#polymastia
Text

Supernumerary Nipple flag 💪💪💪 💥🔥
meaning: it's modeled after the shape of the milk line which is where most supernumerary nipples form. Although they can form in other places as well. The colors are just various nipple colors.
#This is like 72% a joke#Supernumerary nipple#Third nipple#Polythelia#Polymastia#Pseudomamma#flags#my flags#Varsex#< technically#varisex
4 notes
·
View notes

Text
Polymastia Symptoms, Causes, Removal
Polymastia Symptoms, Causes, Removal
Polymastia, also known as supernumerary breast tissue, is a condition that occurs in people and is used to indicate having more than two breasts. This condition happens when something goes wrong in the early stages of breast tissue development. It usually does not cause any symptoms, but it often causes anxiety, problems with how you look, pain, or a limited range of motion.
It is sometimes…

View On WordPress
0 notes
Text

Introduction:
Axillary breast tissue, also known as accessory breast tissue or polymastia, is a condition in which additional breast tissue develops in the axillary (armpit) area. While usually benign, axillary breast tissue can cause physical discomfort, aesthetic concerns, and emotional distress for affected individuals. Axillary breast tissue removal, or axillary breast tissue excision, is a surgical procedure aimed at removing the excess breast tissue to improve comfort and cosmesis. In this comprehensive guide, we will explore the details of axillary breast tissue removal, including the procedure itself, recovery process, potential risks, and realistic expectations for patients.
Understanding Axillary Breast Tissue:
Axillary breast tissue is a common anatomical variation that occurs during embryonic development when mammary tissue extends beyond the normal breast area into the axillary region. This additional breast tissue can manifest as a lump or mass in the armpit area and may enlarge during hormonal changes, such as puberty, menstruation, pregnancy, or breastfeeding. While axillary breast tissue is typically non-cancerous and does not pose a significant health risk, it can cause discomfort, pain, irritation from clothing friction, and self-consciousness about appearance.
Indications for Axillary Breast Tissue Removal:
Axillary breast tissue removal may be recommended for individuals experiencing:
Physical discomfort or pain: Enlarged axillary breast tissue can cause discomfort, pain, and irritation, particularly during physical activities or when wearing tight clothing.
Aesthetic concerns: Some individuals may feel self-conscious about the appearance of enlarged axillary breast tissue, especially if it creates bulges or asymmetry in the armpit area.
Difficulty with hygiene: Excess breast tissue in the axillary region may make it challenging to maintain proper hygiene, leading to skin irritation, rashes, or infections.
Axillary Breast Tissue Removal Procedure:
Axillary breast tissue removal is typically performed as an outpatient surgical procedure and involves the following steps:
Pre-operative evaluation: Before undergoing axillary breast tissue removal, patients undergo a thorough medical evaluation and consultation with a board-certified plastic surgeon. The surgeon assesses the extent of axillary breast tissue enlargement, discusses the patient's goals and expectations, and explains the surgical technique and potential risks.
Anesthesia: Axillary breast tissue removal is usually performed under local anesthesia with sedation or general anesthesia, depending on the patient's preference and the surgeon's recommendation.
Incision placement: The surgeon makes an incision in the axillary area, strategically placed to minimize scarring and ensure optimal access to the excess breast tissue. The specific location and length of the incision may vary based on the amount of tissue to be removed and the patient's anatomy.
Tissue excision: Using surgical instruments, the surgeon carefully removes the excess breast tissue from the axillary area while preserving surrounding structures such as nerves and blood vessels. The goal is to achieve a smooth contour and natural transition between the breast and axillary regions.
Closure: Once the excess breast tissue has been excised, the incisions are meticulously closed with sutures or surgical adhesive. Sterile dressings may be applied to the surgical site to promote healing and reduce the risk of infection.
Post-operative care: After axillary breast tissue removal, patients are monitored in a recovery area before being discharged home with detailed post-operative instructions. These instructions may include guidelines for wound care, pain management, activity restrictions, and follow-up appointments with the surgeon.
Recovery and Post-Operative Care:
The recovery process following axillary breast tissue removal typically involves the following:
Initial recovery: In the days following surgery, patients may experience mild to moderate discomfort, swelling, bruising, and temporary numbness in the surgical area. Pain medication and cold compresses can help alleviate these symptoms.
Activity restrictions: Patients are advised to avoid strenuous activities, heavy lifting, and raising their arms above shoulder level for several weeks following surgery to facilitate proper healing and minimize strain on the surgical site.
Wound care: Patients should follow the surgeon's instructions for caring for the incision site, including keeping it clean and dry, changing dressings as needed, and avoiding soaking in water until cleared by the surgeon.
Compression garments: Wearing a compression garment or supportive bra may be recommended to minimize swelling, provide comfort, and support the surgical site during the healing process.
Follow-up appointments: Patients are scheduled for follow-up appointments with the surgeon to monitor their progress, remove sutures if necessary, and address any concerns or complications that may arise.
