#Healthcare California
Text
Alien and Alive at 1,000 Years [Video]
0 notes
Text

210 notes
·
View notes
Text
"Bria Peacock chose a career in medicine because the Black Georgia native saw the dire health needs in her community — including access to abortion care.
Her commitment to becoming a maternal health care provider was sparked early on when she witnessed the discrimination and judgment leveled against her older sister, who became a mother as a teen. When the Supreme Court overturned Roe v. Wade in 2022, Peacock was already in her residency program in California, and her thoughts turned back to women like her sister.
“I knew that the people — my people, my community back home — was going to be affected in a dramatic way, because they’re in the South and because they’re Black,” she said.
But even though Peacock attended the Medical College of Georgia, she’s doing her obstetrics and gynecology residency at the University of California-San Francisco, where she has gotten comprehensive training in abortion care.
“I knew as a trainee that’s what I needed,” said Peacock, who plans to return to her home state after her residency.
Ever since the Supreme Court decision, California has worked to become a sanctuary for people from states where abortion is restricted. In doing so, it joins 14 other states, including Colorado, New Mexico, and Massachusetts. Now, it’s addressing the fraught issue of abortion training for medical residents, which most doctors believe is crucial to comprehensive OB-GYN training.
A law enacted in September [2023] makes it easier for out-of-state trainees to get up to 90 days of in-person training under the supervision of a California-licensed doctor. The law eliminated the requirement for a training license and also permitted training at programs such as Planned Parenthood that are affiliated with accredited medical schools.
“By allowing physician residents to come to California, where there are more opportunities for abortion training, and by allowing them to be reimbursed for this work, we’re sending a message that abortion care is health care and an essential part of physician training,” said Lisa Folberg, CEO of the California Academy of Family Physicians, which supported the bill.
The question of how to provide complete OB-GYN training promises to become more urgent as the effects of abortion bans on medical education becomes clear: 18 states restrict or ban abortion to the point of effectively stripping 20% of OB-GYN medical residents of the opportunity to get abortion training, according to the Ryan Residency Training Program in Abortion and Family Planning. That’s 1,354 residents this year out of 5,962 OB-GYN residents nationwide.
The restrictions in some cases aim to reach beyond state borders, spooking medical students and residents who fear hostility from anti-abortion groups and right-wing legislators...
Pamela Merritt, executive director of Medical Students for Choice, pointed to a Kansas law that requires repayment of state medical school scholarships — with 15% interest — if residents perform abortions or work in clinics that perform them, except in cases of rape, incest, or a medical emergency.
Doctors point out that abortion training is not just about ending pregnancies. Peacock recalled a patient who started hemorrhaging badly shortly after a healthy delivery. Peacock and her team at UCSF performed a dilation and curettage — a procedure commonly used to terminate pregnancy.
“If we did not have that skill set, and the patient continued to bleed, it could have been life-taking,” said Peacock, chief OB-GYN resident at UCSF...
Peacock, for her part, is adamant about returning to Georgia, where abortions are banned after six weeks. “I’m still going to provide abortions, whether that’s in Georgia or I need to fly to a different state and work in abortion clinics for a week out of the month,” she said. “It would definitely be a big part of my work.”"
-via The 19th, January 2, 2024
#abortion#bodily autonomy#abortion rights#reproductive rights#reproductive justice#united states#us politics#california#georgia#medical student#residency#medical school#healthcare#healthcare access#pro choice#abortion is healthcare#womens rights#trans rights too let's just make that clear#medical training#abortion care#abortion bans#abortion access#doctors#medicine#gynecology#obstetrician#obstetrics and gynecology#gynecologist#good news#hope
179 notes
·
View notes
Text
⚠️TRANS PEOPLE WITH CALIFORNIAN HEALTHCARE: YOUR SURGERIES ARE FREE⚠️
This official page from the California Department of Insurance states "health insurance policies are prohibited from arbitrarily excluding coverage for gender affirmation services including (but not limited to) hormone therapy, mental health services and surgical services."
