#Healthcare
Text
"Cigna tracks every minute that its staff doctors spend deciding whether to pay for health care. Dr. Debby Day said her bosses cared more about being fast than being right: “Deny, deny, deny. That’s how you hit your numbers,” Day said.
...
As ProPublica and The Capitol Forum reported last year, Cigna built a computer program that allowed its medical directors to deny certain claims in bulk. The insurer’s doctors spent an average of just 1.2 seconds on each of those cases.
...
Some of the more astonishing problems that Day spotted have stayed with her. In a case involving a newborn who needed an epilepsy evaluation, Day noticed that a Cigna nurse had listed the mother’s name as the patient, rather than the baby’s. Day fixed that mistake, avoiding what certainly would have been a denial. In another case, a nurse recommended denying payment for an ultrasound of the neck because the treatment wasn’t medically necessary. But the nurse had gotten the body part wrong. It was a hip that was injured, and the imaging was needed. An appeal that landed on Day’s desk involved Cigna’s decision to reject payment for a test because it wasn’t medically necessary for a patient with a sexually transmitted disease. But Day figured out that the patient had toenail fungus, not an STD.
Day said her bosses didn’t want to hear that she was catching errors. By October 2020, Cigna had placed Day on a performance improvement plan that required her to raise her “productivity level” — referring to the score on the dashboard — to at least 70%, which would be a significant jump for her but was slightly below the median for medical directors. The company made the consequences crystal clear: If she failed to successfully complete the plan, she could be terminated."
https://www.propublica.org/article/cigna-medical-director-doctor-patient-preapproval-denials-insurance
232 notes
·
View notes
Text
Alberta Health Services is investigating after an undocumented woman says she was denied an emergency C-section at an Edmonton hospital last month.
Perla Estrada, 35, said a doctor told her to go to the hospital on March 25 after an ultrasound revealed she had low amniotic fluid and needed a C-section.
She said at the Royal Alexandra Hospital, she was told she had to pay $5,000 upfront for the procedure and that no doctor there would see her unless she did so.
As an undocumented person without medical insurance, Estrada said she expected to pay for the cost of her hospital care after the birth, but she did not have enough money to pay the amount upfront.
She later went to the Misericordia Community Hospital, where she had the C-section and gave birth to her daughter Violet. [...]
Continue Reading.
Tagging: @newsfromstolenland, @abpoli
#cdnpoli#healthcare#healthcare access#immigration#racism#xenophobia#Edmonton#Alberta#Royal Alexandra Hospital#reproductive rights#reproductive health
60 notes
·
View notes
Text

Midwife
“Midwife with child in Oslo, Norway.” - via Wikimedia Commons
#wikipedia#wikipedia pictures#medicine#medcore#medicalcore#medicore#medical#medical care#postnatal care#healthcare#healthcare professionals#healthcare provider#pediatrics#hospitals#hospital#hospitalcore#hospital aesthetic#medical aesthetic#oslo#norway#people#nursecore#nursing
34 notes
·
View notes
Text
You are your own best reason to exist.
#quotes#quote#quoteoftheday#quotesoftheday#poems and quotes#writing#writers on tumblr#writerscommunity#aesthetic#self care#self love#existence#beauty of existence#healing#healthcare#mental health#healing journey#new path#new beginnings
21 notes
·
View notes
Text

Gee, I thought these people were the ones who were like “If you don’t like it, you can just move to a blue state.”
And now they’re mad the guy is doing just that?
You can’t oppress and discriminate against someone then be mad when they take their highly useful skill elsewhere.
#lgbtq#news#louisiana#democrats#republicans#politics#healthcare#Nbc#nbc news#transgender#medicine#ron desantis
87K notes
·
View notes
Text



