#Egg Donor
Text
I started writing this letter to my mother because I realized that there are some things that I want to address. I probably won't give it to her; the letter is just a way for me to vent and move towards healing. But lately I keep asking myself, "Why am I still holding onto this anger about her favoritism?" The wound is just so deep that I feel like it will never heal.
When I was little, my mother liked my sister more than me. I was always the one getting reprimanded, scolded, criticized. My mother would even say to me, "You're just like your father! I hate that bastard." She never hit me but her words cut so deep. I could hear the disgust and anger in her voice, sharp as knives. She seemed to be annoyed by me every time I spoke, so eventually I stopped speaking. I buried my emotions deep within me until I could do so no longer. This is the result: a permanently burnt-out, disabled adult who has difficulty expressing their emotions, and even more difficulty recognizing what they need. This is one reason why I will never have children.
If you have kids, please don't make one your favorite. Please don't make one your scapegoat. Please love your kids equally. They didn't ask to be brought into this world, and they certainly didn't ask to have the genes of the ex-spouse that you despise.
#egg donor#sperm donor#disabled#mental health#autism#burnout#neurodivergent#adhd#trauma#complex ptsd#ptsd#shadow work#adult children of emotionally immature parents
19 notes
·
View notes
Text
Am I tripping or are they using some weird dark lipstick to light lip liner combo on Whitney’s lips? I keep thinking her lips are greasy, ashy or something.
When Kimberly started looking at the pros and cons of egg donation, I was hoping they talked about how bad the cons are. Ovarian cysts and endometriosis, a painful inflammatory disease that can cause infertility. If you’re really an unlucky soul, you may sustain debilitating nerve damage that will last a lifetime. it isn’t some easy lend your neighbor some eggs could of deal. It’s an important decision.
I swear Mindy write her female characters like the annoying ass white men she want to be with. Just with a mix of diversity to spice it up.
- One girl gets chlamydia and didn’t think it was important to inform her partners. She doesn’t even think she should inform them that she doesn’t want to be exclusive.
- Bela is a man eater and she treats Eric like shit. Uses men to get ahead. But it always end with it being endearing for her.
- And Kimberly is Kimberly 🙄
But I’m not ready to give up on it just yet. We will continue on….
8 notes
·
View notes
Text
107 days till top surgery pre-op appointment:
I am really considering becoming an egg donor, which will help cover the cost of my surgery in case my insurance doesn't. I'm looking into it and who knows, maybe I'll be chosen soon enough that I'll be able to get it before my surgery???
4 notes
·
View notes
Text
How to refer a friend to become an egg donor
Assisted reproductive technologies have become increasingly popular in recent years, as more people seek alternative methods to start or grow their families. One of these methods is egg donation, where a woman donates her eggs to another person or couple who may not be able to conceive naturally. If you know someone who may be interested in becoming an egg donor, you can refer them to a reputable egg donor agency.
Here are some steps you can take to refer a friend to become an egg donor.
Step 1: Do your research
Before referring your friend to an egg donor agency, it's important to do your research and find a reputable agency. Look for agencies that have been in business for several years and have a proven track record of success. You can also check online reviews and ratings to see what other people are saying about the agency. Additionally, make sure that the agency is transparent about their process and fees, and that they prioritize the health and well-being of the egg donor.
Step 2: Talk to your friend
Once you have identified a reputable egg donor agency, the next step is to talk to your friend about the possibility of becoming an egg donor. It's important to approach this conversation sensitively, as egg donation is a serious commitment that requires careful consideration. Be sure to explain the process thoroughly, including any potential risks and side effects. Encourage your friend to ask questions and do their own research before making a decision.
Step 3: Connect your friend with the agency
If your friend decides to move forward with becoming an egg donor, the next step is to connect them with the egg donor agency. You can either provide your friend with the agency's contact information or offer to make an introduction yourself. Make sure that your friend understands the process and knows what to expect when contacting the agency.
Step 4: Follow up with your friend and the agency
Once your friend has connected with the egg donor agency, it's important to follow up with both your friend and the agency to ensure that the process is going smoothly. Check in with your friend regularly to see how they are feeling and offer support as needed. Additionally, make sure that the agency is communicating with your friend effectively and that they are addressing any questions or concerns that may arise.
Step 5: Celebrate your friend's decision to become an egg donor

Becoming an egg donor is a selfless and meaningful decision, and it's important to celebrate your friend's choice to make a difference in someone else's life. Offer your friend words of encouragement and support throughout the process, and let them know how proud you are of them for taking this step.
Conclusion
Helpcreatefamilies is a reputable agency that specializes in facilitating the egg donor referral process. By partnering with Helpcreatefamilies, you can ensure that your friend receives the highest level of care and attention throughout the process. With a strong focus on empathy, knowledge, communication, attention to detail, relationship-building, flexibility, and work ethic, the professionals at Helpcreatefamilies are dedicated to helping families achieve their dreams of parenthood. If you know someone who may be interested in becoming an egg donor, referring them to Helpcreatefamilies can be a powerful way to help them start or grow their family while ensuring a positive and meaningful experience for all involved.
2 notes
·
View notes
Text
Would You Like to Ask Me Something?
Being Donor Parents
TABLE OF CONTENTS
Chapter 1 Prologue
Chapter 2 The Dry Facts
Chapter 3 Who Needs a Donor?
Chapter 4 Choosing a Donor
Chapter 5 Fertility Treatment
Chapter 6 Adoption
Chapter 7 Wonderful Titles
Chapter 8 The Birth
Chapter 9 Maternity Leave
Chapter 10 The Little Child
Chapter 11 The School Child
Chapter 12 The Teenager
Chapter 13 Why Should We Hide Anything?
Chapter 14 Epilogue
Chapter 15 Thanks
Chapter 1 Prologue
We are in the break room at my workplace - a small room equipped with a sink and the inevitable large coffee machine, a round table with five closely placed chairs, small lockers for our bags, and a shelf filled with papers of both official and personal nature. The neonatal department at a hospital in Denmark is our workplace. Here, sick newborns and premature babies are treated.
I am sitting here with an open lunchbox in front of me, alongside two of my nurse colleagues, a nursing student, and a midwifery student. The atmosphere is, as usual, light, and relaxed. The conversation flows freely with a mix of professional reflections and various personal discussions. Everything is shared here, from challenging situations in the department to everyday concerns at home, dinner plans, and who last went on a date. No topic is too sensitive or too trivial to be discussed in the break room.
The midwifery student looks a bit embarrassed, seeking some reassurance from the nursing student, who seems to have prepared the question with her. "Would you like to ask me something?" I say playfully, fully aware of what awaits me. The students know that I'm lesbian. It was mentioned by a colleague, but it's not something I try to hide. I'm open about my sexuality, though without emphasizing it. "But you can only ask me something I can answer..." I wink at them, and the atmosphere immediately becomes more relaxed.
"Are you the biological mother of your children?" asks the midwifery student cautiously.
"Yes, I'm the one who has carried both of my children," I reply without the slightest hint of being affected, as I've heard this question so many times before.
"May I ask you something else?" the midwifery student continues, clearly nervous about having crossed my boundaries.
"Yes, as long as I can still answer it." I smile again at the students. I'm ready for the next question, which always follows the first one.
"Do your children have the same father?" The students wait eagerly for an answer to something they're not familiar with. And here I am – open and willing to answer all their curious questions.
"My children don't have a father. But they do have the same donor, if that's what you mean!" The conversation about donor parents and donor-conceived children begins.
Here starts the journey into being donor parents, a journey that this text will explore and reflect upon. It is aimed at both donor parents, families, and professionals, in the hope of creating greater understanding and openness about this particular life situation.
At the same time, the assignment is aimed at you, who have donor parents in the family, including grandparents or other relatives of parents to a donor-conceived child. My hope is that this assignment will provide you with a deeper insight into donor parenthood and thus enable you to better support this relationship. I also hope that it will inspire you to dare to talk to your loved ones about being or potentially being donor parents. Your openness and respect as relatives have a significant impact.
Furthermore, the assignment is addressed to you, who are professionally involved with parents who have or are going to have a donor-conceived child. This includes professionals such as gynecologists, midwives, nurses, educators, social workers, and others. I hope that it will provide you with insight into some of the pitfalls that may arise when encountering donor parents as a professional. I hope that it will inspire you in your future relationship with donor parents.
It's important to emphasize that regardless of your relationship with the donor parents, your approach and actions will have an impact on both the donor parents and, importantly, the donor-conceived child. I have endeavored to write in an accessible language, but there will also be some technical terms. In particular, there will be descriptions of humorous and comedic experiences.
It stems from my thoughts and experiences as a prospective parent and up to now, when the children have become teenagers. My reflections and experiences about parenthood are based on my marriage with the children's other mother, which, however, ended when they were very young. Later reflections stem from a mixed life as a single parent with periods of dating, where I have had the opportunity to experience other donor parents up close.
Additionally, it is based on my observations as a nurse in a neonatal department over the past 20 years. Here, in a professional context, I have encountered donorship in many different forms among the co-admitted parents.
I also have several donor parents in my social circle. They will not be directly quoted, but their experiences will contribute to my general observations. When you read the assignment as my friend or acquaintance, remember that it's not you I'm directly portraying, but rather a fusion of my own experiences and observations.
I would also refer to the sperm bank Cryos, as it is the largest sperm bank in Denmark and has provided the sperm for my two children as well as for many public and private fertility clinics.
I am very open about my thoughts and feelings. I have always felt it as my duty as a mother to donor-conceived children to demonstrate great openness and integrity. My children did not choose to come into the world via donor conception, and if I, as a parent, find it taboo to talk about, how will my children feel?
As a wise acquaintance once said: "When we begin to talk about things, normalize and demystify them, it actually becomes even easier for us to act on them." - Johansen - LIVNESS
Remember, it's not a 'one size fits all'. Some of what's described you may recognize, while other parts may be difficult to relate to.
My hope is to create greater openness about being a donor parent, so that all involved parties dare to ask and answer questions. I have attempted to discuss the topic both seriously and humorously.
So, would you like to ask me something?
Chapter 2 The Dry Facts
In 2020, new figures showed for the first time that more than 10% of a birth cohort were conceived through fertility treatment. This means that every 10th child was not conceived in a regular double bed, but rather in a hospital or fertility clinic.
For individuals experiencing involuntary infertility in Denmark, there is the option to use a donor, either in the form of sperm donation or egg donation. It has been illegal for many years to use so-called double donation, where both eggs and sperm from a donor are used. Couples where both the woman and the man experience fertility problems have therefore had to seek treatment abroad to get help with double donation. Fortunately, this has changed, and such couples now also have the opportunity for treatment in Denmark.
In this chapter, I really wanted to provide you with precise numbers for how many children are conceived using donor sperm or donor eggs. Unfortunately, it has proven to be an impossible task. The fact is that there is no centralized database or published statistics that accurately register the number of children born through the use of donor sperm or donor eggs in Denmark. This is partly due to the strict rules of anonymity and confidentiality surrounding donations in Denmark, making it difficult to collect such information. Therefore, we must acknowledge that even though it is of great interest to know the number of children born through donor conception in Denmark, unfortunately, it is something for which we do not have precise data at this time.
During my research, I have attempted to find numbers from both Statistics Denmark, the Danish Fertility Society, the Danish Health Data Authority, and other organizations that might be expected to keep data and statistics on newborns in Denmark. I have even received help from colleagues in the healthcare system who are trained to find numbers in various statistics. Unfortunately, we have all had to conclude that these specific numbers do not exist.
I have been in contact with the sperm bank Cryos, which is Denmark's - actually the world's - largest sperm bank. Cryos supplies sperm to fertility clinics both in the public and private sectors. One of the reasons I chose to contact Cryos specifically is that they provided the donor sperm for the conception of my children. I hoped that they might be able to provide information about the number of children born using their sperm, but unfortunately, that was not possible either.
Some of the questions I wanted answers to from Cryos included, among other things, the number of children born annually in Denmark using donor sperm from them. Unfortunately, they do not wish to answer this question as their success rate for the use of sperm donation is considered a trade secret.
Cryos, however, is willing to disclose that globally, they have contributed to the birth of more than 70,000 children since the company's inception in 1987. This figure is an impressive illustration of the significant role they play in donor sperm and fertility treatment on a global scale.
Since none of the sperm banks in Denmark wish to disclose their success rates and thus the number of children they help bring into the world, we must acknowledge that it is impossible to find the precise number of children born with donor sperm or donor eggs in Denmark. This lack of data makes it challenging to obtain a complete picture of the extent of the impact of donor conception on fertility treatment in the country.
When a couple has received help from a donor to conceive a child, they are not obligated to disclose this. However, there is an exception for lesbian couples and single individuals. This is because the law requires that a man be registered as the father on the child's birth certificate. If there is no male partner present due to the use of a donor, this must be indicated by presenting a donor certificate from the sperm bank.
Today, a child has the right to know their origin via the birth certificate, and it is not possible for a woman to omit listing the father's name on the birth certificate. If there is doubt about paternity, and there are potentially multiple candidates, there are several sections available on both the front and back of the birth certificate to list the names of the different candidates. It is a legal requirement that the mother list the current candidates for paternity.
If there is doubt about paternity after the child's birth, and the potential candidates do not acknowledge paternity, a paternity test may be conducted to determine the child's biological father.
A heterosexual couple can avoid the particular challenge regarding the registration of paternity on the birth certificate. The man's name is automatically entered as the father, regardless of whether he is the biological father or not. Therefore, it will not be apparent whether the couple has been required to use a donor.
In the case of egg donation, it will also not be indicated on the birth certificate, as the pregnant woman is considered the mother, regardless of whether she is the biological mother or not. This reflects a difference in legislation that affects how parenthood is registered in heterosexual couples compared to lesbian couples and single individuals who have used donor sperm or donor eggs.
It is extremely challenging to extract precise figures from a database when it is not mandatory to indicate donation on the birth certificate, and when sperm banks do not wish to disclose information. This makes it an estimation to determine how many children have been born via a donor, whether it is an egg donor or a sperm donor.
Cryos has disclosed how many children each individual donor may contribute to with them. Since Cryos is a global company, these rules vary from country to country due to the different laws and regulations in the field. In Denmark, the rules stipulate that a donor may supply sperm to a maximum of 12 different families. In practice, this means that a donor may have more than 12 children, as it is permitted to create siblings within these 12 families. Therefore, statistically, there may be more than 24 children from the same donor in Denmark.
Cryos har implementeret en regel, hvor deres donor maksimalt må bruges af 25 familier på tværs af landegrænserne. Disse maksimale grænser er primært blevet fastlagt af to hovedårsager. For det første er der naturligvis risikoen for indavl, selvom denne risiko er minimal i lande, hvor befolkningen er stor. Den primære årsag er dog, at hvis en donor skulle have en skjult sygdom, som hverken donor eller sædbanken kender til, så er det af afgørende betydning, at vedkommende ikke er donor til alt for mange børn. Dette sikrer en forsvarlig praksis og reducerer risikoen for eventuelle negative konsekvenser for børnene og deres familier.
At the Danish Health Data Authority, an annual report on "assisted reproduction" is compiled. In 2021, 53,000 Danes between the ages of 25 and 44 experienced difficulties conceiving – this corresponds to 11% of all in that age group, or one in five of those who have attempted to conceive. Approximately 37,560 Danish women received treatment for infertility. Unfortunately, there is no guarantee of success just because one has started fertility treatment and thus receives assistance in becoming pregnant. In fact, only 17% of initiated fertility treatments result in a completed pregnancy. Roughly, this means that approximately 6,170 children were born in 2021 with the assistance of fertility treatment at Danish fertility clinics or hospitals. Of these children, 730 – equivalent to 12% – were born to single women, 5% were born to women with a female partner, and 83% were born to women with a male partner.
However, not all couples undergoing fertility treatment require a donor. First and foremost, the aim is to use the couple's own genes to conceive a child if possible. However, for various reasons, this may not always be possible, and in these cases, treatment with the help of a donor is pursued. The reasons why couples cannot use their own genes can vary and include a range of medical, genetic, or reproductive challenges that necessitate the use of donor sperm or donor eggs to achieve pregnancy and childbirth.
In 2019, approximately 1,000 Danish women began fertility treatment with donor eggs. Of these treatments, around 25% resulted in a clinical pregnancy. Being clinically pregnant means that heartbeats can be seen on ultrasound scanning at 7-8 weeks. This is early in the pregnancy, and unfortunately, there is still a risk that the fetus may not develop normally, and the pregnancy may be lost.
When the Danish Health Data Authority combines their data with the National Patient Register, it is revealed that only about 19.5% of women who became pregnant via egg donation completed the pregnancy. This means that 212 children were born with the assistance of egg donation with treatment initiation in 2019. It is important to note that these figures reflect the complex challenges that women undergoing fertility treatment with donor eggs may experience during pregnancy.
Previously, the donor eggs came from women who were already undergoing fertility treatment and had an overproduction of eggs compared to their own needs. These women were then asked if they would donate their eggs, albeit without receiving significant compensation. Fortunately, this has changed today, where egg donors receive approximately 7,000 Danish kroner as compensation. This amount is intended to cover the costs and time the woman incurs in connection with the treatment required to produce extra eggs and have them retrieved. The process of being an egg donor without undergoing fertility treatment oneself is a somewhat complicated process. It involves hormone therapy to stimulate the ovaries to produce more eggs. Hormone therapy involves injections, which the woman must learn to administer herself at home. The egg retrieval itself is a procedure performed by a fertility doctor under local anesthesia. After the procedure, the woman should rest for the remainder of the day.
It is truly important to acknowledge the significant effort and generosity of women who choose to donate their eggs without undergoing fertility treatment themselves. The process of hormone therapy and egg retrieval can be physically and mentally challenging, requiring considerable effort and often personal sacrifices on their part. The compensation they receive is a form of recognition of this effort and the loss of time and potential work absence they may experience. It is crucial to appreciate and support women who choose to contribute in this way to help others fulfill their dream of having children.
According to the Danish Health Data Authority, nearly 8,500 inseminations with donor sperm were performed in Denmark in 2019. However, it is important to note that 55% of these inseminations were performed on foreign women. Therefore, there were approximately 3,800 Danish women who were inseminated with donor sperm in 2019. Of these inseminations, 561 resulted in a clinical pregnancy. The Danish Health Data Authority has also cross-referenced their own data with the National Patient Register. This allows for a real number of children born in cases of inseminations with donor sperm at fertility clinics. Of the initiated inseminations with donor sperm in 2019, the result was 592 children. The reason for the number of children being greater than the number of pregnancies is that some of the pregnancies consisted of twins and triplets.
