
Last Seen Blogs

zhucharik
zhuchara

tyedi3
alex :3

huntersurfer360
huntersurfer

sfde8871
What An A(i)Hole

goriaucom
Tanpa judul
Text
Why do I become sleepy after eating?

youtube
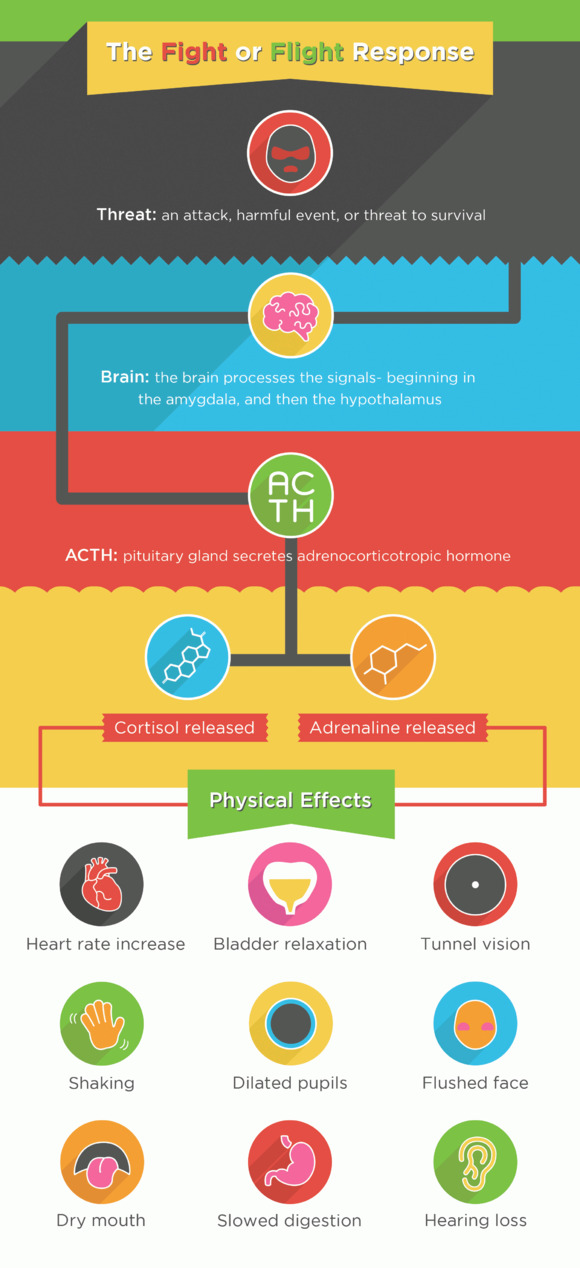
o The autonomic system (which controls involuntary action of the body, organs and glands etc.) comprises of the sympathetic nervous system (SNS) and the parasympathetic nervous system (PNS). *
o The SNS works via a fight or flight response - a primitive stress response when we faced danger by predators. Noradrenaline and adrenaline are catecholamines released by the adrenal gland which works by increasing the heart rate, respiratory rate, dilation of blood vessels in muscles, pupillary dilatation, slowing down of digestion etc. (see the picture below) It has a thoracolumbar outflow T1 to L2/3.
o The PNS works via a rest and digest response - a response when we are relaxed and calm. It has craniosacral outflow - the cranial nerves and S2-4 (the pelvic splanchnic nerves)
o Eating a meal stimulates more bloodflow to the digestive system and stimulates the PNS.
o Eating carbohydrates stimulates insulin production - the hormone that turns sugar into energy. Insulin also drives protein out of the bloodstream into cells. Some proteins however remain in the blood - such as tryptophan and albumin. There is now less competition for tryptophan to cross the blood-brain barrier to hit the brain and make melatonin - a hormone that regulates sleep and serotonin - its precursor.
* the autonomic nervous system also comprises of the enteric nervous system which controls the workings of the gastrointestinal tract.
References
https://www.webmd.com/food-recipes/features/the-truth-about-tryptophan#1
These two Crash Course videos are excellent:
https://youtu.be/0IDgBlCHVsA
https://youtu.be/qqU-VjqjczE
12 notes
·
View notes
Text
Rear Window
Alfred Hitchcock is one of my favourite directors (and that’s from a long list ranging from Wong Kar Wai, Steven Spielberg, Paul Thomas Anderson, David Fincher, John Woo, Zhang Yimou, Martin Scorsese, Ang Lee, Krzysztof Kieślowski, Michael Haneke, Mike Leigh, Christopher Nolan, Akira Kurosawa, Ingmar Bergman, Paolo Sorrentino etc.). The man literally reinvented the thriller and made murder and suspense something of a cinematic staple. When I think of horror, no one did it better than Hitchcock - nothing like the blood and gore of the crass Saw movies but rather in the anticipation and the creation of something horrible in the audience’s mind. And it’s this planting of the seed that causes us to become scared of the dark or empty houses for the days afterwards. Of Hitchcock’s films I have a firm favourite - without a doubt, Rear Window. Rear Window was the first Hitchcock film I ever watched as a pretentious sixteen year old and immediately I was hooked. Every time I watch the film I spot new details in one of the neighbours or in the apartment in Jeffries’ apartment, the changes in attire, the lighting, the set design etc. Watch the opening scene below which demonstrates a masterclass in cinematography. I was watching Rear Window again this summer in 2018 with a new twist given I was recovering from a foot operation and had to be placed in a plaster cast and immobilised. And instead of spying on my neighbours, I began to wonder about the underlying theme of the film and what Hitchcock was threading together scene by scene - voyeurism.
youtube
So what is voyeurism?
Voyeurism is derived from the French voir - to see. Voyeurism is defined as the act of looking at unsuspecting individuals, usually strangers, who are naked, in the process of disrobing or engaging in sexual activity. In fact this phenomenon has existed since ancient times with the Arthurian legend of Lady Godiva who rode on a horse around the streets of Coventry naked, and a Peeping Tom (not Loyd Grossman...you’ll have to be an Old Bean to get this 😪) was struck blind by sneaking a peek.
We will discuss voyeurism in a general sense, not in its strict psychiatric sense - sexual arousal only in voyeuristic activities, symptoms lasting more than six months etc. In fact we are all voyeurs in this sense, our consumption of media in the digital age ranging from reality television, movies, pornography etc.
Just a brief mention of voyeurism in its psychiatric sense - all Japanese cellphones now have the camera feature of a shutter sound when taking a photograph which cannot be disabled. This is because of the vast problem of upskirting particularly in subways. As mentioned voyeurism is vastly prevalent in our society and this example just shows the extent of this type of behaviour.
I recently watched Love Island - a reality TV show set on an sunny island with single men and women dressed in skimpy swimwear. I used to turn my nose up thinking I was above such things but after watching it, I realised I’m really not and I instantly got hooked. It literally is the trashiest thing I have seen on TV and I guess that’s part of its appeal. But it got me thinking about the sheer number of reality TV we watch, ranging from Kim Kardashian, Gogglebox - literally watching people watching television, and countless others. This rapid rise in reality television derives from its cheap cost to commission and its ability to create massive ad revenue. Its addictiveness relies on the savvy work of the producers who cut and paste different segments of dialogue in order to create a reaction in the audience and create drama. It’s a piece of manufactured genius of our modern times.
Admittedly there is a distinction between the true psychiatric definition of voyeurism and this general sense of voyeurism say in reality TV due to the fact that the victim is aware of the fact they are being watched - they have ‘consent’ from the TV producers hence not a true invasion in privacy per say (but you can probably see how this is flawed - hidden cameras where they don’t know they’re being watched and the ignorance of the millions watching and tweeting about them). There isn’t much in the audience of literature regarding this, in fact psychiatry is still rather primitive in our understanding of pathological behaviour and even more primitive in its treatment. So as a result a lot of this entry will rely on generalisation and observation and subjectivity - as with most psychology, but it’s important not to take this at face value. In fact, this entry will probably be my least scientific since there is little in the way of research but I’ll put my two cents in.
So what makes watching others so intriguing? There’s an element of keeping up with the Joneses - a comparison with others (“well I would never do what she did” and “thank God my life isn’t as bad is theirs”), there’s an element of empathy (“I can see myself in that position”) and an element of schadenfreude, public shaming and humiliation (“hahahahaha plebs” and “burn the witch!”).
And this rise in voyeurism is none more apparent in the millennials of the digital age, a mass cult following of youtubers, reaction videos, prank videos etc. There is there intention to offend, shock and cause a reaction (“Omg I can’t believe he did that!”). Passive keyboard warriors, trolling and SJWs hidden by a shield of anonymity where there are extremes of being offensive and too easily offended - a strange sort of hysteria of emotions running wild over logical sense. And hence we arrive at the current state of political commentary in 2018. I can’t be sure if this age of reality TV and shock value hasn’t contributed to political correctness gone mad, but I’d be surprised if it hasn’t. The creation of savvy sound bites, the cutting and pasting of dialogue said out of context and the pointing of figures in a splitting phenonomenon of right and wrong. This is no more apparent than in cyber bullying digital witch hunts which in Jon Ronson’s book So You’ve Been Publicly Shamed which he describes the consequences can be devastating.
There are three agents of the psychic apparatus. We’ll discuss the id, ego and superego in more detail in another movie entry (Fight Club) but for now let’s focus on the superego.
The superego is defined as reflects the internalization of cultural rules, mainly taught by parents applying their guidance and influence. Think of the superego as that nerdy kid in your class who was always a bit of a tattletale but as you realise as you get older was doing the right thing. In a nutshell, the superego strives to act in a socially appropriate manner. Now how does this relate back to Rear Window? Well the concept of watching others who are unsuspecting - “Big Brother is watching you” from Orwell’s 1984. This concept of someone watching you to see if you’re on your best behaviour is a effective way to control societal norms and behaviour. This harkens back to Santa Claus who knows if you’ve been on your best behaviour or not. I’d highly recommend (if I have not already done so) everybody to read Daniel Kahneman’s amazing book Thinking Fast and Slow where although the superego is not mentioned, the concept of acting in societal norms is discussed.
Kahneman discusses a poster in a British university kitchen stocked with tea and coffee where participants are asked whether they would like to make a voluntary donation. The poster is either accompanied by a picture of flowers or eyes looking at the observer on alternating weeks. The pictures are shown below.
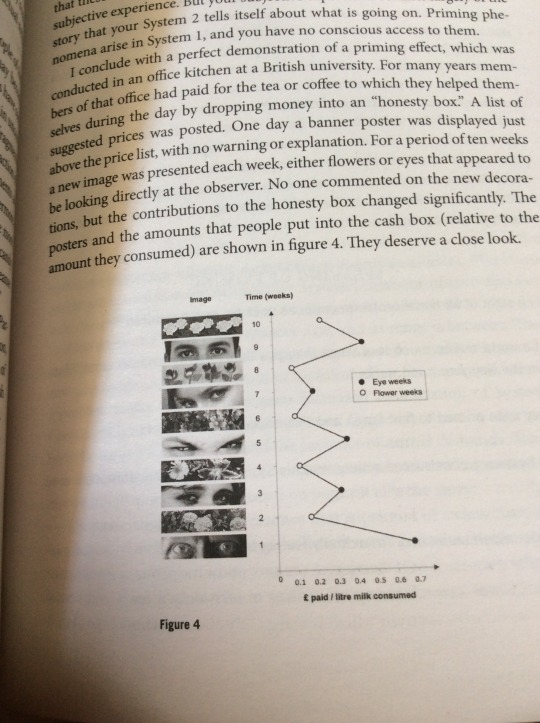
The striking take away message from this is that on the weeks with a picture of the eyes - the donations leapt up to three times as much as the weeks with pictures of flowers...
Another example discussed is the resulting lower prevalence of crime in areas with more surveillance and CCTV cameras (whether they are operating or not). If you have someone watching your every move, you sure as hell are going to be on your best behaviour. Having others who will hold you accountable leads to a very ‘well behaved society’ - a keeping up with the Joneses which can be holistically good but on the flipside a police state of a shaming culture and people living in constant fear.
Then another element we discuss is the humilation and schadenfreude we witness and experience when we’re voyeurs.
youtube
The Victorian freak show and witch hunting shaming of others is seemingly embedded in the human psyche. The gratifying pleasure of seeing others suffer is universal amongst human cultures and even more terrifying is the groupthink social pressure of pointing fingers shaming and how normal people become embroiled in the suffering of others. For reference, the Solomon Asch experiment which demonstrated the ease it took for ordinary people to cause suffering to others by social pressure. A sense of “at least it’s not me” when we watch that tragic family on Eastenders or ‘”that’ll teach them” when we see someone getting a ‘rightful punishment’ is incredibly prevalent amongst all of us. But ultimately we are all social creatures and in a way social beings have all adapted to react to each other and live with each other. And that’s what makes this topic of voyeurism so difficult to explain but also ever so interesting.
So we go back to Hitchcock and voyeurism. What Hitchcock does so masterfully is his control of the camera, what the audience is able to see, his long lingering shots in Rear Window - he is essentially questioning us - the audience. We have been the voyeurs in the whole film, in every film and he does this without once breaking the fourth wall - like this great scene https://youtu.be/QRJ38y4Jn6k
Pondering whether we have been the silent observers in a crime - as Edmund Burke said "The only thing necessary for the triumph of evil is for good men to do nothing." Or whether we are wrongful to peep on other’s business, or our regression to a passive state of being a consumer. Hitchcock leaves these questions unanswered as the film ends with countless new questions beginning to be formed and that’s what makes this film one of the very best.
References
https://www.psychologytoday.com/gb/blog/fulfillment-any-age/201305/who-watches-reality-shows-and-why
https://m.youtube.com/watch?v=Tva0xq-eDvI
Schadenfreude
https://m.youtube.com/watch?v=nZzzwpPcuwk
Schmoop
https://www.simplypsychology.org/asch-conformity.html
Asch experiment
https://www.youtube.com/watch?v=3eblA9LqKA8
Black Mirror: White Bear
Thinking Fast and Slow - Daniel Kaheman
So You’ve Been Publicly Shamed - Jon Ronson
youtube
1 note
·
View note
Text
Why do my ears pop?
youtube
o Normally the air pressure is the same in the outer ear and the middle ear. The eardrum provides a seal between the two chambers.
o When flying however, there are fewer air molecules in the atmosphere. Therefore the pressure in the outer ear is lower, but the pressure in the middle ear stays the same.
o Extra pressure in the middle ear pushes more on the eardrum causing it to bulge out - this is the stuffy feeling we experience. As it is stretched, eardrum is unable to transmit sounds normally.
o Techniques such as chewing gum, yawning etc. the Eustachian tube opens so the middle ear can have the same pressure as the aeroplane cabin.
o Air rushing to or from the ear and the eardrum adjusting causes this popping sound.
5 notes
·
View notes
Text
27 Club

Hello, long time no see.
After some thoughts about my blog, I’ve decided to change it up a bit. During my time in medical school, case-based scenarios were a great way to teach us about medical conditions and diagnosis. I’ve found them an interactive and thought probing way to get into the nooks and crannies of a medical case placing yourself in the shoes of the detective.
In this post, I have six cases for the price of one which I have immensely enjoyed investigating and I hope you will too.
So, without further ado, shall we begin?
Case 1: Mr K.C.
A 27 year old man was found dead in his home at 171 Lake Washing Boulevard East in Seattle, Washington, USA on April 8 1994. Forensic analysis determined he had died by a self-inflicted gun shot wound to the head in a suicide attempt three days earlier on April 5 1994.
What investigations would you do for Mr K.C.?
This particular case is a sadly too common scenario for particular young males aged 20-30 who pose the highest risk in any demographic group to commit suicide. Upon establishing that there are no vital signs from Mr K.C. and no signs of life, a medical doctor or paramedic has to confirm his death.
To declare death, a medical doctor has to go to the corpse and do the following:
· Reaction to voice and pain (sternal rub/pressing on supraorbital nerve)
· Pupil reflexes (fixed and dilated – no reaction to light and often with a dry appearance)
· Central pulse for 1 minute (carotid or femoral)
· Heart sounds for 1 minute
· Respiratory effort and sounds (listen for both sides of chest for 30s each side)
This is to gauge that the recently deceased has no response to pain, no pupillary reflex, no pulses present, no heart sounds and no audible breath sounds. Date and time of the declaration of death is needed. It goes without saying this is a very sensitive time for next of kin and family members so this has to be done in a professional and sensitive manner. And although not an urgent task (not a life threatening emergency), it should be stressed a patient cannot be transferred to the mortuary before the declaration of death.
The following afterlife care discussed will be applicable to the UK health system.The next step will be to issue a death certificate, a doctor will need to sign the death certificate to be given to the next of kin or family.
Upon preparing for the funeral services, the funeral director will need to gain two doctors to complete the cremation form, the primary doctor (normally the GP) can complete the first part called Cremation 4, the second part called Cremation 5 has to be done by an independent doctor who must be qualified more than 5 years who must discuss the case with the primary doctor and the next of kin or family (if not nursing staff/nursing home). An independent doctor was required by law to complete the cremation form after the murders of Dr Harold Shipman to hundreds of his patients. If there is no next of kin, every council will have a designated member to talk with the independent doctor.
Who is Mr K.C?
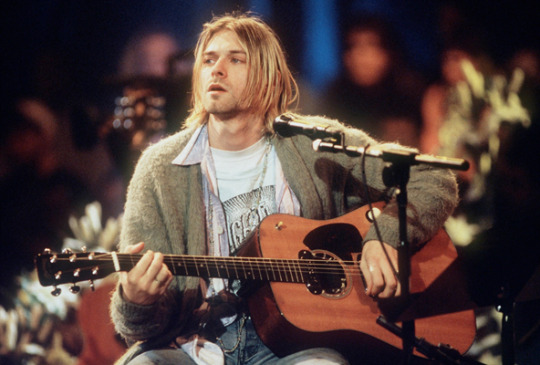
I'd rather be hated for who I am, than loved for who I am not.
Kurt Cobain (February 20, 1967 – April 5, 1994) was the lead singer of the Seattle band, Nirvana whose teenage angst-ridden grunge brought the genre to the mainstream and defined a generation’s rebellion, anger and apathy in the 90s. He was the very definition of cool – not in a suave, Hollywood type of way but in a ‘whatever’ kind of way. He brought a sense of a Rockstar back to childhood neighbourhoods following from the flashy baroque 80s rock and a sense of rebellion back to music. I met an avid Kurt Cobain fan on a coach on the way back from Liverpool who had repeatedly shown me Kurt Cobain covers of Beatles songs which I later realised that John Lennon had been a huge influence on the young frontman of Nirvana. According to the now frontman of the Foo Fighters, David Grohl and the then Nirvana drummer; Kurt Cobain approached his song writing with music first, lyrics second. He often dismissed the relevance of his lyrics yet many of them reveal the sensitivity of the young man bruised by the world – his parents had divorced at the age of 9 which led to him becoming withdrawn from the happy child he was. His musical influences range from radio pop to punk rock to heavy metal whilst he gained artistic inspiration from a range of different books and religions where Nirvana comes from the Buddhist concept of enlightenment. As with the other members of the 27 Club, he was an incredibly complicated figure who was full of contradictions and whose artistic talent spoke to the disenchanted youth of his time. He was also burdened with several medical conditions such as chronic bronchiolitis, depression, and an undiagnosed chronic stomach condition. Kurt Cobain had difficulties with substance abuse which ranged from alcohol, heroin, acid etc. which culminated in his suicide attempts after rehab. His suicide note reveals the extent of his depression and self-hatred which was addressed to his childhood imaginary friend, Boddah.
Case 1 Questions:
What are the risk factors for suicide?
· Mental illness – major depression (increases risk by 20x) and bipolar disorder
· Being Male (3x more likely than being female)
· Previous attempts (increases risk by 40x) and self-harm
· Substance abuse
· Family History
What are the questions asked to assess suicidal risk?
· First and foremost, it is important to assess the patient’s mood – whether they are depressed or suffering from any psychiatric disorders since this undoubtedly will be the biggest risk factor for them.
· Attempt of suicide? Overdose, cutting, burning, attempted hanging – was this planned or impulsive? Have you done this before? Did you think this would kill you? (some suicidal attempts are designed to be non-fatal in an attempt for a cry for help) What was going through your mind at the time?
· Any final acts – such as a suicidal note, will, tying up loose ends such as energy companies
· Precautions taken against discovery? Closing curtain, locking doors, waiting until alone at home etc.
· Alcohol use – amount, strength, previous use
· What did you do after? Did you call anyone – family, friends, 999? (Some patients immediately become regretful and don’t want to die especially in an impulsive suicide attempt. How do you feel about the attempt now? Do you regret it? Do you still feel like you want to take your own life? If you go home now, what will you do? (and the days after) If you feel like this again, what might you do differently? Protective factors – do you have any family members and friends etc. Is there anything to live for? What might prevent you from doing this again in the future? Will you accept treatment?
· Past psychiatric history, past medical history, drug history – antipsychotics, recreational drugs, family history, social history – who are you living with? Where are you currently living? Do you have a good support network? Are you able to carry out your Activities of Daily Living (ADLs)? Do you have children? – neglect, witnessing the episodes, harm towards children? What is your current occupation? Do you have any financial worries?
What are the cardinal symptoms of depression?
· Anhedonia (lack of pleasure doing things they normally enjoy doing)
· Low mood
· Fatigue
· All symptoms lasting more than 2 weeks
What is Section 2, Section 3, Section 4, Section 5(2) and Section 136 of the Mental Health Act 1983?
· Section 2 is designed for Approved Mental Health Professional (AMHP) to assess a patient’s mental disorder in a hospital setting where a patient is detained under a legal framework which lasts up to 28 days. For sectioning a patient, two doctors are required to assess them – one who is Section 12 approved such as a psychiatrist and the other who is normally the patient’s GP.
· Section 3 is designed for Approved Mental Health Professional to treat a patient’s mental disorder in a hospital setting where a patient is detained under a legal framework which lasts up to 6 months and can be renewed.
· Section 4 is an assessment of mental disorder in cases of emergency – patients must stay in hospital for 72 hours so they can be assessed by two doctors.
· Section 5(2) is an assessment of mental disorder for inpatients in a hospital setting where the patients must stay for up to 72 hours to be seen by two doctors to decide if they need to remain in hospital for longer. Section 5(4) lasts up to six hours and is instigated by a mental health nurse who deems the patient to be mentally unwell for discharge.
· Section 136 is the police removal of a patient deemed to have a mental disorder from a public place to a place of safety – such as a hospital.
What is sectioning and when do you section someone?
Sectioning is being kept in a hospital under the Mental Health Act 1983. A patient with a mental disorder is sectioned when they are deemed to be a harm to themselves or a harm to others. It allows the treatment of the mental illness without their consent.
Case 2: Miss A.W.
A 27 year old woman was found dead in her Camden flat on July 23 2011, the cause of death was attributed to alcohol poisoning.
What investigations would you do for Miss A.W.?
Primary Survey (first steps you do in a medical emergency): DR ABC (Danger, Response, (call for help) Airway, Breathing, Circulation) - can also be expanded to DEFG (Disability, Environment, Fluids, Glucose - Don’t Ever Forget Glucose)
Gain IV access
Monitor basic observations (O2 saturation, Blood Pressure, Temperature, HR, RR)
Gain ECG
Bloods
Full Blood Count (Red Blood Cells, White Blood Cells (neutrophils, lymphocytes, monocytes, eosinophils, basophils), Haemoglobin, Haematocrit, Mean Corpuscular Volume, Mean Corpuscular Haemoglobin, Mean Corpuscular Haemoglobin Concentration, Red Cell Distribution and Platelets.
Urea and Electrolytes (Na+, K+, HCO3-, Creatinine, Urea)
Liver Function Tests (ALP, ALT, AST, GGT, Bilirubin)
Venous Blood Gas
Arterial Blood Gas?
C-Reactive Protein (CRP)
Erythrocyte Sedimentation Rate (ESR)
Lactate
Blood Cultures?
Who is Miss A.W?