KNOW YOUR RIGHTS!
#trans heathcare#healthcare#california#american healthcare#american health insurance#american health system#transgender tips#transgender health#trans health#trans issues#trans law#trans laws#trans legislation#transgender laws#top surgery#top surgeon#bottom surgery#transgender
280 notes
·
View notes
Text



Healthcare Organization (Skyline Design x NBBJ)
#art#california#design#frutiger aero#frutiger eco#healthcare#graphic design#leaves#nature#nbbj#photography#skyline design#trees#usa#us
38 notes
·
View notes
Text
The California Faculty Association is going on Strike against the California State University system!
They are fighting for:
Better pay so they can afford to live in the state they're teaching in.
More manageable workloads to allow for effective student support.
Expanded counseling services to improve students' access to mental healthcare.
All of which should be reasonable, considering:

The CSU's expendable net assets have grown from $3.3 billion in 2012, to $8.1 billion in 2022.
If CSU management funded our bargaining proposals from their annual cash surpluses, they wouldn't even have to draw from these reserves.
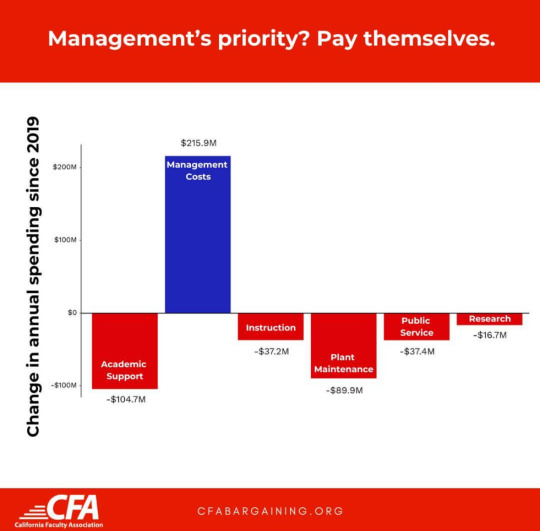
Teachers can do the math, but CSU management is hoping you can't.
#cfa strike#teachers#labor#unions#strikes#education#mental healthcare#california state university#csu#california faculty association#cfa#solidarity forever
67 notes
·
View notes
Video
Childbirth Is Deadlier for Black Families Even When They’re Rich, Expansive Study Finds
https://www.nytimes.com/interactive/2023/02/12/upshot/child-maternal-mortality-rich-poor.html
In the United States, the richest mothers and their newborns are the most likely to survive the year after childbirth — except when the family is Black, according to a groundbreaking new study of two million California births. The richest Black mothers and their babies are twice as likely to die as the richest white mothers and their babies.
Research has repeatedly shown that Black mothers and babies have the worst childbirth outcomes in the United States. But this study is novel because it’s the first of its size to show how the risks of childbirth vary by both race and parental income, and how Black families, regardless of their socioeconomic status, are disproportionately affected.
“This is a landmark paper, and what it makes really stark is how we are leaving one group of people way behind,” said Atheendar Venkataramani, a University of Pennsylvania economist who studies racial health disparities and was not involved in the research.
The study, published last month by the National Bureau of Economic Research, includes nearly all the infants born to first-time mothers from 2007 to 2016 in California, the state with the most annual births. For the first time, it combines income tax data with birth, death and hospitalization records and demographic data from the Census Bureau and the Social Security Administration, while protecting identities.
That approach also reveals that premature infants born to poor parents are more likely to die than those born into the richest families. Yet there is one group that doesn’t gain the same protection from being rich, the study finds: Black mothers and babies.
Are you a Black parent who recently gave birth? Tell us about it.
“It suggests that the well-documented Black-white gap in infant and maternal health that’s been discussed a lot in recent years is not just explained by differences in economic circumstances,” said Maya Rossin-Slater, an economist studying health policy at Stanford and an author of the study. “It suggests it’s much more structural.”
