#there’s already cases of people dying of different variant of covid after being vaccinated
Text
I am just wondering about the sustainability of... doing basically anything around here. Companies are requiring employees to return to work (in many cases, eliminating telework options that existed PRE-pandemic), mask and vaccine mandates are being rolled back, and everything’s open again despite high COVID numbers.
But at the same time, recent studies show that up to 1 in 5 adult COVID survivors develops symptoms of Long Covid. That’s possibly millions of people developing chronic illness symptoms. That sounds difficult for both the healthcare system to manage AND to have any kind of steady, reliable, functional workplace if your coworkers keep being absent due to sickness and then developing long-lasting symptoms after they return (or quitting due to them).
Even for younger people, for whom it’s often not as bad, I’m seeing so many people get hit with post-viral fatigue and other symptoms lingering for a month or more that remind me a lot of mono. Imagine that like half of your friend group had mono... but unlike mono, kept getting infected again and again (I know many fully vaxxed and boosted people who’ve had COVID multiple times due to different variants). People who have always been super healthy and fit getting exhausted easily or developing new daily headaches who never had them before, struggling with ‘brain fog’ making it difficult to work. These are the young, fit ones.
If there are NO mitigation measures in place and we’re just expected to accept that we’re “all going to get COVID sooner or later,” that ignores the fact that people can get it again and again as each new variant arises and immunity wanes. Because everyone seems to agree that COVID isn’t going away but will just continue to mutate and change into new variants, this seems pretty risky, constantly rolling the dice on getting a virus that may cause LASTING health problems in 20% of people. Especially since so many jobs provide little to no health benefits and super low salaries, basically keeping people from effectively managing chronic illnesses that require frequent absences and medical appointments. I guess they think workers are replaceable, but how long before they burn through the supply?
But on the other hand, it’s also not sustainable to just stay in your room with no human contact for the entire rest of your life. I was super cautious for the first 2 years of the pandemic and now I’m finally doing indoor socialization with vaccinated friends and family again (though still not going into indoor public places like restaurants or movie theatres and still order things online rather than going into stores) because if things are never going to get any better, I don’t know how much longer I can wait. I guess I would rather develop lifelong chronic illness from making lifelong memories celebrating Christmas with my family than running errands at Home Depot.
I genuinely don’t know how long all of this is going to last before the widespread infections and chronic symptoms really start messing with... any industry you can possibly imagine. It seems like everyone is experiencing labor shortages already, and that’s only going to grow from here. Yet it’s hard to find anyone caring even a LITTLE about this. I can’t even talk to friends and loved ones about this because they just start trying to comfort me with the bright side of the COVID situation (”Omicron is less deadly! More people are vaccinated now! The chances of young people dying are vanishingly small!”), when those aren’t the things I’m worried about at all.
When I was 23, something weird happened to my body and I can’t quite say exactly what caused it, because it was a perfect storm. I worked a busy, stressful, physically demanding job at a preschool, and I was working about 10-12 hours a day because I was covering a boss on paternity leave. It was a cold, dark, snowy winter and due to the long work hours, I virtually never saw the sun, so it’s possible a Vitamin D deficiency played a role here, or psychosomatic symptoms caused by stress and anxiety, or just plain old repetitive strain on my body from the long hours. I was also diagnosed with a mild underlying condition during all this-- what is now known as Hypermobility Spectrum Disorder. I’ve always had loose, overly flexible joints, but it never caused me serious problems, just made it a little easier for me to get injured than other people and meant I got worn out a little more easily. Things were never bad enough for me to seek treatment until what happened to me that winter, and have never been as bad since.
But it all started with a cold. A weird bad cold that started like any other cold (and lord knows I was always getting colds working at the preschool) but quickly involved joint pain and weakness and tingly numbness in my hands and wrists, then spreading to the rest of my body over the course of a few weeks. I was so fatigued that all I could do after work was lie in bed. I could hardly make it through the work day. My whole body ached and I could barely do anything without exacerbating my constant pain.
I thought I must have mono. I tested negative for that and 11 other things. The only thing I was diagnosed with during my Extensive, Expensive Journey was hypermobility. My doctor said, “It’s probably just a virus,” which could mean anything. But I felt like a ghost of my former self for about 4 months and still had lingering symptoms for almost a year. Things went downhill so fast that I remember looking at a photo of myself doing a cartwheel two months before and crying because I couldn’t imagine ever doing a cartwheel again (which fortunately wasn’t true-- I have no problem doing cartwheels now at age 30). I eventually quit that job and got a less physically demanding office job. The symptoms never came back to the same degree, and I’ll never know what really caused it, but it wouldn’t surprise me if some kind of post-viral malaise played a role there. Even little colds can set off all kinds of storms, let alone a new virus.
When I hear about people with Long COVID, I imagine a workforce full of people who feel the way I felt when I was 23. Can you? I’m not proposing any kind of solution here or saying, “Here’s what I think people should do about it,” so I’m sorry for the gloomy post, but when people ask me why I’m still worried about COVID-19 after all of this time and my multiple vaccinations... this is why.
124 notes
·
View notes
Text
X
#im just ..... so mad at the attitude of reopening and not needing masks#esp wrt to the vaccine is not only not 100% effective and vaccinated people can still transmit covid#but also that it’s known to not work on different newer variants#there’s already cases of people dying of different variant of covid after being vaccinated#and the variants are only going to continue to increase due to big pharmas’ policy wrt parents and the uneven distribution#(there’s also the theory that it’s possible vaccinated might be more vulnerable to newer variants since the vaccine might be confused#by it and mistake it as old variant. it’s not a verified thing i think so i don’t want to say for sure it’s true)#but even without that. with the vaccines not effective for newer variants#that are for sure to spread with all the reopenings etc#it’s just ... very reckless and im mad and i feel like government is just like they won’t do something about it until numbers go up again#even tho we’ve seen from last year when the numbers do actually go up it’s FAR harder to control#like these policies are just like ...... ‘have you learn nothing from last year’ kind of feeling
8 notes
·
View notes
Link
LETTERS FROM AN AMERICAN
September 9, 2021
Heather Cox Richardson
After weeks of pleading with Americans to get vaccinated as Republican governors opposed mask mandates, ICUs filled up, and people died, today President Joe Biden went on the offensive.
Saying, “My job as President is to protect all Americans,” he announced that he was imposing new vaccination or testing requirements on the unvaccinated. The U.S. government will require all federal employees, as well as any federal contractors, to be vaccinated. The government already requires that all nursing home workers who treat patients on Medicare and Medicaid have to be vaccinated; Biden is expanding that to cover hospital workers, home healthcare aides, and those who work in other medical facilities. “If you’re seeking care at a health facility, you should be able to know that the people treating you are vaccinated.”
Using the Department of Labor’s Occupational Safety and Health Administration (OSHA), Biden will also make employers with 100 or more employees require that their employees either be vaccinated or show a negative coronavirus test at least once a week. He pointed out that big companies already are doing this, including United Airlines, Disney… and the Fox News Channel.
Together, the new vaccine requirements will affect about 100 million Americans, making up two thirds of all U.S. workers.
Biden also urged those who run large entertainment venues to require vaccines or show a recent negative test for entry. He has already required teachers at the schools run by the Defense Department to get vaccinated, and today he announced that the government will require teachers in the Head Start program, which is federally funded, to be vaccinated. He called on governors to require that all teachers and staff be vaccinated for coronavirus, as their states already require a wide range of vaccinations for other diseases.
Calling out those like Florida governor Ron DeSantis, who has taken a stand against mask mandates and is threatening to withhold the salaries of school officials who defy him, Biden said that “if these governors won’t help us beat the pandemic, I’ll use my power as President to get them out of the way.”
He is using the Defense Production Act to increase production of rapid tests and has worked with major retailers to sell those tests at cost for the next three months. The government has also expanded free testing at 10,000 pharmacies and will spend $2 billion to distribute nearly 300 million rapid tests to community health centers, food banks, and schools. He has ordered the Transportation Safety Administration to double the fines on travelers that refuse to mask.
After deploying nearly 1000 healthcare workers to address this summer’s surges in 18 states, the president is now sending in military health teams from the Defense Department. Meanwhile, he said, the U.S. continues to donate vaccines to the rest of the world, “nearly 140 million vaccines over 90 countries so far, more than all other countries combined, including Europe, China, and Russia.... That’s American leadership on a global stage, and that’s just the beginning.” The U.S. is now shipping 500 million more Pfizer vaccines to 100 lower-income countries.
“Many of us are frustrated with the nearly 80 million Americans who are still not vaccinated, even though the vaccine is safe, effective, and free,” Biden said. More than 175 million Americans are fully vaccinated, and for the past three months we have created 700,000 new jobs a month. But while nearly three quarters of those eligible have gotten at least one shot, the highly contagious Delta variant has ripped through the unvaccinated, who are overcrowding our hospitals, threatening the health of our children, and weakening our economic recovery.
“[D]espite America having an unprecedented and successful vaccination program, despite the fact that for almost five months free vaccines have been available in 80,000 different locations, we still have nearly 80 million Americans who have failed to get the shot…. And to make matters worse, there are elected officials actively working to undermine the fight against COVID-19,” Biden said. “Instead of encouraging people to get vaccinated and mask up, they’re ordering mobile morgues for the unvaccinated dying from COVID in their communities. This is totally unacceptable.”
“[W]e have the tools to combat COVID-19, and a distinct minority of Americans—supported by a distinct minority of elected officials—are keeping us from turning the corner…. We cannot allow these actions to stand in the way of protecting the large majority of Americans who have done their part and want to get back to life as normal.”
“We’ve been patient, but our patience is wearing thin. And your refusal has cost all of us,” he said. “So, please, do the right thing.”
The Biden administration is pushing back, too, on Texas’s Senate Bill 8, which prohibits abortion after 6 weeks and thus outlaws 85% of abortions in the state. Today, the United States of America sued the state of Texas for acting “in open defiance of the Constitution” when it passed S. B. 8 and deprived “individuals of their constitutional rights.” The United States has a “profound sovereign interest” in making sure that individuals’ constitutional rights can be protected by the federal government, the lawsuit declares. "The act is clearly unconstitutional under longstanding Supreme Court precedent,” Attorney General Merrick Garland said.
What is at stake in this case is the ability of the federal government to defend Americans’ constitutional rights against local vigilantes, a power Americans gave to the federal government in 1868 by ratifying the Fourteenth Amendment to the Constitution after white former Confederates in southern states refused to accept the idea that their Black neighbors should have rights.
Since the 1950s, the Supreme Court has used federal power to protect the rights of minorities and women when state laws discriminated against them. S. B. 8 would strip the government of that power, leaving individuals at the mercy of their neighbors’ prejudices. The government has asked the U.S. district court for the western district of Texas to declare the law “invalid, null, and void,” and to stop the state from enforcing it.
This issue of federal supremacy is not limited to Texas. Glenn Thrush of the New York Times today called out that in June, Missouri governor Mike Parson signed the Second Amendment Preservation Act, which declares federal laws—including taxes—that govern the use of firearms “invalid in this state.” Like the Texas abortion law, the Second Amendment Preservation Act allows individuals to sue state officials who work with federal officials to deprive Missourians of what they consider to be their Second Amendment rights. “Obviously, it’s about far more than simply gun rights,” one of the chief proponents of the bill, far-right activist Aaron Dorr, said to Thrush about his involvement.
There were other wins today for the Biden administration. Today was the deadline for federal agencies to produce a wide range of records surrounding the events of January 6 to the House Select Committee to Investigate the January 6th Attack on the United States Capitol, and according to the committee’s Twitter feed, those records have, in fact, been forthcoming.
And Taliban officials did allow a plane carrying about 115 Americans and other nationals to leave Afghanistan.
Biden’s new approach to the pandemic is, as Josh Marshall of Talking Points Memo points out, good politics as well as good for public health. About 65% of the voting age population is already vaccinated, and older people are both more likely to be vaccinated and more likely to vote. With most Americans vaccinated and increasingly frustrated with those who refuse, there is little political risk to requiring vaccines, while Republicans standing in the way of public health measures are increasingly unpopular. Florida, where deaths from coronavirus soared to more than 300 a day in late August, has begun to limit the information about deaths it releases.
If Biden’s new vaccine requirements slow or halt the spread of the coronavirus, the economic recovery that had been taking off before the Delta variant hit will resume its speed, strengthening his popularity. Those Republican lawmakers furious at the new vaccine requirements are possibly less worried that they won’t work than that they will.
Notes:
https://www.justsecurity.org/wp-content/uploads/2021/09/lawsuit-doj.pdf
https://www.whitehouse.gov/briefing-room/speeches-remarks/2021/09/09/remarks-by-president-biden-on-fighting-the-covid-19-pandemic-3/
https://www.cnn.com/2021/09/09/politics/biden-administration-texas-abortion-law/index.html
https://january6th.house.gov/news/press-releases/select-committee-issues-sweeping-demand-executive-branch-records
https://www.nytimes.com/live/2021/09/09/business/economy-stock-market-news
https://docs.google.com/document/d/1b3CD2rFn105IQ7ziTfcTT5m8bzv1gBXE5-RXEV0phMM/edit
https://www.nytimes.com/2021/09/09/us/politics/missouri-gun-law.html
https://www.cbsnews.com/news/afghanistan-news-taliban-to-let-americans-evacuate-flights-from-kabul-airport/
https://www.nbcmiami.com/news/local/as-covid-deaths-soar-florida-curtails-public-records-on-which-counties-hit-hardest/2547538/
Josh Marshall @joshtpmThe vax mandate is good public health. It’s also good politics. A big majority of the voting age population is already vaxed. About 65%. Propensity to vote and likelihood of being vaxed both rise with age. The vaxed are losing patience w the voluntarily unvaxed who …
288 Retweets1,742 Likes
September 10th 2021
LETTERS FROM AN AMERICAN
HEATHER COX RICHARDSON
#vaccine mandate#COVID-19#public health#vaccination#Federal Government#The US Constitution#political#Heather Cox Richardson#Letters From An American
4 notes
·
View notes
Text
I've seen several articles repeating a very important piece of info about numbers and perception of danger or infection due to the release by different countries and groups.
Since it's been recognized, South Korea has been testing people regardless of symptoms. Italy has been testing people with symptoms and the US has hardly been testing at all.
So when you hear any of the "There are X,000 confirmed cases and X deaths"-type announcements, realize that in many places around the world these are NOT the actual numbers. It is the number of people who have been tested & diagnosed positive (lab confirmed COVID-19) and not the actual number of people who have it. Not even close. They're likely not double or triple those numbers, either. It's probably at least quadruple at a bare minimum, with numbers skyrocketing in larger cities.