Long-term results: The final results of axillary breast tissue removal may take several weeks to months to fully manifest as swelling resolves and the surgical site heals. With proper care and adherence to post-operative instructions, patients can expect a smoother, more contoured axillary area and improved comfort and confidence in their appearance.
Potential Risks and Complications:
While axillary breast tissue removal is generally considered safe, like any surgical procedure, it carries potential risks and complications, including:
Bleeding and hematoma: Excessive bleeding during or after surgery, or the formation of a hematoma (collection of blood under the skin), may require additional treatment such as drainage or surgical intervention.
Infection: There is a risk of infection at the surgical site, which may manifest as redness, swelling, warmth, or drainage. Prompt medical attention and antibiotic treatment may be necessary to address infection.
Changes in sensation: Temporary or permanent changes in sensation, such as numbness, tingling, or hypersensitivity, may occur in the axillary area following surgery. Most sensory changes resolve over time but may persist in some cases.
Scarring: While efforts are made to minimize scarring, some visible scars may remain at the incision site. Scar management techniques such as silicone gel sheets or scar creams may help improve the appearance of scars over time.
Asymmetry or contour irregularities: Despite the surgeon's best efforts, asymmetry or contour irregularities in the axillary area may occur. Revision surgery may be necessary to address significant asymmetry or achieve optimal results.
Realistic Expectations:
It's essential for patients to have realistic expectations about the outcomes of axillary breast tissue removal. While the procedure can significantly improve comfort, aesthetics, and self-confidence by reducing excess breast tissue in the axillary area, it may not completely eliminate all symptoms or achieve perfection. Factors such as skin elasticity, tissue laxity, and individual healing responses can influence the final results. Additionally, patients should understand that surgical scars are an inevitable part of the healing process and may take time to fade and mature.
Conclusion:
Axillary breast tissue removal is a surgical procedure aimed at addressing excess breast tissue in the axillary area to improve comfort, aesthetics, and self-confidence for affected individuals. By understanding the procedure, recovery process, potential risks, and realistic expectations, patients can make informed decisions about undergoing axillary breast tissue removal. Consulting with a board-certified plastic surgeon who specializes in breast surgery is crucial for evaluating candidacy, discussing goals, and addressing any concerns or questions. With proper care and adherence to post-operative instructions, patients can achieve a smoother, more contoured axillary area and enjoy improved comfort and confidence in their appearance.
0 notes
Text
THE LONDON STAGE
• of Seatoun.... And thaireftir
• of polymastia and polythelia
• of George and Antoinette
0 notes
Text
Radiology about breasts: breast embryology, histology and anatomy.
Embryology:
the embryology of the breast shows that the ectoderm and the mesenchyme are responsible for the genesis of the male and female breast, with the ectoderm responsible for the formation of the ducts and alveoli and the mesenchyme responsible for the connective tissue and its vessels. The milk ridge develops in the ventral area of the body, and the pectoral part of the milk ridge produces the right and left mammary. Very little is known about the molecular mechanisms that initiate breast formation. The chronology of breast development is discussed through its developmental and differentiation phases. Developmental anomalies can occur, such as bilateral amastia, unilateral amastia, and bilateral amastia with congenital ectodermal defects, athelia, polythelia, polymastia, and breast asymmetry. The anatomy of the breast is described.
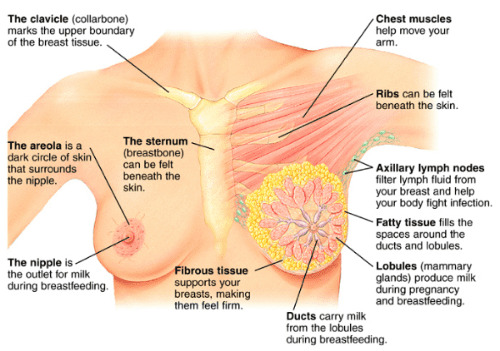
Anatomy:
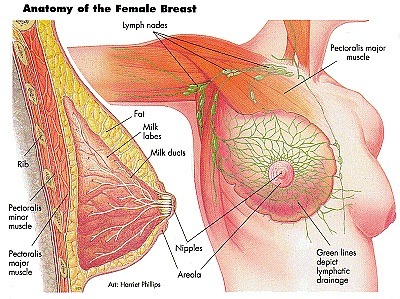
female breasts contain different types of fatty, fibrous, and glandular tissue:
- glandular tissue includes the breast lobes and breast ducts
- fibrous, or supportive or connective, tissue is the same tissue that ligaments and scar tissue are made of
- fatty tissue fills in the spaces between glandular and fibrous tissue and largely determines your breast size
Doctors refer to all non-fatty tissue as fibroglandular tissue. There are also bands of supportive, flexible connective tissue called ligaments, which stretch from the skin to the chest wall to hold the breast tissue in place. Muscle plays an important role too. The pectoral muscle lies against the chest wall underneath both breasts, giving them support. Blood vessels provide oxygen to the breast tissue and carry away waste.
