
juniperpublishersnursing
JuniperpublishersNursing
66 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

pasta-boy
it's pasta time bitch

staticsaffy613
I'd ship it

ira-hayes-blog
drunk on altitude..

karenfordonte
Caring For Donte

almaniya10
تنظيف خزانات
Text
Happy Easter- Juniper Publishers

Juniper Publishers wishes Happy Easter to you and your family members.
0 notes
Text
Severity of Hip Displacement in Relation to Subtypes and Motor Function in Cerebral Palsy- Role of Hip Surveillance | Juniper Publishers

Juniper Publishers-Open Access Journal of Orthopedics and Rheumatology
Authored by Kunju PAM
Abstract
Background: Hip dislocation in children with cerebral palsy (CP) is a common and often over looked problem by the treating pediatricians. Though it can be diagnosed early by using radiographs, knowledge about the standardized methodology and need for periodic surveillance is lacking among primary care pediatricians. Hip surveillance by X-ray pelvis can identify early hip dislocation and it is shown that early intervention may prevent the need for surgery [1].
Methods: The study was done in a tertiary care hospital as a onetime radiological evaluation of children with CP between the age group of 4-9 yrs. One hundred and one children with CP formed our study population.Clinical evaluation for details regarding CP type and assessment of motor ability by gross motor function classification system (GMFCS) was done. A hip X-ray was done for calculation of, migration index for establishing or ruling out hip displacement. Migration percentage (MP) in relation to CP subtypes and GMFCS grades were done.
Results: There were 48 boys and 53 girls (mean age 4.80 years). 12 children were Gross Motor Function Classification System (GMFCS) level 5, while 26 were GMFCS level 4. Out of 36 hemiplegic CP only one had MP > 40. out of 6 children with spastic quadriplegia, 5 (83%) had MP > 40%. Spastic diplegic and choreoathetotic subtypes showed MP >40% in 9 out of 43 and 7 out of 16 respectively.According to the gross motor function classification system, GMFCS level I had no child with MP > 40%. Whereas 50% of children in GMFCS level IV and V had MP > 40% compared to only 4.76% in GMFCS I and II put together.
Conclusion: All the children in this study did not undergo a hip X-ray prior to this study. 22 out of 101 children had severe degree of hip displacement. The maximum number of hip displacements was seen in children with spastic quadriplegia; Spastic diplegic and choreoathetotic subtypes showed intermediate risk of hip displacement and hemiplegia had very low risk. According to the gross motor function classification system,GMFCS level I had no child with MP > 40%. Whereas 50% of children in GMFCS level IV and V had MP > 40%. The study showed the relationship between the CP subtypes and the severity of the motor involvement. It also emphasized the need for early hip surveillance.
Keywords: Hip dislocation; Cerebral palsy; Lateral Displacement; Hip surveillance
Introduction
In children with spastic cerebral palsy reduced activity of the hip abductor muscles in comparison to the spastic adductors leads to diminished growth of the greater trochanter of femur results in pathologic deformities of the hips-femoral anteversion and coxa valga antetorsa [2]. If untreated, dislocation of the hip typically occurs at age 2–7 years with a maximum at the age of 6 years. The incidence of hip displacement in cerebral palsy is related to the severity of involvement; varying from 1% in children with spastic hemiplegia, up to 75% in those with spastic quadriplegia [2,3]. So periodic evaluation of hip function is essential for early intervention and preventive measures.
Hip surveillance is defined as: “The process of monitoring and identifying the critical early indicators of hip displacement” [4].Hip displacement refers to the displacement of the femoral head laterally out of the acetabulum and is measured using a migration percentage (MP). Hip subluxation refers to hip displacement where the femoral head is partially displaced from under the acetabulum while hip dislocation refers to hip displacement where the femoral head is completely displaced from under the acetabulumn [5,6].Hip surveillance is important, to prevent morbidity of spastic hip disease-The aim of the management in children with spastic hip displacement is to maintain flexible, well-located and painless hips with a symmetrical range of movement. The key to achieving this goal is early identification and intervention.
Periodic hip surveillance also helps to reduce the need for extensive surgical procedures which is highly specialized area of orthopedics which may not be available in every center. So primary care pediatrician has a role for hip surveillance and timely referral.
Patients and Methods
The study was done in a pediatric neurology department of a tertiary care hospital as a onetime radiological evaluation of children with CP between the age group of 4-9 yrs prior to the referral to orthopedics. One hundred and one children between the age group of 4-9 yrs. with the diagnosis of CP formed our study population.A pediatric neurologist and physiotherapist in the department examined the children and completed an assessment form. Clinical evaluation for details regarding CP subtype and assessment of motor ability by gross motor function classification system (GMFCS) [6] was done. Winters, Gage, Hicks (WGH) gait type was determined, in addition to inquiring regarding pain during history taking. Orthopedic consultations done whenever required.
Radiographic Examination
Decision for referral for surgery depends on the degree of displacement of the femoral head and acetabular dysplasia. The migration percentages as described by Reimers and the acetabular index described by Hilgenreiner are the conventional measurements of displacement of the hip and acetabular dysplasia in young children with cerebral palsy.Radiographic assessment consists of measurement of migration percentage (MP) from a supine AP pelvis radiograph with standardized positioning [7] (Figure 1). Reimers Hip Migration Percentage is the percentage of body width of femoral capital epiphysis displaced out of the acetabulum (which falls lateral to perkins line) [8].Measurement of migration percentage of femoral head was done as given in the (Figure 2).
In the adult or older child, where the triradiate cartilages are fused and therefore inapparent, the inferior margin of the pelvic teardrop is used instead.The acetabular angle using Hilgenreiner’s line should be less than 28°at birth. The angle should become progressively shallower with age and should measure less than 22° at and beyond 1 year of age.
Present study an anteroposterior (AP) pelvic radiograph at the time of first visit was done. Any decrease in the range of movement at the hip or presence of scoliosis was a definite indication for further detailed radiological examination & immediate referral. In the present study 101 children were assessed between 4 and 9 years of age. Children with MP > 33% and > 40% were compared in relation to those with MP below these limits. Migration percentage (MP) in relation to CP subtypes and GMFCS grades were done.
Results
There were 48 boys and 53 girls (mean age 4.80 years). Distribution of Cerebral Palsy sub types were as follows. Hemiplegic 36 (35.64%), Quadriplegic 6(5.94%), Diplegic 43(42.57%) and Choreo athetotic 16(15%). 12 children were Gross Motor Function Classification System (GMFCS) level 5, while 26 were GMFCS level 4. Results of hip displacement by radiography as measured by MP in relation to CP subtypes and motor severity are presented in (Tables 1&2) and (Figure 3).
Only one child out of 36 children with spastic hemiplegia developed MP > 40%. The maximum number of hip displacements was seen in children with spastic quadriplegia, where 5 of 6 children (83%) had MP > 40%. Spastic diplegic and choreoathetotic subtypes showed intermediate risk of hip displacement (9 out of 43 and 7 out of 16 respectively had MP >40%). In the present study onset of hip displacement could not be assessed as hip surveillance was not done in a periodic basis. Figure 4 shows x-ray hip of 4-year-old with very minimal displacement (MP 33.33%) and Figure 4 shows severe hip displacement in an 8-year-old child.
According to the gross motor function classification system, GMFCS level I had no child with MP > 40%. Whereas 50% of children in GMFCS level IV and V had MP > 40% compared to only 4.76% in GMFCS I and II put together.
Discussion
The natural history of spastic hip disease of CP is progressive lateral displacement of the hip secondary to spasticity and muscle imbalance in the major muscle groups around the hip. Displacement may progress to severe subluxation, secondary acetabular dysplasia, deformity of the femoral head, dislocation and painful degenerative arthritis [4,5]. The long-term effects of dislocation of the hip can be disastrous for individual patients leading to pain and loss of the ability to sit comfortably in up to 50% of cases [6]. Other problems include difficulty with perineal care and personal hygiene, pelvic obliquity and scoliosis, poor sitting balance and loss of the ability to stand and walk [7-11].
A hip is usually considered to be subluxed,if the migration is equal to or greater than 33%. Reimers [17] found that among normal, the 90th gentile for migration percentage at four years was 10% with spontaneous migration of less than 1% per year. An unstable migration percentage is when progression is greater than or equal to 10% over 1 year [12-16]. Present study has shown that even a single radiological evaluation could identify hip displacement in children after the age of 4 yrs. Majority of (5 out of 6) quadriplegic CP, had severe type of hip displacement compared to hemiplegic CP (1 out of 36). Compared to other bilateral types of CP diplegia had lower rate of hip displacement (9 out of 43). This may be because of the less motor function impairment. So GMFCS may be a better predictor for early prediction of hip structural impairment. It is seen that there is direct correlation between the GMFCs class and severe hip displacement. According to the gross motor function classification system, GMFCS level I had no child with MP > 40%. Whereas 50% of children in GMFCS level IV and V had MP > 40% compared to only 4.76% in GMFCS I and II put together.
Subtyping of CP may have a role in predicting occurrence of severe hip displacement as shown by the almost complete occurrence in quadriplegic CP. However, a mere clinical examination and subtyping will not help in identifying severe hip disease in other type of CP. So, a systematic analysis of GMFCS is required for intensified screening of hip dysfunction. Moreover, as described in various guide lines periodic hip surveillance is mandatory for better ambulation and avoidance of surgery. This can be attained by early intervention measures. Figure 4 itself shows the importance of early surveillance. AACPDM - (American Academy for Cerebral Palsy and developmental medicine) recommends following schedule of hip surveillance (Table 3).
Conclusion
Need for hip evaluation in children with CP is emphasized by this study. All the children in this study did not undergo a hip Xray prior to the study. 22 out of 101 children had severe degree of hip displacement. The maximum number of hip displacements was seen in children with spastic quadriplegia and hemiplegia had very low risk. According to the gross motor function classification system, GMFCS level I had no child with MP > 40%. Whereas 50% of children in GMFCS level IV and V had MP > 40 %. The study showed the relationship between the CP subtypes and the severity of the motor involvement in producing hip displacement. Referral to an orthopedic surgeon with experience in treating hip displacement in children with CP is recommended when there is presence of hip pain on history and/or physical examination. Periodic hip surveillance is mandatory for early detection of hip displacement. When the migration percentage is greater than 30% and/or there is less than 30 degrees of hip abduction with or without other findings, referral to an orthopedic surgeon is recommended [1,17].
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Orthopedics and Rheumatology please click on: https://juniperpublishers.com/oroaj/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/oroaj/OROAJ.MS.ID.555848.php
50 notes
·
View notes
Text
Chemical, Photochemical Composition, Physical and Sensory Qualities of acha-Guava Flour Blends and Biscuits | Juniper Publishers
Juniper Publishers-Open Access Journal of Nutrition & Food Science
Authored by Ayo JA
Abstract
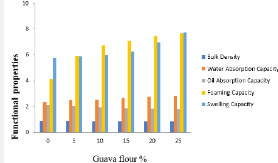
The study investigated the chemical, phytochemical composition, physical and sensory qualities of acha-guava flour blends and biscuit the work was aimed at ameliorating the quality of acha-based biscuits with the addition of guava flour. Flour blends were produced by substituting guava flour into acha flour at 5, 10, 15, 20, and 25%. Proximate composition, pasting properties, functional properties, phytochemical composition, vitamins and mineral of the flour blends were determined. Biscuits were produced from the flour blends and the physical properties and sensory qualities of the biscuits were analyzed. The carbohydrate and protein decreased from 81.60to 77.30 and 8.32to 7.70%, respectively. The moisture content, fat content, fibre and ash content increased from 8.08to 8.44, 1.28 to 2.63, and 0.21to 2.5and 0.20 to 1.62% respectively, with increase in the added guava flour (5-25%). Water absorption, foaming, and swelling capacity of acha flour increased from 2.35to 2.83ml/g, 4.13to 7.65ml/g and 5.75to 7.74ml/g, respectively. Bulk density and oil absorption capacity decreased from .89to .85/cm3 and 2.10 to 1.81ml/g respectively, with increase in the added guava flour (5-25%). The peak viscosity, trough viscosity, breakdown, final viscosity, and setback decreased from 2336.83 to 1107, 1535 to 935, 801 to 172, 3719.8 to 1863, and 2186.0 to 928RVS, respectively, with increase in the percentage guava flour. Iron, carotenoid, vitamin C and total phenol increased from 4.0 to 25.0ppm, 5.36 to 14.17mg/100g, 1.94 to 7.96mg/100g, and 0.22 to 0.86mg/100g respectively, while phosphorus decreased from 1110.10 to 814.3ppm with increase in percentage of added guava flour. There was an increase in break strength and spread ratio ranging from 1.35 to 2.64kg and 4.53 to 5.15 respectively, as a result of the increase in level of guava-flour substitution. The reverse was observed for the thickness, diameter, volume and weight of the biscuit which ranges from .88 to .60cm, 4.34 to 4.13cm, 13.05 to 8.00cm3, and 11.50 to 10.70g respectively. Sensory qualities evaluated were colour, texture, taste, odour, crispiness, and general acceptability with an average mean score ranging from 4.60 to 7.65, 5.50 to 6.85, 6.10 to 7.45, 5.80 to 6.85, 5.55 to 6.85and 6.20 to 7.95. The sample, 95:5% acha-guava blends is the most preferred and acceptable with average mean score of 7.95 and corresponding increment of 0.28, 2.22, 79.38, and 1.3% of ash content, protein, fat and crude fibre respectively.
Keywords: Water absorption; Foaming; acha flour; Peak viscosity; Trough viscosity; Breakdown; Final viscosity
Introduction
Biscuit and Cookies are usually produced from wheat flour and they are the same product since the British call them biscuit while the Americans call them cookies [1,2] identified an increasing tendency among children and adults to move away from traditional eating pattern of three meals a day to eating snacks instead of meal. Biscuits enriched with carrot generally have been found to be rich in carbohydrate and protein; they contain fat (14.10 ± 0.08%), carbohydrate (69.31 ± 0.12%), ash (2.32 ± 0.03%), and protein (8.10 ± 0.01%), fibre (0.93 ± 0.01) and moisture (6.17 ± 0.02) as reported by [3].
Cereal grains like wheat, corn, rice, barley, sorghum, etc. provide 68% of the total world food supplies. Wheat is mainly used as a dietary staple, averaging two-thirds of total consumption [4]. Owing to shortage of wheat, several developing countries have devised programs to assess the feasibility of alternative sources for substituting or blending of wheat flour with other cereals [5].
acha (D. exilis) is of considerable importance in Nigeria where it is commonly eaten, often in preference to other cereals, as many as three times a day as a porridge, couscous or non-alcoholic beverage, valued as a weaning food because of its low bulk and high caloric density with minimal processing requirement, it grows even where rainfall and soil fertility are poor and can be stored in closed containers for many years without need of preservatives [6].
acha contains high water absorption capacity that gives it capacity to be utilized in baked foods. It also contains pentosans which gives it the ability to form gel in the presence of oxidizing agents at room temperature with high residual protein coupled with high levels of Sulphur and hydrophobic amino acid residues which makes it useful in baking [7]. The recent finding of the unique properties of acha flour, particularly in relatively lowering the blood glucose level and which could subsequently reduce the diabetic populace have make researchers to focus on D.exilis [8].
Guava (Psidium guajava) is usually consumed as fresh fruit, being a flavorful and healthy alternative for a snack. It is also served with cream and sugar for dessert or combined with other fruits in cocktails and salads [9]. Guava juice is also very popular, being an excellent juice alternative for infant feeding or may be eaten with salt, pepper, vinegar, soy sauce or may be preserved into jam, butter, marmalades, relishes, and chutneys (Glaucia et al. 2012). Few studies have been conducted on the phytochemistry and total antioxidant capacity of guava, especially processed guava juice or puree. However, it is well documented that guava contains a very high amount of vitamin C, anthocyanin, lycopene, and carotenoids, [10].
The leaves of guava are used traditionally by many people to overcome a wide range of diseases, while the guava fruits are believed to overcome several of problems and a source of antioxidants [11]. Red guava fruit is also believed to help cure dengue hemorrhagic fever (DHF). Guava fruit contains vitamin C, two times higher than other fruits such as orange which makes it an important compound that has an antioxidant activity [12]. Other compounds in guava fruit are carotenoids such as betacarotene, lycopene, and beta-cryptoxanthin, and polyphenols [13]. Lycopene is associated with the prevention of cardiovascular damage due the LDL oxidationas the impact of dyslipidemia [14]. Antioxidant content in guava fruit can be used as a source of natural antioxidants; these include vitamins A, C, and E as well as numerous non-nutritive compounds such as polyphenolics, flavonoids, carotenoids, and thiol-containing compounds. Lycopene content in guava fruit is proven to prevent or delay the oxidative damage of lipids, proteins and nucleic acids caused by reactive oxygen species (ROS) [12].
Resent investigations in relation to the unrealized ability of acha to ameliorate the crises of diabetes and its deficiencies in some nutrient, have called for its fortification to bridge the existing gap. The abundance and perishability of guava with its high nutrient content calls for processing to reduce wastage and could be used as a fortifier or enriched food product with relatively low nutrient.
Fortification of acha biscuits with guava could improve the antioxidant, minerals, vitamin content and add value to the sensory qualities of food products. Also, the use of guava could reduce post-harvest losses, create more market for the raw material and increase the quest for production of nutritious food by food industries. The objective was to determine the chemical, phytochemical composition, physical, and sensory qualities of acha-guava flour blend biscuits.
Materials and Methods
Materials
Cream colored acha grains (D. exilis) purchased from Jos central market in Plateau state, Nigeria while the fresh guava (Psidium guajava (red colored) was obtained from Bayesa, Ussa Local Government, Taraba State, Nigeria. Other ingredients such as baking fat (Simas), baking powder (Omega), and salt (Dangote table salt) were purchased from Wukari New market, Taraba state, Nigeria.
Methods
Preparation of acha flour
acha flour was produced using the method described by Ayo et al. [8]. acha grains were winnowed to remove chaff and dust. Adhering dust and stones were removed by washing in water (sedimentation) using local calabashes and floating foreign materials by decanting. The washed and de-stoned grains were drained and dried in a cabinet drier (Model: CD0005, FT3) at 40°C to a moisture content of about 12%. The dried grains were milled using Attrition milling machine (Inch15HP Super 150-180 Kilogram Tw-HM-1016) and sieved (0.3μm aperture size). The flour was packaged inpolyethylene bag and stored at 5oC as acha flour for later use.
Preparation of guava flour
The procedure as described by Sanjinez-Argandona et al. [15] was modified and used in the preparation of guava flour. Fresh Matured and ripe guava fruit were obtained. Washed, sorted, peeled, sliced and steam blanched (Hughes Blancher Model #:02- 1471) for 3min. The sliced guava fruit were dried at 40°C in oven (San-Del Model 50) and milled using attrition mill (Inch15HP Super 150-180 Kilogram Tw-HM-1016) and sieved (0.3μm aperture size). Packaged in a polyethylene bag and stored (at temperature 5oC).
Formulation of flour blend
The guava flour was mixed with acha flour separately at different proportions (5:95, 10:90, 15:85, 20:80 and 25:75) while one hundred percent (100%) acha flour and wheat was used as the control. The flours were thoroughly mixed using a Kenwood blender to a uniform blend by Ayo & Gidado [3].
Production of acha-gauava composite biscuit
The recipe adopted for the work is shown in Table 1 as described by Ayo & Gidado [3]. The guava powder was substituted into acha flour at 5, 10, 15, 20 and 25% respectively. The sweet potato powder was beaten into the fat until fluffy and acha-guava composite flour and other ingredients were added, while mixing at a medium speed of Kenwood blender. The method described by Ayo & Gidado [3] was used to produce the biscuits.
* Average mean score with the same letter(s) on the same column are not significantly different, p=0.05.
Proximate composition determination
The proximate analysis of samples for moisture content, crude protein, ash, Crude fat, Carbohydrate and crude fiber was carried out on the flour as described by AOAC [16].
Determination of minerals and vitamin
The phosphorous, iron and Vitamin B1 of the acha-guava flour blends were determined as described by AOAC [16] methods while the Vitamin C content was determined by direct calorimetric method as described by Kalia [17].
Determination of phytochemicals
Carotenoids content of the acha-guava flour blends was determined as described by Krishnaiah et al. [18] method, while the total polyphenol was determined by Folin-Ciocalteu’s method using gallic acid as standard as described by Priyanka [19].
Functional properties determination
The functional properties: - bulk density, water absorption capacity, oil absorption capacity, foam capacity and swelling power of the acha–guava flour blends were determined as described by Onwuka [20].
Determination of pasting properties
Pasting properties of the acha-guava composite flour were determined using the Rapid Visco Analyzer (RVA-4, Newport Scientific, Australia and Thermocline for Windows programme).
Determination of physical properties
The breaking weight, volume, break strength and spread ration of acha-guava composite biscuit were determined using the method described by Ayo et al. [8].
Sensory Evaluation
The sensory quality of the acha-guava biscuits was evaluated using twenty untrained panelists, randomly selected from Department of Food Science and Technology Federal University Wukari, Nigeria based on their familiarity with the biscuit. The biscuits, appropriately coded (ACH, RJG, EYM, and AMD) and of the same size and temperature (29 ± 3oC) were placed in white plastic plates separated by compartment and placed in sensory laboratory. The panelists rinsed their mouths with bottled water after tasting each sample and were not allowed to make comment during evaluation to prevent influencing other panelist. A nine-point Hedonic scale with one (1) representing “extremely dislike” and nine (9) “extremely like” was used, presented as a questionnaire. The qualities assessed were color, texture, taste, flavor, crispness and general acceptability as described by Ayo & Gidado [3].
Statistical Analysis
All the analyses were conducted in duplicates in completely randomized design. The data were subjected to analysis of variance using Statistical Package for Social Science (SPSS) software version 23, 2017. Means where significantly different were separated by the least significant difference (LSD) test. Significance was accepted at p<0.05
Results and Discussion
Proximate Composition of acha-guava flour blends
Flours and flour blends were produced from acha and guava flour blend and proximate composition is presented in Table 1. The carbohydrate and protein decreased from 81.60±.39 to 77.30±.02 and 8.32±.03 to 7.70±.02%, respectively. The decrease could be due to poor protein content level in guava flour. The moisture content, fat content, fibre and ash content increased from 8.08±.02 to 8.44±.48, 1.28±.02 to 2.63±.03, and .21±.03 to 2.5±.043 and .20±.02 to 1.62±.06% respectively, with increase (0- 25%). The effect of adding guava to acha are significant, p>0.05. The 75:25% acha-guava samples had the highest value for moisture content, crude fibre, fat and ash, while the 100:0% achaguava samples had the highest value for protein and carbohydrate
The increase in moisture content could be due to the relative increase in the fibre content of the added guava as it is hygroscopic. Fibers have the ability of absorbing moisture. The crude fibre increased with increase in added guava powder. This could be due to the presence of high dietary fibre content in fruits and vegetables [21]. Accurately measuring the fibre content of foods is critical to making a sound benefit claim, whether it is a nutrient claim, structure-function claim, or health claim [22].
Ash content indicates the presence of mineral matter in food. Increase in ash content indicates that samples with high percentage of ash will be good sources of minerals. The carbohydrate decreased with increase in guava powder addition. The results obtained in this study are within the ranges earlier reported for acha [23]. Ayo & Gidado [3] reported similar range for biscuits from acha and carrot flour. Olapade et al. [24] also reported a similar range for biscuits from acha and cowpea flour. The carbohydrate contents of these samples are an indication that the products are good sources of energy.
Functional properties of acha-guava flour blends
The result of the functional properties of acha-guava flour blends are shown in Table 2. The effect of added guava flour (0- 25%) on water absorption, foaming, and swelling capacity of acha flour increased from 2.35±.07 to 2.83±.11ml/g, 4.13±.70 to 7.65±.16ml/g and 5.75±.02 to 7.74±.08ml/g, respectively. Bulk density and oil absorption capacity decreased from .89±.01 to .85±.014g/cm3 and 2.10±.141 to 1.81±.01ml/g, respectively (Figure 1). The 75:25% acha-guava samples had the highest value for water absorption, swelling and foaming capacities and lowest value for bulk density and oil absorption capacity. The increase in the WAC could be due to molecular structure of the guava flour [25]. The effect is significant different, p>0.05. Functional properties are the intrinsic physico-chemical properties that reflect complex interaction between the composition, structure, confirmation and physic-chemical properties of protein and other food components and the nature of the environment in which these are associated and measured.
* Average mean score with the same letter(s) on the same column are not significantly different, p=0.05.
High WAC of composite flour suggests the potential of the flours in the formulation of foods such as sausage, dough and bakery products where hydration to improve dough handling is a preferred characteristic. The observed variation could be due to different protein concentration, their degree of interaction with water and conformational characteristics [26]. The increased swelling capacity of flours depends on the particle size, variety and type of processing methods. The results agreed with the reported quality attributes of biscuit from acha (digitariaexilis) flour supplemented with cowpea (vignaunguiculata) flour by Olapade et al. [24].
The decreased OAC of the flour blends upon addition of guava flour might be attributed to the molecular structure of starch which is loosely linked, allowing for more penetration of liquid materials. The blends could also be used in formulations for products such as ground meat, doughnuts and pancakes, where oil absorption is not of paramount importance [27]. The bulk density of flour is measured without the influence of any compression. This revealed that bulk density depends on the particle size and moisture content of flours. The high bulk density of flour could suggest their suitability for use in food preparations. However, low bulk density would be great significance in the preparation of complementary foods [28].
Pasting Properties of acha-guava flour blends
The results of the pasting properties are shown in Table 3. The peak viscosity, trough viscosity, breakdown, final viscosity, and setback decreased from 16.83±.50 to 1107±.50, 1535±.50 to 935±.50, 801±.50 to 172.±.50, 3719.8±.29 to 1863±.50, and 2186.0±.50 to 928.0±.50RVS, respectively, with increase in the percentage guava flour. The effect of adding guava powder are significant, p>0.05, for all the parameters except for peak time. The 100:0% acha-guava Sample had the highest values for all the properties. Pasting properties are dependent on the rigidity of starch granules, with consequent effect on the granule swelling potential and the amount of amylose leaching out in the solution [29]. The high content of starch in the 100:0% acha-guava (control) sample, compared to other samples may contribute to some extent, to the higher pasting viscosity observed which could be the resultant effect of decrease in viscosities with decrease in the acha flour proportion.
* Average mean score with the same letter(s) on the same column are not significantly different, p=0.05.
High values of breakdown associated with high peak viscosities could be related to the degree of swelling of the starch granules during heat treatment. The peak viscosity often correlates with the quality of end-product and also provides an indication of the viscous load likely to be encountered by a mixing cooker (Sanaa and El-Sayed, 2004). The lower setback viscosities of acha starches could make the suitable for preparing gels with tendencies to synereses [30].
Pasting time of fonio grains (acha) reported by Jideani et al. [31] was significantly higher than that obtained in this study which could be due to climatic and soil factors. A higher pasting temperature indicates high water-binding capacity, higher gelatinization tendency and lower swelling property of starchbased flour due to high degree of associative forces between starch granules [32]. Pasting temperature is one of the properties which provide an indication of the minimum temperature required for sample cooking, energy costs involved and another components stability. Therefore, from the results obtained, 100% acha samples could be said to be more sensitive to heat treatment with less energy consumption, thereby saving time and cost. Ayo & Gidado [3] reported a similar range for pasting properties of acha-carrot biscuits.
Minerals, vitamins and phytochemical composition of acha-guava flour blends
