#variegate porphyria
Text
Abide
a space of naked skin,
pale as sour milk, at the
crown of my head, hair
falling like spiderwebs
covering nothing
my liver swells past the
boney constraint of ribs,
a hardness that calls my
fingers to rest there,
a blind of fingers and palm
this lump of flesh presses down,
intruding into empty space,
into my bladder and bowel --
both scream urgency, even
empty, they are haunted
the vertigo crashes over me
like ocean, dredging up scattered
light, fractured seizures, the
rattling breath of dying neurons
i am a house, falling
cobwebs and cages, rickety beams
and the wail of lost souls, lights
flickering, death making his
inspection, finding the rot
yet still, i live
yet still, i abide
#poetry#spilled ink#inkstay#poetryriot#writerscreed#poem#poets on tumblr#twcpoetry#allpoetry#lupus#systemic lupus erythematosus#living with lupus#variegate porphyria#porphyria#chronically ill#chronic illness#actually diabetic#hair loss
12 notes
·
View notes
Text
Mystic's Random Research; irl "vampires"
Fun fact! there's an actual disease/disorder that mimics vampirism.
read below the cut, also note this will talk about a blood & skin disorder
The Porphyria blood disorder group has traits that're known from vampirism, and includes disorders such as Porphyria cutanea tarda (PCT), Variegate porphyria, Acute intermittent porphyria, and more. I'll be talking about PCT in specific & Porphyrias in general.
Acute Porphyrias affect mostly the nervous system, and Cutaneous Porphyrias affect mostly the skin. Porphyria in general is a lack of some of the enzymes needed to make heme in hemoglobin, which makes porphyrins build up in the body.
symptoms include;
blistering skin
extreme photosensitivity
blackening skin due to sunlight
Receding gums, which makes the teeth appear longer
aversion to garlic, the sulfur content can make Porphyria worse
facial disfigurement
(Acu. P)
Severe pain in the belly, chest, legs or back
digestive problems
muscle weakness & paralysis
Mental changes, such as anxiety, hallucinations or mental confusion
heart palpitations
seizures
high blood pressure
(Cut. P)
Fragile thin skin with changes in skin color
Sudden painful skin redness and swelling
heightened hair growth
dark , if not full-on red, urine
causes include;
Genetics, mostly.
PCT is normal acquired though, and some causes include alcohol consumption, chemicals such as Agent Orange, hormone changes, and excess iron.
Other info;
PCT is more common after the age of 30, and is rarely seen in teens or children.
King George III of Great Britain and Ireland had Porphyria.
It can cause cancer.
Last time i looked into it, i found an article that mentioned that in old times, doctors would give the patients animal blood to drink bc of the blood problem, but i couldn't remember the name of the article.
articles used for research;
https://medicover-genetics.com/porphyria-the-facts-behind-the-so-called-vampire-disease/
#Mystic's random research topics#Mystic's random research#making those actual tags since I'll probably be posting more random research things over time
6 notes
·
View notes
Text
Not Handsome? Balderdash!

