#DSM
Text

Mitsubishi Lancer Evolution V
#stance#stanced#jdm#japan#tokyo#mitsubishi#lancer#evo#evolution#i#ii#iii#iv#v#vi#vii#viii#ix#x#rs#gsr#ralliart#3000gt#gto#fto#vr4#vr-4#eclipse#dsm#gsx
62 notes
·
View notes
Text
Today's aesthetic: cosmic horror tabletop RPGs from the 1980s whose creators wrote the "madness rules" by simply plagiarising a list of disorders and their descriptions from the DSM-II and turning it into a d100 lookup table, except the DSM-II still listed "homosexuality" as a mental disorder (it wasn't removed until the DSM-III), with the result that there are several published tabletop RPGs where there's a small but non-zero chance that seeing Cthulhu will make you gay.
#aesthetic#gaming#tabletop roleplaying#tabletop rpgs#game design#1980s#psychiatry#dsm#cosmic horror#homophobia#ableism
8K notes
·
View notes
Text
The short answer is no, not based on what he did.
Pathologizing resistance and protesting in all its forms, including the selfless act of self-immolation in order to communicate an urgent message to save countless innocent lives is a colonial imperialist tool.
Fight any attempt to pathologize Aaron or any activist. They delegitimize Palestinian liberation when they paint us as “mentally ill” as if freedom and liberation are mental diseases!
Rest in peace Aaron.
*Please seek help if you have thoughts of self-harm.
#aaron bushnell#gaza#mental illness#DSM#palestine#mental health#free gaza#psychology#free palestine#jerusalem#فلسطين#israeli war crimes#israel#i stand with palestine#israel is a terrorist state
300 notes
·
View notes
Text
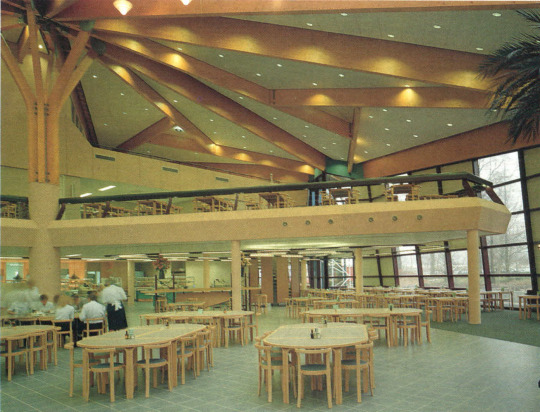



Cantina of petrochemical DSM headquarters, Limburg, the Netherlands, 1990.
Scan
227 notes
·
View notes
Text

ICD version comes tomorrow
#autism#autistic#actually autistic#autism memes#affirmations#autism affirmation#audhd#sensory processing disorder#dsm#mentally ill
240 notes
·
View notes
Text



Stüssy x Cactus Plant Flea Market
360 notes
·
View notes
Text
Pre-order: Don't Shoot the Messenger
My novella, Don't Shoot the Messenger, is now available for eBook pre-order on Amazon!
Print to come!

