
juniperpublishers-jgwh
Juniper Publishres | Journal of Gynecology
Journal of Gynecology and Women’s Health is a peer-reviewed, multidisciplinary, international journal of Juniper group that publishes scientific works within the field of obstetrics, gynecology and women’s health
153 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

luxxlavv
luxx lavv luxx

mahoutokoro-at-nagumo
Mahoutokoro at Nagumo

svaitaib
Svaitaib

purplefictionlover
Welcome

colettecrowe36-blog
Plastinės operacijos Lietuvoje
Text
Acute Intra Amnioti Infection Due to Streptococcus pneumonia

Authored by Ara Dadivanyan*
Introduction
Streptococci are Gram-positive bacteria. Species of Streptococci are classified based on their hemolytic properties as alpha-, beta-or gamma-hemolytic. Beta-hemolytic streptococci are further classified as groups A, B, C, D. The beta -hemolytic streptococci groups A and B are a serious threat to the newborn, and are a frequent cause of neonatal meningitis and septicemia. In the medical settings the alpha -hemolytic streptococci including S.pneumonia can cause serious infection in adults.
Alpha-hemolytic streptococci are best known because of Streptococcus pneumonia- recognized as a major cause of pneumonia in the late 19th century. Streptococcus pneumonia remains the most frequent cause of pneumonia in adults, immune compromised patients, and children. Streptococcus pneumonia causes community acquired pneumonia, a severe disease with the mortality rate 12% or greater Also, Streptococcus pneumonia is a leading cause of bacterial meningitis in adults and young adults in the USA with the mortality rate higher than from the disease caused by any other microorganism.
Streptococcus pneumonia rarely colonize the genital tract, but can cause maternal septicemia, and thus could also infect the fetus via hematogenous dissemination [1]. By it's ability to colonize the lower female genital tract, the parturitional threat to the neonate is real and potentially serious. The purpose of this report is to describe a case of intra-amniotic infection and perinatal septicemia due to Streptococcus pneumonia, and present a diagnostic and therapeutic plan if suspected in the future.
Case Report
A 25 year old female Gravida 3 para 2, at 36-weeks gestation with uncomplicated prenatal care, presented to labor and delivery with a history of 18 hours of spontaneous rupture of membranes (clear amniotic fluid), and complete cervical dilatation. One gram of cefoxitin IV was given for the prolong ruptured membranes followed by a precipitous vaginal delivery of a male infant .The infant Apgars were 9 at one minute, 9 at five minutes, and 8 at ten minutes. There was no history of maternal fever, or colonization with group B streptococcus. Placental cultures from maternal and fetal sites were performed. Placental Gram stain from maternal site demonstrated a few Gram- positive cocci in pairs, with no organisms seen in the fetal site. Microscopic examination of the placenta revealed acute signs of infection consistent with chorioamnionitis. The mother had an uncomplicated postpartum course, and was discharged a febrile on postpartum day one. Placental culture subsequently returned as positive for Streptococcus pneumonia.
At day 1, the infant was transferred from a regular nursery to the neonatal care unit, secondary to tachypnea. White blood cell count was 7.1K/uL with 18% polymorphonuclear cells, and 46% band forms. Hematocrit was 45%. Examination of the infant demonstrated chest retractions requiring oxygen on admission. Blood cultures were drawn. Ampicillin and gentamic in were started. Supplemental oxygen was administered and a chest X-ray showed diffuse infiltrates bilateral, suggesting diffuse areas of pneumonitis. The infant had transient tachypnea, but demonstrated adequate improvement, and oxygen was discontinued the following morning. Blood cultures from the neonate were negative, presumably due to the antepartum intravenous antibiotics, but placental cultures both in maternal and fetal sides indicated growth of Streptococcus pneumonia, which was sensitive to penicillin.Considering the symptomatology and the abnormal blood count, the infant was treated for seven days with ampicillin for suspected Streptococcus pneumonia sepsis. Gentamicin was discontinued after four days. The infant improved rapidly with the antibiotic treatment, and was discharged on the fourth day in a good condition.
Discussion
Streptococcus pneumonia is a Gram-positive alpha-hemolytic streptococcus best known by its ability to cause community acquired pneumonia and bacterial meningitis. It also, though un frequently, colonizes the lower female genital tract posing a parturitional threat to the neonate.
Maternal carriage of Streptococcus pneumonia has been reported to occur in 0.83% of all pregnancies [2]. Though rare, neonatal pneumococcal septicemia can be a highly lethal disease of the newborn. The incidence of the neonatal disease due to Streptococcus pneumonia is higher than the maternal carriage rate, and has been found to cause significant disease in 1 to 2% of infants with early neonatal sepsis [2,3]. The mortality of this condition is as high as 50% with 13% incidence of neurological sequel in the survivors [4].
Urogenital colonization of pregnant women with pneumococci appears rare and is not considered as a part of the normal vaginal flora. Pneumococcal genital infection was more common in the pre-antibiotic era, with a high lethality rate of 26% for localized infection, and 74% for peritonitis [1]. Today, mortality appears to be improving over the 25-year period from 1965 to 1990, as all 24 patients reported worldwide survived their pneumococcal genital infection [4]. We suspect that improvement in universal screening for hemolytic streptococci has resulted in early detection of Streptococcus pneumonia and thus the initiation of early and efficient treatment.
S.pneumonia may reach the fetus or newborn and potentially lead to neonatal infection via four possible mechanisms: transplacentally secondary to maternal bacteremia; ascending infection from the maternal genital tract; passage through a colonized birth canal; or postpartum by respiratory spread.
This highlights the importance to collaborate with microbiology laboratories to be alert to identify and report S. pneumonia when routinely screening for B-hemolytic streptococci. The clinical course of pneumococcal neonatal sepsis is similar to those seen with early onset group B streptococcal sepsis. It has been suggested that administration of penicillin prophylaxis during labor may prevent vertical transmission of pneumococcus to the newborn in patients with positive vaginal isolates [5], perhaps accounting for the drastic but welcome reduction in the neonatal incidence and mortality with S. pneumonia recently.
Because of the high morbidity and mortality of pneumococcal septicemia, it has been proposed that maternal vaginal cultures positive for pneumococcus should be regarded as pathogenic [1,2]. However, because reporting of pneumococcus from vaginal cultures in pregnant women is in consistent, it is unknown how many infants are exposed to pneumococci. Research investigating neonatal host defenses to this specific bacteria are insufficient, and many become necessary if the incidence or severity increases [1,2,6].
Although perinatal infections associated with Streptococcus pneumonia are rare, they may cause significant morbidity and mortality in both neonatal and puerperal patients. Given the reported poor outcomes of neonatal septicemia, maternal vaginal or infant cultures positive for pneumococcus should not be ignored, and these infants should be followed carefully. Based on the literature review, we also suggest that maternal carriage and neonatal colonization be monitored carefully to assess current trends. It should be aggressively treated with empirical antibiotic therapy and initiated during labor as is done with Group B beta-hemolytic streptococci) [3].
Although most of the S.pneumonia infected infants are successfully treated by the Group B streptococci protocols in place, it is important to understand the burden of each individual streptococcal species as resistance pattern may change in the future, as it has with the Group D streptococci.
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
https://juniperpublishers.business.site/
#gynecology#Juniper Publishers PubMed Indexed Journals#journal of gynecology and womens health#breastfeeding#reproduction#sex
0 notes
Text
Beauty Sleep: Sleep Quality for Women is More than a Myth

Authored by Deborah A Goss*
Abstract
The importance of sleep has always been recognized for daytime alertness and improved physical functioning. However, the effect of sleep on the body was frequently attributed to mainly affecting appearance, otherwise referred to as, "beauty sleep.” It was not until the modern era that the essential need for sleep in order to have normal physiologic functioning, and the possible role of disrupted sleep in early morbidity and mortality were recognized.
It is not surprising, that this impact extends to hormonal regulation and function in the female body. It can affect everything from menarche to menopause, and even to the development of comorbidities in women.A brief and focused history and physical exam can alert the clinician to the presence of sleep disorders which can affect maternal-fetal health, worsen post-partum depression, and exacerbate insomnia postmenopausal women. Similarly, it is well known that sleep disorders can worsen diabetes, hypertension, and weight gain; which afflict women at all stages of life. With the advent of home sleep testing, it has become even easier to diagnose many sleep disorders. Importantly, many sleep disorders have effective treatments which not only result in the restoration of normal sleep physiology, but improve the restorative quality and beauty of sleep.
Keywords: Sleep; Fertility; Pregnancy; Menopause; Hormone; Sleep apnea; Insomnia
Abbreviations: AHI: Apnea Hypopnea Index; CPAP: Continuous Positive Airway Pressure; OSA: Obstructive Sleep Apnea; PLMS: Periodic Limb Movement Syndrome; RLS: Restless Legs Syndrome; SIDS: Sudden Infant Death Syndrome
Introduction
Sleep quality effects Women's health during all stages of their lives, with a significant impact on reproductive years. From womb to tomb, sleep significantly affects the secretion and function of female hormones, which in turn, also affect the quality and quantity of sleep [1,2]. This relationship is not a static one. Constant and dynamic changes in body weight and proportion, oropharyngeal structure, hormone secretion, aging, inflammation, immunity and stress each have a role to play While the importance of this relationship is being increasingly recognized, the physiologic pathways and neurobiological controls are incompletely understood and have not yet been fully elucidated.
In addition to biological factors, psychosocial and societal expectations and stereotypes regarding sleep also play a role. This significantly impacts on how women perceive their sleep and the presence of sleep disorders, as well as their approach to obtaining a diagnosis and treatment. The culmination of which can influence morbidity and mortality. Interestingly, sleep is both a voluntary and an involuntary physiologic process which can be enhanced or inhibited to a certain degree, at will [3]. In essence, to some extent, a woman can choose to become a "good” or "bad” sleeper by behavioral changes and medical interventions. The subsequent quality of a young woman's sleep may influence everything from school performance and neurocognitive functioning to weight gain, medical illness, depression, infertility, injuries, and even early death. The focus of this mini-review, is to highlight the basic physiology and pathophysiology of female sleep and the most current and cutting-edge treatment strategies. This will include: normal sleep in women, the effect of sleep on fertility, pregnancy, post-partum depression, insomnia, and the diagnosis and treatment of common sleep disorders.
Discussion
Sleep in young women
During infancy and early childhood, there are few significant differences in the timing, duration and composition of the sleep cycle that are noted in the medical literature. However, the striking prevalence of Sudden Infant Death Syndrome (SIDS) in male infants has led to further studies of gender difference in infant sleep. Interestingly, female infants are less likely to arouse from sleep when exposed to a brief jet of air from a nasal cannula. This difference resolves by age three months [4]. One theory for the cause of SIDS is that it results from an immature autonomic response to reflux, leading to prolonged apnea, cardiac dysrhythmia and death [5]. While GERD may be slightly more common in females, estrogen may have a protective, anti-inflammatory effect against the damage it causes [6]. Similarly bedwetting, sleep walking, and obstructive sleep apnea are also more common in boys, but only obstructive apnea has been directly linked to testosterone.
Sleep and fertility
Puberty is marked by a surge in sex hormones. However, the earliest changes which trigger puberty are thought to center around lipid-related hormones which are, in part, controlled by sleep. In girls, decreased leptin and increased body mass index are thought to lead to increases in growth hormone. The secretion of growth hormone is maximal during sleep [2,7]. There is also a significant increase in grey matter in the brain, especially in girls, which is loosely associated with NREM sleep [8]. Puberty may also lead to delayed bedtime, also known as circadian phase delay, which also decreases fertility.
Adult women have increased slow-wave sleep and increased sleep spindles, compared to men. There are differences in the timing of delta sleep [9]. This in combination with the above, may partially explain the propensity of women towards fibromyalgia, which is hallmarked by the presence of alpha-delta sleep. Another sleep disorder which is also affected by gender is obstructive sleep apnea. Men have an increased rate of sleep apnea, which is attributed to increased testosterone and its deleterious effect on upper airway muscular tone and patency In comparison, women have a lower rate of sleep apnea, except in polycystic ovarian syndrome (PCOS) where the risk can increase by 30- to 40-fold. This is attributed to the high androgen levels that are seen in women with PCOS [10].
Sleep disruption (due to sleep apnea) and deprivation in adult women with PCOS (orin women who perform shift work) has been associated with increased dysmenorrhea, low fertility, increased miscarriages and lower birth rates. This is partly attributed to the disruption of normal reproductive hormones. Women with insomnia can also have decreased fertility. Ironically melatonin used as a treatment for insomnia can also decrease fertility in these women, and should not be used to treat insomnia in women trying to attain pregnancy [10]. Diphenhydramine and zolpidem may be reasonable alternatives, but have not been studied for this purpose. Obstructive sleep apnea, due to PCOS, can be effectively treated with nocturnal continuous positive airway pressure or CPAP. While this can restore normal sleep, the extent to which it can improve conception rates has not been rigorously studied.
In summary, normal sleep is key in the achievement and maintenance of a healthy pregnancy. According to the current literature, it is suggested that all women desiring pregnancy try to maintain seven hours of non-disrupted sleep a night, and avoid late-night bedtimes and shift work. What is not yet clearly delineated in the literature is if women with sleep disorders can have their fertility restored by receiving treatment to restore normal sleep.
Sleep and pregnancy
High progesterone levels in the first trimester of pregnancy can increase daytime sleepiness and fatigue which is characteristic of early pregnancy [11]. As pregnancy progresses, there is significant weight gain and increased upper airway congestion and edema, which can lead to increased snoring and the development or worsening of obstructive sleep apnea. Gestational sleep apnea is linked to an increased risk for complications in pregnancy, including diabetes, hypertension and low birth weight. Whether this is a causal association is uncertain. There are also increased awakenings during pregnancy. This has been attributed to physical discomfort and to hormonal shifts in preparation for nocturnal feedings and infant care post-delivery.
While physical discomfort may disrupt sleep during any trimester, women who complain of discomfort should be asked particularly if they have increased discomfort in their lower extremities, as this can be a symptom of restless legs syndrome (RLS) periodic limb movement syndrome (PLMS). PLMS does occur at high rates in pregnancy, and is worse in the third trimester, when estradiol levels are maximally elevated [12]. However, it is also associated with iron deficiency anemia and uremia and screening labs for these disorders should also be performed. Treatment with iron and folate may improve symptoms in deficiency states, but frequently opioids are required for substantial relief with minimal data available on the best management and dosages.
Gastroesophageal reflux is also increased in sleep in pregnancy and may contribute to the increased incidence of asthma and pneumonia in this population. Diet and lifestyle changes may significantly improve reflux, with avoidance of late night eating and caffeine, in combination with elevation of the head of the bed. Calcium and magnesium supplements are frequently used for mild symptoms, escalating to H2-blockers and proton pump inhibitors for more severe symptoms [13].
Sleep and post-partum period
During young adulthood, many women will voluntarily restrict their sleep to pursue social activities. However, sleep disruption is significantly increased when caring for a newborn. When total sleep time is less than six hours a night, chronic sleep deprivation can occur. Over time, this can lead to impaired glucose metabolism, weight gain and hormonal imbalance [14]. With the addition of a sleep disorder, this is significantly magnified. It can lead to maternal and fetal complications [1517] and turn what should be a time of great happiness and joy, into a time of frustration, exhaustion and depression. For example, treatment of sleep apnea with CPAP may be impractical for a Mom who must leave her own bed very 2-3 hours to care for a newborn and then repeatedly replace her mask and restart her machine. Bed sharing (i.e., infant sleeping in same bed as Mom), is generally discouraged as this can lead to injury to the newborn and poor sleep for the parent.
In addition to medical sleep disorders, serious and potentially fatal psychological disorders, such as depression, bipolar disorder and psychosis, can be triggered and/or exacerbated by sleep loss [14]. These may be mitigated or exacerbated by lactation and breast feeding, which may lead to either improved satisfaction and mood, or frustration and increased sleep loss in which bottle-feeding may significantly improve maternal sleep. Post-partum depression has been found to be worsened by sleep loss, particularly with increased sleep latency and wake after sleep onset [18]. This is an interesting finding, as depression in general, is generally improved by restriction of total sleep time. More studies are clearly needed.
Menopause and sleep
The total quantity of slow wave sleep is diminished as women age. Slow wave sleep is restorative sleep, which results in feeling "refreshed” in the morning. Men tend to lose SWS at an earlier age than women do. After the age of 65, about one third of women report increase difficulty falling asleep and increased awakenings during the night. Sleep disorders, including insomnia, obstructive sleep apnea, PLMS and circadian rhythm disorders also increased in this age group. The combination of the above resulting in difficulty falling asleep, frequent nocturnal awakenings, and then early morning awakening and late afternoon napping [11]. Treatment for sleep apnea in this age group is no longer limited to nocturnal mask ventilation. The availability of small implantable hypoglossal nerve stimulators now allows for a more comfortable and practical solution for women who are intolerant of nocturnal continuous positive airway pressure ventilation (CPAP).
The increase in obstructive sleep apnea may be directly related to the loss of estrogen, which promotes sleep and progesterone, which in addition to estrogen, also may be somewhat protective against apnea and stimulate breathing. It is the loss of estrogen which is also associated with the increased risk of insomnia. Oddly, the supplementation of estrogen and progesterone during menopause does little to improve sleep complaints [19], while targeted sleep therapies for insomnia and vasomotor symptoms during menopause are usually quite effective.
Focused sleep history and physical exam
As described above, there is a marked impact of sleep disorders on the health and well-being of women. It is therefore important for all clinicians caring for these patients to be able to effectively screen for these disorders and recognize when further diagnostic evaluation and treatment is warranted.
A basic sleep history includes and evaluation of the patient's bedroom environment, sleep hygiene, timing of sleep onset, sleep duration, sleep disruption and wake times. It is recommended that the sleep environment be a cool (65 °F or 18 °C) room which is quiet and dark [20]. Light, including both sunlight and electronics, is to be avoided. Sleep onset should be within 30-60 minutes of entering the bed and sleep duration is recommended to be approximately seven hours. If there is a prolonged awakening, the sleeper is encouraged to leave the bedroom and engage in a quiet and non-stimulating activity and return to bed when sleepy. The amount and frequency of sleep disruption during the night should also be noted.
On physical exam, pupil size inconsistent with the luminosity of the room may be related to either excessive daytime sleepiness or to substance abuse. It is not uncommon for patients with sleep disorders to self-medicate with diphenhydramine, melatonin, caffeine, alcohol or other substances. It is worth inquiring with patients what non-prescriptive and/or herbal treatments they are using. The external neck circumference [21] as well as the narrowness of the oropharyngeal airway is also associated with sleep apnea [22]. While, morbid obesity increases the likelihood of sleep apnea, but even patients of normal weights can have severe apnea. However, for the non-Sleep clinician, the use of the STOP-BANG survey and Epworth Sleepiness Scale may be the easiest and effective basic screenings for sleep disorders [23].
Conclusion
It has been clearly shown that the quality and quantity ofsleep can have a dramatic impact on Women's health. The treatment of an underlying sleep disorder, can improve a patient's daytime functioning, and lead to improvement in the management of obesity, depression, diabetes and hypertension. Sleep disorders can be easily screened for by clinicians with a brief clinical assessment and effectively treated. It is also clear that having an adequate quantity of quality sleep can lead to improved physical and mental health, as well as decreased weight, and even improved appearance (with decreased skin aging and improved recovery from UV light exposure [24]. It therefore appears that the ugly truth is that quality sleep is essential for the normal function of the female body, and revealing the beauty without and within.
Acknowledgement
Special thanks to Dr. Abdulla Al-Khan from the Department of Maternal Fetal Medicine at Hackensack University Health Center for many informative conferences and multidisciplinary management of women with complex pulmonary and sleep disorders in pregnancy
Conflict of Interest
Dr. Goss- None. Dr. Ashtyani- None.
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
https://juniperpublishers.business.site/
#Juniper Publishers PubMed Indexed Journals#Juniper Publishers#gynecology#womens health#sexual health#breastfeeding#breast cancer
0 notes
Text
Female Empowerment as Part of the Solution to HIV/AIDS in Tanzania

