#Presepsin
Text
Usefulness of Presepsin Concentrations for Differentiating Sepsis Severity | Chapter 06 | New Horizons in Medicine and Medical Research Vol. 6
The importance of early detection and treatment of sepsis is critical for a better clinical outcome. For the quick diagnosis of sepsis, many sepsis biomarkers are commonly employed. This study looked into the diagnostic accuracy of presepsin, procalcitonin (PCT), and C-reactive protein (CRP) in distinguishing sepsis severity, as well as their link with the Sepsis-related Organ Failure Assessment (SOFA) score.
100 septic patients from two university clinical centres were enrolled in the trial during two time periods. The Sepsis-3 definitions were used to stratify the patients. Biomarkers and the SOFA score were measured four times during the illness. A sandwich ELISA kit was used to measure presepsin. A generalised linear mixed effects model was used to assess changes in biomarker concentrations and SOFA score values during the illness, as well as to quantify differences across severity groups. Multivariate analysis was used to look into the relationship between biomarkers and SOFA score.
Patients with septic shock (n=34) exhibited substantially higher presepsin concentrations on admission than patients with sepsis (n=66), with mean vs. SD of 128.547.6 ng/mL vs. 88.665.6 ng/mL, respectively (p0.001). PCT and CRP concentrations were not substantially different between sepsis severity groups. There was also a high association between presepsin and SOFA score (p0.0001).
Conclusions: In the research groups, presepsin showed a strong ability to differentiate septic shock from sepsis. The severity of sepsis was not differentiated by PCT or CRP.
Author(S) Details
Ajete Aliu-Bejta
ICU Department, University Clinic of Infectious Diseases, Alexander Flemingu, 10000 Pristina, Kosovo.
Anita Atelj
ICU Department, University Hospital for Infectious Diseases “Dr. Fran Mihaljevic”, Mirogojska 8, 10000 Zagreb, Croatia.
Mentor Kurshumliu
“PROLAB” Biochemical Laboratory, Mark Dizdari, 10000 Pristina, Kosovo.
Shemsedin Dreshaj
ICU Department, University Clinic of Infectious Diseases, Alexander Flemingu, 10000 Pristina, Kosovo.
Bruno Barsic
ICU Department, University Hospital for Infectious Diseases “Dr. Fran Mihaljevic”, Mirogojska 8, 10000 Zagreb, Croatia.
View Book:-
https://stm.bookpi.org/NHMMR-V6/article/view/6437
0 notes
Text
Increasing regulatory approval and the introduction of technologically advanced diagnostic solutions are expected to be the prominent factors facilitating market growth over the forecast period. For instance, in May 2020, Beckman Coulter launched its new DxH 690T hematology analyzer with early sepsis indicators in the U.S. Moreover, in August 2018, Japan-based Sysmex Corporation launched its new HISCL Presepsin Assay Kit for determining levels of presepsin, the main test parameter for bacterial sepsis. This kit is designed to achieve early diagnosis of bacterial sepsis with high precision as compared to conventional biomarkers.
0 notes
Text
Global Sepsis Diagnostics Market, Size, Share, Trends, Report & Forecast to 2025
The global sepsis diagnostics market is estimated to grow at a significant CAGR during the forecast period. Sepsis is a major unmet medical need caused by a patient’s overwhelming and life-threatening immune response to infection and can lead to tissue damage, organ failure, and even death. Sepsis affects an estimated 20-30 million people globally every year. According to the Agency for Healthcare Research and Quality, sepsis is the most expensive condition treated in US hospitals, costing more than $20 billion and increasing annually on average by 11.9%.
Get Free Sample Copy @
https://www.omrglobal.com/request-sample/sepsis-diagnostics-market
The key players operating in the global sepsis diagnostics market is also driving the market growth. Players such as Abbott Laboratories, Inc., Becton, Dickinson & Co., Biomérieux SA, Bruker Corp., Danaher Corp., F. Hoffmann-La Roche Ltd., Luminex Corp., Qiagen NV, Siemens AG, Sysmex Corp., Thermo Fisher Scientific Inc., and Trinity Biotech Plc, among others are significantly contributing to the sepsis diagnostics industry growth by adopting various growth strategies. Product launches & developments, partnerships, agreements, and acquisitions are among some of the strategies adopted by the players to sustain in a competitive sepsis diagnostics market globally, during the forecast period.