Just like so many other illnesses, people catch something and that illness starts to set up shop. It takes a bit of time for it to trigger our protections or otherwise draw attention to something being wrong. Before people are even feeling sick, they are already contagious and remain so until the viral load is too low to be a viable danger, which is normally after your symptoms are almost gone. This means you could be contagious for several weeks. This isn't odd, it's just how viruses work and you've likely had this same chain of events occur in your own body when you've caught something. We've all been ticking bombs, we just haven't carried this dangerous of a payload inside our cells before. That hang time where you feel fine but are spreading the disease is the scariest thing about contagious diseases of this type, and is why seclusion and quarantine measures are absolutely vital to halt the spread.
No one is immune to Covid-19.
There is no vaccine or preventative measure.
There is no anti-viral available for it.
It is devastating and it is deadly.
Until broad-scale testing is done and tests are being processed quickly, the number of people with COVID-19 can be estimated but not confirmed. I'm not saying this to make you fly into a panic, I'm saying it because we as humans tend to hear numbers first and think about what they actually respresent second, if at all. We have lagged behind in testing and the tests we did have were faulty, we dragged our heels on allowing additional qualified labs to assist with processing tests, and the information coming from our government covers the entire spectrum : accurate, inaccurate, partial, panicked, apathetic, dismissive, confusing, conflicting....it's not reassuring and it is glaringly obvious we are woefully unprepared. Our country is literally shutting down because we don't have other options.
In the US, our situation is, to put it mildly, a clusterfuck.
How so? Through a combination of things, some of which are:
- We are not testing anywhere as broadly as we should be.
- People are not being informed about the seriousness of COVID-19 (think it is same as flu, that young people can't catch it, that flu shots protect etc) and don't understand the difference between viruses and other types of infections.
- People do not understand how long it takes to identify new viruses, why some strains are different, why similar symptoms do not mean similar diseases, how fast viruses can mutate it adapt of how quickly that can be identified.
- People here don't always understand why different departments or sub-offices in departments can be absolutely vital to their lives, and so often don't notice or care when budgets are slashed, research is stopped, responsibilities shoved onto other already burdened departments, whatever. Not knowing how government works is a sad hallmark of American life and this is going to show us how bad this apathy really is.
- People see the number of departments & offices as bloated government spending, so rarely speak up when any are shut down or downsized.
- Large numbers of people in the USA ignore science, decades of information & factual conclusions and warnings of impact even if it can or does affect them personally.
- Large numbers of people in the US were unaware until very recently that the CDC was decimated by Trump specifically. The EPIDEMIC response division was completely eliminated.
- People in the USA in the whole don't understand how various agencies in the government work together or share information on collaborative projects, so when parts of the USDA were forced from Washington DC to Kansas City, it went unremarked upon and the hundreds of positions remaining unfilled in that department alone are a huge concern. Add in the short-staffing of other agencies and this mean that we may not be able to determine how current events can impact food security, transportation, storage or identify economic issues that farmers may face that relate to COVID-19.
- People are not following suggestions of self quarantine or avoidance, instead since they're off work/school /etc heading to places where hundreds+ mingle or to restaurants & bars where 5-10ft distance between people isn't really possible (not to mention the lack of handwashing, shared faucets, knobs, exits/entrance, soiled glasses & silverware, recycled air blah blah) and when all those places are shut down, we all know there will likely be groups who decide to throw parties or pop-up gatherings because they're bored or whatever, and the first time one of those gets busted by cops or National Guard in masks/gear there's going to be a wild few days.
- Different officials in different states have given different direction regarding actions toward COVID-19, with some pleading for everyone to stay home, period, while others were saying going out should be encouraged because....? Conflicting information creates chaos.
- Not grasping that the reason these precautions are implemented is to slow or halt spread of disease and to limit exposure to people who are at higher risk of dying and to help medical efforts (more sick Med personnel = less ability to treat the sick), because the frequently repeated soundbites & headlines are variants on "old and sick people are at risk, everyone else will be fine". The longer it continues to spread among people means the more difficult it will be to stop long term and the more opportunity for it to mutate. Even if you recover just fine, if you were out spreading it, it is still active in the area, which means people who disregard precautions could catch it multiple times which lowers recovery chances, because young *and healthy* is the phrase, and if you just had COVID-19 for two weeks and fought it off, your immune system is tired and your body needs time to recover. Catching it within a few weeks of surviving it? You won't like those odds.
- In the US much of our culture, belief and ideals of value or worth are tied directly to our place in the work force. This is a line we have swallowed hook and sinker, to the point where it is commonly thought that workers in lower paying jobs or work that doesn't require a college degree are less of a person and less valuable that someone making more money. Now a gigantic amount of those employees are without jobs, and they will continue to be the first ones cut from payrolls, fired and unable to find new jobs because those jobs don't currently exist. Young or not, they can all be added to vulnerable groups because they don't have Healthcare, they don't have months of savings to buy food or pay bills, they may not qualify for unemployment or other assistance.
- We are not stressing that all diseases that spread in similar fashion are still active just like always, so it isn't just about COVID-19. People who catch diseases like regular a/b flu strains, streph throat, bronchitis, etc need doctors too, and those conditions being active mean more groups are put at risk if they catch a 'regular' illness which allows COVID-19 easier access, regardless of age. You can have more than one disease at a time!!
That's just the tip of the yikesberg, y'all.
To reiterate, anyone saying "well we only have like X,000 cases in the US" is wrong. We only have X,000 tested and officially confirmed cases, and we have not increased testing or taken efficient measures of seclusion or quarantine nor provided clear, direct information regarding what is happening. States are also putting out info conflicting with the Feds and other States, too and we are not moving fast enough to get the information we need to effectively head off the spread, contain areas and educate the population.
Again, when they do the math on these, diseases are given a specified number, an R0 sometimes heard or read as 'R-naught' (which can change, getting bigger or smaller depending) that is an estimated number of how many people a single person can infect others in an unprotected group. (ie, how many ppl can catch measles for a single patient in a world without vaccinations, which fun fact the measles R0 is 16+ depending on strain) and COVID-19 has been sitting around 2.3, which is higher than the Spanish Influenza of 1918 and over double the number of a standard modern flu strain. Going by this, it isn't really odd that lots of places are using visual representations of the old "would you rather have a million dollars or be given a penny on day 1 that doubles each day for thirty days?" thing, because 2 people infect 2 more each, then those 4 infect 2 each, and so on.
This is why quarantine and seclusion ate used against diseases we have no treatment for: It's the only way to stop it from continuing to spread. Last week, doctors in Seattle (on of the cities hit hardest at the start) were estimating over 1,100 cases in the city alone. Without being able to test and confirm, they had no hard numbers. This means a single city in a single county in a single state, likely had as many or more COVID-19 cases than what was reported as a national number for all 50 states off Federal numbers.
It also doesn't help that like many viruses, the asymptomatic incubation period of COVID-19 means that people who are contagious and spreading the virus are doing so for longer periods of time. On the far side, symptoms show at 10-14 days. Most patients will be contagious while not feeling noticible symptoms for 24-72hrs, thereby potentially exposing everyone around them during that time. This includes virus left on handrails, doorknobs, elevator buttons, ATMs, physical money, grocery items, you name it. If you aren't following basic hygienic protocol & precautions (washing hands thoroughly with soap for 20 seconds minimum frequently throughout the day, especially after using bathroom/touching public door handles, using handholds on public transport, after unbagging groceries, after exchanging money/using card machines, basically touching anything other people frequently touch), then first, somebody should talk to you about the bare minimums of hygiene expected in non-Pandemic times and two, whup your ass into a slightly more sympathetic and less germ-covered way of life.
SOAP & WATER / ALCOHOL
1) Use actual soap and water to wash your hands thoroughly for at least 20 seconds every time you use the restroom (FOR ANY REASON, EVEN IF CHECKING MAKEUP OR HAIR OR OTHER NON-TOILET USE), before you eat, after you eat, after using any sort of shared touchable object or being in close quarters to it, and if you're unsure if you should wash your hands GO WASH YOUR HANDS.
2) Hand sanitizer is NOT more effective than soap and water. PERIOD. They are also used in the same ineffective way so many people use soap and water: too small an amount, too short of a time and too lazy in coverage. Sanitizer should be applied in a dollop large enough to scrub both hands using motions and medium force as if washing with soap & water (front, back, between fingers, over nails & fingertips, both thumbs, webbing, the FULL HAND) for at least 20-30secs which is how long it should take for the sanitizer to evaporate. Amount used doesn't cover both hands fully? Use more. Hands dry after 8 second if scrubbing after putting dollop in palm? Not enough sanitizer used, add more and try again. Alcohol also may kill the virus, but it does not clean your hands and should never be used as a single or primary measure to avoid infection. Keep a bit on hand for those times when soap & water aren't readily available, use it correctly (dollop large enough to wet all surfaces of both hands, rub hands while being attentive to cover every part, hands should feel wet from the gel for 30+ seconds before they start to dry, because you are substituting the alcohol for water and essentially washing your hands with it!!
"Alcohol free" hand sanitizers are basically useless against most viruses and bacteria, including COVID-19. Hand sanitizers must be at least 60% alcohol to be effective, and many homemade concoctions suggest Vodka in their recipes, which is about worthless due to it being 40%. Others recommend 91-99% Isopropyl Alcohol aka 'rubbing alcohol' which can be even worse if the batch is made incorrectly, because it is easily absorbed by human skin and can cause damages leaving you more vulnerable to infections.
The same reason that alcohol works to kill viruses and bacteria is why it's able to damage human skin. It breaks down lipids (fats) and proteins. So called 'enveloped viruses' (COVID-19 in one) have a thin lipid membrane that they live inside and use to find and latch on to host cells. If that membrane is damaged, the virus has no way of feeling for nor attaching to possible host cells, so it dies.
Alcohol solvents being as successful as they are at breaking down lipids, you can imagine how it could hurt our lipids and protein heavy bodies. Using 90%+ isopropyl alcohol in a DIY could leave you with dry, damaged skin as well as cracks and fissures around your nailbeds. That damage is dangerous because your wet tissues and capillaries are now unprotected and vulnerable to viral attack. These types of alcohol can also be fussy with their high evaporative rates as well as interactions with other possible ingredients suggested by DIYers on line could cause many issues. Even compounding pharmacists and chemists are saying what a pain it is to make correctly! Not all Aloe Vera gels are pure aloe. Not all brands or types of gel or alcohol will work with such general, simplified recipes. Essential oils being added is a whole other thing that adds issues, because while a few can be used internally or in wounds with precautions, too many on the market today fail to clearly disclose their processes or full ingredients, are not meant for internal use (open wounds = internal) and like many supplements they are not regulated by the FDA so not tested or held to standard.
3) If you cough or sneeze, do so into a disposable tissue or napkin. DO IT EVERY TIME, not just with deep or phlegmy/productive ones. If air is being expelled forcefully from your throat, lungs or sinuses, have a clean tissue at the ready. After coughing/sneezing, dispose of the tissue in a trash can with a bag liner so the bag can be tied off before disposal which can help mitigate risk to people cleaning or collecting garbage. If you do not have a tissue/napkin, whatever, turn your head and nestle your exploding face hole(s) snugly into the inside bend of your elbow so any emissions are caught by the fabric. Using the same side if it happens repeatedly so you can keep that fabric close to you and avoid touching others with that area, rather than worrying about both arms. No sleeves? Pull up the collar if your shirt, tuck your face down a bit and hold the collar firm over the bridge of your nose and cheeks (similar to how your hands are when using a tissue) so anything coming out of your face is expelled between the shirt fabric and your body/inner layers. ** IF YOU USE THE ELBOW OR SHIRT TECHNIQUE DO NOT FORGET TO WASH YOUR FACE, NECK AND CHEST THOROUGHLY AS SOON AS POSSIBLE, just as you would your hands (20 sec+, soap & water).
[[Related tip: Carrying a ziploc-type bag with you allows you to tuck dirty tissues away while not smearing whatever all over your pockets or bag interiors, too. Those mini Doggie poop bag things that fit on Keychains or bags are another thing to keep with you, for your own tissues or wipes used to clean handles, or even as a 'glove' in a pinch and since they come in bundles you can share with others who need them.]]
So no matter how you slice it, people who have it are out in public spreading it for a day or two minimum. Young, healthy people who don't feel sick and aren't worried because they're likely to survive it are less concerned with the situation even while they are possibly infecting vulnerable groups. Again, the reason for the social distancing and quarantines is to stop the spread and lower risk for people who can and will die. The fewer people it can infect, the fewer can pass it on. The less interaction we have, the lesser the chance we catch and/or spread it. Right now, we here in the US still don't have but half an idea of an area that MAY have cases, because our government are a bunch of greedy fearmongering idiots who care about money more than people and about being right more than being aware.
So let me ask a question to the thousands of people are still going out at night, eating at restaurants, clubbing, calling ridesharing, resisting seclusion/quaratine and generally being completely selfish uncaring assholes: Should I save a seat in in the front row at my immunosuppressed sibs funeral or would you like your name engraved on a memorial bench slat for my diabetic, post-polio syndrome suffering Mum? I suppose at least that would have symmetry with her, as Americans starved her and didn't care if she lived or died as a child (being Indonesian/Javanese = an evil Jap to Americans then) so young Americans ignoring truths and not giving a shit about their actions potential killing her is pretty fucking disappointingly on brand. She could honestly, truly die with her first and last memories of Americans being blatantly uncaring of her life, mocking her fear, denying her help, and watching her family crying around her. Thanks for that, fellow Americans. (Oh, and if you did read the question, I mention a memorial bench because she's donating her body to science to help other people. Even in her death she gives more of a fuck about other people who are sick and need help than the majority of you assholes.)
Maybe that's too much, so lemme take it back a notch and use something less personal and less technical:
How about we say it's like a drunk driver in an armored HumVee speeding through a parade of golf carts.
The person in the HumVee thinks they're fine and puts a bunch of faith in their strong, durable vehicle and ability to control it, so aren't concerned about whatever obstacles arise. The golf carts, meanwhile, are also vehicles with engines and some manueravbility but minimum protection, and the people inside are basically out in the open.
The HumVee hits the carts and they are destroyed, the passengers hurt or killed, and the drunk dude in the HumVee is fine to trundle on to the next situation.
Healthy/young/wilfully ignorant people are currently behaving like that HumVee dude.
(and obviously I am not including people forced to work in order to not end up homeless as HumVee drivers here, this is pointed at people who are blowing off the situation, ignoring facts and being selfish)
—— Here's some info on what happened during the SARS pandemic, which COVID-19 is related to virally and the contagion spread similar, for anyone who is unfamiliar :
The SARS index patient in Hong Kong was a doctor who had treated SARS patients prior to heading to a family event. He did not think he had SARS, because even tho he had some symptoms, a chest x-ray he had done on himself was clear, so he traveled. He ended up infecting several people at the hotel he stayed at overnight, and more when he checked into the Hong Kong hospital. When he checked into the local hospital, more people were infected, including an American who was in a room on the same floor at the hospital. That American ended up feeling sick after leaving, so checked into a hospital in Hanoi. They shortly called in an infectious disease specialist (a WHO doctor in Bangkok) to the Hanoi hospital. He identified that this disease was an unknown new respitory virus, saw that several staff were already showing symptoms and made the call to warn the global community, giving the disease the tentative name of SARS. The WHO specialist, Dr. Urbani, he was a young, healthy Italian doctor, but he still died a month later.
