#Child & Adolescent Psychiatrist
Text
#best psychiatrist in bangalore#top 10 psychiatrist in bangalore#psychiatrist near me#best psychiatric hospital in bangalore#best psychiatric doctor in bangalore#psychiatric rehabilitation centre#best psychiatrist in karnataka#psychologist near me#children's problem behaviors#child psychiatrist in bangalore#adolescent psychiatrist bangalore#Child & Adolescent Psychiatrist#PSYCHIATRIC TREATMENTS FOR CHILDREN AND ADOLESCENTS#Top Child and Adolescent Psychiatrist in Bangalore#Adolescent mental health treatments#Best Child Psychology Doctors In Bangalore#Child mental health#Adolescent counseling#Pediatric psychiatry#Pediatric mental health specialists#Autism Treatment for Adults & Children#Cognitive Behavioral Therapy Bangalore#autism signs & treatment
0 notes
Text

Child and Adolescent Therapy: Nurturing Young Minds for a Brighter Tomorrow
In today's fast-paced world, children and adolescents face unique challenges that can impact their mental and emotional well-being. Child and adolescent therapy, offered at Akshaya Medical Centre in Vidyaranyapura, Bangalore, plays a pivotal role in providing the support and guidance necessary to nurture young minds and ensure a brighter tomorrow.
Understanding Child and Adolescent Therapy
Child and adolescent therapy, also known as pediatric therapy or counseling, is a specialized form of mental health treatment designed to address the unique emotional and psychological needs of young individuals. These formative years are marked by significant growth and development, but they can also be a time of stress, confusion, and emotional struggles.
The role of a child and adolescent therapist is to create a safe and supportive environment where young individuals can express their thoughts and feelings, build coping skills, and work through various challenges. These challenges can range from academic stress, peer pressure, family issues, emotional disorders, behavioral problems, and more.
Why Child and Adolescent Therapy Matters
Early Intervention: Child and adolescent therapy provides early intervention for mental health concerns. By addressing issues during childhood and adolescence, it can prevent them from developing into more significant problems in adulthood.
Emotional Resilience: Therapy helps young individuals build emotional resilience and coping skills. They learn how to manage stress, express their emotions, and make healthy choices.
Academic Success: Many children and adolescents experience academic stress. Therapy can help them manage the pressure, improve focus, and achieve their academic potential.
Positive Relationships: Therapy fosters better communication and problem-solving skills, which are crucial for building positive relationships with family and peers.
Behavioral Issues: Behavioral problems, such as aggression or withdrawal, can be addressed and modified through therapy, leading to more balanced behavior.
Emotional Disorders: Children and adolescents can be susceptible to emotional disorders like anxiety and depression. Therapy offers strategies to manage and overcome these conditions.
Child and Adolescent Therapy at Akshaya Medical Centre
Akshaya Medical Centre in Vidyaranyapura, Bangalore, offers comprehensive child and adolescent therapy services, delivered by experienced and compassionate professionals. The journey begins with an initial assessment, during which the therapist evaluates the child or adolescent's needs, concerns, and goals.
Therapeutic sessions are tailored to each individual's specific requirements. The therapy may involve talk therapy, play therapy (for younger children), cognitive-behavioral therapy, family therapy, and more. The choice of therapy depends on the nature of the issues and the age and preferences of the child or adolescent.
Our therapists work collaboratively with parents and caregivers to ensure a holistic and supportive approach. They provide guidance to parents on how to support their children outside of therapy sessions, creating a nurturing environment at home.
The Role of the Best Psychiatrist in Bangalore
In some cases, child and adolescent therapy may involve consultation with the best psychiatrist in Bangalore. This is especially relevant when there are concerns about more severe mental health issues or when medication management is required.
The best psychiatrist in Bangalore, working in conjunction with the therapy team, can provide a comprehensive treatment plan that may include therapy, medication, and ongoing evaluation.
The Impact of Child and Adolescent Therapy
Child and adolescent therapy can have a profound and lasting impact on the lives of young individuals. By addressing issues during these formative years, it equips them with the tools and strategies they need to navigate life's challenges successfully. This, in turn, leads to improved well-being, academic success, and the development of healthy relationships.
Therapy helps young individuals build emotional resilience, allowing them to cope with stress and adversity in a healthy way. It provides a safe space for them to express their thoughts, feelings, and fears, fostering emotional growth and self-awareness.
In cases where emotional disorders are present, such as anxiety and depression, therapy offers a path to recovery and healing. It teaches young individuals to manage their symptoms, develop positive coping mechanisms, and regain a sense of control over their lives.
The Role of Parents and Caregivers
Parents and caregivers play a vital role in the success of child and adolescent therapy. They serve as a support system and are integral to the therapeutic process. By working collaboratively with therapists, they can create a nurturing and supportive environment at home, reinforcing the strategies and skills learned in therapy.
Conclusion
Child and adolescent therapy at Akshaya Medical Centre in Vidyaranyapura, Bangalore, holds the promise of nurturing young minds for a brighter tomorrow. By addressing emotional, psychological, and behavioral challenges during these crucial formative years, therapy sets the foundation for a lifetime of mental and emotional well-being. If you have concerns about your child's or adolescent's mental health, seeking the support of child and adolescent therapy professionals is a proactive step in ensuring a brighter and more promising future for the young minds we cherish.
#Child and adolescent therapy#best psychiatrist in Bangalore#adolescent therapist#Akshaya Medical Centre Vidyaranyapura Bangalore
0 notes
Text



Website : https://basepointacademy.com/locations/arlington-tx/
Address : 3900 Arlington Highlands Blvd Suite 237, Arlington, TX 76018
Phone : +1 469-747-1797
BasePoint Academy is a licensed mental health and substance use disorder treatment center serving children, adolescent and teens age 12-18 in the Arlington and Dallas Fort Worth Metro area. Our behavioral health treatment center provides therapy and counseling for teens, anxiety & depression treatment, and primary mental health rehab for teens with secondary drug addiction treatment. We offer some of the leading child psychologists and teenage psychiatrists in the DFW area. Our treatment modalities include resilience therapy, individual therapy, group therapy, CBT, DBT, Trust-Based Relational Intervention (TBRI), motivational interviewing therapy, experiential therapy, solution focused therapy, mindfulness therapy and more.
#teenage psychiatrist#teenage psychologist near me#child therapy dallas#behavioral therapy dallas tx#teenage behavioral treatment center#mental health services for adolescents & teens#teen & adolescent treatment center#teen & adolescent mental health treatment#rehab for teens#rehab for teenagers#drug rehab for teens#rehab for teens near me
1 note
·
View note
Text
One thing I find so interesting about Sam and Dean's childhood is how outsiders must've perceived Dean's outbursts when Sam's safety was at risk.
On the playground, teachers catch Dean pummeling Sam's bully. The kid is on the ground, nose a broken, bloody mess and Dean's still swinging, teeth bared in a silent snarl. Sam is holding his face in his hands, staring, disturbed and somber, at Dean's feral display. Later, there'll be a call from the principal but it's the 90s and John's busy, so of course nobody picks up. The teachers think something is seriously wrong with Dean, but Sam knows the truth. They try to get Dean evaluated by the district's child and adolescent psychiatrist but John's not there to give the green light so it's fruitless. Still, they keep a closer eye on Sam's older brother.
It's that type of raw protectiveness that bleeds into their teenage years and beyond. As an adult, Dean doesn't care how he and Sam are perceived because he's used to the uncomfortable stares, inquiring glances, and veiled whispers. At the end of the day, Sam is his kid, no matter if the dude's a giant grown-ass man. He'll always be that shy, timid kid on that playground.
#supernatural#samdean#sam winchester#dean winchester#bromance#sam and dean#Wincest#Wincest if you squint#supernatural theories#weecest#weirdcest#gencest#parentified child#Spn
690 notes
·
View notes
Text




Published: Jul 13, 2023
As experienced professionals involved in direct care for the rapidly growing numbers of gender-diverse youth, the evaluation of medical evidence or both, we were surprised by the Endocrine Society’s claims about the state of evidence for gender-affirming care for youth (Letters, July 5). Stephen Hammes, president of the Endocrine Society, writes, “More than 2,000 studies published since 1975 form a clear picture: Gender-affirming care improves the well-being of transgender and gender-diverse people and reduces the risk of suicide.” This claim is not supported by the best available evidence.