A Full Report of Global Sepsis Diagnostics Marketis Available at:
https://www.omrglobal.com/industry-reports/sepsis-diagnostics-market
In April 2019, the Scottish Government along with FEAT - The Fiona Elizabeth Agnew Trust, Sepsis Research center started a campaign across Scotland to create public awareness regarding signs and symptoms of sepsis.
In April 2019, the US FDA approved Beckman Coulter Inc., a Danaher Corp. company for its Early Sepsis Indicator. This indicator is a cellular biomarker designed and enables the identification of patients with sepsis or at high risk of developing the disease.
In August 2018, Sysmex Corp., a Japan-based company introduced its new HISCL Presepsin Assay Kit, for the detection of presepsin, the primary test parameter for bacterial sepsis. This kit aid in the early diagnosis of bacterial sepsis with higher accuracies in comparison with conventional biomarkers.
In May 2018, the US FDA approved T2 Biosystems, Inc., a US-based emerging medical examination solutions company for its T2Bacteria Panel. The novel developed panel is intended for the recognition of specific sepsis-causing bacterial pathogens in human whole blood specimens.
In March 2018, Biocartis Group NV, a molecular diagnostics company and Immunexpress Pty Ltd, a host response molecular diagnostic company, committed to improving clinical and economic outcomes for suspected sepsis patients, today announced that they have entered into a partnership agreement aimed at the development and commercialization of Immunexpress’ SeptiCypte test for use on Biocartis’ sample-to-result Idylla platform.
Global Sepsis Diagnostics Market – Segmentation
By Product Type
Instruments
Assays and Reagents
Other Products
By Technology
Molecular Diagnostics
Immunoassay
Others
By Pathogen
Bacterial Sepsis Diagnostics
Fungal Sepsis Diagnostics
Others
Global Sepsis Diagnostics Market – Segmentation by Region
North America
United States
Canada
Europe
Germany
United Kingdom
France
Spain
Italy
Rest of Europe
Asia-Pacific
China
Japan
India
Rest of Asia-Pacific
Rest of the World
For More Customized Data, Request for Report Customization @ https://www.omrglobal.com/report-customization/sepsis-diagnostics-market
About Orion Market Research
Orion Market Research (OMR) is a market research and consulting company known for its crisp and concise reports. The company is equipped with an experienced team of analysts and consultants. OMR offers quality syndicated research reports, customized research reports, consulting and other research-based services.
Media Contact:
Company Name: Orion Market Research
Contact Person: Mr. Anurag Tiwari
Email: [email protected]
Contact no: +91 780-304-0404
0 notes
Text
Các dấu ấn sinh học của nhiễm khuẩn huyết trong quá trình lọc máu liên tục Update 06/2021
Bài viết Các dấu ấn sinh học của nhiễm khuẩn huyết trong quá trình lọc máu liên tục Update 06/2021 được chia sẻ bởi website Blog-Health
#bloghealth #suckhoe #lamdep #sinhly
Bài viết bởi Tiến sĩ, Bác sĩ Trương Ngọc Hải - Bác sĩ Hồi sức - Khoa Hồi sức cấp cứu - Bệnh viện Đa khoa Quốc tế Vinmec Central Park
<!-- -->
Ngày nay, với gần 180 dấu ấn sinh học đã được xác định, nhiều dấu ấn sinh học đang được các bác sĩ sử dụng để phát hiện, theo dõi diễn biến, đánh giá tiên lượng của tình trạng nhiễm khuẩn, nhiễm khuẩn huyết và quyết định ngừng thuốc kháng sinh. Tuy nhiên, các dấu ấn sinh học này có thể bị thải trừ trong quá trình lọc máu liên tục, ảnh hưởng đến độ tin cậy trong xác định mức độ nghiêm trọng của tình trạng nhiễm khuẩn. Cho đến nay, các chuyên gia vẫn đang nỗ lực tìm kiếm dấu ấn sinh học mới không bị thải trừ qua CRRT.