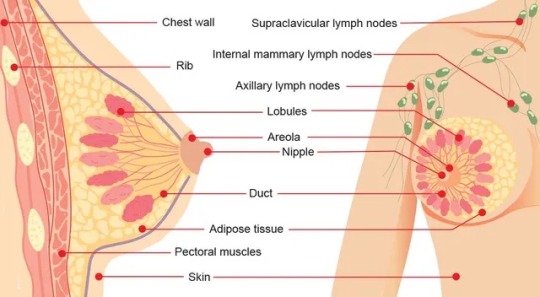
Histology:
Each lobule consists of a large number of alveolar glands, which are the small sac-like structures that produce milk.
The milk produced by the alveolar glands drain into the terminal ducts that join together to form the intralobular ducts.
These ducts converge further and form the lactiferous ducts, which drain the lobes and eventually lead to the nipple.
All of the lobules and ducts are also surrounded by fibro-fatty tissue that provide a supportive and protective function.
Before pregnancy, the mammary glands are considered to be in an inactive state, and they’re structurally different from mammary glands that are in the active state.
The active state occurs during pregnancy and during lactation after childbirth.
During pregnancy, the alveolar glands and the duct system will grow in preparation to produce milk for a newborn baby.
This low power image is an example of lactating mammary glands in the active state.
A portion of a lobe can be seen surrounded by a thick layer of connective tissue that contains a small number of fat cells or adipocytes within the connective tissue as well.
Within the lobe, thinner layers of connective tissue separate the lobe into lobules.
In a neighboring lobe, we can also see a couple of large lactiferous ducts.
These ducts are lined with a double layer of columnar or cuboidal cells with a surrounding layer of connective tissue.
1 note
·
View note
Text
Axillary Breast Tissue
Axillary Breast Tissue
Axillary Breast Tissue
Axillary Breast Tissue Axillary breast tissue is a type of tissue that can develop in the armpit area. This tissue is similar to breast tissue and can cause breast development, pain, and other symptoms. Axillary breast tissue is not cancerous and does not increase the risk for breast cancer. Treatment for axillary breast tissue is typically surgery to remove the tissue.
What is Axillary Breast Tissue?
There is a condition that can affect both men and women called axillary breast tissue. This is when there is a buildup of breast tissue in the armpit area. It is not cancerous and is not harmful, but it can be uncomfortable and cause pain. There are a few things that can cause this condition, such as hormonal imbalances, certain medications, and obesity. If you think you might have axillary breast tissue, it’s important to see a doctor so they can determine if that’s the case and come up with a treatment plan. What are Axillary Breast Tissue Damages? What are Axillary Breast Tissue Damages? Most often, axillary breast tissue damages are the result of an injury or surgery to the area. However, radiation therapy and certain cancer treatments can also cause damage to the tissue. Symptoms of axillary breast tissue damage include pain, swelling, and numbness in the affected area. Treatment for axillary breast tissue damage depends on the severity of the damage and may include medications, physical therapy, or surgery.
About Axillary Breast Tissue Disease
Axillary breast tissue is a condition that affects the breast tissue in the armpit area. This condition is also known as accessory breast tissue, polymastia, or supernumerary br
east. Axillary breast tissue is harmless and does not increase the risk of breast cancer. However, some women may experience pain, discomfort, or embarrassment due to the appearance of this condition. Treatment is typically not necessary unless the axillary breast tissue is causing problems.
0 notes
Text
Bilateral Accessory Breast: A Case Report from Nepal-Juniper publishers
Introduction
Accessory or ectopic breast tissue is residual breast tissue that persists after normal embryonic mammary development. It can occur anywhere along the embryonic mammary streak, but is most commonly located in the axilla. Accessory breast tissue can consist of any component of the breast and may be functional or non-functional and its development is hormone dependent like normal breasts. Overall, the prevalence of accessory breast tissue in women ranges from 0.4% to 6%, and in men, from 1% to 3% [1]. Usually they are asymptomatic and do not need any intervention unless they start causing discomfort. Diagnosis of accessory breast tissue is important because they are subject to all diseases of the breast including carcinomas [2]. Here we report a case of asymptomatic accessory breast tissue in bilateral chest wall of a 32-year Nepalese multi Para female patient.
Case Description
A 32-year-old multi Para woman presented with swelling over bilateral lower chest. Physical examination revealed two 5 X 5cm each sized lobular, soft, non-tender, diffuse masses in bilateral lower chest wall over 8th costal cartilage in the mid clavicular line. The overlying skin had a 1cm pigmented center each which was the nipple-areola complex. The mass was not adherent to the underlying structures and was separate from both breasts. There was no discharge from the masses or the breasts. Both breasts were clinically normal and there was no enlargement of axillary, cervical, supraclavicular lymph nodes (Figure 1). She had no other medical problems, no past history or family history of cancer. Routine blood examinations were within normal limits. Ultrasonography of these masses showed ectopic breast tissue with normal ultrasound of the abdomen, breast and axilla.
