#spring tertiary. -10000
Photo
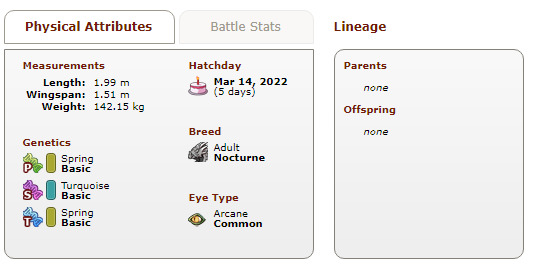


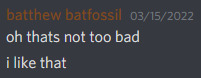


I hatched the ugliest double known to man. and then immediately went through the 5 stages of grief. and turns out it’s kind of hot, actually.
meet Halfway, named as such because she is my 88th double color hatched (spring), out of 177 total, and also my first ever double that I’m actually keeping, what the hell. (89 left to go in my quest to hatch doubles of all colors.)
#I'm picturing hall of the mountain king playing throughout my journey of self discovery#this dragon has everything that I should not like yet it slaps#arcane eyes. -10000#xyx. -10000#spring tertiary. -10000#HOW???#still has yet to be gened because I am tired and I don't feel like geneing right now but they will get it soon. soon#dragon share#thanks to another user for pointing out the ribbon eel scry you saved me#I know not perfectly halfway but it counts alright. we're rounding up
72 notes
·
View notes
Text
Top upcoming smartphones june 2019 in india redmi k20, asus zenfone 6, Oppo K3

Here's a list of smartphones and information that will be launched soon in June 2019 Redmi K20, Asus Zenfone 6, Oppo K3 many more.
Asus Zenfone 6:
Asus recently unveiled its much-awaited flagship a few days back at Spain, the Zenfone 6. The much-hyped smartphone from Asus has been trending in the country since launch. The company is yet to officially confirm the launch date in India, while it’s being expected to hit the country shores in mid-June. Zenfone 6 has been in the news for its unique flipping 48MP dual camera.

The unique technology has been used to offer a full-screen display in the form of a flippable twin camera module that doubles as a front and rear camera. Asus Zenfone 6 runs on the newest Snapdragon 855 with virtually stock ZenUI 6 supported android 9 Pie, a 48MP Sony IMX 586 sensor and an enormous 5,000mAh battery. The smartphone in India is expected to cost the same as its predecessor, Zenfone 5Z.
Key Specification:
Display 6.40-inch
Processor Snapdragon 855
Resolution 1080x2340 pixels
RAM 8GB
OS Android 9 Pie
Storage 256GB
Rear Camera 48-megapixel + 13-megapixel
Battery Capacity 5000mAh
Redmi K20:
The Redmi K20 can launch within the country in june calendar month aboard Redmi K20 professional and ultra-budget Redmi 7A. Backed by flagship-level options, Redmi K20 comes with associate in-display fingerprint sensing element, AMOLED notchless show, pop-up selfie camera, DC Dimming support and a lot of. DC dimming controls the smartphone brightness by variable the facility provide to the processor.

Redmi K20 boasts a 3D four-curved body that includes associate 6.39-inch AMOLED Full HD+ screen running on the recently launched octa-core Qualcomm flower 730 chipset with upto 8GB of RAM and 128GB storage.
Coming to optics, Redmi K20 packs in a triple rear camera that includes 48MP Sony IMX 582 sensing element together with an 8MP pic secondary sensor and a tertiary 13MP fisheye sensor, and eventually a 20MP pop-up selfie camera. it'll run on Android 9 Pie based mostly MIUI 10 with a 4,000mAh battery backing it supporting 18W quick charging.
Key Specification:
Display 6.39-inch
Processor Qualcomm Snapdragon 730
Front Camera 20-megapixel
Resolution 1080x2340 pixels
RAM 6GB
OS Android Pie
Storage 64GB
Rear Camera 48-megapixel + 8-megapixel + 13-megapixel
Battery Capacity 4000mAh
Redmi K20 Pro:
Xiaomi will reveal its absolute first leader arrangement under Redmi in the nation this June. We don't have authority date, however Redmi K20 Pro will launch at some point in June nearby the normal Redmi K20 and Redmi 7A. Prepared to take on the most recent OnePlus 7 arrangement, the up and coming Redmi K20 Pro is keeping no stone unturned. Redmi K20 Pro games a 3D four-bended body highlighting a 6.39-inch AMOLED Full HD+ screen supporting DC diminishing.