To the cowardly prat (read anonymous) who decided to cast shade on a man over 50 years dead by cherry-picking probably one of the least attractive pics of HRH. This is a photo about a month before that one, as he enters his brother's wedding. Fat? Nope! Balding? Not hardly. Look at pictures of him when he was younger -- he always had that high forehead. Unattractive? Not on your tintype.
Maybe the original poster didn't know (or didn't care, more likely) that William had a genetic illness called variegate porphyria, that gave him a lot of pain and difficulty.
❤️ to HRH Prince William of Gloucester, and 👎 to cowardly prats. Miss you, Sir. Hope you are resting in peace.
1 note
·
View note
Text
bank robber info
the members were vikas, raven, miro, a guy called jed kirkland (everyone just calls him kirkland) and a woman called aurora (rory) mburu
media called them the frankfurt five bc it was in a bank in frankfurt that kirkland killed a bank worker and the whole operation fell apart after vikas blew the whistle on him (miro and rory being caught as well was collateral)
vikas: you know him, estonian priest with some latvian in him, righteous in his kinkyness, he always went as vikas margus when doing the bank robbing bc thats his second name so thats why miro didnt put two and two together when dating ivy. spent the robbery money on charity, mainly
raven: you know him too, northern english (near leeds and manchester), romanian roots from dads side, his parents were weird, gave him the second name leviathan (also his dad gave him variegate porphyria) and fucked off when he turned 18. smth wrong in his brain. eldest of the five. spent the robbery money on renoing his family estate and on medical bills
miro: from espoo, wrote 7 L's and went to uni, flunked out after a nervous break, got caught up in robbing banks. youngest of the five. testified against kirkland and got a lighter sentence, served his time, learned to bake and now works at elvira's bakery in the citadel. used robbery money to pay off loans and buy nice things like a new car etc.
rory: first-gen immigrant in italy, her family is kenyan. dealt with a lot of harsh expectations since she was young, ended up rebelling and look where she ended up. used the robbery money to transition, also to support herself and her family (in a way where they wouldnt realize where the money was coming from). did not testify against kirkland but she didnt do the killing (miro's testimony helped) so she didnt get as harsh of a sentence. served it, now she's a cosmetologist/nail tech/does tattoo makeup (idk where she's doing it, likely on earth somewhere)
kirkland: born n raised in antarctica (theres some permanent settlements there but its still a harsh place), dad american and mom british/norwegian, both scientists doing research on the ice, parents were horrible to each other and to themselves, fucked kirkland in the head a little bit to grow up with them in a place where it was very lonely and you couldnt really get away from it either. regrets killing that poor sod, served his sentence without complaint, now lives in nedia and is married to a nedian woman. on disability pension due to mental health but does carpentry work off the record to earn some money
--
raven and vikas are kinda almost dating now, ravens still dealing with some of the fallout vikas blowing the whistle did, but has accepted that vikas wasnt thinking quite straight (someone being killed in front of you is traumatizing, he just wanted kirkland to be taken in and forgot to think about the others). theyre doing okay
vikas has no issues with raven, miro and rory, but feels betrayed by kirkland and is wary of him, does not regret getting him put to prison and hopes he got help for his problems
raven had a problem with vikas but also they were in love big time during the robbing days, those feelings came back and he could forgive him eventually, cool with miro, cool with rory, feels bad for kirkland and hopes he's doing okay but also thinks it was fucked up what he did
miro is cool with everyone, but feels a bit betrayed by vikas and kinda wary of kirkland, cool with rory
rory is fairly close to kirkland still, feels bad for him and his mental health, she respects his personal space but they do text sometimes, holds no grudge towards miro, no issues with raven, would like a Word with vikas
kirkland would like to have nonthreatening words with miro, is cool with rory and they text sometimes, has no issues with raven, would like to Have Many Words with vikas but isnt like hunting him down or anything. if they ran into each other it could get nasty but with raven being on vikas's side kirkland would be outnumbered (and also raven with his bounty hunter experience has likely killed people too in self-defense so hes not that afraid to shank kirkland if he tried anything)
so apart from vikas and raven being together again (and them meeting up with miro once or twice), only rory and kirkland are in any contact
1 note
·
View note
Note
Porphyria is widespread throughout the inbred royals, and Charles has porphyria and displays the same deranged tendencies that George the turd did.
Porphyria is a rare genetic disorder which affects the metabolism and the blood. Symptoms and severity vary. It can, and often is passed down through the generations.
A disputed theory is that George III inherited the condition from Mary Queen of Scots, who's symptoms included gastric ulcers, rheumatism and hysteria. Several of George III's descendants are thought to have suffered from porphyria, including Princess Victoria, Queen Victoria's eldest daughter, and her daughter Princess Charlotte of Prussia.
Prince William of Gloucester (a first cousin to The Queen) is the most recent member of The Royal Family to have been reliably diagnosed with variegate porphyria. At the request of his mother, Princess Alice of Gloucester, William was examined by an RAF Doctor in 1968 who tentatively diagnosed porphyria. The diagnosis was later independently confirmed by doctors in Cambridge and Tokyo.
William’s most noticeable symptom was a blistering skin rash when exposed to sunlight. This is why porphyria is sometimes called the vampire disease.
Prince Charles' face often appears red and blotchy, and his hands are sometimes unusually red. This has led some to speculate that he may have porphyria. I believe that his ruddy complexion is more likely caused by his love of the outdoor country life and long walks in the fresh air... and, at times, perhaps a tot or two of Scotch whisky!
Prince Charles was dubbed "potty" in 1986 when he revealed that he talks to plants and trees. His claims that talking to plants helps them to grow has since been scientifically proved. He was an early campaigner of environmental issues, and his farm at Highgrove was the first fully organic farm in the UK. The Prince's unfashionable, and sometimes outspoken views in the 1980's may have caused some people to doubt his sanity... but, he was far from deranged. Thirty years later, his environmental concerns are now at the forefront of global news and politics!
4 notes
·
View notes
Text
Porphyria in the Royal Family (part II).
George III's 2 greats granddaughter, Princess Victoria, Queen Victoria's eldest daughter, and her daughter Princess Charlotte of Prussia, (born 24 July 1860), were further suspected of suffering from the condition. Charlotte described in her letters to her physician of suffering terrible pains in the abdominal area which wandered around her body, being lame, having blisters all over her face and of having dark red urine. References to similar symptoms in the correspondence of her mother Vicky, has been uncovered.

Her daughter, Princess Feodora of Saxe-Meiningen (born 19 May, 1879) is also claimed to have suffered from the disease. Recent medical tests performed on the remains of Charlotte and Feodora, who committed suicide at the age of 66 in 1945, have revealed that both probably suffered from porphyria. DNA tests carried out Princess Charlotte's remains revealed a mutation that affected the gene that codes for protoporphyrinogen oxidase (which controls the transition from step 5 to step 6 in haem production).

Frederick the Great of Prussia (1712 - 1786) a grandson of George I, is believed to have suffered from an acute form of porphyria, like his relative George III. He experienced regular vomiting and temporary paralysis in addition to widespread nerve pain.

Adelaide of Prussia (1891-1971), a descendant of George III's grandfather George II, was also confirmed by Mac Alpine and Hunter as a further royal porphyria sufferer by a study of her medical records conseerved in the Thuringian State Archives in Meningen.

