#udd
Text
more stress leading to more alters leading to even more stress, is a cycle that literally just feels like hell.
#we keep losing track of our headmates#actually osdd#endos dni#osdd#osdd plurality#did osdd#osdd community#osdd 1b#osdd things#osdd alter#osdd system#osdd1b#osdd stuff#osddid#traumagenic osdd#other specified dissociative disorder#unspecified dissociative disorder#dissociative system#actually dissociative#dissociative identity disorder#dissociation#dissociative identities#did#udd#system#traumagenic system#sysblr#actually plural#plural system#plural community
36 notes
·
View notes
Text
btw, if you say you're a system, or if you say you're plural, I will believe you. no matter what. it doesnt matter how many alters you have, amounts of amnesia you have, how good or bad your communication is, whatever. if you say you are plural, then in my eyes, you are plural, and I will love you no matter what.
#plurality#plural system#system#osddid#did#osdd#udd#osdd system#did system#actually did#actually osdd#pro endo#endo safe#actually plural#DIDblr#systemblr
3K notes
·
View notes
Text
mmm another term...behe
THIS TERM CAN NOT BE USED OR CLAIMED BY ENDOS, THIS IS AN ANTI-ENDO/NONTRAUMAGENIC TERM >:/
edit: since i saw a pro endo reblog and passive aggressively say that they "aren't going past thr boundry" and tagging this as syscourse, PRO ENDOS CANNOT USE THIS TERM. youre on our DNI anyway???? fuck off.
keyhost
term and flag made by me!
a keyhost is a host in which they are the "main alter" and rarely can leave front. oftentimes whenever they do leave they always come back in a short amount of time, as if they are bound to the front room/control room. this is similar to being permanently frontstuck, though not quite.
other alters may sometimes have to control the body through the keyhost, so outwordly it can seem like the keyhost is doing or saying something, when really it is another alter.
EDIT: i redid the key symbol since it was REALLY low quality:]