The smartphone will keep running on the most recent Qualcomm leader processor Snapdragon 855 with three cameras at the back, an indent less presentation, an in-show unique mark sensor and a spring up selfie camera.
Redmi K20 Pro will likewise keep running on the most recent Android Q beta form, a tremendous 4,000mAh battery supporting 27W quick charging and uncommon gaming highlights to offer the best of cell phone gaming background.
Key Specification:
Dual Sim, 3G, 4G, VoLTE, Wi-Fi, NFC
Snapdragon 855, Octa Core, 2.84 GHz Processor
6 GB RAM, 128 GB inbuilt
4000 mAh Battery with Fast Charging
39 inches, 1080 x 2340 px Display
48 MP + 13 MP + 8 MP Triple Rear & 20 MP Front Camera
Memory Card Not Supported
Android v9.0 (Pie)
Redmi 7A:
Xiaomi has unveiled its much-hyped entry-level Redmi 7A smartphone in China home market. the corporate can not wait to launch the phone in India as a successor to the much-hit Redmi 6A smartphone. Expected to be out at a similar value vary , the Redmi 7A smartphone return some upgrades and add-on options . it will have a similar 5.45-inch HD + show as Redmi 6A, same 13MP rear camera and 5MP front camera.

Redmi 7A can launch in India in June calendar month as a successor Redmi successor in the same price range alongside the Redmi K20 series.
Coming to upgrades, Redmi 7A are going to be steam-powered by a 12nm flower 439 chip, larger 4,000mAh battery, new MIUI supported Android 9 Pie and a brand new polycarbonate chassis style on the out giving P2i nano-coating for splash- resistance.
Key Specification:
Operating System Android v9.0 (Pie)
Display 5.45 inches (13.84 cm) bezel-less
display Design Splashproof Performance
Qualcomm Snapdragon 439 Octa core Processor
2 GB RAM
16 GB internal storage, expandable upto 256 GB
Camera 13 MP Rear Camera 5 MP Front Camera
Battery 4000 mAh battery
Connectivity Dual SIM: Nano + Nano (Hybrid) with VoLTE support
SIM1: Supports 4G, 3G SIM2: Supports 4G, 3G Special Features
No Fingerprint Sensor
Face Unlock
5 mm headphone jack present
Real Me X :
Realme recently launched its terribly initial notch-less flagship in China aboard a remodelled Realme three professional as Realme X lite. The new Realme notch-less smartphone runs on same snapdragon 710 chip as Realme 3 professional that includes a full-screen AMOLED display with Associate in-display fingerprint sensor embedded beneath the display.

The company has used a pop-up selfie sensor to supply higher screen space while not a notch.Recent rumours hint at a India launch within the second half of this quarter, Realme X could launch in India in either June finish, or in all probability July.
At the back, Realme X comes with twin cameras that includes the 48MP Sony IMX 586 sensor because the primary shooter. Realme X are launching in India before long, expected to begin at around Rs 18,000.
Key Specification:
Dual Sim, 3G, 4G, VoLTE, Wi-Fi
Snapdragon 710, Octa Core, 2.2 GHz Processor
4 GB RAM, 64 GB inbuilt
3765 mAh Battery with Fast Charging
53 inches, 1080 x 2340 px Display
48 MP + 5 MP Dual Rear & 16 MP Front Camera
Memory Card Supported, upto 256 GB
Android v9.0 (Pie)
Oppo K3 :
Oppo K3 smartphone was launched in 23rd May 2019. The phone comes with a 6.50-inch touchscreen display with a resolution of 1080x2340 pixels and an aspect ratio of 19.5:9.