Home insemination is generally less common in Denmark compared to certain other countries like the USA, where it is often the primary option for insemination with donor sperm, and where the costs are borne by the individual. In Denmark, many prefer to have insemination performed at a fertility clinic, where they can benefit from professional guidance and monitoring throughout the process. This also ensures that the procedure is carried out correctly and under optimal conditions for success.
Yes, it's a challenge that transparency regarding the use of donor sperm in other forms of assisted reproduction besides insemination is not as readily available. This could be due to a lack of reporting or registration of this information in public databases, making it difficult to get a complete picture of the use of donor sperm in these procedures. It underscores the need for more comprehensive data collection and reporting within the field of assisted reproduction to improve transparency and understanding of practices and outcomes.
It sounds sensible and necessary to have clear guidelines and standards to ensure that sperm donation is conducted in a responsible and safe manner. These guidelines from the Health Authority provide both sperm banks and potential donors with a solid framework to work from and contribute to maintaining the quality and safety of donated sperm. It is also important that donors are able to meet certain criteria to ensure that the donated sperm meets the necessary health and quality standards, while also understanding the legal, ethical, and medical implications of their donation.
At Cryos, prospective sperm donors must be between 18 and 45 years old and undergo a comprehensive screening program. This program assesses the donor's mental, physical, and genetic conditions. Potential donors are disqualified if they suffer from certain diseases, have serious hereditary disorders in the family, or do not know their genetic background, such as if they are donor-conceived themselves or adopted. There are also other specific and intimate requirements that are not detailed
Sperm donors are generally encouraged to maintain a healthy lifestyle to ensure optimal sperm quality. This includes a nutritious diet, regular exercise, and avoiding harmful habits such as smoking and excessive alcohol consumption. A healthy lifestyle can help improve both the quantity and quality of the donated sperm, which is crucial for the success of assisted reproductive technology.
Sperm donors have the opportunity to donate sperm 1 to 2 times a week, as long as sperm quality is not negatively affected. For each donation, the donor is compensated with up to 500 Danish kroner. With a bit of quick math, two visits to the sperm bank per week can quickly turn into a significant additional income each month. It is therefore not surprising that many students see this as an attractive income opportunity.
A more accurate conclusion regarding the number of donor-conceived children in Denmark would be that in 2019, 592 children were born following insemination with donor sperm and 212 children were born through egg donation. In addition to this, there is an undisclosed number, which includes the use of donor sperm in artificial insemination and assisted reproduction abroad. This may include women and couples who do not meet the Danish requirements for fertility treatment. Based on this, I estimate that approximately 1000 children are born in Denmark annually with the help of a donor. Compared to the approximately 61,000 children born in both 2019 and 2020, donor-conceived children thus account for around 1.6% of all newborns in Denmark. With this proportion, on average, there is one student who is donor-conceived in every other primary school class. This includes both children who are aware of their donor origins and those whose parents have chosen not to disclose it to them.
Chapter 3 Who Needs a Donor?
There's no doubt that deciding to have a child, whether as a couple or as a single individual, is one of the most significant decisions a person will make in their lifetime. And for a same-sex couple, it's not as simple as deciding one Sunday evening to start trying for a baby. No, the decision becomes a significant one, requiring much contemplation.
This holds true for women without a partner who aspire to become mothers as well.
Living in a lesbian relationship like mine, it's obvious that we needed a donor to expand our family. Currently, reproduction requires both an egg and sperm to conceive a child. But who knows? Perhaps the future and ethical considerations will open the door to the possibility of creating an embryo from two eggs.
However, in our case, we had plenty of eggs, but deciding where the sperm would come from required careful consideration.
Yes, we were faced with the option of seeking help from a man we already knew or choosing an anonymous donor, someone without the desire for further obligations or contact with the child beyond helping us become parents. It's noteworthy that both these types of men, willing to assist without further commitments, do exist.
In our considerations, we also pondered the possibility of seeking help from a gay man or a gay couple, like us, who desired to become parents. Both with a known donor and with a gay man, the child would know the identity of the man who would be the father of our future child. I deliberately use the term "father" here because it would be a man whose identity the child would know and likely develop some form of relationship with. For me, there's a significant difference between a donor whom the child has no relationship with or knowledge of and a father, whose identity the child knows, regardless of the closeness of the relationship.
However, for us, there was no doubt that we did not want to use a man we knew. There were several reasons for this choice.
If we were to have used a man from our social circle or a man simply wanting to donate sperm to our family project, we were concerned about the legal challenges that could arise. Therefore, we would have had to demand that he relinquish parental rights over the child and not seek visitation. This was a requirement I didn't want to impose on anyone. Personally, I believe that few men, immediately after becoming a father—perhaps for the first time—don't wish to be part of their child's life anyway. For us as prospective parents, it was a significant concern and frightening to contemplate if the donor later sought visitation and parental rights. We deemed this concern an unnecessary burden to carry for an unknown duration.
Derudover var hele tanken om at skulle inseminere sig selv eller sin partner med sæd direkte fra en kop, som en måske ukendt mand lige havde leveret, ikke særlig tillokkende. Denne forestilling var ikke helt behagelig for mig. Jeg foretrak klart, at sæden lige havde været igennem et laboratorium og var blevet undersøgt grundigt, før den var klar til inseminering.
The thought of using a gay man or a gay couple in our project has never been entirely remote to me. This is primarily because I have great sympathy and compassion for gay men, who have a much harder time expanding their families than us women. In principle, we can go out on a Friday night and see if we can find a willing "volunteer" for unprotected intercourse, or we can use one of the many other ethically sound ways to acquire sperm, such as through fertility clinics. But gay men can't just find an egg, and certainly not a uterus, to expand their family. They must take the much more cumbersome route through a surrogate mother, or they must start as co-parents, where they can have children with a woman who also desires children. The thought of starting our parenthood as co-parents was the primary reason we didn't choose to have children with a gay couple. As prospective parents, we couldn't imagine having to share our newborn with another set of parents. I realize this may sound very selfish, and I actually believe my stance could have been different if I had known a gay man or couple in the same situation as us, with a burning desire to start a family. But that wasn't our situation.
The choice, therefore, was that we needed a donor.
We were now embarking on all the many considerations involved in starting fertility treatment. One of our first decisions was who would carry the child. For us, however, there was no doubt that it would be me. The whole idea of fertility treatment, hormone treatments, repeated visits to the gynecologist, bodily changes, and especially childbirth, was quite daunting for my ex-wife and certainly not something she desired.
I have always been interested in experiencing pregnancy and childbirth someday. However, it has always been important to me that the circumstances were right before embarking on the baby project. That is, I wanted a partner who also wanted children, as I have never wanted to be a single mother.
If I had a partner who also wanted to be pregnant, I could easily imagine us both carrying a child. I have always felt that my desire to have children would be the same whether I was a biological mother or not. The idea of creating new life and feeling a child grow inside me has always fascinated me. I have no doubt that I would have pushed to experience this experience myself. Although it would have been a great experience to follow my partner's pregnancy, I would be sorry not to have experienced it on my own body, at least once.
When you're a relative, colleague, friend, or healthcare professional, it's important to be aware that there can be many reasons why a person may or may not want to carry a child.
The first question that always arises is whether one desires to be pregnant. Personally, I believe that among lesbian women, there are more who do not have this desire compared to heterosexual women. The reasons for this can be many. One of them can be one's perception of one's body and gender. Another factor can be the concern about the physical changes that pregnancy entails. Many lesbian women find this change daunting and unappealing. Additionally, as a lesbian couple, there are other options for becoming parents without having to carry a child compared to what heterosexual women face. However, these observations are personal assumptions, and there are surely countless other reasons for choosing not to be pregnant.
Furthermore, some women's bodies may be challenged in various ways. This can include physical injuries, such as back problems and other mechanical conditions, which would make pregnancy difficult, or where pregnancy could exacerbate the injuries further. For these women, it will always be a balancing act between the possible discomforts and permanent injuries that pregnancy and childbirth can bring, and the desire to be a biological and gestational mother.
Through many years of working as a nurse in a neonatal unit, I have personally seen some women who have been seriously injured by pregnancy and childbirth. In most cases, this could not have been foreseen in advance. Either because the woman did not know she was latent sick, or because her body reacted strongly to pregnancy or suffered injuries during childbirth.
It is heartbreaking to witness when a new family, which should have been filled with joy over the arrival of the little one, instead has to deal with anxiety, uncertainty, and pain due to the mother's health. The idea of how the formation of their new family should be is shattered when the woman cannot be the present mother she wanted to be, perhaps because of her own poor condition. It is heartbreaking to see when the woman may not even be able to be with her child because of her condition. At the same time, the partner faces a huge challenge in dealing with both the illness of their loved one and the needs of the new family. This situation puts immense pressure on the partner, who is constantly torn between helping their partner and taking care of the new baby. It is certainly not a situation one would wish for any new parents.
It is impressive to see when women, despite their poor health, choose to become pregnant, even though pregnancy may pose a direct risk to their lives. I have great respect for them if they choose to forgo a pregnancy and perhaps even decide not to have children if the risk of complications is so great that it will significantly affect their lives after childbirth. In these cases, the decision about pregnancy is extra difficult and should be carefully considered. In a lesbian relationship, there will still be the possibility for the other partner to carry the pregnancy, but for heterosexual couples where the woman's health does not allow pregnancy, adoption may be the only option to fulfill the dream of expanding the family.
I have great respect for the group of prospective parents who are concerned about passing on specific undesirable genes to their children. For these parents, the decision to have biological children is often accompanied by many considerations and concerns, and sometimes it can lead to them choosing not to have children with their own genes. It is certainly not an easy decision to make, as it involves giving up passing on something that may have affected one's own life.
It is true that many men today experience problems with sperm quality, and research suggests that this problem does not seem to be decreasing in the future. About one-third of men in Denmark today have such poor sperm quality that there is very little or no chance of natural reproduction at home. The causes of poor sperm quality can be diverse and can affect men all the way from the fetal stage. What a man eats and is exposed to during life can also affect sperm quality. Additionally, unhealthy habits such as excessive alcohol consumption and use of harmful substances in youth can also increase the risk of poor sperm quality later in life.
Men can experience fertility issues that necessitate treatment, and in some cases, a direct sperm donor may be required to facilitate family expansion. Through fertility treatment, sperm from a donor can be used to fertilize a woman's eggs, allowing for pregnancy even when the man's sperm quality is insufficient for natural reproduction. This option is invaluable for couples facing challenges with male fertility.
There still exists a certain level of taboo surrounding men's sperm quality and fertility issues in general. This may partly stem from the traditional perception of masculinity and male fertility. Many men feel a sense of shame or inadequacy if they experience problems with their sperm quality. This stigma can hinder openness and discussion on the topic.
However, it's encouraging to see an increasing focus on men's fertility and the options for treating fertility problems in men. Research in this area is advancing, leading to more and more possibilities for medical intervention and treatment. It's important to break down taboos and foster an open dialogue about fertility so that both men and women feel supported and informed when facing challenges in achieving pregnancy.
Breaking taboos surrounding poor sperm quality and male fertility can contribute to a more open conversation about the use of sperm donors and the child's right to know their genetic origin. It's crucial to recognize that fertility problems are not a reflection of a man's masculinity but rather a result of various factors, including genetics, environmental influences, and lifestyle.
By promoting openness and honesty about these topics, we can create a more supportive and informed environment for couples facing fertility challenges. This can also help ensure the child's right to know their genetic heritage and establish a healthy foundation for their identity development. This is an important ethical issue that requires careful consideration of various concerns and values.
And then there are women. And just like with men, women can face many different reasons for not being able to conceive. For a woman, several factors must come together for a child to be conceived. In the process, there's the egg itself, which must be produced and matured. Then the egg must be able to travel freely through the fallopian tubes and meet the strong, chosen sperm cell. Fusion must occur. And finally, there must be an environment in the uterus where the egg has the opportunity to implant and undergo an amazing development, from two cells meeting to a viable baby.
In this process, many challenges and complications can arise. When a couple cannot achieve pregnancy naturally and the man's sperm quality is sufficient for reproduction, it often requires a more thorough investigation to identify the reasons for the woman's inability to conceive. This may involve a comprehensive review of her reproductive health and possible factors that may affect her fertility.
It is not uncommon for women facing these challenges to undergo prolonged and demanding fertility treatment. This may involve various forms of medical intervention, such as hormone therapy, egg maturation, or even assisted fertilization technologies like IVF. This process can be an emotional and physical ordeal, and it's important for women to receive support and guidance along the way.
It's important to remember that regardless of whether fertility problems lie with the man or the woman, it's always the woman who undergoes the most extensive and invasive process, both physically and mentally. Fertility treatment requires a significant amount of strength and endurance from both the man and the woman, as well as from the relationship as a whole. It's a challenging journey that can affect all aspects of their lives and relationships, and it's important for them to support each other throughout the process.
I have great respect for women who choose to opt out when they don't want to subject their bodies to fertility treatment and pregnancy, or who simply don't want children. Unfortunately, I've seen prejudices, discriminatory questions, and deep wonder, both from close relatives and the general environment, directed at these women's decisions. It crosses the line when other people say to a woman, "You're only a real woman when you've been pregnant and had children!" or "Aren't you afraid of being lonely when you get old?" It's hurtful and demeaning when others try to judge when a woman is a real woman or how she should live her life, whether she doesn't have children due to fertility problems or by choice.
Even though the comments are not made with ill intentions, we all, including myself, should remember that we shouldn't be judges of others' lives and the choices they make. There can be many personal reasons for our lifestyles that we don't want to share with others. When as relatives, friends, or colleagues, we push and ask if others aren't soon going to have children, I know we do it because we want what's best for them. Maybe we ourselves have the perception that children are the best thing in the world. But as a colleague, friend, or even as a family member, we don't always know if a couple is struggling with fertility treatment, or if they simply haven't succeeded in getting pregnant. It may also be that the couple, for various reasons, has chosen a childless life.
I generally advocate for openness and believe that it's often the best approach in most situations, but I and everyone else must respect that we don't always know what's best for others. We also don't always know the reasons behind their actions. And it's not our right as relatives always to demand to know it. Many couples choose not to tell their surroundings that they're undergoing fertility treatment. This may be because fertility problems are very personal and intimate matters. However, I am convinced that there are clear benefits to being open about undergoing fertility treatment. Several of the treatments require being present on specific days and times, and I believe that one's workplace would be very understanding of their absence if they were open about the reason. Additionally, the treatments often entail hormonal and psychological challenges. I imagine that one's surroundings would also show greater understanding if they knew the reason for one's mood swings and other reactions resulting from the struggle to have a desired child. In general, I believe that everyone in one's surroundings would show greater understanding and patience if they were aware of the reason, rather than having to guess it.
Unfortunately, there are women who don't manage to have children before they reach their "expiration date." Today, we often postpone having children until we are much older than our bodies are actually designed for. If it were up to our biology, we would probably have children around the age of 20. But before we get there, we need to have our careers in order, find a partner, establish ourselves in a house, and take care of all the practicalities. By the time all of this is in place, we have unfortunately gotten older, and our ability to reproduce has begun to decline.
I can relate to that. I myself wasn't ready to have children in my 20s. At that time, I only had my education sorted out, but there was still much I wanted to explore about life, my sexuality, and most importantly, finding the right partner to start a family with. So, I also ended up being in my thirties before thoughts of children really began to take shape.
Some women experience that their biological clock runs out before they're ready to have children. But fortunately, women today have the option to receive an egg donation from another woman, giving them a chance to fulfill their desire for motherhood. In Denmark, there are certain ethical guidelines regulating the age of women who can receive fertility treatment. Some women and couples who are denied treatment in Denmark due to their age seek opportunities abroad. The rules are often more lenient there, but instead
es, it is certainly an important ethical question whether it is responsible to bring a child into the world when parents are older. It involves a significant amount of reflection and planning from the parents' side to ensure that the child receives the necessary care and support, even if the parents become weak or pass away while the child is still young. A solid social network and the possibility of alternative caregivers are crucial factors in this consideration. It's about considering the best interests of the child and ensuring its best opportunities for well-being and development, regardless of the parents' age.
In a lesbian relationship, where one partner has undergone fertility treatment without success, some couples choose to begin treatment with the other partner. Although, in principle, having two female bodies to attempt to achieve pregnancy may be advantageous, it's important to understand that the decision to start fertility treatment is not made lightly. It's an intense and challenging process where the woman's body is subjected to hormones, and there can be pain during egg retrieval as well as mood swings ranging from frustration to depressive symptoms.
After undergoing prolonged fertility treatment, especially if it does not result in pregnancy, it significantly burdens both the body and the mind. The emotional weight and grief are often present, whether the treatment succeeds with the other partner or not. It's important to acknowledge and support the woman who has undergone the treatment and understand the complexity she has experienced in trying to achieve pregnancy.
And then there's the large group of couples suffering from involuntary childlessness, where the exact cause cannot be identified. Many of these couples also try to use either donor eggs or specifically donor sperm in hopes of achieving pregnancy. In certain cases, it turns out that the use of a donor is the key to achieving family expansion.
There are incredibly diverse reasons why someone may need the help of a donor to have a child. As a relative or friend of an expectant couple who have been open about using a donor, it's important to know that the use of donors in Denmark is subject to some good, and for some, slightly strict, ethical guidelines. However, these guidelines help ensure that couples have a certain level of security regarding the quality and ethics behind the donation.
Chapter 4 Choosing a Donor
There's no doubt that choosing to become a donor must be as significant a decision as choosing to use a donor. Deciding to let one's genes be used without having control over when and to whom must require a lot of consideration. The idea that there are people out there who contain half of one's genetic material and might resemble one both physically and mentally is quite profound. Therefore, I have no doubt that the majority of those who choose to be donors do so for ideological reasons. Sperm banks also don't hide the fact that when you choose to be a donor, you're helping others fulfill their dream.
Of course, I can understand if particularly young men are tempted by the opportunity to earn some extra cash, especially when it comes to financing their studies. Let's face it: it's well-paid work for little effort!
Being a donor as a woman entails working considerably harder, both physically and mentally, for one's earnings. When a man wishes to donate his sperm, there are no requirements regarding appearance. Sperm banks may have branches spread across the world, and therefore, there is a need for sperm donors of many different ethnicities, heights, and builds. There are even periods where sperm banks run campaigns to recruit new donors of a specific ethnicity, as there is high demand for a particular appearance.
When choosing to become a sperm donor, one can do so anonymously or as an open donor, but what does that mean?