We only said goodbye with words
I died a hundred times
You go back to her
And I go back to black
Amy Winehouse (14 September 1983 – 23 July 2011) is the most recent member of the 27 Club in this post. I remember hearing hear voice in the radio years back and mistakenly believing to be a goldie oldie singer only to be informed that it was in fact Amy Winehouse, a contemporary pop artist. She emerged when I really believe British pop music was of musical merit and it hasn’t reached the heights it did back then. Of course, she was plagued by her own personal troubles which plastered the pages of the notorious British media and hounded by the paparazzi. These troubles made themselves into her songs which ranged from topics of drug addiction and broken relationships. It was an intoxicating mix, she was the very embodiment of the tragic musician where news of her death did not come as a surprise. Her name was repeatedly shown in the tabloids with new revelations of crack cocaine, heroin, ecstasy, ketamine and alcohol addiction as well as violent conduct which only served to solidify a caricature painted by the tabloids. Her mental health was shared by her quite openly such as her depression and eating disorders and stated she was a manic depressive. Her drug usage – particularly crack cocaine had led to further complications such as emphysema and atrial fibrillation. A decade back, our understanding of mental health in society was primitive and led to ridiculous tabloid headlines – for instance does anyone remember ‘Wacko Jacko’ describing Michael Jackson? On numerous occasions she was hospitalised for her substance abuse which came during her highest achievements as an artist sweeping the Brit Awards and Grammy Awards. In fact, listening to a friend who was working as a waiter during a private show where Amy Winehouse was due to perform said there were doubts whether she would turn up – she did but in a heavily intoxicated state – then there were doubts as to whether she’d be able to perform. And to everybody’s surprise – she smashed it. Those stories and the media sensation that followed her add a myth like quality to her where you realise that in this world there won’t be another that can match her talent and voice, not even Adele. The documentary, Amy directed by Asif Kapadia furthers this tragic story of Amy Winehouse which I’d highly recommend watching to understand more about her. Her death was reported by the coroner to be accidental alcohol poisoning, her blood alcohol levels were five times higher than the legal drink driving limit which is 0.08% Blood Alcohol Content (Amy Winehouse’s BAC was 0.416%.
Case 2 Questions:
What is the medical management for someone who has overdosed on alcohol?
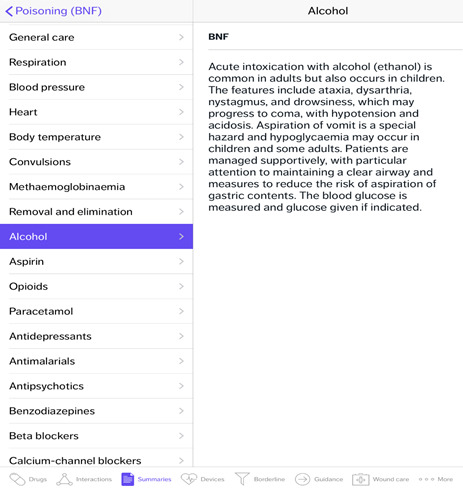
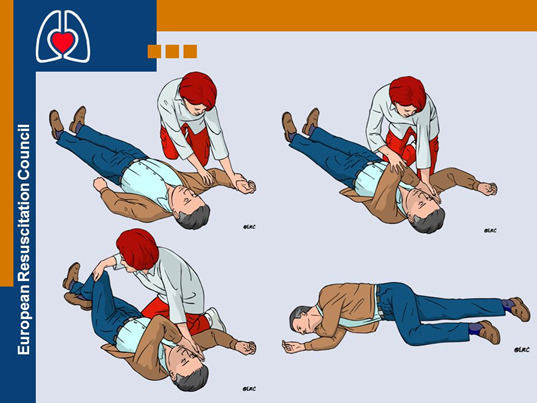
As seen in the British National Formulary (BNF) guidelines, the first thing to do is to take an DR ABCDE approach where these patients are prone to losing the patency of their airway especially if they are unconscious and have lost their gag reflex. Placing them in the recovery position will be key to maintaining the patency of their airway in this case.
What are the signs of alcohol intoxication?
youtube
Mild: Mild sedation, decreased coordination
Moderate: Slurred speech, trouble walking, vomiting
Severe: Decreased effort to breathe, coma
What drugs can be used for alcohol rehabilitation?
· Naltrexone - µ opioid receptor antagonist, blocks euphoric effects
· Acamprosate, reinstates neurotransmitter pathways after acute alcohol withdrawal
· Disulfiram, inhibits acetaldehyde dehydrogenase – causes hangover effect immediately
What is delirium tremens and Wernicke-Korsakoff syndrome?
Delirium tremens is a severe form of alcohol withdrawal around 3 days into withdrawal and lasts for 2-3 days. Symptoms include shaking, shivering, irregular heartbeat, sweating and occasionally high temperatures and seizures. Benzodiazepines are used to treat delirium tremens.
Wernicke-Korsakoff syndrome is found in chronic alcoholics and comprises of the presence of both Wernicke’s encephalopathy and Korsakoff’s syndrome. The cause is Vitamin B1 deficiency (thiamine) and treatment is replenishing the deficiency. Alongside the classical symptoms seen in each disorder, WKS presents with confabulation which is the production of fabricated, distorted or misinterpreted memories about oneself or the world. Wernicke’s encephalopathy presents with the classical triad of ophthalmoplegia, ataxia and confusion.
KS is described as an acute onset of severe memory impairment without any dysfunction in intellectual abilities.The DSM IV lists the following criteria for the diagnosis of alcoholic Korsakoff syndrome:
1. anterograde amnesia
2. Variable presentation of retrograde amnesia
One of:
1. Aphasia
2. Apraxia
3. Agnosia
4. A deficit in executive functions
Alcoholics may have thiamine deficiency because of the following:
· Inadequate nutritional intake: Alcoholics tend to intake less than the recommended amount of thiamine.
· Decreased uptake of thiamine from the GI tract: Active transport of thiamine into enterocytes is disturbed during acute alcohol exposure.
· Liver thiamine stores are reduced due to hepatic steatosis or fibrosis.
· Impaired thiamine utilization: Magnesium, which is required for the binding of thiamine to thiamine-using enzymes within the cell, is also deficient due to chronic alcohol consumption. The inefficient utilization of any thiamine that does reach the cells will further exacerbate the thiamine deficiency.
· Ethanol per se inhibits thiamine transport in the gastrointestinal system and blocks phosphorylation of thiamine to its cofactor form (ThDP).
Case 3 and 4
Miss J.J and Mr J.H
A 27 year old woman was found dead in the Landmark Motor Hotel by her manager on October 4 1970, Hollywood with an official cause of death attributed to heroin overdose and deemed to have died the night previously.
A 27 year old man was pronounced dead at St Mary’s Abbots Hospital at 12:45p.m. on September 18 1970 following an ambulance transfer from the Samarkand Hotel, 22 Lansdowne Crescent, Notting Hill. The post mortem determined the cause of death was aspiration on his own vomit and asphyxiation while intoxicated with barbiturates.
These two cases are grouped together as they both deal with recreational drug overdose.
What investigations would you order?
As mentioned in the cases before you’ve probably noticed a trend. With any medical emergency you have to start with the basic principles – after all genius is simplicity. And that means doing a primary survey (DR ABCDE) to gauge the severity of the medical emergency – whether the patient is in a life threatening state. Airway always kills before Circulation for instance.
Alongside Circulation assessment with fluid resuscitation and ECG monitoring - recreational drugs can cause rhythm abnormalities. It is also important to do a drug screen as to what drugs they consumed then to send off to microbiology and pharmacy. This is important as there are different management options for different drugs and different half lives meaning there may be different metabolisms of the drug and when it begins to take effect. It is also important to get a full clerking (history and examination) this may not be possible from the patient given that they may be inebriated, therefore gaining a collateral history is essential often by a family, friend, police or paramedic.
Who is Miss J.J?