Oppo K3 is powered by an octa-core Qualcomm Snapdragon 710 processor. It comes with 6GB of RAM.The Oppo K3 runs Android 9 Pie and is powered by a 3,765mAh battery. The Oppo K3 supports VOOC fast charging.
As so much because the cameras ar involved, the Oppo K3 on the rear packs a 16-megapixel primary camera and a second 2-megapixel camera. The rear camera setup has optical device. 16-megapixel camera on the front for selfies.
Key Specification:
Dual Sim, 3G, 4G, VoLTE, Wi-Fi
Snapdragon 710 , Octa Core, 2.2 GHz Processor
6 GB RAM, 64 GB inbuilt
3765 mAh Battery with Fast Charging
5 inches, 1080 x 2340 px Display
16 MP + 2 MP Dual Rear & 16 MP Front Camera
Memory Card Supported, upto 256 GB
Android v9.0 (Pie)
Also Read : Top Redmi Phones Between 5000 to 10000 Rs 2019
Vivo Z5x:
Vivo Z5x smartphone was launched in 24th May 2019. The phone comes with a 6.53-inch touchscreen display with a resolution of 1080x2340 pixels and an aspect ratio of 19.5:9.

Vivo Z5x comes with 4GB of RAM.The Vivo Z5x runs Android Pie and is powered by a 5,000mAh battery.
As far as the cameras are concerned, the Vivo Z5x on the rear packs a 16-megapixel primary camera with an f/1.78 aperture; a second 8-megapixel camera with an f/2.2 aperture and a third 2-megapixel camera with an f/2.4 aperture. The rear camera setup has autofocus. It sports a 16-megapixel camera on the front for selfies, with an f/2 aperture.
The Vivo Z5x runs Funtouch OS 9 based on Android Pie and packs 64GB of inbuilt storage that can be expanded via microSD card (up to 256GB). The Vivo Z5x is a dual-SIM smartphone that accepts Nano-SIM and Nano-SIM cards.
Key Specification :
Display 6.53-inch
Front Camera 16-megapixel
Resolution 1080x2340 pixels
RAM 4GB
OS Android Pie
Storage 64GB
Rear Camera 16-megapixel + 8-megapixel + 2-megapixel
Battery Capacity 5000mAh
Read the full article
1 note
·
View note
Link
Multiple sclerosis (MS) is a common neurological disease, and its etiology remains unknown. In recent years, increasing attention has been paid to the possible association between MS and vitamin D deficiency. Here, we review the current literature between MS and vitamin D, showing clear evidence that vitamin D deficiency is a risk factor for MS despite the lack of direct evidence for the effects of vitamin D in MS progression.
Multiple sclerosis (MS) is a chronic, inflammatory, and demyelinating disorder that affects the CNS.1 Multiple sclerosis is a common neurologic disorder; the estimated number of individuals with MS has increased from 2.1 million in 2008 to 2.3 million in 2013.2 Based on the 1975 Kurtzke classification,3 the Arabian Gulf Region is located in a low-risk zone for MS; however, recent studies suggest a moderate-to-high prevalence of MS in this region (31-55 MS patients per 100,000 individuals).4 The risk of MS is determined by genetic and environmental factors. One of the latter is vitamin D deficiency, which has attracted increased attention in the last decade.5 Entering the words “multiple sclerosis” and “vitamin D” as a PubMed search yields approximately 790 results in the last 10 years alone. Approximately one billion people worldwide have vitamin D deficiency or insufficiency.6 In a retrospective observational study of 10,709 patients in tertiary hospital clinics in Saudi Arabia, the prevalence of vitamin D deficiency was found to be 83.6%, which is high.7 The present article reviews the correlation between MS and vitamin D, considering updated studies from the literature.
Vitamin D metabolism
Vitamin D is a fat-soluble vitamin; its 2 main forms are ergocalciferol (vitamin D2), which is of plant origin, and cholecalciferol (vitamin D3), which is of animal origin. Vitamin D2 is considered less bioactive than vitamin D3. Vitamin D can be obtained from food, such as fatty fish, fortified foods, and vitamin supplements. However, the diet provides only a small percentage of human vitamin D intake, and the main source is skin exposure to sunlight. Total-body sun exposure easily provides the equivalent of 250 µg (10000 IU) vitamin D/d.8 In the skin, 7-dehydrocholesterol is photolyzed by ultraviolet radiation (UVR) from the sun and converted to pre-vitamin D3, which is isomerized to vitamin D3.9 The vitamin D binding protein transports vitamin D3 through