As an anonymous donor, also known as a non-ID release donor, the donor is guaranteed anonymity to both donor parents, donor-conceived children, and other parties who might be interested in knowing the donor's identity. The sperm bank is not allowed to disclose information that could identify the donor. As a non-ID release donor, one does not have the opportunity to identify one's donor-conceived children, and therefore, one has also waived the possibility of contacting any potential donor-conceived children.
As an open donor, also known as an ID release donor, one gives permission for the sperm bank to disclose one's identity information to one's potential donor-conceived children. The donor-conceived child will thus have the opportunity to contact the donor. Typically, the child is given the opportunity to receive this information when they reach the age of 18.
It is correct that if one or more children are born with genetic diseases, the donor to these children will be investigated, regardless of whether it is a non-ID release or ID release donor. However, the donor is not legally responsible for any genetic diseases, as long as they have provided accurate information during the screening program to be approved as a donor. It is always a sad situation when a child suffers from a genetic disease and the challenges it entails. Therefore, it is also reasonable to have limitations on how many children a donor may produce.
It is worth noting that when a woman begins fertility treatment, she does not need to undergo the same screening program as the donor. Personally, I would be unsure if I could pass such a screening program. I also have some ancestors' genes that I do not necessarily wish to pass on to my children, but at the same time, my genes are not so poor that they are considered inappropriate to pass on.
For heterosexual couples who spontaneously decide to have children, it is likely that they may not necessarily have an in-depth conversation about their genetic heritage.
As a known donor, one also has the option to determine how much information donor parents and donor-conceived children should have about oneself. One can choose to provide basic information such as hair color, eye color, height, and build. Alternatively, as a known donor, one can choose to create a more detailed profile, sharing additional information about oneself without directly revealing one's identity. This may include details about education, pictures of the donor as both a child and an adult, etc.
Regardless of which type of donor a man chooses to be, he has no legal obligation to the child, and no paternity case can be brought against the donor in question.
My former wife and I, as prospective donor parents, were not in doubt that we wanted to use an anonymous donor.
We carefully considered whether to choose a known donor for our future child. The thought of our child spending their entire childhood speculating about who the donor might be would undoubtedly trigger a multitude of fantasies and imaginings. Who is he? What does he look like? Does he live nearby? And most importantly: Will he like me when we finally meet?
But our biggest concern was different. What if the donor, who had provided his sperm as an open donor, suddenly, 18 years later, had visits from several donor-conceived children knocking on his door? Perhaps he had since started a family and hadn't even considered the consequences of his actions when he donated sperm out of goodwill.
We couldn't imagine the disappointment it would be for our child to be met with a closed door at the donor's, after years of anticipation. It's difficult to envision the pain a young adult would feel if they had been looking forward for years to meeting their donor, only to be rejected or met with coldness.
It was a risk we, as parents, couldn't bear to take, so we decided to set aside our considerations about using a known donor.
We also faced a major dilemma regarding the use of an anonymous donor. Choosing this option would mean that our future child would never have the opportunity to know their biological origins. There would be perpetual uncertainty about whether our child had half-siblings, both here in Denmark and elsewhere in the world. It was a colossal decision, one that we had to consider carefully.
Once we had chosen anonymity with the donor, there was no turning back. It was a decision with permanent consequences that we knew we would have to live with for the rest of our lives.
It's completely understandable that choosing a donor for one's future children can be one of life's most challenging decisions. Making such a decision on behalf of another person is a monumental task, and it's natural to feel anxiety and doubt. However, I believe that when parents have thoroughly considered and discussed all options, and feel confident in their choice, it will also be the right one for their child. Of course, there may be exceptions where things don't go as planned, but that's part of life, and we must do our best with the decisions we make.
My children were born in 2008 and 2011, and at that time, there was only the option to obtain basic information about the anonymous donors. Since we didn't have the choice to get additional information about the donor, it didn't make much of a difference to me. I don't really worry about whether the donor was a carpenter or a medical student or somewhere in between. The most important thing to me is that he helped give us some wonderful children. I don't even need a picture of him as a child or to know what his career was. Who knows if my children will actually resemble him or follow in his footsteps? It's also not certain that they will resemble me or follow in my footsteps, even though I'm their biological mother. Fortunately, they will create their own path in life.
We had really taken the time to consider and discuss what type of donor we wanted, and we were completely sure that we wanted to choose an anonymous donor. So it shouldn't have been emotionally difficult to talk to the gynecologist at the hospital, who was supposed to help us with fertility treatment, about our choice of donor. But it turned out to be far from easy. I consider myself a tolerant person who has great respect for our differences as human beings, and racism is something that is very far from me. But there we were, as future parents, facing a total stranger - the gynecologist - and discussing the act of excluding and including a person as a donor.
I truly felt a wave of shame during that conversation with the gynecologist - a feeling I had never experienced before. It was a discussion about choosing a donor based on criteria like height, build, eye color - and most importantly, skin color! Suddenly, I found myself having to discuss another person's appearance, and it made me incredibly uncomfortable. All I wanted was to have a healthy child. But now I was in a situation where appearance also came into play. Let's be honest - most parents want their child to resemble themselves. My ex-wife and I are both fair-skinned with light brown hair, so it would be natural to choose a donor who resembled us. But I couldn't bring myself to tell the gynecologist that we wanted a donor who was an ethnically pale Dane.
I just sat there with sweaty palms, feeling like I was about to be labeled as racist because we wanted a white donor. That was the last thing I wanted - to be viewed in that way, and I couldn't accept it at all. Fortunately for me, the gynecologist sensed how uncomfortable I was. She quickly broke the silence by saying that it was generally best to choose a donor who resembled the parents. "In your case, it would be a Scandinavian type," she added quite naturally. It was as if a huge weight was lifted off my shoulders. Now it was her recommendation, and we could just say "Yes, please." I still think back to that situation, and I am truly grateful that she, as a gynecologist, was so understanding. She understood how difficult it was for us and provided us with the exact help we needed. We had discussed wanting our child to resemble us somewhat, but having to exclude an entire group of donors based on hair color, eye color, and especially skin color was truly a shameful experience.
Næste punkt på listen var højden på donoren, og sjovt nok var det ikke nær så svært at sige højt. Jeg er selv ret høj, og højden er også en god familietradition. Så for os var det vigtigt, at vores barn ikke endte med at være en gigant. Vores donorprofil blev derfor ret simpel: Skandinavisk type, mellem 180 og 190 centimeter. Det var en bred profil, men for os var det præcis, hvad vi havde brug for som kommende forældre.
When our first child was born in 2008, we received a document with the donor's number. It felt quite strange to receive it. It's a bit like getting a receipt for something you've bought - but in this case, it's about "buying" a child. The thought seems both strange and somewhat unethical when you ponder it. Nevertheless, this document is necessary later on when we need to arrange the birth certificate and stepparent adoption. It's fascinating how a piece of paper can encompass both practical formalities and deep emotional considerations at the same time.
In addition to the legal aspects the document is used for, there is another significant reason why parents are given the donor number. If you later wish for your children to be biological siblings, the donor number is crucial. It allows for obtaining sperm from the same donor for child number 2 or 3. One can contact the sperm bank and request them to reserve sperm from the donor for later use. Here, I almost felt like I was taking ownership of the donor - he was now ours, mine and my children's. Even though we had just become parents, it was clear to us that we wanted the option to have more children with the same donor. I had heard about a lesbian couple in my social circle who had teenage children who were biological siblings. Despite their differences, they felt a strong sense of unity knowing that they shared the same donor. I always thought this kind of security and community was a good idea. Therefore, we also wanted this option if it was available. And it turned out it was when our donor was still active, meaning he was still providing sperm to the sperm bank. We managed to store eight vials. We figured that if it took more than eight attempts to conceive child number 2, we would stop fertility treatment.
In practice, it works like this: you pay for the reserved sperm, and then the sperm bank stores "your" sperm until needed. When you resume fertility treatment, the sperm bank typically sends two vials to the fertility clinic. The first vial is prepared, and if it is of good quality, only this one is used. The second vial remains at the clinic and is ready for use if the first attempt does not result in pregnancy. The vials that leave the sperm bank are not returned. This is because they have been out of the controlled environment of the sperm bank during transport to and from the clinic, which increases the risk of damage.
Once you have completed having the desired number of children, and there are still vials left in storage at the sperm bank, the sperm bank usually offers to buy them back. However, at a price that is not quite the same as the original, but it is reasonable that they receive compensation for their service.
When my children over the years have been curious and asked about their donor, I have been able to share with them the thoughts and considerations behind our choice. It has been important for me to be honest and open about the process. I have told them how we as parents made this decision with great care and love because we believed it was the best for them.
And since I advocate for transparency, my children have naturally received the same information about the donor as we as parents have received. Therefore, they are aware of the hair color, eye color, height, and weight of their donor. This openness has made it easier for them to imagine what hair color and height they will have when they grow up.
I must admit one thing, though. My children have not been informed of their donor number, and they won't be. As parents, we fully agree that knowledge of the donor number will not have any significance for our children's upbringing. At the same time, we actually do not wish to risk finding ourselves in a situation where we discover that some of our friends or acquaintances have used the same donor. That would be an unwanted and potentially awkward situation. The use of the same donor as someone we know would, of course, never be a conscious act, and we did not know the donor's number until our first child was born. It would be somewhat strange to find out suddenly that we have half-siblings in our circle of friends. Fortunately, the other donor parents I have met have had the same attitude. None of us wish to know each other's donor. But at the same time, we agree that if the day comes when one of my children brings home a partner who is also a donor child, we may need to retrieve the donor number. Imagine if the two as partners have the same donor, and they are unaware of it when they start having children. It could really become quite messy with the genes!
My children have not yet asked for their donor number, and I'm really unsure how I would react if they were to ask for it now. Today, there are Facebook groups and other social platforms where one can search for half-siblings using their donor number, both in Denmark and abroad. Initially, I think it's a bad idea to start seeking out the anonymous donor's unknown children. But at the same time, I know myself well enough to know that if my children truly feel strongly about getting their donor number, it will be difficult for me to deny them that. Whether they want it to meet others with the same genes or to fill a gap in their personal history, I wouldn't be able to ignore their needs. After all, it's us as parents who made the decision about donorship on their behalf. Even as I write and reflect on my feelings, I'm still uncertain. But ultimately, I believe my children have the right to get their donor number if they want it. Fortunately, it's not something they're asking about right now. Hopefully, I'll be more clear-headed if this need arises later on.
Chapter 5 Fertility Treatment
Fertility treatment has become an important solution for many in Denmark as the demand has surged over the past few decades. Despite challenges with age and sperm quality, the country has seen a steady stream of around 40,000 treatments annually since 2017. Changes in lifestyle, later age at first birth, and increased awareness about fertility issues have all contributed to this increase, creating a greater demand for methods such as IVF, artificial insemination, and sperm donation to help couples achieve pregnancy.
Before January 1, 2007, it was only permitted for single women and lesbians to receive fertility treatment from midwives, who primarily performed inseminations. Gynecologists, who are usually specialists in fertility treatment, were not allowed to offer their services to single and lesbian women, even though they were responsible for such treatments in both the public and private systems.
However, this practice changed in 2007 when a legal amendment made it possible for anyone, regardless of marital status, to receive the same type of fertility treatment. This opened the doors for single and lesbian women to access a wider range of fertility treatments and professional counseling from gynecologists specializing in the field. This change was seen as a step towards greater equality and equal access to reproductive health in Denmark.
In the fall of 2006, our lives were filled with exciting decisions and expectations. My ex-wife and I had long nurtured the dream of expanding our small family, but as lesbians, we faced a number of limitations in the public system. At that time, legislation only allowed fertility treatment for singles and lesbians at a handful of private clinics, where midwives performed insemination treatments. We were prepared to follow this path, but then came the political decision in the Danish Parliament. Suddenly, it became legal for single women and lesbians to receive fertility treatment at the public's expense. It was a groundbreaking step for equality, where everyone, regardless of sexual orientation, gained the same right to help create a family in the public system. Although we had already considered private treatment, it was meaningful to us that our desire to become parents was now recognized and supported by the law. It felt like a triumph for equality and a tribute to our dream of parenthood.
We were excited about the opportunity to start treatment at our local hospital, which also meant avoiding long drives to a private clinic. Our joy was only amplified when we met a gynecological consultant who radiated enthusiasm and warmth. She was thrilled to be able to help lesbians and single women fulfill their dream of having children in the same way she had been doing for heterosexual couples for years. She had felt discriminated against herself when she couldn't see the logic in not being allowed to perform fertility treatments for lesbians and single women when a midwife had the opportunity.
The gynecologist had a very natural approach to our situation as a lesbian couple wanting to have a child together. She managed to inquire about who wanted to carry the child in a respectful manner, without emphasizing being the biological mother or not. She used terms like partner and co-parent as a natural part of the conversation, which gave us a sense of acceptance and recognition. It created a deep sense of calm and trust in both of us, and we felt that we were in the right place with the right staff, ready to start fertility treatment. It was a safe and competent start to our journey towards parenthood.
The treatment began with hormone therapy for me, followed by insemination. I had to receive a moderate dose of hormones to ensure that there would be at least one egg ready for fertilization in the next cycle. However, hormone therapy can result in multiple eggs ready for fertilization, and doctors will not proceed with insemination if there are more than three fertilization-ready eggs. This is due to the risk that a multiple pregnancy can be dangerous for both the mother and the children. As a gynecologist once explained to me, a woman's uterus is only designed to carry one child at a time. Therefore, a multiple pregnancy can place a significant strain on the body and pose risks. In cases of a pregnancy with more than two fetuses, fetal reduction may be offered to reduce the risks and increase the chances of all children being healthy and viable. The decision regarding fetal reduction is always complex and can have significant consequences for both the mother and the children's future.
Before embarking on the "baby project," I had crossed the magical age threshold of 30 years. It was a fact I couldn't change, but I understood the importance of having my body in good shape to increase the chances of successful fertility treatment. Since we started talking about having children, I had taken steps to eat healthier and be more active. I felt that my body was in good shape, and mentally, I was also ready for the challenge. I must admit that I probably naively thought that the process of getting pregnant would be a breeze with my healthy lifestyle and positive attitude. But I was gravely mistaken.
Before our first fertility consultation with the gynecologist, I had imagined that we would go through a longer approval process before starting the actual treatment. But there we were, ready for our first discussion about fertility treatment. After going through my medical history and explaining what the treatment would involve, the gynecologist suddenly said, "We are ready to start fertility treatment in your next cycle." I should have been overjoyed, but I actually felt a bit overwhelmed. Now it was suddenly a reality. In a month, I could possibly be pregnant! After finishing the conversation with the gynecologist, I was instructed to contact them on the first day of my period to start hormone therapy, so I would be ready for insemination at ovulation.
But the first day of menstruation was delayed. Despite my usual regular cycle and the ability to count exactly 28 days forward, my period did not come. And you might think that I had become pregnant naturally. But no. Virgin births and the intervention of the Holy Spirit are not my style. No, it was my psyche playing a trick on me. The desire for a child combined with the natural anxiety about life changes had apparently caused my body to skip a cycle. I was still amazed that the power of thought could have such a profound impact on the body. When I desperately contacted the gynecologist, she reassured me that I was far from the first woman to experience this. It was not uncommon for women to skip a cycle at the beginning of fertility treatment. Whether this is a fact, I actually do not know, but her assurance helped me relax and keep hope alive.
The second month passed, and my cycle was back on track. I started hormone therapy and was scanned to assess how many eggs were ready for fertilization. One large, well-developed egg was ready for insemination. Everything was as it should be.
The actual insemination takes place on a gynecological bed, where a "stream" of the donor's sperm is gently injected into the uterus. The procedure is relatively simple, but if the cervix is a bit reluctant, the gynecologist may need to assist in opening it. And let me just say, it is by no means comfortable when the doctor needs to use a small clamp to hold onto the cervix to insert the tiny syringe with sperm. Ouch – but all for the sake of having a child, right?
It should be noted that before the insemination, the frozen sperm collected earlier is thawed. After thawing, the sperm is checked to ensure that all the sperm cells are still active and in good swimming condition, even though this time they don't have to swim as far as in natural fertilization.
The notion of romance quickly fades during fertility treatment. You end up in a sterile room with white tiles from floor to ceiling, legs up in gynecological stirrups. And when the gynecologist grabs hold of the cervix with forceps, romance, beauty, and passion are out the window. The only comfort is being able to hold your partner's hand through it all.
Fortunately, I wasn't particularly affected by the hormone treatment, which can be a significant challenge for many women in itself. I also found the insemination itself tolerable, all things considered. I felt like I had complete control over this artificial reproduction process. Now, all that was left was to wait a couple of weeks before I could take a pregnancy test, and then maybe we'd be on our way to having our desired child.
The somewhat naively optimistic approach to the reproductive process was a contributing factor to feeling completely unprepared and almost shocked when I didn't get pregnant after the first attempt. After all, I had done everything "by the book" with the hormone treatment, and my age wasn't an issue either. So why didn't it work? It felt like a defeat, and I began to doubt my own body's ability to conceive. However, the gynecologist reassured me that it's entirely normal not to get pregnant on the first try. Many heterosexual couples try for months and years before succeeding, and even with fertility treatment, there's no guarantee of success. Although the chances of pregnancy are greater with treatment, it's still a process with uncertainties. It gave me some peace of mind to know that multiple attempts are normal and that there was still hope for success.
When embarking on fertility treatment, it's crucial to clarify how open you want to be about the whole process. As I approached 30, it felt like the questions from our social circle about children started raining down on us like confetti cannons at a wedding party. Everyone knew that we couldn't exactly conjure up a child without a little extra help. Therefore, we decided to be completely open about our fertility project from the very beginning.
This openness meant that my employer knew I needed time off at some rather odd times, often in the middle of working hours. Both my family, friends, my employer, and my colleagues were prepared for the possibility of hormonal fluctuations due to the treatment. Fortunately, they never complained, neither along the way nor afterwards. It gave me a great sense of calm knowing that my surroundings understood what I was going through. Not because they had to accommodate me, but because it created an understanding and support that I greatly appreciated. I've never regretted being open about it. I can't even imagine how cumbersome it would have been if every time I had to go to the gynecologist, I had to come up with some excuse or explanation for my absence or my changing mood.
Of course, there's a certain pressure when everyone in your social circle knows you're undergoing fertility treatment. Everyone hopes for success in your journey to conceive, and naturally, they inquire about it. However, I believe we struck a suitable balance where some were more informed than others. Overall, I've always felt that inquiries were made in a caring manner, without becoming overly intrusive. Personally, I much prefer being open rather than keeping things hidden, especially when it concerns something as significant and impactful on one's life as this, which can last for years.