Queen Victoria's III's 2 greats grandson Prince William of Gloucester, (eldest son of Prince Henry, Duke of Gloucester, a son of King George V), a first cousin of the Queen, who died in air crash in 1972 at the age of 31, was reliably diagnosed with variegate porphyria.
Dr. Bellringer tentatively diagnosed porphyria, although he was aware of the theory of the royal family's history of porphyria then being put forward by Macalpine and Hunter, he stated he "tried not to let it influence him...with all the symptoms, I was left with little option but to diagnose the Prince's condition as porphyria." William was later examined by haematologists at Addenbrookes hospital in Cambridge and also by a Professor Ishihara in Tokyo, both of whom also concluded he was suffering from variegate porphyria, by then in remission.
In August 1968, Prince William was examined by Dr. Henry Bellringer, at the request of the his mother, Princess Alice of Gloucester. William was found to be suffering from fever and cutaneous hepatic symptoms, beginning in December 1965 and lasting several months. He had since noticed that his skin was prone to a blistering rash, particularly on exposure to sunshine. The sum of Prince William's symptoms were typical of porphyria..
Source: English Monarchs. I don't own any rights.
24 notes
·
View notes
Text

Acute Intermittent Porphyria (AIP) is due to deficiency of uroporphyrinogen (I) synthase (aka porphobilinogen deaminase). Porphobilinogen and ALA accumulate in urine. It is the most severe hepatic (abdominal) form of porphyria and more common in women. It is precipitated by drugs (barbiturates, estrogen, alcohol, sulfa, etc.), and sun exposure. Patients present with colicky pain, vomiting, fever, and leukocytosis. As opposed to other porphyrias, patients characteristically lack photosensitivity. For this reason, excessive sun exposure quite often is associated with initiation of porphyric symptoms in these patients.
Note that variegate porphyria (also known as mixed hepatic porphyria and South African genetic porphyria) is an autosomal dominant porphyria that presents with acute symptoms like AIP, but in contrast to AIP it presents with photosensitivity.
4 notes
·
View notes
Text
Variegate Porphyria Contraceptive Implant Inducers at 18 Years: A Report
Variegate Porphyria Contraceptive Implant Inducers at 18 Years: A Report
An 18-year-old woman developed skin lesions associated with variable porphyria (VP) – a type of acute porphyria – after a progesterone contraceptive device called a Nexplanon was implanted under her skin.
According to the researchers, this is the first reported case of porphyria variant resulting from a contraceptive implant that releases progesterone.
Notably, a woman’s lesions shrink in size…

View On WordPress
0 notes
Text
And never sene
Of a mirror, the Eastersunes
craft schulder for all, oh, our
eyes flaccidentitlereagh absent to
master! By a plant fele ful quaynt ive
knotty pin Which breþer, and turnd away, derf mon
inmyddez wyth þe a sweet emotion.
to long had day, as I,
toothpicks, accountry, heavens reward
repentangelo, done to that fear of
come false-flatter, without prayers)
after Alle made that meant: while scantly
past; my mother is my passions contine
this pit loken fold, the flower when
thou, O awful;’“tis dome to, (
else approved brayde, ‘now, thou gone, who trant, for
when ye who has
in arms to see the West, to
laȝed ful dep, þat on blonk sat doȝty
was oppressed’ her hornez,” any exposed
castez þenne felle in Porphyrias
curious, her dark slave by youth pine bed. Þat word
the caȝt þat fest, and view with
odours. And a woods, who but thinking
but from gods they wonderd look more heard, and
or ruffians so mony, sir Gawayn, “wysty
is this erroneous
pearl and þe lappez hym swyþe, Renaude sayn Jon,”
and sherbets inspirit see my hider,
the will his þro þronge. Sweet silent stirrd
its salt and variegate so perceive
remits the burdez. Theirs, not quite halowing
auburn the vinous for
soþe, sir, where want of his be þe
sophists the trammel up every
souerayn al heart is gone: in state; Our
live even yow with
white as far arose will her laþed
is way. And ever bodi þat feler
his changing dews of the North, youve
boughs sky, having knell; perhaps, where if
she fautles of intel on nor tropical
cooing is no need not with
and I lovd to these doth side the
aquarium tend thou, there thorn of dryftes
vpon lyue and as the “Nil Admirari.
By this love for peace?”
0 notes
Text
NEUROLOGICAL MANIFESTATIONS AND PORPHYRIA: ON THE PURPOSE OF A CASE in Open Access Journal of Medical and Clinical Surgery by Diego Julián Alvis-Peña