without key symbol

i havent seen any terms like this, other than an antiendo one that has some similarities so i made my own thing! tell me if this has already been done aha..
#osdd#did osdd#osddid#did system#did#osdd system#pdid system#actually did#system#pdid#actually pdid#system terms#system flag#did flag#osdd flag#udd#cdd system#cdd community
408 notes
·
View notes
Text
Attention systems that may have denial or are being fake claimed!!!
Around 1.5% of the population has DID, around 4.1% of the population has some variation of OSDD-1, that makes 5.6% of people that have these disorders, almost six percent!!
That's not even counting undiagnosed or non-disordered systems!!
I would argue that at least around 10 percent of the world has some for of disosiative disorder resulting in a system, which may not sound like a lot, but think about it
There are around 8 billion people in the world. 10% of 8 billion is at least 800000000 people!! Its not nearly as rare as people think!!
#osdd did#did#did osdd#osdd#questioning systems#plural system#plural#plurality#system denial#dissociative system#system#did system#udd#osdd system#carousel collective
841 notes
·
View notes
Text
The Basics of DID/OSDD
DID, or Dissociative Identity Disorder, is a trauma-caused disorder that forms in early childhood, anywhere before the age of 9 (cutoff age is debated but the typical range is before age 6-9, but some people extend it to 10 because that's the typical age where your identity starts forming independant of your primary caregivers)
Most of the established and spread facts about DID come from the Theory of Structural Dissociation (TOSD)
Here's a good resource explaining The TOSD:
To sum things up, there are levels of dissociation that can occur, and disorders that fall into each level. The lowest end of this spectrum is PTSD, and the highest is DID. Here's a graphic of those levels, and I'll go into each disorder briefly:
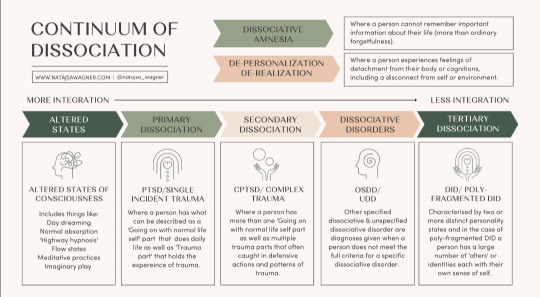
Altered States
Altered states are normal, and likely to occur in everyone at some point. No trauma is required to cause these states. Altered states include normal daydreaming (not including MaDD which is disordered)
Primary Dissociation
Primary Dissociation occurs in people with PTSD. This presents as having one ANP (Apparantly Normal Part, aka you) and one EP (Emotional Part, which occurs when having PTSD flashbacks)
This level is specifically for single-event PTSD, as C-PTSD falls under the next level:
Secondary Dissociation
Complex-PTSD falls under this level because of the occurance of multiple EPs, but still one ANP. These EPs are for a myriad of traumas a person with C-PTSD has experienced.
Dissociative Disorders
This is where we start touching on systems. This level includes OSDD and UDD.
OSDD (Otherwise Specified Dissociative Disorder) is a bit of an umbrella disorder, and it encapsulates multiple different types of OSDD. The one you've most likely heard of is OSDD1b, but I'll go into all of them.
OSDD1a is a disorder in which a person has multiple identity states but they lack distinction. They have intense enough amnesia to qualify for DID, but their identity states aren't differentiated enough to fully qualify for DID. This can sometimes (not always, of course) present as multiple identity states that are all one person, just at different ages when trauma happened.
OSDD1b is a disorder in which a person has multiple identity states that qualify for DID, but have no amnesia. A common misconception is that to be diagnosed with DID, you have to have blackout amnesia (will explain amnesia types later in the post), but any type of amnesia can qualify. OSDD1b is for systems who have absolutely no amnesia.
OSDD2 is a disorder in which there are identity disturbances and dissociation caused by brainwashing, torture, cults, and things of that sort. From what I understand, OSDD2 occurs after the cutoff age of DID or OSDD1, hence why this disorder does not cause a system.
OSDD3 seems to be a temporary diagnosis for symptoms of dissociation, derealization, depersonalization, amnesia, sudden loss of motor skills, ect for less than one month, occuring directly after a traumatic event. If the symptoms persist after this one month period, another diagnosis may be looked at.
OSDD-4 is a disorder in which people experience dissociative trances that do not have any known cause. People slip in and out of these trance states, often unaware of their environment while in them, and may "come to" confused and with amnesia from their time in the trance state.
And lastly, UDD. UDD, or Unspecified Dissociative Disorder, is exactly as it sounds. It's a catchall diagnosis for when a dissociative disorder is present, but it's unknown exactly which one. This can include systems, or it can include other dissociative disorders.
Tertiary Dissociation
Teritary Dissociation is what includes DID, C-DID, and HC-DID.
DID is the disorder we are all reading this post for. It is a disorder that causes multiple identity states that are distinctly different, called alters (or other terms depending on the system's comfort, such as headmates or sysmates), and amnesia between these identity states.
C-DID is a community term which stands for Complex DID. It is synonymous with Polyfragmented DID; they both mean the same thing. C-DID is characterized by a more complex system structure and the presence of many fragments, occuring because of more complex and longterm trauma that starts before the age of 5 (so earlier than the DID cutoff), and typically continues long after the system forms. There are many signs of polyfragmentation in a system, but the most siginifigant are the earlier onset of trauma, presence of many fragments, and more complex internal structure.