The index patient (a respiratory specialist MD, in his 60s) in Hong Kong died, as did the American (a businessman, 48) who caught it from him, as did the WHO doctor (specialist, 46) who treated the American and others at the Hanoi hospital.
Dr. Liu, the one who traveled, was a super-spreader who is linked to the vast majority of Hong Kong SARS, between 75-92%.
The people who were infected at the hotel went on to travel and spread it to Canada (major hospital outbreak from 1 hotel guest), Taiwan, Singapore and Thailand.
This is the perfect example of why having people who may have COVID-19 enter hospitals is a BAD Idea and why having drive-through testing for it, like what was done in S. Korea, is a good idea.
Dr. Liu didn't just infect a handful of people at the hotel, he infected dozens of already sick, compromised people in a hospital, and also infected staff who died.
The Canadian woman from the hotel infected an assumed 100 people at the hospital she entered when arriving home.
This is why the self-quaratine and suggestions need to be taken seriously. Populations who are vulnerable and basically isolated from society because they are in hospitals or rest homes caught it because it was brought to them by a variety of sick people of different ages, health and severity. Sick young people went to hospitals and older people died. This is why everyone is being directed to call hotline before arriving at hospitals full of sick, vulnerable people.
I hope this helps develop a picture of why these quarantine and preventative measures should be taken seriously, and help you understand this example: Bob, a reasonably healthy guy in his 20s, develops a bit of a cough but blows it off as whatever, then goes out with his friends and gets on a train that several nurses who're going to work are on, he could infect them and they could go into work unknowingly carrying a death sentence for someone recovering from an organ transplant or a kid with a compromised immune system waiting for chemo.
Some of the groups that are on the fringes of society and rarely interact with larger groups are still at risk from secondary transmissions from the employees/staff/medical people that assist them. In high population areas or densely populated cities, even things like an apartment building shared laundry or residents-only gyms, common rooms, etc. are all possibly zones of contagion. Wash your goddamn hands, don't touch all the things around you like a child, and if your city has announced positive cases of COVID-19 please acknowledge that even if you have zero symptoms you could still be infected & contagious and take the necessary precautions along with abiding by the requests to not gather or whatever.
If you are young and healthy and get COVID-19, you may recover. The three people who caught it from you may recover. The five people they passed it to may not.
If you still have a job and are financially ok, consider taking the money you normally spend on your weekly bar visit with friends or Tuesday bingo or whatever the fuck and see if there are any groups or whatnot gathering up money/goods for restaurant, service and other workers who no longer have jobs rather than foolishly throwing middle fingers in the air while bitching about how inconvenient everything is because some old pepple may die or some sick or otherwise useless humans suffering or dying isn't something that makes it OK for your life to be messed with. You probably don't read the pleas from doctors around the globe, or the widows of healthy 30 year olds, or Type 1 diabetics being hit hard, or that this is 20X more deadly than any influenza, mild cases can still honeycomb your lungs and the US still hasn't started the testing we need to determine where it is, how fast it is moving, rates and types of transmission, severity, you name it, and the weakens the global effort because we can't provide other countries with information that could help save them from the fate China, Italy and now the USA will go through.
Want to save the world? Grow the fuck up and take yourself out of the possible patient pool, eat a snack, drink some water, take your meds, put on fresh underpants and breathe. Then get used to this new state of suckage, muster up some energy to vote and then maybe take another nap to recover a bit, because I can tell you none of this shit is ending tomorrow except my sliver of willingness to hold my tongue.
Buckle it up, assholes, those HumVees are coming, so let's work together to take them down like Betty White and Mark Hamill are in those carts and you're all that stands between them and certain death. Because....
Here's the worst of it all, youths : you actually are what stands between them and disaster, this is your reality now, so either educate, protect and defend each other because courage and compassion are worth it, or choose to be callous and cruel to each other until those traits kill you, too. If you're lucky, maybe that cruelty will kill you faster than all these fucking Boomers. If I'm lucky, it'll kill me before I have to be sandwiched between two groups who both will do The Most to win because fuck compromise or moderation or change or discovery and fuck science and tradition and casseroles and Boba tea and lord if if I have to go through four more fucking decades of it I'll burn it down my damn self.
This is it, buckaroos. It's the end of the world as we caused it, and I AM SO FUCKING FAR FROM FINE.
#I am angry#I am old#I need a nap#And a real fucking government#And representatives with ethics#Fuck old people I guess#And sick people too#And poor people#Because we gotta get our party on#Sadly not just a Republican Party#Or democratic party#It's a damn pirate ship party of fools#Fuck me man idk wtf happened#Sigh#Covid-19#Pandemics#Oppy is a whole mood right now#Battery low and getting dark#SAME MY ROBOT FRIEND SAME#This is why I feel like Cassandra
4 notes
·
View notes
Text
Perspectives on the Pandemic With Dr. Peter McCullough
Story at-a-glance
Dr. Peter McCullough is an internist, cardiologist and epidemiologist who warns that COVID-19 vaccines not only are failing but are putting lives at risk
McCullough believes if the proper safety boards had been in place, the COVID-19 vaccine program would have been shut down in February 2021 based on safety and risk of death
By January 22, 2021, 186 deaths had been reported after COVID-19 vaccination — more than enough to reach the mortality signal of concern
In his practice, McCullough is seeing an array of neurologic syndromes in people who’ve been vaccinated, with symptoms including blindness, paralysis, difficulty swallowing, headaches, ringing in the ears, myocarditis and more
McCullough also mentions antigenic, or immune, escape, which he believes is driving the creation of COVID-19 variants and making the pandemic worse instead of better
Dr. Peter McCullough has an impressive list of credentials1 — he’s an internist, cardiologist, epidemiologist and a full professor of medicine at Texas A&M College of Medicine in Dallas and is the editor of two medical journals and published hundreds of studies in the literature. He’s also among those brave and courageous persons speaking out about the dangers of COVID-19 jabs, and putting his medical license and future livelihood at risk by so doing.“There’s a hunting that’s going on here that’s very disturbing,” McCullough said in an episode of Perspectives on the Pandemic.2 He was referring to state medical boards hunting down doctors and their and threatening revocation of their licenses based on the spreading of unidentified “misinformation.”“This is absolutely astonishing that this is happening over a fair exchange of ideas,” he said. What is Dr. McCullough sharing that the powers that be don’t want you to hear? It’s about COVID-19 injections and, to sum it up in a sentence, “It’s not working and it’s causing tremendous damage.”COVID Jab Efficacy and Safety Overstated From the Start
In the U.S., Operation Warp Speed is the federal effort that fast-tracked COVID-19 jab candidates to market. Gene transfer technology platforms emerged as the frontrunners, including adenoviral DNA platforms or messenger RNA (mRNA) platforms designed to deliver genetic material to the human body.Once the mRNA is injected, the body then takes up the genetic material and changes in some way. These technologies have been under study for years, in most cases being designed to replace a defective gene, which could potentially be used for cancer treatment, for example. Except historically, “all failed,” McCullough said.
In November 2020, however, Pfizer, in a joint venture with Germany-based BioNTech, announced that their mRNA-based injection was “more than 90% effective” in a Phase 3 trial.3 This does not mean that 90% of people who get injected will be protected from COVID-19, though, as it’s based on relative risk reduction (RRR).The absolute risk reduction (ARR) for the jab is less than 1%. “Although the RRR considers only participants who could benefit from the jab, the absolute risk reduction (ARR), which is the difference between attack rates with and without a jab, considers the whole population. ARRs tend to be ignored because they give a much less impressive effect size than RRRs,” researchers wrote in The Lancet Microbe in April 2021.4Nonetheless, the jabs received emergency use authorization. By giving the emergency authorization, not approval, the jab administration constituted a research trial, with the sponsors being the U.S. Centers for Disease Control and Prevention and the Food and Drug Administration. According to McCullough:5“We’ve never had two government bodies together be a sponsor of a major research program. Shockingly, they did not have, and to this day they’ve never put together, an external critical event committee, an external data safety monitoring board or a human ethics committee. They had these committees in the registrational trials … and these are standard.Every large clinical investigation has these three committees … I chair many of these committees for pharmaceutical companies and the National Institutes of Health. Americans should have had at least weekly, if not monthly, reviews of safety to ensure Americans that the jabs are safe.”
By March 2021, McCullough Was Worried
Initially, McCullough said, it seemed like the experimental jabs might be safe, and about 70% of his patients had received one by December 2020. But by March 2021, he was uncomfortable with what he was seeing. From December 14, 2020, through March 8, 2021, more than 92 million doses of COVID-19 jabs were administered in the U.S.He cited data from the Vaccine Adverse Event Reporting System (VAERS) database, which showed that during that time, there were 1,637 reports of death in people who had received a COVID-19 jab. The CDC and FDA said none of them was related to the jab but, according
to McCullough, by January 22, 2021, 186 deaths had been reported — more than enough to reach the mortality signal of concern to stop the program.“With a program this size, anything over 150 deaths would be an alarm signal,” he said. The U.S. “hit 186 deaths with only 27 million Americans jabbed.” McCullough believes if the proper safety boards had been in place, the COVID-19 jab program would have been shut down in February based on safety and risk of death.Such was the case in 1976, when a fast-tracked injection program against swine flu was halted after an estimated 25 to 32 deaths.6 Yet, despite a much larger death toll, COVID-19 jabs continues. As of August 6, 2021, VAERS COVID-19 data showed 12,791 deaths related to the jabs, according to McCullough, and tens of thousands of hospital and clinic visits.7In an analysis of COVID-19 vaccine death reports from VAERS, researchers found that 86% of the time, nothing else could have caused the death, and it appears the vaccine was the cause.8The researchers noted, “The sample contains only people jabbed early in the program, and hence is made up primarily of those who are elderly or with significant health conditions. Despite this, there were only 14% of the cases for which a COVID injection reaction could be ruled out as a contributing factor in their death.”9Further research shows, McCullough stated, and this is a very important point that I want you to understand and remember: that 50% of the deaths occurred within 48 hours of getting the shot, while 80% occurred within a week. An informal survey on Twitter, to which 10,000 people responded, also asked whether respondents knew someone who died after a COVID-19 jab.Twelve percent said they did. “When people see others in their circle dying, you can’t stop that type of organic COVID jab hesitancy,” McCullough said. Other confirmed adverse effects of the COVID jabs include myocarditis and blood clots.10An Incredible Violation of Human Ethics
Your body recognizes the spike protein in COVID-19 jabs as foreign, so it begins to manufacture antibodies to protect you against COVID-19, or so the theory goes. But there’s a problem. The spike protein itself is dangerous and known to circulate in your body at least for weeks and more likely months11 — perhaps much longer — after the COVID jab.In your cells, the spike protein damages blood vessels and can lead to the development of blood clots.12,13 It can go into your brain, adrenal glands, ovaries, heart, skeletal muscles and nerves, causing inflammation, scarring and damage in organs over time.In his practice, McCullough is seeing an array of neurologic syndromes in people who’ve been injected, with symptoms including blindness, paralysis, difficulty swallowing, headaches, ringing in the ears, myocarditis and more. Other research suggests that the heart, brain, immunologic system and hematologic system may be most at risk from the jabs.14Children, who are at extremely low risk from COVID-19, receive no benefit from the jab, nor do those who have already had COVID and have immunity, McCullough said, calling the situation “a catastrophe in real time” that’s violating human ethics:15“We’ve seen an incredible violation of human ethics. No one, for an investigational product, under any circumstances, should receive any pressure, coercion or threat of reprisal for not participating in the research.”The Pfizer-BioNTech COVID-19 jab received FDA approval on August 23, 2021, but prior to this, million-dollar raffles, free tuition, bonuses and other bribes like free beer and doughnuts were offered to entice people to get injected. When that didn’t work, mandates increased, including for many health care workers, and hundreds of U.S. colleges16 are also requiring students to get jabbed in order to attend.
0 notes
Text
THE FFL 2020/21 END OF SEASON REVIEW
The 29th season of FFL and the first one to start during a global pandemic. The season before had been totally normal till February and nothing like normal after that. That season didn’t finish until August. No Euro 2020 and a September start to the new season. As we approached the start of the football season it looked like Coronavirus was in decline, number of cases and deaths were dropping very low and life felt a bit more normal, we had no idea of the real world horrors that awaited us all. That being said the 2020/21 season was unique, for all the wrong and some right reasons. During the August break there was the Messi saga. Harry Maguire had been scraping with the Greek police. Foden and Greenwood, while on England duty had broken Covid rules and got caught sneaking a couple of Icelandic girls into their hotel room,
The season started much later and as I got my last ever EMR HST for a day at the seaside the last few teams started to flood in. Michael Dymond was last in, would the champions’ league winner feature in the new season. League champion Steve Tatham was among the favourites to do well, along with FA cup winner Matt Wheeler. Jackie knight had been the golden girl and challenged right up to the last game, could she challenge again? Could the big guns of Mullin and the Hawk get back to winning ways after a very disappointing season in 2020. As per normal the Team Aroma girls tried to make some very strange picks, including Hansen, Beckham and sadly retired Aroma’s own Leighton Baines. Kev Dillon shocked the world and picked Liverpool Players. Following in father Danny and Uncle Marc Lawson’s footsteps Anton joined our league. Andy Flanagan almost did a Stuart Pearce and forgot to pick a keeper. All of these issues fixed for the deadline and 33 teams started the league. With no city or Utd playing in week one the normal Bennetts Shield and Champions league had a delayed start.
As I travelled home on the train from Skegness, there was a feeling that this could be a strange season. Leeds ran Champions Liverpool very close in a high scoring game. Pam Taylor, Team Aroma and Anton Lawson were the early pace setters. The first weekend of October saw the Bennett’s Shield and the start of the Champion’s league. The weekend will be remember as the one where Man Utd conceded 6 and Liverpool 7. In the lowest ever scoring match Steve Tatham beat Matt Wheeler by 1 point to win the Shield. This was the only bright spot for either of them all season. A week later and one of the most controversial moment of the season. In a very fiery Mersey Side Derby Pickford and VVD both went for the ball. Pickford’s challenge would change the season for Liverpool. VVD wouldn’t play again all season. Souness called it an assault, he’d know all about that. Pickford got deaths threats and for the rest of the season everything was Pickford’s fault. Bale return to the premier league, but too late to make anyone’s teams. By the end of the month Mark Taylor was top and so were Everton.