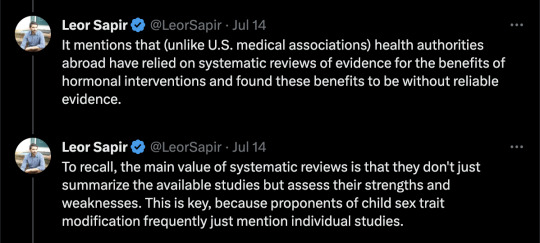
Every systematic review of evidence to date, including one published in the Journal of the Endocrine Society, has found the evidence for mental-health benefits of hormonal interventions for minors to be of low or very low certainty. By contrast, the risks are significant and include sterility, lifelong dependence on medication and the anguish of regret. For this reason, more and more European countries and international professional organizations now recommend psychotherapy rather than hormones and surgeries as the first line of treatment for gender-dysphoric youth.
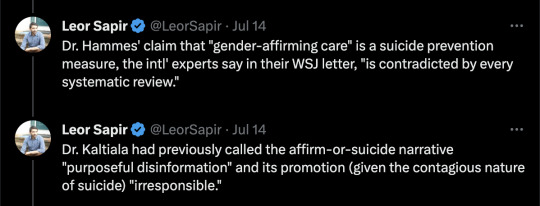
Dr. Hammes’s claim that gender transition reduces suicides is contradicted by every systematic review, including the review published by the Endocrine Society, which states, “We could not draw any conclusions about death by suicide.” There is no reliable evidence to suggest that hormonal transition is an effective suicide-prevention measure.
The politicization of transgender healthcare in the U.S. is unfortunate. The way to combat it is for medical societies to align their recommendations with the best available evidence—rather than exaggerating the benefits and minimizing the risks.
This letter is signed by 21 clinicians and researchers from nine countries.
FINLAND
Prof. Riittakerttu Kaltiala, M.D., Ph.D.
Tampere University
Laura Takala, M.D., Ph.D.
Chief Psychiatrist, Alkupsykiatria Clinic
UNITED KINGDOM
Prof. Richard Byng, M.B.B.Ch., Ph.D.
University of Plymouth
Anna Hutchinson, D.Clin.Psych.
Clinical psychologist, The Integrated Psychology Clinic
Anastassis Spiliadis, Ph.D.(c)
Director, ICF Consultations
SWEDEN
Angela Sämfjord, M.D.
Senior consultant, Sahlgrenska University Hospital
Sven Román, M.D.
Child and Adolescent Psychiatrist
NORWAY
Anne Wæhre, M.D., Ph.D.
Senior consultant, Oslo University Hospital
BELGIUM
Em. Prof. Patrik Vankrunkelsven, M.D. Ph.D.
Katholieke Universiteit Leuven
Honorary senator
Sophie Dechêne, M.R.C.Psych.
Child and adolescent psychiatrist
Beryl Koener, M.D., Ph.D.
Child and adolescent psychiatrist
FRANCE
Prof. Celine Masson, Ph.D.
Picardy Jules Verne University
Psychologist, Oeuvre de Secours aux Enfants
Co-director, Observatory La Petite Sirène
Caroline Eliacheff, M.D.
Child and adolescent psychiatrist
Co-director, Observatory La Petite Sirène
Em. Prof. Maurice Berger, M.D. Ph.D.
Child psychiatrist
SWITZERLAND
Daniel Halpérin, M.D.
Pediatrician
SOUTH AFRICA
Prof. Reitze Rodseth, Ph.D.
University of Kwazulu-Natal
Janet Giddy, M.B.Ch.B., M.P.H.
Family physician and public-health expert
Allan Donkin, M.B.Ch.B.
Family physician
UNITED STATES
Clin. Prof. Stephen B. Levine, M.D.
Case Western Reserve University
Clin. Prof. William Malone, M.D.
Idaho College of Osteopathic Medicine
Director, Society for Evidence Based Gender Medicine
Prof. Patrick K. Hunter, M.D.
Florida State University
Pediatrician and bioethicist
Transgenderism has been highly politicized—on both sides. There are those who will justify any hormonal-replacement intervention for any young person who may have been identified as possibly having gender dysphoria. This is dangerous, as probably only a minority of those so identified truly qualify for this diagnosis. On the other hand, there are those who wouldn’t accept any hormonal intervention, regardless of the specifics of the individual patients.
Endocrinologists aren’t psychiatrists. We aren’t the ones who can identify gender-dysphoric individuals. The point isn’t to open the floodgates and offer an often-irreversible treatment to all people who may have issues with their sexuality, but to determine who would truly benefit from it.
Jesus L. Penabad, M.D.
Tarpon Springs, Fla.
[ Via: https://archive.today/IRShy ]

==
The gender lobotomists just got called out.
#Leor Sapir#Colin Wright#Endocrine Society#gender lobotomy#genderwang#gender ideology#queer theory#sex trait modification#ideological capture#medical malpractice#medical transition#medical scandal#gender affirming care#affirmation model#gender affirming#ideological corruption#religion is a mental illness
283 notes
·
View notes
Text
About Psychiatry stuff in SPYxFAMILY. Part 1
Part 2 here / Part 3 here / Part 4 here
I'm a dumb and I just realized that ch. 29 of the manga will be animated, since Fiona appears for the 1st time in that chapter and she's in the key visual for the 2nd cour.
I'm aware this isn't the first analysis made on this chapter but so far I haven't seen anyone from the Psy world speaking about this. I'm a Clinical Psychologist grounded on Freudian-Lacanian Psychoanalitic theory and I think I can share some knowledge over several aspects of Psychiatry that are depicted in the manga. I've worked with Psychiatrists in the past, albeit for a short amount of time, in a public healthcare institution, so I have a notion of what Psychiatrists do in a public setting like a Hospital.
If there's a Psychiatrist out there who wants to refute this analysis, PLEASE DO SO. I'm more than pleased to learn and have a nice debate.
This is one of the most hilarious chapters in the whole SxF series, so if you don't want the fun to be spoiled, please skip this post!
Let's begin.
1. Working in a Hospital
I'm not sure if this is universal, as healthcare systems around the world differ in several aspects, but the consensus is that a Hospital, which is a public healthcare institution, is specialized in the treatment of the most complex diseases.
In Psychiatry, this usually means dealing with psychosis, drug intoxication, major depressive episodes with suicide attempts and serious personality disorders. Most of these conditions require hospitalization, as the risk of giving just ambulatory care is not enough to guarantee the patient's safety or that of the others's.
There are Hospitals that provide ambulatory care though. Again, it varies from where in the world you are. In my country (Chile) you usually go to the Hospital when your life is at risk, but if you are suffering from a less serious condition (for example, dealing with panic attacks), you'll be transferred to a primary healthcare institution. Unless you live in a rural area.
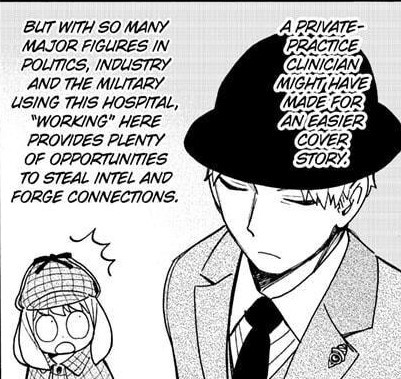
Indeed, working in a healthcare institution means gaining access to any patient's clinical record. But for the objective of Operation Strix, and Loid being a Psychiatrist, I don't think that's of much use, for reasons that I'll cover in Point 3.
2. Specialty in Psychiatry
Psychiatry has several subspecialties, like any other healthcare career. You have Child and Adolescent Psychiatry, Adult Psychiatry (I believe these two are mandatory to become a Psychiatrist but I can't say it for sure), Addictions, Forensics, Emergencies...
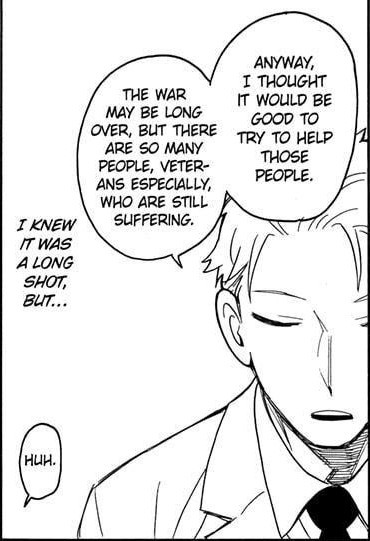
Loid said that he wants to help people affected by the war, veterans specially, so it's a polite guess to say that he's an Adult Psychiatrist. Then again, we have this panel:
The sand box is a diagnostic tool used for children. It's mostly used by Psychologists, as they have more time per session to analyze it. I'll cover the sand box in more detail in Part 4 of this series of analysis, but for now let's say that analyzing it consumes a lot of time that Psychiatrists, in a Hospital, usually don't have.