The results minerals, vitamins and phytochemical composition of acha-guava flour blends shown are shown in Table 4. Iron, carotenoid, vitamin C and total phenol increased from 4.0±.50 to 25.0±.50ppm, 5.36±.04 to 14.17±.06mg/100g, 1.94±.05 to 7.96±.02mg/100g, and .22±.03 to .86±.02mg/100g respectively, while phosphorus decreased from 1110.10±.50 to 814.3±.50ppm with increase in percentage of added guava flour. The effect of adding guava to acha flour are significant, p>0.05 on the vitamin C and phosphorous content. The 75:25% acha-guava samples had the highest value for iron, carotenoid, vitamin C and total phenol. Iron and vitamins (vitamin C and B1) increased as the levels of substitution of guava flour with acha increased (5-25%). The findings agreed with that of Ayo et al. (2010) and Igbabul et al. (2014). Carotenoids are abundant in the red, yellow, orange, and green colored vegetables and fruits. They are, after chlorophyll, the second most widely occurring plant pigment found in nature (MacDougall 2002). The high degree of hydration and long carbon chain length of these molecules makes them hydrophobic and therefore fat-soluble molecules. The major purpose of carotenoids in the human diet is to serve as precursors to pro-vitamin A, a required nutrient for humans (MacDougall 2002).
* Average mean score with the same letter(s) on the same column are not significantly different, P=0.05.
The vitamin C is one of the most abundant antioxidants consumed, with fruits being the main source of the nutrient. Because L-ascorbic acid is an excellent reducing agent and is abundant in nature, it may help stabilize phenolics and other antioxidants during processing by the donation of hydrogen atoms. These compounds could also impart color, astringency, and bitterness and possible nutritional properties [33].
Physical composition of acha-guava blend biscuits
The physical properties of the acha-guava flour blend biscuits are shown in Table 5. There was an increase in break strength and spread ratio ranging from 1.35±.01 to 2.64±.01kg and 4.53±.01 to 5.15±.01, respectively, as a result of the increase in level of guavaflour substitution. The reverse was observed for the thickness, diameter, volume and weight of a piece of biscuit which ranges from .88±.02-.60±.00cm, 4.34±.0-4.13±.04cm, 13.05a±.07-8.00±.14cm3, and 11.50±.00 - 10.70±.71g respectively. The 85:15% acha-guava samples had the highest breaking strength and weight, 75:25% had lower values in volume, thickness and diameter, and 95:5% samples had the highest in diameter, thickness and volume respectively. The effect of adding guava powder are significant, p>0.05, for weight. The increased spread ratio observed in guavaflour substituted biscuit samples could be due to the difference in the particle sizes and characteristics of the constituent flours of guava and acha (Agu et al, 2007). Joel et al. [34]and Olapade et al. [24] reported similar trend in biscuits from wheat and full fat soya and biscuit from acha flour supplemented with cowpea flour. The spread ratio could be an indicator of biscuit quality.
* Average mean score with the same letter(s) on the same column are not significantly different, p=0.05.
Sensory evaluation of acha-guava flour blend biscuits
The sensory qualities evaluated are presented in Table 6 The result showed that the average mean score for colour, texture, taste, odour, crispiness, and general acceptability ranged from 4.60±2.19-7.65±1.09, 5.50±1.76-6.85±1.09, 6.10±1.74- 7.45±1.09,5.80±1.39-6.85±1.38, 5.55±2.09-6.85±1.69 and 6.20±1.9-7.95a±.76. The effect of guava was significant, p>0.05, for colour, texture, taste, crispiness and general acceptability. The relative increase in the average mean scores for texture could be due to the increasing fibre content of the guava with effect on the crispiness of the biscuit. The value for odour of the biscuits was not significantly different (p˂0.05) from each other. The sample, 95:5 % acha-guava blends is the most preferred and acceptable with average mean score of 7.95±.76. This effect on the sensory could be due to inherent flavor compounds in guava. Ayo & Gidado [3] reported a similar range for sensory qualities of acha-carrot biscuits and Dabels et al. [35] also reported similar range of wheat, acha and mung bean composite biscuit (Figure 2).
* Average mean score with the same letter(s) on the same column are not significantly different, p=0.05.
Conclusion
In conclusion, enriched biscuit with guava-flour substitutions were found to be nutritionally superior in fat content, fibre, iron, carotenoid total phenol, vitamin C and B1 respectively. The sample with 5% guava flour was most preferred corresponding relatively high improvement in the ash, fat, fibre, iron, carotenoid, vitamin C, total phenol and vitamin B1 content of the acha based biscuits. The appearance and crispiness of the acha-guava biscuit were greatly improved and acceptable.
The use of acha-guava flour blends in biscuits will go a long way in enhancing nutrition, health and wellbeing of the consumers and reduce the dependence on wheat flour. The properties of acha-guava could also make it a good candidate for use as edible blend and as raw material for several domestic and industrial purposes and in medical sector, acha could recommended as a dietary supplement for diabetic patients due to its high fibre content minerals and vitamins as result of added guava flour.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Nutrition & Food Science please click on: https://juniperpublishers.com/nfsij/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/nfsij/NFSIJ.MS.ID.555727.php
47 notes
·
View notes
Text
Chemical Contaminants and Pollutants in the Measurable Life of Dhaka City
Juniper Publishers-Open Access Journal of Pharmacy & Pharmaceutical Sciences
Authored by AK Mohiuddin
Abstract
Environmental pollution and food contamination are as old as the civilization itself. It is the consequence of the development of civilization, over utilization of nature, industrialization and in fact a price for the progress. It is highly prominent in Dhaka city. Air pollution is mainly due to the vehicle emission, industrial discharge and burning of fossil fuel. The water resource of Dhaka becomes a major health threat due to arsenic contamination, inadequate household/industrial/medical waste disposal and industrial effluent management. Food contamination came from the commercialism of business people who are doing this knowingly to maximize profit. Necessary steps are to be taken to protect the environment for our own existence. This paper reveals chemical pollution and contamination issues of Dhaka city, the capital of Bangladesh.Purpose of the study: Brief review of chemical induced pollution and contamination, their consequences and control. Healthcare providers/Policy makers have a major role play to concerned field.Materials and Methods: Comprehensive literature search followed by consulting healthcare professionals about environmental pollution and food contamination. Hospital, clinic and company personnel, newspaper journalists, NGO workers given their valuable suggestions and asked help for necessary books, journal, newsletters. A few western magazine and newspapers also observed to get necessary concern. Projections were based on public life pattern, their food habits, pollution and contamination sources, waste disposal features of urban life as well as industry and hospital waste disposals.Results and Discussions: Pollution and adulteration are the most notorious enemy of mankind. Civilization has its own drawback that even causing destruction of itself. Very few people raised voice on this but crippled by the facts of commercialism. The scope of this article is limited to chemical pollution of air and water, medical or household waste products and food contaminants and adulterants. A few discussions based on real life experience and recent studies or reports from various journals and news articles are summarized here.Findings: Both general people and the old system, are responsible for this unlivable condition of Dhaka city. Population is not the sole for this instance. A sense of poor rules and regulation is always raised everywhere. Negligence is becoming a wide spread disease contaminating illiterate to well educated, all kind of people.Research limitations: Many articles and documents found in concerned area of research, but the scope of this research is on its focus point chemical hazards and burdens of Dhaka city. Still the most important aspect is covered, but fact is less amount of recent data found in few areas.Practical Implication: The language of this article is too simple to understand by people with simple literacy. Pharmacists, doctors, nurses, hospital authorities, public representatives, policy makers and regulatory authorities must acquire much from this article.Social Implication: Any article or research is based on the think beneficence for mankind, at least going ahead from the present situation, overcoming problems and measures. The article should create an instruction for the future policy makers of both government and other sectors to review the alarming situation of chemical pollutions and food contaminants of Dhaka, along with the whole Bangladesh. Again, world business is moving to Asian countries, Bangladesh will be an important business hub within next few decades. This article should remind policy makers that we should not forget mankind, giving places to industrialization and development.
Keywords: Medical and Household waste; Health Hazard; Chemical Intoxication; Cancer; Food Poisoning; Pathogen; Contaminants
Abbreviations: BDL: Below Detection Limit; BOD: Biochemical Oxygen Demand, also called Biological Oxygen Demand; COD: Chemical Oxygen Demand; DO: Dissolved Oxygen; TDS: Total Dissolved Solid; PH: A Logarithmic Scale used to specify the Acidity or Basicity of an Aqueous Solution; ICDDR, B: International Centre for Diarrheal Disease Research,Bangladesh
Introduction
Contamination is the presence of an unwanted substance where it should not be or at concentrations above recommended. Pollution is contamination that results in detrimental biological effects to resident communities. All pollutants are contaminants, but not all contaminants are pollutants. All elements of the natural environment can be altered, sometimes with harmful results. Air, food, water, and the earth can all become sources of ailment, in the home, public, or work environments. In urbanization, all processes are viewed in relation to the city. Generally, better food supply, good medical care, education, jobs, industrialization, commercialization, electrification, specialization of professions, and entertainment are the basic causes of urban growth. Accessible energy plays an important role in our development with this, people can enjoy all the modern facilities [1-4].By establishing road communication, an undeveloped area may relate to a developed area. It helps the people of the areas, the use of information, technology, and media for an improved standard of living. With increased industrialization, air, in Western, as well as developing countries, now contains toxic substances that are either direct results of combustion or produced by photochemical change. Dhaka, being the capital of Bangladesh ranked 3rd worst in Air Quality Index (AQI) in the world. Besides, the city of nearly 20 million inhabitants, Dhaka faces challenges on this front, ranging from poor sanitation, polluted rivers, and chemical outpouring from the surrounding industries, all resulting from the impromptu nature of urbanization. Food contaminants and adulterants gave a new dimension in city life, together rest of the country. The healthcare providers role in environmental health is related primarily to being alert to the conditions predominant in the community and of working with others to adequately control any of the attendant hazards [5].
Urbanization and Its Impact
Urbanization is one of 21st century’s most transformative trends. Cities are the dominant force in sustainable economic growth, development, and prosperity in both developed and developing countries. In developed countries, the growth of the urban population has stabilized, and urbanization is taking place at a rapid pace. Currently, 55% of the world’s population (four billion people) reside in urban areas which will be nearly 70% by 2050 (United Nations, 2018). By 2030, over 60% people will live in the cities (Megacity Challenges, Siemens AG), two billion more people will have migrated to cities– placing unprecedented pressure on infrastructure and resources, particularly those related to water (According to UN and World Bank) [6]. From 2016 to 2030, a 35% population increase is expected in the top ten megacities.Furthermore, as more than three-quarters (76%) of the world’s mega-cities are coastal, there will be a considerable impact on water ecosystems from ridge to reef. Because of this, local and regional authorities lead initiatives targeting waterrelated obstacles, including housing gaps, climate change and an increased demand for food, energy and water [7,8]. Forecasts indicate cities in developing countries including Karachi, Lagos, and Dhaka will surpass cities like New York, Osaka, and Sao Paulo by 2030 [9]. This represents a 50% increase in demand for energy and water, generating challenges that exert pressure on water resources and threaten global water security.This has a palpable effect on public health, economics, and development. It has been estimated that the urban population in Bangladesh will rise to between 91 and 102 million by 2050, which will be 44% of the total population [10]. The leather tanning industry has been identified as one of the main causes of environmental and water pollution in the Capital city of Dhaka of 10 million people. About 60,000 tons of row hides and skins are processed every year using dehairing, ammonium salt sulphate and chloride during de-liming, solvent vapors which releases a huge quantity of untreated effluent into the open causing air pollution and water bodies [11].
Chemical Pollution and Contamination Due to Urbanization
Smog results from the interaction of the ultraviolet rays in sunshine and the unburned hydrocarbons of automobile engines or factories and smokestacks. These products, when trapped by the thermal inversion engendered by local topography, cause damage to mucous membranes and lungs when inhaled [12]. Acute episodes of air pollution have been found to exacerbate illness and even cause death in people who already have respiratory and cardiovascular diseases. Supporting evidence exists demonstrating that second-hand tobacco smoke increases the risk of cardiovascular diseases or cancer as well [13]. According to World Bank’s Country Environmental Analysis (CEA) 2018 report, air pollution lead to deaths of 46,000 people in yearly in Bangladesh [7]. Waterborne infectious disease is very common today, all the public supplies are literally contaminated with water drainage system reported many places.Many complaints about the taste, appearance, and physical qualities of locally supplied water have led to a brisk in bottled water [14]. Water contamination with ground-source chemicals (e.g., pesticides, fertilizers) remains an ongoing possibility. Food remains a significant vehicle of disease organisms [15]. Foodborne disease more commonly but often incorrectly called “food poisoning,” is grossly underreported. In most instances the illness produced by contaminated food is mild and of short duration, but more severe outbreaks (such as hepatitis A, most commonly seen in public restaurants) can. Epidemics of foodborne disease are dramatic and sudden, and most people become sick within 6 to 24 hours after consuming the contaminated foodstuffs. The epidemic pattern of food-borne disease presents differently from the gastrointestinal symptoms (e.g., nausea, vomiting, and diarrhea) induced by intestinal enteroviruses occur [16].
The Dhaka City at a Glance
Living in Dhaka city endowed with a traffic jam, street foods, unplanned buildings, narrow road space, noise pollution along with environmental pollution and issues of contamination [17]. Some people make joke like “Traffic jams teach us things like patience and how to plan ahead of time” [18]. Many people sleep roadsides, railway platforms, mosques and market places. People rushes this city for job, business and other opportunities like uninterrupted utilities. Along with general people, the city is also heaven for muggers, robbers, thieves, pickpockets, frauds, drug dealers and organized criminals [19]. People rarely can see the sunrise or sunset due to thousands of buildings.Hawkers are illegally occupying the public walkways, pedestrians are now forced to walk on the roads which raises the risks of accidents and adds to the already unbearable traffic congestion in those areas. Economist Intelligence Unit (EIU) The EIU surveyed 140 cities around the world for its Global Liveability Index 2018, scoring them on over 30 specified parameters under five categories: healthcare, infrastructure, culture and environment, stability, education and infrastructure (The Global Livability Index, 2018). All these things make this a difficult to breath place and a second worst place in the world to live in. Some 18,000 deaths from environmental pollution occurred in 2015 in Dhaka Environment Desk (2016).
Air Pollution
The most profound chemicals found harmful to human health and at high enough concentrations (Table 1) can even be fatal are Carbon monoxide (CO), Sulfur dioxide (SO2), Nitrogen oxides (NOx), Ozone (O3), Hydrocarbons (HC) and Suspended Particulate Matter (SPM) found in places surround Dhaka. Possible health hazards found to be headache, eye-nose-throat irritation, allergy, lung injury, trauma and even death with long term exposure [20-24].The AQI in Dhaka during the winter, where more than 4,500 brick kilns operate, typically hovers above 250 – a level considered unhealthy for all groups – but often spikes much higher [25]. Brick kilns, unfit vehicles run by fuels with higher level sulphur, as well as construction works, rundown roads have been identified as major sources of air pollution [26,27]. Day by day the amount of dust include air pollution in the city has been increasing. The air quality, particularly in Dhaka has undoubtedly been getting worse. Air pollution, according to Thomson Reuters Foundation, caused largely by burning fossil fuels, is cutting global life expectancy by an average of 1.8 years per person, making it the world’s top killer [28]. AQI 201 to 300 is marked as “extremely unhealthy” or hazardous air. At present AQI level of Dhaka has 309, which is in extreme “unhealthy” position [7].
Water Pollution
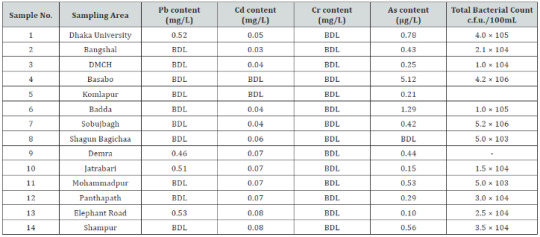
Moving on to the issue of water quality and pollution, the National Sustainable Development Strategy (NSDS) of Bangladesh identifies the following reasons behind degradation of surface water quality:1. Unregulated industrial expansion,2. Rural-to-city migration,3. Encroachment of rivers and water bodies,4. Overloaded infrastructure,5. Confusion about institutional responsibility for the quality of urban water bodies, and6. Insufficient enforcement of environmental regulations [29].The Rivers Buriganga, Shtalakhka, Balu, Tongi Khal and dholeswari which runs past Dhaka City, is at present one of the most polluted rivers in Bangladesh [30]. The city is suffering from an acute lack of domestic water supply. Water is involved in the spread of contagious diseases in essentially two ways. The well-known direct ingestion of infectious agent when drinking contaminated water. The second is due to a lack of enough water for personal solitariness purposes [31]. Approximately 80% of all sicknesses and diseases can be attributed to inadequate water supply and sanitation worldwide [32,33].However, the rivers and canals continued to be encroached upon, and more wastewater from houses and industrial units poured into the rivers without any treatment, with several major sources of pollution being outside the city area—in Ashulia, Savar, Tongi and Gazipur [34]. According to Dhaka Water Supply and Sewerage Authority (DWASA), it can currently supply 75% of water demand, out of which 85% is from groundwater sources (Deep Tube wells) [35]. The presence of toxic metal lead in Elephant road, Dhaka.University, Jatrabari, and Demra area and toxic Penta Chloro Phenol (PCP) and existing pathogenic bacterial load in the WASA supplied drinking water from different areas of Dhaka city were found to be unsuitable for human consumption [36] (Table 2).Some 80% of wastes are being dumped into the rivers in Bangladesh. No wonder our water supplies are in jeopardy. Around 250 industries are discharging chemical pollutants into the Buriganga and Sitalakhya river. Every day 4,000 tons of solid waste and 22,000 tons of tannery waste mixes with water in Buriganga river. Sewage is being discharged directly into the rivers, and the low-lying parts around urban areas [37,38]. By 2021 the garments export target has been set at $50 billion. But the success comes at a huge environmental cost.The dyeing and finishing plants are the major pollutants of water. Turag that flows by Tongi is almost dead with pollution. Its water looks ink black and gives out such a foul smell [39]. Wetlands around Dhaka city are being destroyed through land development and dumping of toxic effluents and untreated sewage. Industrial effluents have destroyed the ecology of rivers near these large urban areas [40]. In Dhaka, 20 canals have disappeared. Liquid and solid wastes, and heavy metals like copper, iron, lead, and nickel are distressing the BOD, COD, DO, TDS, PH of water [4].
Medical and Household Solid Waste
Dhaka City Corporation (DCC) is unable to impose rules on the public. On the institutional side, rules and regulations are not clear. The role and responsibilities of waste generators are not clearly defined i.e., the present law does not provide penalties for illegal disposal of waste or littering. Lack of scientific approaches for problem solving and DCC has shortages of skilled human resources and finances [41]. The accumulating waste is dumped by the residents in the city’s streets, open storm water and wastewater drains or open water bodies where and whenever the collection service is inexistent or dysfunctional [42]. Slum or periphery areas are affected by such a situation.During the annual monsoon rains wastewater and storm water drains which are clogged by solid waste overflow, creating an acute sanitary and hygienic threat in low-lying slum areas particularly. Solid waste generation profile is Per Capita Waste Generation: 0.56 kg/cap/day, Total Waste Generation DCC Area: 5000 tons/day and 70% - 80% of the solid waste is organic. Approximately 200 metric tons of medical wastes are generated in the city per day (Approximately 6% of total waste) (Mohiuddin, 2018). Different industries and their contribution to pollution in Dhaka are: Pulp and paper (47.4%), pharmaceuticals (15.9%), metals (14%), food industry (12.1%), and fertilizers/pesticides (6.6%) [24,37,40].Medical waste may contain highly toxic chemicals and can present a mechanism for transmission of diseases (Table 3). The growth of the medical sector around the world over the last decade combined with an increase in the use of disposable cheap medical products has contributed to the large amount of medical waste being generated. For a megacity like Dhaka, even low hazardous wastes generation rates can lead to the accumulation of large quantity wastes [43].This enormous amount of medical waste poses from different healthcare establishment (HCE) (Table 4) significant health risks to the people associated with waste disposal and treatment. During monsoon, the situation gets worse as medical, toxic chemicals and sewage waste flood Dhaka streets, contaminating dozens of neighborhoods in the process. The reuse of syringes by the general public represents one of the greatest public health problems in the developing world related to health care waste. Worldwide, an estimated 10 to 20 million infections of Hepatitis B and C and HIV occur annually from the reuse of discarded syringe needles without prior sterilization [44].
Food Contamination
Dhaka city now alone generates huge solid wastes per day from industrial discharge, fertilizers, fossil fuels, sewage sludge and municipality wastes and they are the major sources of heavy metals in soils and subsequent uptake by crops, vegetables and other food items causing serious health hazards to human beings [45,46]. A significant transfer of heavy metals like arsenic, cadmium, chromium, copper, lead, mercury, nickel, zinc, molybdenum and vanadium took place from soils to vegetables (spinach, tomato and cauliflower) grown in industrially polluted soils of Konabari at Gazipur and Keraniganj in Dhaka [47]. Industrial wastes and effluents are being discharged randomly on soils, into canals, rivers, along the road sides or in the vicinity of the industrial areas without any treatment where polluted river water is being used for irrigation purpose in paddy and vegetable cultivation causing absorption of heavy metals through the food chain by human beings [48].
Food Adulterants
Important food hazards include microbial hazards, pesticide residues, misuse of additives, chemical contaminants, including biological toxins and adulteration. Although microbiological contamination and chemical hazards have received most attention, it is recognized that food adulteration and food fraud should not be neglected considering their role in public health (FAO/WHO Expert Consultation, 1986). Food adulteration includes various forms of practices, such as mixing, substituting, concealing the quality of food by mis-labelling, putting up decomposed or expired food, and adding toxic substances [49]. About the proportion of adulterated food items in the market varied between 70% to 90%. Nearly 80% food items in the market were found contaminated in a random survey by public health laboratory of Dhaka City Corporation in 2004 [50,51].According to the International Centre for Diarrheal Disease & Research, Bangladesh [52,53], there is approximately 150 food items in the country. A study by the Institute of Public Health (IPH) revealed that more than 50% of the food samples they tested were adulterated. Textile dyes, which are highly injurious to health, are being randomly used to color many types of food. Fish is an essential protein for people of all ages. Many fish sellers spray fish with formalin in an assorted manner, it makes the fish or fruits stiff and keeps them looking fresh for longer. Undoubtedly human health is now under the possession of formalin, in our country about 400 tons formalin is being imported which are goes to human stomach, even though for laboratory or research purposes 100 tons of Formalin is quite enough, 80% of the imported formalin being added to food only for business purposes [54-60] (Table 5).Milk in rural areas is usually devaluated with dirty water, which can cause hepatitis. People are now acquainted with the milk adulteration technique that uses a thickening agent, sorbitol, and detergent. ICDDR, B recent studies shows nearly 75% samples from primary-level producers were contaminated with coliform and more than 50% with fecal coliform bacteria. At the collection points, samples were found contaminated with a high number of coliform bacteria and fecal contamination of more than 90% while more than 40 % of the samples had a high E coli count [52].Vegetable and fruit samples collected from around Savar, Dhamrai and Tongi show the presence of textile dyes, which, in the short-term, will cause diarrhea, food poisoning and gastrointestinal problems, but in the long-term toxic materials will accumulate in the body with serious health implications. In the absence of effluent treatment plants (ETP), the factory wastes are depleted out at will into the farmlands, and ultimately contaminate the farm produce [61]. In Bangladesh, people allowed things like pollution and food contamination to run riot.Till now, neither under the health ministry nor the ministry of science and technology or the ministry of industries, has conducted any examination of the pesticide- residue levels or toxic chemicals in the foodstuff being marketed. These merchants and traders are the enemy not only of the nation and their own children but of the entire mankind. The holy Prophet (PBUH) has disowned those who indulge in this immoral business. He said ‘’ The adulterator is not one of us’’ [58]. Apart from these severe noxious pathogens found in different food samples (Table 6), that are potential causes of stomach problems.Total coliforms and fecal coliforms count (CFU/g) [62]. It is an unfortunate reality that adulteration, especially in food, has become ubiquitous in the society. No one can justify or defend it. Most food products available in the market are adulterated. The average family is eating dangerous colors, chemicals like formalin and carbide, sawdust, soapstone, harmful chemicals and other harmful substances mixed with consumable goods. High level of pesticides content is present in grains, pulses, in fruits and vegetables that we eat [63]. Fecal bacteria found in 97% bottled water [55].Brick dust in chili-powder, colored chalk powder in turmeric, injectable dyes in watermelon, peas, capsicum, brinjal, papaya seeds in black pepper etc. are frequently used [58]. Even more unfortunate is the fact that this nefarious practice increases exponentially during the month of Ramadan. The shopkeepers and the merchants–many of them with a pious façade– try to earn a large amount of profit by this unethical practice, and so they play with the life and health of the people [64,65]. They mix dangerous things in the daily eatables. Even the medicine and drugs are adulterated. Most people can’t even think of having the commodities like ghee, oil, salt and milk, free from impurities [66-70].
Recommendations
Pollution and contaminant control are a never ending, on the other hand a continuous process. It will increase with time as the civilization go ahead. Pharmacists should be aware of the local occupations, companies, and factories and to be cognizant of the initial symptoms of disease. Again, pharmacists should become acquainted with the local community and to adapt the principles of health and medical care to the situations encountered. The pharmacist’s continuing education requirements should include watching the local pattern of society and its diseases and changing the emphasis toward evolving disease patterns and their control.Included in the current environmental issues are the workplace and the future of occupational safety and health regulations, hazards of local ambient environments, such as hazardous and other waste dumps, radioactive waste from weapons production, air emissions, and groundwater contamination of unknown magnitude; the Clean Air act and other and regulatory initiatives; waste reduction and minimization, and radioactive waste and weapons production; global pollution, chlorofluorocarbons and the land ozone layer, the greenhouse effect, and global climate change; and conserving the tropical forest and biological diversity. Government and regulatory authorities are to play strong role in controlling food contaminants and adulteration. An out of the box thinking is decentralization i.e. to move few many important originations away from Dhaka city. With this decentralization, population density will be declined, the ill movement of business Crips will also be diluted.
Conclusion
With constant change to the physical, biological, cultural, social, and economic environment, both pharmacists and citizens should cultivate an informed awareness of these changes, and health providers should adapt their methods of health education, disease prevention, and disease control to the changes in each community. With an unusually large number of people seeking relief from health hazards, providers may play a much more fundamental and personal role in controlling foodborne diseases. The necessary role in environmental health is related primarily to being alert to the conditions prevailing in the community and of working with others to adequately control any of the attendant hazards.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Journal of Pharmacy & Pharmaceutical Sciences please click on: https://juniperpublishers.com/gjpps/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/gjpps/GJPPS.MS.ID.555698.php
#Juniper Publishers#Open Accesss Journals#Juniper Publishers Publishing Group#Juniper Publishers LLC#Juniper Publishers Review
24 notes
·
View notes
Text
Surgical Wound Care-Juniper Publishers