If anything, the study’s findings understate the dangers of childbirth in much of the United States, a variety of researchers said, because California’s maternal mortality rate has been declining over the last decade, as deaths have gone up in the rest of the country.
Rich Families Have More Premature Babies. But Those Babies Are Less Likely to Die.
Perhaps unexpectedly, babies born to the richest 20 percent of families are the least healthy, the study finds. They are more likely to be born premature and at a low birth weight, two key risk factors for medical complications early in life. This is because their mothers are more likely to be older and to have twins (which are more common with the use of fertility treatments), the researchers found.
But even with those early risk factors, these babies are the most likely to survive both their first month and first year of life.
A similar pattern emerged when it came to the health of the parents themselves: Rich and poor mothers were equally likely to have high-risk pregnancies, but the poor mothers were three times as likely to die — even within the same hospitals. Rich women’s pregnancies “are not only the riskiest, but also the most protected,” the paper’s authors wrote.
A pair of charts showing the relationship between a mother’s income and rates of premature births and infant mortality. The first chart shows that as a woman’s income rises, the likelihood of preterm birth rises. The second chart shows that as a woman’s income rises, rates of infant mortality fall.
This finding suggests that the American medical system has the ability to save many of the lives of babies with early health risks, but that those benefits can be out of reach for low-income families.
Resources outside the medical system also play a role. Separate research on children with leukemia, for example, has found that even when treated at the same hospital and using the same protocol, those from high-income families fared better than those from poorer families.
“It’s not just about the medical care that kids are receiving,” said Anna Aizer, a health economist at Brown University. “There are all sorts of other things that go into having healthy babies. If you’re a higher-income mom who can take time off work, who doesn’t have to worry about paying rent, it’s not surprising you’ll be able to manage any health complications better.”
Money Protects White Mothers and Babies. It Doesn’t Protect Black Ones.
The researchers found that maternal mortality rates were just as high among the highest-income Black women as among low-income white women. Infant mortality rates between the two groups were also similar.
Two charts showing the relationship between a mother’s income and rates of infant mortality by race. The first chart shows that as a Black mother’s income increases, the rate of infant mortality generally drops. The same is true in the second chart for white mothers, but at much lower rates than for Black women.
The richest Black women have infant mortality rates at about the same level as the poorest white women.
The babies born to the richest Black women (the top tenth of earners) tended to have more risk factors, including being born premature or underweight, than those born to the richest white mothers — and more than those born to the poorest white mothers. It’s evidence that the harm to Black mothers and their babies, regardless of socioeconomic status, begins before childbirth.
“As a Black infant, you’re starting off with worse health, even those born into these wealthy families,” said Sarah Miller, a health economist at the University of Michigan. She was an author of the study with Professor Rossin-Slater and Petra Persson of Stanford, Kate Kennedy-Moulton of Columbia, Laura Wherry of N.Y.U. and Gloria Aldana of the Census Bureau.
Black mothers and babies had worse outcomes than those who were Hispanic, Asian or white in all the health measures the researchers looked at: whether babies were born early or underweight; whether mothers had birth-related health problems like eclampsia or sepsis; and whether the babies and mothers died. There was not enough data to look at other populations, including Native Americans, but other research has shown that they face adverse outcomes nearing those of Black women and infants in childbirth.
Charts that show the relationship between a mother’s income by group. The groups are Hispanic mothers and Asian mothers. Generally, rates for Hispanic mothers and Asian mothers track more closely with those of white mothers than Black mothers.
Even before the new paper, research found that Black women with the most resources, as measured by education and class mobility, did not benefit during childbirth the way white women did. The new study demonstrates that disparities are not explained by income, age, marital status or country of birth. Rather, by showing that even rich Black mothers and babies have a disproportionately higher risk of death, the data suggests broader forces at play in the lives of Black mothers, Professor Rossin-Slater said.