Authored by Catherine Craig*
Perspective
In less economically developed countries (LEDCs), such as Tanzania, HIV/AIDS is a disease of poverty where prevalence rates are higher for women than for men. The World Health Organization (WHO) stated in 2012 that HIV/AIDS was the second leading cause of death in less economically developed countries (LEDCs) [1].
Although the rates are likely underestimated due to lack of infrastructure for national reporting systems, the HIV rate was reported as 4.7% in 2015, which translated to 1.4 million people living with HIV [2]. The HIV rate in Tanzania is disproportionately higher for women than for men. According to the 2011-2012 Tanzania HIV/AIDS and Malaria Indicator Study (THMIS), the prevalence rate among women was 6.2% whereas the prevalence rate for men was 3.8% [3]. For women, the HIV prevalence was 1% at ages 15-19 and 10% at ages 45-49.4
Because HIV prevalence is higher in women and because the modes of transmission make women vulnerable to infection, empowering women should help to combat HIV and to decrease prevalence rates. In Tanzania, for instance, 80% of HIV infection is transmitted through sexual activity with a heterosexual partner [4]. Thus, if women had more support through education, gender equality initiatives, and control over safe sexual practices, then the rate should decrease in the female population.
Education about HIV is insufficient in schools and communities, with less than 50% of adolescents having adequate knowledge [5,6]. It was estimated that in 2014, 6% of adolescents ages 10-19 were HIV positive [7]. Even if sexual education is available in schools, children often do not complete their education. For example, in 2012 only 45% of secondary students ages 14-17 were enrolled in school [8]. Enrollment rates in schools are even lower for girls. Reasons for this include early pregnancies, lack of access to bathrooms during menstruation, sexual harassment by male teachers and early forced marriages [9].
Gender inequality is another major contributor to high rates of HIV in Tanzanian women. Although gender inequality is illegal, as stated by the Tanzanian Constitution, women often feel powerless to refrain from having sexual intercourse or safer sex with an HIV-infected partner [10]. By refusing to have sexual relations, women are often forced from their homes and consequently lose their financial security [11]. In addition, they are more at risk of sexual assault, with 48% of married women reporting sexual violence in 2010 [3,12]. Women also tend to contract HIV at an earlier age than men, both because they often marry older men and marry earlier in life [13]. For example, a study of Tanzanians aged 15-24 reported that in 2012 there were about 26,000 new infections in women and about 14,000 in men [14].
Several other activities including condom use, polygamy, and prostitution also influence HIV prevalence. Condom use decreases the likelihood of transmitting HIV by 88% [15]. Consequently, the Tanzanian government has implemented a program to supply free condoms. However, distribution to rural areas can be problematic. Also of concern is the Demographic and Healthy Survey and Malaria Indicator Survey 2015-16, which revealed that only 15% of sexually active unmarried women used condoms [16]. Due to inequality in many sexual relationships, women often do not have the power to insist that their partner use a condom.
The practice of polygamy, which is legal under the constitution of Tanzania, is another risk factor that increases the risk of HIV transmission [17]. Contributing to this practice are mobile populations including miners, long distance truck drivers, fishermen, and plantation workers. These men often have sexual activity with sex workers, putting themselves at increased risk of contracting HIV, and then, in turn, infecting their other female partners [18]. This is demonstrated by the International Organization for Migration in 2015, whereby 100% of truck drivers in Dar es Salaam interviewed reported sexual relationships with women at truck stops whom they described as their second wives [19].
Prostitution adds to the high rate of sexual transmission of HIV, especially for women living in poverty, as it provides them with a source of income needed to survive [20]. In addition, if women are IV drug users, their rate of HIV prevalence is double that of their male counterparts. The reason for this is unclear, but it is postulated that if female sex workers are also sharing needles with their customers, then they will be the last to receive the shared needle, thus increasing their potential exposure to an HIV-contaminated needle [21]. Unsafe sexual practices including lack of condom use, polygamy, and prostitution each increase the risk of contracting HIV and if these risk-taking behaviours occur simultaneously, this leaves women even more vulnerable.
Just as women do not have the power to prevent themselves from acquiring HIV, they are similarly limited in their ability to prevent transmission of HIV to their newborn infants. Mother-to- child transmission (MTCT) accounts for almost 20% of new HIV infections in Tanzania [22,23]. 4 Antiretroviral therapy (ART) is provided free through government programs during pregnancy and childbirth and use of ART significantly decreases the risk of transmission to the newborn. Educating and empowering pregnant women to access ART will continue to decrease the rate of MTCT. As of 2015, 14% of pregnant women were not receiving effective ART. However, this is an improvement from 2013, at which time 23% did not receive ART [4]. Other factors responsible for the high rate of MTCT are ineffective ART drug regimens, drug stock-outs, and lack of compliance to treatment [4]. Some ART should be taken with food to avoid gastrointestinal side effects, but impoverished pregnant women cannot always rely on the availability of food, and thus may have poor adherence to treatment. Additionally, if the HIV viral load is high or unknown or if the woman is not taking ART, cesarean section would ideally be performed to decrease the rate of MTCT. However, with an extremely low healthcare worker to patient ratio (3.1:10,000 in 2012), most medical facilities in Tanzania cannot offer cesarean section due to lack of equipment and trained healthcare workers. Following birth, most Tanzanian women breastfeed, regardless of their HIV status, to decrease the risk of infant death from malnutrition. ART is recommended during breastfeeding to decrease MTCT; however, lack of access to ART, drug stock-outs, and intolerable side effects to ART compromise use of ART while breastfeeding as well.
There are several factors that contribute to the high rate of HIV in Tanzanian women, in particular, lack of HIV-related education, gender inequality, and lack of access to resources. If women were given more opportunity to develop strategies to access education and become more financially independent, they could become empowered to minimize the risks of contracting or transmitting HIV in the future.
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
https://juniperpublishers.business.site/
#gynecology#women's health#reproductive health#sex#breastfeeding#Pcos#PCOD#open acess journals#Open acess Publishers
0 notes
Text
Case of Spontaneous Heterotopic Pregnancy in Patient with Intrauterine Contraceptive Device
Authored by Maheshgir S Gosavi*
Abstract
Heterotopic pregnancy is defined as the coexistence of intrauterine and extrauterine gestation. The incidence of heterotopic pregnancy is very low. The frequency was originally estimated on theoretical basis to be 1 in 30,000 pregnancies. We present a rare case of heterotopic pregnancy with non viable intrauterine gestation and right adnexal gestation in a natural conception.
Keywords: Transvaginal sonography; Heterotopic pregnancy; Intra-uterine contraceptive device
Case Presentation
A 32-year-old woman with 6 weeks of amenorrhea presented for emergency ultrasound scan of pelvis with clinical features of p.v.bleeding, lower abdominal pain. Urine pregnancy test was positive.
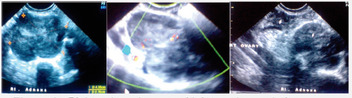
Transvaginal ultrasound revealed mild amount of free fluid in the peritoneal cavity with a intrauterine gestation corresponding to 4 weeks 4 days. Subchorionic hematoma is noted. A complex ill defined right adnexal mass measuring approximately 4.6x3.4cm was also noted (Figure 1). The Doppler study of right adnexal mass showed low resistance flow.
Right ovary is visualised separately from this lesion. Left ovary shows cystic lesion (corpus luteal cyst) measuring 4.6x3.4cm.
I.UC.D was seen in cervix and lower uterine cavity
Provisional diagnosis of a heterotopic pregnancy with ruptured right ectopic gestation was suggested in view of clinical history, mild amount of free intraperitoneal fluid, and an intrauterine gestation. The patient underwent emergency laparotomy. There was ruptured right-sided tubal pregnancy with hemoperitoneum and right salphingectomy was done; curettage of intrauterine pregnancy was done (Figure 2).
Pathology confirms the diagnosis of right tubal ectopic pregnancy and non viable intrauterine gestation.
Discussion
A heterotopic gestation is difficult to diagnose clinically. Typically, laparotomy is performed because of tubal pregnancy. At the same time, uterus is congested, softened, and enlarged; ultrasound examination can nearly always show gestational products in uterus.
The incidence was originally estimated on theoretical basis to be 1 in 30,000 pregnancies. However, more recent data indicate that the rate is higher due to assisted reproduction and is approximately 1 in 7000 overall and as high as 1 in 900 with ovulation induction [1].
The increased incidence of multiple pregnancy with ovulation induction and IVF increases the risk of both ectopic and heterotopic gestation. The hydrostatic forces generated during embryo transfer may also contribute to the increased risk [2] (Figure 3 & 4).
There may be an increased risk in patients with previous tubal surgeries [3].
Heterotopic pregnancy can have various presentations. It should be considered more likely
a. After assisted reproduction techniques.
b. With persistent or rising chorionic gonadotropin levels after dilatation and curettage for an induced/spontaneous abortion.
c. When the uterine fundus is larger than for menstrual dates.
d. When more than one corpus luteum is present in a natural conception.
e. When vaginal bleeding is absent in the presence of signs and symptoms of ectopic gestation [4].
A heterotopic gestation can also present as hematometra and lower quadrant pain in early pregnancy [5].
Most commonly, the location of ectopic gestation in a heterotopic pregnancy is the fallopian tube. However, cervical and ovarian heterotopic pregnancies have also been reported [6,7].
Majority of the reported heterotopic pregnancies are of singleton intrauterine pregnancies. Triplet and quadruplet heterotopic pregnancies have also been reported, though extremely rare [8,9]. It can be multiple as well [4]. They can be seen frequently with assisted conceptions.
Intrauterine gestation with hemorrhagic corpus luteum can simulate heterotopic/ectopic gestation both clinically and on ultrasound. Other surgical conditions of acute abdomen can also simulate heterotopic gestation clinically and hence the difficulty in clinical diagnosis. Bicornuate uterus with gestation in both cavities may also simulate a heterotopic pregnancy.
High resolution transvaginal ultrasound with color Doppler will be helpful as the trophoblastic tissue in the adnexa in a case of heterotopic pregnancy shows increased flow with significantly reduced resistance index.
The treatment of a heterotopic pregnancy is laparoscopy/ laparotomy for the tubal pregnancy
The illustrated case did not have any risk factor for the heterotopic gestation and presented with ruptured tubal pregnancy and history of p.v.bleeding. Patient did not suspected pregnancy as she had I.U.C.D insertion and was post partum last delivery 8 months back.
A heterotopic pregnancy, though extremely rare, can still result from a natural conception; it requires a high index of suspicious for early and timely diagnosis; a timely intervention can result in a successful outcome of the intrauterine fetus.
Conclusions
A spontaneous heterotopic pregnancy can occur in patients who have no known predisposing factor. Early diagnosis has made this disorder amenable to appropriate management. The high-resolution Transvaginal Sonography is very helpful in the diagnosis of this condition [10,11].
Acknowledgement
The author would like to thank the pathologists, gynaecologists who provided very important feedback with regard to the clinical aspect of this patient's condition. They contributed significantly to the patient being promptly diagnosed and receiving a high standard of care.
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
https://juniperpublishers.business.site/
#journal of gynecology and womens health#Juniper Publishers PubMed Indexed Journals#gynecology#reproductive technology#gynecological cancers#gynecology clinic
0 notes
Text
Long Acting Reversal Contraception: Perceptions of High School and Undergraduate Students on a Medical Track

Authored by Stephen Wagner*
Introduction
Despite being the only reversible, top tier, form of contraceptive, currently less than 13% of women utilize LARCs, or long acting reversible contraceptives (American College of Obstetricians and Gynecologists, 2015; American Congress of Obstetricians and Gynecologists, 2011) [1]. LARCs are classified into 3 types: Copper Intrauterine device (1UD), levonorgestrel Intrauterine device, and Etonogrestrel rod contraceptive implants. These three forms of contraceptives are thought to be just as effective as irreversible female sterilization methods and last for anywhere from 3-10 years [2,3]. Unlike other forms of contraceptives, studies have found that women prefer these methods, which have a rapid return to fertility after stopping their use and a lack of day-to-day administration [4]. Furthermore, there are very few restrictions as to who is eligible to receive LARCs. According to the CDC and WHO, there are only 3 groups of women who should be cautious with LARC use: women who are postpartum and breast feeding, those who are at increased risk for deep vein thrombosis or pulmonary embolisms, or women who are at increased risk of uterine fibroids with uterine distension [4,5].
The copper 1UD is a T shaped device wrapped in copper wire that is placed in the uterus and thought to exert mostly pre-fertilization inhibition. This includes inhibition of sperm migration and viability and destruction of the ovum before fertilization [1-3]. The levonorgestrel 1UD is a similar T shaped device as seen with copper lUDs, but instead of being wrapped in copper, it secretes a form of progesterone. 1n addition to the pre-fertilization effects seen with copper 1UDs, there is also an alteration of the amount and thickness of the cervical mucus as well as suppression of endometrial growth. These changes have an effect on the ability of sperm to enter the uterus as well as an effect on the ability of an egg to successfully implant in the endometrium [6]. The copper 1UD has been approved for use up to 10 years while the levonorgestrel has been approved for up to 5 years. Lastly, the etonogestrel rod contraceptive implant is a single rod that is placed sub-dermally and continuously secretes etonogestrel, a form of progesterone, which suppresses ovulation by altering the Hypothalamus-Pituitary-Ovarian axis and by altering the thickness of the cervical mucus, once again successful sperm entry into the uterus [6-9].
Due to the lack of day-to-day administration, LARCs have been implicated in significant reduction in pregnancy rates in populations that do use them. Yet, despite all the benefits, very few women use them, with the most common reasons being barriers to access [5,10,11]. These barriers include higher upfront costs, lack of provider training, and patient awareness. Despite higher upfront costs, studies have shown that LARCs, such as 1UDs, are found to be the cheapest contraceptive method over the course of 5 years [12]. Without financial barriers, patients can often run into the issue of not finding a trained provider to perform the insertion. For example, the contraceptive implant requires special training before performing the procedure [5]. Communities which may experience lack of healthcare access overall, may not have access to a physician who is able to perform LARC procedures. Lastly, one of the major theorized barriers to access is the lack of patient education regarding LARCs. LARCs can be used in many different scenarios, are extremely effective and have very few, rare, complications however, most women are still unaware of these advantage [13]. The gap in education regarding LARCs will be the main focus of our study.
Method
A "primary care workshop” was arranged through the family medicine department at a tertiary care academic center. Target participants were undergraduate students from a number of local colleges and universities who had expressed an interest in pursuing careers in medicine. This single day event entailed a number of lectures, and a variety of small group "breakout” sessions where individuals could obtain additional education in areas of interest.
Residents in obstetrics and gynecology were invited to participate and lead a "breakout” session on contraception. These 30 minute sessions involved both a structured lecture and then a simulation aspect. During the simulation students were invited to place implants and lUDs on mannequins. Immediately prior to and after these sessions students were invited to complete voluntary surveys to assess their knowledge on the subjects covered during the presentation.
45 students in total participated in the four "breakout” sessions offered on contraception. Of these 45, 42 elected to complete the surveys. Following completion the data was collected and compiled in Microsoft Excel. Statistical analysis was performed with both Microsoft Excel and Graphpad Quickcalc. Student T tests were utilized and p values <.05 were considered significant.
Results
On a Likert scale of 1-5, 1 being the most efficient, the average perceived efficiency of each method changed from preworkshop to post workshop. As seen in Table 1, the perceived efficiency of Implant and OCPs both showed a significant change with p-values <0.05. Initially, the average efficiency for the contraceptive implant was ranked as 2.44 which decreased to 1.89 after the workshop with a p-value of 0.036. The perceived efficiency of over the counter pills (OCP) in the pre-workshop test was 2.44 which increased to 3.02 after the workshop with a p-value of 0.005. Additionally, changes in perceptions about the efficiency of using a Condom, IUD, and withdrawal method were also seen but with p values >0.05. Initially, the average efficiency for condoms was ranked at 3.13 and after the workshop, the average increased to 3.56 (p-value=0.069). The average efficiency of IUD use was 2.43 and decreased to 1.97 with a p-value of 0.111 and the average efficiency of the withdrawal method was 4.51 before the workshop and 4.57 after the workshop with a p-value of 0.85 (Table 1).
Table 2 shows the change in responses to various perceptions about LARC use. Initially, 50�x0025; of participants did not think that Tubal ligation is more effective than IUD. After the workshop, 74.4% of participants did not think that tubal ligation is more effective than IUD and 25.6% did think it was more effective (p-value 0.03). When looking at the use of Paraguard in emergency contraception, pre-workshop 33.3% of applicants thought it could be used in emergency while 66.7% thought it could not be. Post workshop, 82 % thought it could be used as emergency contraception while 18% thought it could not (p-value 0.0001). Additionally, when asked about the use of Mirena as emergency contraception, 65% of participants did not think that it could be used while 35% did think it could be used. After the workshop,64.1% thought it could be used while 35.9% did not think it could be used for emergency contraception (p=value 0.87). When asked about how long after intercourse an IUD can be used as emergency contraception, 39% thought it could not be used for up to 5 days afterwards while 70% did think it could be used. After the workshop, 18% thought it could not be used for up to 5 days after intercourse while 82% did think it could be used (p-value=0.02). When asked to assess the statement "OCPs are cheaper than IUD over the course of 3 years”, before the workshop 52.3% of participants thought this was false while 48.7% thought this was true. After the workshop, 77% of participants thought this was false and 23% thought this was true (p=0.02). When asked about risks 55% of participants thought that IUD use was associated with increased risk of ectopic pregnancy while 45% did not. After the workshop, 61.5% of participants did not think that IUD use was associated with an increased risk of ectopic pregnancy while 38.5% thought there was an increased risk (p-value=0.174). Lastly, before the workshop 52.5% of participants disagreed with the statement that "1UDs are associated with increased risk of weight gain” while 47.5% agreed. After the workshop, 71.8% thought it was a false statement while 28.2% thought it was a true statement (p-value=0.10)
When looking at demographic data such as gender, table 3.1 shows that the average perception of effectiveness of OCPs among females changed from 2.321 to 3.080 with a p-value of 0.0005. Females also changed their perception of IUDs from 2.552 to 1.772 with a p-value of 0.013. Other perception changes from pre-workshop to post-workshop among females showed a p-value >0.05. The perceived efficiency of condoms decreased from 3.036 to 3.520, Implant efficiency perceptions increased from 2.464 to 2.000, and withdrawal's perceived efficiency decreased from 4.571 to 4.692. Similarly, with malestable 4.1 shows that all the changes in perceptions of the efficiency of various contraceptive methods had a p-value of >0.05. The perceived efficiency of condoms decreased from 3.264 to 3.636, the perceived efficiency of implants increased from 2.364 to 1.626, the perceived efficiency of OCPs decreased from 2.818 to 2.909, and the perceived efficiency of withdrawal increased from 4.364 to 4.273.
When females were asked about various perceptions regarding LARC use, three statements saw a significant change from pre-workshop and post-workshop answers with p-values <0.05 (Table 3.2). Before the workshop, 30% of women agreed that Paraguard can be used for emergency contraception and after the workshop, 81.5% of women agreed (p-value=0.0001). Before the workshop, 51.8% of women agreed that IUDs can be used up to 5 days post intercourse for emergency contraception and after the workshop, 85.2% of women agreed (p-value=0.007). Furthermore, before the workshop, 46.4% of women disagreed with the false statement "1UDs are associated with weight gain” and after the workshop 74.1% disagreed (p-value=0.037). All other statements saw a change in perceptions but with p-values >0.05. In male responses, Table 4.1, there was only a significant change in perception of emergency use of Paraguard. Before the workshop, 41.7% of males agreed with the statement that Paraguard can be used for emergency contraception. After the workshop 90.9% of men agreed with the statement (p value=0.012). All other statements saw changes but with p-values >0.05 (Table 4.2).
When looking at private university students, we found there was a significant change in perception regarding the efficiency of OCPs before and after the workshop (Table 5.1). Before the workshop, the average effectiveness of OCPs was ranked at 2.44 while after the workshop, the average effectiveness of OCPs was ranked at 2.94 (p-value=0.033). All other perceived efficiencies saw a change before and after the workshop but with p-values >0.05. The perceived efficiency of condoms changed from 3.28 to 3.61, implants changed from 2.11 to 1.78, IUDs changed from 2.61 to 1.89, withdraw perceived efficiency changed from 4.56 to 4.78 (Table 5.1). When assessing public university students, we saw changes in perceived efficiency from pre-workshop to post-workshop, however all had p-values >0.05. The ranked efficiency for condoms changed from 3.00 to 3.5, for implants it changed from 2.71 to 2.00, for OCPs it changed from 2.48 to 3.11, for IUDs it changed from 2.27 to 2.08, for withdraw it changed from 4.48 to 4.368 (Table 6.1).
Among private university students, the most significant change was seen in response to using IUDs as emergency contraception. Before the workshop, 26.3% of students agreed that Paraguard can be used as emergency contraception and after the workshop, 88.2% agreed (p-value=0.0002). All other statements saw a change in the percentage that answered right with p-values >0.05 (Table 5.2). In public university students, the same statement saw a significant change after the workshop.Before the workshop, 39.1% agreed that Paraguard can be used for emergency contraception. After the workshop, 85% agreed (p-value=0.002). Another significant change was seen regarding the false statement that "OCPs are cheaper than IUD over 3 years”. Before the work shop, 33.3% of students false and after the workshop the percentage that answered false rose to 65% (p-value=0.044). All other statements also saw a change in before and after responses to statements with p-values >0.05 (Table 6.2).
Discussion
This study confirmed that misconceptions about LARC use are still widespread. Though educating young adults about LARCs, there can be better awareness and knowledge to support their use in general populations. For example, the perceived efficiency of implants saw a significant increase after the workshop session. Furthermore, many of the true or false questions asked about LARC use played off misconceptions in the general public. We saw that after the workshop, there was a significant shift in the percentage of people identifying the statement correctly as either true or false. Based off the results, some common misconceptions that were significantly clarified after educational intervention were: Tubal ligation is more effective than IUDs, Paraguard can be used for emergency contraception, IUDs can be used as emergency contraception for up to 5 days post intercourse, and that OCPs are cheaper than IUDs over the course of 3 years.
The results of our study highlight the importance of education in eliminating perception barriers that are common in adolescent populations. The American college of Obstetricians and Gynecologists recommend physicians to encourage LARC methods for use by adolescents. 1n order to do this, they recommend counseling and education to occur at all health provider visits with sexually active adolescents [10,12]. While studies have shown that education is needed to help adolescents make decisions, the exact method has not been defined. In one study conducted, they concluded that giving empirical or anecdotal information about LARCs to adolescents does not work as efficiently as given straightforward information that address the advantages and potential disadvantages of LARC [13,14]. Our study conducted an intervention and workshop that gave straightforward information and from the results of the post-workshop data, we can see the effect of this method.
However, education is not the only barrier to LARC use. In order to reduce rates of pregnancy in adolescents, it is critical to identify and address all the various barriers. While education is the most effective method to increase compliance and overcome perceptions, we must address other concerns such as social stigma, financial, long-term effects, and weight gain [15,16].
We also studied the differences between demographics groups such as gender and students from private versus public universities. When comparing males and females, the perception of efficiency of various contraceptives saw no significant change in the rankings from before to after the workshop in males. However, in females, both the efficiency of OCP use and the efficiency of IUD use saw a significant change from the average ranking before the workshop to the average ranking after the workshop. In regards to perceptions about LARC use, women saw a significant change in their perceptions regarding the emergency use of Paraguard, the length of time for which IUDs can be used as emergency contraceptive, and regarding the associated side effects of IUDs. However, the male group only saw a change in their perceptions regarding the use of Paraguard for emergency contraceptive. The reasons behind this discrepancy could be because the educational intervention was more effective in women than men or perhaps because of the small sample size of men in our study. This demographic comparison should be done again with a larger number of males in the study.
Among private university students, the most significant perception change regarding contraceptive efficiency that was seen was about the efficiency of OCPs. On the other hand, in students who attended a public university, there were no significant changes in the perception of efficiency before and after the workshop for any of the contraceptives. Furthermore, in students who attended a private university had a significant change in the in regards to their perceptions of using Paraguard as an emergency contraceptive. Among public university students, the same perception that saw a change in response from before to after the workshop was about using Paraguard as emergency contraceptives. Public university students as also showed a significant change in their perception about the costs of 1UDs compared to OCPs. The potential reasons for the discrepancy between the two groups includes factors such as what education about LARCs and contraceptives that had already been given to students in public v. private universities or the difference in sample size between the two groups. To further studies on this topic such be done with a bigger sample size for each population as well as looking into education programs that students at different universities are exposed to.
There was one instance in which the percentage of participates who answered the statement correctly actually decreased. When asked to identify the validity of the statement "Mirena can be used for emergency contraception”, 65% of participants accurately identified it as a false statement before the workshop, while after the workshop this percentage went down to 64%. While this is not a significant change, we attribute this change to a slight change in sample size that was already small to begin with. Another area of discrepancy was in the demographic comparison in which the average ranked efficiency of withdrawal as a contraceptive actually saw a slight increase. While this slight increase was not found to be statistically significant, we hypothesize that this may change may be due to a smaller sample size as well.
The strengths of this study include a well-planned out workshop and strong survey questions. These questions very accurately reflect the misconceptions of LARCs that exist in the general population. However, if we were to repeat this study, we would try this intervention on a larger sample size to get an even more accurate representation. 1n future studies there would be a benefit to assess a more diverse population and studying the responses according to race and class. There have always been many barriers to access of contraceptives in general, but especially LARCs. By studying different populations for educational interventions, we may be able to illuminate one of the many barriers. It would also be of great use to identify barriers other than financial and educational such as, social or access to physicians who perform these procedures. By identifying barriers, we can further eliminate them.
Despite the overall increase in use of LARCs in the last couple of years, there continue to be a variety of barriers to LARCs. This study demonstrated how misconceptions regarding LARCs continue to prevent their use in young, well-educated populations and showed a modality for improving knowledge deficiencies that can be used.
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
https://juniperpublishers.business.site/
#juniperpublishers#Juniper Publishers PubMed Indexed Articles#gynecology#womens health#reproductive health#breast cancer#breastfeeding#open acess journals#Open acess Publishers
4 notes
·
View notes
Text
Recreational Shooting & Lead Exposure in Pregnant Women