Introduction
In general, the surgical wound care is very important as the management of surgical wound is concerned. The management of post-operative wounds is important to prevent potential complications such as surgical site infections and wound dehiscence from developing. So, general practitioners and the nurses for wound care, who are important part in the sub-acute management of post-operative wounds, should appreciate the physiology of wound healing and the principles of post-operative wound care [1].
Palliative wound care is complex, dynamic, and constantly evolving to balance the individual care needs of the palliative patient and his/her circle of care [2]. The patient's circle of care includes the members of the patient unit including family, significant others, caregivers, and other healthcare professionals who may be external to the current inter professional team [3]. When following a palliative wound care pathway, the focus shifts from traditional wound care, where healing and wound closure are the goals, to promoting comfort and dignity, relieving suffering, and improving quality of life [4]. Palliative care principles are adopted to meet the whole person care needs of terminally ill patients, as well as older and frailer people who often present with chronic debilitating diseases, advanced diseases associated with major organ failure (renal, hepatic, pulmonary, or cardiac), profound dementia, [5] complex psychosocial issues, diminished self-care abilities, and challenging wound-related symptoms, whether the wound has the potential to heal or not. The authors propose a paradigm that could be integrated along the continuum of wound care, and its relevance may vary with the individual's goals, disease processes, and wound condition.
Aim
The aim of this article is to update general practitioners and wound care nurses on the important aspects of surgical wound care since they have to have basic knowledge about the surgical wound care.This includes a review of the physiology behind wound healing, an update on wound cleansing and dressing methods, as well as a guide on how common surgical wound complications also should be managed.
Discussion
The main elements of surgical wound care include timely review of the wound, appropriate cleansing and dressing, as well as early recognition and active treatment of wound complications. Appropriate post-operative surgical wound care is essential in preventing potential complications, such as surgical-site infections (SSIs), wound dehiscence and haematomas. General practitioners play a major part in managing patient's postoperative wounds and it is important to appreciate the principles of post-operative wound management to minimise the incidence of wound complications.
Phases of Wound Healing
Wound healing is a dynamic process consisting of four continuous, overlapping, and precisely programmed phases. The events of each phase must happen in a precise and regulated manner. Interruptions, aberrancies, or prolongation in the process can lead to delayed wound healing or a non-healing chronic wound.
In adult humans, optimal wound healing involves the following the events:
Rapid hemostasis
Appropriate inflammation
Mesenchymal cell differentiation, proliferation, and migration to the wound site
Suitable angiogenesis
Prompt re-epithelialization (re-growth of epithelial tissue over the wound surface) and
Proper synthesis, cross-linking, and alignment of collagen to provide strength to the healing tissue.
The first phase of hemostasis begins immediately after wounding, with vascular constriction and fibrin clot formation. The clot and surrounding wound tissue release pro- inflammatory cytokines and growth factors such as transforming growth factor (TGF)-p, platelet-derived growth factor (PDGF), fibroblast growth factor (FGF), and epidermal growth factor (EGF). Once bleeding is controlled, inflammatory cells migrate into the wound (chemotaxis) and promote the inflammatory phase, which is characterized by the sequential infiltration of neutrophils, macrophages, and lymphocytes. A critical function of neutrophils is the clearance of invading microbes and cellular debris in the wound area, although these cells also produce substances such as proteases and reactive oxygen species (ROS), which cause some additional bystander damage.
Macrophages play multiple roles in wound healing. In the early wound, macrophages release cytokines that promote the inflammatory response by recruiting and activating additional leukocytes. Macrophages are also responsible for inducing and clearing apoptotic cells (including neutrophils), thus paving the way for the resolution of inflammation. As macrophages clear these apoptotic cells, they undergo a phenotypic transition to a reparative state that stimulates keratinocytes, fibroblasts, and angiogenesis to promote tissue regeneration. Inthis way, macrophages promote the transition to the proliferative phase of healing.
T-lymphocytes migrate into wounds following the inflammatory cells and macrophages, and peak during the late- proliferative/early-remodeling phase. The role of T-lymphocytes is not completely understood and is a current area of intensive investigation. Several studies suggest that delayed T-cell infiltration along with decreased T-cell concentration in the wound site is associated with impaired wound healing, while others have reported that CD 4+ cells (T-helper cells) have a positive role in wound healing and CD8+ cells (T-suppressor- cytotoxic cells) play an inhibitory role in wound healing. Interestingly, recent studies in mice deficient in both T- and B-cells have shown that scar formation is diminished in the absence of lymphocytes. In addition, skin gamma-delta T-cells regulate many aspects of wound healing, including maintaining tissue integrity, defending against pathogens, and regulating inflammation. These cells are also called dendritic epidermal T-cells (DETC), due to their unique dendritic morphology. DETC are activated by stressed, damaged, or transformed keratinocytes and produce fibroblast growth factor 7 (FGF-7), keratinocyte growth factors, and insulin-like growth factor-1, to support keratinocyte proliferation and cell survival. DETC also generate chemokines and cytokines that contribute to the initiation and regulation of the inflammatory response during wound healing. While cross-talk between skin gamma-delta T-cells and keratinocytes contributes to the maintenance of normal skin and wound healing, mice lacking or defective in skin gamma-delta T-cells show a delay in wound closure and a decrease in the proliferation of keratinocytes at the wound site.
The proliferative phase generally follows and overlaps with the inflammatory phase, and is characterized by epithelial proliferation and migration over the provisional matrix within the wound (re-epithelialization). In the reparative dermis, fibroblasts and endothelial cells are the most prominent cell types present and support capillary growth, collagen formation, and the formation of granulation tissue at the site of injury. Within the wound bed, fibroblasts produce collagen as well as glycosaminoglycans and proteoglycans, which are major components of the extracellular matrix (ECM). Following robust proliferation and ECM synthesis, wound healing enters the final remodeling phase, which can last for years. In this phase, regression of many of the newly formed capillaries occurs, so that vascular density of the wound returns to normal. One critical feature of the remodeling phase is ECM remodeling to an architecture that approaches that of the normal tissue. The wound also undergoes physical contraction throughout the entire wound-healing process, which is believed to be mediated by contractile fibroblasts (myofibroblasts) that appear in the wound.
The role of stem cells (SC) in cutaneous wound healing and tissue regeneration is a topic of increasing research attention, with a focus on the role of adult stem cells such as epidermal stem cells and bone-marrow (BM)-derived cells (BMDCs). Epidermal stem cells reside in the bulge area of hair follicles and in the basal layer of the epidermis and give rise to the keratinocytes that migrate andre-epithelialize wounds. Normal skin is also a target organ for BMDCs. Two main stem cell populations are present in the bone marrow: hematopoietic SC (HSC) and mesenchymal SC (MSC). BM-MSCs are able to differentiate into a variety of cell types, including adipocytes, osteoblasts, chondrocytes, fibroblasts, and keratinocytes. Endothelial progenitor cells (EPCs) derived from the HSC lineage are key cells that contribute to neovascularization. Both BM-MSCs and EPCs are involved in the cutaneous wound-healing process. Wound-induced hypoxia triggers the mobilization of bone marrow EPCs to the circulation, playing asignificant role in the process of neovascularization.
Several different cell types are involved in the wound- healing process, and, as described above, the cellular activities of any particular cell type may also vary during different stages of repair. The complexity and coordination of the healing process are major hurdles to therapeutic approaches, since any therapeutic must effectively be sequenced to the appropriate stage [6].
Types of Wound Healing
There are two main types of wound healing: primary healing and secondary healing. Most surgical wounds undergo primary closure in which there is minimal tissue loss and the wound edges can be satisfactorily approximated. This allows for primary healing in which there is rapid epithelialisation of the wound and minimal scarring [7].
Secondary healing refers to the process where a fullthickness wound is intentionally left open. This may be due to the presence of infection or an inability to satisfactorily approximate the wound edges. In secondary healing the wound heals by the natural way of granulation, eventual contraction and slow epithelialisation.4-6 Wounds that undergo secondary healing often result in larger scars [8,9].
The following are the most common types of chronic wounds treated at our Wound Healing Program:
Venous Leg Ulcers
Diabetic Ulcers
Pressure Ulcers
Non-healing wounds of traumatic origin
Our program also features Hyperbaric Oxygen Therapy (HBOT), a non-invasive treatment that involves high levels of concentrated oxygen which accelerates cell growth to create healing while it enhances the body's natural healing capabilities and promotes more rapid chronic wound recovery.
The most common indications for Hyperbaric Oxygen Therapy, approved by most insurance companies for the treatment of non-healing wounds, include:
Diabetic wounds of the lower extremities
Chronic refractory osteomyelitis
Compromised skin grafts
Osteoradionecrosis
Late effects of radiation therapy
Crush injuries
Acute carbon monoxide intoxication
Gas Gangrene [10].
Surgical Wound Care
Principles
Regardless of the mechanism of wound healing, the aims of post-operative wound care remain the same: to allow the wound to heal rapidly without complications, and with the best functional and aesthetic results [11].
Wounds intended to be healed by primary healing should, in particular, have their wound edges well approximated. In the initial phases of healing, there is only minimal tensile strength inthe wound as remodelling of the collagen fibres has not occurred. As such, additional support in the form of sutures, staples or tapes is required until full remodelling and epithelialisation occur.
Dressing of the Surgical Wound
Definition of terms
Clean versus sterile technique: Various definitions and descriptions of dressing technique for wound care exist. Terms have been used interchangeably and all are subject to individual interpretation. The following definitions provide a point of reference for the terms used in this document [12].
Sterile technique: Sterile is generally defined as meaning free from microorganisms [13] Sterile technique involves strategies used in patient care to reduce exposure to microorganisms and maintain objects and areas as free from microorganisms as possible. Sterile technique involves meticulous hand washing, use of a sterile field, use of sterile gloves for application of a sterile dressing, and use of sterile instruments. "Sterile to sterile" rules involve the use of only sterile instruments and materials in dressing change procedures; and avoiding contact between sterile instruments or materials and any non-sterile surface or products. Sterile technique is considered most appropriate in acute care hospital settings, for patients at high risk for infection, and for certain procedures such as sharp instrumental wound debridement [14-17].
Clean technique: Clean means free of dirt, marks, or stains. Clean technique involves strategies used in patient care to reduce the overall number of microorganisms or to prevent or reduce the risk of transmission of microorganisms from one person to another or from one place to another. Clean technique involves meticulous handwashing, maintaining a clean environment by preparing a clean field, using clean gloves and sterile instruments, and preventing direct contamination of materials and supplies. No "sterile to sterile" rules apply. This technique may also be referred to as non-sterile. Clean technique is considered most appropriate for long-term care, home care, and some clinic settings; for patients who are not at high risk for infection; and for patients receiving routine dressings for chronic wounds such as venous ulcers, or wounds healing by secondary intention with granulation tissue.
Aseptic technique: Asepsis or aseptic means free from pathogenic microorganisms. Aseptic technique is the purposeful prevention of the transfer of organisms from one person to another by keeping the microbe count to an irreducible minimum. Some authors have made a distinction between surgical asepsis or "sterile technique" used in surgery and medical asepsis or "clean technique" that involves procedures to reduce the number and transmission of pathogens.
No touch technique: No touch is a method of changing surface dressings without directly touching the wound or any surface that might come in contact with the wound. Clean gloves are used along with sterile solution/supplies/dressings that are maintained as clean [18].
Definition of infection: Infection has been defined as a continuum from contamination, colonization, critical colonization, biofilm, and infection.
Contamination: Contamination is the presence of non-replicating microorganisms on the surface of the wound. All open wounds have some level of bacterial burden that is ordinarily cleared by the host [19].
Colonization: In colonization, microorganisms attach to the wound surface and replicate but do not impair healing or cause signs and/or symptoms of infection. The bacteria are not pathogenic and do not require treatment. All chronic wounds are colonized to varying degrees.
Critical colonization: With critical colonization, the organisms attach to the wound surface, replicate and multiply to a level that affects skin cell proliferation and tissue repair without provoking systemic signs of infection. There is no invasion of the healthy tissue at this point.
Biofilm: Approximately 70% of chronic wounds have biofilm. When organisms adhere to the wound surface, they begin to develop biofilm, which is a complex system of microorganisms embedded in an extracellular, polysaccharide matrix that protects from the invasion of other organisms, phagocytosis, and many commonly used antibiotics and antiseptics. Biofilms are difficult to treat and eradicate. Recently it has been proposed that biofilm might be present in all chronic wounds.
Infection: Infection occurs when organisms on the wound surface invade the healthy tissue, reproduce, overwhelm the host resistance, and create cellular injury leading to local or systemic symptoms [20-24] Infection is often described quantitatively as a bacterial count of greater than 1015 colony-forming units (CFU) per gram of tissue. However, some organisms such as beta-hemolytic streptococci impair wound healing at less than 1015 CFU per gram of tissue [25]. According to Kravitz [26] infection should be defined as the presence of bacteria in any quantity that impairs wound healing.
Clinical signs of infection include lack of healing after 2 weeks of proper topical therapy, erythema, increase in amount or change in character of exudate, odor, increased local warmth, friable granulation tissue, edema or induration, pain or tenderness, fever, chills, elevated white blood cell count, and elevated glucose in patients with diabetes. In patients who are immunosuppressed or have ischemic wounds, signs of infection can be subtle. Signs of inflammation such as a faint halo of erythema and moderate amounts of drainage might be the only signs of an infected arterial wound [12].Studies have shown that in chronic wounds, increasing pain, friable granulation tissue, wound breakdown, and foul odor have high validity for infection [27,28].
Complications of Surgical Wound
Two common complications of surgical wounds are infections and wound dehiscence [29].
Disordered wound healing
Most wounds heal without complications and healing is not impaired in the elderly unless there are specific adverse factors or complications. Factors which may affect healing rate are [30]:
Poor blood supply.
Excess suture tension.
Long-term steroids.
Immunosuppressive therapy.
Radiotherapy.
Severe rheumatoid disease.
Malnutrition and vitamin deficiency.
Wound dehiscence
This affects about 2% of midline laparotomy wounds.
It is a serious complication with a mortality of up to 30%.
It is due to failure of wound closure technique.
It usually occurs between 7 and 10 days postoperatively.
Often, it is heralded by serosanguinous discharge from the wound.
It should be assumed that the defect involves the whole of the wound.
Initial management includes opiate analgesia, sterile dressing to the wound, fluid resuscitation and early return to theatre for re-suture under general anaesthesia.
Incisional Hernia [31]
This occurs in 10-15% of abdominal wounds, usually appearing within the first year but can be delayed by up to 15 years after surgery.
Risk factors include obesity, distension and poor muscle tone, wound infection and multiple use of the same incision site.
It presents as a bulge in the abdominal wall close to a previous wound. It is usually asymptomatic but there may be pain, especially if strangulation occurs. It tends to enlarge over time and become a nuisance.
Management: surgical repair where there is pain, strangulation or nuisance. The use of laparoscopic techniques and biosynthetic mesh is being evaluated [32,33].
Conclusion
The management of surgical wounds is very important part of post-operative recovery and the medicals and the wound care nurses should monitor the process of acute wound healing, prevent wound complications and treat appropriately if complications arise. They should care about the wound properly and prevent the wound from its complication which would lead into further complications.
For more Journals in Juniper Publishers please click on https://juniperpublishers.com/journals.php
For more articles in Journal of Nursing & Health Care please click on https://juniperpublishers.com/jojnhc/index.php
#Juniper Publishers#open access journals#Journal of Nursing & Health Care#Wound Care#Health Care#Primary Care#nurse practitioner
0 notes
Text
Psychodermatology: The Overlap of Skin and Psyche-Juniper Publishers