“It’s not race, it’s racism,” said Tiffany L. Green, an economist focused on public health and obstetrics at the University of Wisconsin-Madison. “The data are quite clear that this isn’t about biology. This is about the environments where we live, where we work, where we play, where we sleep.”
There is clear evidence that Black patients experience racism in health care settings. In childbirth, mothers are treated differently and given different access to interventions. Black infants are more likely to survive if their doctors are Black. The experience of the tennis star Serena Williams — she had a pulmonary embolism after giving birth, yet said health care professionals did not address it at first — drew attention to how not even the most famous and wealthy Black women escape this pattern.
But this data shows how the effects of racism on childbirth start long before people arrive at the hospital, researchers across disciplines say, and continue after they leave. The stress of experiencing racism; air pollution in Black communities; and inequitable access to paid family leave, for example, have all been found to affect the health of mothers and babies.
“Even when it’s not about the direct disrespect that’s going on between the patient and the care provider, there are many ways systemic racism makes its way into the well-being of a pregnant or birthing person,” said Dr. Amanda P. Williams, the clinical innovation adviser at the California Maternal Quality Care Collaborative.
California Is a Best-Case Scenario. It Still Lags Behind Other Wealthy Parts of the World.
Many parts of the United States have much higher maternal mortality than California, and fewer policies to support families. California was the first state to offer paid family leave. It has one of the most generous public insurance programs for pregnant women. The state has invested in specific programs aimed at reducing maternal deaths and racial disparities in childbirth.
Yet even in this best-case American scenario, mothers and babies fare worse compared with another rich country the researchers examined: Sweden. At every income level, Swedish women have healthier babies. This held true for the highest-income Swedish women and those from disadvantaged populations, including low-income and immigrant mothers.
A pair of charts showing the relationship between birth outcomes in Sweden and California. The first chart shows that Swedish women have heavier babies at every income level. The second chart shows that Swedish women have lower rates of preterm birth than California women at every income level.
Swedish women have heavier babies at every income level ...
... and far lower instances of preterm birth.
In the United States, earning more regularly translates into superior access to the fastest, most expensive health care. But even with that advantage, the richest white Californians in this study still gave birth to less healthy babies than the richest Swedish women. Their newborns were more likely to be premature or underweight. The two groups had roughly equal maternal death rates.
“That finding really does strongly suggest that it’s something about the care model,” said Dr. Neel Shah, chief medical officer of Maven Clinic for women’s and family health and a visiting scientist at Harvard Medical School. “We have the technology, but the model of prenatal care in the United States hasn’t really gotten an update in the last century.”
A chart showing where the U.S. falls on the spectrum of maternal mortality among peer countries. The U.S. is last in a ranking that includes New Zealand, Norway, the Netherlands, Germany, Sweden, Switzerland, Australia, Britain, Canada and France, in that order.
Paper
Sweden, like most European countries, has universal health insurance with low out-of-pocket costs for the patient. Midwives deliver most babies in Sweden and provide most of the prenatal care, which has been linked to lower C-section rates and lower rates of preterm births and low birth weights. It has long paid leaves and subsidized child care.
Like California, Sweden has also started targeted efforts to reduce maternal deaths. When officials there recognized that African immigrants giving birth were dying more frequently, they began piloting a “culture doula” program, with doulas who were immigrants themselves helping pregnant women navigate the country’s health system.
Local maternal health programs could begin to help reduce racial disparities in the United States, too, as could a more diverse medical workforce, research suggests. Nonprofits and universities have experimented with ways to address racism and poverty, with programs like cash transfers for low-income pregnant women and initiatives to improve the environments of Black communities.
By the time a woman is pregnant, Professor Miller said, “it’s almost too late.”
“Health is going to depend on exposures throughout her life, health care she’s received, environmental factors,” she said. “A lot goes on prior to the pregnancy that affects the health of the mother and baby.”