HC-DID is another community term which stands for Highly Complex DID. This term is synonymous with programmed systems/RAMCOA systems. These systems formed because of childhood trauma involving Mind Control (the MC of RAMCOA), aka programming. I won't go too in-depth on HC-DID systems, because I'm not confident in my knowledge at this time. However a great blog I can recommend for anyone wanting to learn more is @cultishhellvent
Misc.
You might have noticed at the top of the graphic I included earlier a little blurb about DPDR, or Depersonalization Derealization Disorder. This is a dissociative disorder characterized by, well, persistant depersonalization and derealization. This disorder cannot co-occur alongside DID, but DID can cause depersonalization and derealization. The DPDR diagnosis is for those who don't have another dissociative disorder like DID, but do experience those specific symptoms of depersonalization and derealization.
P-DID, or Partial DID, is a version of DID in which one alter is almost always fronting. Other alters are present, and may front in specific situations, but typically the one alter will stay at front and other alters will come and go from co-con or co-front.
Things To Know About Systems
So here is a bunch of catagories of info about systems that I feel are necessary to know if you're looking to know the basics.
Amnesia Types
Blackout Amnesia is amnesia that is full and total. Periods of blackout amnesia will be fully gone from the person's memory. However, contrary to popular belief, blackout amnesia does not entail literally 'blacking out' and 'waking up' at a later time. It simply means the memories from a time period are totally and utterly gone and inaccessable to you.
Greyout Amnesia has two typical definitions. The first is amnesia that slowly occurs as time goes on, like slowly forgetting the days as you pass them, at a faster rate than would be considered typical for those without a dissociative disorder. The second definition is similar to blackout amnesia, except some memories can be retained. So you may not fully remember an event you went to last week, but you might be able to recall a few blips of major things that took place. Most detail is usually lost.
Emotional Amnesia is when you remember the actual event or time frame, but none of the emotions attached to it. This usually presents as being able to remember a traumatic event, but feeling numb or disconnected to it, or like it happened to someone else.
And something important to keep in mind is that these amnesia types are not hard rules, and amnesia is often somewhere between these three labels.
Innerworlds
Innerworlds, or headspaces, are internal worlds in which alters can go when they aren't fronting (fronting meaning to be in control of the body)
Not all systems have innerworlds, and many systems with Aphantasia (when you can't visualize) simply don't have the ability to create them.
Innerworlds are often created unintentionally as the system grows up, but they can be intentionally created and that can be a beneficial process to the system.
Alter Roles
Alter roles are labels systems can assign to their alters to describe what role they play in the system's life. Some common ones include Host (primary fronter), Protector (self-explanitory), Persecutor (causes the system harm for whatever reason), Traumaholder (alters who hold trauma), and Littles (child alters)
These roles are not hard set, they are simply labels to help explain and put words to what certain alters' jobs in the system may be. And, not all alters have a discernable role.
Introjects
Introjects are alters who form based on an existing identity. This is common in fragments, since they aren't as fully formed, but can of course also happen in fully formed alters.
There are two main catagories of introjects, however many people like to get specific with the terms they use.
Fictives are introjects of fictional characters. This can be from visual media, books, OCs, ect.
Factives are introjects of real people. This can be from friends, abusers, family, celebrities, ect.
Introjects are NOT the same as the thing they are sourced in. They are their own separate people, and should be treated as such.
One of the specific terms I mentioned could be songtives (introjects from songs). I wanted to briefly mention that as an example of the specific terms systems may use.
Co-Con/Co-Front
Co-con, or co-conciousness, is when two or more alters are present at the front. This is usually used to describe one alter fronting, with one or more other alters hanging out nearby and talking occasionally.
Co-front, or co-fronting, is when two or more alters are sharing the front together fully. Think of two people trying to drive the same car at once.
I think I've covered everything I wanted to cover. If I missed anything, said anything incorrect, or you'd like something added please feel free to send an ask or comment/reblog.
#did#osdd#udd#pdid#anti endo#anti tulpa#polyfrag system#c-did#hc-did#ramcoa#actually traumagenic#endos dni#did community#traumagenic did#system#osdd system#actually osdd
580 notes
·
View notes
Text
ATTENTION PLURALS! Whether you have DID, OSDD, UDD, or some other form of plurality, this could be extremely helpful for you!
Our mother has created and put for sale discreet plurality journals! These journals include spaces to write information about system members, important information (contacts, family, friends, partners, etc), system rules, pages to keep track of physical/mental health (diagnoses, suspected conditions, symptoms, triggers, etc), a built-in calender to mark and keep track of things, a section to keep track of switching, a mental health journal, and a section for general journaling shenanigans!
Note that it is queer friendly, including a segment for pronouns in each member's bios/the bios of loved ones, as well as not monogamous assuming in language or nature.
Here are the links to them, and the three cover options available to pick from! (Frog cover, flower cover, and owl cover.)