Authored by Vedhapriya Srinivasan*
Abstract
Lead is a known environmental toxin affecting various organ systems. Elevated blood lead levels during pregnancy are associated with gestational hypertension, low birth weight, preterm births and spontaneous pregnancy loss. Lead crosses placenta passively and causes neurodevelopmental problems in the infants. Environmental policies of the United States government has reduced lead exposure from sources like gasoline, lead based paints and lead based industries like battery recycling but lesser known sources like gun ranges and lead bullets used for hunting may serve as potential source of lead exposure. Studies have consistently shown that workers at gun ranges, law enforcement officials who practice and more importantly recreational target shooters have elevated blood levels. Lead bullets used in hunting get fragmented and consumption of game meat can also cause elevated blood lead levels. In this short review we are focusing on gun ranges and game meat hunted with lead bullets as potential sources of lead exposure. Women in reproductive age exposed to lead at gun ranges or from eating game meat hunted with lead bullets may store lead in their bones and this bone stores can serve as an endogenous source of lead during pregnancy and lactation when bone turnover rates are high. With even minimally elevated blood lead levels associated with adverse effects on pregnancy and Neuro behavioral development of the prenatally exposed infants it becomes important for women and caregivers to be aware of this potential source of lead exposure.
Keywords: Gun ranges; Recreational shooting; Hunting; Low lead level; Pregnancy effects
Abbreviations: BLL: Blood Lead Level; CDC: Centers for Disease Control and Prevention; NIOSH: The National Institute for Occupational Safety and Health; ALSPAC: Avon Longitudinal Study of Parents and Children; OSHA: Occupational Safety and Health Administration
Introduction
Lead is a naturally occurring element found in all parts of environment -air, water and soil [1] and has known toxic effects on nervous, gastrointestinal, cardiovascular, hematopoietic and reproductive systems in humans [2]. Elevated blood lead level [BLL] in pregnant women is associated with higher incidence of hypertensive disorders, preterm birth, spontaneous pregnancy loss and low birth weight births [3-5]. Lead also crosses placenta and gets deposited in brain of the fetus to cause neuro developmental problems in the infant [6,7]. Environmental policies of the government along with public awareness, and blood lead level surveillance have reduced lead toxicity from traditional sources like lead based paints, plumbing, gasoline, canned foods and lead based industries [1]. Surprisingly activities such as recreational shooting at gun ranges and hunting with lead ammunition have been identified as sources of lead exposure and have now become the focus of investigation. In this article we will review literature regarding lead exposure at gun ranges and hunting, and its risks to pregnant mothers and their babies.
Background
In 2014 almost 31% of households reported having firearms in the United States, with 9 to 14% women owning firearms [8]. There are 16,000 to 18000 gun ranges with approximately one million law enforcement officers, military veterans and around 20 million active target shooters training in them [9,10]. There are also close to 13 million recreational hunters in the country [11]. With mandatory training hours for law enforcement officials and the gun range industries projected growth in business, more women may be at risk of exposure to lead as they take part in recreational target shooting. They may also be exposed to lead dust brought by their partners from gun ranges and from hunting activities using lead bullets.
Gun range exposure to lead
National Health and Nutrition Examination Survey [NHANES] survey shows the average blood lead level of adults in the United states is 1.2μg/dl [2009-2010], but 1% of women in reproductive age group has blood lead levels more than the CDC/NIOSH reference levels of >5μg/dl [12]. Though average national blood lead levels have dropped over the years due to stricter work place regulations, 95% of elevated blood levels (>25μg/dl) are still due to occupational exposure. Lead exerts its toxicity by forming reactive oxygen species and destroying membranes by lipid peroxidation. Elevated lead levels are associated with toxic effects on various organ systems in adults (Table 1).
Adapted from Kosnet et al, Gagan Flora et al, and ATSDR [13-15].
*Non-specific symptoms: [fatigue, anorexia, constipation, arthralgia, myalgia, headache, decreased libido, sleep disturbances].
Adult Blood Lead Epidemiology and Surveillance [ABLES] is a nationwide program in the United States, conducting adult lead exposure surveillance through mandatory reporting by laboratories and doctors of elevated blood lead levels in persons aged greater than 16 years [13-15]. In 2013 federal funding for state ABLES was discontinued and in August 2015 it resumed. As of December 2015, 28 states entered into collaboration with NIOSH to conduct adult blood levels surveillance program. In a study by Beaucham and colleagues analyzing the ABLES data during 2002-2012 for elevated lead levels according to the source of exposure, a total of 2,056 persons working in police protection and recreational industries like gun ranges had elevated blood levels of >10μg/dl, 1,271 had levels of 10-24μg/ dl and 785 of them had levels >25μg/dl. An additional 2,673 persons had elevated blood lead levels reported from non-work related target shooting of which 1,290 were reported with BLL >25μg/dl and 1,388 with BLLs of 10-24μg/dl [9].
International studies on exposure to lead from indoor gun ranges have consistently found higher BLL in shooting range workers as well as shooters. A cross sectional study done by Mathee et al. [16] at shooting ranges compared 87 shooters with 31 archers as control group and found that shooters had blood lead levels ranging from 2-60μg/dl with a mean of 12.8μg/ dl that was four fold higher than mean blood levels of 3.5μg/dl [Range -2 to 10.4μg/dl) found in archers. Among gun shooters 84.9% had blood lead levels > 5μg/dl and 45.2% had values ≥10μg/dl and 9% had values ≥25μg/dl. A study by Madrid G et al. [17] showed shooters with >12 practice sessions per year had significantly elevated mean lead levels (mean BLL 7.6μg/ dl, range 2.7-51.7μg/dl). Spontaneous pregnancy losses were reported in 24% of women whose partners had practices >12 times a year. This study brings to light possible links home lead from gun ranges on pregnant women. Also blood lead levels varied significantly by shooting site based on ventilation and lead cleaning methods. Shooters practicing at ranges, which were poorly ventilated, with dry vacuum cleaning for lead dust and no proper hand washing facilities had higher blood lead levels [17]. In another study done at indoor firing ranges by Park and colleagues [18], 27% professional shooters (mean BLL 14±8.3μg/dl), 56% of shooting range managers (13.8±11.1) and 60% of shooting range supervisors (6.4±3.4μg/dl) had elevated blood levels. This study also found that almost all sites in the firing range including beaten zones (area in trajectory of bullet) (100%), firing points (53%), waiting rooms (75%) had exceeded the permissible exposure limit (8 hour weighted average of 0.05 mg/mˆ3). In another study of 30 military personnel by Vivante and colleagues, the mean blood lead levels were 8.8±2μg/dL with 5 reported with levels >20μg/dL and 2 with levels >25μg/ dL [19]. Workers at the gun ranges and shooters can potentially carry home lead on clothing and skin and expose pregnant women and children to lead. There are multiple case reports of children with elevated blood level found on routine surveillance where the source was traced back to a relative working in a lead based industry [20,21]. In these investigations lead was detected on work clothes, their homes and even cars. Though none of these studies and findings were in pregnant women, the threat of exposure to lead from work place can be significant.
Hunting with lead shots as a source of exposure
There are currently more than 13 million hunters in the United States. The lead bullets used in hunting have been found to disseminate into the game meat resulting in lead exposure to people who consume it regularly [22-24]. These lead particles may be so small that it is impossible to remove them all as lead bullets fragment upon impact and gets dispersed in the meat that can only be detected by radiograph. The fragmentation increases the lead availability and cooking further increases the dissemination of lead particles [25]. In a case report involving accidental ingestion of air rifle pellet by a young child, elevated blood levels up to 56μg/dL were found [26]. In March 2008 North Dakota Department of Health, Agriculture, Game and Fish recalled donated venison because of lead contamination [27]. Similar contamination was found in Minnesota and since then Minnesota, North Dakota and the Wisconsin Health Departments have advised pregnant women and children <6 years to avoid eating meat hunted with lead bullets [28]. California became the first state to implement legislation requiring non-lead ammunition for hunting by July 2019 [29].
Effects of low level lead on pregnancy
Lead is a known neurotoxin, which has been associated with adverse effects in pregnancy like gestational hypertension, low birth weight, spontaneous pregnancy loss and neuro developmental problems in infants even at lower levels. Due to public health awareness and environmental regulations lead levels have reduced in the United States, and in 2015, NIOSH and CDC labeled blood levels >5μg/dL as elevated levels in pregnant women. Lead is absorbed through ingestion and inhalation, redistributes to soft tissues and bone. A proportion of the absorbed lead is excreted by kidney, with small amount excreted by feces, sweat, and hair and nails [30]. Divalent metal ion transporter (DMT-1) is a protein on apical membrane of cells in the gastrointestinal tract serving as a transporter for iron and also metals like lead, manganese and cadmium. Iron deficiency up-regulates the DMT-1 receptors in the duodenum thereby increasing lead absorption [31]. Studies have also shown that increase in lead levels decrease iron and ferritin levels and iron supplementation in cases of deficiency lowers blood lead levels [19]. Lead crosses placenta [6,7] and levels in umbilical cord and maternal RBC show significant correlation and act as an in utero source of lead exposure to the fetus [32]. Lead is transferred passively in ratio of 0.7:0.9 (fetal: maternal) [5] which then in the fetus crosses the immature blood brain barrier and gets deposited leading to neuro toxicity and intellectual disabilities. Iron deficiency in pregnancy amplifies the negative association between prenatal lead exposure even at low doses of lesser than 5μg/dl (mean of 1.27μg/dL) and cognitive development in children [33]. Low dose iron supplementation may protect the integrity of blood-brain barrier against disruption by lead and reduce lead deposition in brain of fetus as observed in animal studies [34]. Even though only 1% women in reproductive age group are reported to have lead levels of >5 μg/dL, blood levels may not be the only marker of lead toxicity as 90 to 95% of lead accumulates in skeletal bone in adults [35]. Half-life of lead in blood is around 30 days, soft tissues is around 45 days and is 2030 years in bone [36] and this bone stores of lead accumulated during reproductive years in a women, serve as an endogenous source during pregnancy and lactation when bone turnover rates are high [37,38]. Maintaining adequate levels of calcium through diet and supplementation prevents excessive turnover of bone during pregnancy and lactation [39] and serve as a preventive strategy to reduce increased blood lead exposure to fetus and infant [40]. Because of the general decline in the blood lead levels recent studies have focused on adverse effects in pregnancy associated with lower lead levels of 1-5μg/dl and 5-9μg/dl. In a large prospective ALSPAC study in UK by Taylor et al found that preterm births were increased twice and head circumference and crown heel length reduced as lead levels increased above 5μg/dL [5]. In another study by Perkins and colleagues [41] even low blood levels were associated with trend of preterm birth in male infants but no other effects were observed. The National Toxicology Program of the Department of Health and Human Services released a review of health effects of low level lead and found sufficient evidence of neuro developmental effects in infants exposed prenatally to lead like and also low birth weight births in mother with mild elevations in blood lead levels.Because of the detrimental effects of lead at very low levels to the nervous system of fetus and on infants no safe levels have been established [42] (Table 2).
Adapted from *National Toxicology Program-Monograph on health effects of low level lead 2012 [42].
Conclusion
Lead is an environmental toxin associated with adverse effects on pregnancy and long-term neurological and intellectual disabilities in the fetus exposed during prenatal period. Bone lead with its long half-life serves as an endogenous source of lead during pregnancy and lactation even after exposure has been terminated which makes primary prevention of exposure to lead important in women. Women in reproductive age group should be educated about the toxic effects of lead and made aware that lead dust from target practice ranges and lead ammunition used for hunting could be a significant source of chronic lead exposure for themselves and their family. They should also be equipped with knowledge of best practices to avoid lead exposure from recreational shooting and hunting.
Recommendations
In 2002 department of health services in Alaska issued a bulletin stating that a school rifle team practicing at an indoor gun range without adequate lead control measures tested for elevated blood lead-levels and the levels reduced after the gun range maintenance was updated with lead protective measures [43] . In an investigate report of OSHA inspections it was found that from 2004 to 2013, 201 gun ranges were inspected and 1900 lead related violations of safety measures at gun ranges [44] . The NIOSH recommends series of measures to reduce work place exposure to lead at gun ranges like regular maintenance of the gun range, using wet moping technique and High Efficiency Particulate Air [HEPA] vacuums to clean the floors and surfaces, use of good ventilation with either closed system and HEPA filters or direct exhaust systems, proper education of workers, providing protective gears and medical surveillance [45]. Considering the magnitude of the problem we recommend the following measures to limit lead exposure due to target practice and lead bullets used in hunting.
Recreational shooting practice should be performed in gun ranges that have been inspected and found compliant to the lead safety standards put forth by OSHA and NIOSH in the United States and by corresponding agencies worldwide.
Recreational shooters should be educated about the potential exposure to lead and the ways they can reduce the take home exposure such as eating or drinking in the gun ranges, using lead cleaning wipes and maintaining separate clothes and shoes for the gun ranges which should be taken in a plastic bag and washed separately
Non-lead bullets can be considered at target practices and copper bullets as hunting ammunition, which doesn't fragment on impact and is nontoxic [46].
Though ACOG / CDC doesn't recommend routine blood lead level estimation it advises to screen high risk groups and so pregnant mothers should be asked about hobbies like recreational shooting and hunting among family members.
CDC recommends follow up in pregnant women with blood lead levels >5 μg/dl, to identify and eliminate the source.
Iron supplements should be used in cases of deficiency to reduce the toxic effects of lead in fetus.
Calcium intake of 2000 mg per day should be maintained through diet and supplementation to reduce bone turn over during pregnancy and lactation thereby reducing lead release from bone stores [47].
Pregnant women with lead levels >5μg/dl should be followed up every 2-3 months during the ante-natal period and at delivery cord blood levels should be collected to establish neonatal surveillance.
Chelation is not recommended with levels <45μg/dl and breast-feeding should only be discontinued with levels >40μg/dl.
It is advisable for pregnant women to avoid eating meat hunted using lead ammunition.
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
#Juniper Publishers PubMed Indexed Journals#JuniperPublishers#Juniper Publishers PubMed Indexed Articles#juniperpublishersgroup#Gynecologycal Surgeries#women's health
0 notes
Text
Early and Late Onset Preeclamsia: What did really Matter?

