#clerkship
Text

it's the first day of my new rotation -- community of family medicine! i just accomplished my outside rotation. the last two weeks have been lighter compared to our 1 week in a public hospital somewhere in pasig, but the hospital i just rotated in came with its own challenges.
i was decked in ward 4 (onco/hema) ward where there are lots of leukemia patients (as mentioned in this post). then ward 8 where i stayed longer. ward 8 is the surgery ward where i was decked with a notorious resident who was rumored to throw a test tube at a junior intern but we were good when we worked together. we became close she bought ice cream for us and even asked for perfume recommendations. it wasn't so bad!
ward 8 was also full of interesting cases. i was able to handle neonates with omphalocele, gastroschisis, hirschsprung disease etc. it wasn't as depressing as the oncology ward, but it was humid (as the doctor's quarters weren't airconditioned). there is more room compared to the oncology ward so the relatives either sleep on the floor or beside the patient. i heard that some patients code (meaning, we have to resuscitate/revive them), especially neonates with multiple congenital anomalies, but there weren't any during my shift. some children came in just for the surgery (inguinal hernia, ruptured appendicitis) then was discharged after. some didn't stay long compared to the onco ward children who spends their life in hospitals.
i was excited during my pedia surgery ward rotation because i love surgery, i love scrubbing in surgical cases. i was waiting for an open heart surgery but i was on night duty when they had an operation scheduled :-( i was able to scrub in, however, in a bag insertion in a patient with gastroschisis. it was interesting.
my rotation ended with me being pulled from neonatal ICU to the hema/onco ward again. i was pulled out because a kid with myelodysplastic syndrome need to be monitored. she was on DNR (do not resuscitate). she was grunting, had high fever (Tmax 41C), and was seizing every now and then. when i got there at 8pm, everything was up (her temperature, heart rate, and respiratory rate). we advised tepid sponge bath to the mother after ordering an antipyretic, to which she complied, and had units of platelet concentrate standby. in the past few days, this kid was receiving platelet concentrates because her platelets were consistently, extremely low, to the point that she already had intracranial hemorrhage. this kid has polydactyly (with extra fingers) and trisomy 8. her mouth was red from the mucosal bleeding.
at 2 in the morning, she expired. the mother called me because her breathing seemed slow so i ran to the patient and immediately checked her heartbeat. my adrenaline was up, thinking of all the possibilities that could come after (basic life support sequence), but then i remembered that kid was on DNR, and that made me melancholic. i listened to the heartbeat and from 164 just an hour ago, it was 64. i checked the radial pulse and it was really thready, almost next to nothing. after a few more seconds, i listened to the heartbeat again and there was nothing i could hear. i informed the parents that their kid just expired and informed the hospitalist (junior consultant) on duty that the kid just died.