The second round of fertility treatment unfortunately didn't yield the desired result, despite everything seeming to be in order - good eggs, sperm quality, and well-executed insemination, yet no pregnancy. And then, to top it off, the nurses' strike put the entire process on hold. All fertility treatments in the public sector were paused, and consequently, our baby project was also put on hold. It may seem like a bitter pill to swallow, but in the end, it must have been a kind of blessing. It was a well-deserved break - a chance to catch our breath, focus on other aspects of life, and find the strength to continue. But as soon as the strike was over, we were ready to dive back in with renewed vigor and hope.
Third time is indeed the charm for a reason. A total of 3 beautiful eggs were seen on the scan. Despite the significant increase from the previous attempts, where only one egg was present, the gynecologist approved the insemination. It didn't take long for my body to start sending signals that I was pregnant. On the day I took the pregnancy test, I had no doubt. Tender breasts and slight fatigue had already made their appearance. It was definitely positive. During fertility treatment, a pregnancy scan is offered at 7 weeks. Typically, the first scan occurs at 12 weeks, known as the nuchal translucency scan. However, to ensure that the egg has implanted properly after fertility treatment, a scan is conducted in the 7th week of pregnancy.
We were expectant and joyful as we went for the scan. Finally, we were going to see our future child's heart beating. The gynecologist inquired about how I was feeling, and I proudly mentioned how my breasts had been tender but had now returned to normal. He didn't comment on it but suggested we proceed with the scan. With my background as a nurse, I had participated in many scans, so I had an idea of what to look for on the screen. A moment of silence ensued as we stared at the screen, searching for the heartbeat that we had eagerly anticipated seeing. But there was nothing. No little flicker dancing lively on the screen. No sign of life. A pang of anxiety and sorrow pierced our hearts as the gynecologist examined carefully. It was as if time stood still in that moment where our hope was challenged by reality.
A wave of sadness washed over me. I couldn't hold back the tears. I had walked into the room with the conviction that we were going to be parents. Now, that feeling had turned into sorrow. As I lay there, tears streaming down my cheeks and my legs still in the stirrups on the gynecological table, the nurse placed a hand on my thigh. She didn't say anything, as the doctor continued to speak and scan. She simply performed some soothing, compassionate movements on my thigh. I never doubted that she did it with good and caring intentions. But for me, it didn't feel right. I don't know if it's because I'm a lesbian and had my ex-wife by my side. The whole situation just felt totally invasive. To lie there half-naked, crying on a gynecological table with a breathing nurse on one naked thigh and my ex-wife on the other side, holding my hand, was a complete violation of my privacy. However, I never managed to speak up, and I actually believe that many others in similar situations would have appreciated her caring behavior. Just not me.
The gynecologist took his time so we could gather ourselves. He told us that every third pregnancy ends in a miscarriage, with reasons such as an insufficiently functioning placenta or non-viable fetal offspring. Although with my background in healthcare, I already knew these facts, it was still reassuring to hear them reiterated by the gynecologist. He assured us that there was certainly no reason to lose hope that the next attempt could result in a pregnancy. However, I would have to wait for two cycles before resuming treatment. My body needed time to recover fully, even though the pregnancy had been brief.
The 4th and 5th attempts unfortunately ended without success.
When several insemination attempts don't lead to the desired result, one might consider switching donors to increase the chances of success. Some genetic matches simply work better than others. Since our donor pool was quite extensive, it wasn't a problem to find a new donor, and it seemed like standard procedure to switch donors after each unsuccessful insemination attempt. Why not try a new match when there are so many options to choose from?
In the sixth and final insemination attempt, it was just another ordinary day. Unfortunately, my ex-wife couldn't get time off from work that day. I didn't have the day off either, but my boss allowed me to sneak away during my work hours. So, I arrived wearing my nurse uniform to the basement of the hospital where the fertility treatment was to take place. There I was again, in the stirrups, this time dressed in half a nurse uniform, with my name tag still hanging and dangling in the breast pocket. Romance had long disappeared, and this time I was alone. But what wouldn't one do to get all the pieces to fall into place?
A few weeks passed, and finally, all the pregnancy symptoms showed up in my body again, accompanied by two lines on the pregnancy test. This time, my sore breasts were still present at the 7-week pregnancy scan. Everything looked as it should at the scan, and the little heart was beating away at 120 beats per minute. The relief was overwhelming. But at the same time, I think everyone, especially those who have experienced a miscarriage before, carries a small fear inside that something could go wrong. However, I'm not one of those with catastrophic thoughts, which allowed me to enjoy my pregnancy without major worries or complications.
A lovely, big boy was the result. He had been in the making for over 2 years, not least due to the need for 6 insemination attempts, a pregnancy that didn't come to fruition, and a prolonged nurse strike that also didn't yield the desired result. Two years may sound like a long time, but many couples go through a far more challenging and prolonged fertility process than ours.
When our son was around a year old, thoughts of another child began to surface. At that time, the rules were such that one could only receive fertility treatment for one child at the government's expense. If one still needed help to conceive the next child, they had to pay for it themselves at a private clinic.
t was a financial option for us, so we decided to start self-funded fertility treatment. We chose a clinic some distance from our home, primarily because of its well-established reputation and recommendations from friends and acquaintances who had previously used the same clinic.
We had previously stored sperm at the sperm bank after our son was born. So when we decided to start fertility treatment again, our clinic could easily arrange to have the sperm sent so that I could be inseminated with the same donor as before.
The difference between fertility treatment at the private clinic and in the public system was significant. At the private clinic, there was a clear aura of prosperity. The waiting room was furnished with luxurious furniture, the walls were painted in muted colors, and the lighting was pleasant and soft. There was even the possibility of having consultations and inseminations outside regular working hours. Customer service was top-notch, and it was evident that money was being spent to create a comfortable experience for patients.
My fertility journey at the private clinic was very similar to what I had experienced in the public system. I followed the same procedure with hormones and insemination, but this time I was much more relaxed. Knowing exactly what to expect from the treatment, combined with the fact that we already had our desired child, made me feel much less pressured. Perhaps it also helped that the surroundings at the private clinic were more inviting and less sterile, almost cozy even. That likely played a role too.
The treatment process for having our second child required three insemination attempts before I became pregnant. This time, we chose to use the same donor in each attempt because we wanted our children to be full siblings. We were confident that the donor's genes and mine would complement each other well and produce a good outcome. At the private clinic, we were also offered a scan in the 7th week of pregnancy. I wasn't nearly as nervous this time because, just like during the pregnancy with our son, I still had all the signs of pregnancy in week 7. The heartbeat was again quick and regular. After nine months, our second desired child came into the world.
My children know the story of their conception, and to this day, they still find it amusing to hear how they came to be.
Personally, I don't have a problem with one child being conceived at no cost while the other required some financial investment. Overall, throughout their childhood and adolescence, they both cost so much that the difference in what it took to conceive them probably won't be overwhelming in the long run. And I don't want to have to deal with financial micromanagement when it comes to my children.
It's unfortunate if financial constraints prevent prospective parents from pursuing fertility treatment to have a second, third, or fourth child. When it's just about insemination attempts, the costs are often manageable. But if egg retrieval and IVF are necessary, the out-of-pocket expenses become significantly larger. Considering the relatively small costs our daughter has incurred for us, and assuming it would have cost the same to conceive her under the public system, I'm convinced that she would have made a significant contribution to the treasury through a long and productive life. From a political and economic perspective, one could therefore argue whether it wouldn't be more profitable for society if the government covered the costs of fertility treatment for both the second, third, and fourth child. This way, we could have more new citizens who could later contribute to society through work and tax payments. It seems like a win-win situation: prospective parents get help with their dream of a larger family, while society addresses a societal issue.
Chapter 6Adoption
There is a significant difference between being donor parents in a heterosexual relationship compared to a homosexual one. When a heterosexual couple has a child with the help of a donor, whether it's egg or sperm, they don't need to specify this on the birth registration. The woman is simply listed as the mother and the man as the father, automatically granting them legal parenthood of the child, regardless of their biological relationship. However, this process is not as straightforward for lesbian couples and single parents.
When my son was born in 2008, things were completely different. At that time, there was a so-called 3-month rule. Essentially, the biological mother had to take a 3-month pause after the birth. During this time, she had to consider whether it was a good idea for her female partner to be allowed to adopt their newborn child through a so-called stepchild adoption. So, three months had to pass before the partner as the co-mother would have the opportunity to obtain legal rights over the child.
Thankfully, it sounds completely absurd today.
In our case, we had been a committed couple for several years. We were civilly married, blessed in our local church, and co-owned a property. The decision to have children was, of course, a mutual one. But now, we found ourselves in a situation where my ex-wife could not become the legal parent of our newborn child until three months had passed. If something were to happen to me during this period, my parents and sister would have closer legal ties to our son.
As a nurse in a neonatal ward, I have witnessed pregnancies and births where things go terribly wrong. Naturally, there was increased awareness of how we as parents would be positioned if the unthinkable happened—if either I or the baby became seriously ill or died during or after the birth. The thought of a situation where I wouldn't be able to care for our newborn child, and my then-wife had no legal rights, was frightening. In a healthcare system where rules and regulations must be followed, she technically wouldn't even be a legal next of kin to her own child. This thought weighed heavily, especially on my ex-wife, and I understood her concerns.
This had been our joint child project, with me carrying the child, but after the birth, I would have full parental authority. For three months, I would be the only one to receive communications from authorities regarding our child. We talked about it a lot during the pregnancy. It wasn’t that she feared I wouldn’t let her adopt our child, but the idea that we were not equal from the start. What weighed on her mind was the fact that she wasn’t recognized as an equal parent.
When our son was born, the birth certificate listed me as the mother, and under the section for the father, it stated "conceived with donor" along with the donor's number. What exactly would have happened if I had been unable to care for our son, or if the worst-case scenario had occurred and I had passed away, I do not know. We shared our concerns, especially with my family, as they would be the ones immediately involved if something happened to me. Everyone in the family agreed that our son had two parents, both before and after he was three months old. Everyone wanted the adoption to be completed as soon as possible after the three months to avoid any legal complications regarding the family's role. The three-month waiting period felt long for all parties.
Before our son was born, we had requested various adoption forms from the Family Law Administration. So, exactly three months after his birth, the forms were filled out and ready to be submitted. This process went completely smoothly, and the step-parent adoption was quickly approved. We were finally both legal parents of our shared child.
Fortunately, things changed in this area, and there was a legislative amendment where the Danish Parliament abolished the three-month rule. However, there is still not complete equality compared to heterosexual couples, who can still list "mother" and "father" on the birth certificate, regardless of whether they are biological parents or not. As a lesbian couple, we still did not have the option to fill out these sections. This wouldn't make sense anyway, as our future child does not have a father but a donor. If the birth certificate had a section for "partner" instead of "father," or perhaps even an option to note both parents' names, it would have been more appropriate. Instead, we had to write my name under "mother" and attach the step-parent adoption certificate from the Family Law Administration along with the birth certificate. This meant that when we had our second child in 2011, we had all the necessary legal documents ready before our daughter was born. She therefore had both of us as legal parents from the moment she came into the world.
The rules regarding legal parenthood for lesbian couples were changed again in 2014. From that point on, it was no longer necessary for lesbian couples to apply for stepparent adoption for their newborns. However, the changes were not as extensive as one might hope. Today, a married lesbian couple still needs to submit a paper application for co-motherhood registration to the Family Court (formerly the State Administration). This document must be completed before starting fertility treatment, and it requires signatures from both parents and an impartial professional from the fertility clinic. This applies whether the clinic is public or private, but the assisted reproduction must be carried out by professionals using registered donor sperm. The document must be immediately sent to the Family Court before the child is conceived to confirm both women's desire for the upcoming child. The Family Court must approve the co-motherhood, and once the child is born, the new parents must contact the Family Court again to register the co-motherhood.
Overall, this is a rather cumbersome process, especially when you are already married. One cannot help but wonder if there are men who wish a similar procedure existed for all forms of reproduction, so they could avoid becoming fathers suddenly and without their consent. The thought is probably far-fetched and would be impossible to implement in practice.
The change in parenthood legislation has also had a significant impact on midwives. Previously, they were responsible for completing the birth registration, which included establishing paternity. Today, midwives only report the motherhood on the birth certificate, while all matters concerning paternity are handled by Borger.dk and the Family Court and must be reported by the mothers themselves. The motherhood recorded on the birth certificate does not consider whether conception was achieved using donor eggs but is based solely on who gave birth to the child. I find this completely natural, as biology does not play a role in the essence of motherhood for me. For midwives, it must be a relief not to handle questions about paternity, which can be very personal and, in some cases, embarrassing and taboo.
The legal changes in the legislation might seem small at first glance, but for couples who see themselves as equal parents, it is crucial that both have the same legal rights. I could clearly feel the difference in the two years between the births of our children. It provided great security to know that the legal aspects were in place.
As a parent who has experienced the significance of legal equality, I sincerely hope that further changes in the legislation will be made in the future to ensure equality in blended families. Family dynamics and parenthood have changed significantly in recent years, but the legal framework has not always kept pace. Some of the families that could benefit from a change include, for example:
Heterosexual couples who separate and find new partners could benefit from changes in the law, allowing the child to have more than two legal parents. If all parties in such a blended family can agree and see the logic in the child having multiple legal parents, it would be fantastic.
Rainbow families, where, for example, two homosexual couples choose to have children together, could also benefit from changes in the legislation. In today's Denmark, this is not legally possible, but in countries like Canada, it is an option. Here, it can be a joint decision to establish shared parenthood right from conception. It would be beneficial if this possibility were also available for rainbow families in Denmark.
In daily life at home, the legal aspects naturally play no role. However, when we move into the public sphere, the difference between legal and non-legal parents begins to show. Non-legal parents cannot fill out documents for daycare centers and schools, and in all other situations where the child interacts with public authorities, there are limitations.
This can impact the cohesion within the family. The obligation and sense of responsibility towards one's child should ideally feel equal among all parents. When there is no legal equality, the sense of fairness can be challenged. I believe it is important to consider that blended or rainbow families already face emotional inequality, as some are biological parents and others are not. By adding legal inequality, there is a risk of perpetuating inequality in parenthood. I am convinced that in these situations, the child will always view all parents as their parents, whether they are biological, legal, or chosen. The child will only face challenges if disagreements arise among the parents or in the event of an accident. In such situations, it would be in the child's best interest to have legal guidelines and laws in place. If there are disputes about custody, for example, it could be in the child's interest for the law to intervene instead of leaving the decision to one parent. For me, the child's welfare should always come first.
Chapter 7Wonderful TitlesWhen a heterosexual couple has a child, it's often a natural decision to call themselves mom and dad. But for a homosexual couple, the options are much more open. Choosing titles requires careful consideration and can take a long time to find the one that best reflects each family member's identity. The crucial thing is not what you're called, but that your title feels genuine and reflects the relationship you want to have with your child. I'm convinced that if the title feels appropriate for you as parents, it will also feel right for your child.
In our parenting journey, there was never any doubt that we both wanted our titles to be as similar and equal as possible. Even if it meant that the parental title could be a bit long, children have a fantastic ability to adapt and accept what they have grown up with. It's yet another example of how adults set the boundaries.
Therefore, we agreed that we both wanted to be called "mom," whether we were biological parents or not. However, it could be a bit complicated with two parents both being called "mom," so we had to come up with a double title. I, being the biological mother, became "mom" followed by my name, and my former wife, who is the co-mother, became "mom" followed by her name. This created a balance and equality that signaled our desire to be seen as two equal parents. It was important to us that neither our children, ourselves, nor the outside world focused on the biological aspect. Our children had two parents with the same rights and responsibilities, and we were equal in our parenthood.
It has always been completely natural for my children to call us 'mom' followed by our names. However, it should be mentioned that today, since we are separated, the children use the title 'mom' and our names a bit more loosely. When they are alone with us in everyday life, where we do not share a residence, they usually just call the one they are with that week 'mom'. But when they need to talk about the other parent, they typically use the term 'mom' followed by the name. I find this change completely natural, as we all prefer things to be simple, and it's always easiest to just say 'mom'. Today, the children also sometimes just use our names, but that's probably because I rarely refer to myself in the third person as 'mom'. And it doesn't negatively affect me at all when my children call me by my name.
When I talk about my ex-wife to my children, I almost always use the term "mom" followed by her name. However, as the children have grown older, I've noticed that I'm not quite as strict about it anymore. Sometimes I just say her name. This isn't intentional, and it doesn't reflect anything about our parenthood or equality. It's true that even though we, as parents, choose the titles, it can take time for others to get used to them. This applies not only to daycare teachers and school teachers but also to grandparents and friends. It requires a certain level of awareness and respect from all parties to accept and use the chosen terms correctly. It can be a process, but over time, it becomes natural for everyone to respect the family's choices and use the correct titles.Mine forældre har altid gjort meget ud af at respektere mine valg, og denne respekt var selvfølgelig også tydelig i vores valg af titler som forældre. Det er ingen hemmelighed, at det ikke altid er nemt for dem at huske at kalde deres barn - mig - for andet end mit kaldenavn. Det navn har de alligevel kaldt mig i mange år. Men efter kort tid virkede det også, som om vores forældretitler faldt dem helt naturligt.
Here, I clearly believe that the word "tolerance" should be emphasized. It's not constructive to feel offended or upset if my surroundings don't always address me as I prefer. Automatically saying "mom" is not something to blame them for. I know they're doing their best, and it's something I must accept and respect.
The same applies when it comes to daycare centers and schools. Here, we've always been met with great openness and curiosity about our choice of title. Most of the time, we haven't even needed to explain it because the educator or teacher has already asked before we could say anything. We've never been met with puzzlement over our choice; there has only been great respect and acceptance.
In our case, where we both carry the title "mom," educators and teachers quickly realized that it's crucial to have a name after the "mom" title or simply our own names to avoid total confusion. Both I and the children can look puzzled if there isn't a name after the "mom" title. Who exactly are they addressing then?
It's not always easy to remember all the parents' names in a class. I have the advantage that I can just say "Anne's mom" or "Peter's dad," and then everyone knows who I'm talking about. The other parents in my children's classes can't do that. They also need to get to know our names, and so do their children.
Yes, it's absolutely fascinating to see how different parent couples choose their titles. I've heard everything from "Mama" and "Mami" to much more creative titles. There really are no limits to how one can express their parental role!