1. Các dấu ấn sinh học được sử dụng thường xuyên nhất trên lâm sàng
1.1. C-reactive Protein
C-reactive Protein (CRP) chủ yếu hiện diện dưới dạng monome (mCRP) trong máu của bệnh nhân nhiễm khuẩn huyết [5], do trọng lượng phân tử tương đối nhỏ (22- 25 kDa) nên được thải trừ trong tất cả các phương thức CRRT [4]. Ngoài ra, một lượng đáng kể mCRP cũng được hấp phụ trên màng lọc [2, 6]. Hiện nay, nhiều khoa Hồi sức cấp cứu sử dụng các màng lọc có tính hấp phụ cao càng tăng thải trừ mCRP. Nồng độ trong huyết tương của C-reactive Protein có thể thấp giả tạo trong quá trình CRRT, nên nồng độ CRP không đáng tin cậy trong chẩn đoán hoặc đánh giá mức độ nhiễm khuẩn trong quá trình CRRT [7].

CRP xuất hiện trong máu của bệnh nhân nhiễm khuẩn huyết
1.2. Procalcitonin (PCT)
Ở những bệnh nhân nhiễm khuẩn huyết được lọc máu tĩnh-tĩnh mạch liên tục (CVVH), PCT được phát hiện trong dịch siêu lọc của tất cả các bệnh nhân [10]. Hầu hết lượng PCT sẽ được thải trừ qua dòng dịch đối lưu, nhưng cơ chế hấp phụ cũng góp phần thải trừ PCT trong những giờ đầu điều trị [10]. Sử dụng các màng lọc có tính hấp phụ cao càng gia tăng hơn nữa thải trừ CRP và PCT [6, 11].
1.3. Brain Natriuretic Factors
Dấu ấn sinh học BNP và NT-proBNP được ứng dụng gần đây trong nhiễm khuẩn huyết. Cả hai dấu ấn sinh học BNP và NT-proBNP đều bị thải trừ rất dễ dàng qua các loại màng lọc high-flux và low-flux trong CRRT do kích thước phân tử thấp của chúng [13], [14].
2. Các dấu ấn sinh học Cytokine/Chemokine trong nhiễm khuẩn huyết
2.1. High Mobility Group 1 Protein (HMGB-1)
Mặc dù HMGB-1 có trọng lượng phân tử tương đối thấp nên về lý thuyết HMGB-1 có thể bị thải trừ qua cơ chế lọc đối lưu. Tuy nhiên, thực tế HMGB-1 chỉ được thải trừ hiệu quả thông qua cơ chế hấp phụ bằng các loại màng lọc có tính hấp phụ cao, đặc biệt là màng lọc được xử lý bề mặt acrylonitrile 69 (AN69-ST) [15].

Trong cơ chế lọc dối lưu, HMGB1bị thải trừ nhưng không hiệu quả
2.2. Osteopontin
Osteopontin là một protein tích điện âm, có trọng lượng phân tử khoảng 32 kDa. Chưa có bằng chứng thuyết phục lọc máu liên tục có thể thải trừ Osteopontin trong hệ tuần hoàn [16]. Tuy nhiên, CRRT sử dụng các loại màng lọc mới, ví dụ màng lọc AN69-ST – do có bề mặt phủ lớp biopolymer polyethylen nên có mật độ điện tích dương cao, ngoài khả năng tương thích sinh học và tính thấm cao, màng này còn có khả năng hấp phụ mạnh nên có thể gia tăng thải trừ Osteopontin [6].
3. Dấu ấn sinh học trong nhiễm khuẩn huyết có liên quan đến tổn thương nội mô mạch máu – Endocan
Endocan là một loại dermatan sulfate proteoglycan hòa tan có nguồn gốc nội mô mới, có khối lượng phân tử khoảng 15-40 kDa [17, 18]. Các màng lọc CRRT hiện đại có thể thải trừ các chất có trọng lượng phân tử tới 35 kDa. Khi sử dụng màng lọc mới có tính hấp phụ cao, càng gia tăng khả năng thải trừ endocan qua CRRT [6]. Do đó, mức độ tin cậy của endocan trong CRRT có thể bị thay đổi.