Authored by Sri Sulistyowati*
Summary
Preeclampsia is main cause of morbidity and mortality both mother and fetus. Preeclampsia occurs in 2- 10% of pregnancy and that was no changed during the last century. Endothelial dysfunction was believed as cause of preeclampsia incidence until now their mechanism is unknown. Preeclampsia was divided in two kind of preeclampsia, early onset preeclampsia is occur at less <34 weeks of gestation age and late onset preeclampsia is occur at >34 weeks of gestation age. Early and late onset preeclampsia have different etiologic and should be considered as different diseases then there are difference in the term of marker, clinical manifestation, maternal and perinatal outcome, prognosis, and complication. Early onset preeclampsia has a much worse maternal and fetal outcome than late onset preeclampsia
Text
Preeclampsia is a pregnancy associated with hypertensive disease that occurs after 20 weeks' gestation. Preeclampsia is still a major contributor to maternal and fetal morbidity and mortality [1]. The incidence of preeclampsia is 2 to 10% of all pregnancies in the world. According to WHO the incidence is 7 times greater in developing countries compared to developed countries [2]. Preeclampsia cases in Indonesia causing 3040% of maternal death and 30-50% of perinatal death. In Dr. Moewardi General Hospital Surakarta Indonesia maternal mortality which were caused by preeclampsia were 19 ot of 30 maternal mortality cases and increasing to 12 out of 21 in 2013 [3] . Preeclampsia is distinguished into two: early onset where preeclampsia occurs at <34 weeks' gestational age and late onset occurring at >34 weeks of gestation. The early-onset concept of preeclampsia and late-onset of preeclampsia is more modern, and it is widely accepted that these two entities have different etiologies and should be regarded as different forms of disease [4]
The difference between early and late onset preeclampsia
Early onset and late onset preeclampia have different implications for fetuses and neonates, with perinatal mortality rising about 10-fold higher on early onset, and doubling in late-onset. Early onset preeclampsia is a severe pregnancy complication characterized by elevated blood pressure, metabolic and inflammatory changes leading to generalized endothelial dysfunction and end-organ damage due to vascular disorders. Early onset preeclampsia is a potentially life-threatening disease for both mother and baby [5]. Early onset preeclampsia is the most severe clinical variant of disease occurring 5-20% of all cases of preeclampsia and is associated with impaired fetal growth, fetal pathology and uterine blood circulation, small size of the placenta, preterm delivery, neonatal morbidity and mortality. Early onset preeclampsia developments are associated with impaired trophoblast invasion, complete transformation of the uterine spiral artery, immune maladaptation and increased markers of endothelial dysfunction. Preeclampsia late onset is about 75-80% of all cases of preeclampsia; Which are associated with maternal morbidity (metabolic syndrome, impaired glucose tolerance, obesity, dyslipidemia, chronic hypertension), normal birth weight and normal placental volume [6].
Risk Factors
There are differences in risk factors between early-onset and late-onset preeclampsia, a history of chronic hypertension and family history of hypertension. The history of chronic hypertension was significantly associated with an increased risk of early onset onset of preeclampsia, whereas a history of chronic family hypertension was significantly associated with an increased risk of late-onset preeclampsia alone [7]. Early onset preeclampsia predictors are African race, chronic hypertension, previous preeclampsia history and ovulation drug use. Predictors of late-onset preeclampsia and gestational hypertension increase with maternal age and BMI, and family history or preeclampsia history. The rate of early detection of preeclampsia, late-onset preeclampsia and gestational hypertension in screening with maternal factors was only 37.0; 28.9 and 20.7%, respectively, to a false positive rate of 5%. History of preeclampsia or eclampsia in previous pregnancies, passive smoking exposure, inadequate antenatal supervision, family hypertension history in one or more first-degree families, living in a shared family, overweight and lower socioeconomic status were associated with increased risk early onset of preeclampsia and eclampsia [8]. Obesity and obesity increase the risk of preeclampsia, which is explained by elevated levels of fatty acid triglycerides and free fatty acids. These lipid changes may produce a major factor causing endothelial cell dysfunction in preeclampsia with increased circulating levels of lipid peroxide oxidative stress. This can cause endothelial cell damage [9]. Maternal weight B0.2kg per week is a significant protective factor for the onset of preeclampsia. Pre pregnancy BMI <20kg/m2 is a significant protective factor for late onset preeclampsia. The history of chronic hypertension is a significant risk factor for early onset preeclampsia. A family history of chronic hypertension is a significant risk factor for late onset preeclampsia. Chronic hypertension can lead to endorgan damage and complications of blood vessels. This may be the reason why chronic hypertension is associated with early- onset preeclampsia; A family history of chronic hypertension is associated with late onset preeclampsia. This may be explained by genetic predisposition [7].
Markers
Markers for predicting preeclampsia includes: Angiogenic Factors such as Vascular Endothelial Growth Factor (VEGF), Placental Growth Factor (PlGF), Fms-like Tyrosine Kinase (flt) -1 and Soluble Endoglin [10]; P-Selectin [11]; Cells Free fetal DNA [12]; ADAM12 (Disintegrin and Metalloprotease 12) [13];Placental protein 13 [14; Pentraxin 3 [15]; Pregnancy- Associated Plasma Protein A [16]; and Doppler Sonography of Uterine Artery [17].
Maternal and Perinatal Outcome
The ratio of maternal and perinatal mortality of near missed cases are 0.96% and 29.06%. The ratio of cases in which maternal life at risk (maternal and maternal mortality near missed) is 30%. Premature birth, intrauterine death between 20-28 weeks, intrauterine death between 28-37 weeks, first trimester abortion aresignificantly higher in women with early onset preeclampsia compared to late onset. The incidence of disease histories other than chronic hypertension (especially diabetes mellitus), the history of preterm delivery is significantly higher in women with late-onset preeclampsia. The mean gestational age at delivery and birth weight are significantly lower in early-onset preeclampsia. The incidence of stillbirth, early neonatalmortality and late neonatal mortality, cases in which maternal life at risk are significantly higher in women with early onset preeclampsia [9].
Prognosis
Stillbirth, early and late neonatal mortality, cases in which maternal life at risk were significantly higher in early-onset preeclampsia. Women with early onset preeclampsia have higher maternal mortality rates than late onset [9] Early onset preeclampsia also needs longer duration of treatment. Babies born from early-onset preeclampsia mothers particularly are troublesome. Infants commonly suffer asphyxia and lower birth weight, and those are rarely happened in late-onset preeclampsia. This implicates in lower survival rate of baby born from early onset preeclampsia. So it can be concluded that perinatal mortality and morbidity in early onset are way worse [18].
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
#Juniper Publishers PubMed Indexed Journals#JuniperPublishers#open acess journal#openacess publishers#gynecology#women's health
0 notes
Text
Silibinin in Human Breast Cancer: Scope Beyond Placebo!

Authored by Sulbha Mittal*
Abstract
Chemotherapies for breast cancer generally have strong cytotoxicity and severe side effects. Thus, significant emphasis has been placed on combinations of naturally occurring chemopreventive agents. Silibinin is a major bioactive flavonolignan extracted from milk thistle with known chemopreventive activity in various organs. However, the mechanism underlying the inhibitory action of Silibinin in breast cancer has not been completely elucidated. Several investigations have been and are being conducted, to study the effect of Silibinin in human breast cancer cells and protective effect in normal cells. The aim of the present article is to review and summarize the physical properties, mechanism of action, pharmacokinetics, role and potential of Silibinin in breast cancer.
Keywords: Breast cancer; Chemotherapy; Chemoprotection; Phytotherapeutics; Silibinin
Introduction
Breast cancer is the second leading cause of cancer death among women and also is the most common malignancy in women, worldwide, accounting for 1.2 million new cases annually. Breast cancer alone is expected to account for 29% all new cancer diagnoses in women [1]. Individualized, multimodality treatment including surgery, radiation, chemotherapy, with/without immunotherapeutic agent and hormone therapy is presently being used for the treatment of breast cancer. Although many anti-cancer therapies are clinically applicable, they generally have strong cytotoxicity and severe side effects [2]. In an effort to increase the therapeutic efficacy and minimize the systemic toxicity of chemotherapeutic agents, dietary supplements and is given to humans and rodents at doses as high as 1% (w/w) or 2g/kg body weight [7,8]. Many studies have shown that Silibinin blocks experimentally induced malignancies of the prostate, skin, and colon [8-10]. Human trials of Silibinin are underway for treating prostate cancer, and a completed phase I study has shown no toxic effects [11]. Silibinin plays an important role in breast cancer cells [2-12]. However, the molecular mechanisms associated with the chemopreventive effects of Silibinin have not been clearly and systemically elucidated for breast cancer In the present article we have tried to summarize the possible mechanisms of action of Silibinin on human breast cancer cells from the literature available so far
Physical and Chemical Properties of Silibinin
Silibinin (Chemical formula: C25H22O10), (Figure 1) has molecular mass of 482.44g/mol. It has stability of over 2 years at -20 °C. Silibinin has poor water solubility but is readily soluble in organic solvents like ethanol [13-20].
Pharmacokinetic Properties
Silymarin, the active substance in milk thistle, is a mixture of flavonolignans including isomerssilybins A and B, isosilybin A and B, silychristin (also known as silichristin), silydianin (also known as silidianin), and their flavonoid precursor, taxifolin. In the literature, the mixture of the silybins A and B is often referred to as Silibinin. Silibinin is prepared as glycosides of Silybin, which shows more water solubility [21]. Silymarin has very poor bioavailability due to the poor water solubility (<0.04mg/ ml) of its flavonolignan structure [22]. The poor bioavailability considerably limits the clinical applications and therapeutic efficiency of oral Silibinin administration [23]. Newer formulations like Silipide and phosphatidylcholine (Lecithin) have ten times more bioavailability compared to Silymarin [24]. Silymarin inclusion complex with p-cyclodextrin is much more soluble than Silymarin [25].
Metabolism and Excretion
Silymarin undergoes Phase I and Phase II metabolism. Phase II metabolism is by conjugation reactions. Excretion is through bile and urine. Silymarin is known to inhibit P-gp-mediated cellular efflux. The modulation of P-gp activity may lead to altered absorption and bioavailability of drugs. Silymarin is known to inhibits cytochrome (CYPs) enzymes [26,27].
Toxicity
Milk thistle is being used for thousands of years and is generally well tolerated by humans. In rare instances, acceptable and mild side effects may be noted with Silibinin ingestion, which include headache and fleeting gastrointestinal distress [26]. Other possible side effects include- allergic skin reactions, itching, bloating, blood clots, loss of appetite, nausea, constipation or diarrhoea, thrombocytopenia, elevated liver enzymes and bilirubin, fever, giddiness, heartburn, hives, impotence, increased creatinine, insomnia, irritability, joint pain, non-specific muscle and joint pains, taste changes, tremor, and weakness.
The more serious concerns about safety stem from possible drug interactions. P450 substrate agents may interact negatively with Silybummarianum supplementation [27].
Since, milk thistle extracts are known to suppress PPAR, (peroxisome proliferator-activated reactor gamma) individuals suffering from diabetes must seek endocrinologist opinion before taking milk thistle or Silymarin. Milk thistle extract supplements are also known galactogogues. Galactogogues stimulates lactation (milk production). Silibinin or milk thistle supplementation may not be appropriate for pregnant or nursing women. It's also not advisable to take Silibinin or Silymarin with medications used to treat autoimmune diseases or conditions.
Mechanism of Action of Silibinin in Breast Cancer
Several publications have suggested the presence of Silibinin activity in breast cancer cell lines. The combination of Silibinin and cytostatic drugs was analyzed by Tyagi et al. [28] Combination of Silibinin and Carboplatin showed strong apoptotic effects in Michigan Cancer Foundation-7 (MCF-7) cells. However, this effect was not observed when Cisplatin was used. The combination of Silibinin and Doxorubicin resulted in higher rates of apoptotic death compared to each agent alone in the MCF-7 and MDA-MB468 cell lines [28].
Kim et al. [29] while studying the effect of Silibinin on triple negative breast cancer (TNBC) cell motility, found that it suppresses TGF-P2 expression and compared the effects with those in non-TNBC cells. The study suggested that Silibinin suppresses metastatic potential of TNBC cells. In-vitro studies conducted by Wang et al. [30] concluded that Silibinin promotes the sustained superoxide production that was specifically scavenged by exogenous superoxide dismutase (SOD) in MCF-7 cells, while the activity of endogenous SOD was not changed by Silibinin. Study by Tiwari P et al. [31] suggested that Silibinin- induced apoptosis in breast cancer cells (MCF-7 and T47D) is p53-independent and caspase-dependent, mediated by both extrinsic and intrinsic pathways of apoptosis. The action involves both casapase-8 activation and mitochondrial changes and includes loss of mitochondrial membrane potential and Bax/Bcl- 2 redistribution. In another experiment they found that Silibinin- mediated cytotoxic effects were dose and time-dependent in both cell lines and T47D cells were more sensitive than MCF-7 [32]. Kim et al. [29] observed that Silibinin suppressed the epidermal growth factor receptor (EGFR) signaling pathway in SKBR-3 and BT-474 breast cancer cells and may be used as an effective drug for the inhibition of metastasis of human breast cancer [33].
Noh et al. [34] also observed that Silibinin, in pretreated MCF-7 human breast cancer cells, enhances UV B-induced apoptosis. Nejati-Koshki et al. [35] found, the cytotoxic effects of Silibinin on T47D to be dependent on inhibition of estrogen receptor β-expression levels and expression of leptin hormone. The anti-proliferative effect of Silibinin on SKBR3, an ErbB2- overexpressed and ER-negative human breast carcinoma cell line is regulated by the high inhibitory effect on NF-kB [35]. Lu et al. [36] observed that Silibinin inhibited Wnt/p-catenin signaling by suppressing Wnt co-receptor LRP6 expression in human breast cancer cells (MDA-MB-231 and T-47D). Dastpeyman et al. [37] while studying the effect of Silibinin on migration and adhesion capacity of MDA-MB-231 cells (a highly metastatic human breast cancer cell line), showed significant dose-dependent inhibitory effect of Silibinin on proliferation, migration and adhesion of these MDA-MB-231 cells to distant organs. Ohj et al. [38] suggested that Silibinin suppresses 12-O-tetradecanoyl- phorbol-13-acetate (TPA) induced cell migration and matrix metallopeptidase-9 (MMP-9) expression through the MEK/ ERK-dependent pathway in MCF-7 breast cancer cells. Xu et al. [39] used Silibinin-loaded lipid nano-particles (SLNs) and found that those were quiet effective in inhibiting the growth of MDA-MB-231 cells. SLNs exhibited stronger inhibitory effects compared to free Silibinin, on invasion and migration of MDA-MB-231 cells. In an experimental work by Kim et al, Silibinin induced apoptosis in MCF-7 and MDA-MB-231 was found to be dependent on generation of reactive oxygen species (ROS). Silibinin induces cell death through an AIF-dependent mechanism in MCF7 cells and caspase-3 dependent mechanism in MDA-MB231 cells. This results in ROS generation and Notch-1 signaling act upstream of the ERK and Akt pathway [40,41]. Silibinin and Curcumin combination inhibited the growth of T47D human breast cancer cells in a study. The combination was also found to inhibit telomerase expression in T47D cells [42,43]. It was confirmed by Pirouzpanah et al. [44] that Silibinin induced apoptosis mediated by increase in p53, p21, Bak, ATM in mRNA levels. This study announced that Silibinin inhibited proliferation, induced apoptosis and caused cell cycle arrest at G0/G1 phase in human breast cancer (MCF-7) cells. In fact this was the molecular event which was associated with the up- regulation of Bak, p53, p21 and down-regulation of Bcl-xl.
Zheng et al. [45] elaborated the mechanism of Silibinin induced apoptosis. They found that it involved both the extrinsic and intrinsic pathways (ERɑ-MEK/ ERK and ERɑ-Akt/mTOR pathways). In another study, by using an Erβ-selective agonist, they demonstrated that ERp served as a growth suppressor in MCF-7 cells, and the incubation of Silibinin elevated ERβ expression, resulting in tumor growth inhibition. Unlike ERɑ, ERβ did not involve autophagic process in this regulation [45,46]. Khannazer et al. [47] reported that Silibinin treatment in MDA-MB-231 cells increased the expression of chemokine receptors like CXCR3, CCR5 and CCR7. Silibinin has also been found to induce autophagic cell death through ROS-dependent mitochondrial dysfunction and ATP depletion in MCF7 cells [48]. Gao et al. [49] studied the effects of Silibinin on IFNƔ-induced FAT10 expression and chromosome instability in HCT116 and HepG2 cells. These cells were treated with Silibinin before karyotyping was performed. It was observed that Silibinin with FAT10 can modulate IFN-Ɣ-induced chromosome instability, apoptosis sensitivity and suppression of TNF-ɑ-induced tumor growth.
Efficacy and Results
Though the clinical studies for usefulness of Silibinin are in infancy, the extrapolation of outcomes in studies in various malignant conditions so far, leave us quite optimistic. Silymarin whole extract has been also used in clinical trials for the treatment of hepatotoxicity in childhood acute lymphoblastic leukemia (ALL). Silymarin (at target dose of 5.1mg/kg/day) was administered orally for 28 days and it significantally reduced liver toxicity in children with ALL [50]. Recently, a new Silibinin drug formulation, Legasil® administration improved hepatic failure due to extensive liver infiltration in a breast cancer patient [51].
A Phase II trial of the Silibinin containing cream, Difinsa-53 has also been proposed (ClinicalTrials.gov Identifier: NCT02534129) to determine efficacy in delaying, ameliorating, or preventing the radiation dermatitis in patients with breast cancer, undergoing whole breast irradiation. Many other trials are also going on and are likely to guide us further
Conclusion
Silibinin, a flavonolignan, the major active component of the milk thistle plant (Silybummarianum) has been used as medicinal herbs in the treatment of hepatic disorders. Silibinin has shown promising anti-neoplastic effects against skin, breast, lung, pancreatic, colon, cervical, prostate, bladder, and kidney cancer cells. It is safe and the adverse effects observed in the reviewed studies appear to be minimal. However, targeted randomized clinical trials on Silibinin are necessary to establish its safety, efficancy and synergistic effect with various chemotherapeutic drugs in human breast cancer cells. From our review of the literature into the mechanisms of Silibinin-induced apoptosis in MCF-7 and T47 D cells, many findings have contributed significantly to understanding the molecular mechanism of Silibinin-induced apoptosis in-vitro. It is hoped that a large clinical study would address the usefulness of Silibinin in breast cancer therapy.
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
https://juniperpublishers.business.site/
#Juniper Publishers PubMed Indexed Journals#gynecology#womens health#sex#breast#reproductive health#Reproductive organs#menopause#Juniper Publishers PubMed Indexed Articles#urogynecology
0 notes
Text
Early Detection of Type II Ovarian Cancer with Labelled Microbubble Transvaginal Sonography
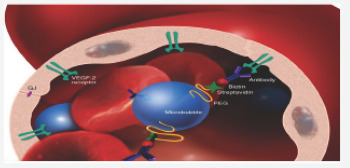
Authored by Arthur Fleischer*
Abstract
Ovarian cancer is the most lethal of all gynecological malignancies. However early detection can potentially improve the survival rate from 50 to 90%. Transvaginal sonography with the use of contrast-enhanced microbubbles has shown promise when used to detect malignant ovarian lesions in several studies [1-3]. This brief communication addresses the need and potential benefits of contrast enhanced transvaginal sonography, as well as directions for future research and clinical applications.
Introduction
Ovarian cancer is the seventh most common cancer in women and the most lethal of all gynecological malignancies in the United States. Each year, more than 22,000 patients are diagnosed with ovarian cancer and 14,000 cancer related deaths are reported [4]. Often presenting with subtle and nonspecific symptoms, ovarian cancer is first diagnosed at advanced stages leading to poorer prognoses. However, early detection can significantly increase the survival rate from 50 to 90%. Earlier diagnosis and cancer confinement to the ovary can lead to much more favorable outcomes for patients [3]. One method to facilitate early detection is through screening, but currently available tools, such as biomarkers and imaging, lack sensitivity and specificity for certain ovarian tumors in early and more treatable stages.
Ovarian cancer is classified into type I and II [5]. Type I carcinomas, most common in Asia, are slow growing, indolent neoplasms that typically arise from a precursor lesion. These include endometrioid carcinoma, clear cell carcinoma, mucinous carcinoma, and low-grade serous carcinoma. Type II carcinomas, most common in the USA and Europe, are clinically aggressive neoplasms that develop from ovarian surface epithelium and/ or de novo from serous tubal intraepithelial carcinomas (STIC). These include high-grade serous carcinomas and are associated with genetic instability, TP53 gene mutations, BRCA 1 and 2 mutations, and high Ki67 proliferation index. Thus theoretically based on growth patterns, annual screening with transvaginal sonography and CA125 alone would be more effective in Asia (predominantly type I cancers) than in the USA and Europe (predominantly type II cancers) [5]. Although there has been successful detection of these lesions in animal studies, early detection of type II ovarian cancer remains a challenge [3,5].
Transvaginal microbubble sonography
Sonography is a non-invasive imaging technique that allows for the real-time evaluation of the region of interest, including functional information on tissue vascularity, and is currently the preferred first-line method of imaging suspicious breast and ovarian lesions. Sonography is widely available, inexpensive, and portable. However, transvaginal sonography lacks sensitivity and specificity for the detection of tumors in early stages. Targeted sonography is the application of targeted contrast agents during ultrasound procedures to image specific biomarkers with many clinical applications including diagnostic imaging, gene and drug therapy delivery, blood flow mapping, selective endothelial receptor imaging, and more. Microbubbles are tiny bubbles used as contrast agents in ultrasound diagnostic procedures. Typically, microbubbles are filled with per fluorocarbon gas inside an outer lipoprotein shell. They are useful because of their small size, 1-7 micron-diameter, and their circulating movements in vasculature, very similar to that of erythrocytes, allowing their utilization to detect neoplastic growth. Microbubbles, injected intravenously, remain purely intravascular in comparison with contrast agents used for MRI and CT exams. They remain in vasculature until the lipoprotein shells are metabolized by the liver and the encapsulated gas is eliminated via the lungs 5-7 minutes after injection. Imaging techniques using microbubble contrast provide quantitative information about blood passage through the capillaries within tissues. Signals acquired from microbubbles can be used to estimate blood flow and quantify abnormal changes which may result from occluded vessels in body tissues and abnormal vasculature as in neoplastic growths. Targeted microbubbles have ligands that attach to endothelial cell surface receptors up regulated in cancer, such as vasogenic epithelial growth factor/VEGF (Figure 1). Transvaginal targeted microbubble sonography provides better characterization, improved detection, and monitoring of cancer in preliminary studies [5]. Contrast enhanced microbubble transvaginal sonography have shown improved accuracy for detection when compared to 2D and 3D Doppler Transvaginal Sonography [6-8].
Success thus far
To date, microbubbles have not been associated with any untoward effects after preliminary studies in millions of patients across the world. In fact, in 2016, the FDA approved the use of Lumason, a microbubble contrast, for improved liver lesion characterization. Microbubbles are also being used in pediatric patients who receive blunt trauma with imaging of the kidneys, spleen, liver and pancreas. Initial studies have demonstrated significant differences in vascular enhancements of benign versus malignant masses [1-3]. Although contrast-enhanced transvaginal sonography cannot distinguish between borderline and malignant masses, both require surgical intervention [3]. In addition, compared to no screening, transvaginal sonography has been associated with an overall 20% mortality reduction in a large prospective study involving over 250,000 women [8].
Potential Applications
Ovarian cancer screening efficacy depends on the cancer subtype [4]. Transvaginal sonography with the use of contrast- enhanced microbubbles can be further studied using different biomarkers, more specifically for type II ovarian cancers. It has also shown promise in preliminary studies and could ultimately become part of ovarian cancer screening secondary to initial assessments. Recent FDA approval will likely lead to further clinical use of microbubbles as contrast agents for various sonography studies. Theranostic applications, which combine a biomarker target and enhanced drug delivery, may be possible in the near future [6].
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
https://juniperpublishers.business.site/
#gynecology#Ovarian Cancer#Transvaginal Sonography#gynecological malignancies#neoplastic growth#blunt trauma
0 notes
Text
Biosensors, the Emerging Tools in the Identification and Detection of Cancer Markers