Freedom's just another word for nothin' left to lose
Nothin', don't mean nothin' hon' if it ain't free, no no
Janis Joplin (January 19, 1943 – October 4, 1970) was the female rebel of the psychedelic rock. She was at the vanguard of her times during the 1960s becoming one of the most prolific female rock stars. She was an incredibly charismatic performer who embodied the hippie movement of her time. She had a difficult childhood with bullying at school which led to her rebelliousness influenced by the Beat poets and the Blues. Even during the early stage of her career she had dabbled in drug use which would lead to her death. She had lost nearly 40kg in weight due to her methamphetamine injections and underwent a brief period of sobriety. Her voice had attracted the attention of the San Francisco psychedelic rock band Big Brother and the Holding Company. During this time she and the band began to increase in profile and had performed in front of the Grateful Dead and Abhay Charanaravinda Bhativedanta Swami Prabhupada, the founder of the Hare Krishna movement. After achieving even more fame, Joplin later left the band and started a new group called the Kozmic Blues Band. It was during this period that she began heavily abusing drugs again and was frequently inebriated in her concerts most notably in Woodstock where she was three sheets to the wind and remarkably pulled through. Joplin was heavily abusing alcohol, cocaine and heroin. Joplin slowly spiralled out of control and on the day before her death, she was snubbed by her friend Peggy Caserta and her 21 year old lover Seth Morgan who had both failed to meet her. Her producer had become concerned after Joplin failed to make a recording session a few days later only to find Joplin had died from a heroin overdose.
Case 3 Questions
What is heroin?
Heroin is a morphine (opiate) based drug where upon injection or snorting, there is a subsequent decrease in subjective feelings of pain and an increase in feelings of pleasure and euphoria.
What are the signs and symptoms of heroin overdose?
Heroin is a potentially lethal drug. Its effects depend on the age and weight of the individual, the amount and purity of the heroin and whether there were any other substances consumed.
· Bluish nails or lips.
· Depressed breathing.
· Weak pulse.
· Pinpoint pupils – classic sign
· Disorientation or delirium.
· Extreme drowsiness.
· Repeated episodes of loss of consciousness.
· Coma.
Other signs and symptoms may involve a closer physical inspection or communication with the user. These include:
· Dry mouth.
· Constipation or spasms of the stomach or intestines.
· Low blood pressure.
Heroin being a drug of the opiate class which are central nervous system depressants – hence they slow down the heart rate and breath. The major threat to life is respiratory depression and hence the DR ABCDE primary survey is essential.
What is the treatment for heroin overdose? Please select the correct option.
· Activated Charcoal
· Naloxone
· Glucagon
· Acetylcysteine
· Haemodialysis
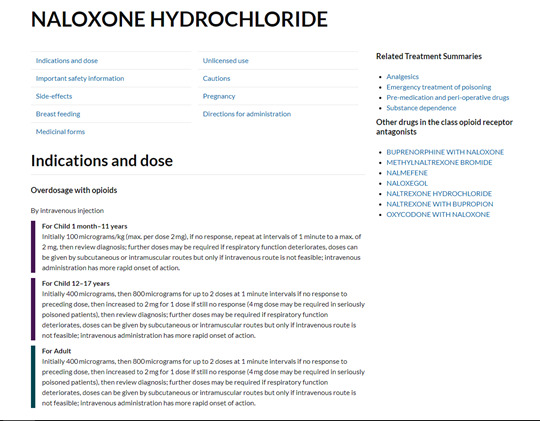
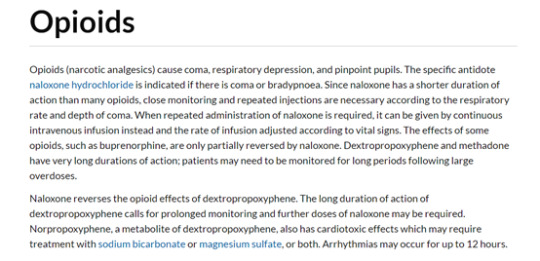
Naloxone is a µ opioid receptor antagonist which blocks the effects of opioids.
youtube
What is cocaine?
Cocaine is a stimulant drug which somewhat has the opposite effects of heroin. The major concern is an arrhythmia which can be rapidly fatal.
What are the effects of cocaine?
Cocaine leads to a high of a dopamine hit, increased alertness, heart rate and euphoria. Cocaine users will become ‘giddy’ – becoming talkative, more energy, restless and more alert etc. The psychological effects include paranoia, anxiety, hallucinations and psychosis.
What the signs and symptoms of cocaine use?
· Arrhythmias (irregular heart rhythm).
· Severe tachycardia (elevated heart rate).
· Very high blood pressure.
· Dangerously high body temperature.
· Sweating.
· Nausea.
· Confusion.
· Severe anxiety or agitation.
· Psychosis.
· Tremors.
· Seizures.
· Stroke.
Another concern is when recreational drugs are mixed together – the whole saying ‘don’t mix your drinks’ applies here since there are different effects at play which means the toxicology will be more complex and hence treatment is more difficult.
Other substances, like cocaine and other stimulant drugs, elicit a physiologic response that somewhat opposes the effects of heroin. Because cocaine, for example, is a stimulant and heroin is a depressant, they create counteracting effects in the body and brain that may make the user less able to sense an impending overdose. However, this combination, commonly referred to as a “speedball,” can be extremely dangerous not only because users are susceptible to the effects of both drugs but also because users may be less aware of heroin’s intoxicating depressant effects and consume higher-than-normal amounts, placing themselves at extreme risk of overdose.
youtube
Who is Mr J.H?
I will be dead in five years’ time, but while I am here, I will travel many highways and I will, of necessity, die at a time when my message of love, peace, and freedom can be shared with people all over the world.
Jimi Hendrix (November 27, 1942 – September 18, 1970) I’m sure needs no introduction. Along Bruce Lee and Steve McQueen he’s the very essence of cool. The first time I heard about Jimi Hendrix was when I was like every other boy learning how to play guitar where you heard rumours of this mystical Rockstar that played the guitar like no other. Although this sounds corny and cliched, I can’t describe my awe listening to Hendrix for the first time. There are great guitarists and then there’s Jimi Hendrix. He quite simply set the benchmark which only he could achieve whilst the rest of us just looked on in amazement. It’s odd when you quite undoubtedly see someone who is unquestionably the best in their field, I don’t think there’s ever been a guitarist like Hendrix who literally transformed the art of the guitar. The closest thing I can compare it to is Miles Davis’ Kind of Blue’s foray into modal jazz. Jimi Hendrix was born James Marshall Hendrix in Seattle, Washington. He was given his big break in England by Linda Keith, the daughter of Alan Keith, a well known disc jockey at the time. And so began his climb to fame where he received a reputation for his live performances which all culminated in his magnum opus Electric Ladyland in 1968 and headlining the Woodstock Festival in 1969. He had popularised the use of the wah-wah board and experimented with the electronic sound pioneering the psychedelic sounds we hear now from heavy metal, hard rock, shoegaze etc. For such a legend whose name is now synonymous with the instrument, Hendrix only gained his guitar at the age of 15 learning the instrument for several hours every day. He had often emulated playing the guitar as a child using a broom, his father had refused to buy him a guitar. His mother had died when he was 16 from a ruptured spleen following liver cirrhosis and his father had refused to take him and his brother to his mother’s funeral – his parents had earlier divorced when he was 9. He had a tumultuous upbringing, only meeting his father when he had returned from his service in the US army and during his childhood his parents both had issues with alcohol which led to several occasions them moving to cheap hotels and his three younger siblings sent to foster families.
Hendrix spent a brief stint in the army where his priorities began to take shape after spending some time in a band. He began to obsess over his guitar which his father had sent other to him, and started neglecting his army duties. He was later honourably discharged on the basis of unsuitability. And quite right, he was forced into the army after being caught in stolen cars and offered the choice between prison or the army. It was after this discharge that Hendrix began to flourish artistically where he learnt how to play the guitar with his teeth, playing the circuit and where he began to form the Jimi Hendrix Experience. What came next was a series of memorable events from releasing Are You Experienced, lighting his guitar on fire to become one of Rock and Roll’s most famous images, Axis: As Bold As Love, Electric Ladyland and finally headlining the Woodstock festival where he performed a memorable rendition of The Star Spangled Banner. This period revealed Hendrix’s perfectionism and attention to detail which were qualities that made him the best. It was also during his climb to fame where he began to descend into his addictions. He had difficulties controlling his drink to which he would have fits of rage, he experimented with a wide range of recreational drugs from cocaine, cannabis, hashish, amphetamines and LSD.
Case 4 Questions
What are barbiturates?
Barbiturates, like opioids are central nervous depressants and have similar side effects. They are used as anxiolytics, hypnotics and anticonvulsants. They work via increasing the efficacy of the GABA transmitter which is an inhibitory neurotransmitter.
What are the signs and symptoms of a barbiturate overdose?
· Impaired judgement.
· Slurred speech.
· Extreme fatigue.
· Poor coordination.
· Shallow breathing.
· Altered consciousness.
· Coma.
· Death.
Complications related to barbiturate overdose may also include:
· Concussions, paralysis, and other injuries resulting from falls or accidents.
· Pneumonia as a result of aspiration of food or fluids into the airways of those with impaired levels of consciousness.
· Miscarriage as a result of damage to the developing fetus.
What is the treatment for barbiturate overdose?
The treatment of barbiturate abuse or overdose is generally supportive. The amount of support required depends on the person's symptoms. If the patient is drowsy but awake and can swallow and breathe without difficulty, the treatment can be as simple as monitoring the person closely. If the person is not breathing, it may involve mechanical ventilation until the drug has worn off.
Supportive treatment often includes the following:
· Activated charcoal may be given via nasogastric tube.
· Intravenous administration of saline, naloxone, thiamine, and/or glucose.
· Intubation and bemegride, or a hand-breather where these are not available until the patient can breathe under their own power.
· Observation in the Emergency Department for a number of hours or admission to the hospital for several days of observation if symptoms are severe.
· Advise the patient about drug misuse or refer for psychiatric consult.
What is serotonin syndrome?
Serotonin syndrome is a medical emergency where upon use of a mixture of certain serotonergic medications such as Selective serotonin reuptake inhibitors (SSRI), serotonin norepinephrine reuptake inhibitors (SNRI), monoamine oxidase inhibitors (MAOI), tricyclic antidepressants (TCAs), amphetamines, pethidine (meperidine), tramadol, dextromethorphan, ondansetron, cocaine etc. The severity of symptoms range from mild to severe and include high body temperature, agitation, increased reflexes, tremor, sweating, dilated pupils, and diarrhea. Body temperature can increase to greater than 41.1 °C (106.0 °F). Complications may include seizures and extensive muscle breakdown.
What is the treatment for serotonin syndrome? Please choose from the following options
· Barbiturates
· Benzodiazepines
· Glucagon
· Acetylcysteine
· Naloxone
· Removal of the offending agent or interacting drugs. In cases of recent ingestion/large overdose, activated charcoal may help to prevent absorption. Supportive measures such as IV fluids and control of agitation with benzodiazepines are also used.
· Mild cases usually resolve within 24 hours of discontinuation and may need supportive measures only. Beware of drugs with long half-lives or active metabolic breakdown products (for example, fluoxetine), where it may take longer.
· Moderately severe cases should have cardiovascular and thermal disturbances corrected and receive 5-HT2A antagonists such as cyproheptadine (as yet there is no definitive evidence for its efficacy).
· Severe cases need aggressive treatment and intensive care with early sedation, neuromuscular paralysis and ventilatory support.
· In the UK, advice for health professionals is available from the Toxbase® website.
What is neuroleptic malignant syndrome?
Neuroleptic malignant syndrome has symptoms similar to serotonin syndrome though the offending drugs are not serotoninergic but rather as its name suggests – neuroleptics which are antipsychotic drugs. Complications include rhabdomyolysis, hyperkalemia, kidney failure and seizures. Instead of serotonin, the neurotransmitter in regard is dopamine and hence the treatment is with dopamine agonists such as bromocriptine. Dantrolene is also used to control malignant hyperthermia and muscle rigidity. Benzodiazepines are also necessary for treatment of agitation.
Case 5 and 6
Mr J.M and Mr B.J
A 27 year old man was found dead in his bathtub on July 3 1971 by his girlfriend in his apartment in the 4th arrondissement of Paris. The official cause of death was listed as heart failure.
A 27 year old man was found dead in the bottom of his swimming pool in the night of 2-3 July 1969 by his girlfriend. His official cause of death was reported to be death by misadventure with autopsy presenting liver and heart enlargement due to alcohol and drug abuse.
These two cases are grouped together due to death by drowning.
Who is Mr J.M?
People are afraid of themselves, of their own reality; their feelings most of all. People talk about how great love is, but that’s bullshit. Love hurts. Feelings are disturbing. People are taught that pain is evil and dangerous. How can they deal with love if they’re afraid to feel? Pain is meant to wake us up. People try to hide their pain. But they’re wrong. Pain is something to carry, like a radio. You feel your strength in the experience of pain. It’s all in how you carry it. That’s what matters. Pain is a feeling. Your feelings are a part of you. Your own reality. If you feel ashamed of them, and hide them, you’re letting society destroy your reality. You should stand up for your right to feel your pain.
Jim Morrison (December 8, 1943 – July 3, 1971) was the prolific front man of the band, The Doors. If we had to summarise Jim Morrison, he would be the intellectual man of psychedelia. The band’s name was taken from Aldous Huxley’s The Doors of Perception (which in itself takes its name from William Blake’s poem The Marriage of Heaven and Hell) where the author describes a drug trip on mescaline – a drug similar to LSD. And indeed Morrison’s persona would take on this vein, the poetic lyrics, wild character, accompanied with the woozy sounds of psychedelic rock was a recipe for groundbreaking evolvement in music. He had other names – Mr Mojo Risin’ (an anagram of Jim Morrison) and The Lizard King – which is immortalized in Lisa Simpson’s parody in The Simpsons.
He was plagued by alcohol dependency throughout his life – causing a Jekyll and Hyde type split between erudite poet and wild Rockstar, which furthered his reputation as the doomed rock poet. With leather pants becoming vogue and inspiring future stars such as Iggy Pop, it was Morrison’s intelligence and wide reaching artistic influences that made him such a towering figure where studied various types of literature, film and cinematography in UCLA, and his upbringing being part of a naval family constantly on the move with a fractured education all culminated in a completely unique voice. It was this that allowed him to one of the leading figures of the Hippie counterculture. And this came with his tumultuous sexual relationships with groupies and his long term girlfriend, Pamela Courson who later found him in his death in his bathtub. His death was later confirmed due to heart failure, but since no autopsy was performed there have been several lingering theories that can never be proven ranging from murder, overdose, suicide etc. Jim Morrison’s death was as enigmatic as his art which was given a new layer upon uncovering a collection of poems which were subsequently named Paris Journal which can be interpreted in a wildly array of meanings and allude to overdose or suicide. The scans of the poems can be found here: https://recordmecca.com/products-page/museum-quality-collectibles/jim-morrison-paris-journal-1971-manuscript-handwritten-paris-notebook-the-doors/
Who was Mr B.J?
Pleased to meet you
Hope you guessed my name, oh yeah
But what's puzzling you is the nature of my game, oh baby
Brian Jones (28 February 1942 – 3 July 1969) was the guitarist and founder of the Rolling Stones. Despite not being one of the names you’d associate with the band – Mick Jagger, Keith Richards, Mick Jones etc. Brian Jones is still widely celebrated in rock music for his influence in forming the Rolling Stones – choosing the name on a whim after a Muddy Waters song Rollin’ Stone Blues Brian Jones had next to him when talking to a vendor on the telephone. Brian Jones was in every essence a Rockstar – by the time he formed the Rolling Stones, he already had three children, he was instrumental in pushing the band to his image and the blues sound of the early Rolling Stones. In many ways he was similar to the other members of the 27 Club with a mercurial personality – shy and introverted one moment to gregarious and extraverted the next. He could be difficult, he had created friction with his bandmates where he had given himself the role of leader and paid himself a cut above the rest which did not sit well with the others. Upon The Rolling Stones gaining their new manager, Andrew Loog Oldham, Jones was marginalized in favour of the more flamboyant Mick Jagger. Being pushed away from his leadership roles and not being able to contribute in the songwriting like Jagger/Richards were able to, he began to descend into drug addiction. He was found in possession of marijuana, cocaine and methamphetamine in his flat. He became alienated and the situation became worsened when his girlfriend of two years, Anita Pallenberg left him for Keith Richards. As the band’s reputation grew, Jones became more and more withdrawn and eventually he was visited by Jagger, Richards and Watts that the band would continue without him. He was later found in the bottom of his swimming pool in Sussex, his death was proclaimed as death by misadventure. Despite this there have been lingering theories including one that he was murdered by a builder, Frank Thorogood which has been adapted into a film. Brian Jones has a distinct connection with Jimi Hendrix and Jim Morrison, other members of the 27 Club with Hendrix dedicating a song to him on US television and Morrison publishing a poem ‘Ode to L.A. While Thinking of Brian Jones’. Both of whom would die in the subsequent two years after Jones’ death.
Case 5 and 6 Questions
What is the first aid for someone who has drowned?
With a Primary Survey (DR ABCDE) to gauge whether Cardiopulmonary Resuscitation (CPR) is needed or not.
• As soon as the casualty has been rescued from the water, check if they’re breathing.
• Ask someone to call 999 or 112 for medical help.
• If the person is unresponsive and not breathing, give them five initial rescue breaths before starting CPR.
• Once you’ve done this, start CPR: 30 chest compressions, then two rescue breaths. Keep giving CPR until help arrives, the casualty regains responsiveness, or you’re too exhausted to keep going.
• If they start breathing again at any time, treat them for hypothermia by covering them with warm clothes and blankets. If they recover completely, replace their wet clothes with dry ones.
• Keep checking breathing, pulse and level of response until help arrives.
https://www.firstaidtrainingcooperative.co.uk/how-to-perform-cpr-on-a-drowning-casualty/
https://www.youtube.com/watch?v=v1YrU55ACbE&t=162s
All of these individuals were famous musicians that changed the music industry in their own ways and are now forever young given their premature deaths at the age of 27. This collective known as the 27 Club is one of the everlasting urban legends and mysteries of music history alongside Paul is Dead, Elvis Presley’s death etc. with the individual deaths being shrouded in some sort of supernatural folklore. And yet this myth persists despite a 2011 BMJ report concluded that the 27 Club is ‘unlikely to be a real phenomenon’ with no risk of death limited at the age of 27. But with humans, we should know we’re more superstitious and illogical than we should be with a snappy punchline or simplification that we accept more readily than the real truth – the cause and effect was due to, black cats and a single person changed the whole of history. But this flaw with our tinted lenses on history definitely makes us more interesting as a whole.
With the 27 Club in mind, Jack Kerouac’s famous words encapsulate the very living soul of these young men and women who were rebellious, wild, daring and utterly mad.
the only people for me are the mad ones, the ones who are mad to live, mad to talk, mad to be saved, desirous of everything at the same time, the ones who never yawn or say a commonplace thing, but burn, burn, burn like fabulous yellow roman candles exploding like spiders across the stars and in the middle you see the blue centerlight pop and everybody goes “Awww!”
On the Road – Jack Kerouac
For evidence whether the 27 Club is a genuine phenomenon, please refer to this study by the BMJ which shows that the 27 Club is a mere coincidence but fame increasing the risk of death. So I guess that clears that up.
https://www.bmj.com/press-releases/2011/12/20/27-really-dangerous-age-famous-musicians-retrospective-cohort-study
https://www.bmj.com/content/343/bmj.d7799
References
https://upload.wikimedia.org/wikipedia/commons/5/56/27_club_Graffiti_in_Tel_Aviv.jpg
http://www.feelnumb.com/2011/03/30/kurt-cobain-wore-a-frightwig-shirt-on-mtv-unplugged/
https://www.cygnethealth.co.uk/service-users-carers/mental-health-act/
https://www.mind.org.uk/information-support/legal-rights/sectioning/#.WzvuIdJKiUk
https://patient.info/doctor/suicide-risk-assessment-and-threats-of-suicide
https://slideplayer.com/slide/8323564/
https://www.thenational.ae/arts-culture/the-short-life-and-enduring-legacy-of-janis-joplin-1.126319
https://www.amazon.com/Hendrix-Poster-Concert-Playing-Guitar/dp/B01DE7QPR2
https://drugabuse.com/library/heroin-overdose/
https://drugabuse.com/library/barbiturate-overdose/#signs-and-symptoms-of-a-barbiturate-overdose
https://patient.info/doctor/serotonin-syndrome#nav-5
http://allthatsinteresting.com/jim-morrison-death
https://www.rollingstone.com/music/music-news/obituary-brian-jones-189861/
0 notes
Text
Being Mortal | When Breath Becomes Air | How We Die
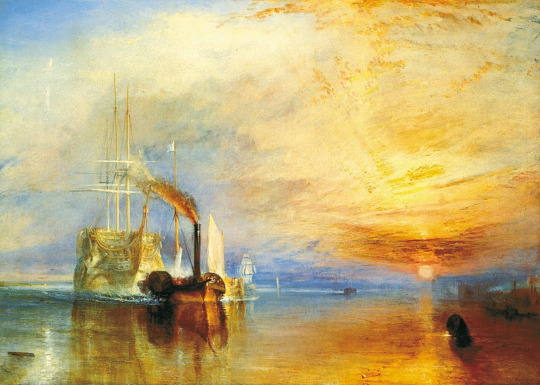
The Fighting Temeraire - J.M.W. Turner
Introduction
Prelude III: Mortality – Santiago Wu
At the break of dawn begins a new day,
Now I am one with the world,
To be part of something greater, I pray.
All of us part of the same mystery unfurled.
Time past and time future,
Everything that came before,
To everything that follows.
All my love to long ago,
And my hopes for days to come.
Heart selfless, soul mindful.
Live, laugh, love —this the meaning of life?
My candle burns at both ends.
All the places I’ll never see,
All the people I’ll never know.
This might be how it ends.
Memento Mori - Remember that you have to die.

Vanitas – Philippe de Champaigne
Death is inextricably entwined with life, hidden in the shadows patiently waiting to take us on the day we take our last breath.
Reading the accounts of dying men and women is truly humbling, whether it be in their twilight years or prematurely - death comes for all of us. All their stories and memories of human life and emotion: all the joy, love, laughter, tragedy, sorrow and regret willing us all to live more fulfilling, meaningful lives.
If I were a writer of books, I would compile a register, with a comment, of the various deaths of men: he who should teach men to die would at the same time teach them to live.
That to Study Philosophy is to Learn to Die – Michel de Montaigne
I think you always know the moment when you finish a book whilst digesting the last words and the text as a whole, its impact and importance in your personal life. The books I am writing about all discuss mortality – a taboo topic normally hushed about and swept underneath carpets. To read and understand the writings of these books in such a raw and honest fashion was a welcome albeit overwhelming change in gear. These books have had a massive impact personally and have formed an epoch in my life and attitudes to life and death. Being Mortal by Atul Gawande When Breath Becomes Air by Paul Kalanithi and How We Die by Sherwin Nuland are books which have the rare privilege of being read more than once, truly understood, annotated to grasp every fragment of detail of wisdom shared in their pages. The authors are doctors (American surgeons, all sons of immigrants). These men had the privilege and the burden of looking after and treating people with fatal illness in their daily practice. Their accounts are beautifully written, one from the perspective of a doctor looking after patients in their end of life and the other written as a patient facing his own death and one written in his twilight years recounting his medical practice and patients and sickness and death. I have heavily quoted all three books because I believe they offer profound wisdom which is literally life-affirming, in fact I have written this for myself as much as my reader in order to truly understand the essence of the lessons of what these three books and their themes can teach us.
I was first introduced to Atul Gawande from the 2014 Reith Lectures on BBC Radio 4 which were a series of four excellently given speeches on life, death and medicine. His deep research on medicine for the dying draws upon many different threads with a surgical precision. His striving to be better and to constantly improve is remarkable and sets a paragon of medical practice. I was humbled by his admissions and failures and his striving to be a better surgeon. The lectures provided a grounding to my burgeoning clinical experience and taught me to never take anything for granted – never to be complacent of my abilities because to have another human being’s life in your hands is a huge privilege which some say is playing god with a small ‘g’. He understands the fine line between offering false hope and deciding when to cut your losses which is never a clear choice. I immediately related to Paul Kalanithi’s love of literature. It is rare in medicine to meet someone who loves literature so much – stories of humanity, emotions ranging from highest peak to lowest ebb… I can tell this deep affection directly influenced his writing and indeed his medicine and approach to life. What made him unique was his relentless quest to search for life’s meaning. With his juggling of both art and science, I immediately remembered my own decision for choosing to enter medicine. Art reflects the universe whilst science explains it. Medicine married the two together. Though in modern medicine, science is king – like Paul Kalanithi, I have a strong affection for my first love of literature which I’ve come to realise expresses and sometimes even explains the universe in better ways than science can. Sherwin Nuland’s ground-breaking book How We Die has been mentioned in circles of medical humanities and referenced by Atul Gawande as the quintessential book on the medical viewpoint of death and mortality. It is easy to see why this book, though nearly thirty years old is still as relevant as ever today. The art of medicine has been revolutionised and become more efficient by multiple progressions and innovations in science and technology but at its heart remains the doctor-patient relationship which Sherwin Nuland writes about in a philosophical and humane way. He marries both medical science and the stories of his patients which from a medical point of view was an utter joy to read. Funny how things have changed since 1994 when Sherwin Nuland wrote his book and also how much they remain the same – sobering to know how despite our scientific and technological advances in medicine, our attitude towards death and dying patients is still primitive and myopic. In How We Die, Sherwin Nuland details the most common causes of death in the developed countries: cardiovascular disease, old age, stroke, infection, murder, HIV/AIDS, cancer in individual chapters with case studies based on his own patients or his family members.
The theme of death and mortality explored in these books led me to think a lot about them especially in my early medical career. When I first started this blog, I wrote of great figures in human history that have sadly left us and their medical conditions. From a great fighter to an entrepreneur to a musician, all were unique human beings with different qualities but what united all of them – and also us, is death. Death is something that is often misconstrued in our modern lives, whether we euphemise, sugar-coat or indeed fear it. The old saying of De mortuis nil nisi bonum or ‘Do not speak ill of the dead’ and Requiescat in pace or ‘Rest in Peace’ pervades our lives even today. We feel sadness when great figures die because of the finality of death – there is no return, we will never know what would have come next. We are reminded of our own lives and within our limited time we too are able to achieve something great. Of course, it is foolish to be able to condense every reference and understand them completely, that will take more than a lifetime to study, a Sisyphean task – death and ars moriendi (the art of dying) being perhaps the biggest and most universal theme of human life across all cultures. There are still works by Heidegger, Nietzsche, the Bible, the Tibetan Book of the Dead, I Ching, the Mahabharata, the Vedas, the Quran, countless poets, novelists, philosophers, scientists etc. that I haven't been able to read in this time, this of course is a study over generations upon generations who still are uncertain about the question of death. I cannot answer these questions death poses, there are mountains upon mountains I will need to ascend in order to catch the slightest glimpse of an understanding. I myself cannot even expect to offer the slightest bit of eloquence of my own voice – I elect instead to let great men and women do that for me for may I learn from them and one day pass on this knowledge. After spending the past year contemplating on death and mortality and reading around the topics from great accounts by humanity, I am certain that what this teaches us is the appreciation of life now in the present. None of us knows when we will die, only we know for certain that we will die. In our cycles of time, this is our time on Earth, our time to live. How we come to peace with death and our mortality is focus of these books I have mentioned and the lessons we can all learn from them.
As I child, I had devoured the Roald Dahl books like any other kid in school I loved his dark wit and unpatronizing creativity in his novels where they provided the first forays into my love for books and imagination. One thing always struck me in his books that I never truly understood until my youth, was his motto that preceded each and every one of his novels. I had a much loved, battered double copy of Charlie and the Chocolate Factory & Charlie and the Great Glass Elevator which I had read several times over. The motto that perplexed me well throughout my childhood was:
My candle burns at both ends
it will not last the night.
But oh my foes and ah my friends,
it gives a lovely light!
How apt of Roald Dahl! Even in children's novels he never hid death from them – didn't the twits shrink away into nothingness and didn't James' parents get squashed by a rhinoceros? It's a beautiful motto, the transience and beauty of life condensed into four lines. When I look back over my life, over petty arguments, being let down and hurt by others, showing loved ones my worst side – I am deeply humbled. Life is short, I don't want it to be marred by acrimony and bitterness and regret. Those are the things that don't matter, the bitter pill you stow away at the back of the mind to learn a cruel lesson from and yet cringe at who you could be and hopefully were. There isn't room for such sourness, when you read the accounts of the dying – there is often the bittersweet feeling of regret and missed opportunity as seen in Top Five Regrets of the Dying by Bronnie Ware, a palliative care nurse.
https://www.theguardian.com/lifeandstyle/2012/feb/01/top-five-regrets-of-the-dying
Here we must focus on the important things – the old sayings of ‘letting the little things go’, and ‘don’t sweat the small stuff’ are true. Do we hold a grudge to everybody who has wronged us? If that’s the case then we’d only hold a grudge to everybody because as Bob Marley said “The truth is everyone is going to hurt you. You just got to find the ones suffering for.” Life is too short for all of the pettiness and trivialities. Forgive and love, it’s the best antidote to bitterness and the best steps to self-love for through only loving ourselves can we love others.
Wherever your life ends, it is all there. The utility of living consists not in the length of days, but in the use of time; a man may have lived long, and yet lived but a little. Make use of time while it is present with you. It depends upon your will, and not upon the number of days, to have a sufficient length of life. Is it possible you can imagine never to arrive at the place towards which you are continually going? and yet there is no journey but hath its end. And, if company will make it more pleasant or more easy to you, does not all the world go the self-same way?
That to Study Philosophy is to Learn to Die - Michel de Montaigne
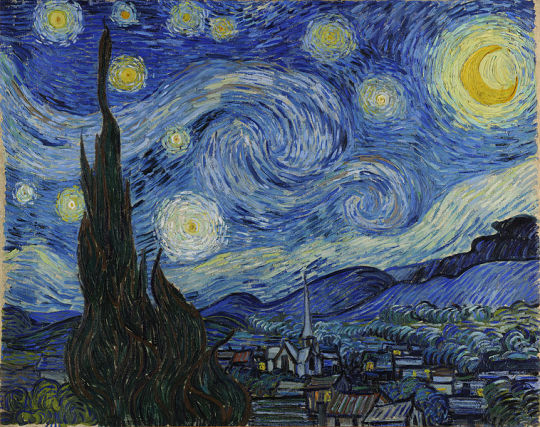
The Starry Night - Vincent Van Gogh
Medicine and death