On questioning she does not recall any problems or symptoms arising from these masses during the pubertal or pregnancy period. This is a case of asymptomatic bilateral accessory or ectopic breast tissue.
Discussion
Accessory breast tissue, ectopic breast tissue, supernumerary breasts, aberrant breast, polymastia are the different terms used interchangeably. Higher incidence of accessory breast tissue is recorded in Asian population, especially in the Japanese, and twice as common in females than in males [3]. Various forms of accessory breast tissue was first described by Kajava [4] in 1915 into eight groups, but this classification has been further simplified as polymastia, polythelia and aberrant breast tissue.
Class I: complete breast including glandular tissue, nipple, and areola.
Class II: glandular tissue and nipple, without areola.
Class III: glandular tissue and areola, without nipple.
Class IV: glandular tissue only.
Class V (pseudomamma): nipple and areola, without glandular tissue.
Class VI (polythelia): the nipple only.
Class VII (polythelia areolaris): the areola only.
Class VIII (polythelia pilosa): hair only.
Polymastia is breast tissue containing glands and duct system communicating with overlying skin. Polythelia is presence of accessory nipples or areole or represented by tuft of hair. Aberrant breast tissue is presence of disorganized secretory glandular tissue not related to skin [5]. Accessory breast tissue is usually misdiagnosed and the women are at times unaware until examined thoroughly by an expert. The differential diagnosis includes lipoma, lymphadenopathy, sebaceous cyst, abscess, hidradenitis suppurativa, follicular cyst among others. Accessory breast tissue is usually asymptomatic and presents with a further diagnostic dilemma in the absence of nipple and areola.
Standard mammograms do not usually show accessory breast tissue, because of its location. Ultrasonography can be of help in the diagnosis of this condition. Fine-needle aspiration is a sensitive in evaluating these masses [6]. Tissue diagnosis obviously is gold standard for confirmation of accessory breast tissue. The typical lobules, stroma and duct may be poorly organized in ectopic breast tissue.
The main complaints at presentation are cyclical enlargement, tenderness, discomfort, pain, milk secretion, and local skin irritation, while psychological embarrassment seems to be the main cause for surgical removal [7]. Accessory breast tissue can develop all disease components of ANDI (aberrations of normal development and involution) that affect the normal breast like abscess, mastitis, milk fistula, cyclical mastalgia, cysts, fibroadenoma, fibroadenosis, hamartomas, phyllodes tumors and carcinoma [8]. The incidence of carcinoma in axillary breast is 0.2% to 6% which is higher than in normal breasts. The increased incidence of carcinoma in accessory axillary breast is attributed to stagnation in the ducts hence infiltrating duct carcinoma is the commonest variant [9].
In asymptomatic patients the management is conservative in most cases of accessory breast tissue through regular followup [10]. In symptomatic patients accessory breast tissue can be removed by excision, liposuction, or both with satisfactory outcomes [11]. The commonly reported complications after removal of accessory axillary breast are incomplete removal of the ectopic breast, poor scar, intercostobrachial nerve injury and lymph edema of arm [7].
Conclusion
Accessory breast tissue is a not an uncommon condition and should be considered as a differential diagnosis by a clinician when appropriate. It can persist as a cause of anxiety among women for fear of a malignant change in it. Such patients should be evaluated completely along with their presenting complaints, past history and family history, general physical examination including breast and axilla and the swelling(s), and this entity must be investigated by radiological and fine needle aspiration cytology and biopsy when required.
To know more about Journal of Head Neck please click on :
https://juniperpublishers.com/jhnss/index.php
To know more about Open access Journals Publishers please click on : Juniper Publishers
0 notes
Photo

And now: The aggregated nipple sponge! Polymastia pachymastia is a common critter of current-swept reefs of the North-East Pacific. They filter microscopic food particles from the wooshing water, like separating wheat from chafe—sorry, chaff.
501 notes
·
View notes
Text
1. What is your favourite kind of "-cide" (e.g., suicide, homicide, matricide, genocide..etc)?
Wtf...
2. Do you prefer soupy noodles or noodles without the broth?
Ya’ll should know by now I love my ramen. I like pasta as well, which as Lane pointed out, is noodles without with broth.
3. Do you listen to Sublime? What's your favourite song of theirs?
I only know Santeria, What I Got, and Take It or Leave It (by Sublime with Rome, but that still counts), all of which I like, but haven’t listened to in a long time.
4. Don't you hate it when you comment/message someone a question and you know they've read it but they don't reply?
Well, I’m not always one to answer right away so I’m understanding and assume they’ll probably answer when they get the chance. Especially if it’s not anything important. If it’s something clearly imporant/urgent; though, then yeah that wouldn’t be cool.