Abstract
Skin, brain and mind are interlinked and dermatological disorders are affected by as well as affect the psychological state of a person. The psychiatric morbidities such as anxiety, depression are common in skin conditions and the quality of life, especially psychological quality of life is adversely affected in psycho dermatological disorders. This article reviews the psychological impact of dermatological disorders and calls for close liaison between dermatology and psychiatry for favourable outcomes of these disorders.
Keywords: Psychodermatology; Psychocutaneous disorders; Psychosomatics
Introduction
Skin is the largest organ of human body; it expresses human emotion in its own unique way such as blushing, piloerection and perspiration. The skin as well as brain originate itself from embryonic ectoderm and responds to same hormones and neurotransmitters [1]. Skin is the also the most visible organ and everything that affects the skin is visible to others as well as to the patient himself forming an important part of one's self-image. In addition to the unpleasant physical sensations that take the person off balance, creating discomfort, irritation, impatience and damage to the physical appearance, skin disorders also compromise the individual's self-image and selfesteem. The psychological impact of dermatological disorders can be devastating to the patients, even though it may not be always associated with physical discomfort or pain [2].
Discussion
The incidence of psychiatric disorders among dermatological patients is estimated around 30 to 60% [3] and patients of chronic dermatological patients experience significant emotional pain [4]. The interaction between nervous system, skin and immunity has been explained by release of mediators from NICS (neuro immuno-cutaneous system) [5]. Psychological stress is believed to disrupt the epidermal permeability barrier homeostasis, and it may act as a precipitant for some inflammatory skin disorders like atopic dermatitis and psoriasis [6]. The psychological factors can be big concern in chronic intractable disorders eczema, prurigo, psoriasis and vitiligo [7-9]. The psychiatric help seeking behaviour in dermatological patients however is not in proportion to the psychiatric morbidity in these patients and patient often resist the psychiatric referrals due to widespread stigma and misconceptions about psychiatric diagnoses. Therefore the liaison between psychiatrists and dermatologist proves very helpful for optimum management of psychodermatological disorders with emphasis on biopsychosocial model of disorders.
Psychodermatology refers to the psychological or psychiatric aspects associated with dermatological disorders. These disorders can be classified into four categories namely:
Psychophysiologic disorders, dermatological conditions associated closely and exacerbated by stress.
Primary psychiatric disorders with dermatological symptoms due to pathological thinking process.
Secondary psychiatric conditions as response to stress of dermatological condition.
Cutaneous sensory disorder presenting as sensory conditions with no underlying dermatological or general medical condition [10].
We in this review endeavour to focus on the psychiatric morbidity in dermatological disorders, which would cover psychophysiologic disorders and psychiatric disorders secondary to dermatological conditions.
Psoriasis
Psoriasis is a chronic skin disease that affects approximately 2-3% of world population, with its onset in the second or third decade of life. This disorder fits the biopsychosocial model of etiology and is caused by the interaction of genetic (polygenic inheritance), environmental and psychological factors [11]. Psychological stress is known to exacerbate the condition and commonly associated with depression, anxiety and somatization [12-15]. Suicidal ideations are not uncommon to be reported in patients of psoriasis and it is associated with significant impairment of quality of life, negatively impacting psychological, vocational, social and physical functioning [15,16]. Five dimensions of the stigma associated with psoriasis have been reported:
Anticipation of rejection.
Feelings of being flawed.
Sensitivity to the attitudes of society.
Guilt and shame.
Secretiveness [17].
However, the severity of psychiatric symptoms may not be always proportional to the clinical severity of psoriasis.
Atopic Dermatitis
Atopic dermatitis is a chronic skin condition with pruritus, scaling, erythema, excoriation and lichenification making it very distressing for the patients. Adults with atopic dermatitis are more anxious and depressed with psychosocial adjustment issue and low self esteem whereas children suffer emotional distress and more behavioural problems [18-21]. Psychological stress may be an acquired factor affectingthe expression of atopic dermatitis [22]. A topic individuals with emotional problems may develop a vicious cyclebetween anxiety/depression and dermatologic symptoms [23].
Acne Vulgaris
Acne is an inflammation of the pilosebaceous glands mostly affecting face and trunk affecting mostly adolescents. It has a great importance among the dermatoses that affect adolescents, in view of its high prevalence in this age group and its effect on the quality of life which becomes more pronounced as the stage of the disease becomes more severe [24]. It is associated with depression and severe cases are more likely to have severe depressive features [25]. Apart from it the drug isotretinoin has side effects in the form of depression and suicidal ideas which needs tobe kept in mind while treating patients of acne.
Alopecia Areata
Alopecia areata is a common disease involving localized loss of hair in round or oval areas, without visible inflammation of the skin in hair-bearing areas. The role of psychological factors in the pathogenesis of alopecia areata is debatable [26]. The psychiatric morbidity in patients of alopecia areata ranges from 25-67% [27-29]. Anxiety and depression remain the commonest comrbid psychiatric disorders in these patients [30,31]. The quality of life is poorer in patients of alopecia areata when compared to control but it does not depend on severity of the illness [32].
Urticaria
Chronic idiopathic urticaria (CIU) is characterized by recurrent urticarial wheals of unknown origin for 6 or more weeks' duration. It is one of the most common and frustrating diseases for both patients and physicians [33,34]. The quality of life of these patients is greatly affected by the disorder [35]. The physical and psychological quality of life in chronic idiopathic urticaria is markedly reduced [36] which is suggestive of the severe distress because of the disorder. When it comes to psychiatric morbidity literature suggests that anxiety and depression is common in cases of urticaria [36,37].
Vitiligo
Vitiligo is a depigmentary disorder which mostly painless, however cosmetic disfigurement is the source of discomfort. It is also unfortunately associated with great social stigma especially in societies like India where once patients of vitiligo were treated as untouchables. Vitiligo runs a chronic and unpredictable course requiring long term treatment but there is no uniform effective therapy and this is usually very demoralizing for patients [38]. Patients reveal indications of significant distress that are related to specific types of social encounters and emotional disturbances [39]. The quality of life in patients of vitiligo is hampered, especially in female patients. The psychological and environmental quality of life is affected in a negative way due to psychosocial impact of the disorder [9] Vitiligo patients are stared at, whispered about or subjected to antagonism, insult, isolation and are greeted differently [38] and high number of patients of vitiligo suffer from depression [40] and tend to feel more hopeless with time [41]. Impact of vitiligo remains more psychosocial than purely medical in this sense.
Conclusion
The research in psychodermatology is growing and insightful. The quality of life in these disorders is affected in most cases and various factors negatively affecting it are the chronicity of disorder, inconveniences of the disorders and therapy, lack of uniform response to therapy, cosmetic impact and easy noticeability. The common comorbidities include anxiety, depression which may not be related to clinical severity of these disorders always but psychological deterioration is invariably associated with an exacerbation of the dermatological condition. The liaison between these two disciplines of psychiatry and dermatology holds the key for favourable outcome of the psychodermatological disorders.
For more articles in Journal of Nursing & Health Care please click on https://juniperpublishers.com/jojnhc/index.php
For more Journals in Juniper Publishers please click on https://juniperpublishers.com/journals.php
#Juniper Publishers#Open Access Journals#Juniper Publishers Publishing Group#Journal of Nursing#Health Care#Psychology Care#Mental Health
0 notes
Text
An Empirical and In Silico Study of the Survival of Dairy Cows in Heterogeneous Population | Juniper Publishers
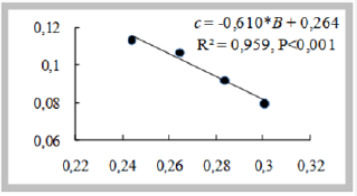
Juniper Publishers-Open Access Journal of Agricultural Research & Technology
Authored by Gennady G Cherepanov
Abstract
The data from biomedical studies show that the patterns of mortality in a population considered as a whole may differ significantly from the mortality rates in the constituent subpopulations. An analysis of empirical data reveals heterogeneity in survival parameters in populations of various types of laboratory animals and humans. The aim of this work is to present empirical data and results of in silico study indicating the possible approaches for early forecasting the viability of dairy cows in heterogeneous populations.
Introduction
The data from bio-medical studies show that the patterns of mortality in a population considered as a whole may differ significantly from the mortality rates in the constituent subpopulations. An analysis of empirical data reveals heterogeneity in survival parameters in populations of various types of laboratory animals and humans [1]. In the study of the health status of the public health in radiation lesions, taking into account the heterogeneity of populations allows obtaining more accurate estimates of risk factors [2]. The fact that the revealed consistent patterns have of general biological nature is evidenced by the results of the analysis of empirical data on the age dynamics of productivity and survival in the populations of dairy cattle [3].Several methodological approaches for early quantifying the viability of cows at the level of group (e.g., bull’s daughters), herd or population were described by the author earlier [4]. The aim of this work is to present empirical data and results of in silico study indicating the possible approaches for early forecasting the viability of dairy cows in heterogeneous populations.Empirical studyAs a material for the study, the records of the age composition of the herds of Black-and-White cows in 16 breeding firms of the Leningrad oblast of Russian Federation in the period 1985–1990 were used, averaged over 5 years to compensate for deviations from stationary state in herds turnover. The dynamics of culling rate of cows from the herd (culling intensity from respective cohort when herd is in stationary state of turnover) in most cases is usually approximated by the Gompertz function yc(t)
Where; t: is number of the current lactation, S: Is the quantity of cows in cohort, ΔS: Is the difference in the number of cows at the previous and current lactation, Δt: 1, B and c are constants.The function, inverse to the culling intensity, characterizes the age decrease of viability. The dynamics of cows leaving the dairy herd over 8-10 lactations in 16 breeding units was approximated by the Gompertz function with an average value of R2 = 0.79.When analyzing the data obtained, a higher level of variability in the parameter B was noted (the intensity of culling at first lactation), compared with parameter c. Previously, certain grounds were obtained for interpreting the reciprocal of yc1 (yс at t=1), i.e. B-1 e-c as an indicator characterizing the viability potential of this group of animals [4,5]. In other words, differences in the level of viability formed at the beginning of reproductive period can determine (on the average, in group or population) differences in the length of productive life (LPL) [4].This pattern will be most clearly expressed if the compared groups or populations have similar values of c in the Gompertz function. This is theoretically possible in a situation if the aging rate, characterized by c, is determined mainly by stable genetic factors, including the breed features. Since the Leningrad type of Black-and-White breed during period of data registration was a stable population, it can be assumed that this population could have the same value of c, and the variations found between the components of this population are due to the heterogeneity of the studied herds in respect to values of the parameter B.As a definite argument in favor of this second interpretation of the variability in parameter с, it can be considered the negative relationship between the parameters B and c detected in 16 studied breeding firms (c = 0.19 - 0.45*B, R2 = 0.69, P<0.001), i.e. the more B, the less с. This gives grounds for assuming that the herds studied are heterogeneous in terms of survival dynamics, while variations in the values of the parameter B have a significant effect on the values of с recorded in the studied herds.Study in silicoTo verify the assumptions made, 4 series of calculations were performed on the Gompertz discrete model implemented in the format Excell MS with a step Δt = 1 to predict survival of cows in four model heterogeneous subpopulations (I-IV) with the same initial number n (1000 cows at the first lactation), each of which consists of four homogeneous groups with different values of the initial number n and parameter B, but with the same value of c (c = 0.1) (Table 1).Note: n: Initial size of the homogeneous groups (number of cows at the first lactation), B: Parameter in Gompertz function, tmax: Maximal length of productive life (in lactation numbers).It is assumed that this model experiment reproduces the main features of the studied situation in which all 16 subpopulations belonging to breeding firms in different regions of Leningrad oblast, consist of several groups homogeneous by parameter c, i.e. having the same value of this parameter, but different values of B. In the calculations, the truncated Gompertz distribution was used and as the maximum LPL (tmax), the value of t was taken, at which the number of unrecorded long-lived cows is a negligible small fraction (less than 2-5%) of the initial number (at the first lactation). Under this condition, the average LPL (T) is approximately 2 times less than the value of tmax [3]. The dynamics of culling rate in the four model heterogeneous populations were approximated by the Gompertz function with a high coefficient of determination (R2 = 0.81-0.92); the values of c in variants I-IV varied from 0.079 to 0.113 (in all homogeneous groups in the subpopulations, c = 0.1), and there was a close negative relationship between the values of B and c (Figure 1).The fact that the correlation between B and c, detected in the modeling longevity in heterogeneous population, is also established on empirical data for 16 breeding farms, supports the above formulated assumption that the rate of aging of dairy cows, characterized by the value of c in Gompertz function, is determined mainly by stable genetic factors, including breed features, whereas the observed population variability of LPL depends on the viability potential formed to the beginning of the reproductive period. Earlier, it was shown that this potential can be expressed as the reciprocal of the culling rate at the first lactation [4]. The results of this in silico study confirmed the presence of a negative correlation between the value of B and the LPL in the total set of homogeneous groups that have the same value of c (Figure 2).The results obtained, and our interpretation of the identified patterns are consistent with the scientific data, indicating that the animal viability is determined not only by genotypic factors, but also by epigenetic modifications, arising in response to endogenous and exogenous effects at the early stages of ontogenesis [6-10]. Since the identified patterns depend not only on the inherited genetic structures, but also on the “history” of events occurring during critical periods of development, descendants are born in cows, and groups (subpopulations) with different potential of viability are formed in herds and populations.
Conclusion
In general, the data obtained suggest that to create optimal type of dairy cows with a balanced ratio of milk productivity and viability, as well as for early prediction of the length of productive life, it is reasonable to create a system of lifelong monitoring of external influences and the physiological status of animals at all stages of ontogenesis, as well as an appropriate data analysis technologies for finding the effective predictive tests. Possible candidates for the role of tests for the prediction of productive longevity should not be search in terms of physiological homeostasis; they are more likely to be found in the area of action of constitutive and epigenetic factors. To extend the length of productive life, in addition to fighting diseases, it is necessary to increase the “initial” value of total resistance, i.e. functional reserves at a young age, with the use of different approaches, including selection, elimination of adverse deviations in the course of embryonic, fetal and postnatal development, as well as the application of technological influences at a young age, contributing to an increase in overall protective reserves.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Agricultural Research & Technology please click on: https://juniperpublishers.com/artoaj/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/artoaj/ARTOAJ.MS.ID.556088.php
#Juniper Publishers#Juniper Publishers Publishing Group#Open Access journals#Juniper Publishers LLC#Juniper Publishers Reveiw
45 notes
·
View notes
Text
Trauma, Mental Health, Coping, Resilience, and Post Traumatic Growth (PG)-Palestinian Experience-Juniper Publishers
For more Journals in Juniper Publishers please click on https://juniperpublishers.com/journals.php
Introduction
Coping
Based on Lazarus and Folkman's [1] model, coping refers to the behavioral and cognitive efforts one uses to manage the internal and external demands of a stressful situation. Coping can be classified as being either problem-focused or emotion- focused in nature. Lazarus & Folkman's [1] stress-coping theory, in which the individual assesses both the relevance of the environmental stressor (i.e. what he or she has at stake in the encounter) and his or her coping options before deciding on coping strategies to deal with the stressor. This theory's general emphasis on “coping,” however, could be expanded to encompass “development” or “growth.” There are three dimensions are most commonly used to categorize coping strategies:
Problem-focused and emotion-focused coping.
Primary and secondary control coping.
Engagement and disengagement coping (also referred to as approach versus avoidance coping) [2].
Problem-focused coping involves activities that focus on directly changing elements of the stressful situation.
Emotion-focused coping involves activities that focus more on modifying one's internal reactions resulting from the stressful situation.
Coping strategies includes a broad diversity of thoughts and behaviors used to manage the demands of a taxing situation [1]. Multiple research groups have attempted to organize coping strategies (and styles) into different categories.
The approach/avoidance construct, as the label implies, indicates whether the individual makes attempts to change the situation or distance him- or herself from the stressor as a way to reduce negative outcomes.
Coping strategies implemented immediately following trauma exposure, and in response to post traumatic stress. Avoidance as a sort of coping, such as behavioral or emotional avoidance, have been associated with increased psychological distress among interpersonal violence PTSD populations [3]. Avoidance behaviors could lead to withdrawal from support networks and reduced opportunities for positive experience, thereby compounding negative affect and reduced emotional experiencing. Approach-oriented coping strategies, such as active coping, planning, and support seeking, have been generally deemed adaptive following exposure to stress [4].
Social support is a variable that has been considered as both a means of coping and a resource contributing to the availability of other forms of coping [5]. The different ways of conceptualizing the role of social support in coping, and the relative lack of studies that examine reciprocal relationships between coping factors, has created some confusion about what roles social support may play in helping women deal with domestic violence.
Resilience
Over the decades, definitions of resilience in sciences concerned with child and family systems have become more dynamic, multilevel, and process oriented in focus, reflecting a broad theoretical shift toward a relational developmental systems framework in life course human developmental science and related fields [6].
Resilience and post traumatic growth (PG) theory and research are rooted in the philosophical stance that emphasizes the consideration of positive (salutogenic), rather than pathological or negative factors in trauma research [7]. Distinctions should also be made between posttraumatic growth and the concepts of resilience, hardiness, optimism, and sense of coherence. All these concepts describe certain personal characteristics that allow people to manage adversity well.
Resilience is usually considered to be an ability to go on with life after hardship and adversity, or to continue living a purposeful life after experiencing hardship and adversity. Smith defined resilience as a process that leads to "strength awareness", but psychological resilience may be operationally defined as strength awareness itself-that is, the belief that one can persevere or accomplish goal-relevant tasks across varied challenges and adverse situations.
Given this growing interest in scalable definitions, resilience can be defined broadly as "the capacity of a dynamic system to adapt successfully to disturbances that threaten its function, viability, or development" [8]. This definition of resilience could apply to an individual, family, computer system, economy, or ecosystem, among other systems. The capacity of any given system to adapt to challenges depends on the function of many interacting, changing systems. The resilience of children and their families are intertwined and also linked to supports and systems beyond the family in community, culture, and the physical environment.
Child resilience investigators have long recognized that resilience is inferred from judgments about risk (discussed further below) and adaptive function or development [9]; What are the criteria or standards by which we identify whether a person, a family, or any other system is adapting well? Issues in defining positive child development, adaptation, competence, or success have received considerable attention in child resilience science. What are the criteria or standards by which we identify whether a person, a family, or any other system is adapting well? One major approach to the criteria for judging adaptation is positive, focused on age-related expectations for behavior and achievement defined by communities and societies, often termed "developmental tasks" [10]. A second approach for judging adaptation, defined by low levels or absence of symptoms or disorder, stems from the initial focus on children at risk for psychopathology in the history of child resilience science. This negative approach has been criticized theoretically [11] and also from a common-sense perspective.
Family Resilience
What does it mean for a family system to be doing well or fulflling its functions effectively? Walsh [12], the concept of family resilience shifted attention from family as a resource or protective system for the individual members of a family to the function of the family unit as a whole, studied in terms of family adaptation or maladaptation in the context of adversity and the family processes that sustain family resilience. McCubbin [13] described the desired outcomes of family resilience in terms of success in fulfilling important expected functions of the family. These tasks included functions such as providing a sense of belonging and meaning, affording economic support, educating and socializing family members, and protecting vulnerable members of the family [14]. The effectiveness or success of a family would then be judged according to these expectations. Again, the criteria were multidimensional.
Post Traumatic Growth
In contrast, post traumatic growth refers to a change in people that goes beyond an ability to resist and not be damaged by highly stressful circumstances. Calhoun defined post traumatic growth as "positive change that an individual experiences as a result of the struggle with a traumatic event". In contrast to the construct of resilience, in which the individual returns to baseline functioning following highly stressful or traumatic experience, post traumatic growth is characterized by post-event adaptation that exceeds pre-event levels. Despite this interesting body of literature, there is still limited evidence on how living in areas of war and political conflict impact on university students, and which types of personal growth they may develop in response in relation to resilience. The aim of this paper to review papers conducted in Gaza Strip targeting children and adults using coping, resilience, and PTG.
Method
The author reviewed all his previous work in the area using the available data.
Results
As shown in the Table 1, 2 & 3 [26].
For more Journals in Juniper Publishers please click on https://juniperpublishers.com/journals.php
For more articles in Journal of Nursing & Health Care please click on https://juniperpublishers.com/jojnhc/index.php
#juniper Publishers#Open Access Journals#Juniper Publishers Publishing Group#Journal of Nursing & Health Care#Mental Health
0 notes
Text
The Exercise Continuum and the Role of Doctors | Juniper Publishers