Authored by Muhammad Torequl Islam*
Abstract
The cancer is chaos, causing impairment by biochemical pathways in a biological system. Mulfunctioning of cells throughout the human body is mostly observed in cancer and is still the outmost lethal disease in the world. There is a difference in expression of parameters within a host during its normal physiology and pathological conditions, those are identified and detected to proceed on for the treatment. A number of conventional methods are available nowadays, despite of their potential limitations. Biosensors, the analytical devices that convert biological responses into electrical signals are now popularly used in many fields such as food industry, metabolic engineering, plant biology, marine science, defense, drug discovery and development. Beside these, in the medical sectors, their important roles are remarkable, especially in the early detection of a disease, and monitoring the therapeutic progression and disease state. To date, diagnostic tests by using biosensors for the early detection of cancer biomarkers are available; these provide noninvasive/minimally invasive assays with high through output and patient survival rate. This paper reviews an overview on biosensor-implementation in some cancers along with their future applicability.
Keywords: Biomarker; Biosensor; Cancer; Diagnosis
Abbreviations: 18F-FDG: 18F-Fluorodeoxyglucose; AFP: Alpha-Fetoprotein; AKT: Protein Kinase B; AMARC: Methylacyl Alpha CoA Racemase; AuNPs: Gold Nanoparticles; B2M: Beta-2-Microglobulin; BRAF: B-Raf; BRCA: Breast Cancer Associated Gene; CA: Cancer Antigen; CAPB: Cocamidopropyl Betaine; CD: Cytotoxic T Cell; CEA: Carcinoembryonic Antigen; CGH: Comparative Genomic Hybridization; CK: Creatine Kinase; CRP: C-Reactive Protein; CTC: Cutaneous T Cell; CYFRA: Cytokeratin Fragment; DD3: Discoidin Domain 3; DDR2: Discoidin Domain Receptor 2; DCIS: Ductal Carcinoma In Situ; DEPDC1: N,N-Diethyl-1,4-Phenylene Domain Containing 1; Dsdna: Double-Stranded DNA; EGFR: Epidermal Growth Factor Receptor; ELAC2: Elac Ribonuclease Z 2; ELF: Epithelial Lining Fluid; ELISA: Enzyme-Linked Immunosorbent Assay; EPCA: Early Prostate Carcinoma Antigen; Epcam: Epithelial Cell Adhesion Molecule; ER: Estrogen Receptor; EXO1: Exonuclease 1; FISH: Fluorescence In Situ Hybridization; FOXM1: Forkhead Box Protein M1; HAPLN1: Hyaluronan And Proteoglycan Link Protein 1; HE4: Human Epididymis Secretory Protein 4; HER2: Human Estrogen Receptor 2; HfO2: Hafnium Oxide; HPC: Haematopoietic Progenitor Cell; HPC1: Haematopoietic Progenitor Cell 1; HPCX: Haematopoietic Progenitor Cell X; HPV: Human Papillomavirus; IHC: Immunohistochemistry; IL: Interleukin; IUPAC: International Union of Pure and Applied Chemistry; KEAP1: Kelch-Like ECH-Associated Protein 1; KRAS: K-Ras; LDCT: Low-Dose Computed Tomography; M-CSF: Macrophage Colony-Stimulating Factor; Mirna: Micro Ribonucleic Acid; MRI: Magnetic Resonance Imaging; MUC1: Mucin 1; NCI: National Cancer Institute; NFE2L2: Nuclear Factor, Erythroid 2 Like 2; NUSAP1: Nucleolar And Spindle Associated Protein 1; P53: Protein 53; PCAP: Pulmonary Capillary Pressure; PET: Positron Emission Tomography; PIK3CA: Phosphoinositide 3-Kinase Catalytic Subunit Alpha; PNA: Peptide Nucleic Acid; PR2: Progesterone Receptor 2; PSA: Prostate-Specific Antigen; PTEN: Phosphatase and Tensin Homolog; QCM: Quartz Crystal Microbalance; QDs: Quantum Dots; Qpcr: Quantitative Polymerase Chain Reaction; RT-PCR: Real-Time Polymerase Chain Reaction; Real-Time qrt-PCR: Real-Time Quantitative Reverse Transcription PCR; RRM2: RNA Recognition Motif 2; SPP1: Secreted Phosphoprotein 1; SPR: Surface Plasmon Resonance; Ssdna: Single-Stranded DNA; TATI: Tumour-Associated Trypsin Inhibitor; TNF: Tumor Necrosis Factor; TPA: Tissue Plasminogen Activator; TPS: Thermoplastic System
Introduction
Evidences suggest that an increasing number of attentions have been focused on developing rapid techniques called 'biosensor technology' for the identification, detection and monitoring of human health-related conditions. The biosensors are the bioanalytical devices, incorporating molecular recognition together with physicochemical transducers, for the analysis of biomarkers. The term "biosensor” was first used by Cammann [1] and its definition was introduced by the International Union of Pure and Applied Chemistry (IUPAC) [2]; finally started the journey in the 1960s by the pioneers Clark and Lyons. A biosensor connects chemistry, biology, and engineering in its fabrication. Based on the mechanism, the materials used in biosensors are: biocatalytic group comprising enzymes, bio affinity group, including antibodies, antigens and nucleic acids, and microbe-based containing microorganisms. Till date, different types of biosensors are: enzyme-based; microbe-based or cell-based; tissue-based; immunosensors; protein, DNA or genetically-encoded biosensors; electrochemical, magnetic, optical, thermal and piezoelectric biosensors. Each biosensor has a conformation and uniqueness in its fabrication and application. A common illustration of the function of biosensor has been shown in Figure 1.
The applications of biosensors are growing day by day. Till date, they can be found in- food and fermentation industry, plant biology, in defense, marine science, drug discovery and medical sciences.
In the diagnostic centers, glucose biosensors are widely used for the detection of blood-glucose levels [3]. Biosensor, based on hafnium oxide (HfO2), is used for the detection of human interleukin (1L)-10 [4] in cardiovascular patients. Biosensors are also engaged in the diagnosis of infectious diseases and anti-microbial susceptibility. Other important applications of biosensors include: quantitative measurement of cardiac markers in undiluted serum, microfluidic impedance assay for controlling endothelin-induced cardiac hypertrophy, immunosensor array for clinical immunophenotyping of acute leukemias, effect of oxazaborolidines on immobilized fructosyltransferase in dental diseases; histone deacylase (HDAC) inhibitor assay from resonance energy transfer, biochip for a quick and accurate detection of multiple cancer markers and neurochemical detection by diamond microneedle electrodes.
According to the National Cancer Institute (NCI), United States 2015 report approximately 1,658,370 new cases of cancer have been diagnosed and 589,430 deaths. The literature says that, in human the most common cancers are: breast, lung, bronchus, prostate, colon, rectum, skin melanoma, Hodgkin lymphoma, thyroid, liver, renal pelvis, endometrial, leukemia and pancreatic cancer [5]. It is doubtless that, the cancer is a multifactorial molecular disease that includes multistage development of tumor cells, caused by a range of genetic or environmental factors, such as exposure to carcinogenic chemicals or radiation, or has a microbiological cause, including bacterial (e.g. - stomach cancer) or viral (e.g. - cervical cancer) infection. In this context, promoter proliferative signaling, escapes from growth suppressors, resistive cell death, replicative immortality, triggering of angiogenesis, and activation of invasion and metastasis are occurring along with the genomic instability, inflammation, and epigenetic changes. Thus, determination of responsible genes, proteins, and abnormalities in the tumor and body fluids such as blood, urine and sputum in the early stage is crucial for an effective treatment.
Microarrays, quantitative polymerase chain reaction (qPCR) and enzyme-linked immunosorbent assay (ELISA) are the frequently used detection methods in cancers. The common disadvantages of these techniques are: expensive, requires highly qualified personnel, time consuming, laboratory-dependent, difficulty in handling, tissue oxidation (qPCR), limited access, destructive testing (microarrays), lack of flexibility in selecting standards, quality and sampling amount [6]. Although, biosensors have limited use in clinics and the molecular markers are not reproducible, but they can overcome other limitations as said above. Moreover, the in situ application, high analytical specificity, cost-effectiveness in time and material consumption, sensitivity through automation, integration of multiple processes in a single device, low-space occupancy and multi-analyte testing capability are the major causes of increasing popularity of biosensors [7,8].
This text focuses a brief scenario on biosensors involvement and applicability in the monitor and detection of early cancer development. Additionally, the hopes and challenges are also plugged in.
Designing of biosensors for early cancer detection
To monoclonal antibodies and aptamers (oligonucleotide or peptide molecules that bind to a specific target molecule) are often used to capture cancer agents, including antigens, while micro ribonucleic acids (miRNAs) corresponds single stranded desoxyribonucleic acid (ssDNA). The transducer, in a biosensor converts the molecular recognition signal to an electrical signal. It may be electrochemical (potentiometry, amperometry, conductometry/impedimetry), optical (fluorescence, luminescence, colorimetric and interferometry), calorimetric (thermistor) or based on mass changes (piezoelectric/ acoustic waves) [9] (Figure 1).
The electrochemical biosensors detect an electrical response when there is a molecular recognition of a specific element. For an example- detection of cancer marker hPRL-3 in breast cancer cells [10]. By utilizing specific DNA sequences, it is possible to recognize elements in cancer and/or conjoined with genetic mutations. BRCA1 and BRCA2 mutations are associated with hereditary breast cancer. This type of biosensor has the ability to detect damaged DNA and carcinogens associated with the damage [11]. Moreover, by using multiple sensors with multiple transducers, it is also possible to detect multiple factors associated with a particular cancer. The cytosensors are the electrochemical-cell-based biosensors utilize living cells as a biological recognition element [12].
Optical biosensors measure the changes in specific wavelengths of light [13]. The biosensors with photonic crystals can capture the light areas or very small volumes and transmit the light to a high electromagnetic field to display the result. These types of biosensors are implemented for monitoring changes in proliferation and apoptosis of breast cancer cells, the rate of drug cytotoxicity and understanding the effectiveness of the treatment. Optical biosensor based on laser-induced fluorescence is evident to use in the diagnosis and monitoring of throat cancer. Interestingly, the use of this biosensor prevented surgical biopsies and the pain associated recovery in more than 200 patients [11].
The mass change biosensors e. g. -piezoelectric biosensors measure the changes in resonance frequency of a piezoelectric crystal in the manner of changing mass on the crystal structure. By using these biosensors coupled with polymerase chain reaction (PCR) amplifications, it is possible to detect the point of mutations in the human p53 gene.
The use of calorimetric biosensors is rarely in the diagnosis of cancer. They measure exothermic reactions. However, in a study with gold nanoparticles (AuNPs), calorimetric biosensors successfully detected two different types of cells in acute leukemia and cells in Burkitt's. Wang et al. [14] suggested that 2D nanomaterial-based biosensors can be used to detect cancer biomarkers. These, mainly cover the graphene, grapheme derivatives (i.e. -grapheme oxide and reduced grapheme oxide), and graphene-like nanomaterials (i.e. -2D layered transition metal dichalcogenides, graphite carbon nitride and boron nitride nanomaterials).
The enzyme-based biosensors have been devised on immobilization methods, i.e. adsorption of enzymes by chemical bonding such as Van der Waals forces, ionic or covalent bonding. The commonly used enzymes for this purpose are oxidoreductases, polyphenol oxidases, peroxidases, and amino- oxidases [15]. The analyte of the tissue-based biosensors are the inhibitors or substrates, including amino acids. On the other hand, the organelle-based biosensors are used to detect the membranes, chloroplasts, mitochondria, and microsomes. Immunosensors act through an interaction between antibodies with their specific antigens. In this case, the antibodies specifically bind to pathogens or toxins, or interact with components of the host's immune system. The microbe-based biosensors detect the microorganisms (both live and dead) or their liberated materials, while DNA biosensors are devised on the property that single-strand nucleic acid molecule is able to recognize and bind to its complementary strand in a sample. In the latter case, an interaction occurs by the formation of stable hydrogen bonds between the two nucleic acid strands [16]. The magnetic (miniaturized) biosensors detect magnetic micro- and nanoparticles in microfluidic channels using the magnetoresistance effect [17]. These can be also applied for the detection of microorganisms.
Biosensor-detectable biomarkers in some cancers
Malignant cells produce biological substances, including pro-inflammatory and inflammatory mediators. Moreover, a number of intra- and intercellular compounds, such as hormones, mucin, isoenzymes, oncogenes, oncofetal antigens, tissue-specific proteins, circulating ribonucleic acids, and some glycoproteins and glycolipids are also the indicators of cancer [18,19]. Some of these markers are organ specific, while others are common. For example, neuron-specific enolase and a breast cancer gene are specific for lung and breast car-cinomas, respectively; whereas cancer antigen 15-3, cancer antigen 125 and carcinoembryonic antigen may be found in breast, lung, or colon cancer. More complications are seen in the expression of miRNAs in some diseases. Otherwise, biomarkers can show different concentration level in different type of cancer [20]. The hysiology, gender and racial factors also have an influence on the levels of a certain or group of biomarkers. Techniques used for biomarkers identification and detection are shown in Box 1.
Gene biomarkers have more specificity in cancers due to the genome diversity. A number of genes have been linked to somatic mutations in human tumor cells or tissues, including oncogenes and tumor suppressor genes, as well as genes encoding proteins that perform key functions in regulation of the cell cycle, DNA repair, and enzyme activity. For example, protein 53 (p53) gene, which is located on the short arm of the chromosome 17 in the human genome and is thought as a guardian of the genome, as it regulates the cell cycle and functions as a tumor suppressor [21]. However, a single mutation in the same location can initiate different cancers depending on the geographical location, ethnic back-ground, and/or gender of the patient. For an example, p53 proline mutation has been found to link in pancreatic cancer in males [22], which has been found to decrease the risk of breast cancer in Arab women [23].
The location of the mutation is also related to the situations of a particular cancer, such as codon 273 mutation in non-small cell lung cancer, while codon 248 for small cell lung cancer in the p53 gene [24]. The other detectable target may be the epidermal growth factor receptor (EGFR), responsible for tumor invasion, angiogenesis, cell proliferation, and apoptosis [25].
Genomic and proteomic analyses are performed to determine potential biomarkers, since the combined data are much more reliable and precise than the data obtained using a single methodology and helpful to find out more specific gene or protein biomarkers for a particular cancer type [26,27]. In protein chip biomarkers, the proteins are isolated and printed on a single slide surface can investigate protein profiling and antibodies via protein-protein interactions [28]. On the other hand, post-genomic technologies and bioinformatics tools are helpful to detect gene expression, mutations, single nucleotide polymorphisms, and cancer biology [29]. Till date, a number of biosensors have been introduced to detect cancer (some of them are shown in Table 1. An electrochemical molecular beacon biosensor has been developed for the sequence-specific recognition of DNA for cancer diagnosis and gene therapy, while the molecular beacon-based biosensors can be used to detect protein biomarkers, small molecules, and RNA . Double stranded DNA biosensors are capable to quantify within the range of 350 pM to 25 nM [30]. Potentiometric biosensors combining the effect and specific molecular imprinting can be used to detect cancer, carcinoembryonic antigen, discriminate between damaged and normal fibrinogen in bleeding disorders, and conformational changes in the protein [31]. Hyaluronan and proteoglycan link protein 1 (HAPLN1) can be used by using an electrochemical open-circuit potential method [32]. On the other hand, piezoelectric biosensor was developed to detect the prostate-specific antigen (PSA) and alpha-fetoprotein (AFP). A titanate zirconate ceramic resonator could success-fully detect PSA and AFP up to 0.25 ng/mL in a short time (30 minutes) with a small sample volume (1 µL) [33].
Nanoparticles have a wide range of applications for detection of different types of disease, such as cancer, infec-tious diseases, and neurological disorders [34]. Short fragments of DNA can be tagged with AuNPs for the detection of targeted gene sequences. On the other hand, quantum dots (QDs) and magnetic iron oxide nanoparticles can be designed for dual-mode imaging of cancer. The silica and iron oxide nanoparticles can be used to detect lung cancer cells [35]. AuNPs-conjugated anti-EGFR antibodies are evident to show 600% higher binding affinity with cancerous cells than noncancerous cells [36]. Manganese oxide nanoparticles combined with magnetic resonance imaging (MRI) can be used to diagnose neurological disorders such as Parkinson's disease, stroke, and Alzheimer's disease [37]. Moreover, there is a chance to attach the affinity ligands such as antibodies to these nanoparticles. The later type of fabrication can detect bacteria, while silver nanorods have been introduced for a rapid quantification and characterization of viruses, by recognizing spectral differences between viral strains, viruses, and viruses with gene deletions in biological samples [38]. The multicolor optical coding using QDs is also another important application in molecular diagnosis [39]. On the other hand, bio conjugated QDs are useful to detect disease progression, and response to therapy [40].
The ovarian cancer exhibits a wide range morphologies and variations in clinical and genetic ways during the process of tumor progression. In this cancer, the beta-2-microglobulin (B2M) is found to over express, that can be a useful tool to detect [41]. However, targeting of a single molecular marker is not enough [42]. In breast cancer, the detection of hormone receptors, such as estrogen (ER), progesterone receptor 2 (PR2) and the EGFR is commonly done. Although, the immune histochemistry (IHC) is used as a quantitative method to detect the expression of HER2 receptors, but is has some disadvantages in fixing protocols, registration systems and level of placement, and the selection of antibodies [43]. On the other hand, in cervical cancer the expression of the E6, E7 and E5 of the high-risk subtypes of human papillomavirus (HPV) oncoproteins can be measured in cervical cancer Although, it requires long periods of latency for the malignant transformation [44], but can be detected using a novel leaky surface acoustic wave peptide nucleic acid biosensor with double two-port resonators.
The linear discriminatory analysis, microarrays and RealTime Quantitative Reverse Transcription PCR (Real-Time qRT-PCR) have been used for the diagnosis of prostate cancer with 100% accuracy [45]. The AMARC (methylacyl alpha CoA racemase), an enzyme involved in the oxidation of branched chain fatty acids, which is evident to overexpress in prostate and some other cancers. In this regard, IHC antigen P504S is helpful to detect AMACR. Additionally, the blood and urine samples are also useful to detect the gene mRNA of AMACR using qRT- PCR, while the nuclear matrix protein, early prostate carcinoma antigen (EPCA) by using ELISA or tissue IHC [46].
In lung cancer, low-dose computed tomography (LDCT) is widely used [47]. A combination of computed tomography and positron emission tomography with 18F-fluorodeoxyglucose (18F-FDG PET/CT) is also used in this case. Generally, the growth of a tumor is accompanied by changes in genes and proteins. Thus the point of methylation or mutations of DNA, RNA and protein expression can be targeted. Some other biomarkers can also be helpful in this purpose, such as altered carbohydrates, cytokines and chemokines, volatile organic compounds from the peroxidation in the cell membrane [48]. In lung cancer, the other mutations can be detected as: BRAF [49], KRAS [50-52], HER2 [53,54], DDR2, PIK3CA, PTEN, AKT, KEAP1, and NFE2L2 [55]. Furthermore, recurrent gene rearrangements involve: ALK, ROS1, RET and NTRK in this cancer [56,57].
The AFP is a normal serum protein synthesized by liver, yolk sac and gastrointestinal tract. Over expression of AFP, is evident to cause liver cancer [58]. On the other hand, C-reactive protein (CRP), synthesized by IL-6 in the liver, circulates in the blood is a prognostic indicator of gastric cancer [59-65]. These types of biomarkers can be detected in serum by using electrochemical and quartz crystal microbalance (QCM) techniques. In breast cancer the detectable biomarkers are: ER, PR, HER2, BRCA1, Ki67, osteopontin, mammoglobin, sirtuins, autoantibodies,CA15-3, CA27.29, CTC, CEA, BRCA1, BRCA2, MUC1, EpCAM,EGFR, miR-21, 16, 27a, 150, 155, 191, 222. In Table 2, a list of biomarkers in some cancers has been shown along with the molecular detection methods [66-76].
Concluding remarks
With the biosensor and molecular techniques, it can be said that a number of molecular markers available may be excellent candidates for the identification and detection by using biosensors. Moreover, the use of biosensors in the early detection of cancer and monitoring the overall progress of disease state is the hopeful keys for the effective treatment, thus reducing the mortality rate of the patients [77-80]. Biosensors can be used in some laboratory tasks, including genotoxic and mutagenic markers such as chromosomal aberrations and micronucleus tests [81-85].
Doubtless, before treatment- proper diagnosis is essential. In this sense, still there is a long way to go to understand a complete set of markers in a particular cancer. Non-specificity in expression of some markers may offer wrong diagnosis, therefore, wrong treatment [86-90]. Otherwise, the problems in the reproducibility of the method and difficulties in the fabrication of the biosensor materials are also should be resolved. The level of detection is another fact in this novel technology, as the expression of biomarkers depends on: duration of disease, patient's pathophysiology, age, gender, genetic diversity, the conditions for taking of tissue, lifestyle of the patient, earlier and concurrent treatment received and so on.
However, continuity in research may be helpful to overcome the overall challenges those are yet to be resolved with the application of the biosensor in cancers. Finally, it is doubtless that, the biosensor technology has opened a hopeful door in the diagnosis, therefore earlier treatment- thus the possibility of an increase in the survival rate or lifespan, by decreasing suffering and mortality rate of the cancer patients [91-95].
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
https://juniperpublishers.business.site/
0 notes
Text
Pelvic Abscess Formation Secondary to the Use of Commercial Hemostatic Topical Agent in an Immune Compromised Patient?
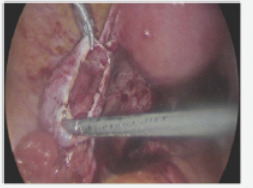
Authored by Rodrigo Ayala-Yáñez*
Abstract
Various hemostatic agents are currently available for routine laparoscopic procedures, avoiding thermal lesions due to energy devices and the complexity of intracorporeal sutures, however, evidence of complications in immune compromised patients is still lacking. We present the case of a severely immune compromised gynecological patient who underwent a routine laparoscopic cystectomy, where a local hemostatic agent was employed; further complications arose, a second diagnostic laparoscopy revealed a pelvic abscess with severe adhesion formation. All under a complicated clinical setting due to an impaired immune response, whether this abscess was caused due to the hemostatic agent or other patient's conditions remains to be determined, still, various clinical factors and patient's response need to be taken into account as the cause of the abscess formation.
Keywords: Hemostatic agent; Pelvic abscess; Laparoscopy; Immuno compromised patient; Cystectomy
Introduction
Bleeding control is one of the most important goals during any surgery. Alternative to the standard suture materials and energy devices, a great variety of topical hemostatic agents and tissue adhesives are currently available in order to improve outcomes such as reduced blood loss, need for blood transfusion, shorter surgery times and risk for re intervention [1,2].
At present, precise indications should be followed since complications may arise as we present in the following case report. The aim of this article is to review the medical and scientific information regarding hemostatic agents.
We present a rare case in an immune compromised patient who underwent a cystectomy, laparoscopic surgery in which the topical hemostatic agent “Surgiflo®” was used to stop oozing .Patient's outcome was complicated with a pelvic abscess and severe adhesion process that required an open surgical intervention.
Case Report
We present the case of a 26-year- old woman, nulligravida with relevant clinical history of systemic lupus erythematosus (SLE), chronic anemia, hypertension, diabetes and end stage renal disease, treated with renal transplant complicated with chronic allograft rejection that conditioned her to require hemodialysis 3 times per week. Current medications include: Tacrolimus, Azathioprine, and Prednisone.
Clinical findings on admission were: acute pelvic pain accompanied with profuse trans vaginal bleeding. Endovaginal ultrasonogram revealed the presence of a 6cm cystadenoma in the left ovary and free fluid in the pelvic cavity. All her laboratory tests were normal no sign of infection was recorded previous to the surgical procedure.
Laparoscopic findings were compatible with endometriosis, adhesions in the cul de sac were identified and surgery was performed with Thunder beat® energy device. Aspiration and capsule resection completed the procedure (Figure 1).
Despite initial hemostasis, posterior cul de sac (where the adhesiolys is took place) presented oozing and the topical hemostatic agent Surgiflo® was applied in order to prevent an hematoma formation, achieving adequate hemostasis (Figure 2). Patient was discharged 2 days later, developing urinary tract infection positive for Ureaplasma urealyticum, that was treated with broad spectrum antibiotics.
Fourteen days later Bacteroides fragilis was inoculated in a blood sample and was treated with vancomycin and ertapenem. Patient's response wasn't satisfactory despite all the precautions and multidisciplinary approaches. She continued to have intermittent fever and diarrhea (although all her coprological cultures were negative).
After four weeks, the patient was readmitted due the presence of persistent fever and pelvic pain. Laboratory tests reported slightly increased leucocytes (9.7x103µL), low hemoglobin of (7.3g/dL), 3 bands, procalciton in of 0.6ng/m Land an elevated Creactive protein (CPR, 13.97mg/dL). Blood, urine, stool and cervicovaginal cultures were negative. Ultrasound reported a 7cm, diameter collection with heterogeneous characteristics with fluid contents located in the posterior cul de sac, compatible with remnants of an hemostatic agent (Figure 3).
Since the etiology of the fever wasn't determined, a second diagnostic laparoscopy was performed. During this procedure, multiple adhesions that distorted normal anatomy were identified, an abscess of 2cm in diameter was found in the posterior cul de sac, firmly attached to the left ovary and rectum. Due to the severe adhesion process, laparotomy conversion was opted. In the open procedure, adhesion removal and exhaustive pelvic cavity lavage were performed, the abscess drained 15 ml of purulent material with no characteristic smell, samples were taken for microbiologic cultures (Figures 4 & 5), (no pathogen was isolated). A sponge like material was found and taken out of the posterior cul de sac, compatible with the common degradation process of the hemostatic agent. Parenteral antimicrobial medication was initiated with adequate response, discharging the patient 1 week later. No further complications were reported.
Discussion
This clinical case presents a severely immunocompromised woman who was attended for a relatively common gynecological condition and subsequently complicated with a pelvic abscess and adhesion process.
The possible associations of hemostatic agents with infective complications are listed as follows:
Histologic changes with granulomatous reaction secondary to foreign material [3].
Delayed time of absorption of some hemostatic agents [4-6].
Biological material agents are prompt for colonization serving as culture media [7,8].
Incorrect amounts and disposal of hemostatic agents may lead to adhesion formation [7,9].
Some agents promote a diminished pH on nearby environments, disrupting local innate defense immune mechanisms such as protease activity [1,10]. On the other hand, oxidized regenerated cellulose hemostatics are considered bactericidal, due to their acidification of the media [2].
Previous studies performed on immunocompetent patients identified risk factors for abscess formation such as untreated pelvic inflammatory disease, endometriosis, previous laparotomy and post-operative hematomas [11-13]. Hemostatic agents have been suggested as an added risk factor for infection in these clinical settings; however we currently lack quality evidence to support this statement. Additionally, studies that address this question in immunocompromised subjects are needed.
Clinical benefits of the hemostatic agents, supported by existing studies are:
Preventing thermal damage on vascular and nerve structures (as when electrosurgery is employed).
Achieving early and adequate hemostatic control in friable tissues.
Better outcomes in patients with hemorrhagic diathesis [14-16].
Risk of infection secondary to fluid hemostatics such as Floseal® or Surgiflo® may be minimized by removing the excess of this topical hemostatic agent from the wound after hemostasis is achieved, since excessive amounts of slowly degrading products can serve as a site for infection development [17,18].
In this, case the underlying clinical conditions placed the patient at higher risk for any type of infection in comparison with the rest of the population, hence, secondary abscess formation couldn't be stablished with certainty.
Finally, current guidelines on late abdominal sepsis state that a possible mechanism explaining the presence of anaerobic pathogens similar to the one presented, is bacterial translocation which presumably caused bacteremia with B. fragilis. No pathogen was inoculated in the second procedure probably due to the previous administration of broad spectrum antibiotics.
Conclusion
Because of the insufficient evidence available, the authors' recommendation is to avoid excessive use of this type of hemostatic in immunocompromised patients.
If strictly necessary, and the patient's condition warrants it, we suggest choosing a rapid resorption hemostat such as Microporous Polysaccharide Spheres like Arista® as first choice, this one shows complete resorption within 48 hours vs gelatin matrix agents that can take 6 to 8 weeks to disintegrate. Surplus hemostatic agents should be removed after achieving the desired effect.
Conflict of Interest
Authors have no disclosures and no conflict of interest.
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
https://juniperpublishers.business.site/
#gynecology#women's health#Hemostatic agent#Pelvic abscess#Laparoscopy#Immuno compromised patient#Cystectomy#fertility#sex#breastfeeding#breast cancer#pregnancy
0 notes
Text
Hysterectomy: Hysteroscopic Sterilization's Unintended Dividend?