About the data
The researchers collected birth certificate data for all babies born to first-time mothers in California from 2007 to 2016. The final sample included 1.96 million births. They collected hospitalization and death records for babies for one year from the California Department of Health Care Access and Information, as well as hospitalization records for mothers for nine months before the birth and a year after. They collected maternal death records for the same period from a Social Security Administration data set. They provided birth records to the Census Bureau, which assigned anonymous identification codes to access I.R.S. data and determine new parents’ incomes in the two years before the birth. (Infant mortality records were available only until 2012. Maternal mortality data covers a longer period than in government records, which generally include data for six weeks after a birth, and most likely capture some deaths unrelated to childbirth.)
In Sweden, the researchers collected similar health and mortality data from the National Board of Health and Welfare. The final sample included 463,865 births. Analogous maternal morbidity data was unavailable. They linked babies to their parents and collected parents’ demographic and financial data from Statistics Sweden. Sweden has a smaller gap between the highest and lowest earners than the United States.
#tiktok#article#new york times#Healthcare#Health Care#infant mortality#california#reproductive justice#reproductive freedom#reproductive rights#reproductive choice#reproductive health#health news#medical studies
106 notes
·
View notes
Text
January 19th 2024
"In California, a person who tests positive for Covid and has no symptoms does not need to isolate, according to new state health guidelines. People who test positive and have mild symptoms, meanwhile, can end isolation once their symptoms improve and they’ve been fever-free for 24 hours without medication — even if that point arrives in less than five days."
Petition to Demand California Reinstate Isolation Guidelines for ALL Positive SARS-2 Cases:
#pandemic#covid#covid pandemic#covid news#mass disabling event#long hual covid#disability#covid19#covidー19#sars cov 2#testing#covid testing#public health#healthcare#health#California
13 notes
·
View notes
Text
Molly Sprayregen at LGBTQ Nation:
In an effort to promote her anti-trans “Protect Children’s Innocence Act,” Rep. Marjorie Taylor Greene (R-GA) hurled insults at a mother who has spent years fighting for the right to affirm her trans daughter’s identity.
Greene reposted an article from the far-right Dallas Express News — a publication the Texas Observer has described as a “‘pink slime’ media site that launders conservative propaganda” — that claimed Anne Georgulas could soon gain the right to “castrate” her daughter without her ex-husband Jeff Younger’s permission “because she believes her son is transgender.”
Greene posted in response that her bill would “stop this evil mentally ill mother from castrating her son.”
“Over 70% of Americans agree with my bill. There’s no excuse as to why my bill has not moved,” Greene added. She did not share where the 70 percent stat came from.
The story in the Dallas Express News is about well-known anti-trans activist Jeff Younger — who has been engaged in years of legal battles with Georgulas over how to raise their trans daughter, Luna, whom he consistently misgenders and deadnames.
[...]
According to the Dallas Express, Georgulas has since moved with her two children to California, where she will have a hearing on April 25 likely regarding access to best-practice gender-affirming care for Luna based on her age, though the far-right publication claims Georgulas is seeking permission to “castrate” her. (Trans youth almost never undergo gender-affirming surgery).
In 2022, California Gov. Gavin Newsom (D) signed a bill protecting transgender youth and their families fleeing prosecution from states that criminalize gender-affirming care, making the state a sanctuary for trans kids and their families.
[...]
Luna’s story has been used by the conservative media over the years to promote the idea that children are being forced by parents to transition medically. The claim that Younger is trying to “save” his child from hormones and surgery, unlikely treatments for a child her age, continues to be perpetuated.
Greene’s “Protect Children’s Innocence Act” would make it a Class C felony to provide gender-affirming care to trans minors, make it more difficult for trans adults to access gender-affirming care by banning some health care programs from covering it, and ban medical schools from teaching about gender-affirming care.
In November, Greene lied during testimony in the House when she claimed that there are “many young people that made the tragic mistakes of having mastectomies, having castrations done to them, having genital mutilation surgeries when they were still in their early, uh, teens, um, maybe even before they were teenagers.”
