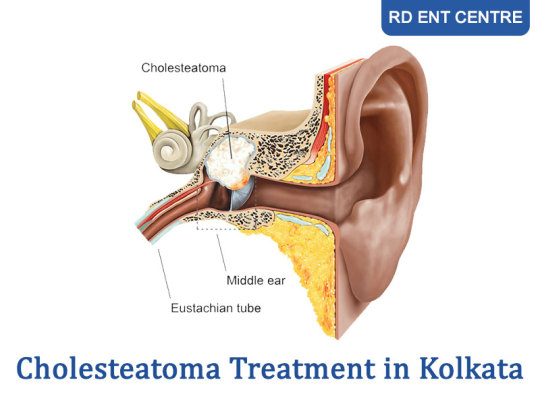
Cholesteatoma is a type of cyst or abnormal skin growth that can develop in the middle ear behind the eardrum. It typically occurs as a result of repeated infections, chronic inflammation, or a perforation (hole) in the eardrum. Cholesteatomas can vary in size and can cause damage to the structures of the middle ear, including the bones responsible for hearing and balance, if left untreated.
Symptoms:
Persistent or recurrent ear infections
Ear pain or discomfort
Hearing loss, which may be gradual
Tinnitus (ringing in the ear)
Drainage from the ear, which may have a foul odor
Vertigo or dizziness
Treatment:
Your doctor might prescribe medicines for treating your condition but surgery is also a very common treatment for cholesteatoma. Get an appointment from the Best ENT surgeon in Kolkata only at RD ENT CENTRE. Visit the official website for more information.
#best ent surgeon near me#best ent doctor near me#ent specialist near me#best ent specialist in kolkata#best ent specialist in mumbai#best ent surgeon in kolkata#best ent doctor in kolkata#rd ent centre
0 notes
Text
WHAT IS MASTOIDECTOMY?

A Mastoidectomy is a surgery on the mastoid bone which is a part of the Temporal Bone- The temporal bone houses the ear.
In Mastoidectomy the mastoid bone is drilled in order to clear disease, create access, make the ear safe from dangerous diseases like Cholesteatoma, and give access for other surgeries including introducing a Cochlear Implant.
#Mastoidectomy#EarSurgery#ENTProcedure#MastoidBone#TemporalBone#Cholesteatoma#EarHealth#SurgicalAccess#CochlearImplant#ENTSpecialist#MedicalProcedure#HealthcareInnovation#SurgicalTreatment#EarSafety#DiseaseClearance#HealthcareProcedure#EarHealthAwareness#HealthcareExplanation#PatientEducation#SurgicalAccess
#ent#ent doctor#ent delhi#ent medicines#ent treatment#ent doctor in vasant vihar#entdoctor#surgeon#ent surgeon
0 notes
Text
I may or may not have a fever. No clue, I don't have access to a thermometer.
If I do have a fever, I'm betting that the consistent dizziness and nausea paired with agonizing pain in my ear over the last two weeks is probably an ear infection growing bacteria no one's ever heard of.
Which is actually good news because it means it's probably not cholesteatoma. Which would be much worse.
Just got a ride it out for another 8 days before I can go to the doctor.
5 notes
·
View notes
Text
#asl#signlanguage#americansignlanguage#hoh#deafpride#deafcan#tiktokcreator#deafawareness#deaf#deafculture#hearingaids#deaftalent#youtuber#chronicillness#rsd#chiari#access#deafgain#cholesteatoma#tiktok#deaf awareness
11 notes
·
View notes
Text
Mastoidectomy with tympanoplasty
Tympanoplasty with Mastoidectomy-various aspects-
Mastoidectomy with tympanoplasty
A tympanomastoidectomy combines a tympanoplasty with a mastoidectomy, two surgical operations frequently carried out simultaneously on a patient's ear to treat a persistent infection and improve hearing.
Surgery of Tympanoplasty with Mastoidectomy
Mastoidectomy is the part of the procedure where the surgeon removes the cholesteatoma matrix (diseased air cells) from the mastoid bone. The temporal bone, which is situated at the sides and base of the skull behind the ear, contains these sick cells behind the honeycombed hollow (mastoid)- for further information pl click on the link given below-
1 note
·
View note
Text
Five steps of Wikipedia for Wednesday, 6th December 2023
Welcome, laipni lūdzam, ողջու՜յն (voġčuyn), добредојде (dobredojde) 🤗
Five steps of Wikipedia from "Balloon Eustachian Tuboplasty" to "Aditus to mastoid antrum". 🪜👣

Start page 👣🏁: Balloon Eustachian Tuboplasty
"The Balloon Eustachian Tuboplasty (BET) is a minimally invasive procedure for the causal treatment of Eustachian Tube Dysfunction (ETD), an often-chronic disorder in which the regulation of middle ear pressure and the removal of secretions are impaired. The dysfunction often causes significant..."
Image licensed under CC BY-SA 4.0? by Magnus Maier
Step 1️⃣ 👣: Eustachian tube dysfunction
"Eustachian tube dysfunction (ETD) is a disorder where pressure abnormalities in the middle ear result in symptoms...."
Step 2️⃣ 👣: Cholesteatoma
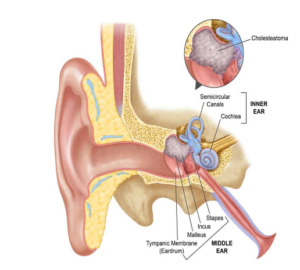
"Cholesteatoma is a destructive and expanding growth consisting of keratinizing squamous epithelium in the middle ear and/or mastoid process. Cholesteatomas are not cancerous as the name may suggest, but can cause significant problems because of their erosive and expansile properties. This can result..."