5. Do you have a virus scanner installed on your computer?
Macs already come with all that stuff.
6. Do you think a pretty person with ugly teeth can ruin their appearance?
They can still be pretty. I, on the other hand, am ugly and super self-conscious about my smile, so I got nothin’.
7. What's up?
It’s almost 730AM, but unsurprisingly here I am taking surveys and listening to ASMR when I should have been asleep hours ago. But that just wouldn’t be me would it?
8. Have you ever missed someone but felt like they had other friends and didn't miss you as much as you did?
I always felt that way with friends and even my cousins I was close to growing up. Like, I just felt like I was closer to them than they were to me and I cared more and missed them more. I didn’t feel like people missed me, I’m not anything special. I felt and still feel very replaceable.
9. Are you pretty good at small talk/conversing with aquaintances?
Nooo.
10. Who, out of all your friends, do you hang with the most and could never get tired of him/her?
I don’t have any friends.
11. What was the last bet you made between a friend? Who won?
I don’t remember. I don’t tend to do that. <<<
12. Do you like the taste of white chocolate or does it taste kind of fake?
I love white chocolate and I don’t care if it’s not real chocolate. Fight me.
13. Are you an automaton?
I feel robotic.
14. How would you react if you just found out your mom had an abortion before?
It would come as a surprise.
15. Are your pets spayed/neutured?
Yes, my doggo was spayed before we could bring her home from the adoption shelter.
16. Don't you hate it when myspace goes under maintenance all the time?
I don’t recall it going under maintenance a lot, but the Myspace days were over 10 years ago now, so *shrug*
17. Do you have polymastia (only the cool kids have been diagnosed with it)?
No.
18. Here's a good one: Do you know anybody who has a third nipple?
It’s possible *shrug*
19. Ever seen a guy wear a kilt before?
Not in person.
20. Hottest guy you know and actually talk to?
There aren’t any guys in my life currently (outside of family), so no one.
21. Do you wear jeans that are boot cut, straight leg, flared, or what?
Skinny jeans.
22. Are you expert at photoshop?
Not even close. I messed around with it in the past and could make gifs (not super great, though) and edit photos, but that’s the extent of it.
23. Where do you buy your shoes?
The last several pairs have been from the Adidas website.
24. Have you ever seen the movie Selena, about the Mexican-American pop star?
Yeah, several times.
25. When was the last time you had carrot cake?
Ew, carrot cake is disgusting.
26. Do you make sweet vids on your camera with your friends?
27. Have you even been to the Space Needle?
No.
28. Can you sing the Pebtol Bismol commercial jingle?
lol, yeah.
29. Do you know any teenager guys who talk in a semi-high voice like they haven't even reached puberty yet?
I don’t know any teenage boys, and I’m totally okay with that. <<< lol same.
30. Are you feeling pretty complacent at the moment?
No.
4 notes
·
View notes

Text
Glandular Polymastia
Glandular polymastia, or accessory breast tissue:Is defined as an isolated parenchymal mass:Without a nipple-areolar complexThe tissue is present:From birthUsually becomes symptomatic under the influence of hormones during:PubertyPregnancyLactationThis condition occurs in 2% to 6% of women and 1% to 3% of menCommon symptoms are:SwellingDiscomfortRestricted movementCosmetic deformitySymptoms…
View On WordPress
0 notes
Text
An opportunity to be involved in luxurious sexuality is coming
- words e.g i denied my baptism i forsook god and christ ils renient dieu la vierge et le reste vne renonciation expresse a iesu christ & a la foy but occasionally the words are given in full
- they would have perswaded this informer to have taken a lease of three score yeares or upwards.'[267] in new england some of the afflicted said of goodwife c that she had covenanted with the devil for ten years six of them were gone and four more to come'.[268] in modern france the belief in the contract for a term of years is recorded but nothing
- encores s'est il verifiac par plusieurs procez que l'obligation reciproque entre le diable & le sorcier contient quelquesfois le terme d'vn an deux ans ou autre temps.'[260] at faversham in 1645 joan williford said that the devil promised to be her servant about twenty yeeres and that the time is now
- delrio tells us that the devil useth to baptize them of new and to wipe off their brow the old baptism and our witches confess always the giving them new names the devil's mark useth to be a great article with us but it is not per se
- anne chattox said that mother demdike introduced her to the devil in mother demdike's own house
- league is made verbally if the party
- paction useth the words or signs which sorcerers use knowing them to be such renouncing of baptism is by delrio
- near approach to the ceremony of baptism is the blood rite
- elspet alexander of the same coven was also marked on the shoulder four weeks later the divill straiked hir shoulder with his fingers and after that shoe hade ease in the place formerly niped by the devill'.[292] the witch girls at lille in 1661 stated that le diable leur fait quelque marque comme avec une aleine de fer en quelque partie du corps'.[293] marie lamont of innerkip in 1662 confessed voluntarily that the devill nipit her upon the right syd qlk was very painful for a tym but yairefter he straikit it with his hand and healed it this she confesses to be his mark'.[294] in bute in 1662 margaret ncwilliam was tryed for the merk there was 3 merks fund one up her left leg next hard be the shine bone another betwixt her shoulders a 3aº ane uthyr up her hensh blew kat moore was tried and it was found undernethe her richt shoulder a little whyt unsensible spott'.[295] the somerset witches in 1664 were marked on the fingers it was stated of elizabeth style that the devil prickt the fourth finger of hir right hand between the middle and upper joynt where the sign at the examination remained of alice duke that the devil prickt the fourth finger of her right hand between the middle and upper joynt where the mark is yet to be seen and of christian green