As stated above, genital gender-affirming surgery is not performed on minors in the U.S., much less on prepubescent children. Some older teens can sometimes get mastectomies if they meet stringent requirements, but that’s rare.
Gender-affirming care for pre-pubescent children involves allowing them to wear the kinds of clothes that they want, calling them by a name and pronouns that affirm their gender identities, and generally supporting their self-expression. Puberty blockers — which have been shown to reduce lifelong suicide risk among trans people — are prescribed after the onset of puberty, and hormone replacement therapy is an option for some trans teens who are a bit older.
Vile anti-trans bigot Congresswoman Marjorie Taylor Greene (R-GA) continues her campaign for her transphobic "Protect Children’s Innocence Act", this time by attacking Anne Georgulas for raising her trans daughter Luna Younger, who has since moved to California to protect her daughter from her anti-trans father Jeffrey.
#Marjorie Taylor Greene#Luna Younger#Jeffrey Younger#Anne Georgulas#Transgender Children#Transgender#LGBTQ+#Anti Trans Extremism#Gender Affirming Healthcare#Protect Children's Innocence Act#Transgender Sanctuary State#California SB107
5 notes
·
View notes
Text
This is pure and simple insanity! What the hell is wrong with the voters in California who are putting their state on the road to a complete collapse?
#leadership#government#democrats#save america#illegal immigration#free healthcare#budget crisis#fiscal responsibility#California exodus
8 notes
·
View notes
Text
RFK Jr. Wants to Make It Easier for Doctors to Spread Medical Lies Mother Jones [Video]
1 note
·
View note
Text
California Gets One Step Closer to Universal Healthcare
4 notes
·
View notes
Text
California is helping to provide abortions to people in red states. They can offer help for travel when needed. Please share this for those in need
#america#american politics#abortion#abortion ban#abortion access#california#womens rights#mysogyny#healthcare#politics#health
17 notes
·
View notes
Text
What is a Bookkeeper’s Role in HIPAA-Compliant Businesses?
Healthcare organizations are expected to save and maintain lives, but as businesses, they must be HIPAA (Health Insurance Portability and Accountability Act) compliant. This is required for healthcare businesses in the United States, a legal requirement designed to protect the privacy and security of patient’s personal health information (PHI).
HIPAA compliance creates a framework for safeguarding sensitive health information for a reliable healthcare ecosystem that can only be promoted by trustworthy professionals.

These professionals in businesses like the top bookkeepers play a crucial role in protecting businesses by utilizing their expertise and ethical practices. Here are some ways in which reliable bookkeepers help and support HIPAA-compliant businesses:
Security
To protect financial records and PHI from unauthorized access, theft, or breaches, bookkeepers must implement appropriate security measures. This includes utilizing secure computer systems, encrypted data storage, and password protection for financial software and databases.
Confidentiality
When handling financial records containing protected health information (PHI), bookkeepers must maintain strict confidentiality. Any individually identifiable health information, such as medical records, payment information, and insurance information, is considered PHI. Bookkeepers should ensure that access to such information is limited to authorized personnel only.
Record Retention and Disposal
Bookkeepers should adhere to HIPAA guidelines for the retention and disposal of financial records that contain PHI. These guidelines specify the minimum retention period for different types of records and the secure destruction methods for disposing of sensitive information.
Monitoring and Auditing
Bookkeepers may be involved in auditing and monitoring financial transactions to ensure HIPAA compliance. This includes reviewing financial records on a regular basis, identifying any discrepancies or irregularities, and reporting any suspected violations to appropriate personnel.
Training and Awareness
Bookkeepers should receive HIPAA training and be aware of the specific requirements for financial transactions and record-keeping. They must understand the significance of maintaining PHI privacy and security, as well as how to deal with any potential breaches or incidents.
Business Associate Agreements (BAAs)
Under HIPAA regulations, bookkeepers who work with HIPAA-compliant businesses may be considered business associates. Any entity that performs services on behalf of a covered entity (such as a healthcare provider) and has access to PHI is considered a business associate. Bookkeepers should have a signed BAA with the covered entity outlining their responsibilities and obligations in terms of PHI protection.