The Doctor – Sir Luke Fildes
“To me, the subject will be more pathetic than any, terrible perhaps, but yet more beautiful.”
Being mortal is about the struggle to cope with the constraints of our biology, with the limits set by genes and cells and flesh and bone. Medical science has given us remarkable power to push against these limits, and the potential value of this power was a central reason I became a doctor. But again and again, I have seen the damage we in medicine do when we fail to acknowledge that such power is finite and always will be.
We’ve been wrong about what our job is in medicine. We think our job is to ensure health and survival. But really it is larger than that. It is to enable well-being. And well-being is about the reasons one wishes to be alive. Those reasons matter not just at the end of life, or when debility comes, but all along the way. Whenever serious sickness or injury strikes and your body or mind breaks down, the vital questions are the same: What is your understanding of the situation and its potential outcomes? What are your fears and what are your hopes? What are the trade-offs you are willing to make and not willing to make? And what is the course of action that best serves this understanding?
The field of palliative care emerged over recent decades to bring this kind of thinking to the care of dying patients. And the specialty is advancing, bringing the same approach to other seriously ill patients, whether dying or not. This is cause for encouragement. But it is not cause for celebration. That will be warranted only when all clinicians apply such thinking to every person they touch. No separate specialty required.
If to be human is to be limited, then the role of caring professions and institutions – from surgeons to nursing homes – ought to be aiding people in their struggle with those limits. Sometimes we can offer a cure, sometimes only a salve, sometimes not even that. But whatever we can offer, our interventions, and the risks and sacrifices they entail, are justified only if they serve the larger aims of a person’s life. When we forget that, the suffering we inflict can be barbaric. When we remember it the good we do can be breathtaking.
I never expected that among the most meaningful experiences I’d have as a doctor – and, really, as a human being – would come from helping others deal with what medicine cannot do as well as what it can. But it’s proved true, whether with a patient like Jewel Douglass, a friend like Peg Bachelder, or someone I loved as much as my father.
Being Mortal – Atul Gawande p259-260
Having the medical perspective of death is something strangely inhuman. The first death with everyone is upsetting and everyone reacts in their own way. Yet witnessing death on a daily occurrence begins to offset this shock to the system, becoming a routine to which medical professional need to learn how to cope with death. Doctors and nurses in A&E departments don’t stop with each death, rather they move onto the next pressing case to attempt to succeed where they failed before. Paramedics share dark humour about death and gore in order to deal with what they see every day. Porters transporting the recently deceased to the morgue don’t cry over the tragedy. Pathologists inspecting the corpses of patients to determine a cause of death don’t become overwhelmed with grief. This desensitisation to death is a double-edged sword, it allows us to function when it should overwhelm us with grief yet does it detach us from our common human empathy, forgetting or indeed denying to ourselves what it feels like? Indeed, I remember my first deaths I saw as medical student, I have always been too guarded and perhaps too detached to cry but the spectre of death haunted me where I felt its presence after seeing a failed cardiac arrest or whilst on an ambulance shift seeing an old man surrounded by his family slowly stop breathing until there were no more breaths. Often, I have reminisced and dreamt about these experiences, I still remember them freshly and yet I still do not know my own thoughts and feelings on them.
As Atul Gawande shows in the second chapter aptly named Things Fall Apart – named after the Chinua Achebe novel which consequently was named after a line in the W.B. Yeats poem The Second Coming ‘Things fall apart; the centre cannot hold;’ When we look at death as a cross sectional timeline we tend to map it in certain ways.
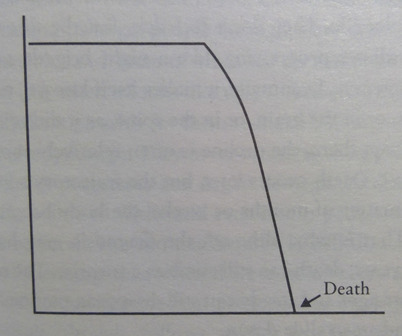
The first is the classic model of how we perceive our lives and death. The classic timeline of good health until old age – when health begins to deteriorate until death.
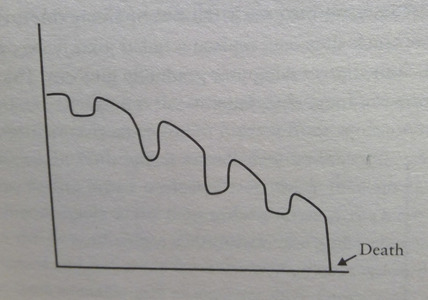
Advances in medical practice have allowed for previous fatal chronic diseases to be treated and hence the ebbing and flowing of improvements and exacerbations in health until senescence takes place. As each second becomes a minute, as each minute becomes an hour, as each hour becomes a day, as each day becomes a month, as each month becomes a year, as each year becomes a decade, we are all ageing with time. Senescence is defined as biological ageing – the gradual deterioration of function. If disease does not take us, then old age surely will.

The third graph Atul Gawande shares with us is the graph of old age, so often medicalised given the plethora of diseases that occur in one’s twilight years. Old age and dying is the primary subject matter of his book where our medical fiddling of patching over the punctures of disease becoming a long, slow fade towards death. How then can we prepare for the inevitable? With every new wrinkle and grey hair, we know we are inching towards old age. With the 150,000 people who die on earth each day, two-thirds are due to old age. In essence, it is a miracle that medical progress has taken us this far, as proposed by Abdul Omran an epidemiologist, quoted by Dr Jonathan Reiner in Dick Cheney’s book Heart, there are three progressive stages of population longevity in the USA: age of pestilence and famine, age of receding pandemics, the age of degenerative and man-made diseases. In our modern age, instead of infectious diseases being the predominant source of mortality in developed countries with the dawn of scientific breakthroughs such as vaccinations and nutritional improvements, this modern post-industrial age presents itself with ischaemic heart disease as the number one most common fatal disease – our new sedentary, calorific lives alongside the meddling of tobacco companies have surely contributed to this. Indeed, as Montaigne wrote in the late sixteenth century. “To die of age is a rare, singular, and extraordinary death, and so much less natural than others: it is the last and extremest kind of dying”. During Montaigne’s time the average life expectancy was nothing to the years we clock up in our modern times with the average age of death now in the UK as 81.60 years.
DNAR stands for Do Not Attempt Resuscitation, it is a form filled out that I have seen in hospitals for patients who are approaching the end of their life or if they are about to have a high risk procedure. The number of times I have seen the form filled out is countless and seeing it from the doctor's perspective as a medical necessity but seeing it from the, often, elderly patient's perspective you note a sign of resignation, fear and sadness. For these patients, they are forced to confront with what might be the end. Patients who are dying will often grieve over their borrowed time left.
The desensitisation of the significance of death from being in the medical field is an odd feeling. When something becomes routine, we become normalised to it. Countless times I have seen doctors and nurses, sign away the paperwork and send the patient to the morgue. My first time seeing someone die was indeed difficult – a cardiac arrest but there’s now a commonplace lack of novelty around death I have often wondered if I was losing my humanity.
I had started in this career, in part, to pursue death: to grasp it, unclear it, and see it eye-to-eye, unblinking. Neurosurgery attracted me as much for its intertwining of brain and consciousness as for its intertwining of life and death. I had thought that a life spent in the space between the two would grant me not merely a stage for compassionate action but an elevation of my own being: getting as far away from petty materialism, from self-important trivia, getting right there, to truly life-and-death decisions and struggles… surely a kind of transcendence would be found there?
But in residency, something else was gradually unfolding. In the midst of this barrage of head injuries, I began to suspect that being so close to the fiery light of such moments only blinded me to their nature, like trying to learn astronomy by staring directly at the sun. I was not yet with patients in their pivotal moments, I was merely at those pivotal moments. I observed a lot of suffering; worse, I became inured to it. Drowning, even in blood, one adapts, learns to afloat, to swim, even to enjoy life, bonding with the nurses, doctors, and others who are clinging to the same raft, caught in the same tide.
When Breath Becomes Air P80-2
This level of detachment I see from colleagues is understandable when we realise the alternative is to open ourselves up to our patients’ pain where we share their grief and predicament. The sheer heat of emotions we experience will also cloud our judgement that we may not be able to serve others who need our care in the best possible way. I remember a session on being taught ‘breaking bad news’ to patients where one horror story came from the doctor breaking down in front his patient and was in turn comforted by the very person he was meant to comfort. The abode to be cruel to be kind is commonplace in medicine, administering a vaccination to a young child, inserting needles to take blood from patients, using scalpels to open the flesh in surgery. There’s a lot of pain in medicine and being swamped and desensitised to it, to an outsider looking in, may see us as cold or inhuman. Indeed, I believed that too as a young medical student but now I realise, it’s just the only human response we can have.
But it is so very difficult to tell your patient that there is nothing more that can be done, that there is no hope left, that it is time to die. And then there is always the fear that you might be wrong, that maybe the patient is right to hope against hope, to hope for a miracle, and maybe you should operate one more time. It can become a sort of folie à deux, where both doctor and patient cannot bear reality.
…
I have learned over the years that when ‘breaking bad news’ as it is called, it is probably best to speak as little as possible. These conversations, by their very nature, are slow and painful and I must overcome my urge to talk and talk to fill the sad silence.
…
I drove away in a turmoil of confused emotions. I quickly became stuck in the rush-hour traffic, and furiously cursed the cars and their drivers as though it was their fault that this good and noble man should die and leave his wife a widow and his young children fatherless. I shouted and cried and stupidly hit the steering wheel with my fists. And I felt shame, not at my failure to save his life – his treatment had been as good as it could be – but at my loss of professional detachment and what felt like the vulgarity of my distress compared to his composure and his family’s suffering, to which I could only bear impotent witness.
Do No Harm – Henry Marsh P151-3
It is a horrible feeling, that somebody’s life is ruined and is at its near end, but we still have patients to treat, our own lives to lead and life goes on…That is the burden of our professional detachment. It’s a delicate fine line to balance upon, I do not suspect that doctors signing DNAR forms find it easy – whether they empathise with the patient’s resignation or whether they are starkly reminded of their own mortality. It is never easy, but the only way is to keep moving forward.
In the medical field, we have the enormous privilege of being with our patients in their lives from cradle to grave – at their strongest but also at their weakest, where the fear of their lives are in our hands. We are bound by a sacred confidentiality to protect our patients and our duty upheld by the four pillars of ethics: respect for autonomy, benevolence, non-maleficence and justice.
Sometimes it is forgotten the fear of what patients go through whether it be a simple medication, routine operation, or terminal diagnosis. The Kübler-Ross model is an oversimplified form of the stages of grief that patients will go through when faced with a terminal diagnosis though not necessarily in this order:
Denial
Anger
Bargaining
Depression
Acceptance
Although oversimplified, the stages give an indication and ballpark figure to gauge what emotions patients are feeling during this difficult time. This is a difficult time for all involved, one of the most if not the most testing time in our lives. This is because we are confronted the cruel finality of death. There won’t be another story following this, this is it – the final chapter. Atul Gawande interviews various medical professionals working in the field of palliative care – the specialty of terminal end of life care. Both Atul Gawande and Paul Kalanithi mention how doctors can bombard patients with information in order to provide informed consent – as both authors say “Doctor informative”, yet both realise the limitations of this approach where the anxiety of patients can be exacerbated by flooding of information when they still do not know how to compute the diagnosis just given.
The options overwhelmed her. They all sounded terrifying. She didn’t know what to do. I realized with shame, that I’d reverted back to being Dr Informative – here are the facts and figures; what do you want to do? So I stepped back and asked the questions I’d asked my father: What were her biggest fears and concerns? What goals were most important to her? What trade-offs was she willing to make, and what ones was she not?
Not everyone is able to answer such questions, but she did. She said she wanted to be without pain, nausea, or vomiting. She wanted to eat. Most of all, she wanted to get back on her feet. Her biggest fear was that she wouldn’t be able to live life again and enjoy it – that she wouldn’t be able to return home and be with the people she loved.
As for what trade-offs she was willing to make, what sacrifices she was willing to endure now for the possibility of more time later, “Not a lot,” she said. Her perspective on time was shifting, focusing her on the present and those closest to her. She told me uppermost in her mind was a wedding that weekend that she was desperate not to miss. “Arthur’s brother is marrying my best friend,” she said. She’d set them up on their first date. Now the wedding was just two days away, on Saturday at 1:00 p.m. “It’s the best thing,” she said. Her husband was going to be the ring bearer. She was supposed to be a bridesmaid. She was willing to do anything to be there, she said.
The direction suddenly became clear. Chemotherapy had only a slim chance of improving her current situation and it came at substantial cost to the time she had now. An operation would never let her get to the wedding, either. So we made a plan to see if we could get her there. We’d have her come back afterward to decide on the next steps.
Being Mortal P234-5
In medicine, the aim is to minimise mortality. We aim to stay up to date with research and novel techniques in order to gain a more positive outcome for all of our patients through the use of scientific data. The Kaplan-Meier curve is an estimator of survival from lifetime data. It is used in medical research, it is used to measure the fraction of patients living for a certain amount of time after treatment. In both Being Mortal and When Breath Becomes Air, the Kaplan-Meier curve was referenced citing both its usefulness but also, its limitations. The Kaplan-Meier curve is purely an estimator and the trends it gives are too general for individual cases. For instance, who's to say that our patients will not fall in the unlucky few that the trend ignores? As seen in Paul Kalanithi's account:
The word hope first appeared in English about a thousand years ago, denoting some combination of confidence and desire. But what I desired – life – was not wat I was confident about – death. When I talked about hope, then, did I really mean, “Leave some room for unfounded desire?” No. Medical statistics not only describe numbers such as mean survival, they measure our confidence in our numbers, with tools like confidence levels, confidence intervals, and confidence bounds. So did I mean “Leave some room for a statistically improbably but still plausible outcome – a survival just above the measured 95 percent confidence interval?” Is that what hope was? Could we divide the curve into existential sections, from “defeated” to “pessimistic” to “realistic” to “hopeful” to “delusional”? Weren’t the numbers just the numbers? Had we all just given in to the “hope” that every patient was above average?
When Breath Becomes Air P133-4
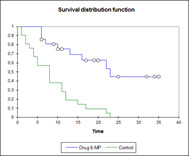
Kaplan-Meier Curve example
Patients when faced with their terminal diagnosis usually do not want to discuss statistics and outcome data. The flawed approach of medical practice is often being in a medical echo chamber where we are within a bubble without yet realising there are patients who do not understand with what exactly they are going through. Most patients haven’t gone through medical training and are not well versed in medical jargon, the bombardment of information can flood the senses and alienate them.
Both Being Mortal and When Breath Becomes Air allude to a future of medicine that is more patient value driven. Of time becoming short and death imminent, what are your values? If you had a bucket-list - what would you place in your top 10, and which ones would you resign away and yet be okay if you didn’t get to complete them? Atul Gawande alludes to Daniel Kahneman’s fantastic book Thinking Fast and Slow which I cannot recommend highly enough. Here he refers to what is termed the Peak-End Rule where upon asking patients to recount an event whose memory has become blurred with time, what is remembered follows this rule. The ‘peak’ or the most memorable part of the event – i.e. a incredibly touching moment, a beautiful goal scored, a worst painful moment of a procedure, and the ‘End’ where we remember the concluding moments of the event. For example, during the 2002 World Cup qualifiers – I remember vividly David Beckham scoring the equalising goal against Greece to send England into the finals. The game had its moments but was a poor performance from the England team. Greece were leading England 2-1 into the 93rd minute and it looked like England were out of the World Cup. Then England were awarded a free kick, and what happened next was history. Even as a seven-year-old, my memories of watching that rather drab football match were elevated considerably in literally the dying seconds of David Beckham scoring that free kick. Atul Gawande notes the story we write ourselves – the narrative of our life. For human beings, life is meaningful because it is a story. A story has a sense of a whole, and its arc is determined by the significant moments, the ones where something happens. We distinguish our experiencing self – which is absorbed in the moment with the remembering self – recognising the peaks of joy and valleys of misery but also how the story works out as a whole. As we know from all stories, endings matter. And no more so than the ending of our lives.
In Abraham Maslow’s A Theory of Human Motivation, it is proposed there is a hierarchy of needs with basic needs for physiological survival, and safety at the bottom, above this is the need for love and belonging, and above this is the desire for growth – attaining personal goals, mastering knowledge and skills, recognition and reward for our achievements. At the crest of the pyramid of this hierarchy of needs is what Maslow terms ‘self-actualization’ – self-fulfilment through pursuit of moral ideals and creativity for their own sake. This is all good and well when we believe we are invincible – everybody wants to live forever but once faced with death – what then becomes important to you?
How we seek to spend our time may depend on how much time we perceive ourselves to have. When you are young and healthy, you believe you will live forever. You do not worry about losing any of your capabilities. People tell you “the world is your oyster,” “the sky is the limit,” and so on. And you are willing to delay gratification – to invest years, for example, in gaining skills and resources for a brighter future. You seek to plug into bigger streams of knowledge and information. You widen your networks of friends and connections, instead of hanging out with your mother. When horizons are measured in decades, which might as well be infinity to human beings, you most desire all that stuff at the top of Maslow’s pyramid – achievement, creativity, and other attributes of “self-actualization.” But as your horizons contract – when you see the future ahead of you as finite and uncertain – your focus shifts to the here and now, to everyday pleasures and the people closest to you.
Being Mortal p97
We need to discuss what is important to a patient who is dying with the utmost importance, we know what one wants at twenty will be drastically different to what one wants at sixty. Similarly, what one wants now may be completely different to six months down the line, all of this even more important now that time is running out and its finite sands trickling away.
Arriving at an acceptance of one’s mortality and a clear understanding of the limits and the possibilities of medicine is a process, not an epiphany.
...
“I wish things were different.”
“If time becomes short, what is most important to you?”
Being Mortal P182
We so often deprive the elderly of choice with regimented medication schedules and restriction of even going outside the house for fear of them falling of injuring themselves. Even in this age of patient-centred care, what hasn’t been realised is what the patient wants. It is this failure in health to recognise that the sick and aged have priorities beyond merely being safe and living longer; that the chance to shape one’s story is essential to sustaining meaning in life.
Wants are fickle. And everyone has what philosophers call “second-order desires” – desires about our desires. We may wish, for instance to be less impulsive, more healthy, less controlled by primitive desires like fear or hunger, more faithful to larger goals. Doctors who listen to only the momentary, first-order desires may not be serving their patients’ real wishes, after all. We often appreciate clinicians who push us when we make shortsighted choices, such as skipping our medications or not getting enough exercise. And often adjust to changes we initially fear. At some point, therefore it becomes not only right but also necessary for a doctor to deliberate with people on their larger goals, to even challenge them to rethink ill-considered priorities and beliefs.
Being Mortal p202
It is this independence and autonomy that gives a patient their dignity – their freedom and their choice to do how they wish. I think everyone wishes to be treated with respect and have their own freedom in their end of years, it is only human to do so. All it takes is basic human empathy to realise how we treat our elderly patients and elderly family members and friends and understand the golden rule in religion: Treat others how you want to be treated.
Medicine, now no less than then, is the art of nurturing the sick to a state of health and recognizing when it is impossible to do so. Should that be the case, ways must be found to de-medicalize the final weeks or days, to nurture the dying and those who love them, and by this means to nurture ourselves. The real truth of healing lies in the nurture.
How We Die P288
All we ask is to be allowed to remain the writers of our own story. That story is ever changing. Over the course of our lives, we may encounter unimaginable difficulties. Our concerns and desires may shift. But whatever happens, we want to retain the freedom to shape our lives in ways consistent with our character and loyalties.
This is why the betrayals of body and mind that threaten to erase our character and memory remain among our most awful tortures. The battle of being mortal is the battle to maintain the integrity of one’s life – to avoid becoming so diminished or dissipated or subjugated that who you are becomes disconnected from who you were or who you want to be. Sickness and old age make the struggle hard enough. The professionals and institutions we turn to should not make it worse. But we have last entered an era in which an increasing number of them believe their job is not to confine people’s choices, in the name of safety, but to expand them, in the name of living a worthwhile life.
Being Mortal p140-141