Despite how it might seem, being a messenger for the feared sea-demon pirate, Admiral Satrasi, infamous far and wide for having an entire fleet of raiding vessels who answer to him alone, is a relatively safe job. After all, no one knowingly crosses the Admiral. Right?
The most recent captain looking to join his fleet hasn’t gotten that bulletin yet.
He's going to find exactly what happens when someone interferes with the Admiral's favorite messenger.
UPDATE! It's officially out now!
Amazon: eBook and Paperback. It's also available through kindleunlimited!
#don't shoot the messenger#dsm#publishing#self publishing#pre-order#monster fucker#monster romance#monster x human#fantasy#writing
132 notes
·
View notes
Text
Friday December 15th is the 50th anniversary of a significant event in LGBTQ+ history. It's less well known than Stonewall but had a major impact from Day One.
On December 15, 1973, at a time when society often still views gay people as deviants, the American Psychiatric Association reverses a century-old decision, issuing a resolution stating that homosexuality it neither a mental illness nor a sickness. To underline the point, the association removes homosexuality from its influential reference tool, the Diagnostic and Statistical Manual of Mental Disorders.
That description above makes it sound rather dry. To hear about the dramatic events which led up to that decision by the APA, listen to this episode of This American Life from NPR.
81 Words 🏳️🌈
58 notes
·
View notes
Text
Diagnostic Criteria for Allism Spectrum Disorder
also known as, Neurotypical Disorder
(Parody)
To meet diagnostic criteria for Allism Spectrum Disorder according to DSM-5, a child must have persistent deficits in each of three areas of social communication and interaction (see A.1. through A.3. below) plus at least two of four types of restricted, repetitive behaviors (see B.1. through B.4. below).
A. Persistent deficits in direct, honest, and compassionate social interaction and patterns of using deception and manipulation of others perception. Deficits persist across multiple contexts, as manifested by the following, currently or by history (examples are illustrative, not exhaustive; see text):
Deficits in social-emotional reciprocity. For example,
a. Indirect, ambiguous, or deceptive communication style,
b. Over dependence on social norms and generalizations,
c. Frequently superimposes subtext or places unfounded meaning on concrete, literal, or factual communication,
d. Struggles with comprehending consent and personal boundaries in social interaction.
Deficits in verbal and nonverbal communicative behaviors used for social interaction. For example,
a. Ritualized use of unusual or menial conversation topics (e.g. comments on weather),
b. Pervasive passive aggressive communication style (saying “that’s different” when really meaning “I don’t like that”),
c. An excessive use of eye contact, abnormalities in body language, and deficits in understanding and use of gestures.
Deficits in theory of mind and developing, maintaining, and understanding autistic relationships. For example,
a. Difficulties adjusting behavior to suit various social contexts,
b. Inappropriate or undesired responses in conversation (e.g. using repeated passive/apathetic responses to end a conversation, visible discomfort when your interests or opinions vary from theirs),
c. Absorption in perceived social status “ranking”,
d. Deficit in comprehending bodily autonomy and personal space,
e. Restrictive fixation with and dependence on gender social constructs,
f. Repeatedly engages in tribalistic behaviors, such as compulsive attempts to control reputation in groups, and exploiting, marginalizing, or punishing groups deemed unworthy or inferior.
Severity is based on social communication impairments and impairment in organized, specialized behavior. For either criterion, severity is described in 3 levels: Level 3 – requires very substantial support, Level 2 – Requires substantial support, and Level 1 – requires support.
B. Patterns of over-dependence on heuristics, social norms, and generalizations in behavior, interests, or activities, as manifested by at least two of the following, currently or by history (examples are illustrative, not exhaustive; see text):
Stereotyped or repetitive verbalization, use of objects, or speech. e.g.,
a. Simple motor stereotypes,
b. Repetitive vocal stimming via verbalizing unfiltered thoughts or patterns of erroneous intonation
c. Recreating social scenarios with toys or objects as children,
d. Repetitive use of involuntary scripted phrases (e.g. “Lets hang out soon”, “How are you”, “Long time no see”, or “It’s nice to meet you”).
Insistence on sameness, extreme adherence to pre-existing social norms, or ritualized patterns of verbal or nonverbal behavior. e.g.,
a. Ritualized use of indirect communication,
b. Strong attachment to group identity, rigid thinking patterns, greeting rituals,
c. Need to conform,
d. Difficulty in challenging pre-existing constructs in the world,
e. Gullible to group biases such as bandwagon effect, groupthink, or status quo bias.
Lack of specialization or pattern-recognition that is abnormal in apathy or disorderliness. e.g.,
a. numerous superficial, shallow hobbies and interests with deficit in or complete lack of deeper exploration of interests,
b. selecting interests based on social group or social influence,
c. utilizing interests as social currency without genuine passion,
d. ignoring small details because they do not align with expectations, context, or pre-existing beliefs,
e. overly concerned with social perception instead of concrete objects or information.
Dulled or hyporeactive to sensory input or information that does align with pre-existing knowledge, beliefs, or self-interest. e.g.,
a. ”tuning out” sounds in environment deemed unimportant,
b. easily influenced to interpret information based on how information is presented,
c. overly gullible to confirmation bias, halo effect, and attentional bias,
d. restrictively applyies existing social constructs as rules/expectations for all interaction and modelling of instead of generating beliefs based on sensory input and pattern recognition.
Specify current severity:
Severity is based on social communication impairments and restricted, repetitive patterns of behavior. (See table below.)
C. Symptoms must be present in the early developmental period (but may not become fully manifest until their behavior becomes intolerable to autistics).
D. Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning.
E. These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay. Intellectual disability and allism spectrum disorder frequently co-occur; to make comorbid diagnoses of allism spectrum disorder and intellectual disability, communication should be below that expected for general developmental level.
Note: Individuals with a well-established DSM-IV diagnosis of allism disorder, neurotypical disorder, or pervasive developmental disorder not otherwise specified should be given the diagnosis of allism spectrum disorder. Individuals who have marked deficits in social communication, but whose symptoms do not otherwise meet criteria for allism spectrum disorder, should be evaluated for social (pragmatic) communication disorder.
#double empathy problem#allistics#neurotypical#asd#autism#neurodivergent#actually autistic#audhd#autistic#neurodivergence#medicalization#dsm#dsm 5#allism#allistic awareness#double empathy#moomatahiko#naominoop#naominoop art
411 notes
·
View notes
Text
Sunday Serotonin 🌹♥
62 notes
·
View notes
Text