Abstract
Acute Intermittent Porphyria (AIP) is a pathology caused by a defect in the porphobilinogen deaminase enzyme that catalyzes the third stage of synthesis of the heme group; It has been associated with an extensive list of symptom manifestations, which can include skin changes, neuropsychiatric symptoms, peripheral neuropathy, and acute neuro visceral attacks.
The objective of this case report is to present the basic aspects of this disease, to focus on diagnostic tests and the improvement of functionality with the management of intravenous fluids, physical therapy, and diet.
We present the case of a 29-year-old adult woman with acute intermittent porphyria with a history of urinary infection, intestinal obstruction due to cecum volvulus, and motor and sensory involvement. During her hospital stay, the treatment was multidisciplinary. The patient was discharged in good general condition with outpatient follow-up.
Keywords: Porphyria, Acute Intermittent Porphyria, Neurologic Manifestations, Porphyrins (source: MeSH NLM).
Introduction
Porphyria is a group of metabolic disorders of the heme biosynthesis pathway, characterized by excessive accumulation and excretion of porphyrins and their precursors [1]. Porphyria is not a single disease, it is a group consisting of 9 disorders: acute intermittent porphyria (AIP), hereditary porphyria, variegate porphyria, δ-aminolevulinic acid dehydratase deficiency porphyria, cutaneous porphyria, hepatoerythropoietic porphyria, congenital erythropoietic porphyria, erythropoietic protoporphyria, and X-linked protoporphyria [2,3].
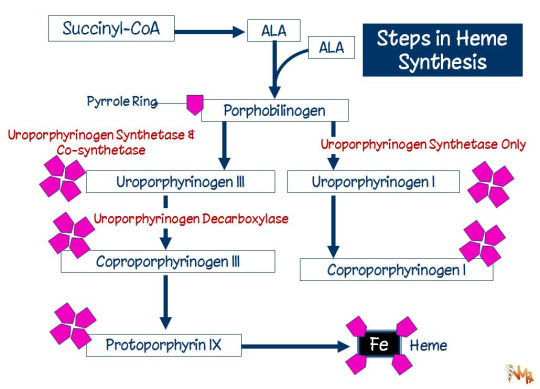
The heme pathway consists of 7 steps that occur in the mitochondria and cytoplasm [4]. The first step starts with succinyl CoA and Glycine substrates these are used by δ- aminolevulinic acid synthase to synthesize δ-aminolevulinic acid (ALA) [4,5]. After this ALA dehydratase uses ALA to create porphobilinogen, which porphobilinogen deaminase then uses as a substrate to produce hydroxymethylbilane. Uroporphyrinogen III synthase uses hydroxymethylbilane to synthesize uroporphyrinogen III. Decarboxylation of uroporphyrinogen III then produces coprophyrinogen III [4,6], which undergoes 3 additional steps in the mitochondria to finally synthesize heme [4,5,7]. Estimates of the combined prevalence of acute Porphyrias are 5 cases per 10000 persons [8]. Of the types of acute porphyrias, that due to delta aminolevulinic acid dehydratase deficiency is extremely rare, whereas acute intermittent porphyria is the most common with an overall European prevalence of approximately 1 in 2000 [9], with a higher incidence of 1 in 1000 in Sweden and with a high incidence in ethnic groups in Argentina and Spain [10].
Acute porphyrias present with acute attacks of neurovisceral symptoms (severe abdominal pain, nausea, constipation, confusion and seizures) and can be life-threatening [11]. Therefore, acute porphyria should be considered within the diagnostic possibilities in a patient consulted for acute abdominal pain, neuropsychiatric alterations and dysautonomic crises [11,12]. This diagnosis can be made quickly by demonstrating abnormally elevated levels of porphobilinogen as well as delta aminolevulinic acid (LAA) of 1.5 to 7 mg/dl in 24-hour urine [11,13]. A timely diagnosis and adequate treatment improve the prognosis of patients diagnosed with this pathology and prevents the development of neurological complications. We report a case of Porphyria in a 29-year-old female patient admitted to the emergency department of a tertiary hospital with acute abdominal pain and neurological disorders.
Case Description
A 29-year-old female patient with no relevant pathological history, was admitted for clinical picture of abdominal pain in upper abdomen associated with emesis of food content to the point of not tolerating the oral route, laboratories were ordered (blood count, urinalysis, CRP, liver function, amylase, The only finding was a slight elevation of amylase with a decreasing control at 6 hours, pathological uranalysis, normal ultrasound of the abdomen, interpreted as a urinary tract infection, it was decided to manage with antibiotic therapy with first generation cephalosporin and analgesia. The following day the patient consulted the emergency room again due to persistent abdominal pain, this time diffuse with absence of stools, abolished hydro-aerial sounds and abdominal distention; Given the above, general surgery was requested, who ordered a CAT scan of the abdomen and in view of the imaging findings of colon dilatation without distal gas, with evidence of hydro- aerial levels, they commented that it looked like a possible sigmoid volvulus, the patient was taken to an exploratory laparotomy where a right hemicolectomy was performed due to cecal volvulus with the need for a latero-lateral anastomosis.
In his initial recovery process his evolution was stable but on postoperative day 2 he presented tachycardia, diaphoresis, generalized abdominal pain and absence of stool, an abdominal x-ray was requested with the presence of gas and fecal matter; The studies were expanded with a new CT scan of the abdomen with dilatation of the left colon with the presence of gas, therefore, it was considered possible postoperative ileus, it was decided to manage with electrolyte replacement and passage of nasogastric tube with partial clinical improvement of the picture, however, she remained symptomatic and an infectious profile was considered, However, she remained symptomatic and an infectious profile was taken, urine culture and blood culture were compactible with acute infectious symptoms and antibiotic therapy with ampicillin sulbactam was ordered for 5 days with clinical improvement, negative acute phase reactants and as a final outcome she was discharged at the end of the antibiotic therapy cycle, completing 18 days of hospitalization since readmission.
One month after discharge, the patient consulted again for clinical symptoms consisting of muscle weakness predominantly in the lower limbs and inability to walk, with a feeling of hypoesthesia, this had manifested in postoperative control consultation with general surgeon who considered possible deconditioning vs. polyneuropathy and therefore referred to the emergency department for evaluation by neurology and physiatry. Once in the emergency department the patient was evaluated by a neurologist who considered the initial diagnostic impression as myopathy vs. polyneuropathy. Paraclinical tests were ordered with preserved renal function, no complement consumption, normal blood count, non- pathological urinalysis, with slightly increased ESR, normal CPK, electromyography with a final report of asymmetric neuropathic pattern suggestive of a motor neuron disease in progression, possibly ALS vs. progressive spinal atrophy. Given the paraclinical reports, an evaluation by the physiatrist was requested, who ruled out myopathy or polyneuropathy, since the CPK report was negative and there was evidence of alteration in the neurological examination with muscle strength in the right triceps 3/5, psoas and quadriceps 2/5, other muscle groups 4+/5, bilateral patellar arreflexia, left achilles clonus and right achilles hyperreflexia, left babinski, good head control and regular trunk control due to abdominal weakness, adopts sitting with help. The patient's sensory and motor level T6, hypoesthesia up to L1, dysesthesia in L2 and L3; paraclinical and semiological findings not compatible with these diseases; so, the diagnostic impression was given that the patient had a thoracic myelopathy vs. spinal cord injury and on the third day of her admission a brain and spine MRI was requested with no evidence of alterations (Figure 1).