The Dance of Death
Unity of death
Michel de Montaigne, a figure so renowned he earned his place in history as one of Ralph Waldo Emerson’s Reputable Men thought deeply about death and mortality amongst other topics and emphasises this point with profound eloquence. His Essay “That to Study Philosophy is to Learn to Die” is a serene meditation of death and life that expresses the contemplation of death far more eloquently than I could ever do it justice.
—let us learn bravely to stand our ground, and fight him. And to begin to deprive him of the greatest advantage he has over us, let us take a way quite contrary to the common course. Let us disarm him of his novelty and strangeness, let us converse and be familiar with him, and have nothing so frequent in our thoughts as death.
That to Study Philosophy is to Learn to Die – Michel de Montaigne
Each of us is facing the same fate; all of us united in the face of death. To death, none of us knows how to react really. Yet we know it's there hanging before us, like Cicero's account of the Sword of Damocles. Nothing in life is ever guaranteed. Our memories of the past and our hope for the future. To our love to long ago and our love for days to come.
I began to realise that coming in such close contact with my own mortality had changed both nothing and everything. Before my cancer was diagnosed, I knew that someday I would die, but I didn’t know when. After the diagnosis, I knew that someday I would die, but I didn’t know when. But now I knew it acutely. The problem wasn’t really a scientific one. The fact of death is unsettling. Yet there is no other way to live.
When Breath Becomes Air P132
Across all cultures from the Mexican tradition of Dia de Muertos (All Souls Day) and Hallowe’en – a contraction of All Hallows’ Evening, Chinese tradition of the Ghost Festival (盂蘭節), Pitri Paksha (पितृ पक्ष) or fortnight of the ancestors, the Japanese term mono no aware (物の哀れ) or the pathos of things. The veneration of the dead where descendants pay their respects to their ancestors is shared across all cultures, no matter the difference in our tongues.
We all strive to understand the mystery of death, where do we go after we die? Will this love survive of us? Was my life a life well spent? These questions are universal and unanswerable. The only thing we know for certain is the only time we have is in the present.
The fear in life is to live a life unspent. Regret is the cruellest wound, like in T.S. Eliot’s narrator in The Love Song of J.Alfred Prufrock, the stings of missed opportunities and paralysing neuroticism tinges the poem with the bitterness of living a life like his.
“We bones, lying here bare, await yours.” in Capela dos Ossos
Vita brevis breviter in brevi finietur,
mors venit velociter quae neminem veretur,
omnia mors perimit et nulli miseretur.
Ad mortem festinamus peccare desistamus.
Life is short, it will end;
Death comes quickly and respects no one,
It destroys everything and has no mercy.
To death we are hastening let us refrain from sinning.
Ad Mortem Festinamus from the Llibre Vermell de Montserrat
There is our fear and loathing against death – like Beethoven shaking his fist at the thunderstorm on his deathbed, or Dylan Thomas’ plea to his dying father. How many of us have been deprived of our future and dreams by lives cut short. Life is never fair when the good may suffer and the evil may revel. We’re all victim to death’s blind snatching of us.
Do not go gentle into that good night,
Old age should burn and rave at close of day;
Rage, rage against the dying of the light.
Do not go gentle into that good night
- Dylan Thomas
The final monologue of Pozzo in Waiting for Godot notes the cruelty of ephemeral life and a resounding cry against death and old age in his final lines in the play:
POZZO:
(suddenly furious.) Have you not done tormenting me with your accursed time! It's abominable! When! When! One day, is that not enough for you, one day he went dumb, one day I went blind, one day we'll go deaf, one day we were born, one day we shall die, the same day, the same second, is that not enough for you? (Calmer.) They give birth astride of a grave, the light gleams an instant, then it's night once more. (He jerks the rope.) On! Exeunt Pozzo and Lucky. Vladimir follows them to the edge of the stage, looks after them. The noise of falling, reinforced by mimic of Vladimir, announces that they are down again. Silence. Vladimir goes towards Estragon, contemplates him a moment, then shakes him awake.
Waiting For Godot – Act 2 – Samuel Beckett
Such in life, what we make of it is how we live. We cannot be overwhelmed by life's brevity, from the Buddhist concept of anicca (impermanence) there is still meaning to be found in life with our families and friends and our fellow human beings. Do resign ourselves to the disillusionment with the disregard of the cosmos like Meursault in Albert Camus’ L’Etranger? We can be all too paralysed with a myopic view upon death where we creep ever deeper into the rabbit-hole of existential crisis, unable to see the wood for the trees. Being inevitable, countless philosophers and wise thinkers have argued our fear of death is pointless. There is a fine line one treads between accepting death resignedly and passively overwhelmed by the indifference of the universe or fearing death.
https://www.youtube.com/watch?v=KXxw-zXRqOs
And which of you by worrying can add a single hour to his life’s span?
Luke 12:25
Yet death is scary, it’s terrifying in fact. It’s the finality of death that makes it so powerful and why it has been feared by our ancestors generations and generations before us. Being aware of our death makes us fearful of how we wish to live, what we wish to achieve, the opportunities we see hanging before us – the most powerful impulse in our life. We cannot escape it through fear because death is the one thing we cannot run away from. Though fear remains, it isn’t the fear of the mystery of death rather the fear of what we may not be able to do, achieve, live in our limited time on Earth.
Such is the importance of the philosophy of how we decide to live our lives, whether it is through religion, philosophy, family, community etc. we need to find meaning in our lives because our days are numbered and we need to make them count.
As Matt Haig argues in his beautiful book Reasons Not To Die “We can just use it in life. For instance, I find that being grimly aware of mortality can make me steadfastly determined to enjoy life where life can be enjoyed. It makes me value precious moments with my children, and with the woman I love. It adds intensity in bad ways, but also good ways.”
Reasons Not To Die – Matt Haig
No matter how brief our lives are, we can still find beauty in its brevity like mayflies rising and falling where we can choose to make it a life well spent. I think all of us face this existential question at some point in our lives where we feel the sands of time trickling away or facing abject boredom as Heidegger describes facing anxiety over your life’s meaning: “Profound boredom, drifting here and there in the abysses of our existence like a muffling fog, removes all things and men and oneself along with it into a remarkable indifference.” It is this boredom when we feel the fear of a conditional life never spent. Boredom I feel is the directionless passivity of allowing yourself to be swept up by the tides and waves of time. That’s why it’s so important to have a purpose, values in life that can steer yourself to a destination where you want to reach. Carpe Diem as the old saying goes, “I am not throwing away my shot!,”
So teach us to number our days, that we may present to You a heart of wisdom.
Psalm 90:12
“The universe is not pregnant with life nor the biosphere with man…Man at last knows that he is alone in the unfeeling immensity of the universe, out of which he emerged only by chance. His destiny is nowhere spelled out, nor is his duty. The kingdom above or the darkness below; it is for him to choose”
Jacques Monod
Ageing and growing old
People want to share memories, pass on wisdoms and keepsakes, settle relationships, establish their legacies, make peace with God, and ensure that those who are left behind will be okay. They want to end their stories on their own terms.
Being Mortal p249
I’ve spoken to elderly patients in the hospital who are simply waiting, waiting to be seen, waiting for treatment, hopefully waiting for the family and friends that never visit. I’ve found myself guiltily detaching myself from the history taking after an hour and a half which I’ve allowed to go on for so long (the history is expected to be taken in less than 10 minutes) because I simply know that they have no one else to speak to, and I may be the only comfort they have in a place that’s too busy for them. It’s a pitiable state and I tried not to realise myself in their situation too much because I very much fear that – the loneliness of existence, your children not even bothering to pay a visit and the doctors and nurses too busy for you, may be me one day. I remember when I was volunteering at an elderly care home on every Sunday afternoon during my teenage years, this being the same care home my Grandmother went to during her twilight years, I always remembered the staff being especially friendly whenever we visited Granny and in volunteering there I hoped I could give something back to their support they gave her. Stepping into the care home, after a few months of volunteering a strange realisation dawned on me. I had never seen any of the residents’ relatives. Of course, this might be down to chance on a Sunday afternoon window where I may have missed them but the look on the residents’ faces betrayed that. They were always ecstatic (which admittedly unnerved me a little initially) whenever I came always eager to share their stories with me. Some weeks they would forget who I was briefly then the slow recognition of who I was as I handed over their tea. I saw the cruelty of dementia threatening to deprive them of their memories and realised then why they wanted to pass on their stories so eagerly so that they may never be forgotten. I met wonderful people there including one Joan Regan who struck me as a woman who was very beautiful in her prime. Joan recounted stories of her youth and her singing career with joy as I listened eagerly. Then one day after locking my bike and getting ready to serve the tea and biscuits, I realised that there was one person missing from the round. Joan wasn’t there. I heard from one of the nurses that she had passed away earlier in the week. The surprising snatching of life at death’s hands came once again, the void Joan left in that room was never filled again.
The specialty of geriatrics is the care for elderly patients i.e. all patients over the age of 65 and gerontology which is the study of the ageing process itself. The care for the elderly is in itself its own specialty given the increased complexity of the decreased physiological reserve the elderly have which in turn presents with increased complications with problems and disease. Many of these elderly patients are on polypharmacy – on a number of different drugs, many of which are to treat the side effects of a certain toxic effect of another, as Paracelsus said: Alle Dinge sind Gift, und nichts ist ohne Gift, allein die Dosis macht dass ein Ding kein Gift ist.
All things are poison, and nothing is without poison, the dosage alone makes it so a thing is not a poison. The drugs which treat are also poisonous and hence strict monitoring of the medication is needed for fear of pushing a patient’s condition into a worse state by iatrogenic problems – problems caused by medical interference.
How we monitor the care for the elderly is measuring their activities of daily living (ADLs), a group of eight markers of basic physical independence: toileting, eating, bathing, grooming, get out of bed, get out of a chair, walking. After often a prolonged stay in hospital, the worst thing to do would be to discharge a patient unable to perform these ADLs independently and hence cause themselves further harm. A study by the University of Minnesota found elderly patients under the care of a geriatrics team were a quarter less likely to become disabled and half as likely to develop depression. This is remarkable, and it is clear why, geriatric teams have set out especially to treat the needs of the elderly and the problems of ageing which other specialties overrun with political and economic burdens on their health systems may overlook.
…In almost none does anyone sit down with you and try to figure out what living a life really means to you under the circumstances, let alone help you make a home where that life becomes possible.
This is the consequence of society that faces the final phase of the human life cycle by trying not to think about it. We end up with institutions that address any number of societal goals – from freeing up hospital beds to taking burdens off families’ hands to coping with poverty among the elderly – but never the goal that matters to the people who reside in them: how to make life worth living when we’re weak and frail and can’t fend for ourselves anymore.
Being Mortal p76-77
The values we see in young children and values which have been handed down over the years: filial piety, mutual respect, treating your neighbour as if you wish to be treated yourself, kindness, gratitude etc. These values are old and they count for something important for they teach us how to live meaningfully. The Japanese have the terms Hanami (flower viewing) where the cherry blossoms start to bloom and Momijigari (leaf peeping) in which the flowers of summer turn into a deep autumnal maple red. There’s a dignity and great beauty in entering the autumn of our years. Such are the seasons of time, we rise, and we fall for the new generation to take its place.
In our ageing population, where in the UK over 10 million are aged 65 or over, these values have never been more important. The elderly population face the trials and tribulations of old age which is a slow frustrating taunt where you slowly become more and more aware of your limitations of your failing body. The circle of life where you are dependent as a child, growing into an independent adult at our zenith, only to become reluctantly dependent in old age. As our grandparents and parents enter their autumnal years, it is key that we are always there for them. Though they may walk a little slower, stoop in their posture, their hearing and eyesight slowly diminish, they are still our heads of our family – the wise voices from the past who have learnt from experience and mistakes as they learnt from their forefathers passing on valuable advice for us in our generation now so that we may pass it on to our future generations.
youtube
https://www.youtube.com/watch?v=VkoDUFNRqpw&feature=youtu.be&app=desktop
The fear is being in the predicament of those poor, elderly patients I have seen in hospital all alone. I cannot help but feel an indignant anger towards their children, how they have failed in their duties as children. And how we have failed as a society that we allow the old to die scared and lonely? Have we become a less compassionate world? I see the arrogance of the young, a contempt for the old and sick by princelings and little princesses spoiled into becoming narcissists who only care for their own needs? When we evaluate how we treat our elders in society and family, our lack of empathy and the lack of dignity we give them is appalling in many cases. The medicalisation of ageing where we sedate them with drugs and try to quiet down their ‘delirium’ whilst worst of abandoning them to isolation whereby we blame their limitations on them.
https://www.youtube.com/watch?v=ww8CH62FZB0
https://www.youtube.com/watch?v=RFc19I3flJM
The elderly still have a lot to offer us, they are not castaways who no longer have any use in society – that is false. We are entering tumultuous, fearful times ahead in our world, we need their patient guiding hands to show us the way who have gone through difficult times themselves. In our age of nuclear families, we have slowly cut off from our parents and grandparents in the extended family model. This deprives us of an extended kinship that grandparents, uncles, aunts, cousins, family friends that can provide vital support to the family. No man is an island after all. Young men and women will speak with their grandparents and know that one day the same fate of ageing awaits them, a humbleness to forces greater than all of us and that we all want the same thing – a meaningful life well spent.
When we take photos, record in a diary, compile an album, we are trying to save the moment, whether it be a child’s first steps, a wedding, a graduation, these are the accumulation of memories that may fondly remembered for future days. Nostalgia and poignancy colour our past days so that we can affirm to ourselves that our days were not in vain.
No man is an island, entire of itself; every man is a piece of the continent, a part of the main. If a clod be washed away by the sea, Europe is the less, as well as if a promontory were, as well as if a manor of thy friend's or of thine own were: any man's death diminishes me, because I am involved in mankind, and therefore never send to know for whom the bells tolls; it tolls for thee.
Meditation XVII – Now, this bell tolling softly for another, says to me: Thou must die - John Donne
Time and Life
What a ridiculous thing it is to trouble ourselves about taking the only step that is to deliver us from all trouble! As our birth brought us the birth of all things, so in our death is the death of all things included. And therefore to lament that we shall not be alive a hundred years hence, is the same folly as to be sorry we were not alive a hundred years ago. Death is the beginning of another life. So did we weep, and so much it cost us to enter into this, and so did we put off our former veil in entering into it. Nothing can be a grievance that is but once. Is it reasonable so long to fear a thing that will so soon be despatched? Long life, and short, are by death made all one; for there is no long, nor short, to things that are no more.
That to Study Philosophy is to Learn to Die – Michel de Montaigne
Did we lament the fact we weren’t alive during the Hanging Gardens of Babylon, the Enlightenment, or Woodstock? Do we lament that will not be alive when the futuristic flying automobiles and hoverboards of Back to the Future II will finally be available? It is a fool’s errand to do so. How lucky we are to be living in our times, over the course of history this is our time to live and breathe – how wonderful it is to feel this gratitude of being alive now? As in Lin Manuel Miranda’s smash hit Hamilton, in the song The Schuyler Sisters – there are words that leave their mark on this gratitude of the present tense. “Look around. Look around. At how lucky we are to be alive right now!”
You were dead for billions of years before you were born, and it didn't bother you one bit. You will be dead for billions more. Your life is an aberration. Enjoy it.
- Mark Twain
“The race of men is like the race of leaves. As one generation flourishes, another decays.”
- Homer
“There is a ripeness of time for death, regarding others as well as ourselves, when it is reasonable we should drop off, and make room for another growth. When we have lived our generation out, we should not wish to encroach on another.”
-Thomas Jefferson
Old men must die; or the world would grow moldy, would only breed the past again.
- Tennyson
It is through the eyes of youth that everything is constantly being seen anew and rediscovered with the advantage of knowing what has gone before; it is youth that is not mired in the old ways of approaching the challenges of this imperfect world. Each new generation yearns to prove itself – and, in proving itself, to accomplish great things for humanity. Among living creatures, to die and leave the stage is the way of nature – old age is the preparation for departure, the gradual easing out of life that makes its ending more palatable not only for the elderly but for those also they leave the world in trust.
How We Die P87
“Give place to others, as others have given place to you.”
- Michel de Montaigne
https://www.youtube.com/watch?time_continue=4&v=yRJBuNwQwzc
How lucky we are to be alive, and what a privilege it is to pass it on. No one can live forever, we should not lament that fact but rather seize life and live it – carpe diem before our time ends.
Everyone hopes to die peacefully and painlessly – I remember even as children we asked each other the question what would be the best type of death? And as morbid eight-year olds that we were, we all agreed to die in one’s sleep would be the ideal departure from this earth. So then with the increasing life expectancy and improved medical care from the dawn of the miracle of modern day medicine, our lives have become more stable as a result and the chance infection or illness to snatch away our lives is now much less common. This presents with a new set of challenges that Atul Gawande talks about namely the notion of how we die. This view has been romanticised and dramatized that our own expectations of the nature of our deaths has become something of a myth. Death presents itself as one of the factors beyond our otherwise controllable lives and this places a much larger emphasis on ars moriendi – the art of dying.
Sherwin Nuland suggests:
“Death with dignity” is our society’s expression of the universal yearning to achieve a graceful triumph over the stark and often finality of life’s last splutterings.
But the fact is, death is not a confrontation. It is simply an event in the sequence of nature’s ongoing rhythms. Not death but disease is the real enemy, disease the malign force that requires confrontation. Death is the surcease that comes when the exhausting battle has been lost. Even the confrontation with disease should be approached with the realization that many of the sicknesses of our species are simply conveyances for the inexorable journey by which each of us is returned to the same state of physical, and perhaps, spiritual, nonexistence from which we emerged at conception. Every triumph over some major pathology, no matter how ringing the victory, is only a reprieve from the inevitable end.
How We Die P10
The patient dies alone among strangers: well-meaning, empathetic, determinedly committed to sustaining his life – but strangers nonetheless. There is no dignity here. By the time these medical Samaritans have ceased their strenuous struggles, the room is strewn with the debris of the lost campaign, more so even than was McCarty’s on that long-ago evening of his death. In the center of the devastation lies a corpse, and it has lost all interest for those, who moments earlier, were straining to be the deliverers of the man whose spirit occupied it.
How We Die P41
When we begin to focus on death, there is an ethical slippery slope of the myth of the good death. In certain societies such as in Holland and Switzerland who have legalised assisted dying there is the worry is that this normalise euthanasia and medicalises old age – where we’re left with a dystopian Logan’s Run scenario. There is no clear answer like any other ethical question, Sir Stephen Hawking himself who said “Where there is life, there is hope” has also said “To keep someone alive against their wishes is the ultimate indignity,” and has spoken out in support of assisted dying. There is no clear answer. In the UK, euthanasia is illegal – but there are so many levels of this question it is impossible to have a complete blanket law for everyone because all cases are not the same.
Our ultimate goal, after all, is not a good death but a good life to the very end.
Being Mortal p245
Assisted living is far harder than assisted death, but its possibilities are far greater, as well
Being Mortal p245
https://www.youtube.com/watch?v=dV6fDJi_6ns
When afflicted by disease and ageing, dying becomes less in line with dignity. We lose control and may forget who we are, we become incontinent, forgetful, weak, short of breath and in pain. Sherwin Nuland argues dignity in death is very rare, there’s the view we’ll be stoic and transcend our circumstances but within the destructive effects of disease this becomes near impossible.
Though the hour of death itself is commonly tranquil and often preceded by blissful unawareness, the serenity is usually bought at a fearful price – and the price is the process by which we reach that point. There are some who manage to achieve moment of nobility in which they somehow transcend the indignities being visited on them, and these moments are to be cherished. But such intervals do not lessen the distress over which they briefly triumph. Life is dappled with period of pain, and for some of us is suffused with it. In the course of ordinary living, the pain is mitigated by periods of peace and times of joy. In dying, however, there is only the affliction. Its brief respites and ebbs are known always to be fleeting and soon succeeded by a recurrence of the travail. The peace, and sometimes the joy, that may come occurs with the release. In this sense, there is often a serenity – sometimes even a dignity – in the act of death, but rarely in the process of dying.
And so, if the classic image of dying with dignity must be modified or even discarded, what is to be salvaged of our hope for the final memories we leave to those who love us? The dignity that we seek in dying must be found in the dignity with which we have lived our lives. Ars moriendi is ars vivendi: The art of dying is the art of living. The honesty and grace of the years of life that are ending is the real measure of how we die. It is not in the last weeks or days that we compose the message that will be remembered, but in all the decades that preceded them. Who has lived in dignity, dies in dignity.
How We Die P268
Themes of death and mortality place life in perspective. Everything that is good is appreciated anew and all the bad and negativities don’t leave their impact that they used to. Not sweating the small stuff and letting the little things go comes from seeing the big picture. When we’re confronted with our mortality, we realise time is limited and that comes with getting the house in order, making sure what we leave behind will be better than before and our loved ones will be okay when we’re gone.
https://www.youtube.com/watch?v=XTvTLGkWYMU
https://www.youtube.com/watch?v=xuGwJs6NLw4
It’s the lesson of life to always be humble. The measure of a person is not how much they know but their confession of how much they do not know. Being humble is the key to constantly improving and striving to make things better for the future. Arrogance and pride can lead to a wave of egocentric complacency which blinds them to the crash that awaits them. By admitting our limitations to greater forces, admitting our own positions as mere mortals can we then realise the folly of playing god. Like the woman in Bob Dylan’s Like a Rolling Stone, karma is a cruel punishment for the proud.
`My name is Ozymandias, King of Kings:
Look on my works, ye mighty, and despair!'
Nothing beside remains. Round the decay
Of that colossal wreck, boundless and bare,
The lone and level sands stretch far away".
Percy Bysshe Shelley
No one knows when their time will be cut short. In When Breath Becomes Air and Mortality by Christopher Hitchens. Both men were afflicted with the emperor of all maladies: cancer. The age-old question of why death comes prematurely denying one of a peaceful death – Why me? The answer: Why not?
In Jean-Dominique Bauby’s poetic and moving account The Diving Bell & The Butterfly, where he is afflicted with locked-in-syndrome – due to a brainstem lesion leaving him unable to move or talk, imprisoning him in his own body. It is something that I can imagine that would be like a living hell. He communicated through blinks to write his memoir and not a word was wasted. It is a beautiful book filled with pastime memories, regret and the daily routine of his new life. Life isn’t fair especially for these men, but their message they leave, is never to take anything for granted for human life is fragile and nothing is guaranteed, and your fortunes may change in an instant.
This examination of mortality has been since the times of Thomas Browne’s Religio Medici (The Religion of a Doctor) a hugely influential book that showcased his own thoughts and philosophy of medicine that elevated the profession to an art.
…this is indeed not to feare death, but yet to bee afraid of life. It is a brave act ofvalour to contemne death, but where life is more terrible than death, it is then the truest valour to dare to live, and herein Religion hath taught us a noble example: For all the valiant acts of Curtius, Scevola or Codrus, do not parallel or match that one of Job; and sure there is no torture to the rack of a disease, nor any Poynyards in death it selfe like those in the way or prologue unto it. Emori nolo, sed me esse mortuum nihil curo, I would not die, but care not to be dead. Were I of Cæsars Religion I should be of his desires, and wish rather to goe off at one blow, then to be sawed in peeces by the grating torture of a disease. Men that looke no further than their outsides thinke health an appertinance unto life, and quarrell with their constitutions for being sick; but I that have examined the parts of man, and know upon what tender filaments that Fabrick hangs, doe wonder that we are not alwayes so; and considering the thousand dores that lead to death doe thanke my God that we can die but once…
Religio Medici Section 43– Thomas Browne
In modern medicine, we have lost the fundamentals of what it is to treat the sick. We have forgotten what it means to have the privilege to speak with and treat our patients. Sometimes have to look back to remember how to realise the future. The age-old duty-bound Hippocratic oath of medicine and its interpolation of Primum non nocere – first do no harm, embedded in a sacred duty for our patients which is at the very centre of medical practice.
http://www.pbs.org/wgbh/nova/body/hippocratic-oath-today.html
In modern malpractice, the fellow humanity of our patients is often forgotten and eroded away to meet the target of cold political drives. The NHS (National Health Service) remains a remnant of the post-WWII desire by Aneurin Bevan to establish a brave new world – a better future for all of humanity to never face the horrors inflicted again. Free healthcare to the point of care where healthcare is a right not just a privilege for the few. I am proud of being part of the NHS and yet fearful for its future. What foundation of this wonderful system laid out in The Citadel by AJ Cronin and the fight against corruption before the NHS. I was gifted this wonderful novel by my Argentine school tutor who always was there to support me through quite a tumultuous time during my schooldays. I am very grateful for all his support and how teachers like himself are so rare nowadays, it is fitting he left me such an inspirational book to carry me forward. Seeing the NHS in crisis by political machinations makes us all realise what a special thing we have and something we should all fight for.
This anxiety and disillusionment I can see with my own eyes the day to day dismantling of what was a sacred institution and to witness the very best of humanity. In medicine, the litigation and blame culture has demanded nothing less than perfect in a beautifully imperfect human service during this consumerist age where the customer is always right because they are ‘entitled’ to the service and profit is always prioritised over people. Atul Gawande and Sherwin Nuland note this in America where Medical professionals concentrate on repair of health, not sustenance of the soul and an experiment in social engineering, putting our fates in the hands of people valued more for their technical prowess than for their understanding of human needs. When I first enrolled in medical school, I was full of giddy excitement which was soon replaced with shock then anger then disillusionment. Many of the medical students I have encountered have been difficult to say the least, of course there are countless that are lovely, beautiful, amazing human beings, yet I cannot help but feel the new age of medicine is recruiting technocrats and vastly intelligent, bright individuals yet lack basic human empathy and humility. Some of the arrogance I have witnessed has been disgusting, the blatant disrespect to others, the objectification of a patient as a mere lump of flesh by others has left me seething and wondering how and indeed why these people choose to become doctors? Unfortunately, this is something I think will only continue, the admission process can only be measured in certain ways – examination scores, grades, yet what is not and cannot be measured is the human behind the paper. The very same predicament is happening with the health system, overrun with middle men and managers who clock and measure every shred of data in order to assess performance. As Sherwin Nuland wrote in his coda to How We Die in 2010 shortly before he died:
Much of the reconfiguration of health care has been hijacked by economic needs.
…
In this New medicine, everything must be measurable. It must come in the form of a datum, to be commingled with other data in order to make the entire group of facts susceptible to quantification and analysis. Empathy, autonomy, caring, and simple unhurried kindness are not measurable and so become swept away as encumbrances to quantifiable efficiency. The individual patient, along with the complexities of his medical and human problems, is rendered invisible and inaudible by being hidden under the collective weight of some researcher’s or bureaucrat ’s protocol. Nowhere is this suffocation more effective than in stifling the care, counsel, and decision-making of those who are dying.
How We Die P279
I see some of my peers and the immense pressure they’re under – whether it be familial or institutional and often give them the ‘benefit of the doubt’ but finding myself under the same pressures I, in a lapse of my own better judgement when I forget who I’m speaking to could be my family member or a close friend, a fellow human being, and instead as mere tools to fulfil checkbox ticks proving my ‘competencies’. Whenever patients wanted to talk more about something but finding myself more preoccupied with looming examinations and hence not giving them the time I should have, or being frustrated a patient executing their right to not be seen and examined after having countless other medical students and doctors looking at their pathology. I am deeply ashamed of myself that I myself have fallen into this trap of forgetting the humanity of medicine – becoming Tolstoy’s stereotype of a doctor.
At the end, we and those who surround us cannot allow ourselves to fall victim to the imposed conditions of regimented men and women who would have us die under the unnatural conditions of a medical, economic, and bureaucratic order in which humanity and love have no place.
How We Die P282
There was no likelihood of guidance, or even understanding, from Harvey’s doctors, who had by then shown themselves to be untouchably aloof and self-absorbed. They seemed too distanced from the truth of their own emotions to have any sense of ours. As I watched them strutting importantly from room to room on their cursory rounds, I would find myself feeling almost grateful for the tragedies in my life that had helped me be unlike them.
How We Die P226
The doctor said that so-and-so indicated that there was so-and-so inside the patient, but if the investigation of so and-so did not confirm this, then he must assume that and that. If he assumed that and that, then…and so on. To Ivan Ilych only one question was important: was his case serious or not? But the doctor ignored that inappropriate question. From his point of view it was not the one under consideration, the real question was to decide between a floating kidney, chronic catarrh, or appendicitis… From the doctor’s summing up Ivan Ilych concluded that things were bad, but that for the doctor, and perhaps for everybody else, it was a matter of indifference, though for him it was bad. And this conclusion struck him painfully, arousing in him a great feeling of pity for himself and of bitterness towards the doctor’s indifference to a matter of such importance…He said nothing of this, but rose, placed the doctor’s fee on the table, and remarked with a sigh: “We sick people probably often put inappropriate questions. But tell me, in general, is this complaint dangerous, or not?…” The doctor looked at him sternly over his spectacles with one eye, as if to say: “Prisoner, if you will not keep to the questions put to you, I shall be obliged to have you removed from the court.” “I have already told you what I consider necessary and proper. The analysis may show something more.”
The Death of Ivan Ilyich - Chapter 4
We offer patients hope in medicine, whenever they are anxious, scared or pessimistic. There is always the possibility things can improve and get better. “Hope is itself a species of happiness, and perhaps the chief happiness which this world affords,” - Samuel Johnson. We must never allow our patients and loved ones lose hope – that we learn early on especially when dealing with patients who are dying. However, when we talk about death with a loved one or a close friend or a patient, and when knowing the condition is terminal, by offering white lies and false hope – we are doing them a disservice. But when there is nothing else to be done, instead of another investigation or procedure that will certainly prove to have the same result – the preparation and openness to talk about death is needed. Death after all is an event, we all must experience it at some point sooner or later. By not being open with our patients and loved ones, we are doing them a disservice – depriving them of their last wishes, their legacies they want to leave behind and the comfort of their loved ones when they go. It is this abandonment that Ivan Ilyich so feels when he is lied to from his doctor and his family about his fatal condition, being kept in the dark and helpless with no one to understand or help. Sherwin Nuland talks about one of his patients who is dying and the preparation of one last Christmas that meant everything to him. The last time to see family and close friends and tie off loose ends, and share that last moment of joy. Medicine with its goals, is not just to prolong life but also about so much more. Doesn’t everyone deserve this frank and open discussion, our preparations for death allow us to live a more fulfilling life to get everything we wanted done, complete our bucket-lists and set our priorities straight.
What tormented Ivan Ilych most was the deception, the lie, which for some reason they all accepted, that he was not dying but was simply ill, and the only need keep quiet and undergo a treatment and then something very good would result. He however knew that do what they would nothing would come of it, only still more agonizing suffering and death. This deception tortured him — their not wishing to admit what they all knew and what he knew, but wanting to lie to him concerning his terrible condition, and wishing and forcing him to participate in that lie.
The Death of Ivan Ilyich – Chapter 7
Death comes for all of us. For us, for our patients: it is our fate as living, breathing, metabolizing organisms. Most lives are lived with passivity toward death – it’s something that happens to you and those around you. But Jeff and I had trained for years to actively engage in death, to grapple with it, like Jacob with the angel, and, in so doing, to confront the meaning of a life. We had assumed an onerous yoke, that of mortal responsibility. Our patients’ lives and identities may be in our hands, yet death always wins. Even if you are perfect, the world isn’t. The secret is to know the deck is stacked, that you will lose, that your hands or judgment will slip, and yet still struggle to win for your patient. You can’t ever reach perfection, but you can believe an asymptote toward which you are ceaselessly striving.
When Breath Becomes Air P114-5
Death is in an old man’s door, he appears and tells him so, and death is at a young man’s back, and says nothing; age is a sickness, and youth is an ambush;
Meditation VII - The physician desires to have others joined with him – John Donne
You return man to dust and say, “Return, O children of man!”
Psalm 90:3
Josiah Royce, a Harvard philosopher wrote a book The Philosophy of Loyalty which tries to answer what is it that we need in order to feel that life is worthwhile? Simply existing and eating, sleeping and in comfort seems to be empty and meaningless. Royce believed that we all seek a cause beyond ourselves – to him, an intrinsic human need.
The only way death is not meaningless is to see yourself as part of something greater: a family, a community, a society. If you don’t mortality is a horror. But if you do, it is not. Loyalty, said Royce, “solves the paradox of our ordinary existence by showing us outside of ourselves the cause which is to be served, and inside of ourselves the will which delights to do this service, and which is not thwarted but enriched and expressed in such service.” In more recent times, psychologists have used the term “transcendence” for a version of this idea. Above the level of self-actualization in Maslow’s hierarchy of needs, they suggest the existence in people of a transcendent desire to see and help other beings achieve their potential.
Being Mortal p127
To find meaning and a cause in your life is the question that countless philosophers and wise sages have asked since the dawn of time. What is the meaning of life?
To die takes courage. Ernest Hemingway described courage as grace under pressure and I think that’s not too far off. Atul Gawande mentions Plato’s Laches where Socrates asks ‘What is courage?’ Atul Gawande then writes how he derived the definition: courage is strength in the face of knowledge of what is to be feared or hoped. Wisdom is prudent strength. He goes further where he mentions two types of courage required in aging and sickness. 1) the courage to confront the reality of mortality – the courage to seek out the truth of what is to be feared and what is to be hoped. 2) the courage to act on the truth we find. He ends by posing One has to decide whether one’s fears or one’s hopes are what should matter most – A truth to live a good life itself. Such with my own experience, much of life is a choice. During the 2 weeks of the London 2012 Olympic Games, I remember my time during the Olympics could either be spent indoors or outside visiting the various events organised during that fortnight during a rather uncertain time for me personally. It was my choice to either experience the atmosphere of the games or rather mope inside. This is a truth that is shared with much of life, life is what you make of it – and no one can take that away from you.
Conclusion