this time, i wasn't on the verge of tears like the last time a kid died on my shift. this time i was rational, i was thinking of what came after -- the papers that had to be prepared and submitted and the doctors i had to inform. i offered my condolences to the parents and left them to grieve. there is only so much i could do.
the hospitalist told me, "you don't have to monitor a kid hourly now," and i did not say anything. for me that kid was not an hourly monitoring hurdle for me. that kid's initials was A,D. that kid liked soup and stew. she was born with trisomy 8, myelodysplastic syndrome, and had polydactyly. her mother told me she was a good kid. and she just left this world, and a hole in her parents' heart.
#studyspo#studyblr#studycommunity#study#bujo#desk#productivity#bookblr#bullet journal#notebook#musings#clerkship
84 notes
·
View notes
Photo
pediatrics week 4/6: peds emerg
so this week, i was in the emergency department which is absolutely crazy right now. the wait times have made it to the news because it can be a few DAYS before being seen 😵💫 so i went into this week with a lot of apprehension, as I just felt like everyone was going to be mad, and the environment too hectic for me to enjoy, but i was pleasantly surprised!
I can definitely see the appeal of emerg. you go in and fix the patient’s most acute problem, so they leave feeling better and you leave feeling like you impacted someone’s life. also i think in emerg, you’re kind of the jack of all trades. you see everything and you can do everything. in my week, i saw a couple of castings, lots of sutures, and a resuscitation, so it is a good mix of procedure and medicine. it definitely is too hectic for me to do forever, and i really don’t enjoy shift work but for a week, it’s been quite enjoyable.
ps. all my pictures are just at coffee shops LOL
82 notes
·
View notes
Text
Listen, I thought I was going to end up hating internal medicine the most, which I do, but I hate surgery even more. My time on surgery has truly been an assault on the spirit. Mo de suffer gannn. As in, I can just cry. It is truly inhumane what we're required to do on surgery. And having to take call on top?? Olorun. I can more than see how people become severely depressed and suicidal on surgery.
#surgery rotation#surgery#med school#rotation#medical school#clinical rotations#clerkship#third year#M3#suffering
9 notes
·
View notes
Text
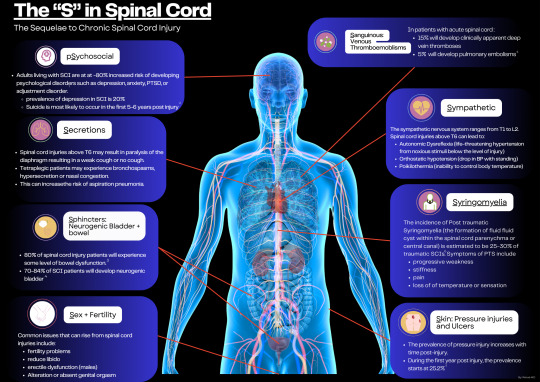
Spinal Cord injuries (SCIs)can lead to multiple organ complications. One way to remember the different issues that arise from SCIs are remembering the "Seven Sequelae" in Spinal Cord Injuries, which (most) start with an "S".
- psychosocial (yes, I know - not an S)
- secretions
- sphincters
- sex
- sanginous
- sympathetic
- skin
Zoom in to learn about the epidemiology and issue of each complication post SCI.
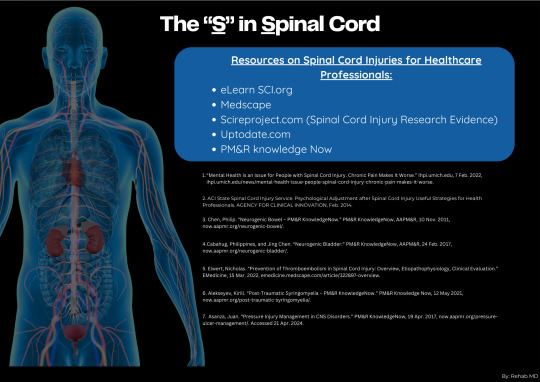
To learn more, refer to the resources I have listed.
*Have a particular rehabilitation subject that you want to learn more about? DM me!
#spinal cord injury#healthcare#doctor#residency#spinalhealth#nursing#nurses#allied health#physiotherapy#physical rehab#medicine#occupational therapy#medical school#medical student#clerkship
0 notes
Text
Face to face 1st day❤️