Authored by E Scott Sills*
Abstract
Although previous work has suggested that the risk for re-operation after hysteroscopic sterilization (HS) is much higher than for patients who undergo standard laparoscopic tubal ligation, few data have been collected on these subsequent procedures. Recently, a descriptive cohort study used a confidential online questionnaire to gather data from more than 3,000 women who developed pelvic pain and other symptoms after HS. Information was obtained on device removal surgery performed secondary to symptoms developing after the Essure procedure. These patients were relatively young, having amean±SD age of 35.6±6.3yrs; hysterectomy was eventually performed in nearly 65% of HS cases. More research is needed to characterize specific gynecological operations after HS, but preliminary findings suggest that the predominant surgical remedy for Essure-associated complaints is hysterectomy for many women. Thus, dissatisfaction with HS may represent an important new indication for hysterectomy and additional study will be crucial to quantify this phenomenon.
Keywords: Contraception; Pelvic pain; Essure; Hysteroscopic sterilization; Hysterectomy
Background
The Essure device (Bayer Corp Whippany, NJ USA) gained approval by the U.S. FDA in November 2002 and remains the only hysteroscopic contraceptive method available in the U.S. The procedure can be completed without anesthesia, involves no incision, and may be performed in as a little as ten minutes by an experienced hysteroscopist [1,2]. The procedure involves introduces a pair of small, flexible inserts consisting of nickel- titanium and polyethylene terephthalate (PET) fibers through the fallopian tubal ostia via hysteroscopy. Once in place, the devices trigger an intraluminal inflammatory reaction resulting in tubal fibrosis and eventual occlusion. While HS enjoyed considerable initial popularity, within several years complications began to appear in the medical literature and were reported to health regulators [3-6]. Fortunately, surgical removal of HS devices has usually resolved symptoms for most patients [7,8]. While there is no consensus on a preferred method to remove Essure implants, hysterectomy has emerged as one way to do this [5,8-10]. The connection between this contraceptive implant and subsequent hysterectomy has only recently been the subject of specific study, however [11].
Hysterectomy is a major operation and is the most frequently performed surgery for women in the United States after cesarean delivery [12]. Accurate data regarding indications for hysterectomy informs a crucial part of monitoring health outcomes. Most estimates of national hysterectomy activity cannot provide a comprehensive assessment because registries are generally limited to surgeries performed in formal hospital settings [13], and hysterectomies are often performed in ambulatory surgery centers outside this data capture remit. A reporting gap also exists with HS, because there is no national registry for this procedure either. Statistical impairments thus exist both for HS and hysterectomy, as reliance on standard hospital reports cannot give a complete audit of either event.
Researchers following hysterectomy have tried to meet this challenge by modifying their study design to follow insurance payments rather than hospital activity [12]. Unfortunately, such an approach does not yield a full understanding of HS, since although this elective sterilization technique is often done on an out-patient basis, it is not uniformly covered by insurance plans in the United States [14-16]. Not even the device manufacturer knows exactly how many patients have had the HS procedure (in the United States or elsewhere) and only data on the approximate number of Essure kits is available [17]. Thus, measuring any common overlap between HS and hysterectomy- both gynecological interventions with substantial public health implications-is difficult.
What happens after HS?
There is no clear consensus on how to manage Essure patients who subsequently develop symptoms after HS [18]. While the notion that these patients might require further surgery is not entirely new, at least for some Essure patients the reliance on hysterectomy can be quite high [11]. One recent analysis evaluated 30-day and 1-year outcomes after >8,000 Essure procedures in New York State and found the risk of undergoing reoperation was more than 10 times higher for HS patients compared to patients undergoing standard laparoscopic tubal ligation [19]. Recent work has extended this observation by contributing a more detailed understanding of surgeries performed after Essure [11].
As HS coils are intended to be permanent contraceptive implants, it is not surprising that familiarity with their surgical excision remains limited [5,8,20]. It is encouraging that satisfactory relief of Essure-associated symptoms has been reported as soon as two weeks following removal [21]. Why might HS be perceived as better than traditional bilateral tubal ligation? A 2009 decision tree analysis to estimate procedure costs is sometimes cited to support the position that HS brings a cost advantage over standard tubal sterilization [22]. Such a model now seems problematic as it incorrectly assumed that patient satisfaction would be similar between the two comparator groups. Because few patients in HS premarketing studies were followed for more than 12 months [23], how many might seek additional surgery to “undo” Essure after the first year of use could not have been known previously. Although it is not surprising that such extra surgery brings additional expense, some research has shown that a priori costs for HS are already higher than for laparoscopic tubal ligation despite shorter operative time and less frequent use of general anesthesia [19]. Controversy also exists concerning the effectiveness of HS as a method of reliable birth control [24,2 5]. This raises the question of device failure with profound economic and social implications of its own [26]. While none of this information was available for consideration when Essure was initially approved by the U.S. FDA in 2002, awareness of such factors now could explain a higher level of patient interest in surgical device removal.
Likewise, hysterectomy may be regarded (either by physicians, patients, or both) as superior to other less invasive surgical approaches for Essure abatement. For example, it is possible that the lack of a CPT code specific to surgical Essure removal favors hysterectomy, a surgery for which multiple CPT codes exist. Despite the known higher cost, intra operative blood loss, overall complication rate and increased recovery time associated with hysterectomy, this surgery could nevertheless be recommended over less aggressive operations for which insurance companies might reject or delay the claim (i.e., no timely disbursement).
Conclusion
Interpreting HS data continues to frustrate regulators, patients, and advocacy groups. Thus, until the regulatory climate changes to enable acquisition of HS data with greater precision, internet-based assessment tools may supply the best available evidence on HS. Indeed, similar patient-completed surveys have been used in previous pelvic surgery contexts with good results [27,28]. There is also the matter of linking HS to whatever operation which followed, and determining what factors (physician and/or patient) resulted in particular post-HS interventions. Like much of the Essure phenomenon, however, this is an underdeveloped area of inquiry awaiting additional research for clarification. The lack of established clinical guidelines for Essure removal appears to permit a considerable range of surgical approaches in routine practice.
For many women, the allure of “non-incisional” permanent contraception as promised by HS would be substantially diminished if major surgery were later needed [9,10]. Given the paucity of meaningful longitudinal data on HS patients, the hysterectomy rate following Essure remains undefined. Yet should this birth control choice even sometimes lead to hysterectomy, caution is appropriate and the issue should receive close scrutiny If the number of HS kits sold worldwide is 750,000 [23], then determining how these devices contribute to overall hysterectomy uptake represents a relevant topic in the domain of international Women's health. Consideration should therefore be given to creating an Essure patient registry, or, alternatively, creating specific ICD-10 codes for patients who present with HS-associated symptoms. These would be cost- effective interventions to enable proper surveillance on this topic.
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
https://juniperpublishers.business.site/
#Contraception#Pelvic pain#Essure#Hysteroscopic sterilization#Hysterectomy#gynecology#gynecological cancers#breastfeeding
0 notes
Text
The Reproducibility of 5D Long Bone Versus VOCAL 3D and Conventional 2D Weight Formulae in Measurement of Birth Weight