the blood to the liver, where vitamin D is hydroxylated by one or more cytochrome P450 vitamin D 25-hydroxylases, resulting in the formation of 25-hydroxyvitamin D3 (25(OH)D3).10 Vitamin D status is reflected by serum levels of 25(OH)D3, which is the longest-living vitamin D metabolite (in terms of half-life).11 The 25(OH)D3 metabolite is further hydroxylated by renal CYP27B1 to 1,25-dihydroxyvitamin D [1,25(OH)2D; calcitriol], which is the most bioactive vitamin D metabolite. Vitamin D signaling is mediated by calcitriol binding to the vitamin D receptor, which forms a nuclear heterodimer with the retinoid X receptor. This complex is capable of binding to genomic vitamin D response elements, modulating the expression of a variety of genes.12 Also, like many other hormones, vitamin D can exert rapid actions at a cellular level (non-genomic effects), these actions are mediated within seconds to minutes.13 It is through these pathways that vitamin D modulates calcium hemostasis and performs its immunomodulatory functions.
Vitamin D as an immunomodulator
Vitamin D receptor expression has been reported in most immune cells,14 as well as in CNS tissues.15 Additionally, the rate-limiting enzyme for vitamin D synthesis, 25(OH)D3-1alfa-hydroxylase (CYP27B1), is expressed in immune cells. These cells are therefore, able to synthesize and secrete active vitamin D in both an autocrine and paracrine fashion,16 indicating that vitamin D plays a role in the immune system. The in vitro addition of 1,25-dihydroxyvitamin D3 (1,25(OH)2D3) to antigen-presenting cells (namely, monocytes, macrophages, and dendritic cells) inhibits the surface expression of major histocompatibility complex II-complexed antigens, and of costimulatory molecules, leading to reduced T cell stimulatory capacity. Additionally, 1,25(OH)2D3 directly exerts its immunomodulatory effects on T lymphocytes by inhibiting the production of Type 1 helper T cell cytokines (considered to be the key mediators in graft rejection and autoimmune diseases) and stimulating the production of Type 2 helper T cell cytokines, which have immunoregulatory functions.17 Furthermore, 1,25(OH)2D3 inhibits T cell and B cell proliferation and blocks B cell differentiation and immunoglobulin secretion. This compound also affects T cell maturation, inducing a shift away from the inflammatory T-helper 17 cells phenotype and facilitating the production of regulatory T cells.18 All of these immunomodulatory effects of 1,25(OH)2D3 can lead to the protection of target tissue in autoimmune diseases and transplantation. However, experimental studies have reported that the observed immunomodulatory effects of vitamin D only occur at hyper-physiologic concentrations, which causes hypercalcemia in humans.17 Therefore, the development of novel vitamin D analogs that have immunosuppressive effects, but do not cause significant hypercalcemia is required. Many clinical trials have been, or are currently being conducted to test the therapeutic application of vitamin D or its analogs in inflammatory processes.19
Vitamin D and MS risk
It is well known that MS is more prevalent in higher latitudes, where sunlight is of lower intensity than in lower latitudes. Recent meta-analyses20 supported a latitude gradient in MS prevalence. Several recent studies found that increased body exposure to sunlight, and hence a decreased susceptibility to vitamin D deficiency, is also associated with a decreased risk of MS,21-26 especially if the sun exposure occurred during childhood and adolescence. Studies have also shown that the birth month is correlated with MS risk; individuals born in the fall (namely, whose mothers were exposed to summer sunlight) have a low MS risk, whereas individuals born in the spring have a higher risk of MS. This observation indicates the presence of an association among maternal sunlight exposure during pregnancy, vitamin D status, and the risk of MS. In 2013, a systematic review27 analyzed published data on the effects of birth month for 151,978 MS patients born in the Northern Hemisphere. The results of this analysis demonstrated a significant increase of MS risk among individuals who were born in April and a reduction in risk in people who were born in October and November. However, sunlight