The Bottomline
Overall compliance with HIPAA is a collaborative effort that involves numerous stakeholders, including healthcare providers, covered entities, and business associates.
Just like any other industry, efficient bookkeeping in healthcare is an essential component for effortless accounting processes to efficiently run a business. Hence it is a must to entrust a healthcare system’s finances only to trustworthy bookkeepers for long-term success.
So if you are a healthcare business owner or a healthcare business manager now is the time to get started! Learn how! Schedule a call now!
#best business blog#recordkeepers#bookkeepers#small business solutions#business tips#full service bookkeeping#healthcare support#los angeles#california
9 notes
·
View notes
Text
An acquaintance from California asked me about proposition 29, so I did some research.
Anyone in California has probably seen those “no on prop 29” ads. Here’s the thing:

This is an effort at equality and transparency. It will SAVE people’s lives and it will do so with equity.
So why is it getting so much negative criticism?
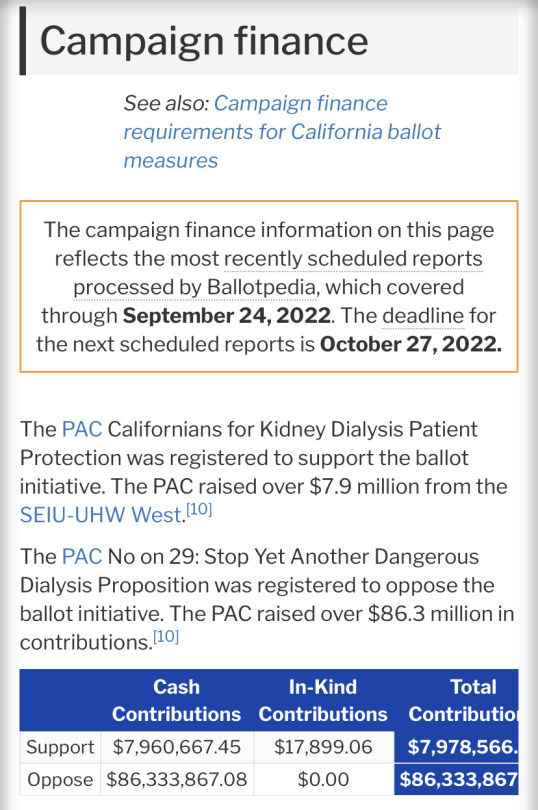
Because the people opposing it are paying over 12 times as much for advertising than the supporters are.
This makes the following statement from one of the opposing organizations particularly ironic:

The more astute among you may have seen the reason why this kind of blatant hypocrisy comes as no surprise: the opposition has the support of the Republican Party, a group that is famous for its blatant hypocrisy and its emotionally-charged and manipulative advertising (see my post re. The correlation between conservative groups and narcisistic sociopathy).
Because the clinics have to provide the dialysis experts at their expense, their opposition was to be expected. But I don’t know how they thought they could get away with spending more on this one campaign than UHW spent for all three of the proposed measures.
Threatening the shutdown of clinics over this measure is extortion, plain and simple. Any of my followers in California should make them regret that come voting time.
Sources:
Most of my info on Opposition and funding for this measure came from ballotpedia, but I also read the actual text of the proposition to verify.
If I missed something, don’t be afraid to tell me! It’s important we get facts and not propaganda, especially when it comes to things like this.
26 notes
·
View notes

Last Seen Blogs

the-smeck-group
Wishes mean nothing, but they're all I have!
the-smeck-group
Wishes mean nothing, but they're all I have!

iris-echos
Echo

sclairy
S.CLAIRY , 100% Made in Italy Luxury Handpainted Porcelain
sclairy
S.CLAIRY , 100% Made in Italy Luxury Handpainted Porcelain