Juniper Publishers-Open Access Journal of Gerontology & Geriatric Medicine
Authored by Andrew Hague
Introduction
Everyone can be placed somewhere on an exercise continuum with the idle at one end and the hyperactive at the other. At both extremes, health suffers. Exercise is essential to health and managing it is the responsibility of individuals but few know what they should do. Doctors seldom teach how to be healthy and act only when repair is needed.
The Idle
In the oceans, lakes and rivers are creatures that stay in one place and water flows over them bringing food to their open mouths and removing waste from the opposite end of their bodies. Of all land animals, humans are the only creatures able to exist by the same idle method. The human brain can contrive a situation in which other humans care for idle ones and this is not about looking after a patient in bed, it is feeding an idle person who commands others. That image, perhaps of ancient kings, is seen by many to represent ultimate ambition; servants supplying all needs. The reality is that the idle one is the one that suffers and those scurrying around have more benefits.These days, physical inactivity is available to all, rich and poor and some of the poor appear to love it. Getting food has become no more arduous than opening a packet. Ordering and paying for it is done by pressing buttons on a smart phone and getting the money in the first place is in some countries only a matter of getting state aid on the grounds of unemployment or being unable to work. The more idle they are, the less they are able to work. The consequences are obesity, diabetes and heart disease. Muscles weaken and joints are unable to carry the added weight. Generally, idleness is accompanied by little mental stimulation which leads to further decay of the body. Doctors are then asked to make repairs. In go the drugs, up go the pharmaceutical profits and up go the costs to insurers and governments. Should the doctor take the smart phone away, ban them from television and send them swimming three times a day because swimming is less damaging to fat limbs than walking and to run is impossible? Such hardship would help the patient and in some rare cases it is being done. Usually they get drugs and a suggestion that they should exercise but no enforcement. This is the situation in the prosperous countries in recent years.
The Hyperactive
In racing sports, they talk of going through the pain barrier. The margin of safety is considerable. Grin and bear it and you will win. By that means, it was not always the strongest who won but the person who could tolerate most suffering. When drugs became available, the pain barrier ceased to be a barrier and the body lost its protection. The determination to win would expose the body to excess stress that could be fatal (Figure 1).I took this photograph of a bicycle hill climb in 1965. Almost certainly no performance enhancing drugs were used. At the finish line, all the competitors were gasping for breath and some lay on their back to recover but they were up again in a few minutes grinning and eager to find out their time. The winner I knew well back in those days and he went on to become the National Hill Climb Champion. He was only a year older than me and, from what I have been able to find out, he died some years ago of a strange illness. He had suffered a crash in a race and had never properly recovered. This, as I see it, is a danger. He had pushed himself too far, not just in physical effort but by taking chances. It was a risk he would not ordinarily have taken but, in a race, where everything is about winning it becomes combat.The drugs scandals at the Olympic games and in the Tour de France cycle race are now headline news. That competitors will sacrifice their lives for the vanity of winning shows the danger of sport at this level.Amongst amateurs, dangers abound. There are combat sports that were encouraged because they prepare soldiers for battle. With less hand to hand fighting in modern armies and more alternatives in schools that are threatened by lawyers there is less boxing but rugby is still popular especially in fee- paying schools. A young boy’s father will tell him that the rough treatment in a game of rugby will make a man of him. If the boy is stocky enough and determined, it is very likely he will have a life changing injury before he is thirty. Physiotherapists and orthopaedic surgeons specialising in joint replacements are grateful to football, squash and tennis for the business it brings. Footballers get kicked as well as adding pressure to their knees and hips. Racquet games twist the knees more violently than straightforward running with the result that a titanium implant is offered as the easy repair. The fact that a revision (another replacement) will be needed ten to fifteen years hence is seldom mentioned.At the extremities of all sports there are dangers even in those that are danger-avoidant. Rock climbing is all about fall prevention until the glory of not using a rope takes over and then there is no back up. Mountaineering is safe until risk taking becomes more attractive than the scenery and the threats of bad weather, an avalanche or thaw (the ice giving way) are pushed to one side believing that these hazards have been overcome before. Confidence leads to invincibility, a concept that has never been proven.Over confidence is as much a danger as depression. The role of exercise in combatting depression with the suicides and anger that arise are seldom appreciated. Mental health benefits from exercise as much if not more than bodily health.There are many activities classed as sports that do not involve muscles and cause damage to the participants and even more so to spectators. Motor racing is a major culprit. Deaths on the track are less than they used to be but they instil a culture of speed which on the public road will kill. It was often commented years ago when people went to the cinema that after a James Bond film the cars were hurtling away a break neck speeds with the drivers inspired by what had enthralled them half an hour before. Motor racing is nonsense. The winner is not the most skilful but the one prepared to take most risk. Is that meritous? It is not even a sport. Shooting must be equally condemned. Just as the ancient Greeks may have delighted in wrestling and the Romans in gladiator fights, those sports gave way to fencing and when those weapons were superseded by guns it was shooting that was applauded. To aim, it is necessary to be fit, so the argument goes, so that one can hold one’s breath when firing to keep the gun steady as one breaths. Does that compare with the fitness of a swimmer or any athlete? When the target for shooting is an innocent wild animal or bird, the claim that this is a sport is hard to sustain.It is a fact that most people are impressionable; they are followers and do not question those they admire. This gives role models a responsibility many of them do not understand. A star footballer is seldom an intellectual. From being groomed at school to being paid to play the game, he has learned only that what he does is right; it must be because he is paid a lot to do it and whatever he does must be right. He has a licence to do anything because at the extreme end of the exercise continuum he excels. Brawn beats brain and entertainment damages a thoughtless majority. Doctors are left to pick up the pieces. Could they have advised so that the damage is avoided?
The Importance of Exercise
Between the extremes of immobility and hyper-activity is where we should be but where is it? A good observation is a report on cycling to and from work:Kevin Murnane writes: The effects of walking and cycling were measured by comparing them with the Non-active mode of transport. Cycling to work was associated with very large health benefits. Commuters who cycled to work had a 41% lower risk of dying from all causes than people who drove or took public transport. They also had a 46% lower risk of developing and a 52% lower risk of dying from cardiovascular disease, and a 45% lower risk of developing and a 40% lower risk of dying from cancer.This is a study of ordinary people doing what everyone does, getting around as easily as possible. When it involves exercise, there are great benefits - listed in the article:a) Cycling makes you happyb) You lose weightc) And build muscled) Without worrying about over eatinge) Good for the lungsf) Cuts heart disease and risk of cancerg) Less damage to jointsh) Saves time and moneyi) Mental skill of route findingj) Better sexk) Better sleepl) More brain powerm) Improved reactions and responsesn) Better immune systemo) More friendsEach one of the above would be a medical breakthrough. To get the lot for free is astounding and true.In richer countries in the last decade cycling has become more popular and is said to be the new golf. For those who have always cycled, it is flattering to be recognised as sensible and not shouted off the road as used to happen. When the scientists investigate, they explain what to the cyclist is obvious.Michelle Arthurs-Brennan reports that a study followed 125 long-distance cyclists. The riders are now all in their 80’s but their immune system function is similar to that of 20-year-olds. The research, published in the Aging Cell journal, showed that the ageing cyclists produced the same number of T-cells - which help the immune system respond to new infections - as adults still in their 20s, and a separate study revealed that cyclists didn’t lose muscle mass, strength, or gain body fat in the same way as non-cyclists.Co-author of the report, Prof Norman Lazarus of King’s College London is 82 himself; he told the BBC: “If exercise was a pill, everyone would be taking it. It has wide-ranging benefits for the body, the mind, for our muscles and our immune system."In parallel, the same journalist presents a report on the sex lives of female cyclists:Saddle discomfort is mentioned and the solution is a well- made lady’s saddle of which there are many on the market. They have a slot along the top to avoid pressure on the genitalia. Usually the nose of the saddle is angled down for a lady whereas a man will have the saddle horizontal. Every woman should be able to ride comfortably. If you have a problem, a good bike shop will help you. (BioFlex O-Zone Gel Womens Saddle - Black).The reports about Robert Marchand are incredible. He is the first of many in his category. One year after setting a new Hour Record for his age category, centenarian cyclist Robert Marchand has decided to hang up his wheels and retire from competitive riding at the grand old age of 106. A multiple record holder for age-group events, Marchand has now been advised not to take on any further competitive events on medical grounds. He can continue cycling but should stop racing. Read the report and note that there is nothing extraordinary about Robert other than he is doing what others half his age could not do. If he can do it, others can. Born in Amiens in 1911, Marchand started riding at the age of 14, but gave up the sport only to return to cycling in 1978 aged 67. Since then he has maintained a daily routine of riding and stretching, eating plenty of vegetables and little meat, not smoking, and generally avoiding alcohol.Here is a report on a study of aging published on 6th January 2015 in The Journal of Physiology:a) Emeritus Professor Norman Lazarus, a member of the King’s team and also a cyclist, said: "Inevitably, our bodies will experience some decline with age, but staying physically active can buy you extra years of function compared to sedentary people.b) "Cycling not only keeps you mentally alert but requires the vigorous use of many of the body’s key systems, such as your muscles, heart and lungs which you need for maintaining health and for reducing the risks associated with numerous diseases."c) On the 8th March 2018, Prof Lazarus’s team published another study in Aging Cell published by the Anatomical Society and John Wiley & Sons Ltd. and appears to be a similar group of people, maybe the same.d) Study confirming old cyclists same as healthy young.e) The benefits of exercise all one’s life has always been known. The biological data is now measured in the Aging Cell report of the study by Birmingham University.f) Dr Ross Pollock, who led the team of scientists from King’s College London, warned that most of us are inactive, which causes ‘physiological problems at any age’.Study of cyclists found they were physically younger than most their age Underwent extensive tests of their heart, lungs and exercise capacity Researchers found they had muscle strength similar to younger people Say it proves cycling keeps the body and the mind staying young Aging and Physical Performance.
Mind and Body
If the articles referred to above suggest that all that is needed to get all the benefits is to move muscle, think again. The mind and body are inseparable. In a paper published last year on The Body’s Operating System, I discussed the effect of mind on body. The interaction is also body on mind. The Birmingham and Kings Studies accurately report the biological effects of exercise. It should be obvious that the same effect will apply to runners, walkers, swimmers and all active people. In these studies, cyclists formed a convenient group that could be identified and measured. Kevin Murnane’s article listing 15 benefits is correct. This includes mental health. One cannot cycle without thinking. The machine has to be maintained. It can fail when you are miles from home and you have to fix it. Problem solving is where our brain excels. It distinguishes us from other animals and has got us to the stage where we can disrupt our environment; to solve the problems we have created (Figure 2).The man repairing a puncture became the British National Hill Climb Champion. With modern tyres and less glass on the road, punctures are not as common as they were. We used to always repair the puncture, not just fit a new tube, and competed to see how many patches were on a tube before it was eventually discarded. You will see that his friends are there to tell him what to do even though he would do better without their distraction. This is social interaction at its best. The group broke up as members dispersed to study and work, married and, in some cases, died. I am still cycling and, if this article makes sense to you, am still fit and cognitively active. The Birmingham-Kings studies required the old cyclists to be able to ride at ten miles an hour for over six hours. Believe it or not that is very easy. Normal cycling speed is 14 mph and a club (chain gang) can be doing evens (20 mph or more). For 10 mph to make the difference between being as fit as a person 40 years younger is very interesting.This shows that the discovery is not that exercise helps, it is that no exercise is damaging. To exercise always all one’s life is normal. To refer to the cyclists as a remarkable minority is to forget what we are, animals born to forage and hunt from dawn to dusk. To feed, we had to exert. When people are astounded that I can ride a hundred miles (160 km) a day, I tell them it is only ten miles an hour for ten hours. If there was more time available, I would be able to cover longer distances. It is not a matter of strength. A normal person is well capable of these distances. The pity is, they don’t know it. Nevertheless, more people are discovering they have hidden talent. Often a bicycle is daunting and they do not live where there are quiet roads. They make go walking, Scottish dancing, swimming or just flogging themselves in the gym.
Resistance
Look at again at the photo of the puncture being repaired. This was before most wheels had quick release hubs. He has taken the tube out of the cover without removing the wheel to avoid getting his hands dirty on the oily chain but he is still going to end up with the grime of the road and aluminium oxide from the rim on his hands and nowhere to wash them. The simple answer is to peel and eat an orange. We were never ill. In the summer of 1966 I cycled from Graz to Athens on unsurfaced roads through the Balkans averaging over a hundred miles a day. There were no plastic bottles of water for sale in shops back then. The water bottle carried in a cage on the bike frame was topped up at roadside wells and pumps. I never had diarrhoea and I drank a lot cycling in the heat through Greece. Nowadays, our exposure to germs is no less but our resistance is far less. Go on an airline flight for a few hours and breath the air expelled by your fellow passengers and be prepared for a sniffling cold for a few days afterwards. These are serious dangers.Exercise in the open air, away from cities and pollution and your immune system improves not just from exercise but from the simple relationship with your environment, a relationship with which we have evolved. India has a campaign for indoor toilets to be flushed clean by water and proper sewage management. Outdoor defecation that had served for centuries became impractical as population density increased and privacy, especially for the girls and women, became difficult. They are moving to a modern system in which chemicals will certainly be used to solve one problem and cause others. The immune systems will adapt maintained by exercise, sleep, diet and a balanced approach to hygiene. We can be too careful.
Sunshine
Use of gyms is growing and is to be encouraged. For a traditionalist and outdoors man like me, a gym is hard work and uninspiring. In some climates, extremes of hot and cold, it can be the only option. In temperate climates the smell of fresh air, birds singing and wind in the face is pleasure. What the scientists investigating the improvement to the immune system did not record is the vitamin D from sunlight. You don’t get it in a gym and the modern practice of protecting the skin from the sun reduces the essential vitamin intake. Sunglasses are worn too often. There appears to be a belief that they protect the eyes. If that were true, I should be blind by now. Bright sunshine tells the skin to beware, it changes and adds protection. People outdoors all the time seldom have the skin cancers that attack those exposed infrequently to unfiltered sun. In high altitude Switzerland and under the thin skies of New Zealand and the southern hemisphere, the conditions are dangerous and protection is essential. Under the haze of The Gulf, sunburn is less a risk.
Diet and Drinks
The old cyclists who have cycled almost all their lives learned what to eat and what to avoid. Very few smoked and that made them outcasts in the 1950s and 60s when the majority of people smoked. You did not need to be a scientist to see that the smoker had not got the puff to pedal. In other words, his lungs were being damaged by smoke. In those days, and I remember them well, almost all doctors smoked. In their ignorance, they gave their patients bad advice.Food was frequently discussed. We had large appetites. There was more organic food fifty years ago and it was fresher because transport was less efficient than today; food had to be grown locally. Knowing what was best to eat was understood by all and we worked it out empirically. One rider worked as a window cleaner during the week and cycled at the weekend so he was physically active outdoors every day in all weathers. He was our advisor and paid little attention to books. His knowledge came from experience. He never added sugar to his drinks or salt to his food and his explanation made sense to all of us. There was enough carbohydrate in a balanced diet and too much sugar meant too little roughage. Bran and the bike kept him regular. The amount of salt added to bread was more than enough in a temperate climate. Maybe in hot weather when sweating increased the water through-put there is a case for additional salt and more fluids but for the mileage we were doing, about 80 miles on a Sunday run, no additives were needed.We learned to not be on the road after 10 o'clock at night because the drinkers would be driving away from the pubs drunk. It was not illegal to be drunk driving a car. Indeed, when there was a crash, the defence was that the alcohol made the driver incapable so it was only an accident, not deliberate bad driving. If the driver was incapable, he could not be blamed. Eventually this nonsense led to laws banning drivers from drinking alcohol and there seems to be a recent understanding amongst the general population that alcohol damages health. Cyclists knew it many years ago and by avoiding alcohol they have maintained good health. People have to be told. Is that the duty of doctors?
Resilience
Whether you are on a mountain ridge in the mist or miles from anywhere on a bicycle, you have only yourself to depend on. You may have companions and they look to you for leadership. You have no choice but to be resilient and carry on, map reading, apportioning your energy, not taking risks. It is all about survival. Move then to a city job and your mental attitude goes with you. Exercise maintained your health mentally and bodily.
The Role of Doctors
Clinical evidence that the minority group of old cyclists have an immune system comparable to people in their twenties is proof that the majority of people are in poor health because they do not exercise. If a doctor’s duty is to improve people’s health, then the doctor has to tell them to exercise and say it before the deterioration goes too far. On the other hand, if a doctor is there only to repair the damage however caused, the doctor can let people make mistakes through ignorance and this will keep the doctor busy and prosperous. Do we not argue that in an ideal world there need be no police? By the same reasoning, doctors should not be needed if people live properly.Has science got us to the stage where all illness is a mistake? Humans live and work in communities with many specialising thanks to their education. Theoretically we can prevent all illness and injury by education, control and prevention. For example, from the earliest age, teach and practice the benefits of exercise. Avoid the dangers of extremes. Control individuals by implanted chips so that everyone is answerable to an artificial intelligence central computer thereby eliminating the benefits of crime and war (and I would resist this being done to me and demand that it be done to others, such is hypocrisy and was well foretold in Brave New World by Aldous Huxley and 1984 by George Orwell). Ensure that the makers of pharmaceuticals and machines serve the majority in the world and not just the rich. Ebola can be controlled. Cancer is avoidable.Guidance on these policies can only be given by those who understand the body and mind and they are doctors. Now is the time for doctors to work towards making themselves redundant. I am sure that will never happen but it ought to be an objective. The police do little to prevent crime. They advise people to lock their doors but does nothing to change the motivation of potential burglars other than apply threats of punishment. Similarly, doctors prescribe drugs on top of drugs without getting to the source of a patient’s problem. People respond to carrot, not stick. The evidence is clear. Most people can be maintained in good health by simply changing their lifestyle so that they exercise as much as their bodies have evolved to do. You are a doctor so tell your patient the blunt truth and when you say to them you don’t want to see them again, you mean it in the friendliest way.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Gerontology & Geriatric Medicine please click on: https://juniperpublishers.com/oajggm/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/oajggm/OAJGGM.MS.ID.555622.php
#Juniper Publishers#Open Access Journals#Juniper Publishers LLC#Juniper Publishers Publishing Group#Juniper Publishers Review
49 notes
·
View notes
Text
Toward Further Professional Development of Nursing in ASEAN -Juniper Publishers