Image licensed under CC BY 2.5? by welleschik
Step 3️⃣ 👣: Base of skull
"The base of skull, also known as the cranial base or the cranial floor, is the most inferior area of the skull. It is composed of the endocranium and the lower parts of the calvaria...."
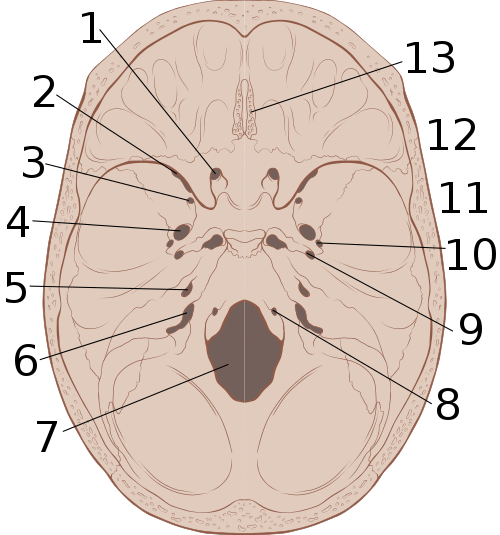
Image licensed under CC BY 2.5? by Patrick J. Lynch, medical illustrator
Step 4️⃣ 👣: Carotid groove
"The carotid groove is an anatomical groove in the sphenoid bone located above the attachment of each great wing of the sphenoid bone. The groove is curved like the italic letter f, and lodges the internal carotid artery and the cavernous sinus...."

Image by Henry Vandyke Carter
Step 5️⃣ 👣: Aditus to mastoid antrum
"The aditus to mastoid antrum (otomastoid foramen), is a large, irregular opening upon the posterior wall of the tympanic cavity by which the mastoid antrum (situated posteriorly) communicates with the epitympanic recess of the tympanic cavity (situated anteriorly). The walls of the antrum are lined..."
Image by Henry Vandyke Carter
0 notes
Text
20 Sep 2023
20th September 2023, Wednesday
Listening: Bad Habit, Foals
Sooo glad things got better. Work was okay. Instagram memories reminded me of my cholesteatoma surgery in 2014!! 🤩

Went through my diary here and I found this, this, this, this, this! It makes me super glad that I documented stuff!
0 notes
Text
The Significance of Mastoidectomy in Ear Health
Mastoidectomy is a critical surgical procedure that plays a pivotal role in addressing various ear-related conditions. Here's a closer look at its importance in the treatment of specific ear ailments:
Chronic Ear Infections:
Chronic ear infections, medically termed chronic otitis media, can inflict persistent pain, hearing impairment, and recurrent infections. When conventional treatments prove ineffective in resolving the root problem, mastoidectomy emerges as a viable solution. Mastoidectomy Surgery involves the removal of infected tissue to ameliorate the condition and alleviate its debilitating effects.
Cholesteatoma:
Cholesteatoma denotes the abnormal growth of skin cells within the middle ear. This condition poses a significant risk of eroding the bones and structures within the ear, potentially leading to hearing loss and other complications. To curtail the progress of cholesteatoma and avert further harm, medical practitioners often opt for mastoidectomy to surgically excise the problematic tissue.
Complications Arising from Acute Otitis Media:
Acute otitis media, commonly referred to as an ear infection, can occasionally escalate into severe complications such as mastoiditis or the formation of abscesses. When confronted with these dire situations, the intervention of mastoidectomy becomes imperative. This procedure aids in draining the abscess and eliminating infected tissue, thereby thwarting the spread of the infection and safeguarding the patient's overall ear health.
In conclusion, mastoidectomy serves as a pivotal tool in the arsenal of treatments for various ear-related conditions. It provides relief and restoration of ear function for individuals plagued by chronic ear infections, cholesteatoma, and complications stemming from acute otitis media. By addressing these issues through mastoidectomy, medical professionals can enhance the quality of life for their patients and mitigate the potential long-term consequences of these conditions.
1 note
·
View note
Text

Mastoidectomy is a surgical procedure performed to remove infected or damaged tissue within the mastoid bone, located behind the ear. It is typically done to treat chronic ear infections, cholesteatoma (abnormal skin growth in the middle ear), or complications stemming from ear infections. During the procedure, an ENT (Ear, Nose, and Throat) surgeon removes the infected tissue to prevent further spread of infection and preserve hearing. This surgery should only be performed by a skilled and experienced ENT surgeon due to the delicate nature of the ear's anatomy and the potential for hearing-related complications.
0 notes
Last Seen Blogs

mariaoglesbyart
Tempest Scribbles

emmanuel-eternal-wanderer
Explore, Try, Feel

lordxxaizen
' All a part of my plan '

ymytrb-blog
Milly

shaniceinwonderlandx
robber emoji