Tempus fugit – time flies
Ultima forsan – perhaps the last [hour]
When I remember my first encounters with death, I was only a young child, but their impact left a clear mark on me. There are always things I wish I did more of and said, I am regretful that I was too immature to understand how precious time was then and took things for granted as a result especially if it was someone who loved me as much as my Granny. She was a truly remarkable woman who the more I learn about the more I am humbled of her ability to overcome hardships and struggle. Her story is for my Dad to tell, to whom she passed on her best qualities and is the best person to pass on her story. The family friends we lost too soon who were amongst the kindest and best people we ever knew. Their stories are also for my Dad to tell who knew them through loyal friendships and unselfish kindness.
The lessons learnt from all of this is to never be complacent with time and death, love each other and appreciate the goodness and kindness in life, all the other negativities are just minor trivialities that have no impact in the bigger picture. To always be humble, to always be kind to each other and to yourself and to be patient with others. To count your blessings and have the courage to deal with life’s trials and the striving to make your life and the lives around you better and to be the master of your own destiny to fulfil God’s work. To be thankful of our opportunities we have been given and to make the most of them. All of this sounds like a cliche but in the face of death, this means everything. And one thing we can be certain of, is that we will die. What we make of life is how we live it. These final extracts voice the beauty of life and the pathos of farewell in the most beautiful and touching ways. I hope these words will resonate with you as they have done with me and hope that they will inspire you all to live your lives to the fullest and most meaningful so that by the time we are at death’s door we will share the same serene gratitude for our lives and hope for the future.
Yet I was still intensely moved and grateful to have gotten to do my part. For one, my father would had wanted, and my mother and my sister did, too. Moreover, although I didn’t feel my dad was anywhere in that cup and a half of gray, powdery ash, I felt that we’d connected him to something far bigger than ourselves, in this place where people had been performing these rituals for so long.
When I was a child, the lessons my father taught me had been about perseverance: never to accept limitation that stood in my way. As an adult watching him in his final years, I also saw how to come to terms with limits that couldn’t simply be wished away. When to shift from pushing against limits to making the best of them is not often readily apparent. But it is clear that there are times when the cost of pushing exceeds its value. Helping my father through the struggle to define that moment was simultaneously among the most painful and privileged experiences of my life.
Part of the way my father handled the limits he faced was by looking at them without illusion. Though his circumstances sometimes got him down, he never pretended they were better than they were. He always understood that life is short and one’s place in the world is small. But he also saw himself as a link in the chain of history. Floating on that swollen river, I could not help sensing the hands of the many generations connected across time. In bringing us there, my father had helped us see that he was part of a story going back thousands of years – and so were we.
We were lucky to get to hear him tell us his wishes and say his good-byes. In having a chance to do so, he let us know he was at peace. That let us be at peace, too.
After spreading my father’s ashes, we floated silently for a while, letting the current take us. As the sun burned away the mist, it began warming our bones. Then we gave a signal to the boatman, and he picked up his oars. We headed back to the shore.
Being Mortal P262-3
Everybody succumbs to finitude. I suspect I am not the only one who reaches this pluperfect state. Most ambitions are either achieved or abandoned; either way, they belong to the past. The future, instead of the ladder toward the goals of life, flattens out into a perpetual present. Money, status, all the vanities the preacher of Ecclesiastes described hold so little interest: a chasing after wind, indeed.
Yet one thing cannot be robbed of her futurity: our daughter, Cady. I hope I’ll live long enough that she has some memory of me. Words have a longevity I do not. I had thought I could leave her a series of letters – but what would they say? I don’t even know if she’ll take to the nickname we’ve given her. There is perhaps only one thing to say to this infant, who is all future, overlapping briefly with me, whose life, barring the improbable, is all past.
That message is simple:
When you come to one of the many moments in life where you must give an account of yourself, provide a ledger of what you have been, and done, and meant to the world, do not, I pray, discount that you filled a dying man’s day with sated joy, a joy unknown to me in all my prior days, a joy that does not hunger for more and more but rests, satisfied. In this time, right now, that is an enormous thing.
When Breath Becomes Air P198-199
I feel grateful that I have been granted nine years of good health and productivity since the original diagnosis, but now I am face to face with dying. The cancer occupies a third of my liver, and though its advance may be slowed, this particular sort of cancer cannot be halted.
It is up to me now to choose how to live our the months that remain to me. I have to live in the richest, deepest, most productive way I can. In this I am encouraged by the words of one of my favourite philosophers, David Hume, who, upon learning he was mortally ill at age sixty-five, wrote a short autobiography in a single day in April of 1776. He titled it “My Own Life.”
…
Over the last few days, I have been able to see my life as from a great altitude, as a sort of landscape, and with a deepening sense of the connection of all its parts. This does not mean I am finished with life. On the contrary, I feel intensely alive, and I want and hope in the time that remains to deepen my friendships, to say farewell to those I love, to write more, to travel if I have the strength, to achieve new levels of understanding and insight.
This will involve audacity, clarity, and plain speaking; trying to straighten my accounts with the world. But there will be time, too for some fun (and even some silliness as well).
I feel a sudden clear focus and perspective. There is no time for anything inessential. I must focus on myself, my work, and my friends. I shall no longer look at NewsHour every night. I shall no longer pay any attention to politics or arguments about global warming.
This is not indifference but detachment – I still care deeply about the Middle East, about global warming, about growing inequality, but these are no longer my business; they belong to the future. I rejoice when I meet gifted young people – even the one who biopsied and diagnosed my metastases. I feel the future is in good hands.
I have been increasingly conscious, for the last ten years or so, of deaths among my contemporaries. My generation is on the way out, and each death I have felt as an abruption, a tearing away of part of myself. There will be no one like us when we are gone, but then there is no one like anyone else, ever. When people die, they cannot be replaced. They leave holes that cannot be filled, for it is the fate – the genetic and neural fate – of every human being to be a unique individual, to find his own path, to live his own life, to die his own death.
I cannot pretend I am without fear. But my predominant feeling is one of gratitude. I have love and been loved; I have been given much and I have given something in return; I have read and travelled and thought and written. I have had an intercourse with the world, the special intercourse of writers and readers.
Above all, I have been a sentient being, a thinking animal, on this beautiful planet, and that in itself has been an enormous privilege and adventure.
My Own Life – Oliver Sacks
Further Reading:
http://www.bbc.co.uk/programmes/b04bsgqn - Reith Lectures 2014
http://www.pbs.org/wgbh/frontline/film/being-mortal/
https://www.theguardian.com/lifeandstyle/2012/feb/01/top-five-regrets-of-the-dying
https://www.nytimes.com/2014/01/25/opinion/sunday/how-long-have-i-got-left.html?mcubz=1
https://en.wikipedia.org/wiki/Danse_Macabre
https://en.wikipedia.org/wiki/Memento_mori
Gratitude - Oliver Sacks
Do No Harm - Henry Marsh
Reasons to Stay Alive - Matt Haig
Mortality - Christopher Hitchens
Nausea - Jean-Paul Sartre
Waiting for Godot - Samuel Beckett
Devotions Upon Emergent Occasions – John Donne
The Wasteland, The Love Song of J. Alfred Prufrock, The Hollow Men, Four Quartets – T.S. Eliot
In Memoriam: Poems of Bereavement introduced by Carol Ann Duffy
Essays, That to Study Philosophy is to Learn to Die - Michel de Montaigne
Randy Pausch’s Last Lecture https://www.youtube.com/watch?v=ji5_MqicxSo
Steve Jobs’ Stanford commencement speech https://www.youtube.com/watch?v=UF8uR6Z6KLc&t=1s
Virgil – Georgics
How We Die – Sherwin Nuland
The Death of Ivan Ilyich – Leo Tolstoy
The Citadel – A.J. Cronin
https://www.youtube.com/watch?v=dV6fDJi_6ns House speech on dignity
https://www.youtube.com/watch?v=mjQwedC1WzI
https://www.philosophersmag.com/opinion/18-close-encounters-of-the-cancer-kind
https://www.philosophersmag.com/opinion/17-death-and-its-concept
https://philosophynow.org/issues/27/Death_Faith_and_Existentialism
https://www.theguardian.com/lifeandstyle/series/reports-of-my-death Clive James
https://www.theguardian.com/culture/2015/mar/15/clive-james-interview-done-lot-since-my-death
https://en.wikipedia.org/wiki/Capela_dos_Ossos
http://www.online-literature.com/tennyson/718/
https://en.wikipedia.org/wiki/The_Dream_(Rousseau_painting)
http://www.imdb.com/title/tt0825232/
https://en.wikipedia.org/wiki/David_Livingstone#Stanley_meeting
http://www.parliament.uk/business/publications/research/key-issues-for-the-new-parliament/value-for-money-in-public-services/the-ageing-population/
https://en.wikipedia.org/wiki/Veneration_of_the_dead
Josiah Royce – The Philosophy of Loyalty
https://people.umass.edu/biep540w/pdf/Stephen%20Jay%20Gould.pdf
https://www.youtube.com/watch?v=KXxw-zXRqOs
https://www.youtube.com/watch?v=7Dgn97v3q28
https://www.youtube.com/watch?v=MhxJ1EzKUoM
http://www.lifehacker.co.uk/2017/09/09/what-it-feels-like-to-die
https://en.wikipedia.org/wiki/Death
http://psychclassics.yorku.ca/Maslow/motivation.htm
https://archive.org/stream/philosophyloyal00roycuoft/philosophyloyal00roycuoft_djvu.txt
https://www.jstor.org/stable/3349959?seq=1#page_scan_tab_contents
http://classics.mit.edu/Plato/laches.html
https://www.youtube.com/watch?v=rDjmDHiSTm8
https://archive.org/details/IkiruToLive
http://penelope.uchicago.edu/letter/letter.html
Calvary
Momijigari
Day of the Dead
Grapes of Wrath – John Steinbeck
Tibetan Book of the Dead
War and Peace, The Death of Ivan Ilyich – Leo Tolstoy
For Whom the Bell Tolls - Ernest Hemingway
In Search of Lost Time - Marcel Proust
To Calvary (Gagulta) – site of Jesus’ crucifixion, Place of the skull
youtube
#death#mortality#rip#restinpeace#momento mori#tempus fugit#life#living#halloween#carpediem#be humble#humility#gratitude#thank you
2 notes
·
View notes
Text
Why does meditation work?
Here’s a ASAP Science video on the benefits of meditation
youtube
o Meditation leads to decreased anxiety and depression, and increased pain tolerance.
o Mediation has been found to increase memory, self-awareness and goal setting, improved immunity
o Meditators have higher levels of alpha waves (9-13 Hz) - reduce negative mood, tension and anger
o Grey matter is more dense in the cortex - responsible for higher order brain functions, and less dense in amygdala (stress and emotion centre) and meditation counteracts the shrinkage of grey matter during ageing.
Meditation as mentioned in the above video (and many more in the Further Reading section) has several benefits - a mental training for the brain. But why does it actually work? Thus far, the exact mechanisms are still unknown but there are theories in recent years that give a better picture of how meditation works on the brain. The most probable effect on the brain is stimulating the autonomic parasympathetic response (rest and digest) rather than the sympathetic response (fight or flight). Until further research in neuroscience, we will not know exactly what triggers off a parasympathetic response but it is likely similar to theories regarding sympathetic responses which have been developed due to our evolutionary responses to hunt and flee.The parasympathetic response has the following effects on the body: SSLUDD - sexual arousal, salivation, lacrimation, urination, defection, digestion. The PSNS response also leads to a reduction of stress hormones such as catecholamines and cortisol, the slowing down of the heart rate and lower blood pressure.
Mentioned earlier was how meditation tunes the brainwaves towards an alpha wave predominance. See Figure 1 for a brief overview of the different brainwaves. The differences are all to do with different electrical activity in the brain and the different frequencies transmitted according to the different type of activity performed.
Figure 1: Brainwaves seen on EEG
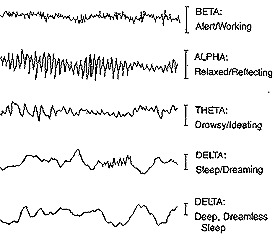
There’s still a lot of holes in the knowledge of the exact details why but from this information we can say that meditation taps into brain activity associated with relaxation hence leading to a parasympathetic response - or is it vice versa? Either way, the science shows it works - we may not know why exactly it works but no doubt further research will give us more answers. Interestingly David Nutt, psychiatric professor at Imperial has recently published research showing that meditation has similar effects to certain hallucinogenic drugs - in this example, Ayahuasca a South American hallucinogen with LSD like effects. This has been shown with brain imaging such as fMRI and EEG. After attending a recent talk by David Nutt, he elaborated on this link where both meditation and hallucinogenic drugs dampen down brain activity in the brain. This sounds counter-intuitive but it makes sense if you think of it like an overheated computer (which our busy minds are) and a reset button. And excitingly this isn’t just a temporary relaxation, meditation can actually rewire our brains with structural and neurophysiological changes.
Figure 2: Beta wave activity in brains before and after meditation
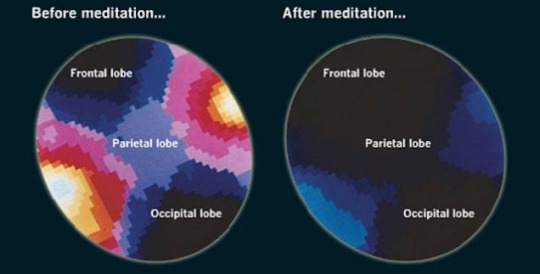
So far, we have an good idea of how meditation works but it is an area ripe for future research especially with the correlation with hallucinogens. The next few years will provide us with more answers no doubt.
I cannot emphasise enough how important meditation is. Modern life is rubbish. Living in the city, busy people. deadlines, commuting - stress is inevitable. We weren’t meant to function like this - we’re not machines. In recent years, meditation has boomed in popularity in the west (mainly due to yuppie cultural appropriation). However what thousands of years of wisdom gives to our daily lives is the key to confronting with the negative aspects of life fuelled by stress. Meditation can be thought of as an exotic, fabled practice an abstract supernatural ritual described in Herman Hesse’s Siddartha or in Frank Herbert’s Dune or George Lucas’ Star Wars. But in reality it is astonishingly simple, sitting or standing, on the tube or at home, it can be practised anywhere and anytime. There are many different types ranging from mindfulness of breathing to metta bhavana. But all with a purpose of acceptance. Only through acceptance instead of resistance will tension dissolve. In Yuval Noah Harari’s excellent book Sapiens: A Brief History of Humankind (which by the way I cannot recommend strongly enough - read it!) in pages 441-442 gives the best explanation for meditation I’ve found.
People are liberated from suffering not when they experience this or that fleeting pleasure, but rather when they understand the impermanent nature of all their feelings, and stop craving them. This is the aim of Buddhist meditation practices. In meditation you are supposed to closely observe your mind and body, witness the ceaseless arising and passing of all your feelings, and realise how pointless it is to pursue them. When this pursuit stops, the mind becomes very relaxed, clear and satisfied. All kinds of feelings go on arising - joy, anger, boredom, lust - but once you stop craving particular feelings, you can just accept them for what they are. You live in the present moment instead of fantasising about what might have been.
Sapiens: A Brief History of Humankind - Yuval Noah Harari
I’d highly recommend using headspace though there are other apps such as calm and stop, think & breathe. The key part of meditation is the daily consistency. It’s like studying for an exam consistently everyday vs cramming the night before. This practice of meditation serves as a microcosm of getting sh*t done in life.
For me personally, I’ve had my fair share of struggles like everyone else. Depression, feuds, worries, anxiety, stresses, death, grief. Life isn’t easy, but isn’t that the whole point?! No diamond ever become a diamond without pressure. No one ever achieved anything without hard graft.
“Easy choices, hard life. Hard choices, easy life.” - Jerzy Gregorek
If you can meet with Triumph and Disaster
And treat those two impostors just the same;
If - Rudyard Kipling
Marcus Aurelius, the great Roman Emperor in his famous and aptly named Meditations was and still is the most famous face of stoicism, an ancient Greek school of philosophy defined by their superhuman quality of indifference to the vicissitudes of fortune and to pleasure and pain, expressed this truth over a millennium ago
You have power over your mind - not outside events. Realise this, and you will find strength.
Meditations - Marcus Aurelius
Now doesn’t that sound uncannily like meditation? Now shall we all just appreciate how wonderful it is to simply be present.
Further reading
https://www.youtube.com/watch?v=jH7WoeBVtXY
https://www.youtube.com/watch?v=yZY-TH4KHlg
https://www.youtube.com/watch?v=LkoOCw_tp1I
https://www.youtube.com/watch?v=q0DMYs4b2Yw
https://www.youtube.com/watch?v=FAcTIrA2Qhk
https://www.youtube.com/watch?v=wirV265ZYSw
https://www.youtube.com/watch?v=qzR62JJCMBQ
http://www.freemeditation.com/meditation-basics/how-does-meditation-work/
https://www.scientificamerican.com/article/what-is-the-function-of-t-1997-12-22/
http://metro.co.uk/2017/04/05/taking-hallucinogenic-drugs-has-similar-effects-to-meditation-on-the-brain-6554913/
http://yang-sheng.com/?p=10991
https://en.wikipedia.org/wiki/Brain_activity_and_meditation
https://www.headspace.com/
https://www.calm.com/
https://www.stopbreathethink.com/
5 notes
·
View notes
Text
Bob Marley | Oliver Sacks | Sergei Rachmaninoff
Bob Marley (6 February 1945 - 11 May 1981)
“The truth is, everyone is going to hurt you. You just got to find the ones worth suffering for.”
I mentioned in a post I did a while back I would return to talk about Rachmaninoff - in that particular post I didn’t mention the disease he died from, melanoma. Another musical legend died from the same disease, one who wasn’t from the path of classical music but reggae - a genre which he popularised on a worldwide level with his band, The Wailers which spanned a decade before he embarked on his solo career. Bob Marley was a unique figure in the musical industry with his Rastafarian beliefs permeating into his music and lifestyle. Rastafarianism centred around the Emperor Haile Selassie I of Ethiopia and pan-Africanism. Among smoking marijuana and dreadlocks - based on Samson in the Bible which prohibits the cutting of hair, the Rastafarian movement had their own unique traditions including one that would lead to the death of Bob Marley. Among his music and his propulsion of Jamaican culture on a worldwide level, Bob Marley was also a keen footballer which may be the most pleasant surprise in his biography. He relocated to Bloomsbury, London during which he recorded his aptly named magnum opus, Exodus. The spiritual and laid back nature of the album as an extension of Marley’s life which came after an assassination attempt in Jamaica. The album is a swirling drug trip of politics, religion and sex where it has earned its place in history in its 40th year. As with many musical artists that entered the public consciousness, Bob Marley’s time on Earth was tragically short - he was only 36. And
Bob Marley performing I Shot The Sheriff
youtube
Oliver Sacks (9 July 1933 – 30 August 2015)
“If we wish to know about a man, we ask 'what is his story--his real, inmost story?'--for each of us is a biography, a story. Each of us is a singular narrative, which is constructed, continually, unconsciously, by, through, and in us--through our perceptions, our feelings, our thoughts, our actions; and, not least, our discourse, our spoken narrations. Biologically, physiologically, we are not so different from each other; historically, as narratives--we are each of us unique.”
Oliver Sacks is known as the Poet Laureate of Medicine. It’s easy to see why. His books are portals into how he approached medicine and his patients, always placing them at the forefront of everything he did. His writing style resonates with his empathy and compassion seeing his patients as equals and teachers. I’d highly recommend his most famous works The Man Who Mistook His Wife For A Hat and Awakenings as entry points to the writings of Oliver Sacks. Robin Williams (mentioned in an earlier post) played Sacks in the film adaptation of Awakenings in perhaps his most tender role. It was actually reading The Man Who Mistook His Wife For A Hat a few years ago that inspired me to start this blog. The miscellaneous collection of patient led stories and case studies gave an otherwise abstract disease an added depth and emotional resonance. Sacks was able to tap into the human side of medicine when in recent years it has become so regimented and industrialised and from a recent patient’s words ‘heartless’. Sacks reminds me of the duty of a doctor, and that’s the duty of a human being. Never for one moment does Sacks forget that he himself could be the patient in front of him, and neither does he take it for granted that anything less than the best he can do is enough for them. Losing Oliver Sacks to me was like losing one of the old inspirational classical doctors of another time - smart, eccentric but always caring. How much better the world would be if everyone took their time, observed, listened and cared like Oliver Sacks?
Oliver Sacks in a PBS interview in 1989
youtube