Authored by Wael S Nossair*
Abstract
Objective: To assess the accuracy of of 5D automated measurement of long bones, three dimensional VOCAL measurement of fetal thigh volume in prediction of fetal weight in comparison to the conventional two dimensional Hadlock formulas.
Methods: Fifty pregnant women with singleton pregnancy at 37 to 41 weeks of gestation admitted for planned delivery within 48 hours were enrolled. All patients were examined by 2D, 3D VOCAL and 5D long bones for the purpose of estimating the fetal weight. Each technique was performed by the same examiner for all the patients who were blinded to the results of the two other techniques. Results were compared to actual birth weights using a unified weight scale. The accuracy, precision and agreement between the three types of ultrasound were calculated as well the time needed to perform each technique.
Conclusion: Three dimensional ultrasonographic measurement of fetal thigh volume is more accurate than two dimensional Hadlock formulas in fetal weight estimation in our population. The new 5D automated long bone represent a faster, more convenient and accurate method for assessment of birth weight.
Keywords: Birth weight measurement; 5D Long bone; Vocal
Introduction
The assessment of fetal weight is an important indicator for the fetal nutritional state and one of the factors affecting critical obstetrics decisions [1,2]. Over the last decades estimation of the fetal weight was based on 2D ultrasound formulae which had the disadvantage of being inaccurate as shown in pervious systematic reviews [3] and also failed to predict neonatal adipose tissue status which is more affected by nutritional status [4]. Significant improvement of the measurements was achieved after incorporating measurements of the thigh volume using 3D ultrasound [5]. Fractional limb volume is a fetal soft tissue parameter that is based on 50% of the long bone diaphys is length to avoid the falsies obtained from difficult volume acquisition near the end of long bones [6]. Further improvement in accuracy was recorded following the use of VOCAL technique which can be more precise in obtaining volume from regular shaped objects [7]. However, 3D-ultrasound still requires time and effort in reconstructing the image and is affected by the angle used and the experience of the sonographer which affects its reproducibility. To overcome these defects, long bone automated detection system, five-dimensional 5D Long Bone (5D LB) was introduced with an automated system that allow the volume measurement to be completed in just a few seconds and eliminate operators variability which makes it more useful in clinical practice [8]. Also the fact that ethnic and racial variation exists in fetal biometry [2], mandate testing the hypothesis that 5D or 3D ultrasonography measurement of fetal thigh volume may be more accurate in prediction of fetal weight in comparison to the conventional two dimensional Hadlock formula in this study population.
Patients and Methods
This study is a prospective study conducted at Zagazig University Hospitals, and Agial Fertility Center. Accordingly throughout the period between June and December 2016, 50 pregnant women with singleton pregnancy at 37 to 41 weeks of gestation, who were admitted for planned deliverywithin 48 hours either by induction of labor or elective caesarean section, were enrolled. Gestation age was calculated from the first day of the last normal menstrual period (LMP) provided it is sure and reliable (regular cycles for the preceding three months with no history of hormonal contraception or recent termination of pregnancy). Otherwise gestation age was calculated from early first -trimester ultrasound with crown rump measurement. Patients with fetal anomalies, abnormal amount of liquor and factors influencing proper measurements as pelvic lesions were excluded from the study. Demographic data were recorded and all patients underwent a formal 2D ultrasound scan by the same examiner to calculate the expected fetal weight by using the Hadlock IV model, which incorporates biparietal diameter (BPD), head circumference, abdominal circumference (AC) and femoral diaphysis length (FL) [9]. 3D ultra sonography were used by another examiner blinded to the previous measurements for thigh volume measurement according to the principle described by Benini et al. [7]. "The conventional plane for measurement of femur length was first identified for orientation of the thigh then the plane was rotated to put the femur accurately in a horizontal position. A stepwise measurement using the Virtual Organ Computer-aided Analysis (VOCAL) technique were performed as follows: The data set containing the fetal thigh was initially displayed on the screen in three orthogonal planes, the sagittal view of the femur were displayed in Plane A and this image were rotated so that the orientation of the thigh and whole diaphysis coincides with the y-axis. Two demarcating arrows were positioned at each end of the diaphysis to define the limits of the thigh to be included in the volume calculation. Volume estimates were computed utilizing the VOCAL program with a manual trace at 30 of rotation. At the end of the 180 rotation, the built in software was used to calculate the volume automatically” Birth weight (BW) were calculated through the following formula BW =1025.383+12.775 x Thigh volume. Biometric measurements were taken as the average of 2 readings. The machine used for examination was Voluson E6 BT12 with a volumetric abdominal probe RAB 6D-4D curved Array (General Electric Medical Systems, AUSTRIA). Subsequently, the long bone length was measured by another analyzer using the 5D LB with the following procedures described by Hurr et al. [8]. "The volume data used in the manual 3D-ultrasound measurement were displayed in an offline multiplanar mode, and the 5D LB set key was pressed on the system, wherein the system automatically analyzed the 3D volume data, reconstructed the 3D image of the long bones, and displayed the measured lengths of the long bones on the screen” After delivery all neonates' weights were obtained using the same digital weight scale immediately after birth and recorded in the hospital files.
Ethical consideration
Institutional review board (IRB) approval: The protocol was discussed by the ethical scientific committee for approving the study and informed consent was obtained before participation. Acceptance of local institutional committee and the ethical committee of the faculty of medicine was obtained before commencing the trial and all participating women signed a written informed consent after proper explanation.
Sample size calculation
The required sample size has been calculated using G *Power software version 1.1.7 (Germany). The primary outcome measure is the accuracy of 2D, 3D or 5D ultrasonography for estimating the actual weight of the newborn obtained immediately after delivery. So, it was estimated that a total sample size of 50 patients on whom estimation of the birth weight was undertaken would achieve a power of 90% (type II error, 0.1) to detect a statistically significant difference between the overall accuracy of any two techniques for a median effect size (Cohen's dz) of 0.5 using a two- sided paired t test with a confidence level of 95% (type I error, 0.05). This effect size has been chosen as it could be regarded as a clinically relevant difference to seek in this study.
Results
Data are mean±SD or number (%).
Data are mean±SD.
Signed error is the estimated weight by US minus the actual birth weight.
Signed percentage error is the estimated weight by US minus the actual birth weight/actual birth weight *100.
Absolute error is the unsigned difference between the estimated weight by US and the actual birth weight.
Absolute percentage error is the unsigned difference between the estimated weight by US and the actual birth weight/actual birth weight *100.
T: Statistic; Df: Degree of Freedom
¶Paired Student t test.
50 women underwent the three modalities of ultrasound within 48 hours of delivery. The characteristics' of the included patients are summarized in Table 1.
Comparing the accuracy of 2D ultrasound to 3D ultrasound in the assessment of birth weight (Table 2) showed that 2D estimated fetal weight was significantly less accurate than 3D estimated fetal weight as measured by absolute birth weight estimation error and percent birth estimation error. On the other hand comparing the accuracy of 5D to 3D ultrasound showed a statistical significance in favor of the 5D but the difference was so small to impose a clinical significance in obstetric practice [10,11].
Discussion
The accurate prediction of birth weight is essential not only in macrosomic fetus to avoid unplanned birth injuries or operative deliveries but also in low birth weight growth restricted fetus to avoid perinatal asphyxia [12-14]. Previous studies demonstrated up to 10% standard error for most of the commonly used 2D formulae for estimation of fetal weight specially at the birth weight extremities [5]. It is debatable if this observation is attributed to inter-observer variability or to the lack of incorporation of soft tissue measurements in most of these formulae [2]. Subsequently improvements in the accuracy of BW estimation were achieved after incorporating measurement of fetal weight using 3D with earlier study showing absolute percentage errors of less than 6% [7].
In the current study 2D EFW was significantly less accurate that 3D EFW as measured by absolute BW estimation error & absolute percentage BW estimation error. Also in this study, 3D U/S EFW was significantly more precise than 2DU/S EFW as determined by absolute BW estimation error & absolute percentage BW estimation error. These results agreed with the previous work of Schild et al. [15], Isobe [16] and Sriantiroj et al. [17] who agreed that fractional ThV was the best predictor for actual birth weight and is superior to 2D U/S formulae which need head measurement which is usually inaccurate at term pregnancy especially if the fetal head is deeply impacted in the pelvis and also lacks the ability to assess the effect of fat distribution in the limbs, facts which further compromised fetal- weight estimation by 2D formulae.
On the other hand, Lindell et al. [18] reported no difference between 2D and 3D ultrasound in the estimation of fetal weight in a group of women with post term pregnancy, a different cohort from our study population, also Bellini et al. [7] postulated that the previous superiority of 3D formulae over 2D might be attributed to phenotypic differences between different patients used to create each of these formulae. Yang et al. [2] emphasized on the fact that ethnic and racial variations can significantly affects fetal biometry which prompt careful interpretation of data obtained from different studies.
Despite the obvious superiority of 3D ultrasound in estimation of fetal birth weight, the technique is still operator dependent and requires a learning curve for proper acquisition and manipulation of volume data [8]. In an effort to overcome this drawback, long bone automated detection system by 5D was introduced to create an operator independent, quick and efficient method for accurate estimation of fetal birth weight. In the current trial, this fully automated system revealed absolute birth weight estimation error of 0.95% which is comparable to the previous work of Hurr et al. [8] who reported an overall error rate of 5.4% in a larger sample [8].
In the current trial, 3D assessment of fetal volume was done using the VOCAL technique with a 30° rotation angle which was previously shown by Benini et al. [7] to be significantly faster than multi planner method (P<0.001). A former trial reported that 3D volume data was acquired within 2 minutes and interpreted in 6 to 7 minutes [19].
The points of strength in this study lies in its ability to complete the three modalities in all patients who were examined with the same examiner for each technique, all patients were delivered within 48 hours from the ultrasound scan detected to avoid falsies from longer intervals and birth weights were recorded by the same digital weight scale attended by an examiner to ensure accuracy.
On other hand the authors recognize the fact that fetuses with abnormal growth were not assessed as the random selection resulted in a study population which was within normal range of birth weight. The implication of these findings on babies in the extremes of body weight might be a point of interest for future research.
Acknowledgement
The authors acknowledge the effort of all the members of the fetal Medicine Unit Ain Shams University Maternity Hospital in the procedures done and the work of Dr. Sameh Michelle Hakim Biostatistician in the data analysis.
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
https://juniperpublishers.business.site/
#Birth weight measurement#5D Long bone#Vocal#gynecology#women's health#prediction#fetal weight#menstrual period#biparietal diameter#abdominal circumference#inter-observer variability
0 notes
Text
Eating Disorders and Reproduction in Women

Authored by Bayramova AN*
Keywords
Malnutrition is a major problem in developing countries, and obesity and eating disorders are increasingly common in developing as well as developed countries. The reproductive axis is closely linked to nutritional status, especially under nutrition in the female, and inhibitory pathways involving detectors in the hind brain suppress ovulation in subjects with weight loss. Recovery may occur after minimal reacquisition of weight because energy balance is more important than body fat mass. Anorexia nervosa and bulimia nervosa affect up to 5% of women of reproductive age causing amenorrhoea, infertility and, in those who do conceive, an increased likelihood of miscarriage.
Keywords: Contraception; Miscarriage; Nutrition; Obesity; Reproduction
Introduction
Nutrition problems are strikingly different in developing nations (deprivation and under nutrition) and developed nations (eating disorders and obesity), although obesity is on the increase even in developing countries. Malnutrition is associated with 55% of deaths among children under the age of five. Over 4 million of the 12 million annual deaths are in sub-Saharan Africa alone, where every third child is underweight and two out of five are stunted. Iron deficiency anaemia is a contributing factor in over 20% of post-birth maternal deaths in Africa and Asia. Nearly 67 million children are wasted (weigh less than they should for their height); and about 183 million weigh less than they should for their age. Unfortunately, reducing poverty and increasing food production by themselves cannot solve the nutrition problems of the poor in developing countries [1]. Major public health and social expenditures are needed to address these devastating conditions that at present cannot be remedied substantially by medical practice.
In contrast, developed nations experience little deprivation, but eating disorders and obesity are increasingly common and may be amenable to medical intervention. For females, reproduction involves much greater energy expenditure than for males, and as a protective mechanism against under nutrition, the reproductive axis is closely linked to nutritional status. As one consequence, eating disorders leading to loss of weight are associated with reduced frequency or cessation of ovulation. Since energy balance more than absolute weight loss is the key factor, there may be a return of ovulation after no more than a small percentage change in body weight recovery. Obesity, however, is a less reliable risk factor of infertility except among obese women who also have polycystic ovarian disease. This review of nutrition and reproduction will address the clinical conditions that are associated with underweight in developed countries. It will outline the physiological mechanisms and clinical conditions associated with under nutrition.
Under Nutrition
Physiological mechanisms
The reproductive system is extremely sensitive to influences from the external environment [2]. Most animals adjust their pattern of reproduction so that the chances of their offspring surviving are maximal. A common strategy involves timing of conception by photoperiod and/or rainfall which usually ensures that birth takes place in a season when food and climatic conditions are favorable, such as spring.
Reproduction involves much greater energy expenditure in the female than in the male. The nourishing of the offspring during pregnancy and lactation and their subsequent rearing to adulthood are the biggest expenditure of energy that a female mammal will make in her lifetime. Hence, the female reproductive system is much more sensitive to disruption than the male.
Because reproduction involves energy expenditure, it is sensible that the physiological control mechanisms are linked to those involved with appetite and nutrition [3]. Food is used as a source of energy for a variety of essential and nonessential functions. In times of deprivation it is necessary to ration available oxidizable substrate in favour of those essential functions involved in staying alive, e.g. keeping warm [4]. Reproduction is expendable at least in the short term and can be deferred until times are more favorable. During lean times animals have devised a number of strategies to reduce energy output such as huddling together in insulated nests (houses), daily torpor or hibernation. Very little energy is diverted to storage of fat. Rather, calories are mobilized from fat stores in an attempt to maintain energy balance. Thus, it is energy balance not fatness per se that regulates reproductive function.
Energy balance and ovulation
Approximately 1-5% of women suffer from 'weight-related amenorrhoea' [5]. Because many girls with delayed puberty are relatively thin during adolescence it has been suggested that a certain critical body weight (47kg) or body fat content is required for onset of cyclical ovarian activity [6,7]. However, although ovarian activity and fat content are correlated they are not causally linked. It is relatively easy to dissociate fatness and reproductive function. Thus, for example, menstrual cycles return in some female athletes when energy expenditure is reduced such as after an injury long before there is any change in body weight or an increase in body fat [8].
Reproductive function, like appetite, is responsive to shortterm changes in metabolic food oxidation. For example, many breeds of sheep are capable of altering their ovulation rate and hence the number of lambs they carry depending on body condition (Martin et al., 2004). Feeding underweight sheep high- calorie supplement of lupins or clover hastens the onset of the breeding season ('flushing') and increases the ovulation rate. A similar effect can be produced by administration of a glucogenic 'drench' [9].
The mechanisms involved in this adjustment of reproductive function involve the availability of calories. When Syrian hamsters are administered 2 de-oxy-d-glucose (DG), which limits glucose oxidation, ovulatory cycles are interrupted rapidly (Schneider and Wade, 1990). It is likely that this involves both central and peripheral mechanisms. In sheep and rats infusion of DG directly into the lateral ventricles depressed LH secretion [10,11]. Subsequent experimentation has helped define the pathway by which calorie deprivation leads to short-term inhibition of reproductive function. It appears that in the rat the metabolic signals are detected by chemo receptors in an area of the hind brain area (postrema (PA)). The signals involved in this are not entirely clear but probably include leptin and insulin/ glucose [12,13].
Epinephrine, nor-epinephrine and neuropeptide Y (NPY) neurones connect to the forebrain to influence GnRH secretion in the hypothalamus [14]. When the animal is replete, the system is free running. The 'brake' is only applied during times of negative energy balance and involves NPY neurons [14,15]. Nutrition and reproduction [3]. NE, nor-epinephrine; NPY, neuropeptide Y; PA, postrema.
Recent observations in women with 'hypothalamic amenorrhoea' have suggested that these experimental studies are relevant to clinical disorders. Women with anovulation associated with strenuous exercise or who are underweight, have low levels of leptin, LH and estradiol [16]. The frequency of gonadotropin pulses is too low to sustain development of antral follicles to the point of ovulation. When leptin was injected to restore levels to normal, there was an immediate increase in the frequency of LH pulses within 2 weeks, followed by growth of large ovarian follicles. Ovulatory cycles were restored in three out of eight women. Whether leptin acts directly on the hypothalamus or increases the availability of oxidizable metabolic substrates or both is unknown. It is likely that leptin plays a significant role in mediating this event although it should be noted that when nutritionally starved animals are refed the frequency of LH pulses increases long before there is an increase in circulating leptin [17].
Energy balance and implantation
Nutrition not only influences ovulation and fertilization but also implantation and early fetal development. Paradoxically overfeeding of sheep in the first few weeks of pregnancy results in an increase in embryonic mortality associated with low levels of progesterone [18]. The level of nutrition during pregnancy has a profound effect on fetal development and subsequent susceptibility in adulthood to disease. When ewes were underfed during mid pregnancy there was an increase in the incidence of pre-term birth [19]. The concept of fetal programming in utero which was originally derived from epidemiological studies in man has been confirmed in a number of experimental studies in animals [20,21]. Thus there is little doubt that nutrition plays an important role during pregnancy as well as in determining the timing and quality of reproductive activity.
Eating disorders
Under nutrition implies inadequate food intake or faulty assimilation due to low-caloric intake or limited nutritional diversity. In developed countries it is most commonly found in women with eating disorders.
Although records of under nutrition from developing countries are scarce, the experience from the Dutch famine in 1944-1945 is relevant to modern countries with a high prevalence of malnutrition. In the Western Netherlands, average daily intake fell from 1500 to less than 700 kilocalories from October 1944 to January 1945 and the birth rate fell 9 months after October 1944. Future reproductive life was affected among women who were severely affected by famine at 3 to 13 years of age: they had a 1.9 fold higher risk (95% CI=.3 1.8) of having fewer than the desired number of children in their lifetime [22].
Under nutrition due to eating disorders may affect ovulation and fertility, alter the response to conventional treatment and assisted reproduction technology for infertility and have effects on pregnancy and the newborn.
The relevant eating disorders are bulimia nervosa (excessive eating and compensatory activities such as vomiting or laxative abuse) and anorexia nervosa (low body mass index (BMI) and fear of weight gain]. Both commonly onset in adolescence and occur in 3% of young women [23].
Milder eating disorders (not otherwise specified) occur in a further 3-5% of women [24]. Anorexia nervosa (1% of young women) is defined as body weight less than 85% of expected weight or BMI less than 17.5kg/m2, coupled with intense fear of weight gain and an inaccurate perception of body image. Bulimia nervosa (1⌝-5% of young women) involves recurrent binge eating, compensated by recurrent purging, excessive exercise or fasting, excessive concern about body weight or shape and the absence of anorexia nervosa [20]. Full recovery with bulimia nervosa is more likely (74%) than with anorexia nervosa (33%), but to achieve these recovery rates required a median of 90 months of follow-up with treatment and relapses occurred in about one third of full recoveries [25].
Effects on fertility
Menstrual periods often cease after a 10-15% decrease in normal body weight. In theory the mechanisms include altered regulation of gonadotropin-releasing hormone secretion and changes in the dopaminergic and opioid systems. Amenorrhoea occurs in 15-30% of women with anorexia nervosa [26,27]. Amenorrhoea is also a component of the female athletic triad, along with osteoporosis and milder versions of the eating disorders [28]. Oligoamenorrhoea may occur with bulimia nervosa even in women with BMI in the normal range. The amenorrhoea persisted in 30% of patients who had regained their normal weight during recovery from anorexia nervosa with amenorrhoea [29].
With respect to fertility, anorexia nervosa or bulimia nervosa was present in 5 (8%) of 66 consecutive infertility clinic patients; non-specified eating disorders were found in a further six (9%) [24]. Seven of the 11 women with eating disorders were among the 12 of 66 with oligoanovulation; thus, in this small group, eating disorders were present in about 60% of women with oligoanovulation. Although women with anovulation are unlikely to conceive, fertility may be normal in later years among women who achieve normal weight after recovery from eating disorders [28,30]. Women with a history of anorexia nervosa and community controls had similar rates of pregnancy, mean number of pregnancies per woman and age at first pregnancy [31]. After 11.5 years of follow-up in 173 women with bulimia nervosa, 75% had been pregnant at least once and only 2% reported that they were unable to conceive [32].
Effects on treatment for infertility
Under nutrition is not a reliable predictor of conception among infertile women. In 244 cycles of GnRH treatment for oligoamenorrhoea in 48 women, pregnancy rates were not affected by patients' weight or weight loss [33]. With assisted reproduction (ART) treatment, BMI was <20kg/m2 in 22% of 398 French women: the delivery rates per started cycle were 21% in underweight women and 15% in those with BMI 2025kg/m2 [34]. Among 2860 Norwegian women having ART, BMI was <18.5kg/m2 in 3%; the live birth rates per started cycle were 21%, both in underweight women and in those with BMI 18.5-25kg/m2 [35].
Effects on pregnancy
Women with a history of being anorexic may have more abortions: 27% in a cohort of 66 anorexics versus 13% in a control group [31]. In contrast, a larger follow-up study of 246 women with either anorexia or bulimia reported that 54 women had 82 pregnancies of which 46 (56%) were live births, 25 (31%) were therapeutic abortions and only 11 (13%) were spontaneous abortions [36].
During pregnancy, women with eating disorders have higher rates of hyperemesis gravidarum, anaemia, impaired weight gain and compromised intrauterine fetal growth [23,37]. Premature delivery is more likely in underweight women. A case control study found that BMI <20kg/m2 was associated with a four-fold higher likelihood of pre-term labour (OR=3.96, 95% CI=2.61- 7.09) after adjusting for other known factors [38]. Rates of cesarean delivery, post-natal complications and post-partum depression are higher among mothers with anorexia nervosa [31,39]. Under nutrition is associated with low birth weight (3233g compared with 3516g for normal controls) [37].
Factors associated with premature delivery [38]. OR, odds ratio; CI, confidence interval; body mass index Kg/m2 (standing at work >2h/day, stress score: arbitrary scale.
Among women with eating disorders, postponement of conception until remission is recommended because of the impact of low nutrition, but all pregnant women with past or current eating disorders should be viewed as being at high risk and should be monitored closely both during and after pregnancy to ensure optimal maternal and fetal outcomes [35]
Conclusion
While deprivation and under nutrition are major causes of disease and death in developing countries, eating disorders is more likely to interfere with reproduction in developed countries. Because preservation of female energy expenditure for reproduction is essential, appetite and the reproductive axis are closely linked to nutritional status. As a safeguard against untimely reproduction due to under nutrition, ovarian activity is suppressed in women with eating disorders and exercise amenorrhoea through pathways in the hindbrain. It is the balance between energy consumption and utilization that is crucial more than the body fat mass, thus recovery of ovulation may occur after a small percentage gain in weight [36-121].
The combined prevalence of bulimia nervosa and anorexia nervosa is approximately 5% among women of reproductive age, and the likelihood of cure is higher with bulimia nervosa. Both disorders suppress ovulation in severely affected women and account for up to 60% of women with anovulatory infertility. Pregnancy among underweight women increases the risk of premature labour.
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
https://juniperpublishers.business.site/
#gynecology#Contraception#Miscarriage#Nutrition#Obesity#Reproduction#ectopic pregnancy#open acess journals#osteoporosis
1 note
·
View note
Text
Can Intra Operative Radiotherapy Treatment for Breast Cancer Challenge the Medical Cost?