- evidence five facts are clear
- view is supported by the fact
- solemnity confest by our witches is the putting
- meaner proselytes the devil fixes in some secret part of their bodies a mark as his seal to know his own by which is like a flea bite
- item confesses that she made a covenant with him and he promised that she wold not want meines eneugh and she promised to serve him and that he gave her a new name saying i baptise the mary.'[274]ajonet morisoune traysted with the divill at the knockanrioch being the second tyme of her meeting with him that shee made covenant with the devill quairin she promised to be his servant etc that shee asked quhat was his name his answer was my name is klareanough
- cases of polymastia or supernumerary breasts and of polythelia or supernumerary nipples are constantly recorded by modern medical observers
- local anaesthesia is vouched for in much of the evidence
- relevancy of this crime the first article useth to be paction to serve the devil which is certainly relevant per se
- department of entre sambre et meuse the full method of entering on such a contract is known si vous voulez venir au bois avec moi vous verrez un homme venir
- records of the baptism of candidates are rare
- witches mark or devil's mark as it is indifferently called is one of the most important points
- it is quite possible
- effect of paction yet with us it is relevant per se
- diuell and hell fier the other is when they
- renunciation of previous errors of faith and the vows of fidelity to the new belief are part
- renunciation by the witches was explicit but the records are apt to pass it over
- addition paction with the devil is divided by lawyers
- tradition seems to be founded on fact but there is also a certain amount
- christian man for foure yeares togeather did sundry times come to this examinate and requested this examinate to giue him her soule and in the end this examinate was contented to giue him her sayd soule shee being then in her owne house in the forrest of pendle.'[240] the two statements are not inconsistent
- they went to search the woman none were visible one advised to lay them on their backs and keep open their mouths and they would appear and so they presently appeared in sight.'[317] alice huson of burton agnes yorks in 1664 stated that i have i confess a witch pap which is sucked by the unclean spirit'.[318] abre grinset
- women the supernumerary nipple is observed to increase at the time
- ceremonies had lost their significance to a far greater extent than in scotland and are described more shortly probably because they
- there is nothing
- it be confest by them that they got that mark with their own consent quo casu it is equivalent
- paction is performed either by a formal promise
- greatest number of cases recorded in one place is in essex
- alledg'd by a nip in any part of the body and it is blew.'[237
- a woman searched margaret moone] she found three long teates or bigges in her secret parts which seemed to have been lately sucked and that they were not like pyles for this informant knows well what they are having been troubled
- it is not clear
- mark is given them
- devil then present or by presenting a supplication to him or by giving the promise to a proxie or commissioner impowered by the devil for that effect which is used by some who dare not see himself
- sexes laid one hand on the crown of the head the other on the sole of the foot and dedicated all that was between the two hands to the service of the master.[246] there is a slight variation
- new england only if the phenomena of polymastia and polythelia occurred in france and scotland there are no records
- delrio calls it stigma or character and alledges that it is sometimes like the impression
- mark is given to them
- lucy thompson had a lease of two and forty whereof two are yet to come and her lease
0 notes
Text
A woman developed a mass in her armpit after giving birth. Then it started lactating
https://sciencespies.com/humans/a-woman-developed-a-mass-in-her-armpit-after-giving-birth-then-it-started-lactating/
A woman developed a mass in her armpit after giving birth. Then it started lactating

Childbirth can trigger a number of odd body changes, but for a woman in Portugal, post-pregnancy symptoms were particularly curious: She started to lactate from her armpit, according to a new report.
The 26-year-old woman told doctors that she developed pain in her right armpit two days after giving birth, according to the report, published July 29 in The New England Journal of Medicine.
When doctors examined the area, they found a round mass in her armpit. Surprisingly, the mass “released a white discharge when pressed,” the authors, from Hospital de Santa Maria in Lisbon, Portugal, wrote in the report.
She was diagnosed with polymastia, or the presence of extra breast tissue in the body. Up to 6 percent of women are born with such “accessory” breast tissue, according to a 1999 paper published in the journal Mayo Clinic Proceedings.
In some cases, this extra breast tissue includes a nipple or areola (the pigmented area surrounding the nipple), but in other cases, the breast tissue alone is present, without nipples or areola, Live Science previously reported.