Endocan có thể bị thải trừ qua màng lọc CRRT
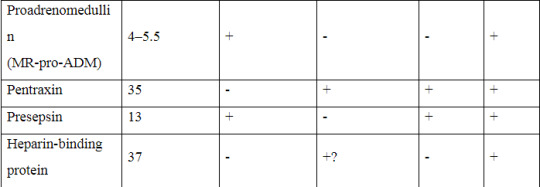
4. Dấu ấn sinh học trong nhiễm khuẩn huyết có liên quan đến dãn mạch – Proadrenomedullin (MR-proADM)
Trọng lượng phân tử của MR-proADM là từ 4 đến 5,5 kDa, nên cũng có thể bị CRRT loại bỏ. Nghiên cứu của Mueller và cộng sự cho thấy sự sụt giảm đáng kể của MR-proADM (45, 65%) nếu sử dụng màng lọc high-flux [20] (đặc biệt là với ngưỡng lọc 35 kDa của các màng lọc CRRT hiện đại [6]). Cần có thêm các nghiên cứu xác định có hay không khả năng thải trừ MR-proADM bằng cơ chế đối lưu trong CRRT.
5. Dấu ấn sinh học khác trong giai đoạn cấp tính – Pentraxin
Pentraxin-3 (PTX3) là một glycoprotein được các tế bào nội mô và tế bào viêm phóng thích khi nhận kích hoạt của cytokine và endotoxin. PTX3 phản ánh tình trạng viêm của các mạch máu tại chỗ và tải lượng vi khuẩn tốt hơn CRP [23]. Do đó, PTX3 có thể là một dấu hiệu thích hợp hơn CRP về phản ánh mức độ nghiêm trọng và tiên lượng của nhiễm khuẩn mô mềm hoại tử. Theo báo cáo của Hansen, mối liên quan có ý nghĩa thống kê giữa nồng độ PTX3 cao và sự xuất hiện của sốc nhiễm khuẩn, cắt cụt chi, nhu cầu lọc máu và nguy cơ tử vong ở bệnh nhân bị nhiễm khuẩn hoại tử mô mềm [23].
Hầu hết ở các bệnh nhân, PTX3 trong huyết tương ở dạng đơn phân có trọng lượng phân tử khoảng 35 kDa [23] và do đó trên lý thuyết có thể được thải trừ bằng CRRT. Gần đây, Schilder và cộng sự đã chứng minh tuy PTX3 được hấp phụ một ít nhưng phương thức CVVH không thải trừ được PTX3 bằng cơ chế đối lưu, dẫn đến nồng độ PTX3 trong huyết tương không thay đổi [24]. Cần nghiên cứu thêm khả năng tăng thải trừ PTX3 với phương thức CVVH sử dụng các loại màng lọc có đặc tính hấp phụ cao [24, 25].
Pentraxin-3 (PTX3) có mối liên quan đến tình trạng sốc nhiễm khuẩn
6. Dấu ấn sinh học nhóm dấu ấn tế bào trong nhiễm khuẩn huyết – Presepsin
Gần đây, sCD14-ST còn được gọi là presepsin, đã được xác định là một dấu ấn sinh học tiềm năng của nhiễm khuẩn huyết [26]. Presepsin được phân mảnh từ một glycoprotein lớn hơn và có trọng lượng phân tử khoảng 13 kDa. Độ thanh thải của presepsin có thể còn cao hơn dự kiến vì phân tử này có thể “kết dính” vào màng lọc có tính hấp phụ cao [6].
7. Dấu ấn sinh học về đông máu trong nhiễm khuẩn huyết - Heparin Binding Protein
Heparin Binding Protein (HBP) còn được gọi là protein kháng khuẩn mang điện tích dương, có trọng lượng phân tử là 37 kDa [28] và do đó có thể được CRRT thải trừ thông qua cơ chế đối lưu [6]. Sử dụng các màng lọc có tính hấp phụ cao có thể giúp tăng cường khả năng thải trừ HBP thông qua cơ chế hấp phụ [6].