The pandemic hadn’t gone and cases were starting to rocket again, by early November the UK were in Lockdown 2. Football did continue, but behind closed doors and with fake crowds. The very busy fixtures and players coming down with Covid meant that players were dropping like flies. This hurt the FFL managers as much as their Premiership counterparts. Defending Champions league Champion Michael was out the Champions league at the first group stage, along with Steve Tatham, Disco Lee Ritchie and Jackie Knight. By December Taylor was top and Taylor was bottom, sorry Dad. With some matches being cancelled due to the virus there were delays in the champions’ league. The pubs in Lincoln stayed closed, we were out of Lockdown 2, but into tier 4. Pen points were rolling in everywhere with so many players missing. It was already looking like a very low scoring season.
The Christmas number one was The Hawk, with Kieron 2nd and Mark Taylor 3rd. It was a very strange Christmas, Boris had promised a nearly normal one, but the emergence of a new variant from Kent quickly ran through the country like wildfire. The government promised a 5 days of Christmas, but quickly tried to stop this. Unfortunately nothing could stop the full force of this second wave. 40k, 50k even 60k new cases in one day and up to 1500 people dying per day. The UK death toll quickly passed over 100k. Lockdown 3 started and this was going to last much longer than 2. It was a very difficult and dark winter, the second wave was far deadlier than the first. The one bit of hope came in the first use of vaccines. Could these Jabs return life to normal?
By mid-January The Hawk, Kieron and Mark were top 3, but now Vicky Phillips was starting to challenge. The Champions league second group stage fixtures were still delayed, due to covid, but the FA Cup cut off point saw Danny Lawson and Jackie Knight just make it at the expense of Robyn Stanney. Vicky Phillips was now up to 3rd and in her best season. The champions’ league Semi-finals finally took shape. Kieron would play Stally and The Hawk would play Mark Kiszka. In fact both Kieron and The Hawk were looking at possible trebles.
By mid-February and Kieron had an 11pt lead over the Hawk, with Vicky 3rd and Mark 4. Kieron would play Vicky in the FA Cup semi-final. However in the Champions league Stally beat Kieron over two legs and Mark Kiszka beat the Hawk. Things were going wrong for the Hawk, out the FA cup and now out the Champions league, plus a 13 point gap to lead leader Kieron. Kieron was on for the Double and would play Danny Lawson in the FA Cup final. Kieron was looking good, but pen points and missing key players made it far from certain. Road maps out of lockdown were now being talked about. Case numbers were dropping, but still so many people dead, over 120k. The roll out of the vaccine was bringing hope that an end was in sight.
Early April and over two legs Stally won a record 4th Champions league. Once again Mark Kiszka just missed out again. Kieron was still top, but much closer, with The Hawk right on him. Cup finalist Danny Lawson was in contention too. Suddenly and out of the blue the future of football as we know it came crashing down. The so called big 6 in England joined Spanish and Italians in a break away super league. For a short time it really looked like the end of Football, but a fan backlash, backed by ex-players and even the government challenged this. A very quick and embarrassing U-TURN saw the clubs plans fall apart. The Super league was hopefully dead and gone. By the end of April only Kieron and The Hawk had passed 200 points, but were miles off Kieron’s 414 world record.
May the 1st and FA cup final weekend, Kieron v Danny. I even got the coolest man in football (James Richardson) do the preview and since outdoor hospitality was now open we did this over a cappuccino in Aroma. Man Utd were due to play Liverpool, but a mass protest against the owners and the super league brought chaos. Fans even got inside the stadium and onto the pitch. A protest also took place outside the players hotel. The match was cancelled and our FA cup was abandoned. A week later and the FA cup final took place. Both teams were missing Aubameyang so Greenwood came in for Danny and scored, Aguero for Kieron. If Aguero had slotted his penalty away, Kieron would have won, but a terrible so called Panenka cost him dearly. As a result the scores were level and it went to a Tie break six. A goal from Dallas and a clean sheet from Alisson won Danny Lawson his first trophy since 2001. Worse would come for Kieron, with Man City winning the league and resting Ederson and Pope being injured Kieron started getting penalty points, Even when Ederson returned, his defence didn’t. Allisson scored and this added to the Hawks total. Very quickly The Hawk passed him and both Mark’s closed the gap.
Leicester City won their first ever FA Cup, beating Chelsea in front of some fans. Yes limited crowds were now back, the vaccine programme was making a difference, even I had my first jab, but the emergence of a new variant from India was starting to threaten the return to normal.
Final week of the season and The Hawk was clear of Kieron, Mark Kiszka and Mark Taylor. Senol Durmush, Tappy, Jackie Knight, Goodo and Oliver Taylor-Yassin were battling for the final champions league spots. Lee Ritchie and Chris Geoghegan were trying to avoid the wooden spoon. Penalty points had completely derailed Kieron’s season, at one point he was on for a possible treble, but not anymore.
The final Sunday saw The Hawk increase his lead and win his first ever FFL Title. Kieron Mullin ended with nothing. Mark Kiska came third and Danny Lawson came 4th with the FA Cup. Mark Taylor 5th and Vicky Phillips 6th. Senol Durmush, Jackie Knight and Pam Taylor took the final champions league spots from Tappy, Goodo and Ollie.
Thank for another great season of FFL, it’s the 30th season next time and I look forward to this, but before then its Euro FFL this summer, can Flynny defend his title?
Final thought. Is it really all Pickfords fault?
MT
0 notes
Text
3 Breakthrough Covid-19 Coronavirus Deaths Among 700,000+ Fully Vaccinated In Oregon
https://sciencespies.com/news/3-breakthrough-covid-19-coronavirus-deaths-among-700000-fully-vaccinated-in-oregon/
3 Breakthrough Covid-19 Coronavirus Deaths Among 700,000+ Fully Vaccinated In Oregon

This is a reminder that while the available Covid-19 vaccines can protect you against getting more severe Covid-19, they are not like gigantic concrete full-body condoms. Even after getting fully vaccinated, you can still be infected with the Covid-19 coronavirus.
Case in needle point. In Oregon, at least 168 fully vaccinated people have had “breakthrough” Covid-19 coronavirus infections so far. Of those, 19 ended up being hospitalized, and three died, according to the Oregon Health Authority (OHA). Fully vaccinated means that you are at least two weeks past getting the second dose of the Pfizer/BioNTech or Moderna vaccine or one dose of the Johnson & Johnson vaccine, which should be enough time for your immune system to build up enough protection. A breakthrough infection is when an infection occurs in a fully vaccinated person. None of the breakthrough cases in Oregon, otherwise known as the Beaver State, were associated with a severe acute respiratory syndrome coronavirus 2 (SARS-CoV2) variant.
Before you say “dam” what’s happening in the Beaver State, keep in mind that Oregon hasn’t been the only state to report such breakthrough cases. A month ago, I reported for Forbes on three breakthrough cases found in Hawaii. More recently, Paula Pasche covered for The Oakland Press the 246 breakthrough Covid-19 cases that have occurred in Michigan, resulting in 11 hospitalizations and three deaths. So, it’s clear that getting fully vaccinated does not necessarily mean that you can’t get Covid-19 and can’t suffer bad consequences.
Nevertheless, don’t go running outside, waving your hands above your head, telling others in a panic, “see the vaccine doesn’t work, see the vaccine doesn’t work.” Instead, use one of those hands to grab a piece of toast. Use the other hand to get some avocado, and put said avocado on the toast. Then calmly place this combination of avocado and toast, otherwise known as avocado toast, in your mouth, chew while smiling, and take a sip from the cup of proper perspective.
Consider how many people in Oregon have already gotten fully vaccinated: over 700,000. A quick calculation on your abacus will reveal that less than 0.03% of all fully vaccinated people there have had breakthrough Covid-19 coronavirus infections so far. Of the breakthrough infections, less than 2% ended up in death. Oh, and many of these breakthrough infections were actually asymptomatic, meaning that they didn’t result in symptoms.
Then imagine how many more people may have gotten infected and ended up dying had these 700,000 plus people had not been vaccinated. All of this strongly suggests that the Covid-19 vaccines are working, that they are indeed offering protection.
Healthcare workers at the Portland Veterans Affairs Medical Center receive COVID-19 vaccinations. … [+] (Photo by Nathan Howard/Getty Images)
Getty Images
Here’s the take home message though. Just because you are fully vaccinated doesn’t mean that you may go back to doing whatever you were doing before 2020. This isn’t the time to do group hugs, build human pyramids, or play Twister with others, especially those who may not yet be vaccinated. This isn’t the time to forego face mask wearing, social distancing, hand-washing, disinfecting, and all the things that you should have been doing over the past year. It’s still important to maintain a six foot or one Denzel (since Denzel Washington is about six feet tall) distance from others, regardless of whether you are vaccinated.
As Covid-19 cases continue to surge in different parts of the U.S., a major concern is that people will relax other precautions after getting fully vaccinated. Remember, the Covid-19 vaccine is still like Swiss cheese. Despite being impressive, it still does have some holes, and in general, it’s a good idea to keep your holes as covered as possible. This is especially true right now when the U.S. is still in the danger zone of the pandemic with the SARS-CoV2 still circulating widely and the weather not quite warm or humid enough to potentially slow transmission of the virus. Premature relaxation of other precautions and the spread of more contagious SARS-CoV2 variants could be continuing highways to the danger zone.
So if you have the urge to “return to normal” as soon as you are fully vaccinated, wait for it, wait for it. Returning to normal really depends on how soon others can get vaccinated and the U.S. can get the Covid-19 coronavirus under control.
#News
0 notes
Link
Virus Variants Threaten to Draw Out the Pandemic, Scientists Say For weeks, the mood in much of the United States has been buoyant. Cases, hospitalizations and deaths from the coronavirus have fallen steeply from their highs, and millions of people are being newly vaccinated every day. Restaurants, shops and schools have reopened. Some states, like Texas and Florida, have abandoned precautions altogether. In measurable ways, Americans are winning the war against the coronavirus. Powerful vaccines and an accelerating rollout all but guarantee an eventual return to normalcy — to backyard barbecues, summer camps and sleepovers. But it is increasingly clear that the next few months will be painful. So-called variants are spreading, carrying mutations that make the coronavirus both more contagious and in some cases more deadly. Even as vaccines were authorized late last year, illuminating a path to the pandemic’s end, variants were trouncing Britain, South Africa and Brazil. New variants have continued to pop up — in California one week, in New York and Oregon the next. As they take root, these new versions of the coronavirus threaten to postpone an end to the pandemic. At the moment, most vaccines appear to be effective against the variants. But public health officials are deeply worried that future iterations of the virus may be more resistant to the immune response, requiring Americans to queue up for regular rounds of booster shots or even new vaccines. “We don’t have evolution on our side,” said Devi Sridhar, a professor of public health at the University of Edinburgh in Scotland. “This pathogen seems to always be changing in a way that makes it harder for us to suppress.” Health officials acknowledge an urgent need to track these new viruses as they crawl across the United States. Already, B.1.1.7, the highly contagious variant that walloped Britain and is wreaking havoc in continental Europe, is rising exponentially in the United States. Limited genetic testing has turned up more than 12,500 cases, many in Florida and Michigan. As of March 13, the variant accounted for about 27 percent of new cases nationwide, up from just 1 percent in early February. The Biden administration has pledged a “down payment” of $200 million to ramp up surveillance, an infusion intended to make it possible to analyze 25,000 patient samples each week for virus variants. It’s an ambitious goal: The country was sequencing just a few hundred samples each week in December, then scaling up to about 9,000 per week as of March 27. Until recently, B.1.1.7’s rise was camouflaged by falling rates of infection over all, lulling Americans into a false sense of security and leading to prematurely relaxed restrictions, researchers say. “The best way to think about B.1.1.7 and other variants is to treat them as separate epidemics,” said Sebastian Funk, a professor of infectious disease dynamics at the London School of Hygiene and Tropical Medicine. “We’re really kind of obscuring the view by adding them all up to give an overall number of cases.” Other variants identified in South Africa and Brazil, as well as some virus versions first seen in the United States, have been slower to spread. But they, too, are worrisome, because they contain a mutation that diminishes the vaccines’ effectiveness. Just this week, an outbreak of P.1, the variant that crushed Brazil, forced a shutdown of the Whistler Blackcomb ski resort in British Columbia. The world is caught in a sprint between vaccines and variants, and the shots eventually will win, scientists say. But because each infection gives the coronavirus a chance to evolve still further, vaccinations in the United States and elsewhere must proceed as fast as possible. Infections are rising again, driven to an uncertain degree by B.1.1.7 and other variants. Earlier this week, Dr. Rochelle Walensky, director of the Centers for Disease Control and Prevention, pleaded with Americans to continue to practice masking and social distancing, saying she felt a sense of “impending doom.” “We have so much to look forward to — so much promise and potential of where we are and so much reason for hope,” she said. “But right now I’m scared.” ‘More infectious for more days’ The coronavirus was supposed to be slow to change shape. Like all viruses, it would pick up mutations and evolve into thousands of variants, scientists said at the beginning of the pandemic. But it would not change significantly for years — a stupid virus, some called it. The pathogen defied those predictions. “We expected the virus to change,” said Dr. Michael Diamond, a viral immunologist at Washington University in St. Louis. “We didn’t quite anticipate how quickly it was going to occur.” A variant is of concern only if it is more contagious, causes more severe disease, or blunts the immune response. The variants identified in Britain, South Africa, Brazil and California all fit the criteria. B.1.1.7, the first to come to widespread attention, is about 60 percent more contagious and 67 percent more deadly than the original form of the virus, according to the most recent estimates. Updated April 3, 2021, 12:13 p.m. ET The variant is no different from the original in how it spreads, but infected people seem to carry more of the virus and for longer, said Katrina Lythgoe, an evolutionary biologist at the University of Oxford. “You’re more infectious for more days,” she said. So contagious is B.1.1.7 that Britain succeeded in driving down infections only after nearly three months of strict stay-at-home orders, plus an aggressive vaccination program. Even so, cases fell much more slowly than they did during a similar lockdown in March and April. In continental Europe, a wave of B.1.1.7 cases was building for months, mostly unnoticed beneath a steady churn of infections. The variant wave is now cresting. Poland’s rate of daily new cases has quintupled since mid-February, forcing the closure of most public venues. Germany’s has doubled, triggering a ban on nighttime gatherings in Berlin. In France, where B.1.1.7 is causing three-quarters of new infections, some hospitals have had to move coronavirus patients to Belgium to free up beds. Roughly as many people are dying each day from Covid-19 in Europe as were this time a year ago. For too long, government officials disregarded the threat. “Case plateaus can hide the emergence of new variants,” said Carl Pearson, a research fellow at the London School of Hygiene and Tropical Medicine. “And the higher those plateaus are, the worse the problem is.” In the United States, coronavirus infections began a rapid decline in January, soon prompting many state leaders to reopen businesses and ease restrictions. But scientists repeatedly warned that the drop would not last. After the rate bottomed out at about 55,000 cases and 1,500 deaths per day in mid-March, some states — notably Michigan — began seeing an uptick. Since then, the national numbers have steadily risen. As of Saturday, the daily count was up to nearly 69,000, and the weekly average was 19 percent higher than the figure two weeks earlier. Even when cases were falling, researchers questioned the notion that vaccinations were the reason. Millions of Americans are immunized every day, but even now only 31 percent have received a single dose of a vaccine, and just 17 percent of the population have full protection, leaving a vast majority susceptible. “The fact is that we’re still in a position now where we don’t have enough vaccinated people,” said Kristian Andersen, a virologist at the Scripps Research in San Diego. “And if we, like Texas, say we’re done with Covid-19, B.1.1.7 will come in and remind us that we are not right. I have no doubt about it.” The variant is particularly pervasive in Florida, where the state lifted restrictions and initially did not see a surge. Officials in other states cited this as a rationale for reopening. But now Florida’s infection rate is curving upward. The variant may only have been obscured by what scientists like to call seasonality. Respiratory infections are usually rare in Florida in the spring, noted Sarah Cobey, an evolutionary biologist at the University of Chicago. Coronavirus infections peaked in Florida last year in the summer, as heat drove people indoors, and may do so again. “I still don’t think we’re out of the woods,” Dr. Cobey said, referring to the country at large. “If we don’t have another wave this spring, then I’m going to be really, really worried about the fall.” While most vaccines are effective against B.1.1.7, researchers are increasingly concerned about other variants that contain a mutation called E484K. (Scientists often refer to it, appropriately, as “Eek.”) This mutation has evolved independently in many variants worldwide, suggesting that it offers the virus a powerful survival advantage. In laboratory studies, the Pfizer-BioNTech and Moderna vaccines seem to be slightly less effective against B.1.351, the variant identified in South Africa. That variant contains the Eek mutation, which seems to enable the virus to partly sidestep the body’s immune response. The vaccines made by Johnson & Johnson, AstraZeneca and Novavax were even less potent against B.1.351. “I think for the next year or two, E484K will be the most concerning” mutation, said Jesse Bloom, an evolutionary biologist at the Fred Hutchinson Cancer Research Center in Seattle. The mutation slightly alters the so-called spike protein sitting on the surface of the coronavirus, making it just a bit harder for antibodies to latch on and destroy the invader. The good news is that the virus seems to have just a few survival tricks in its bag, and that makes it easier for scientists to find and block those defenses. “I’m feeling pretty good about the fact that there aren’t that many choices,” said Michel Nussenzweig, an immunologist at Rockefeller University in New York. The Eek mutation seems to be the virus’s primary defense against the immune system. Researchers in South Africa recently reported that a new vaccine directed against B.1.351 ought to fend off all other variants, as well. Pfizer, BioNTech and Moderna already are testing newly designed booster shots against B.1.351 that should work against any variants known to blunt the immune response. Instead of a new vaccine against variants, however, it may be just as effective for Americans to receive a third dose of the Pfizer-BioNtech or Moderna vaccines in six months to a year, said Dr. Anthony S. Fauci, head of the National Institute of Allergy and Infectious Diseases. That would keep antibody levels high in each recipient, overwhelming any variant — a more practical strategy than making a specialized vaccine for each new variant that emerges, he said. “My only concern about chasing all the variants is that you’d almost be playing Whac-A-Mole, you know, because they’ll keep coming up and keep coming up,” Dr. Fauci said. In one form or another, the new coronavirus is here to stay, many scientists believe. Multiple variants may be circulating in the country at the same time, as is the case for common cold coronaviruses and influenza. Keeping them at bay may require an annual shot, like the flu vaccine. The best way to deter the emergence of dangerous variants is to keep cases down now and to immunize the vast majority of the world — not just the United States — as quickly as possible. If significant pockets of the globe remain unprotected, the virus will continue to evolve in dangerous new ways. “This might be something that we have to deal with for a long time,” said Rosalind Eggo, an epidemiologist at London School of Hygiene and Tropical Medicine. Still, she added, “Even if it changes again, which it is very likely to do, we are in a better, much stronger position than a year ago to deal with it.” Source link Orbem News #draw #Pandemic #Scientists #Threaten #Variants #Virus
0 notes
Text
January 3, 2021
My weekly roundup of things I am up to. Topics include dietary needs, farmer well-being, cooking, reform, vaccine distribution, scientific progress, and a health update.