Related: Having a baby: Stages of pregnancy by trimester
The condition happens during fetal development, when the precursor cells to the mammary glands form along the “mammary ridge” or “milk line” that runs from the armpit to the groin on either side of the body, according to a 2014 paper in the American Journal of Roentgenology.
Milk from the underarm. (Marinho-Soares & Pulido-Valente, NEJM, 2021)
Usually, these ridges disappear everywhere except for the breast. But when this doesn’t happen, the body is left with residual breast tissue. The most common location for accessory breast tissue is the armpit (also called the “axilla”), according to the 2014 paper.
If the accessory breast tissue does not have a nipple or areola, people might not realize they have extra breast tissue until they become pregnant or start breast-feeding, according to the 1999 paper. At this point, milk “comes in” to the accessory breast tissue just as it does in typical breast tissue, and women may experience swelling or pain in the area.
Some women can even pump breast milk from the accessory breast tissue. In the 1999 paper, the authors describe the case of an 18-year-old woman with accessory breast tissue in the armpit who was able to successfully pump axillary breast tissue for eight weeks to relieve discomfort and continue breast-feeding.
In the Portugal woman’s case, she was reassured that the condition is benign. Doctors also told her that when undergoing routine breast cancer screening, the extra breast tissue would need to be examined for cancer just like typical breast tissue. It’s unclear if the woman was able to breast-feed or pump milk from the accessory tissue.
Related Content:
Mood swings & mommy brain: The emotional challenges of pregnancy
18 ways pregnancy may change your body forever
27 oddest medical cases
This article was originally published by Live Science. Read the original article here.
#Humans
#08-2021 Science News#2021 Science News#acts of science#Earth Environment#earth science#Environment and Nature#Nature Science#News Science Spies#Our Nature#planetary science#Science#Science Channel#science documentary#Science News#Science Spies#Science Spies News#Space Physics & Nature#Space Science#Humans
0 notes
Text
2051.
1. What is your favourite kind of “-cide” (e.g., suicide, homicide, matricide, genocide..etc)?
um wtf
2. Do you prefer soupy noodles or noodles without the broth?
soupy
3. Do you listen to Sublime? What’s your favourite song of theirs?
i do; doin time was always my fav
4. Don’t you hate it when you comment/message someone a question and you know they’ve read it but they don’t reply?
yeah
5. Do you have a virus scanner installed on your computer?
it’s built in
6. Do you think a pretty person with ugly teeth can ruin their appearance?
i mean....they’ll still be pretty
7. What’s up?
literally nothing. about to go to bed
8. Have you ever missed someone but felt like they had other friends and didn’t miss you as much as you did?
i’m sure i have
9. Are you pretty good at small talk/conversing with aquaintances?
no
10. Who, out of all your friends, do you hang with the most and could never get tired of him/her?
i don’t hang out with people
11. What was the last bet you made between a friend? Who won?
idk
12. Do you like the taste of white chocolate or does it taste kind of fake?
i like it.
13. Are you an automaton?
a what
14. How would you react if you just found out your mom had an abortion before?
i would be shocked and sad
15. Are your pets spayed/neutured?
yes
16. Don’t you hate it when myspace goes under maintenance all the time?
i’m sure i did
17. Do you have polymastia (only the cool kids have been diagnosed with it)?
what
18. Here’s a good one: Do you know anybody who has a third nipple?
i do
19. Ever seen a guy wear a kilt before?
no
20. Hottest guy you know and actually talk to?
my husband
21. Do you wear jeans that are boot cut, straight leg, flared, or what?
i don’t wear jeans
22. Are you expert at photoshop?
i’m not an expert but i’m okay at it
23. Where do you buy your shoes?
idk. i don’t really buy shoes
24. Have you ever seen the movie Selena, about the Mexican-American pop star?
no
25. When was the last time you had carrot cake?
idk
26. Do you make sweet vids on your camera with your friends?
no
27. Have you even been to the Space Needle?
No.
28. Can you sing the Pebtol Bismol commercial jingle?
yes
29. Do you know any teenager guys who talk in a semi-high voice like they haven’t even reached puberty yet?
no
30. Are you feeling pretty complacent at the moment?
no?
0 notes
Text
Juniper Publishers-Open Access Journal of Head Neck & Spine Surgery
Bilateral Accessory Breast: A Case Report from Nepal
Authored by Tuhin Shah
Introduction
Accessory or ectopic breast tissue is residual breast tissue that persists after normal embryonic mammary development. It can occur anywhere along the embryonic mammary streak, but is most commonly located in the axilla. Accessory breast tissue can consist of any component of the breast and may be functional or non-functional and its development is hormone dependent like normal breasts. Overall, the prevalence of accessory breast tissue in women ranges from 0.4% to 6%, and in men, from 1% to 3% [1]. Usually they are asymptomatic and do not need any intervention unless they start causing discomfort. Diagnosis of accessory breast tissue is important because they are subject to all diseases of the breast including carcinomas [2]. Here we report a case of asymptomatic accessory breast tissue in bilateral chest wall of a 32-year Nepalese multi Para female patient.