This panel suggests that Loid has worked with children before as a Psychiatrist, and we see him later in chapter 67 with a child (although it's not clear if the child is his patient), so here are another 2 polite guesses:
-Loid's a General Psychiatrist
-Berlint General Hospital's Psychiatric Ward is understaffed and they put their Psychiatrists to do whatever is needed at the moment, regardless of their specialties. It sure doesn't look that poor of a Hospital to me, but who knows...
My bet is option 1. Poor guy.
3. Donovan Desmond as a potential psychiatric patient

In the first chapter of the manga, Donovan is described as a hikikomori, meaning someone who withdraws from social interaction. This word also describes a psychopathological condition of japanese young lads that spend months, even years, holled up in their homes without interacting with anybody aside from their families (if they have). The word itself doesn't have a pathological connotation tough.
In English, the closest concept to "hikikomori" as a psychpathological meaning would be Autism, which isn't equivalent at all. And, when a person is so reclused, we tend to pair it with paranoia, as it often leads to social withdrawal as well. The important thing here is, as you probably are thinking right now, the reason fo such decision. And this reason is always given by the symptoms.
Paranoia is a type of psychosis in which a person suffers from delirium and hallucinations related to being endangered or threatened by something. Of course, a proof of reality is useless for these patients, as their perception of reality itself is disturbed. An UFO is watching over you at all times? I can't precisely prove that it's false, as I lack proof of the very existence of UFO, and even if I have it, the delirium would probably shift to attack me as I turn into a conspirator against the patient's truth.
Not that we clinicians waste time trying to do so, though. In these cases, the Psychiatrist kicks in and administers a dose of antipsychotic drugs. Psychotic paranoia often needs hospitalization and a strong compromise from the patient's family to constantly supervise him/her. After that, comes a long process of social rehab.
A very characteristic feat of paranoid people is that THEY NEVER SEEK FOR PROFESSIONAL MENTAL HEALTH CARE HELP BY THEMSELVES. Paranoids often arrive to a Psychiatric Emergency Room dragged by a third party due to bizarre behaviour, self-aggression and/or attempts to hurt others.
There are people that is not psychotic and suffer from this kind of fear of pretty much everything as well, but it's hard to determine if they really aren't psychotics, as their reasons to recluse themselves strongly resemble a delirium. The key that helps to discern if it's a psychotic paranoia or not is finding the hole in which a patient allows himself to doubt. In paranoid psychosis there's absolute certainty, while in neurosis there is room for doubt.
These "neurotic paranoids", as we'll call them for now (it doesn't exist as a nosograhical entity anywhere; please don't waste your time looking it up in the DSM xD), tend to abandon therapy pretty soon, as they fight for sticking with their motives to recluse themselves. They don't want to realize what drive them to behave like that. Patients suffering from obsessions will probably act this way, as well as some hypochondriac and anorexic patients. Bear in mind that this is not a norm; everything depends on the symptoms.
All of this begs the question: Would Donovan Desmond ever need Psychiatric help from Dr. Loid Forger?
His interaction with Loid in chapter 38 suggests that he's not reclusive for a mental condition, but he does have a certain level of "neurotic paranoia", as he can't bring himself to really trust any other person much. If nobody is truly sympathetic to each other, they could pose a threat at any moment, right?
Since he's clearly not psychotic, because he can hold an interaction with Loid in the same shared reality (not a dellirium, I mean), one can safely assume that he does trust someone, at least one single person. When a psychotic person suffers from paranoia, there's not a single hole in their life that is not filled with suspicions of others being dangerous. This isn't the case for Donovan.
We see him walking with a lot of guards, so he must trusts them. And he seems to be closer to Demetrius as he goes with him to the Imperial Scholar get-togethers, so that also counts. He even takes a detour to meet Damian. Seems like he can trust his family members, and that alone could be a measure of love, albeit in a really weird scale.
Tsundere?
That aside, given the social status of the Desmonds, if they ever need psychiatric help, they probably would consult a private clinic instead of going to a public hospital. Unless they find themselves in a reeeeaaaally desperate situation.
So, the answer is no... for the most part. Good try, though, Twilight.
I'll cover more stuff in the next part. This one turned out unexpectedly long. It's been fun ruining the fun for those who don't know about mental health though.
474 notes
·
View notes
Text
🤎 ‘BLACK STORIES We Should All Know’
👉🏾 RUSSELL LEDET was a security guard at a Baton Rouge hospital when he decided to become a doctor
👉🏾 he would ask other doctors if he could shadow them - they told him a security guard can’t be a doctor
👉🏾 one day he asked Dr. Patrick Greiffenstein and he said YES
👉🏾 they did the necessary paperwork so Russell could shadow Dr. Greiffenstein and Russell Ledet’s life changed
👉🏾Russell Ledet earned his MD, PhD, and MBA
👉🏾He got accepted into Indiana Triple Board Program to become a Pediatrician, Adult Psychiatrist, and Child & Adolescent Psychiatrist
👉🏾he is the founder of 15 WHITE COATS and he served in the US Navy 🇺🇸
👉🏾sources: The15WhiteCoats.org + BBC.com + Fox8Live.com
📸 Dr. Russell Ledet + Sydney Labat + Fox8Live.com
26 notes
·
View notes
Note
if you're still taking requests, plz a scenario, with Hannibal, with a Fem S/O who is Aspect of Gluttony, usually eating things that are inedible, raw meat or even eating more than their own size, imagine them meeting for the first time in his office for an appointment and she is wearing a muzzle to stop her from eating things, bonus her personality is calm, soft spoken and gentle, the duality of when she is hungry.
Thank you for your attention and time, drink water!
Thanks anon for the great scenario! S/O reminds me a lot of six from little nightmares. I drew inspo from that, I hope you like it, tell me if you do and don't be shy to give me critique! I wrote this as a one shot let me know if you want anything different
Hannibal x Fem!Reader
Jack had called will in on a case. The cold autumn air bit his skin as he was lead through the frigid forest to the crime scene Hannibal following close behind "Victim was found by a hiker, who thought it was a wild animal attack until they saw.. Well the bite marks". Lying on their back laid the victim their face was mauled beyond recognition their shirt was torn exposing their half eaten chest. Their arms were eaten down to the bone stomach ripped open messy unorganized rips and tears littered their body. Hannibal frowned he knew exactly who did this your bite marks were all over the victim your saliva messily strewn about they would surely trace it back to you.He likes encourageing you behavior but it seems like you might not come back from this. Will stood in his usual trance and reconstructed it in his head. He was suddenly running through the forest, it was sunset and his mind was in a manic haze " It's happening again, i grip my stomach falling against a tree." He looked up to the sound of rustling leaves and jogger approached "Hey ma'am are you ok? "they questioned stopping at their side. He looked up Continuing to Narrorate" I so sorry, I don't want to hurt you, but the hunger.. " he stands up straight " I warn the victim, telling them to go away but they do not listen, I can't hold back any longer". "I lunge at the victim biting their neck and ripping out a chunk, they fall back shocked choking on blood I proceed to maul them trying desperately to quench my hunger." " it feels like I think for hours trying and failing to stop,not stopping until I could no longer fit any more in my stomach." He rises " when I finally come back to my senses, I'm horrified of what I've done. I run away. " Will finally snaps out of it. " The victim was eaten alive". So it was some type of sick cannibal, hunting for sport? "." no, this was too desperate, too rushed, they couldn't stop themself, they tried going into the woods so they couldn't hurt anybody, unluckily for them, they ran into this person.

Hannibal remembers the first time you met like it was yesterday, you came to his office for an appointment , as a child you were usually quite well behaved, but as you grew you developed a violent hunger,you ate very large amounts but it was never enough,when hungry you would eat anything you could fit into your mouth. often lashing out at anyone who tried to stop you. Soon enough you began eating everything you could get your hands on frenzied hungers grew worst, your parents were concerned, but finally drew the line when they found you eating the corpse of your beloved childhood hamster. They sent you to multiple facilities, and did many tests to try to figure out was wrong but no one seemed to quite know the reason.You lived most of your adolescence in and out of therapy. You were able to handle it better eventually you were at a place where you were able to suppress the urges,able to move out, get a job and live a relatively normal life. You saw a psychiatrist regularly going to therapy, but you're violent hunger returned, your psychiatrist couldn't handle it anymore and referred you to Hannibal. That's how you ended up sitting in this office.