Authored by Maha Abdel Hadi*
Mini Review
Concerns over the global increase of breast cancer burden coupled with the long term high cost incurred by the treatment of advanced disease and palliative care renders many women with suboptimal management especially in developing countries and countries of limited resources.
Emerging alarming reports indicate that 57% of cancer cases occur in low and middle income countries. 50%-90% of these underprivileged patients requiring radiotherapy are deprived from access to radiation facilities limiting the surgical options to liberal adoption of mastectomies. This is one of the mean reasons that deters women from seeking early medical advise [1]. The late presentation of the young women in their reproductive age is both disturbing and disruptive. Partial treatment contributes to advanced disease for potentially treatable cases [2].
The scarcity of breast cancer awareness programs coupled with the young age and delayed presentation further compounds the problem. These programs consist of poorly attended didactic lectures focused on early detection with no details on management [3,4].
The costs for cancer treatment are prohibitive, in the economically challenged developing countries many are deprived from cancer care. In the United States as the estimated costs of breast cancer treatment range from $US20 000 to $US100 000. Similar costs have been reported from the United Kingdom and other developed countries [5].
Early diagnosis of breast cancer management impacts positively on the overall costs as compared to advanced disease and palliative care [6].
Radiotherapy remains an integral adjuvant component in the treatment of segmental breast resections, yet, the number of Radiation Oncology centers and their geographical distribution is alarming. The underprivileged developing world takes the brunt of its inability to provide adequate centers to overcome the disease burden. Worldwide is scarce and mainly clustered in developed countries [7,8].
The introduction of this modern modality as an exclusive treatment or boost therapy for breast cancer is a breakthrough. It expected to provide a practical solution since it has proven to be a convenient and an efficient method of therapy suitable for conventional operating rooms.
It may aid to encourage early presentation in a subset of women who would resist disclosure and refuse treatment because of the limited surgical options . It may also encourage oncologists to utilize the option of Neo- adjuvant chemotherapy in order to propagate breast conserving surgery.
Conclusion
While developing countries and countries with limited resources remain disadvantaged by the scarcity of radiotherapy centers, IORT may offer an alternative solution for a selected subset of women with breast cancer. In addition, its introduction may have a positive impact on the early detection.
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
https://juniperpublishers.business.site/
#gynecology#open acess journals#reproductive health#openacess publishers#womens health#breastfeeding#breast#sex#pregnency
0 notes
Text
Low Cost Cervical Cancer Screening in Poor Resource Settings

Authored by Nandini Manoli*
Abstract
Cervical cancer (CC) is the fourth most common cancer in women, and the seventh overall, with an estimated 528,000 new cases in 2012 Although the annual number of cases has increased, cancer of the cervix has declined in relative importance: it was the second most common cancer of women in 1975. In addition, the incidence and mortality of CC is variable within low- and middle-income countries (LMIC). In India, there are 20.2 per 100000 new cases of CC diagnosed and 11.1 per 100000 deaths annually, accounting for more than one fifth of the global CC deaths. In sub-Saharan Africa, 34.8 per 100000 women are diagnosed with CC annually and 22.5 per 100000 women die from this disease. Therefore, various cost effective methods are required besides conventional pap smear screening to detect cervical cancer in low resource settings. Various other methods are being introduced in low and middle income countries (LMIC) to improve detection at low cost. The tests discussed are manual liquid based cytology (MLBC), HPV testing, cell block with marker study, and visual inspection by ascitick acid(vIA).The various methods should be implimented by national screening programs in LMIC countries.
Introduction
Cancer of the cervix uteri. Cervical cancer is the fourth most common cancer in women, and the seventh overall, with an estimated 528,000 new cases in 2012. Although the annual number of cases has increased, cancer of the cervix has declined in relative importance: it was the second most common cancer of women in 1975. As with liver cancer, a large majority (around 85%) of the global burden occurs in the less developed regions, where it accounts for almost 12% of all female cancers High- risk regions, with estimated ASRs over 30 per 100,000, include Eastern Africa (42.7), Mela-nesia (33.3), Southern (31.5) and Middle Africa (30.6). Rates are lowest in Australia/New Zealand (5.5) and Western Asia (4.4). Cervical cancer remains the most common cancer in women in Eastern and Middle Africa. There were an estimated 266,000 deaths from cervical cancer worldwide in 2012, accounting for 7.5% of all female cancer deaths Almost nine in 10 (87%) cervical cancer deaths occur in less developed regions .The average risk of dying from cervical cancer before age 75 is three times higher in the less than in more developed regions Mortality varies 18-fold between the different regions of the world, ranging from less than 2 per 100,000 in Western Asia, Western Europe and Australia/New Zealand to above 20 per 100,000 in Melanesia (20.6), Middle (22.2) and Eastern (27.6) Africa [1,2].
In addition, the incidence and mortality of CC is variable within low- and middle-income countries (LMIC). In India, there are 20.2 per 100000 new cases of CC diagnosed and 11.1 per 100000 deaths annually, accounting for more than one fifth of the global CC deaths. In sub-Saharan Africa, 34.8 per 100000 women are diagnosed with CC annually and 22.5 per 100000 women die from this disease. In contrast, in western Asian countries, only 3.8 per 100000 new cases are diagnosed per year and 1.6 per 100000 die from CC. Therefore, if the chances to survive CC are considered, a woman in Thailand will have an approximately 58% chance of survival, while in India she will only have a 42% chance. This survival is even more critical in Sub-Saharan Africa, where women only have a 21% chance to survive CC. Overall, the mortality to incidence ratio of CC is 52%, 2.
The requisites for cervical screening
It is imperative by looking at the incidence and mortality rates of cervical cancer CC in developing countries (LMIC),. an effective screening procedure is followed. An ideal screening test is one that is minimally invasive, easy to perform, acceptable to the subject, cost-effective and efficacious in diagnosing the disease process in its preinvasive or early invasive state [3].
About conventional pap smear (CPS)
From following its introduction by Papanicolau in 1927 exfoliative cervicovaginal cytology has been extensively investigated and used as a screening test for cervical cancer [4]. The standard technique for Pap smear collection is to sample the portio vaginalis of the cervix and the endo cervical canal using a cervical spatula and endocervical brush. The collected sample is smeared on a slide and then fixed immediately with cytology fixative. Most clinicians are concerned with reducing sampling errors by focusing on the technic of smear acquisition and eliminating drying artifacts through rapid fixation [3].
Its limitations in low resource settings
a) Incorrect and inadequate sampling in 5-10% of cases [5].
b) Only up to 20% of harvested cells are transferred on the slide leading to a reduction in the sensitivity of the test [5].
c) Mean sensitivity of only 55-60% [6].
d) Reported false negative rates varying from 25 to 50%[7] .
e) Reported false positive rates varying from 15 to 20 %[8] .
f) Inter observer variation in the interpretation of cytological abnormality making reporting subjective and poorly reproducible [9].
Methods to overcome these limitations
Other Screening tests for cervical carcinoma include
Fluid sampling techniques with automated thin layer preparation (liquid based cytology)
Automated cervical screening techniques
Neuro medical systems
HPV testing
Polar probe
Laser induced fluorescence
Visual inspection of cervix after applying Lugol's iodine (VILI) or acetic acid (VIA).
Speculoscopy
Cervicography [10]
Some of the other methods besides CPS are being implemented in various centers especially the higher diagnostic centers reaching out to urban population of women who are economically more independent, educated aware of health issues. Of these fluid cytology has made a beginning.
Liquid based cytology-types
Recently liquid based cytological technologies have been developed and have gained popularity because in preliminary studies the use of such techniques was associated with a reduction in the incidence of inadequate cervical smears [11,12]. Two such technique that have been extensively tested are Thin Prep (Cytyc Corp, Boxborough, MA) and Autocyte (Tri Path Imaging, Burlington, NC). These fluid sampling devices have been approved by the USFDA. Automated liquid based cytology (LBC) have made entry in developing countries like India. Semi automated methods within house methodology are being introduced in various centers.
Manual liquid based cytology
On the other hand, Manual Liquid Based Cytology (MLBC) is a technique that enables cells to be suspended in a monolayer and thus improves detection of precursor lesions and improvement of specimen adequacy. MLBC has been reported to improve the effectiveness of cervical cancer screening in a population by increasing the detection of histologically confirmed neoplastic and preneoplastic disease while simultaneously decreasing over diagnosis of benign processes. Also, in case of MLBC, the residual sample can be used for other tests like detection of HPV DNA, immunocyto chemistry on cell block thereby increasing the utility of MLBC.
HPV methods
Several studies support that HPV testing is feasible in low- resource settings and appears to be the best strategy for CC in this context A large-cluster randomised trial from rural India showed that a single round of HPV screening could reduce the incidence and mortality from CC of approximately 50%, whereas approaches based on VIA and cytology had little effect on these outcomes. Until recently, the greatest limitations of HPV testing were the need for expensive laboratory infrastructure and the 4-7 h time to process the test. The development of rapid molecular methods for detecting HPV DNA screening (eg care HPV, qiagen, genexpert-cepheid) or other POC type of tests is a milestone in CC screening in low-resource settings. This is because these new options may make screening more feasible in the future and reduce the infrastructural requirements of previous screening programmes [13,14]
Human papillomavirus (HPV) detection by PCR in our setup
Polymerase chain reaction (PCR) was used to detect the presence of HPV in the extracted DNA. PCR was done at two levels: First a pair of consensus primers such as MY09/11 and GP5+/GP6+ amplifying a 450bp and 150bp length of L1 region respectively was employed in the reaction and then the positive samples were subjected to type specific PCR to detect the most common high risk HPV subtypes like HPV-16 and HPV-18. A brief master mix was prepared containing 2U/μL of Taq ploymerase (Himedia), 2μM of dNTPs, 10x buffer with 25mm MgCl2 (working =1x buffer) and 0.2μM of each of forward and reverse primers. DNA concentration ranging from 50-80ng/reaction was added and the total reaction was made upto 30μL using PCR grade water. Amplification was performed in the Mastercycler gradient (Eppendorf) at 95°C for 5min, followed by 32 cycles of 94°C for 1min, 60°C for 45sec, 72°C for 1min and a final extension of 72°C for 2min. GAPDH gene was used as internal control to check the adequacy of PCR reaction and DNA from HeLa cell line and Siha cell line was used as positive control for HPV-18 and HPV- 16 respectively, while water was used as negative control. The amplified PCR products were elecrophoresized on 2% agarose gel with a 100bp ladder (Himedia). Our current PCR set-up gives rapid, type-specific HPV detection with a turnaround time of less than 24hrs and cost-effectiveness compare to commercial avilable alternatives. Nevertheless, type-specific HPV testing is valuable to check the burden of HPV infections epidemiologically. Therefore, it can be considered as an indispensable tool to detect HPV types. It has to be developed further so as to be used as a primary screening method as national programme for hpv detection at low cost in a poor resource country like India.
Cell block and P-16 biomarker
Cell blocks can be prepared from all types of cytological specimens, except preparations with low cellularity such as cerebrospinal fluids. There are several techniques to produce cell blocks, such as cyto centrifugation, either with direct formalin fixation or fixation after addition of plasma-thromboplastin. Cell blocks perform in a highly reproducible way when stained with most antibodies, except for some used in the work- up of lymphoid lesions. One distinct advantage of cell blocks is that many slides can be prepared for extensive panels of immunostains. In addition, the quality control of cell block staining is identical to that of histopathology. The morphology of cell blocks is identical to that seen in histological specimens and therefore familiar to most pathologists. Cell blocks closely resemble Formalin- Fixed Paraffin-Embedded sections and can be stained using methods already established in general immunohistochemical laboratories, which probably explains their providing the best quality of imunocytochemical reactions.
The increased sensitivity of cell blocks in the diagnosis of malignant conditions of cervix may be due to better preservation of cytomorphologic features, better staining characteristics of the nucleus, nucleoli, and cytoplasm, clear recognition of nuclear and cytoplasmic features [15-17].
The oncogenic activity of E7 protein may also be tested indirectly by the host cyclin-dependent kinase inhibitor p16Ink4a. This kinase inhibitor decelerates the cell cycle by inactivating the cyclin-dependent kinases (CDK4/CDK6) involved in retinoblastoma protein phosphorylation. Over expression of p16INK4a in almost all cervical pre cancer (High- grade lesions) and invasive CC has been shown to be directly linked to the transforming activity of E7 oncoprotein, which is produced by HPV. Cellular accumulation of p16INK4a can be measured by cytochemistry on cell blocks. LBC, direct smears and cervical biopsies. other useful marker studied is ki67. As a combination with p16INK4a [18,19].
Visual inspection with acetic acid (VIA)
Visual inspection tests with 3%-5% acetic acid (VIA) and/ or Lugol's iodine (VILI) appear to be a satisfactory alternative screening approach to cytology. These tests have been used since the 1990s, mainly in poor resource settings. They are simple, cost-effective with relative ease of use, and may be performed by different healthcare workers (physicians, nurse, midwives and technicians). Moreover, this approach does not require high technology or infrastructure and has been shown to reduce mortality in developing countries. The visible changes that occur in the cervix after application of acetic acid are immediate, and can be categorized as negative or positive for cervical neoplasia. These immediate results facilitate a same-day screen and management strategy. Therefore, this allows most of the eligible women to participate in the programme by minimizing repeat visits. Evidence shows that this single-visit approach leads to the most significant decrease in high-grade cervical intraepithelial neoplasia (CIN) and it is regarded safe, acceptable and fairly effective in India and Sub-Saharan Africa. Despite the limitations of the concept of "screen and treat”, it helps to overcome barriers of time, distance and loss to follow-up. [20,21]. In our set up we work with an NGO who regularly check the rural women population of our district by VIA .all VIA cases where the squamocolumnar junction is inadequate are subject to pap smear screening.
The future of cervical cancer detection in low resource settings
The future of cervical cancer detection has many problems to be tackled even though attempts are being made to improve health care in low to middle income countries (LMIC). The factors which require attention are creating more awareness among rural population, national health programmes which include pap smear screening as mandatory in both urban and rural women with each having an health card as it happens in developed countries. Better training of health providers that includes primary health workers and doctors trained for this programmes.
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
https://juniperpublishers.business.site/
#gynecology#urogynecology#women's health#sex#menopause#endometriosis#Endometrial Biopsy#endometrial ablation#breastfeeding
0 notes
Text
Cervical Cancer: Ethiopia´s Outlook

Authored by Netsanet Abera Asseffa*
Abstract
Globally, cervical cancer accounted for an estimated 528,000 new cancer cases worldwide and for 266,000 deaths in 2012. In Ethiopia, 35.9 new cases of cervical cancer are diagnosed and 22.6 die from it, per 100,000 women annually.
There are many factors associated with cervical cancer in Ethiopia such as Human Papilloma Virus (HPV), cultural factors, Poverty, Co-infection and lack of awareness. Ethiopia has no standard policy or protocol for cervical cancer screening rather it is patchy or inconsistent. Ethiopian women typically present for cancer care at a late stage in the disease, where treatment is likely ineffective. To produce significant decrease in incidence and morality , barriers should be addressed as well research studies should be strengthened in the areas of cervical cancer.
Keywords: Cervical cancer; Screening; Outlook; Ethiopia
Introduction
Cancer begins from a single cell though its transformation into tumour cell is progressive [1]. Cervical cancer is a malignant neoplasm from cells originating in the cervix uteri [2]. A sexually transmitted virus called HPV is responsible for more than 99% of cervical cancer cases and its precursors [3]. Any woman who is sexually active is at risk of getting HPV. Globally, cervical cancer accounted for an estimated 528,000 new cancer cases worldwide and for 266,000 deaths in 2012. Although it occurs worldwide, but the highest incidence and mortality rates are found in low income countries, despite the fact that it is preventable [4]. In some developing countries cervical cancer kills more women than maternal mortality, for example in Chile, South Africa and Argentina [3].
Ethiopia is among the least urbanised countries in the world (84% of the population reside in rural area) [5]. It is the second most populous nation in Africa with about 44 million females [6]. There are nearly 26 million Ethiopian women who are over the age of 15 and believed to be at risk of getting HPV, the causative agent [7]. In Ethiopia, 35.9 new cases of cervical cancer are diagnosed and 22.6 die from it, per 100,000 women annually [8]. The objective of this review is to demonstrate Ethiopia's stand on incidence, mortality, factors associated, screening service and treatment of cervical cancer
Methods
Search strategies and inclusion criteria
The electronic databases Medline, PubMed, Ethiopia's medical and Reproductive health journals, and Bio MED central were searched for relevant articles. Inclusion criteria of the articles were:
Published during 2000-2015;
Quantitative or qualitative study;
Reported in English;
Related to Ethiopia, sub-Saharan Africa and published in peer-reviewed journals. The full texts of the potentially relevant articles were retrieved and data extraction were then undertaken.
Incidence and mortality
In sub-Saharan Africa, 34.8 new cases of cervical cancer are diagnosed per 100 000 women annually, and 22.5 per 100 000 women die from the disease [9]. Sub-Saharan Africa has 22% of all global cervical cancer cases [10]. In Ethiopia, it has been estimated that about 7,000 of new cervical cancer cases occur every year and about 5,000 die from it [11]. This figure could be low given that the nation has no cancer register centre as well cervical cancer screening and treatment service is either not available or inconsistent.
Factors associated with cervical cancer in Ethiopia
Human papilloma virus (HPV): It has been established that cervical malignancy is associated with HPV infection. The worldwide prevalence of infection with human papillomavirus (HPV) in women without cervical abnormalities is 11-12% with higher rates in sub-Saharan Africa (24%) [12]. In Ethiopia no data is available on burden of HPV infection, nevertheless about 35.8% of women in the general population are estimated to harbour cervical HPV infection at a given time in the Eastern Africa, the region Ethiopia belongs to [13].
Cultural factors: There are many cultural factors that contribute to the acquisition of HPV and its progression to cancer. This includes High parity, early marriage, multiple sexual partners, and diseases that reduce immunity status. High parity has long been suspected of being associated with an increased risk of cervical cancer. A study has found a direct association between the number of full-term pregnancies and squamous-cell cancer risk: the odds ratio for seven full-term pregnancies or more was 3.8 compared with nulliparous women and 2.3 compared with women who had one or two full-term pregnancies. They concluded that High parity increases the risk of squamous-cell carcinoma of the cervix among HPV-positive women [14]. An Ethiopian woman has 4.8 average numbers of children [15].
Early marriage is norm and commonly practiced in the northern part of the nation, has a link with development of cervical cancer. A study has found out that cervical cancer risk is closely linked to age at first birth; the odds ratio was highest among women who gave birth at age 16 or younger (4.4), and then ranged from 2.5 among those who initially delivered at ages 17-19 to about 2.2 among those who did so at age 20 or older [16]. According to EDHS 2011 and the median age at first marriage is 16.5 [15]. Polygamy is acceptable in some cultures in the country which increase the likelihood of getting HPV infection for the women.
The other factor is having multiple sexual partners which puts at risk of getting HPV as well sexually transmitted diseases. A hospital based cross-sectional study conducted in southern Ethiopia showed that life time number of sexual partners and history of sexually transmitted disease were found to be associated (on multivariate analysis at p-value less than 0.05) with precancerous cervical cancer lesion [17].
Co-infection: Cervical cancer was made an acquired immunodeficiency syndrome (AIDS-) defining illness in 1993. Pathfinder International Ethiopia estimated that about 534,000 HIV positive women are among the most vulnerable to develop cervical cancer [18]. A comparative cross-sectional study was conducted in northern Ethiopia which showed that 63.6% of HIV positive women were found to have cervical epithelialcell abnormality than there counterpart (HIV negative women). In the same study they concluded that those with HIV positive status were at greater risk of getting cervical cancer as compared to those with negative status [19].
Poverty: Poverty is endemic in the sub-Saharan Africa, the nation belongs to. A study that has found out a strong association between cervical cancer and the level of development, rates being at least four-fold higher in countries defined within the low ranking of the Human Development Index (HDI) compared with those in the very high category [12]. Cervical cancer is believed as the disease of the low socio-economic class.
Lack of awareness: Cervical cancer is nearly 100% preventable if it is detected early; however service accessibility and Women's awareness matters a lot. A recent qualitative study done in Ethiopia has shown that people believe that breaching taboo or undertaking unacceptable behaviour as aetiology of cervical cancer. The study concluded saying that there is very low level of awareness about cervical cancer. In the same qualitative study, participants from rural areas of Ethiopia neither know nor heard of cervical cancer. The sad news is that when women were briefed about signs and symptoms of cervical cancer many mentioned number of women who suffered from such symptoms and passed away without knowing what it was [20]. Moreover, a cross sectional study done among HIV positive women in the capital city of Ethiopia showed that only 1/3rd of participants knew about cervical cancer and most of their source were health professionals [21]. In most populous nation of Africa, personal barriers to screening include the lack of awareness, and belief that cervical cancer is not preventable [22].
Prevention and screening of cervical cancer
Detection of cancer at an early stage may be considered as a marker for access to health care and preventive health services, including cervical cancer screening. Both incidence and mortality can be reduced by detecting precancerous lesions then prompt treatment which can prevent its progression, thereby increasing patient survival.
Nevertheless, there are many barriers to establishing cervical cancer screening programs in Ethiopia. These include lack of trained professionals, the demands of conflicting health needs such as preventable communicable diseases, poorly developed health care services that tend to focus more on curative than preventive health care, and the fact that women are often uninformed as to their needs for preventive health care. Hence, cervical cancer is eclipsed by other health priorities.
It is worth mentioning that the success of screening programmes is determined by various factors such as good attendance rates by women at high risk, careful planning and execution of the program. Ethiopia has no standard policy or protocol for cervical cancer screening rather it is patchy or inconsistent [14].
Treatment of cervical cancer
Basically, non-physicians can perform the simple and affordable screening and treatment procedures such as Visual inspection with acetic acid to screen and cryotheraphy to treat, provided that they receive adequate and on-going training. Sadly, Ethiopian women typically present for cancer care at a late stage in the disease, where treatment is most ineffective [23]. In addition, public oncologic treatment is located only in the capital city, Addis Ababa, at Black Lion Hospital; the centre is believed to be the most crowded as it serve the whole nation and deals with all types of cancer treatment. Brachy therapy treatment is not available in Ethiopia [24].
Conclusion
In Ethiopia multiple factors contribute to the development of cervical cancer such as competing health interests, lack of awareness, unavailability of cervical cancer screening, treatment services and among others. Ethiopian mother are losing their lives from preventable disease. To produce significant decrease in incidence and mortality, barriers should be addressed, awareness should be created and there must be an effective screening and prevention services that facilitate early detection and treatment. Research studies should be conducted in the areas of cervical cancer to fill gaps in availability of information/ data.
Acknowledgement
I take this opportunity to sincerely acknowledge Professor A.O. Arwojolou, Professor of Obstetrics and Gynaecology, University of Ibadan, Nigeria for providing necessary assistance which buttressed me to perform my work comfortably. I am also indebted to thank Mr.TeferaTesfamicheal, Cervical Cancer Prevention Project South Regional Coordinator, CDC, for reviewing my work.
Competing Interests
I declare that I have no competing of interests.
For more open access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s Health please click on: https://juniperpublishers.com/jgwh/
To read more......Full text in Gynecology and Women’s Health in Juniper Publishers
https://juniperpublishers.business.site/
#reproductive health#gynecology#urogynecology#fertility#sex#women's health#Infertility#HPV infection#HPV genotype
0 notes