Sergei Rachmaninoff (20 March 1873 - 28 March 1943)
Music is enough for a lifetime - but a lifetime is not enough for music
Rachmaninoff by the time of his death had been diagnosed with advanced melanoma. The biography of a great composer no doubt is dramatic with its tumultuous events and tragedies and Rachmaninoff is no different. The death of his sisters growing up in 19th century Russia, his struggling academic grades, a forbidden love with his neighbour, Vera, the death of his idol, Tchaikovsky from cholera all had a bruising impact on the young man and had shaped his music to the masterpieces we hear now. One piece of his biography is especially revealing of his character, the failure of his Symphony No.1 which was widely panned by critics led Rachmaninoff to a deep depression that lasted 3 years. Where he had placed his hard work and precious time into creating his symphony only for it to trashed by critics which led him down a path of endless self-criticism exacerbating his depression. It was only with the help of Nikolai Dahl and his hypnotherapy and psychotherapy sessions and adjustments to his personal life including sleep regulation, appetite and support from close friends and family that Rachmaninoff began to recover from his ‘self-imposed exile’ which culminated in probably the most beautiful piece of art from Russia, his Piano Concerto No.2. Rachmaninoff began to enjoy his success he had striven for so long during a happy time in his life with his marriage to his wife, Satina. This time also came with great turmoil especially with the 1905 revolution but his loyalty and love for his motherland obliged him to stay when there were enthusiastic offerings from America. Further tragedy struck when his close friend during his time at the Moscow Conservatory, Alexander Scriabin died which was quickly followed by Taneyev, another friend and finally Rachmaninoff’s own father. Further political turmoil came with the 1917 revolution (see the classic film Dr Zhivago as a reference to the horrors afflicted) which placed Rachmaninoff in an dire situation citing his aristocratic birth in the midst of a Bolshevik regime that began to seize land ‘for the people’. Here he gained permits to Scandinavia where he spent the duration of the war working as a concert pianist where he worked tirelessly to improve his technique. During his increasing financial woes, he eventually relented and set off for New York City from Oslo in 1918. Here he now saw the success and love he had for so long rejected and it was in America where he met his compatriot, Vladmir Horowitz in the basement of Steinway Hall in 1928 who is known as the master of Rachmaninoff’s Piano Concerto No.3. (see the 1996 film Shine as a tribute to this magnificent piece). Rachmaninoff even acknowledged this himself stating "This is the way I always dreamed my concerto should be played, but I never expected to hear it that way on Earth." after one of Horowitz’s performances in Rachmaninoff’s twilight years.
Why Rachmaninoff is so important to me, it is his humanity. During the face of great tragedy which he felt so keenly as the sentimental soul he was and suffered greatly during it, he strove to continue despite all his self-doubt and self flagellation as a failure. He was just so human. You can feel his tragedy and grief embrace your very soul and yet find profound beauty in his works. This is true art, the expression of one’s soul and the uncanny ability to deeply connect with your fellow human beings. Tolstoy’s War and Peace comes to mind, another Russian export that can match the heights of Rachmaninoff’s compositions. The tragedy, the love, the family, the war, the evil, the kindness, the resilience and the struggle during the 1812 French invasion of Russia where it seemed all hope had been lost. And it was this - hope that is the crowning quality of humanity. My thoughts return to my childhood reading one of my sisters’ hand me down Enid Blyton books The Land of Far-Beyond and the final chapter always struck me deeply even as a kid. Out of faith, hope, and love. It is hope that is the greatest of these three. Where there’s life, there’s hope.
Sergei Rachmaninoff performing Rhapsody on a Theme of Paganini in 1934. Of the 24 variations, pay especially close attention to the 18th (the most well known and romantic) and the 24th, the legendary finale requiring superhuman technical skill to pull off (in fact Rachmaninoff himself doubted his ability to play this and as a teetotaller had a creme de menthe before his performance to help steady his nerves and consequently became known as the creme de menthe variation.
youtube
So what did these three men have in common? Melanoma.
Melanoma is the most dangerous type of skin cancer and the 5th most common cancer in the UK. Melanoma derives from cancer in the pigment containing cells called melanocytes. Although melanoma is most associated with melanocytes of the skin, as in Oliver Sack’s case it can occur in the eye - e.g. uveal melanoma - the uvea is the collective term for the structures: iris, ciliary body and choroid (Figure 1 & 2). Bob Marley had discovered acral lentiginous melanoma (Figure 3) growing underneath the nail of a toe following a football game injury, which due to his Rastafarian beliefs against amputation ultimately led to Sergei Rachmaninoff by the time of his death already had advanced melanoma where it is probable that metastasis had already occurred.
Figure 1: Diagram of the eye
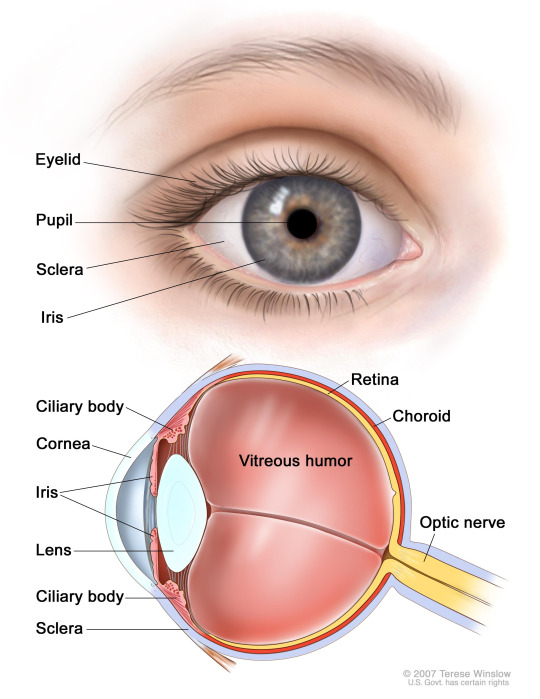
Figure 2: Uveal melanoma
Figure 3: Acral lentiginous melanoma in nail bed

See the video below by Armando Hasudungan which provides a good introduction to melanoma
youtube
One of the most common cancers in young adults - most commonly seen on backs in men and legs in women. The primary risk to melanoma is intermittent exposure to UV radiation and sunlight.
Risk factors - FH, PMH, light physical features, immunosuppression, Multiple freckles and moles (atypical mole syndrome)
Features using a dermatoscope (glorified magnifying glass with a torch)- pigmented, aymmetrical, uneven borders, bleeding. See ABCDE (Figure 4) for good heuristic to diagnose melanoma
EFG - elevated above skin surface, firm to touch, growing - criteria for nodular melanoma, most dangerous form
Protective factors - protection against sun and UV radiation e.g. sunhats, sunscreen, restriction of time spent in sun, regular skin check ups
Figure 4: ABCDE checklist
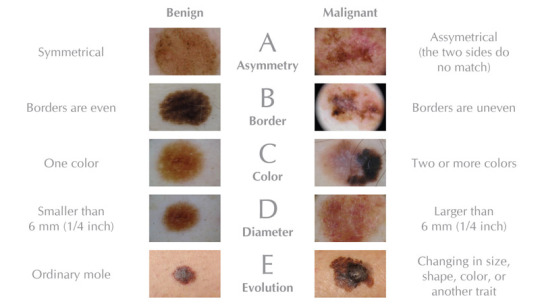
The video below by Podmedics provides more detail about melanoma:
youtube
Risk factors: multiple benign/atypical naevi, giant pigmented hairy naevus, genetic predisposition (>2 first degree relatives affected, CDKN2A mutation), previous skin cancer, immunosuppression, Fitzpatrick skin type I (see Figure 5, often auburn haired, very pale individuals - again another heuristic - dermatology is full of them!, intermittent exposure to sunlight - UV radiation - UVB 315-280 nm and less so UVA 400-315 nm, sunbeds etc (see youtube video in Further Reading for why), geographical location, increasing age
Glasgow 7 point criteria (Figure 6)
Superficial malignant melanomas: superficial spreading, lentigo maligna, acral lentiginous
Deeper malignant melanoma: nodular, mucosal, neurotropic, desmoplastic
Investigations: excisional biopsy, lymphoscintigraphy - tracing lymph drainage, sentinel lymph node biopsy (if primary melanoma <1mm in depth), staging - USS/CT/MRI/PET/CXR, bloods - LFTs and LDH if liver mets suspected
Management : education, wide location excision +/- skin grafting, chemotherapy, biologics e.g. interferonalpha-2b, IL-2, BRAF inhibitors: dabrafenib, vemurafenib.
Prognosis - Breslow thickness, Clark level, poor prognosis: ulceration, mitotic rate, location of lesions, males>females.
Figure 5: Fitzpatrick skin types