Dietary Needs
I got three sections done on Urban Cruise Ship this week. The first of them is on Dietary Needs. The main goal here is to have an assessment of dietary needs for the purpose of recommending food production systems. It does little good to focus on raw calorie count but then be deficient on vital nutrients. A secondary goal is to identify solutions for meeting needs that are currently unmet. Iodizing salt is one key example of this.
Like most sections, what I have now is only a start. But a start is necessary before the finish.
Farmer Well-Being
The second section is this one with several aspects of farmer well-being. A couple of interesting points:
- Urbanization is driven by three major trends: rural-to-urban migration, the indigenous growth of cities, and the reclassification of villages as cities as they grow. Most development literature focuses on the first trend but neglects the other two.
- There is some anxiety in the literature about the “uncontrolled growth of cities”, though I have yet to see a good exposition of how and why urban growth should be controlled. I remain skeptical. Nevertheless, I had gone into this topic expecting to find that the literature was generally anti-urban, and I have found it to be much more nuanced than that.
- Estimates vary, but I figure that about 1% of the Earth’s surface area is urban. Meanwhile, agricultural yields are still growing and population growth is slowing. For these reasons I think it is very unlikely that urbanization would pose any real threat to food security.
- Urban agriculture is a complex topic for which there is limited data. But unless we are talking about greenhouses, hydroponics, or other forms of intensive agriculture, I would not expect urban agriculture to be very important. It is something people generally do for exercise or aesthetic reasons, not to grow food.
- A number of NGOs extol the value of “local knowledge” in agriculture. I cited several studies that look into the subject more deeply, but I don’t have anything quantitative. Obviously there is a danger of romanticizing indigenous cultures, but it is something worth looking at more seriously.
Cooking
The third section I did this week is on Cooking. The use of polluting, biomass-based cookstoves is perhaps the leading indoor air pollution issue globally. While we debate electric versus natural gas stoves in the Western world, moving to any form of modern energy for cooking is far more important. Aside from pollution, traditional cooking takes a lot of time (estimates I’ve seen are hundreds or even thousands of hours per year) gathering fuel, which is unpleasant, especially if the fuel is animal dung.
Despite the risks, I did cite the AGA study I mentioned a few weeks ago that it costs $572-806 per ton to decarbonize by banning gas appliances. I don’t generally like citing industrial trade groups since there is an obvious bias, but after looking some more I still don’t see any other reliable estimate of carbon mitigation costs.
I also whipped up a chart of saving energy while cooking. Efficiency matters too, though I am generally skeptical of highly distributed solutions because it is not easy to make the general public change cooking habits. But there are plenty of small, easy things on the efficiency front.
American Reform
This Palladium article came out a few days ago, arguing that reforming American institutions is the answer to the threat posed by China’s rise. It is worth reading.
I’ve generally taken a dovish view on China. Not that I think the CCP is admirable in many respects but I see little coming from the Chinese that is a real threat to American power or well-being. Furthermore, even as the United States has its own challenges going forward, China is facing severe demographic and debt crises and is probably not far from its geopolitical high water mark. Avoiding the impulse to panic is the wisest course.
Nevertheless, articles such as the linked Palladium one use China as a bit of a morality tale: it’s a pretext for the United States, or the Western world more broadly, to get its own house in order. In this regard the China threat is perhaps a noble lie: a statement that is not true but is meant to motivate valuable action.
Vaccine Distribution
This week there has been much anxiety about the slow pace of vaccine distribution in the United States. These articles by Marginal Revolution, Scott Aaronson, and John Cochrane are good representatives.
“Distressing” would seem like an understatement of the appropriate response to the distribution. The CDC initially proposed on racial equity metrics in vaccine allocation, a plan that bears an uncomfortable resemblance to eugenics. Aside from that, the obsession of distributing vaccines in “the right order” seems to have displaced the need to do it quickly. Thousands of people are dying every day in the United States. The seeming lack of urgency about this fact is probably the most disqualifying fact that has emerged about the public health profession.
While distribution could be much faster, I’m not sure we’re doing such a terrible job. The United States is one of the better countries in terms of vaccines distributed per person. Commentators have compared the US unfavorably to Israel. It seems to me that Israel is an exceptionally well-run country by many metrics; another example is the rate of water recycling and desalination. Israel, along with Singapore, Taiwan, and a handful of other states, seems to show high levels of state capacity. Replicating that is far from a straightforward matter.
Any serious attempt to look at the Covid-19 failure will have to grapple with the fact that failure seems to have been uniform across the federal, state, and local governments in the US, as well as the fact that most countries did poorly. Hopefully the final chapters of this episode are now being written, but with the new variant, with high reproduction rate, spreading around the world, I am worried.
Scientific Progress
There continue to be a flurry of articles about scientific progress, including this one by Eli Dourado which is pretty good. Eli makes a strong case that there are many technologies on the drawing board, and the world is not facing apparent stagnation for want of ability to invent new things. We have to look harder at the diffusion mechanisms. Apparently it is much more difficult to make robots do useful things than to make them dance.
What Eli doesn’t do so well is give us a sense of what those diffusion mechanisms look like. The basic question I want answered remains: why has productivity growth slowed most of the time since the 1970s and especially since 2005, and what if anything do we expect to be different about the 2020s such that diffusion would increase again?
A couple of nitpicks, since Eli goes into some topics that I work in. It it my understanding that the main bottleneck to wind and solar expansion right now is siting, not energy storage, and so the extended discussion that Eli gives to energy storage may be premature. He discusses enhanced geothermal, as have several other commentators recently, which is a bit puzzling to me since enhanced geothermal has been a hot topic since at least the 2000s, and I don’t see a lot of sign that things the area has significantly evolved recently. He discusses small modular reactors, noting with disappointment the recent delay in the NuScale project, though there isn’t a serious attempt to examine the drivers of nuclear costs. There is also discussion of electrolyzed aviation fuel, a concept which I support but I doubt will be economically viable this decade.
Maybe the 2020s will be the decade for autonomous vehicles, drones, and tunnels. The first two of these items have been on the agenda for a long time, and why they haven’t been commercialized already gets back to the question of technology diffusion noted above.
Regarding farming, I continue to expect that greenhouses and hydroponics with natural light, rather than vertical farming, will be the main drivers of agricultural intensification. Even with recent advances in LED technology, artificial lighting is just too expensive. And we can still get plenty of agricultural intensification with natural light. Eli predicts that lab-grown meat may be successful where plant-based meat substitutes are not. That comes down to market acceptance. Plant-based options tend to be cheaper and have lower environmental impacts. Established options like the Boca Burger have shown that they have a market, albeit a limited one. Why will lab-grown meat have greater market share? This could very well be the case, but I’d need to see the reasoning for it.
Health Update
With the start of the new year, this seems like a good time to take stock of where I am health-wise.
I was in quarantine for two weeks at the end of December. My wife was in Floria, and due to potentially being at higher risk, I decided to be away from her. Quarantine time was extended because she got a minor cold. All measures taken to avoid the virus are either underreactions or overreactions; the trouble is that we don’t know in advance which is which.
I was feeling under the weather for the first two days this year, but now I am better. Aside from being a bit more tired than usual, by all outward signs I have recovered to pre-stroke levels. Being tired may be an after-effect of the stroke, the result of being cooped up in a hospital bed for a while, or it may be a long term trend that I didn’t notice until now.
My appetite is down significantly; again it is not clear why this is the case. This is a welcome change, since I have lost about 10 pounds since the peak and I was getting pudgy before (I still am a bit). I also drink one cup of coffee per day, down from 3+ before the stroke. This is due to a lack of desire for coffee, not any deliberate effort to cut back.
Some time in January I am due to go in for an angiogram, which should check whether the procedure I had in September was successful. I don’t know if the Covid situation has disrupted that schedule.
0 notes
Link
(Via: Hacker News)
What Happens Next?
COVID-19 Futures, Explained With Playable Simulations
"The only thing to fear is fear itself" was stupid advice.
Sure, don't hoard toilet paper – but if policymakers fear fear itself, they'll downplay real dangers to avoid "mass panic". Fear's not the problem, it's how we channel our fear. Fear gives us energy to deal with dangers now, and prepare for dangers later.
Honestly, we (Marcel, epidemiologist + Nicky, art/code) are worried. We bet you are, too! That's why we've channelled our fear into making these playable simulations, so that you can channel your fear into understanding:
The Last Few Months (epidemiology 101, SEIR model, R & R0)
The Next Few Months (lockdowns, contact tracing, masks)
The Next Few Years (loss of immunity? no vaccine?)
This guide (published May 1st, 2020. click this footnote!→1) is meant to give you hope and fear. To beat COVID-19 in a way that also protects our mental & financial health, we need optimism to create plans, and pessimism to create backup plans. As Gladys Bronwyn Stern once said, “The optimist invents the airplane and the pessimist the parachute.”
So, buckle in: we're about to experience some turbulence.
The Last Few Months
Pilots use flight simulators to learn how not to crash planes.
Epidemiologists use epidemic simulators to learn how not to crash humanity.
So, let's make a very, very simple "epidemic flight simulator"! In this simulation, Infectious people can turn Susceptible people into more Infectious people:
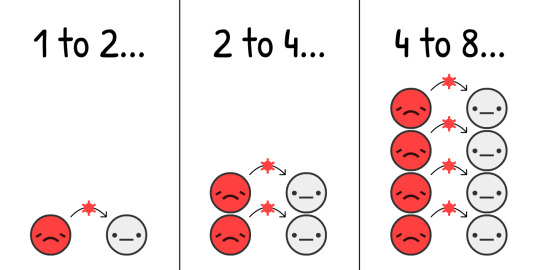
It's estimated that, at the start of a COVID-19 outbreak, the virus jumps from an to an every 4 days, on average.2 (remember, there's a lot of variation)
If we simulate "double every 4 days" and nothing else, on a population starting with just 0.001% , what happens?
Click "Start" to play the simulation! You can re-play it later with different settings: (technical caveats: 3)
This is the exponential growth curve. Starts small, then explodes. "Oh it's just a flu" to "Oh right, flus don't create mass graves in rich cities".