Opinion
The Association of Southeast Asian Nations (ASEAN) Mutual Recognition Arrangements (MRA) on Nursing Services was signed in 2006 with the aim of facilitating the mobility of nursing professionals, the exchange of information and expertise on standards and qualifications, the promotion of adaption of best practices on professional services, and the provision of opportunities for capacity building and training of nurses within ASEAN [1]. To implement the MRA on nursing, the ASEAN Joint Coordinating Committee on Nursing (AJCCN) was established in 2007.
In 2015, the delegations from each ASEAN member country reported numerous achievements at the AJCCN Meeting [2]. For instance, Cambodia, Lao PDR, and Vietnam have greatly enhanced their regulatory frameworks for nursing and developed laws and regulations regarding nursing professionals over the last decade. Commendable achievements represents not only the enforcement of legal documents but also upgrading of nursing education programs [3]. For example, Lao PDR established a 3-year Higher Diploma of Nursing program in 2009 and a 4-yearBachelorof Nursing Science program in 2011. All ASEAN member countries have now implemented bachelor-level nursing education programs. On the other hand, the difficulty in determining good educational qualifications has been pointed out, because several kinds of nursing education programs are running within ASEAN member countries [4].
The ASEAN MRA on Nursing Services has enhanced the nursing profession at the ASEAN regional level as well as at the national level, but some challenges remain. The first such challenge is the institutional capacity in establishing a functional license and registration system. Cambodia, Lao PDR, and Vietnam still need to develop further legal documents to implement licensing and registration systems within their respective regulatory frameworks. The institutional capacity of regulatory bodies, either as professional councils or ministries of health, need to be further strengthened to implement sound regulatory systems in national contexts. Second, further investment in faculty development is needed to ensure the quality of education. The academic level of nurses has been rapidly elevated in Cambodia, Lao PDR, and Vietnam, but the number of nursing educators who hold bachelor's degrees is limited, and no master's and/or PhD courses are available in those countries [5]. Faculty development needs more attention to enlarge the critical mass of nursing educators who hold higher degrees in nursing. Third, cultural competency in addition to language skill for professional nurses working away from their home country should be considered. The sensibility of cultural competency for nurses is distinguished from that of other professionals in the MRA, because the nursing profession prioritizes human quality of life, not only medical paradigms. However, the present nursing curricula, even though upgraded, do not fully reflect this aspect. Fourth, continuing development of professional nursing education programs is needed. Short nursing education programs such as technical nursing programs might not be abolished at once from the perspective of ensuring equitable service delivery at the national level by the nursing workforce in member countries. Nurses who graduate from various nursing education programs are employed nationwide and need appropriate career paths for professional development.
For more articles in Journal of Nursing & Health Care please click on https://juniperpublishers.com/jojnhc/index.php
For more Journals in Juniper Publishers please click on https://juniperpublishers.com/journals.php
#Juniper Publishers#Open Access Journals#Journal of Nursing & Health Care#Juniper publishers Publishing group#Intensive Care
0 notes
Text
Liposome-Actuated Enzyme Systems: A Benchmark for Controlling Biomineralization | Juniper Publishers

Juniper Publishers-Open Access Journal of Material Science
Authored by Martín G Bellino
Abstract
Key to the realization of versatile nano structures are simple, efficient methods of synthesizing materials that mimic aspects of Biomineralization. Liposome-permeability that controls enzymatic reactions may provide blueprints for bio mineral design.
Keywords:Biomineralization; Enzymes; Liposomes; Enzymatic control; Membrane permeability
Opinion
Although it is difficult to overstate the importance of enzymes in biology, these famous macromolecules are also becoming more prominent in nano biotechnology. The appeal of enzymes to nano scientists is three-fold: first, it is a natural nano scale material; second, its capability to furnish high specificity and efficient chemical conversion (which is its main role in biology); and third, this ability to catalyst a large number of chemical reactions can be exploited in industrial processes, waste treatments, pharmaceutical products, and biosensors. Lipid vesicles (liposomes) are best known as the vehicles for administration of nutrients and pharmaceutical drugs, but they are also a versatile tool for nano technological purposes, because liposomes can be designed such that the lipid membranes become into well-defined nanostructures. By exploiting these exquisite nano species, liposome-based nano compartments that sequester active enzymes can be built simply by synthesizing the liposomes in presence of enzymes [1]. Current biomedical applications include, for example, the entrapment of lysozymes into liposomes in order to develop novel therapies in storage diseases [2]. In another approach, enzyme-containing vesicles have been investigated as possible micro reactor system for the decontamination of industrial wastes [1].One challenge in fields ranging from nanotechnology to biomaterial science is the design of versatile methodologies to attain the control of enzymatic activity. Although liposomes have been used to encapsulate a wide variety of enzymes the emergent properties of systems in which enzymatic activity is controlled by surrounding liposomes have not been fully explored. Our group recently pioneered the use of designed liposomes as a robust scaffold to produce enzymatic control that does not occurs in a free enzyme system [3]. The lipid membranes of the liposomes entrapping enzymes reported by Municoy et al. are not merely static barriers between the interior and exterior environments; they are dynamic skins [3]. Properties of vesicles at the interface level, such as membrane permeability, tuned through a thermal input, allow a controlled transportation of substrates across the barrier, thereby modulating enzymatic activity externally. We used this nano-assembly to switch the reactivity of ureases through the change of the liposome permeability by means of temperature control. This synergic interplay between enzymes and liposomes that mimicking crucial aspects of cellular biochemistry such as confinement and enzymatic regulation, allows emerging bio systems capable of actively reconstructs its surface from a sacrificial mesoporous silica film to create a fully 3D silica shell on liposomes, through a self-catalyzed precipitation process. In this sense, bio mineralization is an inspiration for materials chemistry. Bio minerals are usually synthesized in aqueous media under ambient conditions, and these approaches can lead to materials with a reduced ecological footprint. Earlier attempts to create bio mineralized materials have mainly focused on homogeneous precipitation from salt solutions that are being alkalinized by the decomposition of urea catalyzed by free ureases [4]. These studies aimed to create nano/micro particle precipitates that can have important applications, such as fuel cells. In contrast, the controlled precipitation described by Municoy et al. is not primarily based in intrinsic enzymatic catalysis. Rather, theincentive for this work comes from the desire to create shellcontrolled enzymatic entities. Such entities are ubiquitous in nature, for example in micro compartment that sequesters ethanolamine metabolism in the bacterium Escherichia coli [5], where conformational flexibility encoded within shells allows selective transportation of components across the barrier. The liposome-controlled enzymatic reconstruction of a 3D interface composed of silica shells on liposomes in the system of Municoy et al. has a similarity to these functional structures within the cell. Municoy et al. showed that subtle changes in temperature have a pronounced impact on the silica precipitation, which in turn determines the morphology of their nanostructures. At high temperature, only some large shapeless particles were observed. In contrast, precipitation at lower temperature affords spherical morphologies which reflect the size and shape of the liposomes because the silica solidifies around them. Temperature was the mechanism for controlling enzymatic activity through membrane permeability and was crucial in the formation of nano structured silica. Some of the most exciting developments in material science concern the design of bio inspired synthesis methods mimicking the remarkable in vivo control of the precipitates morphology, as these features exceed the capabilities of present day in vitro materials engineering. The interplay of control of enzymatic activity and liposome membrane permeability could lead to simple routes to develop intricate bio mineralized structures such as diatoms [6]. It will be interesting to learn more about the role of these parameters in directing bio mineralization. Municoy et al. report a first step in this promising direction. It will also be exciting to explore this bio inspired approach for lantanidebased material synthesis, which would launch the production of a diversity of new functional hybrid nanostructures for advanced applications.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Material Science please click on: https://juniperpublishers.com/jojms/index.php
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/jojms/JOJMS.MS.ID.555556.php
#Juniper Publishers#Open Access Journals#Juniper Publishers Publishing Group#Juniper Publishers LLC#Juniper Publishers Review
34 notes
·
View notes
Text
Toward Further Professional Development of Nursing in ASEAN -Juniper Publishers