"If a pig catches both a human influenza A virus and an avian influenza A virus at the same time, it can spark a process known as viral reassortment — a genetic exchange in which flu viruses swap gene segments."
"Those swaps can introduce dramatic changes, producing a new virus with certain properties of a non-human strain coupled with the capacity to infect and spread between people."
"The death rate in humans may be upwards of 50 per cent, World Health Organization data suggests, though it's possible that milder infections are getting missed, skewing the case fatality ratio. Still, in a population that's never been exposed, the global impacts could be dire."
"More human cases could also be happening under the radar among farm workers who've moved to the U.S. from abroad, don't speak English as their first language, and may be hesitant to seek medical help, he added."
"So I think there's probably underreporting on both sides," Armstrong said."
"If [H5N1] gets into a population where there's constantly animals going in and out … it might not ever leave."
I've been watching this develop for the past several days, and apart from being terrified most people will not take this seriously (I've seen a handful of people already shout conspiracy on social media and it's alarming to see, as always). What I wanted to point out is that pandemics are going to continue to be our 'normal.' I watched a great video on YouTube a while ago (I believe it was by Vice?) that touched base on how this is going to become our new reality because of multiple factors (such as our proximity to animals, and environments/etc). It was when Covid hit and they did a piece debunking some of the misinformation floating on the internet. If I can find it I will post it here because it was informative and relevant to pretty much any world crisis we will see around any virus that spreads among a human population.
This post isn't trying to fear monger anyone, I just hope more people are aware of what is happening because this is important to talk about. There are already cases (of cows getting this bird flu) in the US, and I won't be surprised if there will be instances in more countries around the world. As usual, keep washing your hands/keeping good hygiene practices, masking up (and if you aren't I hope you consider it), and taking precautions if you do happen to visit/work or go near a pig or poultry farm too:
I'll keep track of this here of course, but please stay informed folks. And also FU to any governments who will try to minimize this or try to diminish the severity until it's too late and community spread happens like Covid because their actions are influenced by capitalistic interests.
Update (April 7th, 2024, 9:32pm EST): to anyone wondering where some of the source information originates from -here is a link to the CDC. They are tracking documented avian virus outbreaks in the US and the public can access it here:
#current news#current events#global news#united states#cattle#cows#cattle farming#avian flu#bird flu#h5n1#mask up#pandemic#covid#covid isn't over#covid conscious#covid is airborne#covid is not over#viruses#fuck capitalism#anti captialism#healthcare#public health#world health organization#cdc#news update#update
16K notes
·
View notes
Text

49K notes
·
View notes
Text

11K notes
·
View notes
Text
Horrible fact of the day: Chevron just released a new boat fuel that WILL give you cancer.
Not "might", not "could", WILL. It has a cancer ratio of 1.3:1, as in, in a group of 10 people, 10 would contract CANCER.
(Edit: apparently some articles are now saying 1.4:1, and some are saying a little under that. Either way, the consensus seems to be anywhere between a 95-100+% of contracting cancer, with some expectations of this fuel not even needing a full lifetime of exposure for you to get Cancer.)
The EPA's safety limit is 1:1,000,000 as in 1 in a million people get cancer.
The EPA approved it anyways. I am not joking. The EPA approved a boat fuel that has a near 100% chance of giving someone cancer. It has such a good chance of giving someone cancer that if you DIDN'T get cancer YOU WOULD BE AN OUTLIER.
Fuck the oil industries.
Edit: If you find this (rightfully) horrifying, have you considered industrial sabotage? /hj
This isn't something we can vote away. This isn't something the rich are gonna apologize and make a 10 minute apology video for this. They don't care if you starve or wither in hospitals or get blown up in their wars.
If you don't know where to get started:
If you already know what to do, then it's time to do it. Participate in mutual aid, raise awareness in real life as well as online, participate in or train in self defense and emergency medical training classes.
#anarchy#chevron#fuel#oil#news#health#healthcare#cancer#research#anarchism#leftism#anarchist#leftist#communist#socialism#socialist#eco#green#earth
33K notes
·
View notes
Text
The study itself is titled, “Long-Term Regret and Satisfaction With Decision Following Gender-Affirming Mastectomy,” and sought to study the rate of regret and satisfaction after 2 years or more following gender affirming top surgery. The study’s results were stunning - in 139 surgery patients, the median regret score was 0/100 and the median satisfaction score was 5/5 with similar means as well. In other words… regret was virtually nonexistent in the study among post-op transgender people.
In fact, the regret was so low that many statistical techniques would not even work due to the uniformity of the numbers:
In this cross-sectional survey study of participants who underwent gender-affirming mastectomy 2.0 to 23.6 years ago, respondents had a high level of satisfaction with their decision and low rates of decisional regret. The median Satisfaction With Decision score was 5 on a 5-point scale, and the median decisional regret score was 0 on a 100-point scale. This extremely low level of regret and dissatisfaction and lack of variance in scores impeded the ability to determine meaningful associations among these results, clinical outcomes, and demographic information.
The numbers are in line with many other studies on satisfaction among transgender people. Detransition rates, for instance, have been pegged at somewhere between 1-3%, with transgender youth seeing very low detransition rates. Surgery regret is in line with at least 27 other studies that show a pooled regret rate of around 1% - compare this to regret rates from things like knee surgery, which can be as high as 30%. Gender affirming care appears to be extremely well tolerated with very low instances of regret when compared to other medically necessary care.
[...]
The intense conservative backlash, to the point of disputing reputable scientific journals, likely stems from the fact that reduced regret rates weaken a central narrative these figures have championed in legal and legislative spaces. Over the past three years, anti-trans entities have showcased political detransitioners, reminiscent of the ex-gay campaigns from the 1990s and 2000s, to argue that regrets over gender transition and detransition are widespread. Some have even asserted detransition rates of up to 80%, a claim that has been broadly debunked. Yet, research consistently struggles to find substantial evidence supporting this narrative. The rarity of detransition and regret is underscored by Florida's inability to enlist a single resident to bear witness against a lawsuit challenging the state's ban on gender-affirming care.
19K notes
·
View notes
Text
"The Biden Administration last week [early December, 2023] announced it would be seizing patents for drugs and drug manufacturing procedures developed using government money.
A draft of the new law, seen by Reuters, said that the government will consider various factors including whether a medical situation is leading to increased prices of the drug at any given time, or whether only a small section of Americans can afford it.
The new executive order is the first exercise in what is called “march-in-rights” which allows relevant government agencies to redistribute patents if they were generated under government funding. The NIH has long maintained march-in-rights, but previous directors have been unwilling to use them, fearing consequences.
“We’ll make it clear that when drug companies won’t sell taxpayer funded drugs at reasonable prices, we will be prepared to allow other companies to provide those drugs for less,” White House adviser Lael Brainard said on a press call.
But just how much taxpayer money is going toward funding drugs? A research paper from the Insitute for New Economic Thought showed that “NIH funding contributed to research associated with every new drug approved from 2010-2019, totaling $230 billion.”
The authors of the paper continue, writing “NIH funding also produced 22 thousand patents, which provided marketing exclusivity for 27 (8.6%) of the drugs approved [between] 2010-2019.”
How we do drug discovery and production in America has a number of fundamental flaws that have created problems in the health service industry.
It costs billions of dollars and sometimes as many as 5 to 10 years to bring a drug to market in the US, which means that only companies with massive financial muscle can do so with any regularity, and that smaller, more innovative companies can’t compete with these pharma giants.
This also means that if a company can’t recoup that loss, a single failed drug can result in massive disruptions to business. To protect themselves, pharmaceutical companies establish piles of patents on drugs and drug manufacturing procedures. Especially if the drug in question treats a rare or obscure disease, these patents essentially ensure the company has monoselective pricing regimes.
However, if a company can convince the NIH that a particular drug should be considered a public health priority, they can be almost entirely funded by the government, as the research paper showed.
Some market participants, in this case the famous billionaire investor Mark Cuban, have attempted to remedy the issue of drug costs in America by manufacturing generic versions of patented drugs sold for common diseases."
-via Good News Network, December 11, 2023
#united states#us politics#biden administration#executive order#prescription drugs#medical news#healthcare#healthcare access#biden#big pharma#drug prices#public health#nih#national institutes of health#good news#hope
10K notes
·
View notes
Text
#the supreme court#roe v wade#roe versus wade#politics#scotus#obama#activism#human rights#abortion#reproductive rights#healthcare#feminism#women’s rights#meme#memes#*mypost
114K notes
·
View notes
Text
#women’s rights#can’t believe this is the world we live in now#activism#feminism#roe vs wade#roe versus wade#roe v wade#supreme court#scotus#politics#human rights#reproductive rights#american politics#america#healthcare#gun control#feminist#*posts
90K notes
·
View notes
Text
*Not counting routine checkups or normal doctor's visits– this is asking about serious illness, injury, etc where you were in a bed.
–
We ask your questions so you don’t have to! Submit your questions to have them posted anonymously as polls.
#polls#incognito polls#anonymous#tumblr polls#tumblr users#questions#medical#hospital#healthcare#doctors#polls about health
7K notes
·
View notes
Text