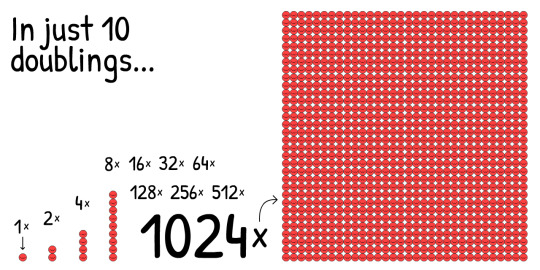
But, this simulation is wrong. Exponential growth, thankfully, can't go on forever. One thing that stops a virus from spreading is if others already have the virus:
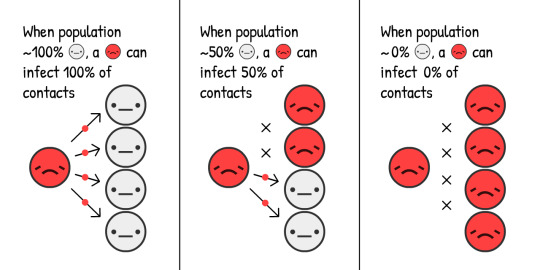
The more s there are, the faster s become s, but the fewer s there are, the slower s become s.
How's this change the growth of an epidemic? Let's find out:
This is the "S-shaped" logistic growth curve. Starts small, explodes, then slows down again.
But, this simulation is still wrong. We're missing the fact that Infectious people eventually stop being infectious, either by 1) recovering, 2) "recovering" with lung damage, or 3) dying.
For simplicity's sake, let's pretend that all Infectious people become Recovered. (Just remember that in reality, some are dead.) s can't be infected again, and let's pretend – for now! – that they stay immune for life.
With COVID-19, it's estimated you're Infectious for 10 days, on average.4 That means some folks will recover before 10 days, some after. Here's what that looks like, with a simulation starting with 100% :
This is the opposite of exponential growth, the exponential decay curve.
Now, what happens if you simulate S-shaped logistic growth with recovery?
Let's find out.
Red curve is current cases ,
Gray curve is total cases (current + recovered ), starts at just 0.001% :
And that's where that famous curve comes from! It's not a bell curve, it's not even a "log-normal" curve. It has no name. But you've seen it a zillion times, and beseeched to flatten.
This is the the SIR Model,5
(Susceptible Infectious Recovered)
the second-most important idea in Epidemiology 101:
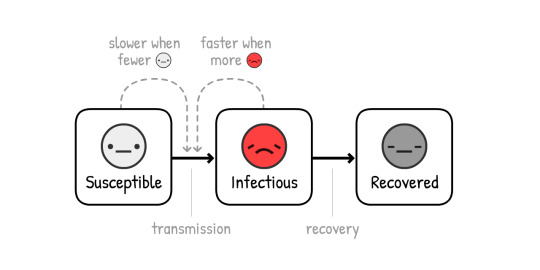
NOTE: The simulations that inform policy are way, way more sophisticated than this! But the SIR Model can still explain the same general findings, even if missing the nuances.
Actually, let's add one more nuance: before an becomes an , they first become Exposed. This is when they have the virus but can't pass it on yet – infected but not yet infectious.
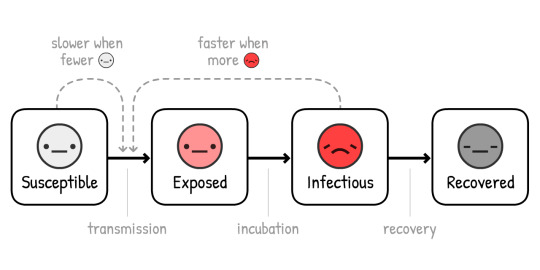
(This variant is called the SEIR Model6, where the "E" stands for "Exposed". Note this isn't the everyday meaning of "exposed", when you may or may not have the virus. In this technical definition, "Exposed" means you definitely have it. Science terminology is bad.)
For COVID-19, it's estimated that you're infected-but-not-yet-infectious for 3 days, on average.7 What happens if we add that to the simulation?
Red + Pink curve is current cases (infectious + exposed ),
Gray curve is total cases (current + recovered ):
Not much changes! How long you stay Exposed changes the ratio of -to-, and when current cases peak... but the height of that peak, and total cases in the end, stays the same.
Why's that? Because of the first-most important idea in Epidemiology 101:

Short for "Reproduction number". It's the average number of people an infects before they recover (or die).
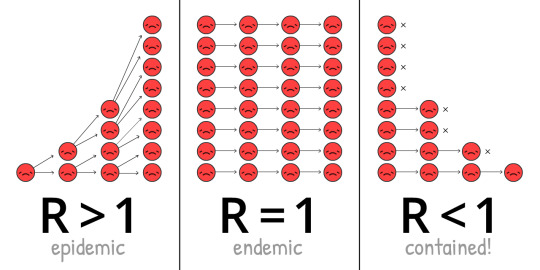
R changes over the course of an outbreak, as we get more immunity & interventions.
R0 (pronounced R-nought) is what R is at the start of an outbreak, before immunity or interventions. R0 more closely reflects the power of the virus itself, but it still changes from place to place. For example, R0 is higher in dense cities than sparse rural areas.
(Most news articles – and even some research papers! – confuse R and R0. Again, science terminology is bad)
The R0 for "the" seasonal flu is around 1.288. This means, at the start of a flu outbreak, each infects 1.28 others on average. (If it sounds weird that this isn't a whole number, remember that the "average" mom has 2.4 children. This doesn't mean there's half-children running about.)
The R0 for COVID-19 is estimated to be around 2.2,9 though one not-yet-finalized study estimates it was 5.7(!) in Wuhan.10
In our simulations – at the start & on average – an infects someone every 4 days, over 10 days. "4 days" goes into "10 days" two-and-a-half times. This means – at the start & on average – each infects 2.5 others. Therefore, R0 = 2.5. (caveats:11)
Play with this R0 calculator, to see how R0 depends on recovery time & new-infection time:
But remember, the fewer s there are, the slower s become s. The current reproduction number (R) depends not just on the basic reproduction number (R0), but also on how many people are no longer Susceptible. (For example, by recovering & getting natural immunity.)
When enough people have immunity, R < 1, and the virus is contained! This is called herd immunity. For flus, herd immunity is achieved with a vaccine. Trying to achieve "natural herd immunity" by letting folks get infected is a terrible idea. (But not for the reason you may think! We'll explain later.)
Now, let's play the SEIR Model again, but showing R0, R over time, and the herd immunity threshold:
NOTE: Total cases does not stop at herd immunity, but overshoots it! And it crosses the threshold exactly when current cases peak. (This happens no matter how you change the settings – try it for yourself!)
This is because when there are more non-s than the herd immunity threshold, you get R < 1. And when R < 1, new cases stop growing: a peak.
If there's only one lesson you take away from this guide, here it is – it's an extremely complex diagram so please take time to fully absorb it:
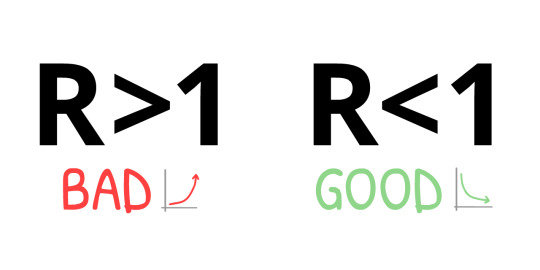
This means: we do NOT need to catch all transmissions, or even nearly all transmissions, to stop COVID-19!
It's a paradox. COVID-19 is extremely contagious, yet to contain it, we "only" need to stop more than 60% of infections. 60%?! If that was a school grade, that's a D-. But if R0 = 2.5, cutting that by 61% gives us R = 0.975, which is R < 1, virus is contained! (exact formula:12)
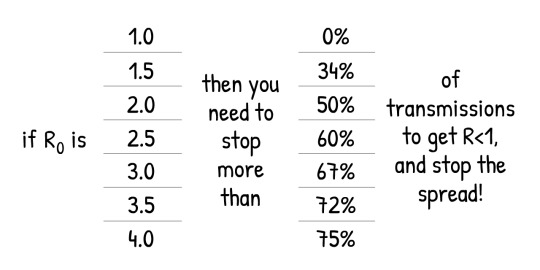
(If you think R0 or the other numbers in our simulations are too low/high, that's good you're challenging our assumptions! There'll be a "Sandbox Mode" at the end of this guide, where you can plug in your own numbers, and simulate what happens.)
Every COVID-19 intervention you've heard of – handwashing, social/physical distancing, lockdowns, self-isolation, contact tracing & quarantining, face masks, even "herd immunity" – they're all doing the same thing:
Getting R < 1.
So now, let's use our "epidemic flight simulator" to figure this out: How can we get R < 1 in a way that also protects our mental health and financial health?
Brace yourselves for an emergency landing...
The Next Few Months
...could have been worse. Here's a parallel universe we avoided:
Scenario 0: Do Absolutely Nothing
Around 1 in 20 people infected with COVID-19 need to go to an ICU (Intensive Care Unit).13 In a rich country like the USA, there's 1 ICU bed per 3400 people.14 Therefore, the USA can handle 20 out of 3400 people being simultaneously infected – or, 0.6% of the population.
Even if we more than tripled that capacity to 2%, here's what would've happened if we did absolutely nothing:
Not good.
That's what the March 16 Imperial College report found: do nothing, and we run out of ICUs, with more than 80% of the population getting infected. (remember: total cases overshoots herd immunity)
Even if only 0.5% of infected die – a generous assumption when there's no more ICUs – in a large country like the US, with 300 million people, 0.5% of 80% of 300 million = still 1.2 million dead... IF we did nothing.
(Lots of news & social media reported "80% will be infected" without "IF WE DO NOTHING". Fear was channelled into clicks, not understanding. Sigh.)
Scenario 1: Flatten The Curve / Herd Immunity
The "Flatten The Curve" plan was touted by every public health organization, while the United Kingdom's original "herd immunity" plan was universally booed. They were the same plan. The UK just communicated theirs poorly.15
Both plans, though, had a literally fatal flaw.
First, let's look at the two main ways to "flatten the curve": handwashing & physical distancing.
Increased handwashing cuts flus & colds in high-income countries by ~25%16, while the city-wide lockdown in London cut close contacts by ~70%17. So, let's assume handwashing can reduce R by up to 25%, and distancing can reduce R by up to 70%:
Play with this calculator to see how % of non-, handwashing, and distancing reduce R: (this calculator visualizes their relative effects, which is why increasing one looks like it decreases the effect of the others.18)
Now, let's simulate what happens to a COVID-19 epidemic if, starting March 2020, we had increased handwashing but only mild physical distancing – so that R is lower, but still above 1:
Three notes:
This reduces total cases! Even if you don't get R < 1, reducing R still saves lives, by reducing the 'overshoot' above herd immunity. Lots of folks think "Flatten The Curve" spreads out cases without reducing the total. This is impossible in any Epidemiology 101 model. But because the news reported "80%+ will be infected" as inevitable, folks thought total cases will be the same no matter what. Sigh.
Due to the extra interventions, current cases peak before herd immunity is reached. In fact, in this simulation, total cases only overshoots a tiny bit above herd immunity – the UK's plan! At that point, R < 1, you can let go of all other interventions, and COVID-19 stays contained! Well, except for one problem...
You still run out of ICUs. For several months. (and remember, we already tripled ICUs for these simulations)
That was the other finding of the March 16 Imperial College report, which convinced the UK to abandon its original plan. Any attempt at mitigation (reduce R, but R > 1) will fail. The only way out is suppression (reduce R so that R < 1).
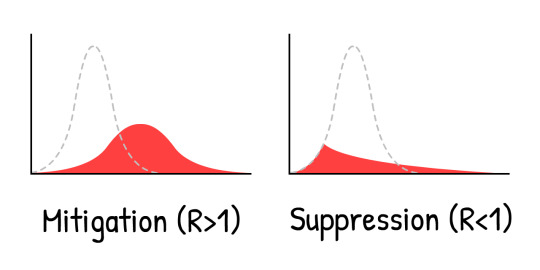
That is, don't merely "flatten" the curve, crush the curve. For example, with a...
Scenario 2: Months-Long Lockdown
Let's see what happens if we crush the curve with a 5-month lockdown, reduce to nearly nothing, then finally – finally – return to normal life:
Oh.
This is the "second wave" everyone's talking about. As soon as we remove the lockdown, we get R > 1 again. So, a single leftover (or imported ) can cause a spike in cases that's almost as bad as if we'd done Scenario 0: Absolutely Nothing.
A lockdown isn't a cure, it's just a restart.
So, what, do we just lockdown again & again?
Scenario 3: Intermittent Lockdown
This solution was first suggested by the March 16 Imperial College report, and later again by a Harvard paper.19
Here's a simulation: (After playing the "recorded scenario", you can try simulating your own lockdown schedule, by changing the sliders while the simulation is running! Remember you can pause & continue the sim, and change the simulation speed)
This would keep cases below ICU capacity! And it's much better than an 18-month lockdown until a vaccine is available. We just need to... shut down for a few months, open up for a few months, and repeat until a vaccine is available. (And if there's no vaccine, repeat until herd immunity is reached... in 2022.)
Look, it's nice to draw a line saying "ICU capacity", but there's lots of important things we can't simulate here. Like:
Mental Health: Loneliness is one of the biggest risk factors for depression, anxiety, and suicide. And it's as associated with an early death as smoking 15 cigarettes a day.20
Financial Health: "What about the economy" sounds like you care more about dollars than lives, but "the economy" isn't just stocks: it's people's ability to provide food & shelter for their loved ones, to invest in their kids' futures, and enjoy arts, foods, videogames – the stuff makes life worth living. And besides, poverty itself has horrible impacts on mental and physical health.
Not saying we shouldn't lock down again! We'll look at "circuit breaker" lockdowns later. Still, it's not ideal.
But wait... haven't Taiwan and South Korea already contained COVID-19? For 4 whole months, without long-term lockdowns?
How?
Scenario 4: Test, Trace, Isolate
"Sure, we *could've* done what Taiwan & South Korea did at the start, but it's too late now. We missed the start."
But that's exactly it! “A lockdown isn't a cure, it's just a restart”... and a fresh start is what we need.
To understand how Taiwan & South Korea contained COVID-19, we need to understand the exact timeline of a typical COVID-19 infection21:
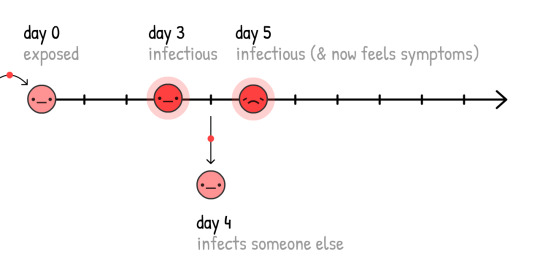
If cases only self-isolate when they know they're sick (that is, they feel symptoms), the virus can still spread:
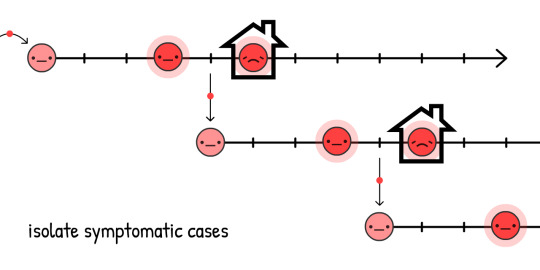
And in fact, 44% of all transmissions are like this: pre-symptomatic! 22
But, if we find and quarantine a symptomatic case's recent close contacts... we stop the spread, by staying one step ahead!