Many people use the term "mom" for the biological mother and "mama" or "mamma" for the co-mother. However, it should be noted that "mama" is also often used as a mother term in a heterosexual relationship here in Denmark. This typically happens when the mother may come from another country where "mama" means mother in that language. I think, for example, of my Norwegian colleague and my Russian girlfriend. They both use the title "mama," even though they are biological mothers, because it means "mother" in their native language.
And I also know several lesbian couples who use the term "mami" for the co-mother. But many of the lesbian couples I know actually prefer to call the biological mother "mom" and address the co-mother by her name. Here, I must emphasize that regardless of whether parents have a title or use their nickname, it does not affect their parenthood in any way. Not in the eyes of the children either.
The funny thing is, others can be scandalized when your children don't use the title "mom." My friend, who is heterosexual, is addressed by her nickname by her children. This surprises both colleagues and friends, but she doesn't mind. She's open-minded and doesn't want to impose a specific title on her children. Her husband and everyone else also use her nickname, so it's natural for the children to do the same. Some say, "It's a shame her kids don't call her mom," but it's her choice.
It's probably also significant how much emphasis is placed on using the word "mom" in the family and surroundings. Questions like "Are you going to mom's?" or "Does mom need to pick you up?" are often asked. Many look forward to becoming parents, so it's entirely natural for them to refer to themselves as mom or dad in the third person.
I've never actually been particularly preoccupied with my title as a mother. But I do get quite warm-hearted when I see how much joy and enthusiasm others put into their parental title.
The same applies, of course, to gay couples, who also need to find a way to differentiate themselves from each other as parents. When we talk about the next generation, the grandparents, it can also get quite confusing. There's a risk of double roles, for example, with both a grandmother and a grandfather. One solution here could be for one set of grandparents to choose to be called grandma and grandpa instead, leaving room for grandma and grandpa.
In our case, both my ex-wife and I were in complete agreement that my parents should be called grandma and grandpa. My ex-wife's parents were much more uncertain about what they wanted as their title. After much consideration and trying out various grandparent titles, they ended up also wanting to be called grandma and grandpa. Today, my parents are known as grandma and grandpa, and my ex-wife's parents are called grandma and grandpa followed by their nicknames. It makes for quite long titles, but the children have no trouble figuring it out. And neither do others, I suppose.
When it comes to titles, there's one I prefer to avoid being associated with in relation to my children. That's the title of father.
That's the only time I might correct other people. When I'm asked if my children have the same father, I always say, "No, they don't have the same father, but they have the same donor."
For me, the title of both mother and father requires being present in the child's life. One is not entitled to this title if they are not present. And in my children's case, where the donors are anonymous, they will never have a father!
When I explain my viewpoint on this to those who use the term "father" regarding my children's donor, I have never encountered anyone who has opposed this perspective. Everyone, after giving it some thought, completely agrees that one cannot be called "mother" or "father" if they have never been present in the child's life. In such cases, they are a donor.
I am fully aware that, in principle, it might seem insignificant. But for me, it holds a certain importance. I am convinced that this stems from my own experiences of having had an absent father in my life, which has been a significant and often painful absence. In contrast, I view the donor as an active choice that has been enriching.
The children have also never referred to their donor as "father." It's worth mentioning that they have grown up calling him "donor," as they have never heard us, as parents, refer to him in any other way.
Chapter 8The Birth
The birth process is one of the most stressful times for all expectant parents, where everything culminates. It is not uncommon for fertility treatments to deeply affect expectant parents, creating a certain nervousness around the birth. Parents deeply wish for their upcoming child to have a smooth welcome into the world. When labor begins, the stress level among the parents-to-be rises, making the presence of competent professionals who assist during childbirth immensely important.
During birth preparation, a conversation with the midwife includes noting the family structure in one's medical record. This means that when you arrive at the maternity ward and labor begins, the midwives will typically have had the opportunity to read your record and thus be aware of the family construction.
In our situation, this meant that the midwife was aware that we were a lesbian couple. There was no confusion about whether the person I brought along for this significant event was my sister or a friend.
In the delivery room, there is a whiteboard where the midwife notes the progress of the pregnancy and the expected birth weight. At the top of the board, there are two sections: one for "mother" and one for "father." My name was listed under "mother," and my ex-wife's name under "father." In the spirit of equality, one might have preferred "partner" instead of "father." To make it even clearer, there could be a combined section for "parents." This would also give the midwife the option to add additional names if the family structure required it.
During my first delivery, everything proceeded relatively smoothly. We never felt that any of the professionals we encountered during the pregnancy and birth disrespected or failed to acknowledge our family structure. After our son had rested on my chest for a bit right after he was born, it was time for me to be stitched up where he had caused some tears. I had to hand him over to my ex-wife.
In many cases, it can be beneficial to be stitched up while the newborn still lies on the mother, as the baby has a calming and almost pain-relieving effect. However, my body was shaking so much that I was afraid I might drop him. It then became my ex-wife's crucial task to take over and provide our newborn son with the essential skin-to-skin contact.
Like most other couples, we had discussed the importance of our son's initial attachment to both of us. Skin-to-skin contact is of immense significance because it releases oxytocin, also known as the love hormone, which is released in the brain. This hormone plays a crucial role in strengthening the bond between parents and child. Therefore, our son spent a lot of time in the following period alternating skin-to-skin contact with both of his mothers.
During my second birth, everything was very different. As with the first birth, we were greeted by a well-informed midwife. Unfortunately, the labor was prolonged, and it was clear that the information about our family structure had not been passed on to the next shift. A new midwife and a midwifery student took over, and we barely had time to introduce ourselves before my daughter was born very quickly after just a few pushes. I was bleeding heavily, which required more professional hands in the delivery room than those who had initially managed the birth. My ex-wife stood by my head, observing the situation. She could see how our daughter started having breathing difficulties while lying on my chest, as I continued to bleed profusely.
Several people now rushed into the room. As it was daytime, there were more doctors available, some accompanied by students. An additional midwife was called in to assist with our daughter, who needed help with her breathing. She took care of her until a pediatrician and a medical student arrived and took over the treatment.
While this was happening, two gynecologists and their medical students also entered the delivery room to assist me. The situation became a bit chaotic, with so many people managing two patients at once in the same space. Amid this confusion, the chief gynecologist didn’t look at the whiteboard and therefore didn’t get an overview of who my relative was. Given my critical condition and the need for immediate treatment, the chief gynecologist decided that my ex-wife could not stay by my side. She was asked to stand behind a screen in the middle of the room and wait there. I still believe the chief gynecologist assumed my then-wife was a friend who was there for support during the birth. Lesbian couples were still a rarity in the maternity ward at a provincial hospital in Jutland in 2011. My ex-wife remained calm and didn’t interfere by my bedside, so I am convinced that if the chief gynecologist had known she was my partner and not a friend, she would never have asked her to move behind the screen.
Fortunately, I knew the pediatrician who came to help our daughter. We had worked together for several years through my job as a neonatal nurse, so she was aware that I had a female partner. When the pediatrician heard that my ex-wife had been sent away from my side and behind the screen, she immediately called her over and asked her to come to the table where they were helping our daughter with her breathing. This allowed her to keep an eye on both me and our daughter. The pediatrician's actions had a significant impact on my ex-wife's perception of the situation. She felt demoted in her status when the gynecologist sent her away, reducing her from a partner to just a friend. However, at the same time, the feeling of recognition in her role as a parent was positive when the pediatrician called her over to the table with our daughter. There, she could observe the doctors' efforts and participate in the care for our daughter, providing her with some comfort and support in this first encounter with the new world.
It was a relief when our daughter's breathing quickly improved, and she no longer needed assistance. I was also starting to recover, and the bleeding had stopped. However, there was still some stitching to be done to repair my injuries. I had lost so much blood that fatigue was beginning to overwhelm me. So it was with relief that I could turn my gaze to the side and see our newborn daughter sleeping peacefully on my ex-wife's chest. Once again, it was she who had the honorable task of having the first skin-to-skin contact with our child.
We never later discussed with the maternity ward staff how frustrating it was that my ex-wife was asked to leave my side. With my experience from the many births I have been a part of as a professional, I know how important it is for the partner to be allowed to stay, as long as they remain calm and do not become unwell themselves.
The joy of becoming parents again overshadowed any desire to discuss our feelings of not being recognized as a couple during the birth. It is clear that the gynecological chief's primary focus was on stabilizing my condition and not necessarily considering who my relative by my side was. I can't really blame her for that. However, in hindsight, I regret that we didn't address it. Not to place blame on anyone, but rather to create a reflection on the situation that could perhaps help other families in the future.
Even though we, in the neonatal department where I work, place great emphasis on diversity in families and our broadly defined concept of normality, we can sometimes mistakenly assume the role of the accompanying person. This is especially evident in situations where the accompanying person cannot immediately be identified as a father, grandparent, or sibling. There can also be a significant age difference between the birthing woman and her partner, and it could be a woman accompanying the child to the neonatal department.
In these cases, it is crucial for us as staff to ask open questions to the relatives to clarify their connection to the child. A neutral question like "What is your relationship to the child?" allows us to obtain this important information without assuming anything about the relative's role or assumptions. I have never experienced anyone taking offense at this question, as it respects their integrity and opens up for a more nuanced understanding of the family context.
Even though we as staff are aware of the different family compositions, we can still miss the mark entirely. I vividly remember an episode where a child arrived at the department accompanied by our doctor and a man. Although we began treating the child, it quickly became clear that the man was the child's father. To reassure the relatives and signal that the child is doing better, we often engage in small talk with them. It has an incredibly calming and soothing effect for them to see that we as staff have time and energy for more than just treating the child. In this situation, my highly competent colleague began commenting on how adorable a boy the father had. Unfortunately, my colleague took the conversation a step further and said, "I think he looks like you too?!" However, the father looked a bit puzzled and calmly explained that he was not the biological father of the boy. The boy was conceived with the help of donor sperm. Although the man considered himself the father of his son, he was not the genetic father. My colleague apologized for her comment, and fortunately, the father took it in stride. His approach to being a donor parent was perfect in my eyes. He didn't take my colleague's remark as an insult, but rather as ordinary small talk. She couldn't have known that the boy was conceived with the help of a donor, as this information is usually in the child's records. I have great respect for his openness. It would have been easy for him to just say "yes" and omit mentioning the use of a donor. To me, he will always be a role model for us donor parents.
This story dates back many years, but it has been a continuous learning experience for us nurses in the neonatal department. I don't think any of us nurses have commented on whether a child resembles their parents or not since then. It's simply an unnecessary comment that can only go wrong. If it were to happen again, it would always be with good intentions.
Chapter 9Maternity LeaveThe rules and distribution of parental leave are undoubtedly a dynamic process that is constantly changing. These rules have been central in the fight for gender equality. However, I believe that sometimes there can be more political focus than focus on what is best for the family and especially for the child. As the non-birthing parent, one has the same rights regardless of gender.
I definitely share the concern that the parental leave system is not individualized for each child. It would give the parenting couple the opportunity to adapt the leave according to their family's needs and dynamics. Especially in the case of twins or triplets, each child would have the right to a parent on leave, ensuring a more fair distribution. Unfortunately, today it can happen that a child is "cheated" out of dedicated leave if there are multiple children born at the same time. It is worth mentioning that many multiple births occur as a result of fertility treatment, and parents in these situations often do not want to undergo further treatments after having multiple children at once.
It is really positive to hear that parental leave rules are still under discussion. It suggests that there is attention to the topic and a willingness to improve conditions for parents. I truly hope that these discussions lead to changes that better meet the needs of modern families.
Since we were both women, the parental leave rules were not crucial for gender equality in our case. My ex-wife was entitled to 14 days of leave like all partners, while I had the right to a longer period. We could determine the allocation of the latter part of the leave ourselves. Before the children were born, we had already discussed that I would like to return to work a little earlier than usual, while my ex-wife wanted to take the rest of the leave.
As I was breastfeeding our children, it was natural for me to take the first part of the leave, and then my ex-wife took over the remaining part. Thus, I stayed at home for 7 months before my ex-wife took over with an additional 3 months of leave before the children were to start daycare. We agreed that this distribution would create optimal conditions for a strong attachment to both of us. While it would have been ideal to share the leave more equally, the decision for 7 months was based on the Danish Health Authority's recommendation of 6 months of breastfeeding as a minimum. For me, it was important to try breastfeeding, although I had no problem with formula feeding if breastfeeding did not succeed.
Since I was the one staying home with the children in the first period, it was natural that I had the most contact with them. As they were also breastfed, it meant that I was the one who had close contact and intimacy with them at every meal around the clock. As parents, we had considered the distribution of the daily tasks around the children. This resulted in when my ex-wife came home from work, it was her who changed diapers and took care of bathing the children. I actually can't remember if I ever bathed the children in their first six months of life. Even though I work in the neonatal department and am used to handling newborns, I had no problem leaving some of the practical tasks around the children to my ex-wife. I never minded not being the one to give the children their first bath, etc. I really tried to be more of a guide in handling the children when they were very young than wanting to be in control. Whether this has succeeded, I cannot say for myself.
As a mother, I also needed some time away from home during the parental leave, preferably without the baby. After a whole day of taking care of one's child, you are constantly "on" and coordinating everything based on the child's needs and routine. Therefore, I really enjoyed going shopping after my ex-partner was done with work. Just a short trip of 30 to 40 minutes, where I only had to think about myself and the items that needed to go in the basket. It felt like a little freedom to be out shopping, and for my ex, it was a sign of trust that I was okay with letting her be alone with the children.
The same need arose for my ex-wife when she was the one at home on parental leave. However, for her, it was a bit easier to participate in leisure activities in the afternoon and evening, as she was not bound by having to be home for the baby's feeding times like I was while I was on parental leave and breastfeeding.
I cannot say for certain whether our alternating handling of the children from the very beginning has resulted in them being more attached to one of us than the other. Our children have never preferred to be with one parent over the other or only been comforted by one. It has always been irrelevant which of us was there to help them. Fortunately, separation anxiety is not something we have experienced in our family.
I was offered to participate in a mothers' group like any other new mothers, but I was unsure whether to accept the offer. Not because I didn't want to form social bonds with other new mothers, but rather because I feared that my professional knowledge would take over, and I would end up functioning as a professional advisor rather than just being a new mother like the others. I wanted to experience motherhood without having to bear the burden of my professional responsibility all the time. It's hard to say whether it was my own approach to the mothers' group or the composition of the mothers that led to both the group I participated in with our son and the one with my daughter quickly falling apart. Perhaps we were just a group of very different women, or maybe there were other factors that complicated the collaboration. One factor that likely played a role was that I had to return to work long before the other mothers in the group. My ex-wife had already made it clear from the beginning that she did not want to take over my place in the mothers' groups. Since the mothers' groups usually met in the morning, it became difficult for me to continue participating as I often had to be at work at that time.
It turned out that I found my social community in a group of women I had met during childbirth preparation classes. We had attended aqua aerobics for pregnant women together, and even after giving birth, we continued to meet up. Perhaps it was here that I had my social needs met. As a result, our meetings continued, and the other two mothers' groups faded into the background for me.
Chapter 10 The Little Child
During the period from the end of parental leave until the child starts school, the little one encounters many new people. Usually, the child begins in daycare or nursery, later transitioning to kindergarten. During this early phase of life, both the donor-conceived child and the donor parents establish many new relationships, both professional and personal.
In this period, the child's awareness evolves from believing that its everyday life and surroundings are the same for everyone else. Slowly, throughout the kindergarten years, the child begins to understand that others may live slightly differently than themselves. The little one moves from a daily life where differences such as skin color, a missing limb, and various family structures are not seen as differences but simply as part of reality.
Gradually, however, the child begins to recognize our differences. This new perception of oneself and others is largely shaped by the adults around the child. The attitudes and views on diversity held by adults influence the child and its perception of the world. Here, the child can learn tolerance and openness towards differences, but it can also learn intolerance and fear towards what is different.
When our son was about to begin his life in childcare, he started with a private childminder in our small village. At this point, he was still so young that he didn't have to consider on his own that our family was different from the other children's families. It was only us as donor parents who had to navigate our unique family structure in relation to the other parents.
The childminder never had any problem with our son having two mothers, and she addressed us as "mom" followed by our names. It also didn't seem that the other parents had any objections to us, but we didn't have significant relationships with them. This was mainly because we were constantly waiting for our son to start in the nearby nursery instead.
As my ex-wife had the last part of the parental leave, it was also her responsibility to introduce our son to institutional life. However, it was not an easy task for her. Her instinctive need to protect and shield him from challenges became a challenge for both of them. Farewell scenes often became lengthy and ended in tears - sometimes from both of them. I wasn't entirely sure if it was our different personalities or the fact that she wasn't the biological mother that mattered. At that time, I believed it was our personality differences coming into play, as it seemed significantly harder for my ex-wife to leave our son than it was for me. I am just a bit firmer and think "that's just how it is."
Over time, I have become more doubtful about whether being a biological or non-biological parent has a greater emotional impact on us than I previously thought. My ex-wife has always struggled to set boundaries for the children, and she is the perfect example of a helicopter mom who wants to remove all obstacles from their path.
I understand that I might risk stepping on some toes, even though it's certainly not my intention. I've noticed, both in my close relationships and among friends and acquaintances, that non-biological parents often tend to avoid conflicts with their children. It's hard to say whether this is due to a deep-seated fear of rejection by one's child. If this fear is present, I can understand it, but I don't always think reality reflects that. Personally, I've never heard my own children or other donor-conceived children say, "You're not my real parent!" in a conflict situation, so I believe the fear is unfounded. However, it's still important to discuss these concerns with one's partner to create a more trusting and harmonious family. Today, I'm convinced that this was a bigger issue in our parenthood than I initially realized.
It should also be considered that we belong to the generation where helicopter parenting has become prevalent. We eagerly want to protect our children from all forms of discomfort, and in principle, there's nothing wrong with that. However, the question is whether we're actually doing our children a disservice by doing so.
I've always had a fundamental sense of being a good mother. Yes, I make mistakes and do inappropriate things around the children, just like any other parent does. But fundamentally, I have no doubt that I'm a good mother, and no matter what I do, the children will continue to love me. This belief gives me peace in my role as a mother, and it's something I wish my ex-wife could also achieve. She carries an insecurity about being good enough and equal as a mother compared to me, an insecurity that I've always found completely unfounded.