Bảng sau đây tóm tắt tất cả các dấu ấn sinh học được mô tả trong tổng quan này với thông tin về trọng lượng phân tử, khả năng thải trừ bằng cơ chế đối lưu và/hoặc hấp phụ, ghi nhận nghiên cứu đã có và cần nghiên cứu thêm. Qua đó cho thấy, các dấu ấn sinh học đều có thể được thải trừ qua CRRT, đặc biệt khi sử dụng màng lọc có tính hấp phụ cao. Vì vậy chưa có bất kỳ dấu ấn sinh học nào phản ánh chính xác tình trạng nhiễm khuẩn ở bệnh nhân đang được CRRT. Cần thực hiện nhiều nghiên cứu để đánh giá, tìm ra dấu ấn sinh học mới đáng tin cậy phản ánh tình trạng nhiễm khuẩn trong quá trình CRRT. Nhiệm vụ này còn trở nên phức tạp hơn khi màng lọc có tính hấp phụ cao đã nâng ngưỡng lọc lên tới 65 kDa.

Dấu ấn sinh học về đông máu trong nhiễm khuẩn huyết
Tài liệu tham khảo
1.Pierrakos C, Vincent JL. Sepsis biomarkers: a review. Crit Care. 2010;14:R15.
2. Honore PM, Jacobs R, De Waele E, Van Gorp V, Spapen HD. Biomarkers of inflammation during continuous renal replacement therapy: sensors, players, or targets? Blood Purif.
2014;38:102–3.
3. Tillett WS, Francis T. Serological reactions in pneumonia with a non-protein somatic fraction
of pneumococcus. J Exp Med. 1930;52:561–71.
4. McFadyen JD, Kiefer J, Braig D, et al. Dissociation of C-reactive protein localizes and amplifes inflammation: evidence for a direct biological role of C-reactive protein and its conformational changes. Front Immunol. 2018;9:1351.
5. Taylor KE, van den Berg CW. Structural and functional comparison of native pentameric,
denatured monomeric and biotinylated C-reactive protein. Immunology. 2007;120:404–11.
6. Dahaba AA, Elawady GA, Rehak PH, List WF. Procalcitonin and proinflammatory cytokine
clearance during continuous venovenous haemofltration in septic patients. Anaesth Intensive
Care. 2002;30:269–74.
7. Matsui T, Nakagawa T, Kikuchi H, Horio H, Hashimura K. The effect of continuous renal
replacement therapy with the AN69ST membrane on inflammatory markers and the level of
consciousness of hemodialysis patients with stroke: comparison with hemodialysis with low
blood flow rate. Pril (Makedon Akad Nauk Umet Odd Med Nauki). 2018;39:29–35.
8. Taylor R, Jones A, Kelly S, et al. A review of the value of procalcitonin as a marker of infection. Cureus. 2017;9:e1148.
9. Vijayan AL, Ravindran S, Saikant R, Lakshmi S, Kartik R. Procalcitonin: a promising diagnostic marker for sepsis and antibiotic therapy. J Intensive Care. 2017;5:51.
10. Level C, Chauveau P, Guisset O, et al. Mass transfer, clearance and plasma concentration of
procalcitonin during continuous veno-venous hemofltration in patients with septic shock and
acute oliguric renal failure. Crit Care. 2003;6:R160–6.
11. Honore PM, Jacobs R, Joannes-Boyau O, et al. Newly designed CRRT membranes for sepsis and SIRS—a pragmatic approach for bedside intensivists summarizing the more recent
advances: a systematic structured review. ASAIO J. 2013;59:99–106.
12. N L, Zhang Y, Fan S, Xing J, Liu H. BNP and NT-proBNP levels in patients with sepsis. Front Biosci (Landmark Ed). 2013;18:1237–43.
13. Pirracchio R, Salem R, Mebazaa A. Use of B natriuretic peptide in critically ill patients.
Biomark Med. 2009;3:541–7.
14. Wahl HG, Graf S, Renz H, Fassbinder W. Elimination of the cardiac natriuretic peptides
B-type natriuretic peptide (BNP) and N-terminal proBNP by hemodialysis. Clin Chem.
2004;50:1071–4.
15. Yumoto M, Nishida O, Moriyama K, et al. In vitro evaluation of high mobility group box
1 protein removal witvarious membranes for continuous hemofltration. Ther Apher Dial. 2011;15:385–93.