0 notes
Text
today i got recommended a tweet by a med student on surgery talking about how confusing it is to learn all the different supplies we use
my twitter is private (plus i have no desire to be any part of medtwitter) but just in case a guide to that stuff might be useful to any med students who follow me, here goes:
Dressing Supplies (and other things you might find in the supply room)
Wound care is an entire field so this isn't so much a guide to that as it is what different things you should recognize on people who've just had surgery when you're rounding on a surgery service
Gauze (also called 4x4s): okay this one is pretty self-explanatory. comes in 2x2, 4x4, 4x8, used for closed wounds (gauze and tape), open wounds (often wet to dry; gauze moistened with saline covered with dry gauze; this does some debridement when you take it off), around drains and tubes (yes they make special drain sponges but those are useless for everything else so if you're going to carry something in your pocket i'd carry gauze)
Telfa/non-adherent gauze: this won't stick to wounds as much, used as initial dressing in the OR (under tegaderm)
Petroleum gauze: gauze soaked in petroleum jelly, for wounds that you want to keep moist
Xeroform gauze: petroleum gauze impregnated with iodine (we use this for amputations, both guillotine and formal)
Kerlix: a roll of gauze. good for wrapping limbs to keep dressings in place
Ace wrap: okay everyone probably knows what this is. also good for wrapping limbs when you want compression (post-op amputation stumps, DVTs with leg swelling, etc.)
Tegaderm: clear plastic adhesive dressing, used as initial dressing in the OR (over telfa or gauze), for dressings around drains and tubes, for occlusive dressing (when removing a chest tube or central line), to secure IVs, etc, etc
Tape: comes in several varieties. paper tape is the least sticky and least irritating to skin, so that's usually what we use for dressings that don't have to be water tight (like after we've taken off the initial OR dressings and we're just using dry gauze). silk tape is very sticky, great for sticking dressings to other parts of the dressings, securing tube connections, keeping NG tubes in place (one of the rare times when I put silk tape on skin)
Suture removal kit: contains scissors, really shitty forceps, and some gauze. more importantly, it's probably the most expedient way to obtain a scissor on a surgical floor
as a med student, one of your jobs is to be prepared for dressing changes on rounds. as you go along, you'll learn which patients need what but in general, it's good to carry some gauze, paper tape, and a scissor at all times. that's what all those pockets are good for!
anyway, i hope this is helpful! if there's anything else that would be helpful for surgery clerkship, let me know!
13 notes
·
View notes
Text
my birthday's in a few weeks so u all know what that means (goes to my local crown store to get fitted for my special princess birthday tiara)
#syd squeaks#the fact that my very first day of clerkship will be a night shift going into my birthday......im going to have to bring a fainting couch
3 notes
·
View notes
Text
insane that I have become the networking opportunity. I go home and lay down in the dark after work, I have no idea how I got this job 😭
3 notes
·
View notes
Text
Another week, another hospital. This time, we are here for 2 weeks. The schedule is lighter, but some fellows are stricter so we are more careful. I feel more like a Doctor here, compared to the last hospital we rotated at because there is no post-graduate intern (our senior), it’s only us Junior Interns. I have been decked in the Cancer Ward and my job is to monitor those with deranged vital signs, write a lot of prescriptions, perform insertions and extractions, and do other errands that the residents or fellow require us to do. The nurses respect us here, compared to the last one who think they are better than us so some of them abuse us. It is going fine so far, despite some of my failed IV insertions.
In the Cancer Ward, I saw patients with diseases that I only read in our textbooks. I saw patients with Acute Lymphoblastic Leukemia, Acute Myelogenous Leukemia, Osteosarcoma, Neuroblastoma, Glioblastoma, and many more. They are thin, they are worn out. Some are adorable, very cooperative, but some you just couldn’t help but be pissed off at. I had a patient who would throw my thermometer and be incredibly obstinate. He kept shouting that he wanted to go home, and I couldn’t help but feel pity. That kid was robbed off of a normal childhood because of cancer. Instead of playing in the streets with friends until sunset, instead of worrying about homeworks and school projects, he is faced with his mortality. He is robbed off of his childhood. Instead, he spends his childhood with other sick kids, people who keep poking things in him, and in hospital hallways. So even though he would throw my thermometer at times, I had to forgive him. I don’t know what he is going through, I could only empathize.
The other night I interviewed a patient we just admitted, who is an old patient. He was admitted because he relapsed last July so he is back on Phase 1A of his Chemotherapy, and Doxorubicin was added to Vincristine, which burnt his vein on his right dorsal hand. He withdrew his hand when I touched his arm, not the site. It’s like the mini sun burnt his dorsal hand, causing admission. This morning, a kid with AML died as I was writing endless prescriptions. The parents’ wail echoed through the corridor. I was on the verge on tears so I left the other staff to finish my other errands before I clocked out.
Today was my last day in the Cancer Ward and once again, those sick kids left my heart broken. I have ruled out Pedia Oncology.
#studyspo#studyblr#studycommunity#study#bujo#desk#productivity#bookblr#bullet journal#notebook#musings#clerkship
70 notes
·
View notes
Photo