After our divorce, we've thankfully been able to talk about it, but it has always pained me to hear her say that she's nervous I'm a better mother than her. I'm convinced that the children have never seen or experienced it that way. We're just very different. We do things in different ways, and we prioritize different things. From my perspective, neither the children nor I have seen a difference in our motherly roles based on biology. It's quite clear that the children quickly mastered the art of figuring out who to persuade to turn a firm "no" into a more compliant "yes."
It's a familiar challenge in many relationships where the roles in parenting aren't quite balanced. Even in relationships without the involvement of a donor, this uneven distribution of responsibility can create tension. For me, it became exhausting to be the perpetual "no-sayer" while she took on the role of the more indulgent and coddling parent. Honestly, I have a preference for saying "yes." It's just so much more fun. This skewed distribution of parenting responsibilities really left its mark on our relationship, and unfortunately, we weren't able to correct it in time. Along with other factors, this led us to choose to go our separate ways when our children were nearly 4 and 2 years old. Even after a divorce, it can be difficult to break out of the roles one has previously held. Personally, I really enjoy the freedom I have now to distribute the roles of "yes-sayer" and "no-sayer" more evenly. The difference between my ex-wife and me is still evident, especially when it comes to dropping off the children at daycare. When I dropped off the children, it was a quick affair: a hug, a kiss, and then I was out the door again. When it was her turn to drop off the children, they stood at the window waving goodbye, and the farewells often ended in tears. It's hard to say whether it's our personalities shining through or if our different biological relationship with the children plays a role. I know that I'm a more direct type. Therefore, I've always seen it as not a big deal for the children to be in daycare since I had to go to work, and there were no alternatives. For me, it was about making the situation as easy and conflict-free as possible. When things couldn't be different, the solution for me was to get it over with as quickly as possible. But for my ex-wife, it was different. She thought it was a pity for the children to be in daycare all day.
Another point is that children can react differently depending on which parent they interact with. This resulted in my ex-wife being called in for a conversation to improve the drop-off situations. However, I only found out about this much later, when she told me herself. I was very surprised, as at that time, we were divorced and didn't talk daily. I wasn't aware of the drop-off problem at all.
Looking back today, I wish we had been better at communicating about our parental roles and our emotional experiences as parents. This included not only our daily interactions with the children but also our inner feelings about parenthood. With the clear hindsight that hindsight provides, we should have had these conversations before the children were born. Even though I knew our approaches to parenting were different, I hadn't expected our emotional reactions to parenthood and the fear of not being good enough as parents to be so different. It has always been completely acceptable for me to take the children to the doctor for vaccinations or other less pleasant things. Even though it's not exactly fun - there are probably no parents who think so - there are just certain things that need to be done. The children and I even joke that I could be the chairwoman of "Mothers who can't figure out how to coddle their children." There's not always room for complaints when a band-aid needs to be removed, a bone needs to be examined for a fracture, or When I look back on my marriage and divorce, I can only urge all future parents, especially prospective donor parents, to have an in-depth conversation about the expectations and feelings in your upcoming parenthood. I have no doubt that I would have done things differently, and at the very least, I would have been more attentive to certain things if I had known from the start that she was afraid of not being as good a mother as I was. Whether it would have saved our marriage, I dare not say. But I could probably have been even more supportive and affirming in her role as a mother. Whether it would have made it easier for her to set boundaries and let go of the children, I don't know. One thing is for sure, though: It is incredibly destructive for a relationship if one tries to set boundaries and parent while the other sends conflicting signals or even cancels out the "no" that has just been given. When you have solidarity and a common direction in parenting, you undoubtedly get the furthest both as parents and as partners. It not only creates coherence in family life but also strengthens trust and cooperation between parents, which is crucial for a healthy relationship.
As the children grew older and began to develop their language, it also became more evident to them that their family was different from the other children's in the institution. This became especially clear during their preschool years. When the other children asked, "Where is your dad?" or "Is your dad picking you up today?" my children always answered that they didn't have a dad. However, they had to get a bit older before they really understood the concept of a donor, but they were fully aware that they didn't have a father, but two mothers. It was still difficult to hide from the children that they were conceived with the help of a donor when living as a lesbian couple. It was really challenging for both us and the educators to teach the children that it's called mothers and not "mumies". One thing was to get our own children to understand it, but teaching all the other children in the institution the same thing was a completely different challenge.
It has always fascinated me to observe how children in kindergarten talk about different family structures. They were all aware that our family lived differently from theirs, and that our children were picked up by two moms. It was wonderful to see the immediate acceptance and joy among the children. When my children told the others that they didn't have a dad, but instead two "mummies," the other children took it completely naturally. Even though they may not have fully understood the concept of a "donor" and what it entailed, it wasn't important to them in their daily lives. Their approach was simple and effortless.
My absolute favorite experience from when my children were in kindergarten is when my mom was picking up my daughter one day. They were out on the playground with a bunch of other children, and my daughter knew that it was grandma who would be picking her up that day. My mom found her among the other children and said it was time to go home. Suddenly, a boy came up to them, looked curiously at my mom, and asked my daughter, "Is it true that you have two 'mummies'?" My daughter confirmed that yes, she actually had two moms. Then the boy looked up at my mom again, almost enviously, and asked, "Do you also have two 'grandmummies'?" And proudly, my daughter replied, "Yes, I actually also have two grandmummies." My mom couldn't help but smile, as it was clear that this boy had a very special relationship with his grandma. And to be lucky enough to have two of them! There was no doubt that he thought my daughter was very fortunate. It's so lovely to see how children's logic can be so simple and beautiful. In my circle of friends, I know several grandmothers who are just as cherished, but for this boy, grandma was really important.
To assist our children, educators, and the other children in the daycare, we purchased the book "Wonderful Families". It's about an apartment building where different families live on different floors. Each chapter describes a family, and all families are composed in different ways. The conclusion in each chapter is that the most important thing in a family is to be happy and take care of each other. The families include a divorced family, a blended family with yours and mine children, a family with a father from the Middle East, a family with an adopted child, and notably a family consisting of a lesbian couple and their daughter, who came into the world with the help of a donor.
This book has undoubtedly been a favorite among our children. Seeing the different family forms in a book has been fascinating for them and has given them a sense of peace. Being able to recognize other families that resemble ours has strengthened their sense of community. Our book has been borrowed by the daycare provider, the nursery, and especially the kindergarten several times. I think that all daycares should have a similar book as an educational tool to show the diversity in society's families. And of course, the most important message is that we should take care of each other and be happy - that's the most important thing in any family.
As my children become more reflective during their time in kindergarten, there arises a greater curiosity about their origins. This curiosity began for my son when he was almost 6 years old. One day, he came and asked me if it wasn't true that I had given birth to him. Well, I could only confirm that. "So, aren't you my real mom then!?" he asked afterwards. No, I definitely didn't think so. Now it was important for me to find the right way to explain it so he didn't feel wrong. I affirmed to him that I am his biological mother, but we also had a little chat about how that doesn't necessarily make me his "real" mother. Being a biological parent didn't make me more or less of a real mother. A real mother is one who is present in the child's life and takes care of the child. This task and role were fulfilled by both my ex and me, so we were both real mothers. He thought that was a good explanation, and there were no further questions from him. He asked a bit about how someone gets pregnant when there isn't a dad, but I thought it was a bit early to have the birds and bees talk, so we had a lighter version of the topic. He seemed to understand and accept this without any issues. He ended up saying that the donor was a super cool person. Imagine, such a donor would help his mothers have children. My son thought that was a good deed. There's no doubt that our gratitude as parents to the donor for helping fulfill our dream of having children has influenced our children's perception of the donor. The donor is simply our family's little superhero.
As my daughter was only 4 years old at the time when my son started her turn to ask the same question as her brother had done a year earlier. However, I think she thought a bit more about the composition of the family than he did. Perhaps it was because she was younger, or maybe it was because she was slightly more reflective than he was. But the questions from her were many and came on several occasions. She was a bit more insistent in asking who was the real mom. However, each time she had to conclude for herself that she thought we were both equally her mom.
The question of who are the "real" or "less real" parents still exists among some adults. Unfortunately, there are still some who claim that one is a more "real" parent if they are biological. However, I can only reiterate that this is not the case. Parenthood should be judged based on one's presence, actions, and above all, love for the child.
Chapter 11The School ChildWhen children are about to start school, their awareness of themselves, their family, and the world around them expands significantly. Previously, they were accustomed, from daycare and kindergarten, to other children rarely questioning our different family structures. But now the situation was quite different. Our children would interact with new children whom they did not know before. And they were now at an age where they began to wonder and ask more probing questions, both to our children, the teachers, and their own parents at home.
After much consideration, we decided that our children should attend a private school. Since our son is two years older than our daughter, he was the one who would start school first and thus be the guinea pig for the school start. No one knew him, and no one knew us. In contrast, our daughter could start at a school where at least the teachers were familiar with her family background.
The school we chose is a large school with a strong focus on academic achievement and, importantly, well-being and prevention of bullying. I have never been afraid that our children would end up as victims of bullying. I believe that being bullied largely depends on the child's personality rather than their family background. At the same time, I am aware that our children come from a different family than the majority of the other children.
It became even clearer to us when we, as the only lesbian couple with children on a school with 1200 students, realized that the school had never before had students with homosexual parents. It was quite incredible, but it actually happened in 2014! Whether there are other donor-conceived children at the school, we have actually never discussed with the teachers or the management. It is, in principle, a private matter, but as humans, we naturally feel drawn to communities where we feel we belong. It could have been interesting and rewarding for both our children and other donor-conceived children at the school to have such a community.
Before our son was to start school, we met with the upcoming kindergarten teachers. It was evident that they were prepared to meet a family with a different composition. They asked probing questions about our family and the use of titles, primarily directed at our son. He was open and confident, and it seemed like he was comfortable sharing his family's unique story with the teachers. He told without hesitation that he had a donor and not a father, that we were divorced, where he lived, and much more. For him, sharing about his family was not associated with guilt or shame, but only openness and naturalness.
The two kindergarten teachers later ended up being the homeroom teachers for both my son's and my daughter's classes. Both teachers did an excellent job explaining to the other children in the class how there are many different family forms. We lent the book about the wonderful families to the teachers again, and it was read aloud to the class several times. The interesting thing about school age and beyond is that children begin to meet others with different family forms than their own. Their ability to reflect and their attention to diversity grow significantly.
The transition from kindergarten to school went smoothly. All the students in the two classes accepted and understood that my children had two mothers. The challenge was just figuring out which one of us was which. It can still cause some confusion at times. I must admit that I don't know all the names of the other children's parents, but luckily I can just say, for example, "Nicolai's dad" or "Julie's mom". It's just easier that way.
And then comes the next challenge: where the children live during the respective weeks. It's a challenge for both students, their parents, and especially the teachers.
I remember a funny episode when my daughter was in 1st or 2nd grade. One day she came home from school crying. Up until then, there had never been any problems with the acceptance of our family situation among the other students. But that day, my daughter was completely distraught. A boy from her parallel class had called her a liar. He had heard from some of the other students in his class that my daughter had two mothers. He couldn't understand it because everyone has a mom and a dad. He then went home to his parents and asked them if it could be true that someone could have two mothers. His parents confirmed that it wasn't possible. I'm not sure why his parents said that. Perhaps they hadn't considered that there could be children with lesbian parents at the school, or perhaps they believed that there always had to be a mom and a dad because it takes a man and a woman to make a child. The resolution to this misunderstanding came when my daughter's teacher had a conversation with both my daughter and the boy. He explained the situation, and my daughter's reality was acknowledged. The teacher also had a conversation with the boy's parents and explained the situation. I had a longer conversation with my daughter about how you're not a liar when you tell the truth. Others may not know the truth and therefore think you're lying, but that doesn't make you a liar.
When children reach 4th to 6th grade, they gradually become more aware of their own identity and sexuality. This reflection and wonder really came to the forefront one day when I was driving with my children. At that time, they were in 2nd and 5th grade, respectively. I told them that my then- girlfriend’s son had just gotten a partner.
"Oh, how lucky she is, because he's just incredibly sweet," exclaimed my son from the backseat. "It's not a girlfriend he's gotten, but a boyfriend," I corrected him from the driver's seat. "Oh, well then he's really lucky," my son corrected himself. We could all agree on that. There was complete silence in the backseat, and I could see in the rearview mirror that my son seemed very thoughtful. Suddenly he exclaimed, "So, that means he's gay!" Yes, we could also agree on that. It was quiet again, and I could see that my son was thinking deeply in the backseat. And then came the great, lovely logic from him. "It's only natural, since his parents are gay - I mean, lesbians. So, it's in his genes," my son concluded. I wasn't quite sure what to say to this conclusion. While I believe that homosexuality isn't chosen, I don't think it's hereditary. There was silence again in the backseat, and my son was thinking hard before he came to the final conclusion. "That can't be entirely true!? Because then I'll have to be gay too, and I'm way too fond of girls for that..." I really had to restrain myself from bursting out laughing. Hearing my child draw such big conclusions about life and love was truly fantastic. Instead, I had to try to give a politically correct explanation that homosexuality is neither hereditary nor environmentally determined.
My son breathed a sigh of relief because he actually didn't want to break up with his girlfriend, whom he had been with since 1st grade.
It may be that topics surrounding family compositions and sexuality have been more common in our family because of its makeup. My children have definitely been more aware of who they are but also of who others are. Today, there's so much focus on how each person identifies themselves. I must admit that even though I'm an open LGBT+ person, I don't quite have a handle on what all the '+'s stand for. So it's good to have an 11-year-old daughter who has a complete grasp of all the terms.
We've talked a lot about there being incredibly many different ways to be, and that it's important not to put people in boxes that close completely. Everyone should have the opportunity to be themselves and perhaps change later in life. In 4th to 6th grade, few are completely clear about who they are and what their sexuality will be. This process takes many years, but it's at this age that the foundation for openness, respect, and tolerance towards others' different sexualities is laid. Children's openness develops best if we as adults are open about our own identities. That's why I immediately said yes when my son in 6th grade asked me to come and tell his class what it means to be lesbian and choose to use a donor to have a child. He thought it might be relevant for some of his classmates in the future. "There might be some in my class who become homosexual when they grow up, or who need a donor to have a child," he said. I believe that my openness can help my children face the world so that with their background as donor children and with two women as parents, they have an easier life. By being open to the outside world, I hope that the world will also become more open to them.
In 6th grade, students have sex education for one week each year. Therefore, I contacted my son's homeroom teacher, who was in charge of the instruction. I asked him if he thought it would be relevant for me to come and talk about being a lesbian and about having children with the help of a donor. Fortunately, he was immediately on board with the idea. He believed that it could provide a different perspective to the instruction when I could speak from my own experiences, rather than him having to explain it from teaching materials. Instruction and lectures are usually not worse off if the speaker can draw parallels to themselves and their own experiences. So, I was ready.
I didn't create a big PowerPoint show or a detailed outline of the things I wanted to talk about. I've shared the story of "coming out of the closet," being a lesbian, and the decision to have children via a donor so many times that I don't need a script. I know all the topics by heart, both the serious and well-documented version, and the more humorous and personal version. Of course, I would present the fun version to the students in my son's 6th grade class. I wasn't nervous because I knew all the students in the class more or less well. They have witnessed my son's family structure and the fact that he is a donor-conceived child throughout their schooling. However, I might have been a little more nervous if I had to present to a class where I didn't know the students beforehand.
I just had a chat with my son before the presentation to check how he felt about me discussing such personal things. Even though he had asked, he could still have had cold feet at the thought of it becoming a reality. But he was actually totally cool with it. He just thought it would be cool for his classmates to have the same knowledge as him, and he had no problem with me basing it on our story.
On the day of the presentation, my son's homeroom teacher asked if he could be present during my presentation and possibly ask additional questions. That was fine with me - my openness was not only aimed at the students but also the teachers.
I started by telling the students that they were welcome to ask questions throughout the presentation. I was open to answering anything they wanted to know - except for one thing: sex!
I also asked them to remember one important thing: When they asked a question, it should be done with respect. As long as the question was asked in a respectful manner, it would always be appropriate. They should therefore ask themselves if their question was motivated by genuine curiosity or just to impress. They all accepted this premise. Now the presentation could begin.
I briefly talked about my experiences from elementary school and high school, where I often felt different without fully understanding why. Back then, there wasn't much focus on the LGBT+ community either in school or in the media, so I didn't know anyone who was homosexual, and the thought that I could be myself seemed distant. It wasn't until my 20s that I began to understand why I felt different.
The children listened with interest, and to my surprise, my son suddenly raised his hand. "Mom, can you tell us about the time you had to tell grandma and grandpa that you had a girlfriend." It was truly touching to see my son show such courage and openness by wanting me to share that story again in front of his classmates. It filled me with immense pride.
It was really interesting to see the students become so engaged in the topic of having a donor-conceived child. Their curiosity and creativity really came through. One of the students even humorously remarked that if one's partner wasn't so attractive, they could just choose a donor instead. It was a bit of a funny comment that made us all smile, although it also made me think about the importance of appreciating and loving our partners for more than just their looks.
It was surprising for the students to learn that both men and women in heterosexual relationships can have difficulty conceiving and may need the help of a donor. One of the boys had even heard that sperm cells could die if a man's testicles got too hot, for example, by sitting with a laptop in his lap for a long time or using the seat warmer in the car. It was a thought-provoking comment that made us all reflect on how fragile fertility can be and how important it is to take care of our bodies.
Jeg var very careful when we touched on this topic. I am well aware that in principle, there could be one or more students in the class besides my own son who were donor-conceived. They might be aware of it themselves, but they could also be living in uncertainty. I tried to explain that when you live in a lesbian relationship like me, it would be impossible to hide from your children how they were made. But that as a heterosexual couple, you could keep it hidden if it were necessary to use a donor. I tried with all my abilities to explain to the students that if a heterosexual couple chooses to keep the donorship hidden from their child, it will always be to protect themselves and the child. I also tried to explain to them that they shouldn't go running home to their parents and interrogate them about whether they were conceived using a donor or not. However, I couldn't help but interject that I believe it is immensely important to be honest as a parent about this to your child. I am convinced that a child can sense if there are secrets in the family, and this will affect the child psychologically.
We also talked about how both biological and non-biological parents have the same rights, and how both parents feel equally as parents towards the child. Here, my son raised his hand again because he wanted to interject that he also sees my ex and me as equal parents. Yes, he actually rarely thinks about who is biological and who is not.