Hannibal opened the door to you "Ms. L/N I suppose? " he asked glancing down at your muzzle,paying it no mind. You nodded "Come in". You walked as he lead you to his desk " please, sit", he motioned to the chairs next to it" It's a pleasure to meet you Dr. Lecter"."The pleasures all mine, now what brings you here? " " Well other than the referral I come here for my..hunger problems. "I see I infer that's why your wearing a..muzzle of sorts? " "Yes, you see when I get hungry I can't seem to stop myself, I have this intense urge to eat things I shouldn't and I always end up giving in" he tilted his head " what are these things that you 'shouldn't eat " " well, any food I can get my hands on really, trash, small animals bugs, small dogs, Recently what got me here, human flesh.. " this caught his attention "You have eaten.. People? " he said calmly very good at hiding his excitement "Well yes and no.. I had taken a bite out of someone's arm in an episode and I must admit it was quite.. Odd. I've never tasted such a thing" he sat for a second "have you thought a lot of eating another person" "it has crossed my mind" "Do you want to? "
After that first appointment he was instantly taken by you, intrigued. You had an inherently calm and gentle nature, outside of your ravenous spouts you loved animals and were quite polite. But when you're hungry, there's something so different, so passionate, so deliciously violent that drew him in to your sweet perfume. The more he saw you, the more he wanted to see what you are capable of, to push your limits. He wouldn't admit it but he was obsessed with you, he began to act as a friend outside of the office, this turned to him taking you to the opera and even to your protests he took you home to make you dinner.
You sat in his dining room , figeting, nervous.What if you lost your cool? How embarrassing would it be. You didn't have much time until a heavenly smell hit your nose so familiar, yet you couldn't put your finger on it. Your stomach grumbled and you were glad that you still had your muzzle on. You could feel your hunger rising you needed to eat soon or you would break. Luckily for you he soon came out with a beautifully cooked steak, it looked a bit odd and smelled so familiar, but you were so overcome with hunger. You didn't care quickly, taking off your muzzle " I must warn you, doctor Lecter I'm quite a messy eater. " " I assure you with your condition that's perfectly fine and please, call me Hannibal." You gave him a smile before diving in you were done in a flash, but it was weird you were oddly sated usually you be far more hungry but something about that meat...it was all too familiar you looked at him,still eating his food"That was lovely what was that might I ask"."Steak"This was the start to an odd relationship to say the least.He began to fuel your need for human flesh without you knowing but it was only a matter of time until he led you where you were now. Desperate in the woods,shaken and trying to catch your breath running as blood surrounded your mouth. Terrified, but by God you were finally full
Hope you enjoyed! 💗
181 notes
·
View notes
Text
Laura and Esme
I got hooked on General Hospital as a child because a babysitter watched it. The storyline that got me hooked was Leslie lying on the witness stand, because I thought the courtroom witness stand was like Wonder Woman's lasso and you couldn't lie, so I wanted to see how Leslie would overcome that. (Like I said, I was just a child ;-) )
But today I was reminded why Leslie was lying. When Laura was 14 or 15, she was seduced by her mother's adult lover, and eventually snapped and murdered him. She then developed amnesia about what she'd done, and to protect her Leslie falsely admitted to the murder.
But...plot twist. Laura got her memory back and pretended to still have amnesia, letting her mother go to prison for a crime she'd committed.
Of course, she went on to do great things, even saving the world a few times. But she's never really been the paragon of virtue that traditional soap heroines were supposed to be.
This got me to wondering if Laura sees herself in Esme. Laura had been adopted by sketchy parents only to discover her real parentage in adolescence. She was even held prisoner by the father of the man who held Esme prisoner. And then there's the whole young felon who gets away with her crimes and fakes amnesia angle. (Remember, Nicholas is the product of Stavros' rape of Laura.) I've been banging my head against the wall wondering how Laura could be so gullible as to believe Esme's lies.
Now I suspect she doesn't. Even her advice today ("Don't think about the past; look to the future") suggests she knows Esme has her memories back. I think she wants to "save" Esme as a symbolic way of saving the young woman she was. Laura believes there's good in Esme because she believes there was good in her. It would also explain why Laura is more supportive of Esme than she is of Spencer. She doesn't identify with Spencer in quite the same way.
If my theory is correct, it's pretty twisted, and it's too bad Port Charles doesn't have a psychiatrist who isn't Laura's husband. But it would explain a lot.
14 notes
·
View notes
Text
With roughly 90% of her caseload identifying as transgender, adolescent therapist Adeola Baker* is raising red flags about the “social contagion” of gender ideology. According to Baker, many medical professionals are leaving the field entirely because they’re encouraged to unequivocally affirm identities rather than find the root cause of their patient’s mental health issues.
Just five years ago, adolescent therapist Adeola Baker* recalls the majority of her caseload was children struggling with depression, anxiety, trauma, bullying, or family issues. Today, she says the field has “radically changed” before her eyes and now roughly 90% of her cases are children identifying as transgender.
In the past, before a minor could be prescribed hormones such as testosterone, Baker says the child was required to see a therapist—like herself—and go through multiple therapy sessions. Today, she says very few gender clinics even require these formal letters from therapists.
“Essentially what they want is for us to see them one time, write them a letter saying it’s fine, and just put them on their way,” says Baker. “I have a problem with that.”
Baker feels that adults “should be able to live their lives in peace” if they identify as transgender, but likened the current climate surrounding the normalization of gender ideology among children to a social contagion.
“These kids have friends who are on testosterone and they want to be cool and be on testosterone too”
Baker says, noting that she had had cases in the past with children who were diagnosed with gender dysphoria. However, Baker attributes this current explosion in her gender-related caseload to overarching behavioral patterns being spread through social influences.
“A lot of these kids don’t have gender dysphoria,” she begins, explaining that there’s a difference between diagnosable gender dysphoria and her new patients who identify with neogenders and neopronouns.
“This isn’t a joke; they’ve self-identified as trees, dolphins, dogs, bugs, paintbrushes, vampires, zombies, wolves, puppies, and clouds. I had a piano and a saxophone once too.”
In her professional work, Baker has noticed that this increase in “kids who have caught onto the social contagion” and treat their gender identity as a personality quirk are actually making it more difficult for people with diagnosable gender dysphoria to receive the therapy they need.
“Gender clinics are shutting down left and right because you can’t tell anybody ‘no’ anymore”
she says, noting that because pediatricians, children’s psychiatrists, and therapists are being discouraged from finding the root cause of their patient’s mental health issues, many are leaving the field entirely. As a result, Baker says the decline in medical professionals willing to work in affirmation-focused clinics is what’s causing clinics to shut down, not transgender-exclusionary legislation.
“You have to say yes. The official standpoint from all the pediatrician networks is affirm, affirm, affirm,” Baker says.
Baker, who has been diagnosed with Asperger’s syndrome, a form of autism spectrum disorder, understands firsthand the identity issues that many young people with developmental disorders face. Data suggest that people who identify as transgender or nonbinary are up to six times more likely to also be on the autism spectrum. Baker also points out that there are more concurrent issues at hand, such as sexual assault trauma.
“A lot of these kids on the spectrum have identity issues. Then they say to themselves, ‘Oh, it’s because my brain is wrong. I’m actually a boy.’ I can say this as a person on the spectrum that had those same identity issues as a teenager”
she explains, sharing that many therapists are essentially being told to go along with children’s self-diagnoses. Baker continues:
“We are being told, ‘Don’t investigate what’s going on. Don’t find out if they have a comorbid personality disorder or if they have a comorbid issue like being on the spectrum.’ Affirm, affirm, affirm. Anything other than affirmation is just ‘transphobia.’”
Between her own practice, her husband’s work as a pediatric nurse, and the many colleagues she has in the medical industry, Baker says there’s a staggering number of medical practitioners who are critical of gender ideology but don’t speak out due to fears of being “doxxed” or receiving rape and death threats. For instance, one of Baker’s colleagues, a Licensed Clinical Social Worker from California, was allegedly reported to the California Board of Behavioral Sciences and almost lost her license after facing complaints for not affirming kids.