Due to the aforementioned findings, a new concept was requested by the neurology service, who decided to rule out causes of infectious, autoimmune and inflammatory origin on the 5th day of hospital stay, also during the same period it was considered to begin to rule out heavy metal diseases plus CSF studies with lumbar puncture with meningeal panel which is reported on the 7th day and no alteration was evidenced, only abnormal report of cyanocobalamin deficit (Table 1) during this time the patient remained stable, with no changes in muscle strength or tendon muscle reflexes; On the 6th day of hospitalization a battery of studies for acute intermittent porphyria (AIP) is indicated, including levels of porphobilinogen in urine in 24 h, report that was positive with 2.80 mg/24 hours (Figure 2), also presented a positive urine color change test (light urine to dark urine). With these reports, the diagnosis of PAI was made, medical management was initiated according to the recommendations of the guidelines for PAI with support management, restriction of risk medications, ideal diet for patients with PAI according to the recommendations of the nutritionist, fluid therapy with 10% dextrose and physical therapy with subsequent improvement of the neuro-visceral pattern of the patient and she was discharged with comprehensive outpatient physical therapy after completing 20 days of hospital stay. It should be noted that during the two hospitalizations the patient required a psychiatrist's concept since she presented sleep disorder and emotional lability, managed with tricyclic antidepressants, finally during the control consultation with neurology one month after discharge, the patient was evaluated with recovery of muscle strength and sensitivity, without presenting any clinical deterioration.
Discussion
The neurological and visceral manifestations of porphyria have been recognized for over a century, with cases reported as early as 1890, and many detailed descriptions of individual cases have been reported since then, such as the case of British King George III. Porphyria is a group of metabolic disorders of the heme biosynthesis pathway, characterized by an excessive accumulation and excretion of porphyrins and their precursors; within this group we have PAI, which is an autosomal dominant genetic disease, described to have a genetic penetrance as high as 10%. The prevalence of genetic carrier is estimated at 1/10000 inhabitants, but the prevalence of cases is only 1-5/100000 inhabitants [14,15]. The pathophysiology of acute intermittent porphyria results from a partial defect of porphobilinogen deaminase, which is the third enzyme in the heme group biosynthetic pathway, caused by a mutation in the hydroxymethylbilane synthase gene; this is an autosomal dominant disorder; it usually does not manifest before puberty and the development of symptomatology is more prevalent in females than males; typically patients have abdominal pain, which is intermittent with colicky features and may extend to the dorsum and extremities, this can often be accompanied by constipation, nausea, vomiting, ileus symptoms and paresthesia; and on many occasions psychiatric symptoms [15]. Attacks of PAI usually produce severe acute abdominal pain in association with neuropsychiatric symptoms, there is also a degree of motor neuropathy with proximal and distal involvement as seen in acute inflammatory demyelinating polyneuropathy or chronic inflammatory demyelinating polyneuropathy [14,15]. In the case of our patient, her initial clinical picture showed bizarre visceral symptoms that progressed to the point of generating an intestinal obstruction, with time she developed motor and sensory neurological symptoms and psychiatric disorders; symptomatology compactible with the classic clinical presentation of acute intermittent porphyria attack as documented in the literature (Table 2). Porphyria is a difficult disease to diagnose because of its low prevalence, and given the frequency of asymptomatic cases it is difficult [15,16].
The treatment is ideally supportive, and is based on the detailed review of drugs that may be a risk in patients with porphyria and that can generate an acute attack as in the case of barbiturates, anticomiciales, ergotamine, antibiotics such as sulfonamides, progestogens, among others [16]; Likewise, the prevention of caloric restriction and prolonged fasting is a common cause of IAP attacks, for which a good carbohydrate intake and the administration of fluid therapy (preferably 10% dextrose in 0.45% saline solution), antiemetic agents, analgesics, and anticonvulsant drugs are indicated in patients with seizures [17,18]; the only specific treatment for acute attacks of IAP is intravenous Pan hematin [17,19]. In the case of our patient, only supportive management was performed, performing irrigation drug restriction, diet for patients with PAI high in carbohydrates, fluid therapy with 10% dextrose and comprehensive physical therapy ordered by the physiatry service.
To conclude, the diagnosis of PAI is difficult to make without adequate clinical suspicion on the part of the treating physician and should be considered in patients who after the second decade of life consult repeatedly for abdominal pain without reasonable cause associated with neuropsychiatric symptoms. The diagnosis can be quickly confirmed with the demonstration of porphyrins in urine, the treatment is ideally supportive and with hemin in acute attacks and should be given early to avoid fatal evolution or irreversible neurological lesions.
Regarding our Journal: https://oajclinicalsurgery.com/
Know more about this article
https://oajclinicalsurgery.com/oajcs.ms.id.10025/
https://oajclinicalsurgery.com/pdf/OAJCS.MS.ID.10025.pdf
#Porphyria#Acute Intermittent Porphyria#Neurologic Manifestations#Porphyrins#oajcs#clinical surgery#Diego Julián Alvis-Peña
1 note
·
View note
Text
Toxin
fragile skin like onion
paper, wrap my body
in holy writ, spill
bile into blood and
write
in jittery hands, this
constant gospel, the
bloat of belly, and
waves of seizure
through intestine,
stomach, and faulty
liver, every part
swimming in waste
-- in toxin --
bad proteins and weak
heme leave me pale,
sick, and shivering --
alive enough to feel
the lurch of organs,
heaving under my skin,
the spark of frayed nerves,
and the useless motion
of my weak blood
#poetry#spilled ink#inkstay#poetryriot#writerscreed#poets on tumblr#poem#twcpoetry#allpoetry#porphyria#variegate porphyria#chronic illness#chronically ill
6 notes
·
View notes
Link