I concluded the presentation by telling them that my son had asked me if he could also become a donor when he grew up. And no, he couldn't, because he himself is a donor-conceived child. One of the other boys raised his hand and asked if he could then become a donor. Well, there wouldn't immediately be anything wrong with that. Then the talk went lively among the boys. They wanted to know how often you could donate sperm, and how much you could earn each time. They all got dollar signs in their eyes. Just imagine being able to earn money by "jerking off". Fortunately, the lesson was almost over, because the boys were laughing and joking so much at the thought of their new earning opportunity that it was almost impossible to get them back on a serious track again. But that certainly didn't matter. My whole plan with this presentation was precisely for the students to leave with an openness and curiosity towards this new and different knowledge. Even though there was a lot of laughter and some funny comments made, respect for me and the students internally never disappeared.
When the class ended and the bell rang, my son came over and gave me a hug. "That was really awesome, Mom!" he said with a smile. I could see the pride shining from him, and I must have been beaming just as much as him, because I was so proud that he had asked me to do this. And that we had done it together. Imagine that he had wanted to and dared to ask more detailed questions during my presentation in front of his entire class. It's openness, and it's fantastic, and it can only serve as a role model for others.
Next year, my daughter will start 6th grade. We haven't talked yet about whether she wants me to come and give the same presentation in her class. She will have the offer, but I won't be surprised if she says no. Not because she is less open than my son. She is just in a different place and has much more knowledge about the subject than he did at this time. She's the one who can tell me about all the '+'s in LGBT+. In many ways, she's also more mature than her older brother was when he was in 6th grade. I don't think she would find it particularly amusing if the boys in her class started a verbal competition about who could earn the most as a sperm donor. But we'll see what the future holds. Right now, I just know that she will also have the offer.
Chapter 12The Teenager
Welcome to teenage life! This is where the big thoughts really start to sprout, and the question of "Who am I?" becomes more and more prominent. But it's also a fantastic time! I enjoy being challenged both as a mother and as a person, and having a teenager in the house really puts you to the test. My teenagers not only have to figure out who they are themselves, but they also suddenly become much more aware of who I am and everyone else in their surroundings. No one escapes a bit of analysis - not grandparents, who may change a bit with age, or a teacher at school who stands out with their teaching style and approach to students. Everyone is seen through the teenagers' magnifying glass.
For my children, the transition to adolescence also marks a significant shift. At their school, all the sixth graders are separated, welcoming a lot of new students. This results in the formation of new seventh-grade classes with both new and old students. The safe and familiar role that the students have had in their previous 7 years of schooling is now completely gone. The comfort of knowing that everyone in their class and parallel class knows them and knows about their family is suddenly gone.
The difference between starting in the early years with a family background that is different from most people's is just significantly less noticeable and visible when you're 5-6 years old than when you're a teenager. Children in preschool have not yet been shaped by categorical thinking and stereotypes, and their tolerance for diversity is just greater when you're still a naive and open-minded child. So, having to stand as a teenager in a new class with 25 students, of whom you only know two from your previous class, is slightly anxiety-provoking. Fortunately, discussing difficult things is not something we shy away from in our family. So, the conversation about what my son could expect to encounter in the new class has been had a couple of times over the kitchen table before the start of school.
Before the end of the sixth school year, the new seventh-grade class had to meet for an information evening. Here, the new class was welcomed by their upcoming class teacher and taken to their new classroom. There, they quickly got to meet each other, make some creative name tags, and prepare a short presentation about themselves and their family. When we parents later arrived in the class, each student had to stand up, tell where they lived, which school they came from, and, most importantly, they had to point out their parents. This scenario was neither something our son nor us as parents were prepared for, and I just managed to think, "Uh, this is going to be challenging for him." But he did it. He stood up, and without hesitation in his voice, he introduced us as his two mothers. I had a mixed feeling of feeling a bit sorry for him and at the same time being super proud of him. I felt a bit sorry for him because no teenager in a completely new class wants to be different. I was incredibly proud because he managed to take on such a challenge with ease. That's just the way he is.
When we walked home from the meeting, I asked him if any of his future classmates had asked about his family situation. They hadn't. Everyone had probably been busy being new, and he might not have been the only one feeling different. I guess that's just part of being a teenager. I could then tell him that none of the other parents had asked us questions about our family structure either. The focus was solely on our children, upbringing, rules, and having a child in a new class. In a way, I was relieved that our family structure wasn't a focal point, but at the same time, humans are naturally curious.
Ultimately, I always prefer direct communication with other parents if they have questions or curiosity, rather than it going through the children. At the same time, I fully understand that most parents in a new class don't want to pry or wonder about the other parents at such a first meeting like this.
During the summer vacation before my son started seventh grade, we had another talk about how he thought it would be to start in a new class with our family background. Like so much else in adolescence, my son thought "it's going to be totally awkward." It's a lifelong process for my children to "come out of the closet." They have to come out of the closets labeled "rainbow family" and "donor child." These closets they will continue to step out of every time they form new relationships – and they should do that for the rest of their lives.
I could understand my son's reaction to how it might be a bit awkward to talk about his background as a rainbow and donor child. I've been in that situation countless times, where I had to explain my background, lifestyle, and choices, so I know how challenging it can be. We talked back and forth about how he could present it to his future classmates.
We discussed which words and phrases he could use. What did the others already know about a rainbow family beforehand, and what would be completely new to them? Suddenly, my son looked at me and said, "I actually don't think it's my job to tell my new classmates that I'm a donor child. That should be yours. I didn't choose to be a donor child. You know exactly why you made the choices you made. I mean, you chose an anonymous donor, and it was you who carried me." For once, I was completely speechless. Wow, he was absolutely right. I asked him how he wanted this information to be conveyed to his new classmates.
My son was clear about it. He wanted me to come and share with the new class about our life as a rainbow family and our decision to have a donor child. He wanted me to present something similar to what I had done in his old 6th grade. I completely agreed with this. As mentioned earlier, I certainly don't believe in overprotecting my children or hiding the challenges they face. But this bump in my children's road is the result of a decision we as parents have made. I want to help make this situation a little easier for them. However, I am well aware that my children will face similar challenges several times in their lives. These times I can neither nor should I remove for them. But right now, the most important thing for me is to signal to my children that there is nothing dangerous, unsafe, or awkward about openly discussing these topics. For me, the best way to be a good example for my children is by showing openness and courage to talk about the things that make our family unique. Remember, there's nothing dangerous about bringing up the subject, as long as the recipients are open and kind - and a group of newly formed teenagers should be.
My son and I agreed that I should contact his upcoming class teacher before the start of school and offer her the opportunity for me to come and share our experiences of being a rainbow family and our decision to have a donor child. Fortunately, she thought it was a fantastic idea and appreciated our openness. We agreed that I would come already on the students' second day of school, where the day would be used to strengthen the cohesion and well-being of the new class. The students were informed that there would be a presentation on community, diversity, and openness.
The class teacher made a brief introduction about diversity and experiencing things in different ways. Two students were asked to come up to the board, where they stood and looked at a piece of paper on the floor with a large number written on it. For one student, the number appeared as a 6, but for the other student, standing on the opposite side of the paper, the number appeared as a 9. Now the two students had the opportunity to explain to each other why they understood the number the way they did. It was a fantastic and slightly challenging task, but it made all the students in the class aware that something that is essentially the same can be perceived very differently. Above all, it became clear that it can be difficult to understand what others see when you see something completely different yourself. This was a brilliant introduction to my upcoming presentation for the students about being a rainbow family and choosing to have children with the help of a donor.
My presentation was very similar to the one I gave to the 6th grade. However, it was clear that the students this time didn't know each other, so there weren't as many funny comments and detailed questions as last time. The only one who dared to raise his hand again was my son. He thought I had forgotten something that I had included last time I gave the presentation. But all the students were sitting attentively and listening, and when I asked afterwards if they had gained new knowledge, there were eager nods.
Whether it was an advantage to give this presentation on the second day of school in a completely new 7th grade, or if we should have waited six months until they were better acquainted, I don't know. But when I talked to my son about it afterwards, he expressed that he thought it was nice that everyone now knew how things fit together. He didn't have to explain anything to anyone because I had covered most of it. He thought the timing was fine because if we had waited six months, he would definitely have had to answer the questions himself before I came and gave the presentation.
Absolutely, it was a clear signal to the students from both the class teacher's and my side that we should be able to discuss our differences and choices without it turning into conflict. It was important for us to show that the challenges and thoughts that the students grapple with can and should be shared openly. Our hope is that they learned that it's okay to have different viewpoints without it creating discord. You don't need to understand others to respect them.
Giving our children a solid foundation is crucial for any parent. Being a child in a rainbow family or being a donor child certainly doesn't have to be a disadvantage. In fact, a lot of research shows that children of lesbian parents generally perform better in school. Additionally, they often have higher self-esteem than their peers. As society evolves, we also see more diverse forms of families, and more research is being conducted in this area. Studies focus on the well-being of children in different family situations and compare them with each other.
One of the significant reasons why children in rainbow families statistically perform better, I believe, is because they are all planned and wanted children. In rainbow families, no child is born unplanned. Furthermore, it's impossible for us to hide how our children were conceived. My children have always known they have two mothers, and from the day they began to talk, we have openly discussed it. There has always been a natural openness about being a donor child because we have never been able to hide it from them.
I must emphasize once again that I believe it is detrimental to both the child and the parenthood to keep significant secrets. The use of a donor in the efforts to expand the family constitutes such a significant secret. The unsaid, the secrets, and sometimes outright lies can be felt by the child and be a burden for the parents. Regardless of when the secret is revealed, whether in the child's life or the adult's, the truth will have significant consequences. Many donor-conceived children have later revealed that they could sense there was a secret in the family. Many of them have tried to inquire about what it could be, but they have always felt rejected. For many of these donor-conceived children, who are now adults, this has had significant psychological consequences.
Playing with open cards is not only beneficial for yourselves but also for your children. Hiding the truth about their background can lead to unnecessary complications and confusion. Being a parent is not just about biology but about love, support, and commitment. If even a teenager can handle the awkwardness of discussing their family situation, then surely we as adults can too. If we perceive it as awkward, we risk others feeling the same way. Let's break the taboo and be proud of our families, no matter how they are composed.
Chapter 13Why Should We Hide Anything?
I love in every way that my children are growing up. Their way of seeing the world and starting to become more and more reflective brings both challenges and great joy into my daily life. When I look at them now, I think that so far it has gone really well. I have two lively and curious young people who are not afraid to ask questions, both to themselves and to the world around them. This curiosity and wonder about almost everything will, however, also bring challenges in the future. For it is clear that they will become more and more curious about themselves and their origins.
Currently, only my ex-wife and I know the children's donor number. We have told our children that as parents, we fundamentally want it to remain that way. Originally, they do not need the donor number, so why should they know it? But today, with your donor number in hand, you can do more than just find your donor. There are now several online forums on social media where donor-conceived children, using their donor numbers, search for half-siblings both nationally and internationally. Since the same donor can be used in both Denmark and abroad, my children are aware that they potentially may have many half-siblings scattered around the world.
I have spent some time considering how I will handle it if my children one day ask for their donor number. It will require a good conversation where we sit down and talk about their expectations for this information and, most importantly, what lies behind their desire to know the donor number.
If they have a burning desire to know if they have half-siblings, it's a desire I may not fully relate to. I think they have each other as siblings, and that should be enough. But I have already accepted that I cannot determine what my children want. As parents, we will therefore have to accommodate their wishes. I have never been in the same situation as them.
I have always known where my genes come from (I can't completely deny it from an appearance standpoint). Therefore, I can never fully understand what it feels like to be a donor-conceived child. Although I feel that I have a great rapport with my children, and that they can tell me everything about their thoughts and feelings, I am aware that there will be things they do not share with me. This could well be one of the things they choose to keep to themselves. However, I hope with all my heart that they will use each other as siblings and also lean on the other donor-conceived children they know in their community.
The biggest problem, as I see it, could arise if the children have very different approaches to seeking out half-siblings. Imagine if one of my children has a burning desire to find any potential half-siblings around the world, while the other has no desire whatsoever to explore or gain knowledge about it. This could potentially create discord between them.
Most of all, it could potentially lead to one of them gaining knowledge about their biological origins that the other does not want to have. How to handle such a situation, I currently have no solution for. I may possibly find myself in a situation where I have to consider both my children's very different wishes and needs. There is no doubt that it will require in-depth dialogue and reflection for both me and the children to prevent such a situation from escalating into a family crisis. I am keeping my fingers crossed that this never happens.
At the same time, I think it might be good that the thought of this potential scenario has crossed my mind. It means that I can be just a little prepared if it should happen.
But if the day comes when they want to search for half-siblings, I hope they will stop there. I have heard of other donor-conceived children who have started an intense hunt to find the identity of their donor, even though he has been anonymous from the start. In my view, this is by no means fair. Both I and my children must respect that the man who is their donor has chosen to remain anonymous.
We, as parents, are eternally grateful for his donation and that he has contributed to me being able to give birth to two wonderful children. This gratitude must manifest itself in a deep respect for his choice to remain anonymous. It would, in my eyes, be immoral and an intrusion upon him if my children or any of his donor-conceived children were to begin an intense search for his identity.
At the same time, I know that my children did not choose an anonymous donor themselves. We, as parents, did. I may sound harsh when I say that there are just not all things in life that one gets to choose. And this, certainly not insignificant thing, they did not get to choose for themselves. If this choice, which we as parents have made for the children, turns out to be an identity and life challenge for them, it is something we as parents will have to work through together with them, and not by finding the identity of the anonymous donor.
Life is truly a dynamic journey, and that's precisely what makes it both challenging and exciting. It's a constant flow of experiences, challenges, and opportunities that shape our journey through existence. That's what makes life so fascinating and valuable.
I am now convinced that it will not lead to a crisis for my children that they do not have the opportunity to know their biological origins. They have always known the honesty and truth surrounding our use of an anonymous donor. I will always argue that you always get furthest with the truth. The truth can be difficult and harsh, and it can feel unfair and despairing. But the truth gives you something concrete to relate to. What is the reason that some donor parents do not want their child to know the truth? I simply do not understand it. For me, there is always a world of difference between being a parent and being a biological parent. If only the biological parents initially had the ultimate parental right, many children in the world would be in a dire situation. I think, for example, of adopted children. Would their adoptive parents never be able to be their real parents because they are not biological!? I also think of the children who live in foster families, where foster parents play such an important and crucial parental role in the child's life. In some cases, these children see their foster parents as their "real" parents.
No parent should feel less valuable just because they are not biological parents. When no parent feels less valuable, there is no reason to keep anything silent. And when nothing is kept silent, it creates the openness that our donor children need. The more open we are as donor parents, both to ourselves and to the world, the more openness and tolerance our children will encounter. When all is said and done, it's about the well-being of the children.
Chapter 14Epilogue
The clock reads 2 in the morning. The office is quiet. Both parents and children are asleep, and the screens on the wall show with their neon blue numbers and green lines, pulsating in steady heartbeats, that all the babies are calm and stable in the Neonatal department tonight.
I glance at my colleague. She's relatively new to the department, and it's the first time I'm alone on the night shift with her. She looks up at me curiously. "Do you want to ask me something?"
"Isn't it true that your child was also conceived with the help of a donor?" I say. "Yes, he is. Aren't your children too?" she responds with a small smile.
I inquire a bit more about whether she used an anonymous donor and where he was made. I'm cautious with my questions since I don't know her that well yet. I know from myself that it's a very personal issue. It can be sensitive, and if nothing else, it's just very private. But she tells me without hesitation how things are in her family. Her son is a bit older than my children. Back when he was conceived, the times and regulations were completely different.
She is just as open about the topic as I am. Whether it's because she's sitting here with me, who is in the same situation, I don't know. But it's clear that she's been asked this question so many times that she answers reflexively, just like I do when I'm asked.
Her openness and honesty give me courage. Courage to tell her about something that only very few know I'm working on.
"I'm writing a paper about being a donor parent," I tell her. I sit a bit nervously, waiting for her reaction. Will she find it interesting, silly, or irrelevant?
She inquires a bit about what it specifically entails. I tell her about the different sections and how it's written for everyone who comes into contact with donor parents. It's an informational book meant to provide insight into aspects of life as a donor parent that people may not be aware of. But most of all, it's meant to be an assignment that opens up and encourages dialogue about being a donor parent, I explain to her.
She smiles at me. "That's a really great idea. I wish I had read it before we started the whole project with a child back then," she says. I breathe a sigh of relief. Maybe this paper isn't such a bad idea after all, which I'm almost finished writing. It's one thing for my closest ones to think it's a good idea, but it's another for an almost outsider donor parent to also think the idea is good. I can feel how much her opinion means to me. It gives me renewed energy to finish the paper so it can go out and have its own life. A life that invites more openness, tolerance, and curiosity.
Chapter 15Thanks
I hope you have gained a little more insight into what it means to be donor parents - the considerations involved, and especially some of the emotions that can be associated with it. I hope that you've found a smile on your face while reading. And I hope that you feel inclined to share your thoughts with others about being donor parents, whether they are or will become donor parents themselves, or whether you're a relative or professional. My hope is that you feel encouraged to be open.
To all the professionals I've encountered in the context of fertility treatment, pregnancy, birth, daycare, and school: I am deeply grateful for your open and professional approach to me and my family. Remember that the way you carry out your work has a much greater impact than you might realize.
To all the donor parents I've met throughout my life: You have been a source of great inspiration to me. Some of you are closely involved in my private life, while others have played a more peripheral role because I've met you through my work, at a party, or in other contexts.
To those of you who are donors: You are the greatest gift to us all. Thank you.
#sperm donor#egg donor#donor parents#rainbow families#fertility treatment#parenting#children#egg donation#equality#equal rights#womens rights#lesbain#lesbian parents#adoption#homosexual#danish
0 notes
Text
BECOMING AN EGG DONOR: ANSWERS TO YOUR FREQUENTLY ASKED QUESTIONS
A crucial part of assisted reproductive technology (ART) is egg donation, which gives infertile people and couples hope. In order to help another person or couple (the recipients) who are unable to conceive with their own eggs, a lady (the donor) donates her eggs. For people struggling with infertility, this selfless act of kindness can bring their hopes of parenting closer to reality for those facing fertility challenges..
Deciding to donate your eggs to help a family in their journey to have a child is a deeply meaningful decision that requires careful consideration. If you’re considering egg donation, you likely have inquiries. Happy Future Surrogacy is here to address the common questions from potential egg donors as they weigh the choice of offering this invaluable contribution as they consider the possibility of offering this remarkable gift.
WHO CAN BECOME AN EGG DONOR?