Through the “affirming” medical professionals, however, Baker says that many transgender-identifying children sign informed consent without reading into the details about the medications they’re then placed on. Then, they get prescribed high doses of testosterone. According to Baker, patients are supposed to start off at 50 milligrams of testosterone but routinely get prescribed 400 milligrams without fully understanding the implications of such high doses.
Baker points out that some young adults who took hormone replacements for many years are now infertile.
In the case of “gender-affirming surgeries,” young males who underwent penile inversions or young females who got hysterectomies don’t have the necessary genitalia anymore to consider having children of their own in the future. Baker says that in most places, it’s illegal for a girl under 18 to undergo a hysterectomy, but once these patients turn 18, she has observed medical professionals permitting the procedures despite the girls still being in high school.
In April 2022, Baker met with an “affirming therapist” who writes notes for transgender-identifying youth to be cleared for testosterone prescriptions, double mastectomies, and other surgical procedures. When Baker asked the therapist what would happen to these patients if they ever wanted to have kids, she says the therapist insisted her patients know they don’t want children.
“But how is that? I didn’t decide I wanted kids until I was 26 when I met my now-husband,” Baker says. “I had trauma, which is why I work with kids with trauma. Up until the age of 26, if you asked me, ‘Do you want to have kids?’ I would’ve said no. How does a 14-year-old know they never want to have kids?”
(...)
Since her specialty is trauma in youth, Baker’s caseload includes a lot of young people with unique gender identities. But, as a therapist, Baker doesn’t feel that it’s her place to unequivocally affirm “delusions” and wishes more medical professionals would try to address the root issues going on with their patients’ mental health.
“Ultimately, it comes down to the fact that we are the adults,” she says. “It’s our job to make the difficult decisions for children whose brains aren’t fully developed until they’re 24 or 25.”
*Name has been changed to protect anonymity.
35 notes
·
View notes
Text
thinking abt my murder family dynamics as always and the specific problem of why abigail doesn't find a way to just escape the whole situation with hannibal and will, because she is definitely physically capable of doing that and she's not stupid, she knows hannibal is dangerous and might kill her
first place! she's an adolescent of an age group typically at least ready to TRY leaving home, but she's established as being particularly attached to her parents and having a close bond with them. maybe she didn't look forward to leaving home any more than her dad did, and she would have gravitated back home any chance she could like elise nichols. when she's orphaned and loses her home at the start of the season it fundamentally unmoors her emotionally. in a lot of ways she's still a child and not really keen on the idea of striking out on her own in the face of all that loss. alana bloom wants to support her to be more self sufficient or at least not to try to replace her parents with substitute figures right away, BUT, CRUCIALLY,
its not JUST that she doesn't want to be alone in a purely homesick sense. she cannot SURVIVE on her own. she's physically powerless, and worse than that she is in very immediate danger of being charged as an accomplice to her father, and that's not a danger she can shake off by being independent and starting over with a clean slate. she ropes alana in to feeling as much like a guardian as a psychiatrist and seems to foster that protectiveness in her, and does the same to hannibal and will. she latches on to all of them as they latch on to her and does everything she can to put them in a position to protect her. even freddie gets the honorary abigail guardian treatment, though the connection is less 'will you be my mummy🥺' and more 'i will be the goose that lays golden eggs if you help me look innocent'
it helps in hannibal's case that he is doing the same work right back and they immediately become codependent as shit. he thrives on making people with less power feel dependent on him, she needs someone to ensure her survival, she lets him know that she has dirt on him, he puts her in a position to get in trouble and then rescues her from it, they hide a body together. its a blackmail based relationship on both sides that immediately turns into playing house and fostering genuine emotional connection.
will fundamentally can't really offer her the same sense of safety because he's visibly unstable and also carries the risk of turning her in if he finds out she's guilty, and then she's afraid that he's just flat out a threat to her safety (and he IS, there is a part of him that feels betrayed by her and wants to kill her in retribution or to protect her by making her safe in death or whatever jumbled up mess of her father's feelings he's stewing in)
so will isn't safe for her and alana keeps a little too much professional distance to protect her the way she needs, and then hannibal pulls the rug out from under her and reveals that he is much, much more dangerous than she had assumed. and in that moment there's an implicit threat that she will let him help her by faking her death or he will kill her outright. evolve or die.
but after that? she could find a way to leave any time, after hannibal hides her away and gets busy with his long-distance flirtation with will and the FBI. she's not tied up in his basement. she's a free agent, she may even be in a separate safe house. but she never runs away. maybe its not totally rational: the emotional connection is there - she reminds him of his sister, he reminds her of her father. but i think she knows very well that his caring about her doesn't make him less of a threat to her safety. still, while the relationship is obviously precarious, he has always helped her and done exactly as he promised to do, and she has no reason to believe he will betray that. AND she has a good reason not to act out against his wishes in any way even if to do so WOULD make her safer and more in control. when she dug up the body they hid together, he gave her an implicit threat: his protection is conditional.
if she stays and does what he tells her to do, she trusts that he'll keep his promises. if she runs, she does not have that guarantee. it's a very smart calculation - but (scorpion and the frog parable) she realizes too late she was wrong about that
#this post was gonna be brought to u in purple by sheer dint of tumblr mobile having some goddamn Thing Going On#hannibal meta#been trying to untangle this knot of character motivation yk#abigail hobbs#hannibal lecter#long post
25 notes
·
View notes
Text
I think everyone who wants to be informed about neurodivergent issues and how they intersect with race ought to read up on the absolute shitfucked situation surrounding oppositional defiant disorder (ODD), a bullshit diagnosis that’s often applied in super racist ways.
So first of all, here are the diagnostic criteria from the DSM. I’m linking it, but I know a lot of people won’t click, so I’ll list it too.
A. A pattern of angry/irritable mood, argumentative/defiant behavior, or vindictiveness lasting at least 6 months as evidenced by at least four symptoms from any of the following categories, and exhibited during interaction with at least one individual who is not a sibling.
Angry/Irritable Mood
1. Often loses temper.
2. Is often touchy or easily annoyed.
3. Is often angry and resentful.
Argumentative/Defiant Behavior
4. Often argues with authority figures or, for children and adolescents, with adults.
5. Often actively defies or refuses to comply with requests from authority figures or with rules.
6. Often deliberately annoys others.
7. Often blames others for his or her mistakes or misbehavior.
Vindictiveness
8. Has been spiteful or vindictive at least twice within the past 6 months.
B. The disturbance in behavior is associated with distress in the individual or others in his or her immediate social context (e.g., family, peer group, work colleagues), or it impacts negatively on social, educational, occupational, or other important areas of functioning.
C. The behaviors do not occur exclusively during the course of a psychotic, substance use, depressive, or bipolar disorder. Also, the criteria are not met for disruptive mood dysregulation disorder.
It’s also worth noting that in an accompanying “severity” section, the diagnostic criteria notes that this diagnosis can be applied at the “mild” level even if the person only meets diagnostic criteria in a single setting, like school or home, but has no symptoms anywhere else! Another note that I left out because it was super long but is accessible in the link specifies that if they’re older than 5, the person being diagnosed only needs to show these “symptoms” once a week. There is no adjustment made anywhere for the situation the person might be in, meaning that even if someone is being actively harassed by others and only lashing out in reaction to that - you know, like any person would do - they can still be diagnosed with ODD. As you can see, noncompliance with authority is directly listed as a “symptom,” multiple times, without any concern for evaluating whether there might have been valid reasons for that defiance.
On its own I think it is already fairly obvious that this is a diagnosis intended mainly to pathologize people who won’t blindly submit to anyone in a position of power over them, hurt them in retaliation for their defiance, and enforce compliance with authority. A child who stands up against abusive parents, an activist who defies the police, and a worker who refuses to comply with abusive workplace conditions could all be diagnosed with ODD without even really stretching the criteria.
However, where this becomes especially insidious is its interaction with race and ADHD. Black children are disproportionately likely to be diagnosed with ODD, and it’s a heavily stigmatized diagnosis that follows them and continues to pathologize any attempt to exert personal agency for the rest of their lives. In a study where psychiatrists were sent vignettes about a child’s behavior and asked to diagnose the child, vignettes labeled as being about Black children received 56% more diagnoses of ODD than vignettes labeled as being about White children - aside from the labeled race, these vignettes were otherwise completely identical.