Case Description
A 32-year-old multi Para woman presented with swelling over bilateral lower chest. Physical examination revealed two 5 X 5cm each sized lobular, soft, non-tender, diffuse masses in bilateral lower chest wall over 8th costal cartilage in the mid clavicular line. The overlying skin had a 1cm pigmented center each which was the nipple-areola complex. The mass was not adherent to the underlying structures and was separate from both breasts. There was no discharge from the masses or the breasts. Both breasts were clinically normal and there was no enlargement of axillary, cervical, supraclavicular lymph nodes (Figure 1). She had no other medical problems, no past history or family history of cancer. Routine blood examinations were within normal limits. Ultrasonography of these masses showed ectopic breast tissue with normal ultrasound of the abdomen, breast and axilla.
On questioning she does not recall any problems or symptoms arising from these masses during the pubertal or pregnancy period. This is a case of asymptomatic bilateral accessory or ectopic breast tissue.
Discussion
Accessory breast tissue, ectopic breast tissue, supernumerary breasts, aberrant breast, polymastia are the different terms used interchangeably. Higher incidence of accessory breast tissue is recorded in Asian population, especially in the Japanese, and twice as common in females than in males [3]. Various forms of accessory breast tissue was first described by Kajava [4] in 1915 into eight groups, but this classification has been further simplified as polymastia, polythelia and aberrant breast tissue.
Class I: complete breast including glandular tissue, nipple, and areola.
Class II: glandular tissue and nipple, without areola.
Class III: glandular tissue and areola, without nipple.
Class IV: glandular tissue only.
Class V (pseudomamma): nipple and areola, without glandular tissue.
Class VI (polythelia): the nipple only.
Class VII (polythelia areolaris): the areola only.
Class VIII (polythelia pilosa): hair only.
Polymastia is breast tissue containing glands and duct system communicating with overlying skin. Polythelia is presence of accessory nipples or areole or represented by tuft of hair. Aberrant breast tissue is presence of disorganized secretory glandular tissue not related to skin [5]. Accessory breast tissue is usually misdiagnosed and the women are at times unaware until examined thoroughly by an expert. The differential diagnosis includes lipoma, lymphadenopathy, sebaceous cyst, abscess, hidradenitis suppurativa, follicular cyst among others. Accessory breast tissue is usually asymptomatic and presents with a further diagnostic dilemma in the absence of nipple and areola.
Standard mammograms do not usually show accessory breast tissue, because of its location. Ultrasonography can be of help in the diagnosis of this condition. Fine-needle aspiration is a sensitive in evaluating these masses [6]. Tissue diagnosis obviously is gold standard for confirmation of accessory breast tissue. The typical lobules, stroma and duct may be poorly organized in ectopic breast tissue.
The main complaints at presentation are cyclical enlargement, tenderness, discomfort, pain, milk secretion, and local skin irritation, while psychological embarrassment seems to be the main cause for surgical removal [7]. Accessory breast tissue can develop all disease components of ANDI (aberrations of normal development and involution) that affect the normal breast like abscess, mastitis, milk fistula, cyclical mastalgia, cysts, fibroadenoma, fibroadenosis, hamartomas, phyllodes tumors and carcinoma [8]. The incidence of carcinoma in axillary breast is 0.2% to 6% which is higher than in normal breasts. The increased incidence of carcinoma in accessory axillary breast is attributed to stagnation in the ducts hence infiltrating duct carcinoma is the commonest variant [9].
In asymptomatic patients the management is conservative in most cases of accessory breast tissue through regular followup [10]. In symptomatic patients accessory breast tissue can be removed by excision, liposuction, or both with satisfactory outcomes [11]. The commonly reported complications after removal of accessory axillary breast are incomplete removal of the ectopic breast, poor scar, intercostobrachial nerve injury and lymph edema of arm [7].
Conclusion
Accessory breast tissue is a not an uncommon condition and should be considered as a differential diagnosis by a clinician when appropriate. It can persist as a cause of anxiety among women for fear of a malignant change in it. Such patients should be evaluated completely along with their presenting complaints, past history and family history, general physical examination including breast and axilla and the swelling(s), and this entity must be investigated by radiological and fine needle aspiration cytology and biopsy when required.
For more articles in Open access Journal of Head Neck & Spine Surgery | Please click on: https://juniperpublishers.com/jhnss/index.php
For more about Juniper Publishers | Please click on: https://juniperpublishers.com/pdf/Peer-Review-System.pdf
0 notes
Last Seen Blogs

zeepatnablog
Untitled

eu-nao-lirico
Eu, Não-Lírico
melted-paradise
Melted Paradise

rottenluci
art blog!

kas14
Slytheringirl14