Figure 6: Glasgow 7 point checklist
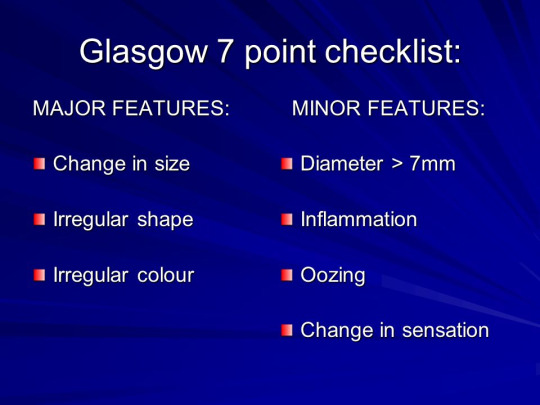
Breslow thickness is a useful diagnostic tool for invasive melanomas. It is the measuring in mm vertically from the top of the granular layer (Epidermal layers from superficial to deep: Come Let’s Get Sun Burned, Stratum Corneum, Stratum Lucidum, Stratum Granulosum, Stratum Spinosum, Stratum Basale) to the deepest point of the tumour. The thicker the melanoma, the more likely it is likely to metastasise.
Clark level of invasion is the anatomical plane of invasion (dermal layers from superficial to deep: papillary dermis to reticular dermis)
Level 1: in situ melanoma
Level 2: Melanoma invasion into papillary dermis
Level 3: Melanoma filled papillary dermis
Level 4: Melanoma invaded reticular dermis
Level 5: Melanoma invaded subcutaneous tissue
Staging of melanoma is the process determining the size/depth of the melanoma and how far it will spread. The classification used is the TNM (tumour, node - lymph, metastasis) which then determines the stage of the cancer (0 to IV) - (Figure 7). The most common metastases from melanoma are the liver, lungs, brain and bones.
Figure 7: Staging of melanoma
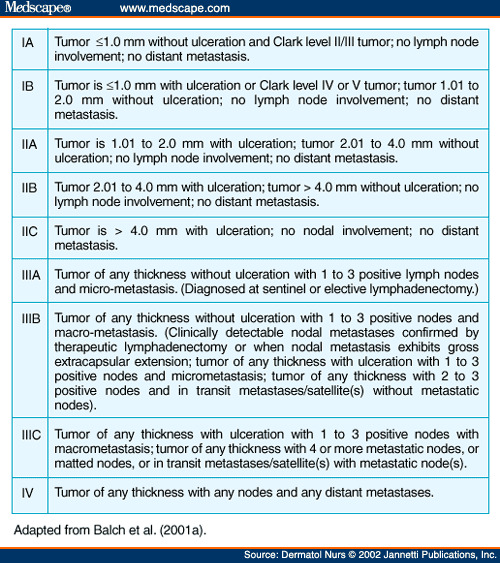
Just a brief mention of uveal melanoma - often referred to as ocular melanomas. It is clear that UV radiation plays a role in the formation of uveal melanoma. The treatment is normally enucleation - the removal of the eye. Given this is a localised cancer, radiotherapy is used - namely brachytherapy is often used as another form of treatment. The liver is the most common location for metastasis from ocular cancer. Oliver Sacks found he had this metastasis to the liver himself to which he wrote a moving article in the New York Times in which the link can be found below.
Melanoma is common. It also kills. That’s why it’s so important to protect yourself in the sun. As seen from this post, all three mentioned were men which fits with the stats that men are more likely to get melanoma than women. I think Hugh Jackman (Wolverine) also had melanoma which fits with his Australian background as well. Something so seemingly harmless as the sun can also lead to metastasis riddling the whole body. So keep checking for any moles, changes, I cannot stress this enough. We have lost three fantastic people mentioned due to this disease, and the fact is the prognosis is remarkably good for early detection (localised melanoma) with five year survival rates of 98% which drops drops staggeringly to 17% with metastasis. The old quote of prevention is better than cure rings true here. I conclude with this poignant quote which reinforces why I write this blog.
“In examining disease, we gain wisdom about anatomy and physiology and biology. In examining the person with disease, we gain wisdom about life.”
Oliver Sacks
Further reading
http://www.bbc.co.uk/news/health-32749634
https://www.youtube.com/watch?v=1vJSsJdSosU
https://www.dermnetnz.org/topics/melanoma/
http://www.bad.org.uk/library-media/documents/Melanoma%20-%20Diagnosis%20and%20Staging.pdf
https://www.nytimes.com/2015/02/19/opinion/oliver-sacks-on-learning-he-has-terminal-cancer.html
0 notes
Text
B.B. King | Johnny Cash
B.B. King (September 16, 1925 - May 14, 2015)

Better not look down
If you want to keep on flying
Put the hammer down
Keep it full speed ahead
Better not look back
Or you might just wind up crying
You can keep it moving
If you don´t look down
The King of the Blues is quite an apt name for such a figure in the world of music. B.B. King was born Riley Ben King, later named B.B. after his nickname Blues Boy King on the Memphis radio station WDIA. How someone could be such a living embodiment of the blues - a genre tinged with suffering and sadness with the brave bounce of hopeful optimism, is remarkable. I’d recommend listening to his classic 1965 album Live at the Regal if you want to hear the visceral talent of the man and proof why we will never have another King of the Blues again. Some musicians’ lives are littered with scandalous affairs and addictions etc. But B.B. King was someone who lived and breathed his music - this was apparent by his absolute passion for touring where he was famous for playing around 250 shows each year! His quirky naming of his Gibson guitar ‘Lucille’ after a woman whom two fans were fighting about and his famed stage presence and his impact on western music are his legacy to the world he left when he passed away in 2015.
Here is B.B. King’s The Thrill is Gone
youtube
Johnny Cash (February 26, 1932 - September 12, 2003)

Go tell that long tongue liar
Go and tell that midnight rider
Tell the rambler,
The gambler,
The back biter
Tell 'em that God's gonna cut 'em down
Tell 'em that God's gonna cut 'em down
The Man in Black, a name derived from his all black wardrobe. Johnny Cash was the embodiment of the Americana of old with a cowboy swagger and romantic outlaw presence. If there was a musician who had the tumultuous lifestyle of a rock star - it would be Johnny Cash who was addicted to amphetamines and barbiturates and started drinking heavily on tour during his early career. His dealings with drugs had almost led to a premature death in 1965 where he had started a forest fire that nearly killed him in his drugged state. He married twice and his second wife, June Carter who supported him throughout his on-off rehabilitation and his later conversion to Christianity and whose death preceded his by four months.
Here is Johnny Cash’s Folsom Prison Blues
youtube
So what did these two men have in common apart from being legends in American music? They both were diagnosed with Diabetes Mellitus - namely Type 2 Diabetes Mellitus. B.B. King died from congestive heart failure and diabetic complications and Johnny Cash died from diabetic complications - autonomic neuropathy associated with diabetes (he had earlier been diagnosed with the Multiple System Atrophy - Shy-Drager Syndrome)
Here is an excellent video that explains Diabetes Mellitus really well:
youtube
Diabetes Mellitus - high levels of blood sugar (diabetes - passing through: urine, mellitus - honey: sweet)
Insulin - decreases blood sugar level
Glucagon - increases blood sugar level
T1DM - relative lack of insulin, genetic, normally younger, treatment - insulin.
T2DM - insulin resistance, risk factors - obesity, lack of exercise, normally older, treatment - anti-diabetic medications
Symptoms: polyphagia - excess hunger, glycosuria - excess glucose in urine, polyurina - excess urination, polydipsia - excess thirst
Diagnosis: fasting blood glucose - after 8 hours fasting, random blood glucose - anytime, 2 hour post-prandial (oral glucose tolerance test) - 2 hours after 75g of glucose + HbA1c: 3 month average plasma glucose concentration (>48 mmol/mol (>6.5 DCCT%)


Diabetic Ketoacidosis
Medical emergency - complication of T1DM
Lipolysis - fats to fatty acids. Liver converts fatty acids to ketone bodies
Ketone bodies (acetoacetic acid, beta-hydroxybutyric acid) are acidic
Kussmaul respiration - exhaling CO2
Hyperkalemia - H+ in, K+ out of cells - K+ enters blood
High anion gap - difference in unmeasured ions in blood
Causes - stress, infection, adrenaline released, glucagon released
Ketone bodies break down into acetone (pear drops smell on breath)
Symptoms: nausea, vomiting, cognitive changes, cerebral oedema
Treatment: fluids, insulin, electrolytes (potassium)
Hyperosmotic Hyperglycaemic State
Medical emergency, more common in T2DM
High levels of glucose lead to water leakage from cells to blood vessels
Leads to extreme urination and hence dehydration
Treatment
T1DM
Multiple daily injection (basal-bolus) insulin regimens: regimen of choice as it offers more flexibility
Once daily insulin regimen
Twice daily mixed insulin regimens
Continuous subcutaneous insulin infusion/ insulin pump therapy
T2DM
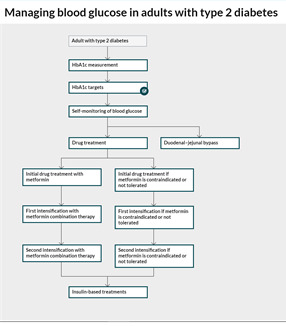
Metformin (caution if eGFR <45 ml/min/1.73m2, stop <30 ml/min/1.73m2). If contraindicated start with: DPP-4 inhibitor or pioglitazone* or sulfonylurea
Double therapy: Metformin + DPP-4 inhibitor or + pioglitazone or + sulfonylurea. If metformin contraindicated: DPP-4 inhibitor + pioglitazone, DPP-4 inhibitor + sulfonylurea or pioglitazone + sulfonylurea
Triple therapy: Metformin + DPP-4 inhibitor + sulfonylurea or metformin + pioglitazone or insulin based treatment. If triple therapy not tolerated: consider metformin + sulfonylurea + GLP-1 mimetic for patients with BMI >35kg/m2
*Pioglitzone - do not give if heart failure, hepatic impairment, DKA, bladder cancer, macroscopic haematuria
Better explanation of anti-diabetic drugs:
youtube
Further reading
http://www.diabetes.co.uk/diabetes_care/blood-sugar-level-ranges.html
https://patient.info/doctor/diabetes-mellitus-pro
https://pathways.nice.org.uk/pathways/type-2-diabetes-in-adults#path=view%3A/pathways/type-2-diabetes-in-adults/managing-blood-glucose-in-adults-with-type-2-diabetes.xml&content=view-index
0 notes
Text
Disney psychological disorders

Check out this cracking video, finally explains all those disney neurotics!
https://www.youtube.com/watch?v=bBK8uiDT5yw
0 notes
Text
Robin Williams

(July 21, 1951 - August 11, 2014)
Robin Williams was the face of the 80s and 90s for many of us. His innocent comedies of a more innocent time ranged from Mrs Doubtfire, Aladdin, Patch Adams, Good Will Hunting, Dead Poets Society, Awakenings, Jumanji and Night at the Museum. He always injected his idiosyncratic burst of crazy energy into a film which elevated a simple script into something hilarious and unique. Robin Williams was suffering from Lewy body dementia when he took his own life in 2014.
Here are two of my favourite scenes from Robin Williams.
Patch Adams (1998)
youtube
Awakenings (1991)
youtube
SciShow explains Lewy Body Dementia in a great way below:
youtube
3rd most common form of dementia after Alzheimer’s Disease and vascular dementia
Often mistaken for PD with slow movement, stiffness and tremor
Cause is unknown, only evidence for diagnosis is the findings of lewy bodies on imaging hence the recent breakthrough in knowledge.
Lewy bodies are clumps of protein formed from alpha-synuclein folding incorrectly
In DLB (dementia with lewy bodies), lewy bodies clump in cerebral cortex and the substantia nigra - the region of the brain responsible for coordination (hence the overlap with PD).
Hallucinations, loss of spatial reasoning, sleep disorders, cognitive and memory impairment - symptoms to distinguish from PD and are similar to Alzheimer’s Disease
Investigations:
History and examination: symptom assessment
Brain scans: MRI, CT, SPECT (single proton emission computerised tomography)
Treatment:
No current cure for DLB
Anticholinesterase inhibitors e.g. donezepil may help with symptom relief
Levodopa also used
Antipsychotic drugs are avoided due to side effect profile
Further reading:
http://www.nhs.uk/Conditions/dementia-with-lewy-bodies/Pages/Introduction.aspx
0 notes
Text
Why are chemotherapy and radiotherapy used in cancer?
youtube
o Chemotherapy uses anti-cancer chemicals for treatment of the whole body (metastasis). Can be administered through injection, intra-arterial, intra-venous, topical or orally. Long course treatment schedule (weeks to months). More expensive.
o Radiotherapy uses ionising radiation for treatment of a specific area of the body. Can be administered through external or internal injection and orally. Treatment schedule depends on severity. Cheaper than chemotherapy.
Side effects in both include fatigue, hair loss, lower immunity.
http://www.differencebetween.com/difference-between-chemotherapy-and-vs-radiotherapy/
2 notes
·
View notes
Text
For more great videos check out SciShow on youtube: https://www.youtube.com/user/scishow
Why is tape sticky?
youtube
o viscoelastic property - properties of both a solid and a liquid
o fluid properties of van der Waals bonds and electrostatic attraction (with dipoles in solids) make tape sticky
1 note
·
View note
Text
Why do suction cups stick?
Suction cups for use in cars are now everyday objects with uses of holding your GPS navigator or smartphone. But how do they actually work?

In scientific terms, gravity and friction are the two main forces that make it possible for suction cups to work. Gravity pulls the molecules in the air toward earth, creating atmospheric pressure of roughly 14.7 pounds per square inch at sea level. A good cup on a slick surface causes that pressure to be applied to the outside of the cup, pushing it down onto the surface. Friction keeps the cup from sliding.
The principle of pressure: P =F/A
P = pressure
F = Force
A = Area
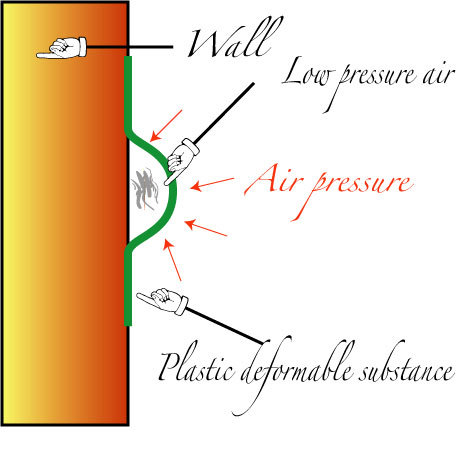
When suction cups are pressed against the car window, the air inside it is pushed out hence eliminating the pressure inside the cup and forming a partial vacuum which seals the cup tightly with no air allowing to come in. This is because the pressure of the cup is lower than outside, when the air pressure drops (i.e. opening the cup) then the air pressure on the outside becomes lower than inside.
The above equation can be reformed to a Force formula (F=AP) where the higher the area, the greater the force - hence bigger suction cups are more sticky.
youtube
Further reading:
https://www.youtube.com/watch?v=6_aQfFrcP6M
https://suctioncups.com/pages/suction-cups-101
1 note
·
View note
Text
Why does hair go lighter in the sun?

Hair is a collection of dead cells hence when the UV radiation in sun bleaches and oxidising the melanin (the pigment cells in cells) in the hair into a colourless compound hence giving a lighter appearance with no ability to produce any more melanin. (Previously it was thought that the outermost layer of skin was dead but since this has been proven not to be the case - hence when sun shines on skin - they can make more melanin hence a darker appearance with a tan.)
Also check out the links for more information about skin and the sun:
http://genetics.thetech.org/ask/ask180
https://www.sharecare.com/health/healthy-skin/is-outermost-skin-layer-dead
2 notes
·
View notes
Text
Why does hair go darker when wet?

This is all due to light striking an object (in this case - hair) and the light reflecting back into our eyes to give the illusion of colour. Some of this light is absorbed by the pigment of the hair.
In wet hair, the light reflecting off the surface of the wet hair reflects back to the inside surface of the water film where it is reflected back onto the hair again (total internal reflection) thus creating another chance for the light to be absorbed making the hair appear darker. Wet hair also clumps together with the hair strands coming closer together (electrostatic properties of water) which allows for less reflection off the hair and for more absorption.
For a better explanation check out the video below:
youtube
http://www.sciencefocus.com/qa/why-does-hair-get-darker-when-wet
http://wonderopolis.org/wonder/why-does-your-hair-look-darker-when-its-wet
https://www.thenakedscientists.com/forum/index.php?topic=9494.0
1 note
·
View note
Video
Check out more of TED Ed for interesting lessons http://ed.ted.com/
youtube
o involuntary spasm of the diaphragm causes closure of the vocal cords
o inhalation of air by spasm of diaphragm prevented by closure of the opening of the vocal cords (glottis) - causes hic sound
1 note
·
View note
Text
Why do anti-histamines make you sleepy?

It’s hayfever season again and the pollen count is particularly high this year. For hayfever sufferers there’s a fine line we tread of sneezing non-stop or being bunged up on anti-histamines which have the unfortunate side effect of making you tired. In fact many sleeping aids use antihistamines for this very purpose.
So why do anti-histamines make you tired? First of all, an anti-histamine is a type of drug that opposes the activity of the histamine receptors in the body. There are 4 different types of histamine receptor - the relevant histamine receptor we will discuss involved in allergy is the H1 receptor.
Histamines are nitrogenous compounds in our bodies involved in local immune functions and inflammatory responses with a central response in causing an itch (which is why we itch during an allergy).
Histamines are released when our immune systems detect a potentially dangerous foreign substance (an allergen) which triggers the release of white blood cells (cells that protect the body from infection): basophils - released in allergic response, and eosinophils - released in parasitic infections and in allergic response, and mast cells - a type of white cell which contain histamine that seek out cells with a histamine receptor.
Histamines induce an inflammatory response which: dilates blood vessels increasing the blood flow to the site of the injury. The blood vessels also become more permeable which allows proteins and white blood cells to seep into the damaged or infected tissue. It is these histamines that cause the symptoms associated with allergies: sneezing, itch (pruritus), chest congestion, wheezing.
These mast cells in the first instance of contact with an allergen become primed by releasing IgE which by the second time of contact with an allergen leads to the release of histamine. (see Figure 1)
Histamine release occurs when allergens (such as pollen in hayfever) bind to these mast cell bound IgE antibodies (immunoglobins = antibodies) which leads to the degranulation of the mast cells. IgE antibodies are the immunoglobulins involved in Type 1 hypersensitivity (immediate hypersensitivity) which is an allergic reaction provoked by re-exposure to an allergen.
Figure 1: IgE - Type 1 hypersensitivity
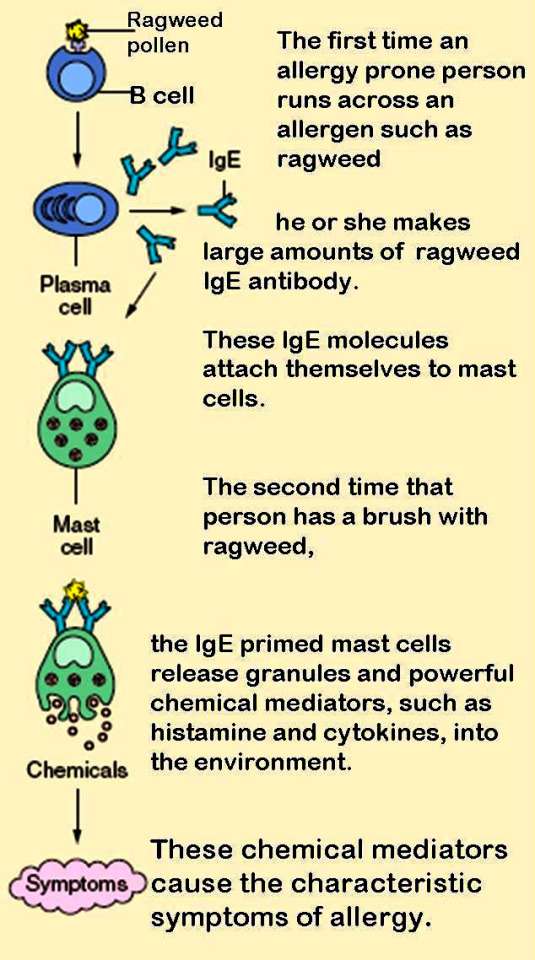
Anti-histamines work by blocking the the attachment of histamines to their receptors hence preventing them from carrying out their functions.
To understand why anti-histamines cause drowsiness firstly we need to understand the actions of histamines. (Figure 2 - stolen from wikipedia)
Figure 2: Function of Histamine
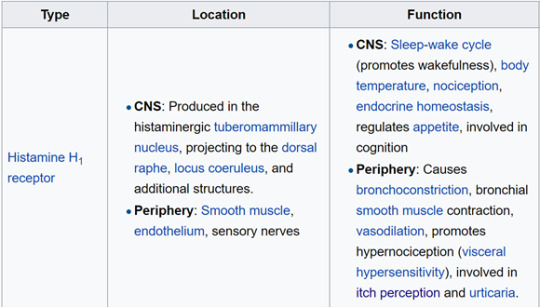
As you can see sleep-wake cycle is regulated by histamine - it is this disruption of histamine by anti-histamines by crossing the blood-brain barrier that leads to sleepiness. There is this property in all anti-histamines even in those marketed as non-drowsy - the effect is reduced somewhat but not entirely avoidable.
Popular types of antihistamine include:
Cetrizine
Chlorphenamine
Loratadine
References
https://www.livescience.com/41999-antihistamines-drowsy-benadryl-allergies.html
http://universityhealthnews.com/daily/energy/the-myth-of-non-drowsy-allergy-medication/
3 notes
·
View notes