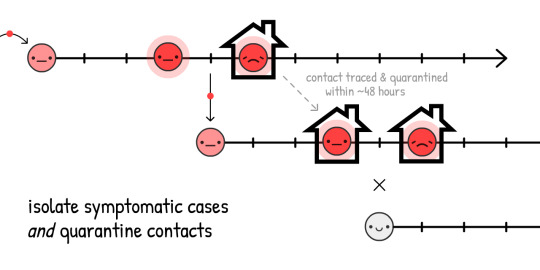
This is called contact tracing. It's an old idea, was used at an unprecedented scale to contain Ebola23, and now it's core part of how Taiwan & South Korea are containing COVID-19!
(It also lets us use our limited tests more efficiently, to find pre-symptomatic s without needing to test almost everyone.)
Traditionally, contacts are found with in-person interviews, but those alone are too slow for COVID-19's ~48 hour window. That's why contact tracers need help, and be supported by – NOT replaced by – contact tracing apps.
(This idea didn't come from "techies": using an app to fight COVID-19 was first proposed by a team of Oxford epidemiologists.)
Wait, apps that trace who you've been in contact with?... Does that mean giving up privacy, giving in to Big Brother?
Heck no! DP-3T, a team of epidemiologists & cryptographers (including one of us, Marcel Salathé) is already making a contact tracing app – with code available to the public – that reveals no info about your identity, location, who your contacts are, or even how many contacts you've had.
Here's how it works:
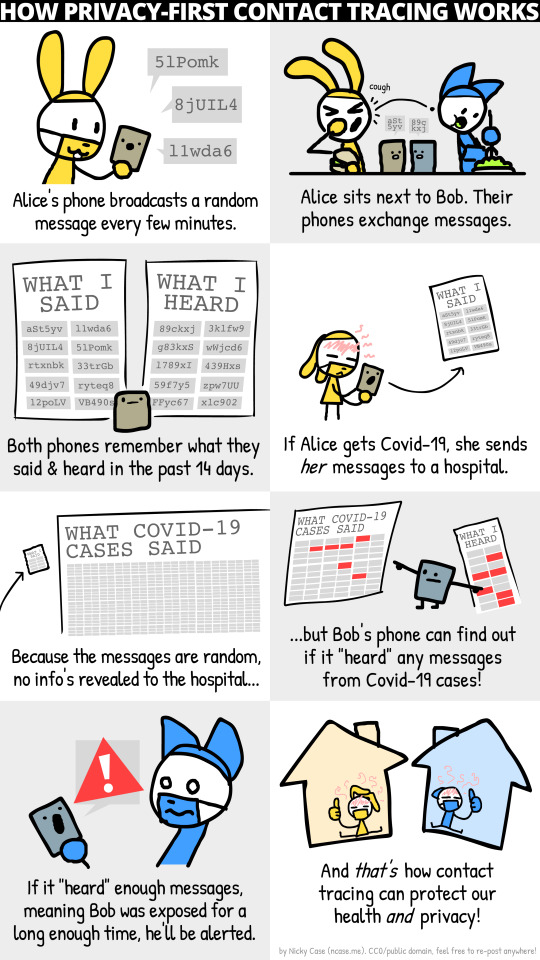
(& here's the full comic)
Along with similar teams like TCN Protocol24 and MIT PACT25, they've inspired Apple & Google to bake privacy-first contact tracing directly into Android/iOS.26 (Don't trust Google/Apple? Good! The beauty of this system is it doesn't need trust!) Soon, your local public health agency may ask you to download an app. If it's privacy-first with publicly-available code, please do!
But what about folks without smartphones? Or infections through doorknobs? Or "true" asymptomatic cases? Contact tracing apps can't catch all transmissions... and that's okay! We don't need to catch all transmissions, just 60%+ to get R < 1.
(Rant about the confusion about pre-symptomatic vs "true" asymptomatic. "True" asymptomatics are rare:27)
Isolating symptomatic cases would reduce R by up to 40%, and quarantining their pre/a-symptomatic contacts would reduce R by up to 50%28:
Thus, even without 100% contact quarantining, we can get R < 1 without a lockdown! Much better for our mental & financial health. (As for the cost to folks who have to self-isolate/quarantine, governments should support them – pay for the tests, job protection, subsidized paid leave, etc. Still way cheaper than intermittent lockdown.)
We then keep R < 1 until we have a vaccine, which turns susceptible s into immune s. Herd immunity, the right way:
(Note: this calculator pretends the vaccines are 100% effective. Just remember that in reality, you'd have to compensate by vaccinating more than "herd immunity", to actually get herd immunity)
Okay, enough talk. Here's a simulation of:
A few-month lockdown, until we can...
Switch to "Test, Trace, Isolate" until we can...
Vaccinate enough people, which means...
We win.
So that's it! That's how we make an emergency landing on this plane.
That's how we beat COVID-19.
...
But what if things still go wrong? Things have gone horribly wrong already. That's fear, and that's good! Fear gives us energy to create backup plans.
The pessimist invents the parachute.
Scenario 4+: Masks For All, Summer, Circuit Breakers
What if R0 is way higher than we thought, and the above interventions, even with mild distancing, still aren't enough to get R < 1?
Remember, even if we can't get R < 1, reducing R still reduces the "overshoot" in total cases, thus saving lives. But still, R < 1 is the ideal, so here's a few other ways to reduce R:
Masks For All:
"Wait," you might ask, "I thought face masks don't stop you from getting sick?"
You're right. Masks don't stop you from getting sick29... they stop you from getting others sick.
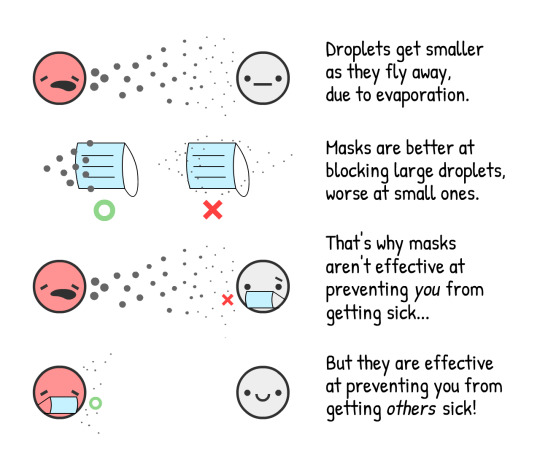
To put a number on it: surgical masks on the sick person reduce cold & flu viruses in aerosols by 70%.30 Reducing transmissions by 70% would be as large an impact as a lockdown!
However, we don't know for sure the impact of masks on COVID-19 specifically. In science, one should only publish a finding if you're 95% sure of it. (...should.31) Masks, as of May 1st 2020, are less than "95% sure".
However, pandemics are like poker. Make bets only when you're 95% sure, and you'll lose everything at stake. As a recent article on masks in the British Medical Journal notes,32 we have to make cost/benefit analyses under uncertainty. Like so:
Cost: If homemade cloth masks, same as the cost of all that soap for handwashing. If surgical masks, more expensive but still pretty cheap.
Benefit: Even if it's a 50–50 chance of surgical masks reducing transmission by 0% or 70%, the average "expected value" is still 35%, same as a half-lockdown! So let's guess-timate that surgical masks reduce R by up to 35%. (Again, you can challenge our assumptions by turning the sliders up/down)
Here's a calculator of how masks reduce R! You can switch between cloth & surgical: (assumes cloth masks are 2/3 as effective as surgical masks33)
(other arguments for/against masks:34)
Masks alone won't get R < 1. But if handwashing & "Test, Trace, Isolate" only gets us to R = 1.10, having just 2/3 of people wear cloth masks would tip that over to R < 1, virus contained!
Summer:
Okay, this isn't an "intervention" we can control, but it will help! Some news outlets report that summer won't do anything to COVID-19. They're half right: summer won't get R < 1, but it will reduce R.
For COVID-19, every extra 1° Celsius (2.2° Fahrenheit) makes R drop by 1.2%.35 The summer-winter difference in New York City is 15°C (60°F), so summer will make R drop by 18%.
Summer alone won't make R < 1, but if we have limited resources, we can scale back some interventions in the summer – so we can scale them higher in the winter.
A "Circuit Breaker" Lockdown:
And if all that still isn't enough to get R < 1... we can do another lockdown.
But we wouldn't have to be 2-months-closed / 1-month-open over & over! Because R is reduced, we'd only need one or two more "circuit breaker" lockdowns before a vaccine is available. (Singapore had to do this recently, "despite" having controlled COVID-19 for 4 months. That's not failure: this is what success takes.)
Here's a simulation a "lazy case" scenario:
Lockdown, then
A moderate amount of hygiene + "Test, Trace, Isolate" + cloth "Masks For All", then...
One more "circuit breaker" lockdown before a vaccine's found.
Not to mention all the other interventions we could do, to further push R down:
. . .
We hope these plans give you hope.
Even under a pessimistic scenario, it is possible to beat COVID-19, while protecting our mental and financial health. Use the lockdown as a "reset button", keep R < 1 with case isolation + privacy-protecting contract tracing + at least cloth masks for all... and life can get back to a normal-ish!
Sure, you may have dried-out hands. But you'll get to invite a date out to a comics bookstore! You'll get to go out with friends to watch the latest Hollywood cash-grab. You'll get to people-watch at a library, taking joy in people going about the simple business of being alive.
Even under the worst-case scenario... life perseveres.
So now, let's plan for some worse worst-case scenarios. Water landing, get your life jacket, and please follow the lights to the emergency exits:
The Next Few Years
You get COVID-19, and recover. Or you get the COVID-19 vaccine. Either way, you're now immune...
...for how long?
COVID-19 is most closely related to SARS, which gave its survivors 2 years of immunity.36
The coronaviruses that cause "the" common cold give you 8 months of immunity.37
There's reports of folks recovering from COVID-19, then testing positive again, but it's unclear if these are false positives.38
One not-yet-peer-reviewed study on monkeys showed immunity to the COVID-19 coronavirus for at least 28 days.39
But for COVID-19 in humans, as of May 1st 2020, "how long" is the big unknown.
For these simulations, let's say it's 1 year. Here's a simulation starting with 100% , exponentially decaying into susceptible, no-immunity s after 1 year, on average, with variation:
Return of the exponential decay!
This is the SEIRS Model. The final "S" stands for Susceptible, again.
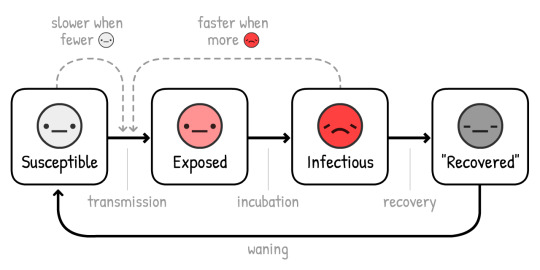
Now, let's simulate a COVID-19 outbreak, over 10 years, with no interventions... if immunity only lasts a year:
In previous simulations, we only had one ICU-overwhelming spike. Now, we have several, and cases come to a rest permanently at ICU capacity. (Which, remember, we tripled for these simulations)
R = 1, it's endemic.
Thankfully, because summer reduces R, it'll make the situation better:
Oh.
Counterintuitively, summer makes the spikes worse and regular! This is because summer reduces new s, but that in turn reduces new immune s. Which means immunity plummets in the summer, creating large regular spikes in the winter.
Thankfully, the solution to this is pretty straightforward – just vaccinate people every fall/winter, like we do with flu shots:
(After playing the recording, try simulating your own vaccination campaigns! Remember you can pause/continue the sim at any time)
But here's the scarier question:
What if there's no vaccine for years? Or ever?
To be clear: this is unlikely. Most epidemiologists expect a vaccine in 1 to 2 years. Sure, there's never been a vaccine for any of the other coronaviruses before, but that's because SARS was eradicated quickly, and "the" common cold wasn't worth the investment.
Still, infectious disease researchers have expressed worries: What if we can't make enough?40 What if we rush it, and it's not safe?41
Even in the nightmare "no-vaccine" scenario, we still have 3 ways out. From most to least terrible:
1) Do intermittent or loose R < 1 interventions, to reach "natural herd immunity". (Warning: this will result in many deaths & damaged lungs. And won't work if immunity doesn't last.)
2) Do the R < 1 interventions forever. Contact tracing & wearing masks just becomes a new norm in the post-COVID-19 world, like how STI tests & wearing condoms became a new norm in the post-HIV world.
3) Do the R < 1 interventions until we develop treatments that make COVID-19 way, way less likely to need critical care. (Which we should be doing anyway!) Reducing ICU use by 10x is the same as increasing our ICU capacity by 10x:
Here's a simulation of no lasting immunity, no vaccine, and not even any interventions – just slowly increasing capacity to survive the long-term spikes:
Even under the worst worst-case scenario... life perseveres.
. . .
Maybe you'd like to challenge our assumptions, and try different R0's or numbers. Or try simulating your own combination of intervention plans!
Here's an (optional) Sandbox Mode, with everything available. (scroll to see all controls) Simulate & play around to your heart's content:
This basic "epidemic flight simulator" has taught us so much. It's let us answer questions about the past few months, next few months, and next few years.
So finally, let's return to...
The Now
Plane's sunk. We've scrambled onto the life rafts. It's time to find dry land.42
Teams of epidemiologists and policymakers (left, right, and multi-partisan) have come to a consensus on how to beat COVID-19, while protecting our lives and liberties.
Here's the rough idea, with some (less-consensus) backup plans:
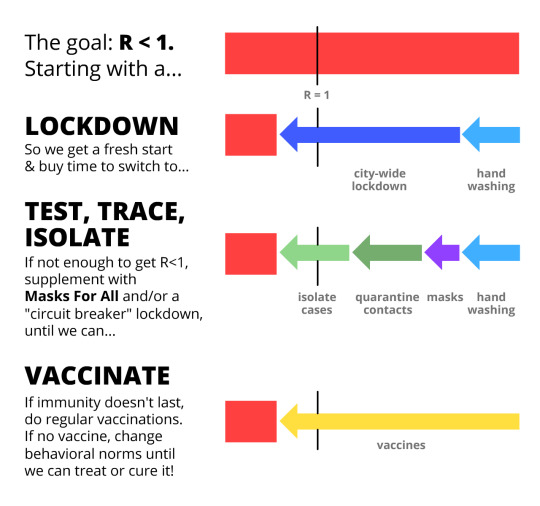
So what does this mean for YOU, right now?