16. Honore PM, Jacobs R, Hendrickx I, De Waele E, Van Gorp V, Spapen HD. To counteract or to clear high-mobility group box-1 protein in influenza A (H1N1) infection? That may become
the question. Crit Care. 2015;19:401.
17. Honore PM, De Bels D, Attou R, Redant S, Gallerani A, Kashani K. Endocan removal during continuous renal replacement therapy: does it affect the reliability of this biomarker? Crit Care.2019;23:184.
18. Hureau M, Gaudet A, De Freitas Caires N, et al. Endocan is a reliable biomarker during continuous renal replacement therapy. Crit Care. 2019;23:296.
19. De Freitas Caires N, Gaudet A, Portier L, Tsicopoulos A, Mathieu D, Lassalle P. Endocan,
sepsis, pneumonia, and acute respiratory distress syndrome. Crit Care. 2018;22:280.
20. Mueller T, Gegenhuber A, Kronabethleitner G, Leitner I, Haltmayer M, Dieplinger B. Plasma concentrations of novel cardiac biomarkers before and after hemodialysis session. Clin
Biochem. 2015;48:1163–6.
21. Elke G, Bloos F, Wilson DC, et al. The use of mid-regional proadrenomedullin to identify
disease severity and treatment response to sepsis—a secondary analysis of a large randomised
controlled trial. Crit Care. 2018;22:79.
22. Honore PM, De Bels D, Attou R, Redant S, Kashani K. The challenge of removal of sepsis
markers by continuous hemofltration. Crit Care. 2019;23:173.
23. Hansen MB, Rasmussen LS, Garred P, Bidstrup D, Madsen MB, Hyldegaard O. Pentraxin-3 as a marker of disease severity and risk of death in patients with necrotizing soft tissue infections: a nationwide, prospective, observational study. Crit Care. 2016;20:40.
24. Schilder L, Nurmohamed SA, ter Wee PM, et al. Putative novel mediators of acute kidney
injury in critically ill patients: handling by continuous venovenous hemofltration and effect of
anticoagulation modalities. BMC Nephrol. 2015;16:178.
25. Honore PM, Spapen HD. Pentraxin-3 to better delineate necrotizing soft tissue infection: not
really! Crit Care. 2016;20:173.
26. Zhang X, Liu D, Liu YN, Wang R, Xie LX. The accuracy of presepsin (sCD14-ST) for the
diagnosis of sepsis in adults: a meta-analysis. Crit Care. 2015;19:323.
27. Honore PM, Jacobs R, Hendrickx I, De Waele E, Van Gorp V, Spapen HD. Presepsin and
sepsis-induced acute kidney injury treated with continuous renal replacement therapy: will
another promising biomarker bite the dust? Crit Care. 2015;19:428.
28. Honore PM, De Bels D, Barreto Gutierrez L, Redant S, Spapen HD. Heparin-binding protein
in sepsis: player! predictor! positioning? Ann Intensive Care. 2019;9:71.
29. Tverring J, Vaara ST, Fisher J, Poukkanen M, Pettilä V, Linder A, FINNAKI Study Group.
Heparin-binding protein (HBP) improves prediction of sepsis-related acute kidney injury. Ann
Intensive Care. 2017;7:105.
30. Honore PM, Jacobs R, Hendrickx I, De Waele E, Van Gorp V, Spapen HD. ‘Biomarking’ infection during continuous renal replacement therapy: still relevant? Crit Care. 2015;19:232.
31. Schadler D, Pausch C, Heise D, et al. The effect of a novel extracorporeal cytokine hemoadsorption device on IL-6 elimination in septic patients: a randomized controlled trial. PLoS One. 2017;12:e0187015.
32. Honore PM, Hoste E, Molnár Z, et al. Cytokine removal in human septic shock: where are we and where are we going? Ann Intensive Care. 2019;9:56
source https://blog-health.com/cac-dau-an-sinh-hoc-cua-nhiem-khuan-huyet-trong-qua-trinh-loc-mau-lien-tuc/
0 notes
Text
Global Sepsis Diagnostics Market Size, Share, Forecast 2019-2025
The global sepsis diagnostics market is estimated to grow at a significant CAGR during the forecast period. Sepsis is a major unmet medical need caused by a patient’s overwhelming and life-threatening immune response to infection and can lead to tissue damage, organ failure, and even death. Sepsis affects an estimated 20-30 million people globally every year. According to the Agency for Healthcare Research and Quality, sepsis is the most expensive condition treated in US hospitals, costing more than $20 billion and increasing annually on average by 11.9%.