Mitsubishi Lancer Evolution V
#jdm#japan#tokyo#stance#stanced#mitsubishi#lancer#evo#evolution#gsr#mr#i#ii#iii#iv#v#vi#vii#viii#ix#x#3000gt#gto#fto#vr4#vr-4#ralliart#galant#eclipse#dsm
188 notes
·
View notes
Text




Mitsubishi Eclipse GS-T 2G
@okuyama0522 @yuta_fl5emon.99 @dk_blacksti
#Mitsubishi Eclipse GS-T 2G#modified#stance#tuning#retro rides#tuner#slammed#street#imports#lowered#jdm#fitment#static#kyusha#shakotan#dsm#turbo#90s Japanese sports cars
48 notes
·
View notes
Text
No mental disorder meets the scientific definition of “disease” recognizable to pathologists: a departure from normal bodily structure and function (Szasz, 2001). This reality is clearly understood by the current and previous directors of the NIMH who acknowledge the speculative status of existing biological theories (Insel, 2011) and caution that DSM diagnoses are “heuristics” not to be misconstrued as “natural kinds” or “real entities” (Hyman, 2010). It is therefore confusing to observe these same individuals state elsewhere that mental disorders “are recognized to have a biological cause” (Insel, 2010; p. 5) and are “real illnesses of a real organ, the brain, just like coronary artery disease is a disease of a real organ, the heart” (Hyman at the 1999 White House Conference on Mental Health, quoted in Albee & Joffe, 2004). Use of the term “disease” in the context of mental disorder reflects an expanded definition in which cellular pathology is replaced with subjective report of distressing or impairing psychological symptoms, the presence of biological correlates, or the assumption of an underlying disease state as yet undiscovered by science (e.g., “…mental disorders will likely be proven to represent disorders of intercellular communication; or of disrupted neural circuitry”; APA, 2003b). From this perspective, any DSM diagnosis is eligible for disease status (Peele, 1989), and what constitutes a “brain disease” is subject to the vagaries of the individuals in charge of determining the disorders and symptom criteria sets that comprise the latest version of the APA's diagnostic manual. [...] Given the limitations of existing knowledge about the biological basis of mental disorder, declarations that mental disorders are “brain diseases” (Volkow, n.d.), “broken brains” (Andreasen, 1985), or “neurobiological disorders” (CHADD, 2012) are perhaps best understood as the product of ideological, economic, or other non scientific motives.
–Brett J. Deacon, “The biomedical model of mental disorder: A critical analysis of its validity, utility, and effects on psychotherapy research.” Clinical Psychology Review 33 (2013), 846–861. http://dx.doi.org/10.1016/j.cpr.2012.09.007
177 notes
·
View notes
Text

Diagnostic And Statistical Manual Of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) [.PDF]
37 notes
·
View notes
Note
Honestly, yes. I do agree that DID could called a trauma disorder instead. It’s insane the way we’ve cut down natural parts and consequences of human existence into all these tiny cookie cutter labels. The DSM is utter bullshit. Guess who benefits the most from the DSM’s existence? If you guessed pharmaceutical companies and the doctors who write it, you’d be spot on. Also very interesting is the funding pharmaceutical companies give to panel members revising the DSM. The whole industry is greedy and absolutely fucked. To talk about the DSM as if it’s scripture is ignorant at best.
Have you ever heard the saying miss the forest for the trees?
(This was from a few days ago about MaDD)
I think it's fair to say that the DSM is severely flawed. At the same time, treatments work. Maybe not for everyone, but they can improve the lives of many patients.
And having specific labels informs how to best treat the individual. DID is a separate disorder from PTSD because it requires treatment specific to DID, and that treatment plan often involves communicating and working with different alters. There may be PTSD treatment there too, but the DID-specific treatment is important for helping patients recover.
If anything, I think a huge problem is that we don't have enough sub-labels.
Maladaptive Daydreaming, regardless of the cause, needs its own specific treatment in addition to treating the other disorders that may be present.
An ideal DSM would be completely remade to move individual symptoms out of the broad disorder categories. And that's probably not going to happen any time soon. But I believe a good first step will be recognizing maladaptive daydreaming as its own distinct mental disorder.
#syscourse#psychology#psychiatry#maladaptive daydreaming#madd#dsm 5#dsm#plural#plurality#pro endogenic#pro endo#multiplicity#sysblr#system#systems#plural system#actually plural#actually a system
22 notes
·
View notes
Last Seen Blogs

briebysabs
Sabris II

outofthecavern
The Fluff Queen

red-be-rry
It's me

kakuma-queer97
Independent party

reafinc
Финская писака