Requirements for egg donors vary depending on the fertility clinic or egg donation agency. Generally, donors should be between the ages of 18 and 30, in good physical and mental health, have a healthy lifestyle, and be willing to undergo medical and psychological evaluations. Some clinics may also have specific height, weight, and educational requirements.
WHAT IS THE PROCESS FOR BECOMING AN EGG DONOR?
The process typically involves an initial screening to determine eligibility, followed by medical and psychological evaluations. Once approved, the donor will undergo ovarian stimulation with hormone injections to produce multiple eggs. The eggs are then retrieved through a minor surgical procedure performed under sedation. After retrieval, the eggs are fertilized with the recipient’s partner’s sperm (or donor sperm) in a laboratory, and resulting embryos are transferred to the recipient’s uterus.
WHAT ARE THE RISKS OF EGG DONATION?
Egg donation is generally considered safe, but like any medical procedure, it carries some risks. The most significant risk is ovarian hyperstimulation syndrome (OHSS), a potentially serious condition caused by the fertility drugs used to stimulate egg production. Other risks include infection, bleeding, and reaction to anesthesia. However, serious complications are rare, and fertility clinics take precautions to minimize risks.
WILL I BE ABLE TO HAVE CHILDREN AFTER DONATING AN EGG?
For over two decades, individuals have been contributing their eggs through donation, with studies indicating that their fertility is comparable to those who haven’t donated. Although humans are born with a set number of eggs, only one typically ovulates each month, while the rest are naturally reabsorbed. Egg retrieval merely utilizes those eggs that would otherwise go unused during the monthly cycle.The retrieval process simply takes advantage of the eggs that are not used during the month.
IS EGG DONATION ANONYMOUS?
Whether egg donation is anonymous or not depends on the preferences of the donor and recipient(s), as well as the policies of the fertility clinic or egg donation agency. Some donors and recipients choose to remain anonymous, while others opt for open donation, where identities are disclosed and contact may be maintained between parties.
WILL I BE COMPENSATED?
Yes, egg donors are typically compensated for their time, effort, and any associated expenses. Compensation varies depending on factors such as location, demand for donors, and the specific requirements of the clinic or agency.
WHAT ARE THE LEGAL IMPLICATIONS OF EGG DONATION?
The legal implications of egg donation vary by country and jurisdiction. In many places, egg donors sign legal contracts yielding any parental rights or responsibilities for any resulting children. It’s important for both donors and recipients to understand the legal framework surrounding egg donation in their location and to consult with legal professionals if needed.
CAN I DONATE EGGS MULTIPLE TIMES?
It is generally recommended that egg donors undergo no more than six cycles of egg donation in their lifetime to minimize potential risks to their health. Each donation cycle requires a period of recovery, during which the donor’s body replenishes its egg supply and returns to its normal hormonal balance.
IS EGG DONATION PAINFUL?
Egg donation involves a few stages, including ovarian stimulation and egg retrieval. While some discomfort, such as minor bruising or bloating, may occur during the hormone injections for ovarian stimulation, the egg retrieval procedure itself is performed under sedation or anesthesia to minimize any pain or discomfort. After the procedure, donors may experience mild cramping or discomfort, which typically resolves within a few days. Overall, while individual experiences may vary, most donors find the process manageable, and fertility clinics prioritise donor comfort and safety throughout the process.
WHAT ARE THE BASIC REQUIREMENTS OF EGG DONATION AT HAPPY FUTURE SURROGACY?
Age between 18 and 30.
Maintaining physical health and having regular menstrual periods.
BMI of 28 or less, indicating proportionate weight to height.
Not using contraceptive implants or Depo-Provera injections for birth control (or willing to remove if currently using).
Non-smoker and abstaining from recreational drug use.
Willingness to undergo a series of injectable medications as part of the process.
Absence of family history of inheritable genetic disorders.
Demonstrating reliability and maturity by attending all appointments and adhering to medical instructions.
No history of genetically transmitted diseases or sexually transmitted diseases within the past year, and never testing positive for AIDS or HIV.
Becoming an egg donor is a very great decision that can profoundly impact the lives of others, offering hope and the opportunity for parenthood to those facing infertility challenges. At Happy Future Surrogacy, we understand the significance of this journey and are committed to guiding potential donors through every step with compassion and support. If you meet the criteria and feel compelled to start this incredible journey of generosity, consider joining our community of egg donors. Together, we can make dreams of parenthood a reality. Ready to make a difference? Apply to become an egg donor with Happy Future Surrogacy today and help create families. Your selfless contribution could change lives forever.
#surrogacy#surrogate mother#surrogacy california#surrogate#intended parents#fertility clinic#surrogacy process#egg donation#egg donation california#egg donor
0 notes
Text

Explore the option of egg donor in Cyprus, a destination renowned for its high-quality fertility treatments and diverse donor pool. Gain insights into the screening process, donor selection criteria, and the supportive environment provided by clinics to intended parents seeking to realize their dream of parenthood.
0 notes
Text
Women who wish to begin their motherhood journey but are unable to with their own eggs due to various reasons, maybe they are born without ovaries, have entered menopause, unsuccessful IVF attempts, or people who have genetic diseases and do not want to pass it on to their children are the ones who can consider using donor eggs. Seeking assistance from an egg donor Mumbai can provide viable solutions for those facing such challenges.
0 notes
Text
Read FAQ about Egg Donor
0 notes
Text
Tips for Men Using Egg Donors
Embarking on the egg donor journey is a significant step for couples facing fertility challenges. While the focus often revolves around the woman's experience, it's crucial to recognize the role of men in this process. Here are six essential tips for men navigating the complexities of utilizing an egg donor:
Open Communication: Establishing open and honest communication with your partner is paramount. Discuss feelings, concerns, and expectations openly to ensure both partners are on the same page throughout the journey. This fosters a supportive environment and strengthens the bond between you and your partner.
Educate Yourself: Take the time to educate yourself about the egg donation process. Understand the medical procedures, emotional aspects, and legal implications involved. Knowledge empowers you to make informed decisions and be an active participant in the process.
Seek Emotional Support: The emotional aspect of using an egg donor can be challenging. Consider joining support groups, either in person or online, where you can connect with other men going through similar experiences. Seeking counseling or therapy can also provide valuable emotional support during this journey.
Be Involved in the Selection Process: Participate actively in the selection of the egg donor. Discuss criteria that are important to both you and your partner, such as medical history, personal traits, and values. Involvement in this process ensures that you feel connected to the choice being made.
Manage Expectations: Understand that the journey may have its ups and downs. Managing expectations and being adaptable to unforeseen circumstances is crucial. Recognize that each step forward, no matter how small, is progress toward building your family.
Celebrate Milestones: Celebrate milestones and achievements along the way. Whether it's a successful medical procedure or a positive emotional breakthrough, taking time to acknowledge and appreciate these moments reinforces the positivity in your journey.
Navigating the egg donor process requires both partners to be actively engaged and supportive. By following these tips, men can contribute to creating a more positive and fulfilling experience for themselves and their partners on the path to parenthood.
0 notes
Text
The Ultimate Guide to Understanding Egg Donation
Introduction
In the realm of assisted reproductive technologies (ART), egg donation stands as a beacon of hope for individuals and couples struggling with infertility. This remarkable procedure involves a woman, known as an egg donor, selflessly gifting her eggs to another woman, the intended recipient, who is unable to produce her own eggs due to various factors such as age, medical conditions, or genetic disorders. These donated eggs, carefully selected based on stringent egg donor requirements, are then meticulously fertilized with the sperm of either the intended father or a donor. Subsequently, the resulting embryos are strategically implanted into the recipient's uterus, following a detailed egg donation process. This creates a pathway to pregnancy, allowing the recipient to carry and birth a child, thus exemplifying the profound impact of the egg donation journey on the lives of those involved.
Demystifying Egg Donation: Understanding the Process and Rationale
Egg donation, also referred to as oocyte donation, emerges as a viable fertility treatment option for couples or individuals grappling with infertility challenges. It entails a process where one woman, an egg donor, generously donates her eggs to another woman, the intended recipient, empowering her to achieve the dream of pregnancy and parenthood through the intricacies of the egg donation process. This method has proven to be a transformative solution, offering hope and a renewed sense of possibility to those facing obstacles on their journey to building a family.
Egg donation is often considered when a woman faces difficulties in producing her own eggs for a variety of reasons, including:
Age-Related Decline in Ovarian Reserve: As women age, their ovarian reserve, the number of eggs available for ovulation, inevitably diminishes. This reduced ovarian reserve can lead to decreased fertility and hinder the likelihood of conception.
Medical Conditions Affecting Egg Production: Certain medical conditions, such as premature ovarian failure (POF), endometriosis, or ovarian cysts, can significantly impact a woman's ability to produce eggs.
Preventing Genetic Disorders: Individuals with genetic disorders may opt for egg donation to prevent passing on these disorders to their biological children.
Egg Donor Requirements: Ensuring Suitability for the Process
To become an egg donor, individuals must adhere to specific criteria, ensuring their suitability for this remarkable procedure and meeting the rigorous egg donation requirements. This careful selection process is in place to guarantee the health and well-being of both the egg donor and the intended recipient. Egg donors play a crucial role in providing a pathway to parenthood for those facing infertility challenges. By meeting the stringent egg donation requirements, donors contribute to the success of the egg donation process, facilitating the realization of dreams for individuals or couples longing to build a family.
Age: Typically, potential egg donors range from 21 to 35 years old.
Physical and Mental Health: Good overall health, no significant medical conditions, and no family history of major genetic disorders are essential for egg donors.
Psychological Evaluation: Emotional stability and suitability for the donation process are assessed through comprehensive psychological evaluations.
Commitment to the Process: Willingness to undergo medical evaluations, hormone therapy, and egg retrieval procedures is crucial for egg donors.
Navigating the Egg Donation Process: A Step-by-Step Guide
The egg donation process typically involves a series of meticulously planned steps:
Initial Screening: Potential egg donors undergo rigorous medical and psychological evaluations to assess their suitability for the donation process.
Ovarian Stimulation: The donor's ovaries are stimulated using hormonal medications to encourage the production of multiple eggs.
Egg Retrieval: The eggs are meticulously retrieved from the donor's ovaries through a minimally invasive procedure called ultrasound-guided transvaginal aspiration (TVA).
Fertilization and Embryo Transfer: The retrieved eggs are carefully fertilized with the sperm of either the intended father or a donor. The resulting embryos are nurtured in a laboratory, and the healthiest embryo is selected for transfer into the recipient's uterus.
Emotional and Ethical Considerations: Navigating the Complexities of Egg Donation
Egg donation is a complex procedure with both emotional and ethical considerations. For egg donors, the process can involve physical discomfort, hormonal fluctuations, and emotional challenges, underscoring the importance of comprehensive counseling and support tailored to address both the emotional and physical aspects of the egg donation process. Understanding and meeting the stringent egg donation requirements becomes pivotal in ensuring the health and well-being of the donors involved.
For intended parents, egg donation raises questions about genetic relationships, family dynamics, and the emotional well-being of the child. Open communication and counseling can empower intended parents to navigate these issues and prepare for the unique aspects of parenting a child conceived through egg donation. By embracing transparency and seeking support, both egg donors and intended parents can navigate the intricate emotional landscape that accompanies the egg donation process, fostering a more informed and compassionate approach to the journey of creating a family.
Conclusion: Embracing Hope and Understanding in the Realm of Egg Donation
Egg donation stands as a testament to human compassion and the unwavering pursuit of parenthood. It offers a valuable option for individuals and couples facing infertility challenges, providing a path towards fulfilling their dreams of family. While egg donation is a complex process with emotional, ethical, and medical considerations, understanding and meeting the stringent egg donation requirements are crucial aspects of ensuring the health and well-being of both egg donors and recipients.
It is important to recognize the profound impact the egg donation process has on individuals and families. Seeking comprehensive information, counseling, and support is essential for both egg donors and intended parents to make informed decisions and navigate the intricate emotional landscape that accompanies egg donation responsibly and successfully. By acknowledging the challenges and embracing the necessary support systems, individuals can embark on the journey of egg donation with confidence, compassion, and the shared goal of building families and creating new beginnings.
0 notes
Text
About half the ads I get are for paid egg donation, which is a little creepy cause they must know I'm a single fertile woman who doesn't currently want children and does need money and that's why I'm being targeted, but also very funny cause there's no way I'd even be allowed to donate. Like you can tell all this about me but you can't tell that I have ovarian issues and several genetic health conditions? Kind of a skill issue. I Google something like "should I go to martial arts after an asthma attack" or "what happens if I accidentally missed a lamotrigine dose" or "second ovarian cyst within six months" at LEAST twice a week idk why they can't put the pieces together I make it so easy for them
Like I'd totally do it for 8k but I promise you you do NOT want my eggs. I don't even want my eggs.
1 note
·
View note
Text
An egg donor in Ukraine is a woman who voluntarily provides her eggs for use in assisted reproductive procedures, such as IVF. Egg donation is a crucial aspect of fertility treatments for individuals or couples facing challenges with conception. Ukraine has become a popular destination for egg donation due to its established medical infrastructure and legal frameworks in assisted reproduction. Connect us now for egg donation services
0 notes
Text

Become a Surrogate
Are you dreaming of starting or growing your family but facing challenges on the path to parenthood? Surrogacy could be the beautiful solution you’ve been searching for.
Why Choose Surrogacy? Surrogacy offers a unique opportunity to create or expand your family, allowing you to be a part of every step, from conception to birth. It's a path that turns dreams into reality, providing a way for those who cannot carry a pregnancy to still experience the joy of parenthood. Reach out to us to learn more and take the first step toward your future family.
#surrogacy#surrogate mother#surrogacy california#surrogate#intended parents#fertility clinic#surrogacy process#egg donation#egg donation california#egg donor
0 notes
Text
Reproductive procedures' success is greatly influenced by the selection of the egg donor. Among many other considerations, individuals and couples considering using donor eggs for pregnancy should consider the donor's educational background.
0 notes
Text
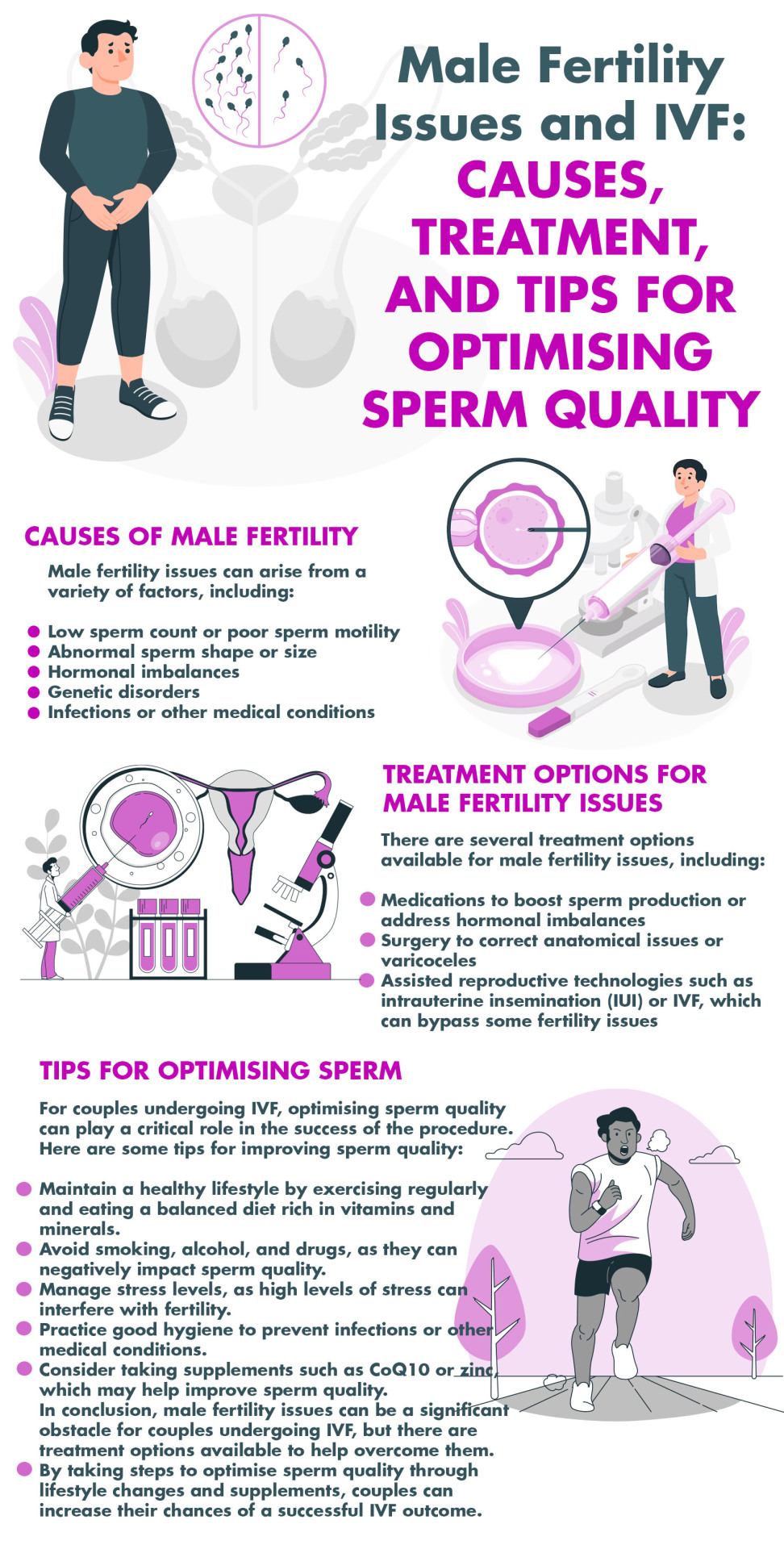
Male fertility issues have a global impact on many couples, contributing to nearly 40% of infertility cases and significantly affecting the success rates of in vitro fertilization (IVF). These problems, which include low sperm count, poor sperm motility, abnormal sperm shape, hormonal imbalances, genetic disorders, and infections, necessitate diverse treatment approaches like medications, surgeries, and assisted reproductive technologies such as IUI or IVF. To improve the likelihood of successful IVF outcomes, couples can optimize sperm quality through lifestyle adjustments, avoidance of harmful substances, stress management, good hygiene practices, and considering supplements like CoQ10 or zinc. Click here to learn more about male fertility issues.
0 notes
Last Seen Blogs

fbbmax
fbbmax

are-we-not-all-things
the-subsect

sapphic-skam
er du lesbisk?

dokidobe
yellow.dr.monv

its-justmythoughtsandstuff
Thoughts and Stuff