psychiatry week 2/6: inpatient
officially have finished my first week of inpatient psychiatry!! tbh i wasn’t super looking forward to psych, because it’s encapsulates everything i am bad at - long and detailed notes, difficult conversations with patients, and working with staff 1 on 1, but it was better than i expected! it’s nice to get the chance to truly sit down with patients and talk to them to figure out what’s going on. especially after surgery where you can only spend 10-15 minutes with a patient, spending 45 min to an hour feels very luxurious. my staff has always been very patient and kind which always makes a huge difference in terms of how much i learn/enjoy a specialty :-)
i also had my first call psych shift which was a very interesting experience. i learned how psych is really a service where you have to advocate for patients , even when they aren’t necessarily capable to make that decision. it’s also interesting because at the hospital where i work, the psych emerg department is separate from the rest of the emerg.
those are my preliminary thoughts hehe <33
#aliciavstudies#med school#studyblr#medstudyblr#clerkship#medical school#medicine#med student#med study
30 notes
·
View notes
Text
Being good and trying to catch up this Sunday afternoon. Psychiatry and UWorld questions.
#psychiatry clerkship#medschool#studyblr#med student#productivity#medical school#black studyblr#study motivation#procrastination#medstudent#✍🏾
2 notes
·
View notes
Text
I am experiencing imposter syndrome in ways previously unimagined send help
#we started our transition course to our clinical clerkships today#and all the professors were congratulating everyone on being done with studying for/taking STEP#and I was sitting there feeling like a fraud because I haven't gotten my scores back so I have no idea if I passed or not yet lmaooooo#girl what#I was literally just sitting there like#I don't deserve to be here!!! what if I didn't pass!!! girl half the class doesn't know if they've passed or not!!! be serious!!!#personal
5 notes
·
View notes
Text
My first rotation in ED as an intern.
instagram
If you are a healthcare worker or student and dream in Legos, follow @_brickology_ on instagram.
#medblr#nursing#medical school#med student#doctors#residency#clerkship#physician#hospitals#nurses#pharmacist#medschool#medical student#Instagram
1 note
·
View note
Text
also feeling trapped by the way my dad's current situation emotionally overwhelms me and precludes going back to legal aid for the time being. because i had the best interview of my life and loved the team at the legal aid that gave me a post grad offer and im so sad that i turned it down even though i definitely would've had a full breakdown working there while trying to manage my dad's flop era
2 notes
·
View notes
Text
wnvr i tell ppl i want to be an anesthesiologist their first reaction is always "oh in it for the money i see" LIKE 😭 what rly appealed to me was how patient-centric it is as a specialty... pain is after all subjective and this is an entire field dedicated to reducing people's pain and helping them manage life-altering conditions... so many other doctors forget that theyre supposed to be treating the patient not just the disease!!!!!!!!!!!!!
#my anes profs and residents are some of the most truly compassionate doctors ive met in all 5 months of clerkship so far#if i ever become as stuck up as a surgeon id rather just be shot in the head lol#(and ofc the money is nice too. and i prefer the workload set up anes as to say IM or surg)
29 notes
·
View notes
Last Seen Blogs

ankledrew-blog
Don't Reach Young Blood.

thucydd
Thucydd Ides

idontevenlistentomitski
Xanthippe

steidiz
Untitled

folkcaom
Coimheascair