Opinion
The Association of Southeast Asian Nations (ASEAN) Mutual Recognition Arrangements (MRA) on Nursing Services was signed in 2006 with the aim of facilitating the mobility of nursing professionals, the exchange of information and expertise on standards and qualifications, the promotion of adaption of best practices on professional services, and the provision of opportunities for capacity building and training of nurses within ASEAN [1]. To implement the MRA on nursing, the ASEAN Joint Coordinating Committee on Nursing (AJCCN) was established in 2007.
In 2015, the delegations from each ASEAN member country reported numerous achievements at the AJCCN Meeting [2]. For instance, Cambodia, Lao PDR, and Vietnam have greatly enhanced their regulatory frameworks for nursing and developed laws and regulations regarding nursing professionals over the last decade. Commendable achievements represents not only the enforcement of legal documents but also upgrading of nursing education programs [3]. For example, Lao PDR established a 3-year Higher Diploma of Nursing program in 2009 and a 4-yearBachelorof Nursing Science program in 2011. All ASEAN member countries have now implemented bachelor-level nursing education programs. On the other hand, the difficulty in determining good educational qualifications has been pointed out, because several kinds of nursing education programs are running within ASEAN member countries [4].
The ASEAN MRA on Nursing Services has enhanced the nursing profession at the ASEAN regional level as well as at the national level, but some challenges remain. The first such challenge is the institutional capacity in establishing a functional license and registration system. Cambodia, Lao PDR, and Vietnam still need to develop further legal documents to implement licensing and registration systems within their respective regulatory frameworks. The institutional capacity of regulatory bodies, either as professional councils or ministries of health, need to be further strengthened to implement sound regulatory systems in national contexts. Second, further investment in faculty development is needed to ensure the quality of education. The academic level of nurses has been rapidly elevated in Cambodia, Lao PDR, and Vietnam, but the number of nursing educators who hold bachelor's degrees is limited, and no master's and/or PhD courses are available in those countries [5]. Faculty development needs more attention to enlarge the critical mass of nursing educators who hold higher degrees in nursing. Third, cultural competency in addition to language skill for professional nurses working away from their home country should be considered. The sensibility of cultural competency for nurses is distinguished from that of other professionals in the MRA, because the nursing profession prioritizes human quality of life, not only medical paradigms. However, the present nursing curricula, even though upgraded, do not fully reflect this aspect. Fourth, continuing development of professional nursing education programs is needed. Short nursing education programs such as technical nursing programs might not be abolished at once from the perspective of ensuring equitable service delivery at the national level by the nursing workforce in member countries. Nurses who graduate from various nursing education programs are employed nationwide and need appropriate career paths for professional development.
For more articles in Journal of Nursing & Health Care please click on https://juniperpublishers.com/jojnhc/index.php
For more Journals in Juniper Publishers please click on https://juniperpublishers.com/journals.php
0 notes
Text
Global Thalassemia Research: A Scientometric Assessment of Publications Output during 2008-17 | Juniper Publishers
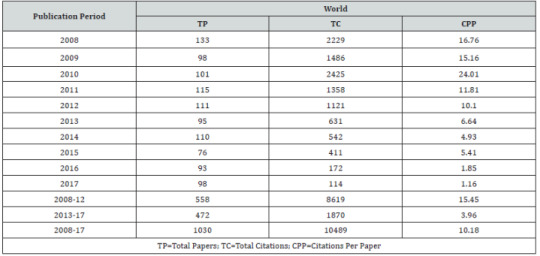
Juniper Publishers-Open Access Journal of Blood Research & Transfusion
Authored by Ritu Gupta
Abstract
The present study examined 1030 global publications on thalassemia research during 2008-17, as indexed in Scopus database, with a view to understand their growth rate, global share, citation impact, international collaborative papers share, distribution of publications by broad subjects, productivity and citation profile of top organizations and authors, preferred media of communication and bibliographic characteristics of high cited papers. The annual and cumulative global publication output on thalassemia research decreased from 133 to 98 and 558 to 472, witnessing -1.63% during 2008-17 and -15.41% growth from 2008-12 to 2013-17. The citation impact per paper of global publications in thalassemia research was averaged to 10.18 during 2008-17, however, decreasing from 15.45 CPP during 2008-12 to 3.96 CPP during 2013-17. Among 75 participating countries, the top 10 countries global publication share ranged from 3.50% to 17.86% during 2008-17, with highest publication share (17.86%) coming from U.K., followed by Italy (14.47%), USA (9.61%), India (8.93%), etc. during 2008-17. 81.65% of the cumulative global publication share comes from top 10 countries during 2008-17, showing increase from 80.11% to 83.47% from 2008-12 to 2013-17. Three out of 10 countries have scored relative citation index more than the average of 1.34: USA (2.62), Italy (1.75) and U.K. (1.71) during 2008-17. Medicine, among four broad subjects, contributed the largest publications share of 86.89%, followed by biochemistry, genetics & molecular biology (17.86%), pharmacology, toxicology & pharmaceutics (2.82%) and immunology & microbiology (2.04%) during 2008-17. Beta Thalassemia accounted for the highest global share (57.38% share), followed by Alpha Thalassemia (19.13% share), Haemoglobin E Thalassemia (5.92% share), etc. during 2008-17. Among 396 organizations and 594 authors contributing to global thalassemia research, the 10 most productive global organizations and authors together contributed 27.28% and 15.05% respectively as their share of global publication output and 56.46% and 24.77% respectively as their share of global citation output during 2008-17. Amongst 996 journal papers (in 369 journals) in global thalassemia research, the top 15 most productive journals contributed 34.74% share of total journal publication output during 2008-17. Only eight publications were found to be high cited, as they registered citations from 118 to 694 during 2008-17 and they together received 1949 citations, which averaged to 243.625 citations per paper.
Keywords: Thalassemia research; Global publications; Scientometrics; BIbliometrics
Introduction
Thalassemias (also known as Mediterranean anemia) are described a group of inherited or genetic blood disorders. Thalassemia causes the body to make fewer healthy red blood cells and less hemoglobin than normal. Hemoglobin is an iron-rich protein in red blood cells. In thalassemia cases, where insufficient haemoglobin is present in the blood, oxygen does not reach all the parts of body properly. It causes starvation of oxygen in various organs and thereby increasing their inability to function properly. Thalassemia is inherited that means at least one parent is a carrier of the disease; it’s either genetic mutation or deletion of main gene fragments. If only one parent is a carrier, patient develops thalassemia minor, wherein there are no symptoms or may develop minor symptoms like minor anemia. In cases where both parents are carriers of the trait, the patient develops serious form the disease called thalassemia major (almost 25 per cent of the cases) [1-3].People who have thalassemia can have mild or severe anemia (uh-NEE-me-uh). Anemia is caused by a lower than normal number of red blood cells or not enough hemoglobin in the red blood cells. Anemia can result in feeling tired and pale skin. There may also be bone problems, an enlarged spleen, yellowish skin, dark urine, and among children slow growth [1-3].Haemoglobin is made up of two types of proteins, Alpha globin and Beta globin. In thalassemia, a defect occurs in a gene that controls production of one of these proteins. The main forms of thalassemia are:(i) Alpha-thalassemia: It is a major serious disease in which no alpha globins are formed and thereby anemia begins even before the birth of the baby. Pregnant mother carrying the baby is herself at serious risk of pregnancy and delivery complications. This form is generally incompatible with life;(ii) Beta-thalassemia: Thalassemia major (Cooley ’s anemia) causes severe life-threatening anemia. Other symptoms include paleness, poor appetite, frequent infections, enlargement of organs and jaundice. This is a serious form that requires regular Blood Transfusions. Thalassemia intermedia is a less severe form in which blood transfusions are not required;(iii) Delta-thalassemia: Just like beta-thalassemia, in this mutation affect ability of the gene to produce delta chains and(iv) Combined haemoglobinopathies: Thalassemia can exist in combination with other haemoglobinopathies;(a) Haemoglobin E/thalassemia is clinically similar to Beta-thalassemia major or thalassemia intermedia. It is common in Thailand, parts of India and Cambodia;(b) Haemoglobin S/thalassemia is clinically similar to sickle-cell disease with feature of spleen enlargement too. It is common in African and Mediterranean countries;© Haemoglobin C/thalassemia causes moderately severe anemia with spleen enlargement and is common in African and Mediterranean countries and(d) Haemoglobin D/thalassemia is common in northwest parts of India and Pakistan [1, 4].Treatment depends on the type and severity. Treatment for those with more severe disease often includes regular blood transfusions, iron chelation, and folic acid. Iron chelation may be done with deferoxamine or deferasirox. Occasionally, a bone marrow transplant may be an option. Complications may include iron overload from the transfusions with resulting heart or liver disease, infections and osteoporosis. If the spleen becomes overly enlarged, surgical removal may be required [1].As of 2013, thalassemia occurs in about 280 million people, with about 439,000 having severe disease. It is most common among people of Italian, Greek, Middle Eastern, South Asian and African descent. Males and females have similar rates of disease. It resulted in 16,800 deaths in 2015, down from 36,000 deaths in 1990. Those who have minor degrees of thalassemia, similar to those with sickle-cell trait, have some protection against malaria, explaining why they are more common in regions of the world where malaria exists [1].Literature reviewThere is no specific bibliometric study on Thalassemia research output so far. However, there are few bibliometric studies focusing on overall blood diseases. Among such studies, Daneshmand, Forouzandeh, Azadi and Cheraghzadeh Dezfuli [5] examined quantitative and qualitative evaluation of hematological research output in five Islamic countries; Iran, Turkey, Malaysia, Saudi Arabia and Egypt; which have the most scientific productions from 1996-2013. Gupta [6] analyzed the heredity blood disorders research output, using Scopus database during 2002-11 on different parameters including the global publications share and citation quality of top 10 leading countries, India’s growth, citation impact, share of international collaborative papers, contribution of major collaborative partner countries, contribution of various subject fields and by type of heredity blood disorder, pattern of research communication in most productive journals, productivity and citation profile of top Indian institutions and authors and characteristics of high cited papers.
Objectives
Based on publications covered and indexed in Scopus database, the present study analysed the global Thalassemia research during 2008-17. In particular, the study analyses the growth rate in global publications; global publication output and citation impact of world and top 10 most productive countries; its broad publication distribution by broad subject areas; its leading organizations and authors, in terms of publication output and citation impact; its leading media of communication, particularly the most productive journals and bibliographical characteristics of its 8 highly cited papers.
Methodology
Few quantitative and qualitative bibiometric indicators have been used in this study to measure the performance of global Thalassemia research output. The basic publication data for the present study was retrieved and downloaded from the Scopus database for 10 years during 2008-17. For retrieving publication data from the Scopus database, the authors have used the Keyword such as “THALASSAEMIA “ in “Keyword” tag or ‘’Article Title’’ tag and further restricting the search to the period 2008- 17 in “date range tag” for searching the global publication data on Thalassemia and this becomes the main search string. When the main search string with restricted to individual top 10 most productive countries name in “country tag”, the publication data on the individual country in Thalassemia research were obtained. The search string is further refined, as provided in Scopus database, by restricting to “subject area tag”, “country tag”, “source title tag”, “journal title name” and “affiliation tag”, to get information on the distribution of publications by subject, collaborating countries, author-wise, organization-wise and journal-wise, etc. For citation data, citations to publications were also collected from the date of publication till 4 July 2018.(KEY(THALASSAEMIA) OR TITLE(THALASSAEMIA)) AND PUBYEAR > 2007 AND PUBYEAR < 2018Go toAnalysisThe world has published 1030 publications on thalassemia research in 10 years during 2008-17, which decreased from 133 publications in 2008 to 98 publications in 2017, registering annual average growth rates of -1.63%. The cumulative growth of world publications on thalassemia research decreased from 558 during 2008-12 to 472 publications during 2013-17, witnessing a growth rate of -15.41%. The average citation per publication (CPP) registered by global publications on thalassemia research was 10.18 during 2008-17, which decreased from 15.45 CPP during 2008-12 to 3.96 CPP during 2013-17. Of the total global publications, 73.40% (756) have appeared as articles, 10.97% (113) as reviews, 6.99% (72) as letters, 2.43% (25) as book chapters, 1.75% (18) as conference papers, 1.65% (17) as notes, 1.26% (13) as editorials, 0.58% (6) as short surveys, 0.49% (5) as erratum, 0.39% (4) as articles in press and 0.10% (1) as book (Table 1).
Global publication share & citation impact of top 10 most productive countries
The global thalassemia research output originated in 75 countries during 2008-17, of which 43 countries contributed 1-5 papers each, 5 countries 6-10 papers each, 20 countries 11- 50 papers each, 5 countries 51-100 papers each and 2 countries 101-83 papers each during 2008-17. Table 2 lists the output of top 10 most productive countries in thalassemia research during 2008-17. The cumulative publication and citation share of 10 most productive countries in thalassemia research was 81.65% and more than 100% of the world publication and citations output during 2008-17. Individually, the global publication share of these 10 countries varied from 3.50% to 17.86% during 2008- 17, with highest publication share (17.86%) coming from U.K., followed by Italy (14.47%), USA (9.61%), India (8.93%), Greece (6.60%), Malaysia and Thailand (5.73% and 5.44%), Pakistan, and Australia (4.85% and 4.66%) ,and Iran (3.50%) during 2008- 17.The global publication share showed increase in Greece, U.K., Italy, Iran and USA (from 0.08% to 1.09%), as against decrease in Malaysia, India, Thailand, Australia and Pakistan (from 0.02% to 1.48) from 2008-11 to 2012-17. U.K., Italy and USA together accounts for 41.94% and 80.94% share of global publications and citations output, while 7 other countries together have global publication and citation share from 39.71% to 28.64% during 2008-17. Among top 10 countries, USA registered the highest citation impact per paper of 26.66, followed by Italy (17.79), U.K. (17.40), Greece (12.0), Thailand (8.96), Australia (9.63), Iran (8.75), Malaysia (5.73), India (5.50) and Pakistan (3.14) during 2008-17. Three out of 10 countries have scored relative citation index more than the average of 1.34: USA (2.62), Italy (1.75) and U.K. (1.71) during 2008-17.
Subject-wise distribution of research output
As per the Scopus database classification, the global thalassemia research output is distributed across four sub-fields during 2008-17. Among 4 sub-fields, medicine registered the highest publications share (86.89%), followed by biochemistry, genetics & molecular biology (17.86%), pharmacology, toxicology & pharmaceutics (2.82%) and immunology & microbiology (2.04%) during 2008-17. The publication activity, as seen through activity index from 2008- 12 to 2013-17, witnessed decrease in medicine (from 104.36 to 95.66), as against increase in biochemistry, genetics & molecular biology (from 94.30 to 107.65), pharmacology, toxicology & pharmaceutics (from 63.65 to 144.19) and immunology & microbiology (from 52.74 to 157.20) from 2008-12 to 2013- 17. Biochemistry, genetics & molecular biology registered the highest citation per paper of 9.83 among four subjects, followed by medicine (9.75), biochemistry, genetics & molecular biology (9.38), pharmacology, toxicology & pharmaceutics (9.38) and immunology & microbiology (6.43) during 2008-17 (Table 3).
Type of thalassemia research
Of the type of thalassemia global research output, Beta Thalassemia accounted for the highest publication output and global share (591 papers, 57.38% share), followed by Alpha Thalassemia (197 papers, 19.13% share), Haemoglobin E Thalassemia (61 publications, 5.92% share), etc. during 2008- 17 as seen in Table 4. The global publication share increased in case of Alpha Thalassemia and Delta Thalassemia, as against decrease in case of Beta Thalassemia, Haemoglobin E Thalassemia, Haemoglobin S Thalassemia, Haemoglobin C Thalassemia and Haemoglobin D Thalassemia from 2008-12 to 2013-17. Haemoglobin D Thalassemia registered the highest citation impact per paper of 25.41, followed by Haemoglobin C Thalassemia (16.69), Haemoglobin E Thalassemia (15.54), Haemoglobin S Thalassemia (13.96), Alpha Thalassemia (12.79), Delta Thalassemia (11.62) and Beta Thalassemia (11.24) during 2008-17.
Profile of top 10 most productive organizations
396 organizations participated in global thalassemia research, of which 306 organizations contributed 1-5 papers each, 44 organizations 6-10 papers each, 37 organizations 11-20 papers each, 7 organizations 21-30 papers each and 2 organizations 31-45 papers each. The productivity of 10 most productive organizations in global thalassemia research varied from 19 to 45 publications and together contributed 27.28% (281 publications) publication share and 56.46% (5922) citation share to its cumulative publications output during 2008-17. The scientometric profile of these 10 organizations is presented in Table 5.a) Four organizations have registered higher publications output than the group average of 28.10: University College London, U.K. (45 papers), Mahidol University, Thailand (34 papers), University of Oxford, U.K. (30 papers) and Universita degli Studi di Milano, Italy (29 papers) during 2008-17;b) Six organizations have registered more than the average citation per publication (21.07) Weatherall Institute of Molecular Medicine, U.K. (31.57), Universita degli Studi di Milano, Italy (28.31), IRCCS Foundation, Rome, Italy (26.13), University College London, U.K. (22.42), Ospedale Maggiore Policlinico Milano, Italy (22.32) and American University Beirut Medical Centre, Lebanon (21.68) during 2008-17;c) Six organizations have achieved more than the average share of international collaborative publications (50.89%): American University Beirut Medical Centre, Lebanon (63.64%), University College London, U.K. (62.22%), Universita degli Studi di Milano, Italy (58.62%), Weatherall Institute of Molecular Medicine, U.K. (57.14%), University of Oxford, U.K. (56.67%) and IRCCS Foundation, Rome, Italy (56.52%) during 2008-17;d) Six organizations have registered the relative citation index more than average (2.07): Weatherall Institute of Molecular Medicine, U.K. (3.10), Universita degli Studi di Milano, Italy (2.78), IRCCS Foundation, Rome, Italy (2.57), University College London, U.K. (2.20), Ospedale Maggiore Policlinico Milano, Italy (2.19) and American University Beirut Medical Centre, Lebanon (2.13) during 2008-17.
Profile of top 10 most productive authors
594 authors participated in global thalassemia research, of which 518 authors contributed 1-5 papers each, 59 authors 6-10 papers each, 16 authors 11-20 papers each and 1 author 27 papers. The productivity of 15 most productive authors in global thalassemia research varied from 12 to 27 publications and together contributed 15.05% (155 publications) publication share and 24.77% (2598) citation share to its cumulative publications output during 2008-17. The scientometric profile of these 10 authors is presented in Table 6.a) Four authors have registered higher publications output than the group average of 15.5: C. M.D. Coppellini (27 papers), V. De Sanctis (17 papers), E. George and A.T. Taher (16 papers each) during 2008-17;b) Five authors have registered more than the average citation per publication (16.76) of all authors: M.D. Coppellini (27.07), R. Galanello (24.79), S. Daar (22.25), A.T. Taher (18.75) and A.Maggio (17.58) during 2008-17;c) Six authors have achieved more than the average share of international collaborative publications (45.16%) of all authors: T S. Daar (75.0%), A.T. Taher (62.50%), M.D. Coppellini (55.56%), S. Fucharoen and R. Galanello (50.0% each) and S.L. Thein (46.15%) during 2008-17;d) Five authors registered the relative citation index more than average (1.65) of all authors: M.D. Coppellini (2.66), R. Galanello (2.43), S. Daar (2.19), A.T. Taher (1.84) and A. Maggio (1.73) during 2008-17.
Medium of communication
996 journal papers were published in 369 journals in global thalassemia research, of which 337 journals contributed 1-5 papers each, 20 journals 6-10 papers each, 8 journals 11-20 papers each, 2 journals 21-30 papers each, and 33-123 papers each. The 15 most productive journals in global thalassemia research contributed from 8 to 123 papers and together contributed 34.74% share (346 papers) to the total journal publication output during 2008-17. The publication share of these top 15 most productive journals increased from 34.33% to 35.22% from 2008-12 to 2013-17. The most productive journal (with 123 papers) was British Journal of Haematology, followed by European Journal of Haematology (33 papers), Blood Transfusion (23 papers), Cochrane Database of Systematic Reviews (23 papers), Journal of Clinical & Diagnostic Research (19 papers), International Journal of Laboratory Haematology (18 papers),
Highly cited papers
There were 8 highly cited papers, which have received citations from 118 to 694 during 2008-17. These 8 highly cited papers together received 1949 citations, leading to average citation per paper of 243.625.a) Of the 8 highly cited papers, all involved the participation of two or more organizations (of which 3 national collaborative and 5 international collaborative).b) Among high cited papers, the largest participation, was with from U.K. (6 papers), followed by USA (3 papers), Italy (2 papers), Canada, Germany, Greece, Lebanon and Netherlands (1 paper each).c) Among 8 highly cited papers, 4 appeared as articles, 3 as reviews and 1 as conference paper.d) The 8 highly cited papers involved the participation of 99 authors and 60 organizations.e) These 8 highly cited papers were published in 6 journals, of which 3 papers in British Journal of Haematology and 1 paper each in European Journal of Haematology, Journal of Cardiovascular Magnetic Resonance, The Lancet, Nature and Orphanet Journal of Rare Diseases.
Summary
1030 global publications on thalassemia research, as indexed in Scopus database, were published during 2008-17 and they decreased from 133 to 98 in the year 2008 to the year 2017, registering -1.63% growths per annum. Their cumulative global publication output on thalassemia research decreased from 558 to 472, witnessing -15.41% growth from 2008-12 to 2013-17. The citation impact per paper of global publications in thalassemia research was averaged to 10.18 during 2008-17, however, decreasing from 15.45 CPP during 2008-12 to 3.96 CPP during 2013-17.The global publication share of the top 10 most productive countries among 75 participating countries in thalassemia research varied from 3.50% to 17.86% during 2008-17, with highest publication share (17.86%) coming from U.K., followed by Italy (14.47%), USA (9.61%), India (8.93%), Greece (6.60%), Malaysia and Thailand (5.73% and 5.44%), Pakistan, and Australia (4.85% and 4.66%) ,and Iran (3.50%) during 2008- 17. Together these top 10 countries contributed 81.65% global share and more than 100% of the world publication and citations output during 2008-17. The global publication share, however increased from 80.11% to 83.47% from 2008-12 to 2013-17. The global publication share showed increase in Greece, U.K., Italy, Iran and USA (from 0.08% to 1.09%), as against decrease in Malaysia, India, Thailand, Australia and Pakistan (from 0.02% to 1.48) from 2008-11 to 2012-17. Three out of 10 countries have scored relative citation index more than the average of 1.34: USA (2.62), Italy (1.75) and U.K. (1.71) during 2008-17.Medicine, contributed the largest publications share of 86.89% in thalassemia research, followed by biochemistry, genetics & molecular biology (17.86%), pharmacology, toxicology & pharmaceutics (2.82%) and immunology & microbiology (2.04 during 2008-17. As per the Scopus database classification, the global thalassemia research output is distributed across four subfields during 2008-17. The publication activity showed decrease in medicine, as against increase in biochemistry, genetics & molecular biology, pharmacology, toxicology & pharmaceutics and immunology & microbiology from 2008-12 to 2013-17. Among seven subjects, biochemistry, genetics & molecular biology registered the highest citation per paper of 9.83 among four subjects, followed by medicine (9.75), biochemistry, genetics & molecular biology (9.38), pharmacology, toxicology & pharmaceutics (9.38) and immunology & microbiology (6.43) during 2008-17 .Beta Thalassemia, among different types of thalassemia research, accounted for the highest global share (57.38% share), followed by Alpha Thalassemia (19.13% share), Haemoglobin E Thalassaemia ssaemia ( 5.92% share), etc. during 2008-17. The global publication share increased in case of Alpha Thalassemia and Delta Thalassemia, as against decrease in case of Beta Thalassemia, Haemoglobin E Thalassemia, Haemoglobin S Thalassemia, Haemoglobin C Thalassemia and Haemoglobin D Thalassemia from 2008-12 to 2013-17.Among 396 organizations and 594 authors contributing to global thalassemia research, the 10 most productive global organizations and authors together contributed 27.28% and 15.05% respectively as their share of global publication output and 56.46% and 24.77% respectively as their share of global citation output during 2008-17. The leading organizations in research productivity were: University College London, U.K. (45 papers), Mahidol University, Thailand (34 papers), University of Oxford, U.K. (30 papers) and Universita degli Studi di Milano, Italy (29 papers) during 2008-17. The leading organizations in terms of relative citation index were: Weatherall Institute of Molecular Medicine, U.K. (31.57), Universita degli Studi di Milano, Italy (28.31), IRCCS Foundation, Rome, Italy (26.13), University College London, U.K. (22.42), Ospedale Maggiore Policlinico Milano, Italy (22.32) and American University Beirut Medical Centre, Lebanon (21.68) during 2008-17.British Journal of Haematology was the most productive journal (with 123 papers) in global thalassemia research, followed by European Journal of Haematology (33 papers), Blood Transfusion (23 papers), Cochrane Database of Systematic Reviews (23 papers), Journal of Clinical & Diagnostic Research (19 papers), International Journal of Laboratory Haematology (18 papers), etc. during 2008-17. Among the 996 journal papers (in 369 journals) in global thalassemia research, the top 15 most productive journals contributed 34.74% share of total journal publication output during 2008-17, which increased from 34.33% to 35.22% from 2008-12 to 2013-17.There were 8 highly cited papers, which have received citations from 118 to 694 during 2008-17 and together have received 1949 citations, with an average citation per paper of 243.625. These 8 highly cited papers resulted from participation of 99 authors and 60 organizations and were published in 6 journals, of which 3 papers in British Journal of Haematology and 1 paper each in European Journal of Haematology, Journal of Cardiovascular Magnetic Resonance, The Lancet, Nature and Orphanet Journal of Rare Diseases.Conclude that there is an urgent need to review the current status of epidemiology, management and control of Thalassemia disorders globally. In this context, there is a need to identify the local and regional problems, needs and priorities for improving control policies; to prepare guidelines for the control of Thalassemia disorders; fundraising to support programs for control of Thalassemia disorders and develop cost-effective approaches and interventions for the control of Thalassemia disorders.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Blood Research & Transfusion please click on: https://juniperpublishers.com/oabtj/classification.php
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/oabtj/OABTJ.MS.ID.555594.php
#Juniper Publishers#Juniper Publishers Review#Open Access journals#Juniper Publishers Publishing Group#Juniper Publishers LLC
28 notes
·
View notes
Text
Immunological Approach of Personalized Treatment for Recurrent Implantation Failure Patients Undergoing IVF | Juniper Publishers
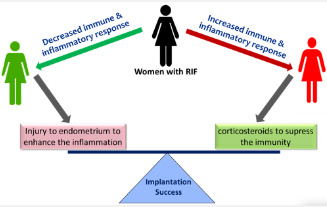
Juniper Publishers-Open Access Journal of Reproductive Medicine
Authored by Indira Hinduja
Abstract
Genes related to immune and inflammatory response initiate the process of endometrial receptivity. It stimulates the cascade of biological functions like cell differentiation, vasculogenesis, and expression of cell adhesion markers at the endometrium to which the invading embryo attaches. Dysregulation in immunological response results in impairment in endometrial receptivity leading to implantation failure. In our study, we have evaluated the expression of genes involved in immune and inflammatory response in recurrent implantation failure patients and designed the personalized immunological treatment and cycle in which the embryo transfer to be recommended, based on the gene expression results. We achieved success in two out of four cases having normal expression and down-regulation of immune response respectively, in natural cycle. However, the approach is required to be implemented in larger cohort of implantation failure patients to confirm its efficiency.
Keywords: Endometrial receptivity; Implantation failure; Immune and inflammatory response; Genes; Cell differentiation; Vasculogenesis; Endometrium; Immunological treatment; Embryo transfer; Natural cycle; Window of implantation; Blastocyst; Monocytes; Natural killer cells; Tumor necrosis factor; Pro-inflammatory cytokines; Interleukin; Leukemia; Chemotaxis; Unexplained infertility; Oocytes; Immunological genes
Abbreviations: WOI: Window Of Implantation; TNFα: Tumor Necrosis Factor; IGF: Insulin-Like Growth Factor; PAEP: Progestogen Associated Endometrial Protein
Introduction
Immunological and inflammatory response plays very crucial role in making the endometrium receptive. In normal fertile women, under the influence of progesterone and estrogen, during the window of implantation (WOI) and before the arrival of blastocyst, immune cells like monocytes and natural killer cells migrate to the endometrium. Additionally, inflammatory factors like tumor necrosis factor (TNFα) and interferon-γ are secreted by the endometrial stromal cells to initiate the inflammatory action. These markers secrete pro-inflammatory cytokines such as interleukin (IL)1, IL6, leukemia inhibitory factor (LIF), leptin, Insulin-like growth factor (IGF)2, IL18 in the endometrial tissue [1]. The chemotaxis of monocytes to the secreted cytokines brings about the differentiation of monocytes into dendritic cells and macrophages in the presence of IL4 and Granulocyte-macrophage colony-stimulating factor GMCSF. Immune cells also get differentiated to specific decidualized cells having peculiar characteristics e.g. NK cells loses its cytotoxic property when gets differentiated to decidualized NK cells. The chemotaxis and migration of these immune cells to the decidualized endometrium stimulates the endometrial cells to secrete various chemokines, growth factors and expression of cell adhesion molecules. Thus, the immunological and adequate inflammatory response has been observed to plays vital role in decidualization, tissue remodeling, angiogenesis, vasculogenesis, and cell adhesion.
Based on the study performed by our group [2], it has been observed that the immunological and inflammatory genes were downregulated in recurrent implantation failure patients undergoing 2 or more IVF cycles with unexplained infertility. The down-regulated expression of these genes was observed in endometrial tissue when patient group as well as healthy fertile oocyte donors (control group) were under the influence of ovarian stimulation. We have shortlisted panel of 70 genes involved in immune and inflammatory response. However, genes such as Progestogen Associated Endometrial Protein (PAEP), CD4, C-X-C Motif Chemokine Ligand 14 (CXCL14), Interleukin 6 Signal Transducer (IL6ST), LIF, Phospholipase A2 Group IIA (PLA2G2A), were validated by real time PCR. The protein expression was also assessed by immunohistochemistry for LIF, IL6ST and PAEP gene, confirming the significant down-regulation [2].
The significant differential expression of these genes in RIF cases Vs oocyte donors highlights the role of immunological processes in endometrial receptivity. Therefore, impairment in immune response and imbalance between pro-inflammatory and anti-inflammatory response could be accountable for defective endometrial receptivity [1–3]. It has been reported that, the hormonal administration in IVF protocol can be detrimental to the endometrial receptivity [4]. Though in our previous study, this hormonal bias was ruled out by considering both the case and control group undergoing same protocol of ovarian stimulation, the protocol of embryo transfer would also affect the receptivity. Thus, the regulation of immune and inflammatory cells in stimulated cycle, hormonal replacement cycle and natural cycle would be different which may cause implantation failure.
Therefore, in each RIF patients, it is essential to evaluate the expression of immune and inflammatory markers in WOI of the same characterized cycle as of embryo transfer. Based on the evaluation of panel of immunological markers, the approach of personalized treatment can be planned for RIF patients. In this approach, the RIF patients had undergone the evaluation of panel of markers involved in immunological response such as PAEP, LIF, IL6ST, CXCL14, PLA2G2A, Indoleamine 2,3-Dioxygenase 1 (IDO1), CD4, CD247. On stimulating the ovaries and retrieval of the oocytes, the embryos of RIF patients were fertilized and cryopreserved until their transfer. In the next natural menstrual cycle, the endometrial biopsy was collected on day LH+6, confirming the ovulation by monitoring the follicular growth by USG and LH surge by ‘ovulation LH kit’. Total RNA was extracted from endometrial tissue using Trizol reagent and were subjected to cDNA preparation using ‘first strand cDNA kit”, Invitrogen as per the manufacturer’s instructions. Real time PCR was performed using 18S housekeeping gene as a normalizer. The CT values of these genes were compared to control groups i.e. healthy fertile women in natural cycle (LH+6th day). The fold change was calculated using 2ΔΔCT method. The down-regulation or upregulation of these markers having fold change >2 was considered abnormal and were subjected to further personalized treatment.
The down regulation indicates the need to elicit the inflammatory response in endometrium by scratching the endometrium or introducing injury to endometrium using Gynetics suction curette. In such cases we could use the mechanistic approach reported by Gnainsky et al. [3], in which induced endometrial injury stimulates the immune markers and their migration to the implantation site, which reside in the functionalis layer of the endometrium and gets activated in next menstrual cycle during WOI under the influence of steroid hormones. On the other hand, the up-regulation of above mentioned immune markers is suggestive over-expression of genes related to immune response and would be recommended the administration of immunosuppressant (Figure 1). In all the down-regulated, up-regulated and normal cases, the embryo transfer is to be performed in natural cycle on day LH+5 by monitoring the follicular growth, without giving any hormonal supplementation for preparation of endometrium.
This approach agrees with the study reported by Roberson et al. [5] suggesting that it is very essential to treat the infertility immunologically by giving corticosteroids, only after the evaluation of immune response in the endometrium. This is because the controlled inflammation and stimulation of immune cells are important factors to achieve receptivity and successful implantation [5]. We have evaluated four such cases, of which one showed down-regulated panel of immune markers who had undergone the ‘injury to endometrium’ in secretory phase. In this patient, the embryos were transferred in its next natural cycle. In other case, the panel of immunological genes were normal when compared to fertile women. In this case, the embryos were transferred in the next natural cycle. Both these patients had conceived having positive urine pregnancy test and the presence of gestational sack. The conception was confirmed by assessment of heart bits of the fetus. Hence, out of four, IVF was successful in two patients on managing them using personalized approach with respect to immunological status of the endometrium to achieve the receptivity. The fold change of both these patients is shown in Table 1.
Conclusion
The implementation of this approach needs to be substantiated in larger population of RIF patients. Thus, the immune response and its proper regulation is observed to play vital role in endometrial receptivity. In IVF, the stated approach of embryo transfers in natural cycle on assessment of immunological regulatory genes would help in improving the success rate of IVF. The endometrial tissue assessment in natural cycle and even the transfer of embryo in natural cycle would help to nullify the hormonal bias of other generalized protocols of ovarian stimulation, replacement therapy and the preparation of endometrium in frozen embryo transfer cycle.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Reproductive Medicine please click on: https://juniperpublishers.com/gjorm/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/gjorm/GJORM.MS.ID.555667.php
39 notes
·
View notes
Text
Strategies to Improve Clinical Nurses' Performances and Competencies in Providing a Good Pain Management to Hospitalized Children in Indonesia -Juniper Publishers