also has an immunosuppressive effect,28 and UVR was recently found to suppress experimental autoimmune encephalomyelitis.29,30 Therefore, the effects of sunlight on MS risk could be related to sunlight itself; instead of vitamin D. Studies that evaluate either serum vitamin D levels or vitamin D intake, are needed to determine whether vitamin D deficiency is a risk factor for MS independent of sun exposure. The strongest evidence in this regard came from a large prospective case-control study31 of more than 7 million US military personnel from whom serum samples were obtained before any appearance of MS symptoms. This study concluded that, among Caucasians, there was a 41% decrease in MS risk for every 50-nmol/L increase in 25-hydroxyvitamin D; the effect was stronger for samples taken before the age of 20. Another case-control study32 prospectively collected blood samples from 192 MS patients and showed that serum 25-hydroxyvitamin D (25(OH)D) levels ≥ 75 (versus < 75) nmol/L in the blood were associated with a 61% decrease in the risk of MS. A recent study concluded that sun exposure and vitamin D status independently affect the risk of MS.24 Vitamin D intake and the risk of developing MS were assessed in a large prospective cohort that included approximately 200,000 women.33 In this study, the incidence of MS was 41% lower among women with a vitamin D intake of ≥ 400 IU/day, compared with women who did not take supplements.33 Another 2 studies concluded that the intake of fatty fish was associated with a decreased risk of MS, even at higher latitudes.34,35 Mirzaei et al36 studied a large cohort and analyzed the association between maternal milk intake, maternal dietary vitamin D intake, and predicted maternal serum 25(OH)D during pregnancy and their daughters risk of developing MS. The study showed that the relative risk of MS was significantly lower in women whose mothers had high milk or vitamin D intake during pregnancy than in women born to low-intake mothers.36 However, another study of a large cohort of US women showed that total vitamin D intake during adolescence was not associated with the risk for MS in adulthood.37 In addition, 25(OH)D levels during the neonatal period were not associated with the risk of MS in a large population-based case-control study.38 This data may support the hypothesis that vitamin D consumption throughout an individual’s entire lifespan, rather than over a short period of time, may contribute to the risk of MS.
Conclusion
In conclusion, it is clear from observational studies that vitamin D deficiency is a modifiable risk factor for MS. Therefore, persons who are at risk for MS (for example, first-degree relatives of MS patients, or patients with a single episode demyelinating attack) should be screened for vitamin D deficiency. As stated previously, evidence for the effect of vitamin D on disease progression is lacking, but it is known that MS patients have an increased prevalence for vitamin D deficiency (due to for example, immobility, sun avoidance, corticosteroids, and anti-epileptic use). These patients are also susceptible to osteoporosis.70 Therefore, vitamin D levels should be determined, and deficiency should be treated. The optimal serum vitamin D levels for exerting immunomodulatory effects have not been clinically established. Based on bone health criteria, the US and Canadian Institute of Medicine (IOM) recently stated that individuals are vitamin D sufficient at 25OHD levels ≥ 50 nmol/L; levels above 75 nmol/L have not consistently been associated with an increased benefit. Although risks have been identified for some outcomes at levels above 125 nmol/L, it has been suggested that up to 4000 IU/day of vitamin D intake is unlikely to cause toxicity, even in healthy individuals.71 Some experts favor maintaining 25(OH)D levels between 75 to 125 nmol/L in MS patients, as these levels are still within the safe range of the IOM report, and immunomodulatory effects have been observed in hyper-physiologic ranges in experimental studies. However, the long-term effects of such high levels are unknown.
2 notes
·
View notes
Last Seen Blogs

miamisslynn
One Day At A Time

ptysiaonhigh-blog
Bez tytułu

kgmioml
Kgmioml
thehtg-therealone
Untitled

nylilcosmos
nylil