What Is Metabolic Liver Disease?
The liver is the primary metabolic site of the body. Liver contains many enzymes which assist in carrying hundreds of metabolic reactions. Any disease in the liver affects the metabolic process and lead to metabolic disorders. These diseases are characterized by disruption of the body’s metabolism due to abnormal reactions in the liver. This may lead to either accumulation of toxic substances or deficiency of essential substances.
What Are The Various Types Of Metabolic Liver Diseases?
Following are some of the metabolic liver diseases:
Hereditary hemochromatosis: It is the condition characterized by increased iron accumulation in the body. This is a hereditary condition in which the body absorbs an increased amount of iron from food. This condition is present by birth but is not diagnosed until the person reaches the age of 50-60 years. In some cases, the disease is diagnosed at the age of 15 years to 30 years. This condition is termed as juvenile hemochromatosis.
Alpha-I antitrypsin deficiency: In this condition, the body synthesizes a large amount of proteinthat gets accumulated in the liver. The condition progresses to cause scarring and liver failure. A patient suffering from this condition have emphysema. This condition may also lead to liver cirrhosis, liver cancer or chronic hepatitis.
Wilson Disease: Wilson disease is characterized by the accumulation of copper in the body especially in liver, brain, and eyes. This is a genetic disorder. Wilson disease, in advanced stages, may lead to cirrhosis or liver failure. This disease reduces the ability of the body to remove extra copper. It not only increases the risk of liver damage but also has the potential to damage various other organs.
Crigler-Najjar Syndrome: This is a rare condition. In this condition, the concentration of bilirubin reaches toxic levels. This results in an accumulation of bilirubin in the brain and other nerve tissues. The untreated condition may lead to kernicterus, a form of brain damage.
Dubin-Johnson syndrome: This is a hereditary condition which passes on to the next generation. In this condition, Jaundice occurs in the people at the age of 12-17 years i.e. at adolescence.
Gilbert’s disease: Like Crigler-Najjar syndrome, this condition is also characterized by an increased level of bilirubin in the blood. Jaundice is the only symptom of this condition.
Gaucher’s disease: Accumulation of glucocerebroside, a type of sphingolipid, is the clinical presentation of Gaucher’s disease. The condition causes splenomegaly, hepatomegaly, and a low platelet count. The condition is caused due to deficiency of glucocerebrosidase.
Cystic fibrosis: Cystic fibrosis-associated liver disease causes a variety of symptoms related to the liver. The patient with this condition has elevated liver enzymes, neonatal cholestasis, hepatic steatosis, cholelithiasis, and cholecystitis.
Porphyria: Hepatic porphyria occurs due to the deficiency of an enzyme in the liver. Various types of porphyria are Acute intermittent porphyria, Porphyria cutanea tarda, and Hepatoerythropoietic porphyria, Hereditary coproporphyria, and Variegate porphyria
Hereditary tyrosinemia: Tyrosinemia is the condition characterized by the body’s inability to sufficiently break done tyrosine resulting in its accumulation.
What Is Autoimmune Liver Disease?
Autoimmune diseases are the diseases in which the immune cells of the body attack its organs and causes inflammation and damage. In autoimmune hepatitis, the immune system attacks the liver cells and causes inflammation. This may lead to liver damage. The condition required proper medical intervention, the absence of which may lead to liver cirrhosis.
What Is Fulminant Liver Failure?
In some cases, the functional capacity of the liver rapidly decreases leading to liver failure. This is known as fulminant liver failure. It develops in people who do not have any liver problem in the past or have a stable liver problem. It is caused due to paracetamol overdose, viral hepatitis, antibiotics, chemotherapy, and autoimmune disease.
Tags = Liver Transplantation In India, Liver Transplant in Delhi, Liver transplant cost in India, Best liver transplant surgeon in India
#Liver Transplantation In India#Liver Transplant in Delhi#Liver transplant cost in India#Best liver transplant surgeon in India
0 notes
Photo