Get Free Sample Copy @ https://www.omrglobal.com/request-sample/sepsis-diagnostics-market
The key players operating in the global sepsis diagnostics market is also driving the market growth. Players such as Abbott Laboratories, Inc., Becton, Dickinson & Co., Biomérieux SA, Bruker Corp., Danaher Corp., F. Hoffmann-La Roche Ltd., Luminex Corp., Qiagen NV, Siemens AG, Sysmex Corp., Thermo Fisher Scientific Inc., and Trinity Biotech Plc, among others are significantly contributing to the sepsis diagnostics industry growth by adopting various growth strategies. Product launches & developments, partnerships, agreements, and acquisitions are among some of the strategies adopted by the players to sustain in a competitive sepsis diagnostics market globally, during the forecast period.
A Full Report of Global Sepsis Diagnostics Market is Available at: https://www.omrglobal.com/industry-reports/sepsis-diagnostics-market
In April 2019, the Scottish Government along with FEAT - The Fiona Elizabeth Agnew Trust, Sepsis Research center started a campaign across Scotland to create public awareness regarding signs and symptoms of sepsis.
In April 2019, the US FDA approved Beckman Coulter Inc., a Danaher Corp. company for its Early Sepsis Indicator. This indicator is a cellular biomarker designed and enables the identification of patients with sepsis or at high risk of developing the disease.
In August 2018, Sysmex Corp., a Japan-based company introduced its new HISCL Presepsin Assay Kit, for the detection of presepsin, the primary test parameter for bacterial sepsis. This kit aid in the early diagnosis of bacterial sepsis with higher accuracies in comparison with conventional biomarkers.
In May 2018, the US FDA approved T2 Biosystems, Inc., a US-based emerging medical examination solutions company for its T2Bacteria Panel. The novel developed panel is intended for the recognition of specific sepsis-causing bacterial pathogens in human whole blood specimens.
In March 2018, Biocartis Group NV, a molecular diagnostics company and Immunexpress Pty Ltd, a host response molecular diagnostic company, committed to improving clinical and economic outcomes for suspected sepsis patients, today announced that they have entered into a partnership agreement aimed at the development and commercialization of Immunexpress’ SeptiCypte test for use on Biocartis’ sample-to-result Idylla platform.
Global Sepsis Diagnostics Market – Segmentation
By Product Type
Instruments
Assays and Reagents
Other Products
By Technology
Molecular Diagnostics
Immunoassay
Others
By Pathogen
Bacterial Sepsis Diagnostics
Fungal Sepsis Diagnostics
Others
Global Sepsis Diagnostics Market – Segmentation by Region
North America
United States
Canada
Europe
Germany
United Kingdom
France
Spain
Italy
Rest of Europe
Asia-Pacific
China
Japan
India
Rest of Asia-Pacific
Rest of the World
For More Customized Data, Request for Report Customization @ https://www.omrglobal.com/report-customization/sepsis-diagnostics-market
About Orion Market Research
Orion Market Research (OMR) is a market research and consulting company known for its crisp and concise reports. The company is equipped with an experienced team of analysts and consultants. OMR offers quality syndicated research reports, customized research reports, consulting and other research-based services.
Media Contact:
Company Name: Orion Market Research
Contact Person: Mr. Anurag Tiwari
Email: [email protected]
Contact no: +91 780-304-0404
0 notes
Quote
Kon gak isok ngrubah cara kerja lingkunganmu, isok e merubah presepsine kene dan beradaptasi baik2 nang keadaan iku...
Lalu semua bahagia
0 notes
Last Seen Blogs

temeyes
and run wild, i will.

brittanymeitse
Brittany Tse.

famouspeanutnight
Untitled

herblawyerup
Parsley Botch

slavesofpop
Slaves Of Pop