For everyone: Respect the lockdown so we can get out of Phase I asap. Keep washing those hands. Make your own masks. Download a privacy-protecting contact tracing app when those are available next month. Stay healthy, physically & mentally! And write your local policymaker to get off their butt and...
For policymakers: Make laws to support folks who have to self-isolate/quarantine. Hire more manual contact tracers, supported by privacy-protecting contact tracing apps. Direct more funds into the stuff we should be building, like...
For builders: Build tests. Build ventilators. Build personal protective equipment for hospitals. Build tests. Build masks. Build apps. Build antivirals, prophylactics, and other treatments that aren't vaccines. Build vaccines. Build tests. Build tests. Build tests. Build hope.
Don't downplay fear to build up hope. Our fear should team up with our hope, like the inventors of airplanes & parachutes. Preparing for horrible futures is how we create a hopeful future.
The only thing to fear is the idea that the only thing to fear is fear itself.
0 notes
Link
As Mask Mandates Lift, Retail Workers Again Feel Vulnerable Marilyn Reece, the lead bakery clerk at a Kroger in Batesville, Miss., started noticing more customers walking around the store without masks this month after the state mandate to wear face coverings was repealed. Kroger still requires them, but that doesn’t seem to matter. When Ms. Reece, a 56-year-old breast-cancer survivor, sees those shoppers, she prays. “Please, please, don’t let me have to wait on them, because in my heart, I don’t want to ignore them, I don’t want to refuse them,” she said. “But then I’m thinking I don’t want to get sick and die, either. It’s not that people are bad, but you don’t know who they’ve come into contact with.” Ms. Reece’s heightened anxiety is shared by retail and fast-food workers in states like Mississippi and Texas, where governments have removed mask mandates before a majority of people have been vaccinated and while troubling new variants of the coronavirus are appearing. It feels like a return to the early days of the pandemic, when businesses said customers must wear masks but there was no legal requirement and numerous shoppers simply refused. Many workers say that their stores do not enforce the requirement, and that if they do approach customers, they risk verbal or physical altercations. “It’s given a great false sense of security, and it’s no different now than it was a year ago,” said Ms. Reece, who is not yet able to receive a vaccine because of allergies. “The only difference we have now is people are getting vaccinated but enough people haven’t gotten vaccinated that they should have lifted the mandate.” For many people who work in retail, especially grocery stores and big-box chains, the mask repeals are another example of how little protection and appreciation they have received during the pandemic. While they were praised as essential workers, that rarely translated into extra pay on top of their low wages. Grocery employees were not initially given priority for vaccinations in most states, even as health experts cautioned the public to limit time in grocery stores because of the risk posed by new coronavirus variants. (Texas opened availability to everyone 16 and older on Monday.) The issue has gained serious prominence: On Monday, President Biden called on governors and mayors to maintain or reinstate orders to wear masks as the nation grapples with a potential rise in virus cases. The United Food and Commercial Workers union, which represents nearly 900,000 grocery workers, said this month that at least 34,700 grocery workers around the country had been infected with or exposed to Covid-19 and that at least 155 workers had died from the virus. The recent mass shooting at a grocery store in Boulder, Colo., has only rattled workers further and added to concerns about their own safety. Diane Cambre, a 50-year-old floor supervisor at a Kroger in Midlothian, Texas, said she had spent much of the past year worrying about bringing the virus home to her 9-year-old son and dreading interactions with customers who were flippant about the possibility of getting sick. She wears a double mask in the store even though it irritates her skin, already itchy from psoriasis, and changes her clothes as soon as she gets home. After Gov. Greg Abbott of Texas said on March 2 that he would end the statewide mask mandate the next week, Ms. Cambre said, customers immediately “started coming in not wearing a mask and stuff, and it’s been pretty hard getting anybody to wear one.” Management is supposed to offer masks to people who aren’t wearing them, but if they don’t put them on, nothing else is done, she said. Asking customers to wear masks can result in tense exchanges and even tantrums from cart-pushing adults. “Some of our customers are drama-prone, so they’ll start yelling, ‘I’m not wearing that mask,’ and you can tell they’re very rude in their voice and very harsh,” Ms. Cambre, a U.F.C.W. member, said. Overseeing the self-checkout aisles has been especially challenging, she said, because customers who need help will demand that she come over, making it impossible to maintain six feet of distance. At times when she has tried to explain the need for distancing, “they say, ‘OK, and that’s just a government thing,’” she said. “It really takes a toll on you mentally.” A Kroger representative said that the chain would “continue to require everyone in our stores across the country to wear masks until all our frontline grocery associates can receive the Covid-19 vaccine,” and that it was offering $100 one-time payments to workers who received the vaccine. The differing state and business mandates have some workers worried about more confrontations. The retail industry was already trying to address the issue last fall, when a major trade group helped put together training to help workers manage and de-escalate conflicts with customers who resisted masks, social distancing and store capacity limits. Refusing service to people without masks, or asking them to leave, has led to incidents in the past year like a cashier’s being punched in the face, a Target employee’s breaking his arm and the fatal shooting of a Family Dollar security guard. This month in League City, Texas, near Houston, a 53-year-old man who refused to wear a required mask in a Jack in the Box confronted employees and then stabbed a store manager three times, according to a report in The Houston Chronicle. On March 14, a San Antonio ramen shop was vandalized with racist graffiti after its owner criticized Mr. Abbott on television for lifting the Texas mask mandate. On March 17, a 65-year-old woman was arrested in an Office Depot in Texas City after she refused to wear a mask or leave the store, just days after an arrest warrant was issued for her in Galveston, Texas, for behaving similarly in a Bank of America location. MaryAnn Kaylor, the owner of two antique stores in Dallas, including Lula B’s Design District, said the mask mandate repeal mattered a lot for stores and people’s behavior. “He should have focused more on getting people vaccinated instead of trying to open everything up,” she said of Governor Abbott, noting that Texas has one of the country’s slowest vaccination rates. “You still have cases every day in Texas, and you have people dying still from Covid,” she said. “This complete lifting of mandates is stupid. It shouldn’t have been based on politics — it should have been based on science.” Some Texans have started to seek out mask-friendly establishments. Ms. Kaylor said that lists of Dallas businesses that require masks had been circulating on Facebook, and that people were consulting them to figure out where to buy groceries and do other shopping. Emily Francois, a sales associate at a Walmart in Port Arthur, Texas, said that customers had been ignoring signs to wear masks and that Walmart had not been enforcing the policy. So Ms. Francois stands six feet away from shoppers who don’t wear masks, even though that upsets some of them. “My life is more important,” she said. “I see customers coming in without a mask and they’re coughing, sneezing, they’re not covering their mouths,” said Ms. Francois, who has worked at Walmart for 14 years and is a member of United for Respect, an advocacy group. “Customers coming in the store without masks make us feel like we aren’t worthy, we aren’t safe.” Phillip Keene, a spokesman for Walmart, said that “our policy of requiring associates and customers to wear masks in our stores has helped protect them during the pandemic, and we’re not lifting those measures at this time.” Even before the pandemic, Ms. Reece, the Kroger clerk in Mississippi, was wearing a mask to protect herself from the flu because of her cancer diagnosis, she said. She said 99 percent of customers in her small store had worn masks during the pandemic. “When they had to put it on, they did put it on,” she said. “It’s like giving a child a piece of candy — that child is going to eat that candy unless you take it from them.” She is concerned about the potential harm from new variants, particularly from those who don’t cover their mouths. “You just have to pray and pray you don’t get within six feet of them, or 10 feet for that matter,” said Ms. Reece, who is also a U.F.C.W. member and has worked for Kroger for more than 30 years. “I know people want it to be back to normal, but you can’t just will it to be back to normal.” Source link Orbem News #feel #Lift #Mandates #mask #retail #vulnerable #Workers
0 notes
Link
As Mask Mandates Lift, Retail Workers Again Feel Vulnerable Marilyn Reece, the lead bakery clerk at a Kroger in Batesville, Miss., started noticing more customers walking around the store without masks this month after the state mandate to wear face coverings was repealed. Kroger still requires them, but that doesn’t seem to matter. When Ms. Reece, a 56-year-old breast-cancer survivor, sees those shoppers, she prays. “Please, please, don’t let me have to wait on them, because in my heart, I don’t want to ignore them, I don’t want to refuse them,” she said. “But then I’m thinking I don’t want to get sick and die, either. It’s not that people are bad, but you don’t know who they’ve come into contact with.” Ms. Reece’s heightened anxiety is shared by retail and fast-food workers in states like Mississippi and Texas, where governments have removed mask mandates before a majority of people have been vaccinated and while troubling new variants of the coronavirus are appearing. It feels like a return to the early days of the pandemic, when businesses said customers must wear masks but there was no legal requirement and numerous shoppers simply refused. Many workers say that their stores do not enforce the requirement, and that if they do approach customers, they risk verbal or physical altercations. “It’s given a great false sense of security, and it’s no different now than it was a year ago,” said Ms. Reece, who is not yet able to receive a vaccine because of allergies. “The only difference we have now is people are getting vaccinated but enough people haven’t gotten vaccinated that they should have lifted the mandate.” For many people who work in retail, especially grocery stores and big-box chains, the mask repeals are another example of how little protection and appreciation they have received during the pandemic. While they were praised as essential workers, that rarely translated into extra pay on top of their low wages. Grocery employees were not initially given priority for vaccinations in most states, even as health experts cautioned the public to limit time in grocery stores because of the risk posed by new coronavirus variants. (Texas opened availability to everyone 16 and older on Monday.) The issue has gained serious prominence: On Monday, President Biden called on governors and mayors to maintain or reinstate orders to wear masks as the nation grapples with a potential rise in virus cases. The United Food and Commercial Workers union, which represents nearly 900,000 grocery workers, said this month that at least 34,700 grocery workers around the country had been infected with or exposed to Covid-19 and that at least 155 workers had died from the virus. The recent mass shooting at a grocery store in Boulder, Colo., has only rattled workers further and added to concerns about their own safety. Diane Cambre, a 50-year-old floor supervisor at a Kroger in Midlothian, Texas, said she had spent much of the past year worrying about bringing the virus home to her 9-year-old son and dreading interactions with customers who were flippant about the possibility of getting sick. She wears a double mask in the store even though it irritates her skin, already itchy from psoriasis, and changes her clothes as soon as she gets home. After Gov. Greg Abbott of Texas said on March 2 that he would end the statewide mask mandate the next week, Ms. Cambre said, customers immediately “started coming in not wearing a mask and stuff, and it’s been pretty hard getting anybody to wear one.” Management is supposed to offer masks to people who aren’t wearing them, but if they don’t put them on, nothing else is done, she said. Asking customers to wear masks can result in tense exchanges and even tantrums from cart-pushing adults. “Some of our customers are drama-prone, so they’ll start yelling, ‘I’m not wearing that mask,’ and you can tell they’re very rude in their voice and very harsh,” Ms. Cambre, a U.F.C.W. member, said. Overseeing the self-checkout aisles has been especially challenging, she said, because customers who need help will demand that she come over, making it impossible to maintain six feet of distance. At times when she has tried to explain the need for distancing, “they say, ‘OK, and that’s just a government thing,’” she said. “It really takes a toll on you mentally.” A Kroger representative said that the chain would “continue to require everyone in our stores across the country to wear masks until all our frontline grocery associates can receive the Covid-19 vaccine,” and that it was offering $100 one-time payments to workers who received the vaccine. The differing state and business mandates have some workers worried about more confrontations. The retail industry was already trying to address the issue last fall, when a major trade group helped put together training to help workers manage and de-escalate conflicts with customers who resisted masks, social distancing and store capacity limits. Refusing service to people without masks, or asking them to leave, has led to incidents in the past year like a cashier’s being punched in the face, a Target employee’s breaking his arm and the fatal shooting of a Family Dollar security guard. This month in League City, Texas, near Houston, a 53-year-old man who refused to wear a required mask in a Jack in the Box confronted employees and then stabbed a store manager three times, according to a report in The Houston Chronicle. On March 14, a San Antonio ramen shop was vandalized with racist graffiti after its owner criticized Mr. Abbott on television for lifting the Texas mask mandate. On March 17, a 65-year-old woman was arrested in an Office Depot in Texas City after she refused to wear a mask or leave the store, just days after an arrest warrant was issued for her in Galveston, Texas, for behaving similarly in a Bank of America location. MaryAnn Kaylor, the owner of two antique stores in Dallas, including Lula B’s Design District, said the mask mandate repeal mattered a lot for stores and people’s behavior. “He should have focused more on getting people vaccinated instead of trying to open everything up,” she said of Governor Abbott, noting that Texas has one of the country’s slowest vaccination rates. “You still have cases every day in Texas, and you have people dying still from Covid,” she said. “This complete lifting of mandates is stupid. It shouldn’t have been based on politics — it should have been based on science.” Some Texans have started to seek out mask-friendly establishments. Ms. Kaylor said that lists of Dallas businesses that require masks had been circulating on Facebook, and that people were consulting them to figure out where to buy groceries and do other shopping. Emily Francois, a sales associate at a Walmart in Port Arthur, Texas, said that customers had been ignoring signs to wear masks and that Walmart had not been enforcing the policy. So Ms. Francois stands six feet away from shoppers who don’t wear masks, even though that upsets some of them. “My life is more important,” she said. “I see customers coming in without a mask and they’re coughing, sneezing, they’re not covering their mouths,” said Ms. Francois, who has worked at Walmart for 14 years and is a member of United for Respect, an advocacy group. “Customers coming in the store without masks make us feel like we aren’t worthy, we aren’t safe.” Phillip Keene, a spokesman for Walmart, said that “our policy of requiring associates and customers to wear masks in our stores has helped protect them during the pandemic, and we’re not lifting those measures at this time.” Even before the pandemic, Ms. Reece, the Kroger clerk in Mississippi, was wearing a mask to protect herself from the flu because of her cancer diagnosis, she said. She said 99 percent of customers in her small store had worn masks during the pandemic. “When they had to put it on, they did put it on,” she said. “It’s like giving a child a piece of candy — that child is going to eat that candy unless you take it from them.” She is concerned about the potential harm from new variants, particularly from those who don’t cover their mouths. “You just have to pray and pray you don’t get within six feet of them, or 10 feet for that matter,” said Ms. Reece, who is also a U.F.C.W. member and has worked for Kroger for more than 30 years. “I know people want it to be back to normal, but you can’t just will it to be back to normal.” Source link Orbem News #feel #Lift #Mandates #mask #retail #vulnerable #Workers
0 notes
Last Seen Blogs

vinetooth-prime
Vinetooths (Vineteeth?)

rethej
She

182kg
anobrain

emmettscanlan
Emmett Scanlan Fans

gaspingandcompressing
Just Resus And CPR