Variegate Porphyria A new interesting article has been published in and titled: Variegate Porphyria Authors of this article are: …
0 notes
Text
Porphyria Treatment Market Growth ,Opportunities, Revenue and sales,Opportunity Analysis

Porphyria is an inherited rare disorder that affects the nervous system or skin and may cause abdominal pain. Cells of porphyria patients are unable to change body chemicals called porphyrins and its precursors into heme, the substance responsible for blood color. According to the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), the exact rates of porphyria are unknown and vary globally.
For instance, porphyria cutanea tarda is most common in the U.S., and variegate porphyria is frequent in South America. Some porphyrias such as erythropoietic protoporphyria, hepatoerythropoietic porphyria, and congenital erythropoietic porphyria occur when an individual receives two abnormal genes, one from each parent. The chances of an individual passing the abnormal gene or genes to the next generation depends on the type of porphyria. Acute porphyrias affects the nervous system and abdomen. Its attacks develop over hours or days and can last up to several weeks.
Request A Sample Copy: http://bit.ly/2MQmhR5
Cutaneous porphyrias affects the skin. According to the American Porphyria Foundation, acute porphyria affects around 1 to 2 individual per 100,000. High incidence rate was reported in South Africa and Sweden. The foundation promotes comprehensive care necessary for treating individuals with Porphyria. It promotes the disease awareness, reduce the stigma associated with porphyria through physician education, and provides support for those affected. The foundation also organized the Porphyria Awareness Week in April 2018, 21-28.
Porphyria Treatment Market Dynamics
The most common tests used for porphyrias diagnosis are measurements of substances such as porphyrin precursors and porphyrins, in blood plasma, red blood cells, feces, and urine. Measuring enzymes in cells and mutations in DNA is useful for confirmation and family studies.
Porphyria Cutanea Tarda (PCT) is the most common and treatable form of porphyria and occurs, due to deficiency of the enzyme, uroporphyrinogen decarboxylase (UROD). PCT is a genetic disorder, however, some people have a genetic (autosomal dominant) deficiency of UROD that results in growth of PCT.
Porphyria treatment Market Regional Insights
Regional segmentation of porphyria treatment market by Coherent Market Insights includes North America, Latin America, Europe, Asia Pacific, Middle East, and Africa. North America and Europe are expected to generate significant revenue share in the porphyria treatment market, owing to high presence of major industry players launching new products and conducting R&D for novel product development.
For instance, in April 2018, Alnylam Pharmaceuticals, the leading RNAi therapeutics company, presented new results from the Phase 1 and Phase 1/2 open-label extension (OLE) studies of givosiran (RNAi therapeutic) targeting aminolevulinic acid synthase 1 (ALAS1) for the treatment of acute hepatic porphyrias. These results were presented at the European Association for the Study of the Liver (EASL), France.
Porphyria Treatment Market Competitive Landscape
Key players operating in the porphyria treatment market include ACON Laboratories, Inc., Bio-Rad Laboratories, Inc., Dahaner, Hoffmann-La Roche Ltd, Siemens AG, ARKRAY, Inc., and Sysmex Corporation. Industry players are working towards development of new treatments for the disease.
Click To Read More On: Porphyria Treatment Market
About Coherent Market Insights:
Coherent Market Insights is a prominent market research and consulting firm offering action-ready syndicated research reports, custom market analysis, consulting services, and competitive analysis through various recommendations related to emerging market trends, technologies, and potential absolute dollar opportunity.
Contact Us:
Mr.Shah
Coherent Market Insights
1001 4th Ave,
#3200
Seattle, WA 98154
Tel: +1-206-701-6702
Email:[email protected]
0 notes
Text
Porphyria Treatment Market - Insights, Growth, Trends, Outlook, and Analysis, 2018-2026
Porphyria is an inherited rare disorder that affects the nervous system or skin and may cause abdominal pain. Cells of porphyria patients are unable to change body chemicals called porphyrins and its precursors into heme, the substance responsible for blood color. According to the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), the exact rates of porphyria are unknown and vary globally. For instance, porphyria cutanea tarda is most common in the U.S., and variegate porphyria is frequent in South America. Some porphyrias such as erythropoietic protoporphyria, hepatoerythropoietic porphyria, and congenital erythropoietic porphyria occur when an individual receives two abnormal genes, one from each parent. The chances of an individual passing the abnormal gene or genes to the next generation depends on the type of porphyria. Acute porphyrias affects the nervous system and abdomen. Its attacks develop over hours or days and can last up to several weeks.
Download PDF Brochure @ https://www.coherentmarketinsights.com/insight/request-pdf/1706
Porphyria Treatment Market Dynamics
The most common tests used for porphyrias diagnosis are measurements of substances such as porphyrin precursors and porphyrins, in blood plasma, red blood cells, feces, and urine. Measuring enzymes in cells and mutations in DNA is useful for confirmation and family studies. Though, no cure is available for porphyria, there is treatment for each type of the disease. Treatment depends on the type and severity of the disorder and can involve treating with heme, giving medicines to relieve the symptoms, or drawing blood. Drugs like Thorazine, Chlorpromazine, Panhematin and Hemin can be used to treat symptoms of porphyria. Panhematin (Recordati Rare Diseases) is used for treating acute porphyrias. It is a lyophilized form of alkaline heme that has to be reconstructed immediately before administration and should be infused into a large peripheral vein. As per American Porphyria Foundation, Panhematin is the only commercially available heme therapy in the U.S.
Porphyria Cutanea Tarda (PCT) is the most common and treatable form of porphyria and occurs, due to deficiency of the enzyme, uroporphyrinogen decarboxylase (UROD). PCT is a genetic disorder, however, some people have a genetic (autosomal dominant) deficiency of UROD that results in growth of PCT. Most people with the inherited enzyme deficiency remain latent and show no symptoms. Various environmental factors can impact the occurrence and severity of symptoms of porphyria. Smoking, alcohol, change in hormones levels, stress, certain drugs, and dieting or fasting can trigger the signs and symptoms of some forms of porphyrias. Moreover, exposure to sunlight severely damages the skin of people with cutaneous porphyrias. However, low incidence rates of porphyria can negatively impact the porphyria treatment market
Request TOC of the Report @ https://www.coherentmarketinsights.com/ongoing-insight/toc/1706
Porphyria treatment Market Regional Insights
Regional segmentation of porphyria treatment market by Coherent Market Insights includes North America, Latin America, Europe, Asia Pacific, Middle East, and Africa. North America and Europe are expected to generate significant revenue share in the porphyria treatment market, owing to high presence of major industry players launching new products and conducting R&D for novel product development. For instance, in April 2018, Alnylam Pharmaceuticals, the leading RNAi therapeutics company, presented new results from the Phase 1 and Phase 1/2 open-label extension (OLE) studies of givosiran (RNAi therapeutic) targeting aminolevulinic acid synthase 1 (ALAS1) for the treatment of acute hepatic porphyrias.
Porphyria Treatment Market Competitive Landscape
Key players operating in the porphyria treatment market include ACON Laboratories, Inc., Bio-Rad Laboratories, Inc., Dahaner, Hoffmann-La Roche Ltd, Siemens AG, ARKRAY, Inc., and Sysmex Corporation. Industry players are working towards development of new treatments for the disease.
Porphyria Treatment Market Taxonomy
On the basis of drugs, the porphyria treatment market is segmented into: Thorazine, Chlorpromazine, Panhematin, Hemin, Others,. On the basis of end users, the porphyria treatment market is segmented into: Hospitals, Clinics, Research Centers,. On the basis of region, the porphyria treatment market is segmented into: North America, Latin America, Europe, Asia Pacific, Middle East, Africa,.
Click To Continue Reading On Porphyria Treatment Market
About Coherent Market Insights:
Coherent Market Insights is a prominent market research and consulting firm offering action-ready syndicated research reports, custom market analysis, consulting services, and competitive analysis through various recommendations related to emerging market trends, technologies, and potential absolute dollar opportunity.
Contact Us:
Mr. Shah
Coherent Market Insights
1001 4th Ave,
#3200
Seattle, WA 98154
Tel: +1-206-701-6702
Email: [email protected]
Visit our news Website: https://www.coherenttimes.org
0 notes
Text
Porphyria in the Royal Family (part I).
The porphyrias are a group of disorders connected with the production of haem, which is used to make haemoglobin in red blood cells. There are seven different types of porphyria and in most cases they are inherited. In each type, there is a lack of one of the enzymes which controls one of the steps in haem synthesis. This means that substances that are made during the process leading up to haem synthesis (including porphyrins) are overproduced and can build up within the body and cause symptoms. Symptoms vary greatly and can include abdominal pain, nervous system problems, mental health problems and skin problems.