Probably the best article I’ve seen about this topic is Ballentine’s 2019 Understanding Racial Differences in Diagnosing ODD Versus ADHD Using Critical Race Theory, which is sadly behind a paywall. Since you can’t read it directly unless you find some way around that, I’ll provide a basic summary even though I can’t really do it justice, but the actual article goes into far more detail so if you can figure out a way to get ahold of it that would be better. Basically, though, epidemiological studies find that White kids have equal or even higher rates of ODD than Black kids, but real-world inspections of who actually gets diagnosed show that Black kids are disproportionately diagnosed with ODD, while White kids are disproportionately diagnosed with ADHD when showing similar symptoms, likely because of racist perceptions of Black kids as more dangerous or defiant than White kids even when their behavior is the exact same. This is especially bad because ODD diagnosis is associated with increased rates of incarceration and other negative outcomes, so it is pushing kids who are are already vulnerable towards those outcomes, and because a child who is diagnosed with ODD when they should’ve been diagnosed with ADHD instead won’t get ADHD treatment that they may need, and there are already racial disparities in access to ADHD treatment.
Both the papers linked operate under the assumption that ODD is a valid diagnosis, but honestly, I think it should be removed from the DSM entirely, for reasons previously stated - not only is it often applied in a racist way, the whole diagnostic criteria are based on enforcing compliance and someone who has been diagnosed with ODD is at high risk of not having their agency respected or their concerns taken seriously, because disagreements with authority and dissatisfaction with mistreatment become viewed as “symptoms” rather than completely normal and human.
#this is kind of a lazy overview of the topic but. its tumblr. like 2 people will read it probably#and i need to wrap it up and get back to writing my actual paper for school about it.#i just got so mad writing the paper i couldnt keep it to the word doc. you know how it is
21 notes
·
View notes
Text
By: Christina Buttons
Published: May 13, 2024
A guide to the international debate on youth medical transition, where medical authorities in the United States depart from a growing international consensus.
The world is reacting to the U.K.'s Cass Review and associated systematic evidence reviews, which found "remarkably weak" evidence supporting medical interventions for gender transition in minors. Released on April 9, 2024, the final report from the national gender clinic service for those under 18—following four years of meta-analyses of the available literature—dealt a major blow to the gender-affirming model of care and marked its termination in England.
NHS England, which commissioned the report, expressed gratitude to Dr. Hilary Cass and committed to implementing her recommendations. These advocate for primarily relying on psychotherapy to address gender-related distress in minors and discontinuing the use of puberty blockers as part of England’s publicly funded healthcare system. The NHS predicted the landmark review would have "major international importance and significance"—a prediction that has proven correct. Just one month later, we are already beginning to see its impact.
What’s New
Scotland and Wales
In response to the Cass Review, Wales and Scotland have joined England in halting new prescriptions of puberty blockers for minors under 18 diagnosed with gender dysphoria. Additionally, in Scotland, cross-sex hormones will not be available to those under 18. In the last few years, beyond the U.K., Sweden, Finland, and Denmark have adopted a more cautious approach by placing restrictions on medical interventions for the treatment of gender dysphoria in minors. Norway has also signaled intentions to follow a similar path.
Germany
Now, Germany has emerged as the latest country to initiate steps towards placing restrictions on gender transition treatments for minors. Earlier this week, the German Medical Assembly, a pivotal body representing medical professionals across the country, passed a resolution that calls for the restriction of puberty blockers, cross-sex hormones, and surgeries for gender dysphoric youth to strictly controlled research settings. Another resolution passed that stated minors should not be permitted to "self-identify" into a chosen sex without first undergoing a specialist child and adolescent psychiatric evaluation and consultation.
While national restrictions have not yet been formalized, experts in gender medicine research are describing this update as a “major development” — especially considering that Germany has been one of the most permissive countries on this issue.
Read the SEGM Analysis
Belgium
Additionally, in Belgium, leading physicians are advocating for significant reforms in the treatment protocols for gender dysphoria in children and adolescents. According to an April 2024 report authored by pediatricians and psychiatrists P. Vankrunkelsven, K. Casteels, and J. De Vleminck from Leuven, there is a pressing need to follow the precedents set by Sweden and Finland, where hormones are regarded as a last resort. Their findings and recommendations were published in a prestigious medical journal associated with Dutch-speaking medical faculties in Belgium and their alumni associations.
International Bodies
International bodies such as the United Nations (UN) have also responded to the Cass Review. The United Nations Special Rapporteur on violence against women and girls, Reem Alsalem, issued a statement on the UN’s website declaring that the Review’s recommendations are essential for protecting children, especially girls, from harm.
In addition, the European Society of Child and Adolescent Psychiatry (ESCAP), a prominent umbrella association of 36 Child and Adolescent Psychiatry societies worldwide, recently issued a policy statement on child and adolescent gender dysphoria. They urged healthcare providers to "not to promote experimental and unnecessarily invasive treatments with unproven psycho-social effects and, therefore, to adhere to the ‘primum-nil-nocere’ (first, do no harm) principle."
These responses stand in stark contrast to that of World Professional Association for Transgender Health (WPATH), a body-modification advocacy organization. WPATH emailed a statement to its subscribers in response to the Cass Review, vehemently rejecting its findings and adhering to its ideological beliefs. WPATH criticized the Cass Report as “harmful” and "rooted in a false premise" that suggests distressed children can be helped without "medical pathways.”
United States
In response to the Cass Review, the American Academy of Pediatrics (AAP) and the Endocrine Society (ES) recently provided statements to WBUR, doubling down on their endorsement of the gender-affirming model of care and medical interventions for minors. Both blamed “politics” for spreading “misinformation.” Meanwhile, prominent gender clinicians have expressed to WBUR that they are “perplexed and concerned” by these organizations’ statements, given the Cass Review’s findings.
WPATH, AAP, and ES continue to mislead the public by claiming that the gender-affirming model of care adheres to the principles of evidence-based medicine (EBM), despite clear evidence to the contrary. Their recommendations for medical interventions are not grounded in robust evidence but rather rely on "circular referencing" of each other’s guidelines, effectively creating a citation cartel.
Comprehensive Overview of the International Debate On Youth Transition by Country
In recent years, there has been an ongoing debate about the best approach for treating gender-distressed youth, addressing the global increase in young people, primarily adolescent females, seeking services from gender clinics. Countries with pediatric gender clinic services have shown varied responses, ranging from highly medicalized treatment pathways to approaches that prioritize psychotherapy.
Nations such as the UK, Sweden, Finland, and Denmark have taken unified steps to heavily restrict medical transitions for minors, aligning their guidance with the results of systematic evidence reviews, with Norway similarly indicating moves in this direction. Elsewhere, medical and health authorities remain divided on best practices, although there are signs of some reevaluating their positions on the medical transition of minors. This guide will highlight significant updates and changes observed in these practices over recent years.
The Netherlands
In the Netherlands, the birthplace of the Dutch Protocol—the highly medicalized approach to treating youth with gender dysphoria—is facing increased scrutiny. As of 2023, there is a growing debate within medical, legal, and cultural realms about the practice of youth gender transitions.
On February 15, 2024, the Dutch Parliament ordered an investigation into the physical and mental health outcomes of children who have been prescribed puberty blockers. Despite these developments, the guidelines for treating gender dysphoria have not yet been updated.
In April 2024, Amsterdam UMC, the Dutch clinic that pioneered youth gender transition practices, issued a statement in response to the Cass Report. The clinic commended several elements of the report but expressed disagreement with its conclusion that the evidence supporting the use of puberty blockers is insufficient.
In May 2024, one of the Netherlands' national newspapers profiled the new policy statement from The European Society of Child and Adolescent Psychiatry (ESCAP) that advocated for a non-medicalized approach to treating child and adolescent gender dysphoria.
Norway
In 2023, the Healthcare Investigation Board of Norway (Ukom) issued recommendations urging the Ministry of Health and Care to instruct the Directorate of Health to revise the national professional guideline for gender incongruence, drawing on systematic evidence reviews. Additionally, the Ukom report proposed classifying puberty blockers, as well as hormonal and surgical interventions for children and young people, as experimental treatments. This classification would subject these treatments to more stringent regulations regarding informed consent, eligibility, and outcome evaluation. However, Norway has not yet issued any explicit new guidelines following these recommendations.
Denmark
In July 2023, Ugeskrift for Læger, the journal of the Danish Medical Association, reported a significant shift in Denmark's approach to treating youth with gender dysphoria. Instead of receiving prescriptions for puberty blockers, hormones, or surgery, most young people referred to the centralized gender clinic now receive therapeutic counseling and support.