#moodboard#aesthetic#icons#pinterest#indie#cottagecore#foodie#health & fitness#healthcare#healthly#fitness food#cottage aesthetic#fruit#fruits basket#fruits and vegetables#fruit salad#strawberry#kiwi#banana#grapes#orange#colorful#that girl#just girly things#girly tumblr#insta girl#inspo#instagram#instagood#instagram icons
3K notes
·
View notes
Text
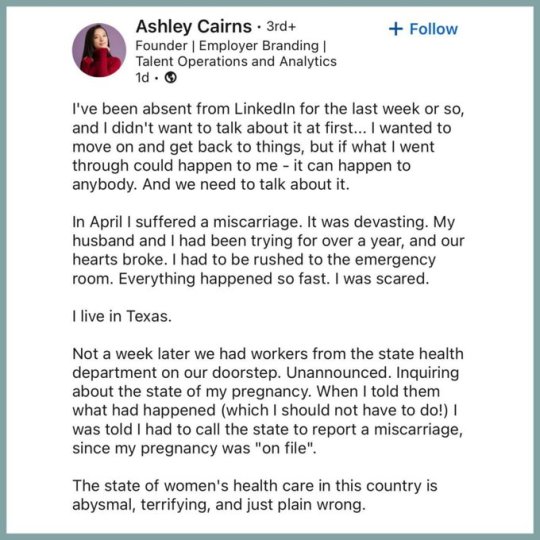

This sounds like something from The Handmaid’s Tale, ffs.
#News#texas#politics#the handmaid’s tale#tht#tw miscarriage#reproductive rights#linkedin#conservatives#democrats#republicans#donald trump#healthcare
26K notes
·
View notes
Last Seen Blogs

ruthypie100
AndNowforSomethingCompletelyDifferent
kargototo
kargototo

no-entry-access
it's sixday my dudes

wheelsofwhisky
A Perfect Place for Whisky Lovers

orea22
Frenesí