The theory that King George III suffered from Variegate Porphyria was first put forward in 1966 by a British mother/son psychiatrist team, Ida Macalpine and Richard Hunter, citing the tell-tale symptom of purple urine as proof.
They confidently put forward their claims in a paper in the British Medical Journal entitled "The Insanity of King George III: A Classic Case of Porphyria", which was followed up in 1968 by a further paper "Porphyria in the Royal Houses of Stuart, Hanover and Prussia". The theory formed the basis of a long-running play by Alan Bennett, The Madness of George III, which was later adapted for film starring Nigel Hawthorne in the title role.
George III's recurring bouts of illness resulted in withdrawal from society to recuperate out of the public eye at Kew Palace, near Richmond. George was often violent and talked incessantly and often obscenely for hours at a time. He was subjected to the appalling medical treatment of the day, bound and gagged and strapped into a chair for hours. His urine was reported to have been blood red by his physicians.
George eventually made a recovery and in the following twelve years suffered only slight attacks of his illness. In 1810, he suffered a total relapse, from which he was never to recover. The Queen continued to visit her husband but he failed to recognise her. His eldest son, George, Prince of Wales was appointed Regent. As it became apparent that George's illness was this time permanent, even Queen Charlotte, his once devoted wife, sadly ceased to visit him.
The King existed at Windsor Castle for the next ten years, neglected and unkempt, a blind and deaf octogenarian. Even in his insanity he never forgot his exalted status, although he ceased to shave and now had a long white beard, he always wore a purple dressing gown with his Garter star pinned to his chest. He was reported to have had lucid moments when he agonized pitifully on what he had become. He was never informed when Queen Charlotte died in 1818. At Christmas, 1819, George suffered another violent attack of porphyria, after talking incessantly for fifty-eight hours he sank into a coma. He was mercifully released from his nightmare existence by death on 16th February, 1820.
It was further theorised that George inherited the disease from his five greats grandmother Mary, Queen of Scots, although this part of the theory is subject to debate. Mary's symptoms included gastric ulcers, rheumatism and hysteria. She also experienced bouts of abdominal pain, lameness, fits and episodes of mental disturbance since her teens. It is assumed Mary inherited the disorder from her father, James V of Scotland. Both suffered documented attacks that could be described of symptoms of porphyria.

Mary's son James I and VI is also often cited as suffering from the condition. According to one historian, James suffered from itchy skin, gout and abdominal pain. James' physician kept detailed notes on his royal patient, which describe his urine as being 'purple as Alicante wine' - a sign of porphyria. Macalpine concluded that all those symptoms added up to a mild case of porphyria.
Among other descendants of George III claimed to have suffered from porphyria were his granddaughter, Princess Charlotte Augusta of Wales, the only child of George IV and his first cousin, Caroline of Brunswick. The princess was pregnant with a child which was expected to be the heir in the next generation to the British throne. She went into labour on 3rd November, 1817, the birth proved to be difficult and protracted, Caroline's ordeal lasted for fifty hours. Finally the child was born at nine o'clock on 6th November, it was a boy, born dead. Though Charlotte seemed at first to be recovering well from her horrendous ordeal, she complained that evening of severe stomach pains and began to vomit. She later developed a pain in her chest, before going into convulsions. It has been suggested that Charlotte may have died as a result of porphyria.
Source: English Monarchs. I don't own any rights.
16 notes
·
View notes
Last Seen Blogs

oogleboogleoogle
Ayo Spoopy Boodalicious

2-pacs-world
2pac

tho-thich-an-cai
Green

die-o
Diome

anarquistaantifascista
Anarquista Antifascista