Opinion
In this brief article I would like to point out that effective pain management for pediatric patients remains an elusive goal in Indonesia. Many of Indonesian children endure pain from surgery, illness, nursing interventions and other medical procedures during hospitalization. However, little attention has been given to Indonesian children's pain management and care. Children's pain is often not recognized, is ignored or even denied. The management of pain in children fails to be given appropriate priority and children's pain is not properly managed in a variety of clinical situations in Indonesia. Globally, pain in children is an issue in hospitalized children and a public health concern of major significance in most parts of the world [1,2]. This report describes contemporary thinking about pain in children and its management in order to identify those factors that must be considered in developing some strategies to improve clinical nurses' performances and competencies in providing good pain care to Indonesian pediatric patients.
Several factors have been identified in the literature that may contribute to barriers to providing adequate pain management to children. These barriers can be grouped into four themes: nurses-related barriers, patient-related barriers, physician-related barriers and system-related barriers [3-5]. A current study conducted by Mediani [1] found that Indonesian nurses practicing in today's pediatirc healthcare environment are confronted with increasingly complex moral and ethical dilemmas. Pediatric nurses encounter these dilemmas in situations where their ability to provide a good pain care is frequently hindered by conflicting values and beliefs of other healthcare providers. Mediani [1] identified that the organisational context of the hospitals impacted on nurses' pain assessment and pain management practices. This effect was juxtaposed with their need to provide effective pain care. Within the reality of the practice setting nurses experienced many professional role tensions when managing pain in hospitalized children, which influenced their perceptions of their role as professional nurses. The professional role tensions occurred as a result of the conflict between the nurses' perceptions of the barriers to pain management and their views on how the role of pain management should be carried out.
A significant finding of this evidence was the nurses' suggestions for improving pain management practice in the context of pediatirc settings in Indonesia. Several strategies have been proposed in literature as means of overcoming some barriers indentified in current evidence and are presented in this paper. One an important strategy is the need to empower nurses to provide good pain care.Other strategy is needed to develop a team approach to pain management that would include both nurses and the medical profession. Nurses' professional autonomy, control over nursing practice, and effective inter-professional collaboration are viewed as core elements of nursing practice, and correlate with improved patient outcomes. Another important aspect that identified from the current evidence was nurses' knowledge gaps appear to persist, in particular in relation to pain assessment skills for assessing children's pain, basic knowledge and principles of pharmacological pain management for children, pain medication including the dosage, action and side effects of analgesic drugs and their management. Therefore, it is suggested that the hospital organization should provide nurses with training courses or in-service education about pain management in children, and provide an opportunity for nurses who had graduated from the diploma of nursing program to undertake a Bachelor's degree in nursing. Professional competence is a prerequisite for providing morally responsible care. The elements of a profession, such as formal education based on theoretical knowledge, a code of ethics, professional organizations that guide practice and the provision of necessary service to society, all serve to develop professional competence. Standards for ethical conduct are also necessary in order to provide morally responsible care.
To sum up, the importance of providing effective pain care cannot be over emphasized. Nurses have obligations to patients, one another to assure optimal pain management, personal wellbeing, and quality of life for all paediatirc patients with whom they come in contact. There is a give and take to empowerment, so nursing must be prepared to reshape the health care environment and act as its full partner. Both the culture of the profession and the culture of the workplace must be transformed. Creating an environment that supports both formal and informal continuing educational opportunities and learning will provide for autonomous clinical nursing practice.
For more Journals in Juniper Publishers please click on https://juniperpublishers.com/journals.php
For more articles in Journal of Nursing & Health Care please click on https://juniperpublishers.com/jojnhc/index.php
#Juniper Publishers#Juniper Publishers Publishing Group#Open Access Journals#Juniper Publishers Review#Pediatric Nursing#illness#journal of nursing#open access public health journals
0 notes
Text
Impact of Cialis on Haemoglobin Concentration and Lipid Profile of Wistar Male Rats | Juniper Publishers

Juniper Publishers-Open Access Journal of Pharmacy & Pharmaceutical Sciences
Authored by Nzor Joyce Nornubari
Abstract
Erectile dysfunction (ED) is the consistent or recurrent inability of a man to attain and/or maintain a penile erection enough for sexual activity, currently phosphodiesterase (PDE) inhibitors are used in the treatment of erectile dysfunction. This research work is set out to determine the lipid profile and haemoglobin concentration of wistar male rats administered with cialis, forty-five male albino wistar rats with an average weight of 100 g were used for the study. Cholesterol, high density lipoprotein (HDL), low density lipoprotein (LDL) and triglycerides concentration increased non-significantly at the 7th, 14th and 21st day following treatment, haemoglobin concentration also increased but its increase was significant as compared to the control animals. The elevated lipid profile with corresponding increase in hematocrit is as a result of reverse cholesterol transport mechanism. However due to the observed effect of the drug on lipid profile, utilization of the drug should be monitored as elevated lipid profile could pose as a risk factor for the development of other diseases.
Keywords: Haemoglobin; Male Rats; Lipid; phentolamine; Triglycerides
Introduction
Drugs such as trazadone, phentolamine, yohimbie etc. and diverse therapeutic method such as urethral suppositories and penile prosthetic surgery has been used in the past decades for the management of erectile dysfunction [1]. These therapeutic methods were stopped because of their invasive, dangerous and hostile nature associated with the therapy procedures, likewise the drugs for their ineffectiveness [2]. Erectile dysfunction (ED) as defined by Sinha [3] is “the consistent or recurrent inability of a man to attain and/or maintain a penile erection sufficient for sexual activity”, currently phosphodiesterase (PDE) inhibitors are used in the treatment of erectile dysfunction.Erection working normally involves combined effort of nervous, hormonal and vascular systems. Disorders of the nervous and hormonal systems contribute to erectile dysfunction which is caused primarily by diseases and improper functioning of the vascular system. Erectile dysfunction is grouped based on the cause of erectile dysfunction into organic and psychogenic causes, PDE inhibitors are used in the management of erectile dysfunctioning associated with organic (physical) causes [3]. Erection is achieved primarily through nitric oxide (NO) and other neurotransmitters releases due to sexual stimulation; pathways involving cavernous and pudendal nerves, supraspinal structures including the medial preoptic area and paraventricular nucleus of the hypothalamus [4].Nitric oxide synthase from the cavernous (autonomic) nerves synthesizes nitric oxide which initiates erection and the erection is sustained during sexual stimulation by nitric oxide synthase of the endothelium [5]. Crossing the cell membrane through passive diffusion NO activates guanylyl cyclase (sGC) which acts on guanosine triphosphate (GTP) converting it to cyclic guanosine monophosphate (cGMP), protein kinase G is activated due to amplified amount of cGMP. Protein kinase G phosphorylates ion channels leading to potassium channel opening and closing of calcium channel, the reduction in calcium concentration in the cytosol promotes the relaxation of the muscle [6]. Phosphodiesterase (PDE) inactivates cyclic guanosine monophosphate; PDE-5 inhibitors prevent the catabolism of cyclic GMP [7].Currently, there are four available registered PDE-5 inhibitors they are sildenafl, vardenafl, tadalafl and avanafl, tadalafil trade name cialis is more of the most potent PDE-5 inhibitors, its action is competitive and reversible. Lipid plays important structural and membrane role in the body, irrespective of these beneficial roles accumulation or elevated amount of blood cholesterol, low density lipoprotein (LDL) is detrimental to health, thus it is vital that blood cholesterol level, LDL and other parameters associated with lipids be monitored especially when consuming other medications. Haemoglobin is responsible for the transportof oxygen in erythrocytes and contains iron, its decrease with or without an absolute decrease in red blood cells leads to anaemia. It is in this perceptive that this research work is set out to determine the lipid profile and haemoglobin concentration of wistar rats administered with Cialis.
Material and Methods
Drugs and Chemicals
Cialis manufactured by Lilly pharmaceutical company Indonesia was purchased from a local pharmacy in Choba, Rivers state Nigeria. The chloroform used as anesthetic for the animals was manufactured by Shiv Shakti Trading corporation india, all other reagents used were also of analytical grade and the randox kit used were obtained from Randox chemical Laboratory (Crumlin, UK).
Experimental Animals
Forty-five male albino wistar rats with an average weight of 100 g obtained from animal house in the Department of Biochemistry University of Port Harcourt Nigeria were used for the research, following acclimatization the animals were grouped into five groups each containing nine rats; one group served as the control while the remaining four groups were administered 0.15 mg/100 g body weight, 0.35 mg/100 g body weight, 0.55 mg/100 g body weight and 0.75 mg/100 g body weight for a duration of 21 days. At the end of each week (7th, 14th and 21st) three (3) rats from each group was sacrificed and analysed.
Collection of Blood
Anesthesia (chloroform) was used to immobilize the animals after which blood samples for the various groups were collected into lithium heparin bottles, centrifuged for five minutes and stored for further analysis.
Estimation of Lipid Profile and Haemoglobin Conentration
Cholesterol, triglycerides and HDL (high density lipoprotein) were assayed on the principle that enzymatic hydrolysis and oxidation yields a colored product which can be quantified, randox test kit as used by Nzor, Onuoha, Samuel, Okari and Archibong [8] in the determination of lipid profile were also used to test for cholesterol, triglycerides and HDL. While LDL (low density lipoprotein) concentration was obtained using friedwald’s formular [9] and haemoglobin concentration was estimated using direct cyanmethaemoglobin methods [10].
Analysis of Result
Results obtained from analysis were subjected to statistical analysis using IBM SPSS 23 (IBM Inc., Armonk, NY, USA). The data obtained from statistical analysis are represented as mean values plus or minus standard deviation, at 95 % confidence level (P ˂ 0.05) the statistical values were considered significant (Tables 1-5).Table 1: Effect of Cialis on haemoglobin concentration of wistar rats. Alphabet a stand for significant difference between the control groups and test group.Table 2:Effect of Cialis on Cholesterol concentration of wistar rats.Table 3: Effect of Cialis on HDL concentration of wistar ratsTable 4: Effect of Cialis on LDL concentration of wistar rats.Table 5: Effect of Cialis on triglyceride concentration of wistar rats
Discussion
From the data obtained in this study, cialis administration increased haemoglobin concentration significantly in a dose dependent mode, likewise similar effect of increase in concentration level was observed on the lipid profile with significant increase HDL level. Haemoglobin plays a vital role in the transport of oxygen from the lung to the tissues of the body that requires it and in turn transports carbon dioxide back to the lung for expiration. Reduction in haemoglobin concentration is accompanied by either a decrease or not in red blood cell concentration and could progress to anemia. Cilias is usually consumed by older men. Extremely low haemoglobin concentration is a risk factor for the development of dementia and cognitive impairment especially for older individuals.Drugs which results to a decrease in haemoglobin concentration would be detrimental to the health specifically when used by advanced persons [11]. Correlation exist between lipid profile and haemoglobin concentration, an individual with reduced haemoglobin concentration would likely also have reduced cholesterol and lipoproteins levels resulting from dilution of the plasma, amplified cholesterol demand due to increased erythropoiesis etc [12,13]. High level of LDL and cholesterol are risk factor for the development of diabetes and atherosclerosis and as such must be monitored and caution taken if a medication would alter their concentration. Lopes, Munhoz, Antonangelo [14] in their study stated that elevated lipid profile with corresponding increase in hematocrit is attributed solely to the mechanism of reverse cholesterol transport. In conclusion Cialis administration on wistar rats increases the haemoglobin concentration significantly and slight alteration of lipid profile in an increasing pattern.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Pharmacy & Pharmaceutical Sciences please click on: https://juniperpublishers.com/gjpps/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/gjpps/GJPPS.MS.ID.555699.php
#Juniper Publishers in USA#Open Access Journlas#Juniper Publishers LLC#Juniper Publishers Review#Juniper Publishers Publishing Group
31 notes
·
View notes
Text
Stressful Life Events for Suicide. Suicide in Intensive Care Units and in Primary Care Units-Juniper Publishers

Abstract
Background: As a stressful life event characterized and is considered an event that periods preceding the occurrence of a disease and / or a self-destructive behavior, which results in a change or imbalance in the level of the individual’s adaptation to its environment. The impact of stressful life events such as death, divorce, etc or the various changes of life such as change house, retirement, etc on the mental and physical health of a person it has been investigated by several researchers worldwide. The article reviews the impact of the stressful life events for suicide and suicide in Intensive Care Units and in Primary Care Units.
Methods: Literature review studies, articles have been recovered for review of computer searches. No time limit was set. Used those articles written in Greek and English.
Conclusion: The involvement of stressful life event plays an important role in suicide event. Nursing and medical staff in the Intensive Care Units must be aware of their attitudes towards the patients that have committed suicide. Future surveys must focus on the prevention, treatment and development protocols of suicide in Primary Care.
Keywords: Suicide; Stressful life events; Intensive care unit; Primary care
Introduction
The impact of stressful life events (stressful life events, eg, death, divorce, etc.) or the various changes of life (eg, change house, retirement, etc.) on the mental and physical health of a person, it has been investigated by several researchers worldwide. The term stressful life events (stressful life events), it is frequently found in the literature of the science that deals with suicide and negative life events (negative life events), as well as adverse life events (adverse life events) [1,2].
As a stressful life event characterized and considered, an event that periods preceding the occurrence of a disease and / or a self-destructive behavior, which results in a change or imbalance in the level of the individual’s adaptation to its environment without it the definition excludes events occurring in past tense, which may carry long stressful effect on the individual. A stressful event can be independent of the personal responsibility of the individual (eg, loss of loved one) or to be dependent directly and / or indirectly to the person (eg, job loss). Particular issues in research of stressful life events are the concept of change occurring in the person’s life after the existence of such an event, the desirability or not of the fact, the gravity, and the address of the person [3]. Accepting the importance of stressful life events and their association with adverse health dimensions in person, led several researchers to develop questionnaires and semi structured interviews for more detailed information and recording of the person’s living conditions. Quantitative assessment of stressful life events initiated by Holmes and Rahe (1967) who created the Social Readjustment Rating Scale (SRSS), and then internationally similar questionnaires was presented by several researchers, while in Greece built by Madianos [4].
As far as that concern the gender and specifically for men, the main reason for admission to the ICU was car accidents (64.4%) followed by the pathology problems (12%), postoperative monitoring (6.2%), work accidents (5.6%), crimes (5.3%), drugs (3.6%), and finally the suicide attempt (2.9%) [5]. Surveys have shown that as many as 83% of suicide attempters are not identified as a danger to themselves by healthcare providers, even when examined by professionals in the months before their suicide attempt [6].
Stressful Life Events in Suicide
An extensive body of psychological autopsy studies during the last half century, says that almost all suicides had experienced at least one stressful life event (usually more than one), within the last year before their death. They have play role in recent months and/or weeks before the self-destructive behavior [7]. Specific events seem to have a special weight and increase the risk of suicide of a person, such as interpersonal conflicts (family or relationships with third parties), separation/divorce, physical illness, unemployment, problems at work, financial problems, serious injury or attack, mourning the person loss, domestic violence, problems with the law (imprisonment). In men suicides, presented more frequent stressful life events such as separation/divorce, physical illness, unemployment, problems at work, financial problems, and grief. In younger persons, seems to precede suicidal behavior stressful events such as interpersonal problems/loss, family relationship problems, rejection, unemployment/employment problems, violation of law, economic problems, change of residence/move, and events that are the result of personal their behavior, while in older people physical diseases is most often a predisposing factor [8,9].
However, most research on the nature and effect of stressful life events on suicide have been conducted in developed countries. Vijayakumar, John, Pirkis, and Whiteford (2005) support that a variation is observed as to which events are related to subsequent suicide of a person in developing countries. Problems in marriage and other family problems recorded in India and Taiwan, while events such as a social change occurs only in developing countries. In particular, data from mainly descriptive studies, indicate that modernization in many Asian countries has resulted the birth of cultural tensions, the presence of socio-economic stressors, and the collapse of the traditional family system. These facts led some people in suicidal behavior [10].
However, Yufit & Bongar [11] support that although the recent stressful events may be plays an important role for the subsequent suicide of a person, these events should be seen in a broader context, and examine the structure of the personality, and the ability to address (or is vulnerable) stress, failure and loss. Moreover, Maris et al. [12] argued that most people do not commit suicide because of anxiety and stressful life events, but those that commit a suicide or make an attempt are particularly sensitive and vulnerable to face a stressful event and fail to cope. They point out that all people have a pain threshold, beyond which the individual can not cope with the stress and then the self-destructive behaviors are the last resort.
Suicide in Intensive Care Unit
A study conducted on the medical intensive care unit of the university hospital in Germany, between January 1993 and December 1999 showed that because of the excellent care in the prehospital phase and in the emergency room the number of patients requiring treatment on the intensive care unit was rather low [13].
The aim of a study that took place in Greece was to explore the attitudes of Greek nurses' working in surgical, medical, orthopedic, Emergency department and Intensive Care Units towards attempted suicide. Nursing staff frequently encounter suicidal patients and therefore must be aware of their attitudes towards this group of patients as part of their therapeutic role. A nurse's positive attitudes towards attempted suicide can play an important role in preventing a future suicide attempt or a fatal suicide [14].
Suokas and Lonnqvist, compared emergency department nursing staff attitudes to self-harming clients with intensive care staff and found that emergency nursing staff to be more negative towards these clients than the intensive care staff [15].
Suicide in Primary Care
Craig et al. in a in a survey that took place in primary care a novel contextual rating of the potential of stressors in to produce symptoms for 'secondary gain'. In the 38 weeks before symptom onset, psychologisers and somatisers were more likely to have experienced at least one stressful event. Prevention programs have recommended for the improving detection of depression by primary care professionals and this may reduce suicides among women [16].
According to Goodwin et al. [17] supports that some physical disorders may be associated with increased suicidal ideation and may also play an important role in the relationship between suicidal ideation and depression among patients in primary care. Doctors in Primary care may wish to attend an in depth evaluation of psychiatric problems, especially current suicidal ideation, among patients with determinate physical illnesses.
Moreover, Maniou et al. [18] in a primary care survey conducted in Crete say that suicide committed the 4.4% of the general population that took part in the research. Moreover, in the same survey the 1% thinks to hurt himself and the 11.8% says that no one deserves to live.
Conclusion
The involvement of stressful life event plays an important role in suicide event. Nursing and medical staff in the Intensive Care Units must be aware of their attitudes towards the patients that have committed suicide. Future surveys must focus on the prevention, treatment and development protocols of suicide in Primary Care.
For more Journals in Juniper Publishers please click on https://juniperpublishers.com/journals.php
For more articles in Journal of Nursing & Health Care please click on https://juniperpublishers.com/jojnhc/index.php
0 notes