France
In 2022, the National Academy of Medicine in France advised exercising "the utmost medical caution" for the use of puberty blockers and cross-sex hormones for children and adolescents, citing the risk of regret. Despite this caution, the prescription of these treatments remains permissible at any age with parental authorization.
A 2023 poll by the Journal International de Médecine found 84% of healthcare professionals in France are in favor of a moratorium on the administration of hormonal treatments for trans-identified minors.
In March 2024, French senators released a 369-page report advocating for the cessation of cross-sex hormones and puberty blockers on minors. Based on the findings of this report, lawmakers have drafted a bill that is set to be debated on May 28, 2024.
Italy
In January 2023, the Italian Psychoanalytic Society (SPI) wrote a letter to Italian Prime Minister Giorgia Meloni, expressing "great concern" over the "ongoing experimentation" with drugs designed to halt puberty in children and calling for a "rigorous scientific discussion."
In March 2024, the Vatican’s doctrine office, after five years of preparation, released a report approved by Pope Francis that declared gender-related surgeries to be "a grave violation of human dignity."
In April 2024, five Italian medical organizations released a joint position paper on managing adolescent gender dysphoria. This document, which extensively references WPATH, supports the medical transition of minors.
Sweden
In 2022, Sweden's National Board of Health and Welfare declared that the potential harms of puberty blockers and gender-affirming hormone treatments for individuals under 18 years of age surpass the possible benefits for this demographic. The board recommended that such treatments should primarily occur within a research setting to better assess their effects on gender dysphoria, mental health, and quality of life among young people. Additionally, it noted that hormone treatments could still be administered in exceptional circumstances.
In April 2023, a systematic review conducted by researchers from Karolinska Institutet, University of Gothenburg, Umeå University, and the Swedish Agency for Health Technology Assessment and Assessment of Social Services was published in Acta Paediatrica. This review assessed the existing evidence on hormonal treatment for individuals under 18 years old with gender dysphoria. The researchers concluded that such interventions “should be considered experimental treatment rather than standard procedure.”
Finland
Finland was the first Western country to conduct a systematic review of the evidence for youth gender transition, that led to a significant update of its guidelines in 2020. Observations from Finnish gender clinics showed that hormone treatments do not typically improve—and can worsen—the functioning of gender-dysphoric youth. In response, the country's Council for Choices in Health Care revised its guidelines to emphasize psychosocial support as the primary approach and restricted hormonal interventions to exceptional cases. These interventions are permitted before age 18 only if the individual's cross-sex identity is confirmed as permanent and causes severe dysphoria, the child fully understands the significance, benefits, and risks of the treatments, and there are no contraindications.
In October 2023, Dr. Riittakerttu Kaltiala, a leading Finnish gender clinician and researcher at Tampere University Hospital, wrote an op-ed in The Free Press, titled "Gender-Affirming Care Is Dangerous. I Know Because I Helped Pioneer It.” She highlighted concerns about the practice of pediatric medical transition in the U.S. and the lack of solid evidence supporting the efficacy of medical transition in reducing suicide rates among young people.
In February 2023, a landmark study from Finland revealed low suicide rates among trans-identified youth and found no evidence of benefits from gender reassignment. The study showed that, after accounting for psychiatric needs, there was no statistically significant evidence that gender-referred youth have higher suicide rates compared to the general population. The authors concluded that the risk of suicide related to transgender identity and/or gender dysphoria "may have been overestimated."
England
In January 2020, National Health Service (NHS) England formed a Policy Working Group (PWG) to conduct an assessment of the existing research on the use of puberty blockers and feminizing/masculinizing hormones in children and young people with gender dysphoria. This was aimed at shaping a policy stance on their continued application. The findings from these reviews were released in March 2021.
In February 2022, the interim report to the Cass Review was published, which had been commissioned by NHS England to evaluate the Gender Identity Development Service (GIDS) at the Tavistock and Portman NHS Foundation Trust, the UK's only national clinic for children and adolescents with gender dysphoria. The review highlighted significant concerns about the clinical decision-making framework, noting a lack of robust evidence and consensus on the most effective treatments.
In July 2022, NHS England announced it would close GIDS in Spring 2023, which was delayed until Spring 2024. Two new regional hubs opened in London and the north of England to move away from a single-service model.
In October 2022, the NHS England issued new draft guidance following their systematic evidence review, stating that there is "scarce and inconclusive evidence to support clinical decision-making" for minors with gender dysphoria, and for most who present before puberty, it will be a "transient phase" requiring psychological support rather than medical intervention.
In March 2024, NHS England announced that it would end the prescription of puberty blockers at gender clinics for children due to insufficient evidence regarding their safety and effectiveness. These treatments will now only be accessible through clinical research trials.
On April 9, 2024, the final 388-page report of the Cass Review was published, along with 9 studies (8 of which were systematic evidence reviews) by the University of York.
Ireland
In March 2023, HSE published a review of the interim Cass Report to assess Gender Identity Services for children and young people in Ireland.
In April 2024, the Health Service Executive (HSE) announced the development of a new clinical program for gender healthcare, scheduled over the next two years. They also stated that the final report for the Cass Review will be included as part of this process.
Canada
In January 2024, Alberta announced the implementation of measures that significantly restrict medical transitions for minors. This policy establishes Alberta as the only province in Canada to enforce such limitations on gender transition procedures for individuals under 18. Under the new regulations, minors are prohibited from undergoing any gender-related surgeries, and those aged 16 and younger are prevented from accessing puberty blockers or cross-sex hormones.
United States
The three main organizations that have issued guidelines on youth medical transition include the American Academy of Pediatrics (AAP), the Endocrine Society (ES), and the World Professional Association for Transgender Health (WPATH). Other groups, such as the American Medical Association, have either publicly supported “affirming” medical practices without presenting evidence, or have aligned themselves with the guidelines set by one or more of these three organizations. Notably, none of these organizations have yet conducted systematic reviews of the evidence, which are designed to avoid selective inclusion of studies and biased interpretations.
Leaders at the American Academy of Pediatrics (AAP) ignored five resolutions from its members over four consecutive years, each urging that youth transition guidelines be aligned with findings from systematic evidence reviews. In August 2023, the AAP Board of Directors finally agreed to conduct their own systematic review of the evidence and consider updating its guidance. At the same time, the Board "voted to reaffirm" its 2018 policy statement on gender-affirming care.
In 2022, Florida took the lead as the first state to curtail the widespread administration of hormonal and surgical interventions to the increasing number of gender-dysphoric youth. Early in the year, Florida’s public health authority commissioned an overview of existing English-language systematic evidence reviews. Based on the findings from this review, the Florida Boards of Medicine subsequently decided to halt the provision of gender-transition services to minors, unless conducted within research settings across the state.
As of April 2024, 24 states have now placed age restrictions on hormonal and surgical sex-trait modification interventions for minors. Democrats in four states (Texas, Louisiana, New Hampshire, and Maine) have voted in favor of age restriction laws or against turning their states into hormone sanctuaries.
Spain
In 2018, the Spanish Association of Paediatrics and the Spanish Society of Paediatric Endocrinology published a statement endorsing youth medical transition.
In 2022, the directors of Spain’s Society of Psychiatry, Association of Child and Adolescent Psychiatry, and Society of Endocrinology expressed their opposition to a proposed law that would enable minors to access medical transition procedures. El Mundo, the second-largest daily newspaper in Spain, highlighted this controversy on its front page with the headline: “Psychiatrists explode against the Trans Law: It can bring a lot of pain and regret to many people.”
Australia and New Zealand
In August 2021, The Royal Australian and New Zealand College of Psychiatrists (RANZCP) issued its first position statement focused on the mental health needs of individuals with gender dysphoria, followed by an update in September 2021. This statement was the first from a professional body that did not explicitly endorse a gender-affirming approach.
Australia has experienced considerable debate in recent years regarding youth medical transition. This topic has been extensively covered by Australian journalist Bernard Lane for his Substack, Gender Clinic News.
New Zealand's Ministry of Health was expected to release an evidence brief in early 2024, aimed at reviewing the current evidence on the safety of puberty blockers. Although the publication has been delayed, it is anticipated to be released soon.
In April 2024, Guardian Australia reported that neither New South Wales or Victoria have plans to make changes to puberty blocker prescribing or accessibility as a result of the Cass Review.
International Bodies
In July 2023, for the first time, international experts publicly weighed in on the American debate over "gender-affirming care." 21 leading experts on pediatric gender medicine from eight countries wrote a letter expressing disagreement with US-based medical organizations over the treatment of gender dysphoria in youth, urging them to align their recommendations with unbiased evidence “rather than exaggerating the benefits and minimizing the risks.”
In January 2024, the World Health Organization (WHO) updated its announcement on developing healthcare guidelines for “trans and gender diverse (TGD) people.” The WHO stated in an FAQ that it would not be making recommendations that impact minors. Importantly, they made the following admission: "[O]n review, the evidence base for children and adolescents is limited and variable regarding the longer-term outcomes of gender affirming care for children and adolescents" (January, 2024).
Further Information
For additional information, one of the studies that contributed to the Cass Review conducted a survey of European gender services for children and adolescents from September 2022 to April 2023. Additionally, a Wikipedia page provides an overview of the "legal status of gender-affirming healthcare" (for adults) in various countries worldwide.
If you found this guide helpful, I am working on developing an information-based website that will feature up-to-date data, counterarguments to activist claims, explainers on research, and useful resources related to gender pseudoscience.
#Christina Buttons#systematic review#Cass report#Cass review#gender affirming care#gender affirming healthcare#gender affirmation#medical scandal#medical corruption#medical malpractice#head in the sand#willful ignorance
13 notes
·
View notes
Text
At about the time her daughter reached the age of 12, American health executive Laurie saw her once confident, happy child turning into someone she barely recognized. At first, she thought a bad case of adolescent angst was to blame.
Initially, her daughter had trouble sleeping and grappled with episodes of self-loathing and anxiety, but by the time she was 14, she had started cutting herself and was having suicidal thoughts.
Without Laurie knowing, she had been sneaking away her confiscated smartphone and spending hours online at night, trawling through posts about self-harm and eating disorders on social media platforms.
"One day she said to me: 'Mom, I'm going to hurt myself badly if I don't get help,'" Laurie said as she described the mental health crises that have plagued her daughter for the last two years, disrupting her education and devastating the family's finances.
She asked to use only her first name in order to protect the identity of her daughter.
Paying for her daughter's care - therapists, a psychiatrist, and multiple residential treatment facilities across the country - has nearly bankrupted Laurie, who recently sold her house in California and moved to a cheaper home in another state.
In August, she filed a lawsuit on behalf of her daughter against the social media platforms she blames for the ordeal: Instagram, Snapchat and TikTok.
The case is one of dozens of similar U.S. lawsuits which argue that, when it comes to children, social media is a dangerous product - like a car with a faulty seat-belt - and that tech companies should be held to account and pay for the resulting harms.
12 notes
·
View notes
Text
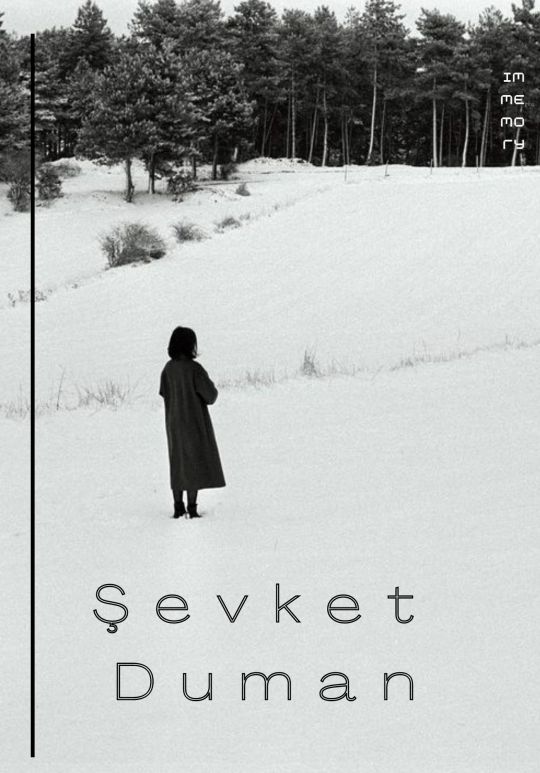







My name is Şevket, I was born in Istanbul in 1991. After graduating from medical school in Izmir, I became a child and adolescent psychiatrist in 2021.
I believe that art is born at the intersection of the body and psyche, desire and demand, subjectivity and objectivity, the internal and external.
My works are a manifestation of what cannot be expressed in words, the emotions that can be felt only through the imaginary.
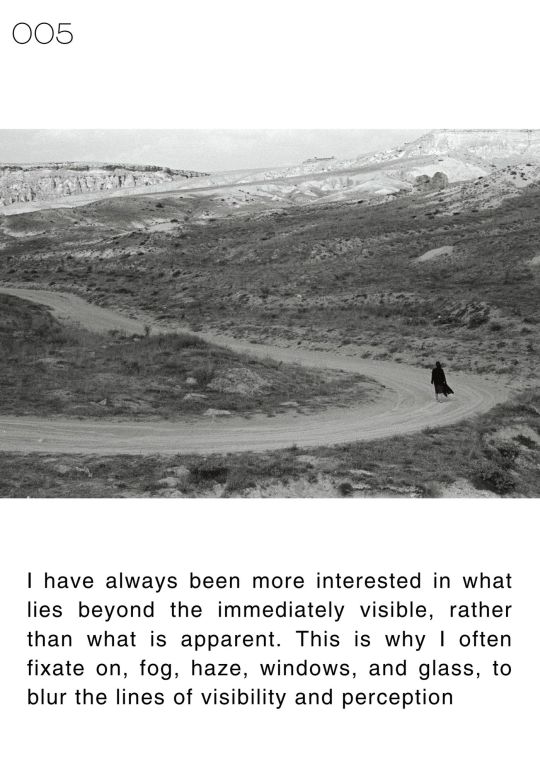
I have always been more interested in what lies beyond the immediately visible, rather than what is apparent. This is why I often fixate on, fog, haze, windows, and glass, to blur the lines of visibility and perception.
12 notes
·
View notes
Note
Not an ASPD culture thing, but an interesting study I found. (here: https://pubmed.ncbi.nlm.nih.gov/16629347/)
Basically, the study took a sample of a population who expressed antisocial behaviors and may have been diagnosed with ASPD. While most had evidence of a conduct disorder prior to 15 years of age, about 2.3% of people who otherwise would have met the criteria for ASPD did not show evidence of conduct disorder before 15 years of age (at least, this is how I understood the study).
I find this really interesting, since it provides some evidence to a thought I had in the back of my head that it feels kind of really weird that a diagnosis of ASPD requires a separate diagnosis, especially since there's some issues with conduct disorder as it's defined and diagnosed right now (ex.: doesn't take into account many different forms of aggression that may be shown instead of physical or sexual aggression). I feel like ASPD requiring evidence of conduct disorder prior to the age of 15 ignores the fact that a lot of people with ASPD may not have shown evidence of it, because they had to mask and act "normal" in order to avoid getting harmed in some way.
Like, as it stands right now (to my understanding), you can have every single symptom of ASPD, but if you didn't show signs of conduct disorder prior to the age of 15, you can't/won't be diagnosed, and... that just seems extremely fucking weird to me. Sure, maybe the majority of pwASPD will have shown evidence of conduct disorder in adolescence, but at least some won't, and a not-insignificant chunk of people who may otherwise have been diagnosed with ASPD are being totally ignored or brushed off because of that one criteria.
I agree entirely on this. One of the professionals I work with was leaning away from ASPD because of this exact issue. However, upon talking to my psychiatrist on a day when my symptoms were more flared and telling her honestly about how I feel about people, as well as doing 2 different screener tests, I did receive a diagnosis.
That said, my psych is really good at listening to her patients, better than most doctors I've ever met. Most doctors, I think, would have missed my ASPD because of the lack of conduct disorder criteria being met.
I will note for anyone working on a diagnosis that you don't have to have actually been diagnosed with conduct disorder as a child, you just have to (when talking through what your childhood was like) have had symptoms that could have qualified you for a conduct disorder diagnosis.
#aspd-culture-is#actually antisocial#actually aspd#antisocial personality disorder#aspd#aspd awareness#aspd culture#aspd traits#aspd culture is#anons welcome
11 notes
·
View notes
Last Seen Blogs

endeverstar
mouthwords are not a superior way to communicate

theopinionyoudidntaskfor
The Opinion You Didn't Ask For

lemontreehotelamritsar
Untitled

medicine-san
little star

usoppsweave
usopp’s got bundles, ok?