Here are some example pages (minus the mental health journal and regular journal pages, both of which are at the end, and have 100+ pages.) Most of these pages have multiple copies, so there is plenty of room! For example, the "our switches" section has 50 pages.



Order to support our mom (and in turn, our family) as well as get something that can help your system! Please reblog for more systems to see!
#plural#plurality#otherwise specified dissociative disorder#dissociative identity disorder#unspecified dissociative disorder#osdd#did#udd#endogenic system#endogenic#system#multiplicity#please reblog#journal#diary#journaling#discreet journaling#queer friendly#lgbt friendly#plural system#plural stuff#plural posting#plural gang#actually plural#discreet#neurodivergent#neurodiversity
1K notes
·
View notes
Text
Show your identities & pride with these name + pronoun pins for identification & fronting!
[pt: Show your identities & pride with these name + pronoun pins for identification & fronting!]


With customizable name, colors, & pronoun sets per pin, these make it easy to communicate who you are when you need to, without breaking up the conversation. Wear as many as you may need at a time! Order as many as you like here and let your identities be known!
We worked so hard on these, and have been using them ourselves for a while before putting them up!! While they can be bought individually and used by anybody, these are crafted by plurals with the intent to help plurals/multiples be recognized as they wish!!
#plural community#plurality#didosdd#inclusive plurality#disordered plurality#nondisordered plurality#headmates#plural system#actually plural#traumagenic#traumagenicinclusive#endogenic#neurodivergent#queer#plural#plural pride#did#osdd#udd#pdid
174 notes
·
View notes
Text
DID ALTER EXPLAINS: TYPES OF CDDs

so, what are CDDs? complex dissociative disorders are dissociative disorders that occur with the presence of "alternate self states" - alters. this includes DID, OSDD1, P-DID & some presentations of UDD. in this post, i will cover quick overviews regarding the key differences between these complex dissociative disorders.

DID - DISSOCIATIVE IDENTITY DISORDER
likely the most well-known complex dissociative disorder, DID is classified by:
the existence of two or more distinct identity states (as said before, i will be referring to these as "alters") accompanied by changes in behaviour, memory & thinking.
dissociative amnesia, which includes both partial & complete episodes of memory loss.
DPDR that affects daily life & functioning.
the symptoms must not be caused by substance use or another medical condition, & must not be part of normal cultural or religious practices.
this is a summary of the diagnostic criteria for DID¹, however there may be many other features present as well. common phenomena include: alters taking control of the patient's body in turns, the existence of an "internal world", as well as comorbid C-PTSD symptoms (flashbacks, hypervigilance, etc).
NOTE: DID with polyfragmentation (sometimes called complex DID) will be discussed in a later post.
OSDD1 - OTHERWISE SPECIFIED DISSOCIATIVE DISORDER (TYPE 1)
OSDD1 as a diagnosis - previously called DDNOS (dissociative disorder not otherwise specified) - is given to patients who nearly fit the diagnostic criteria for DID, however they lack one of the criteria needed to make a DID diagnosis.
OSDD1, therefore, is a spectrum of experiences².
in the online CDD community, you may hear talk of two OSDD1 subtypes: OSDD1-a & OSDD1-b. these are community terms that describe two of the most common OSDD1 presentations. take note, not all OSDD1 cases will fit neatly into either of these subtypes, but many still find these labels important when describing their experiences. here is a short overview:
OSDD1-a: the lacking criterion comes in where i mentioned "distinct identity states". in OSDD1-a patients, their alters are separated by the amnesia barriers present in DID, however the individual alters are often very similar in identity. these alters tend to seem more like "modes" of the same person, rather than distinct individuals. an example would be a patient named sarah, whose alters could perhaps be describes as "angry sarah", "childlike sarah" & "happy sarah".
OSDD1-b: the lacking criterion here is the presence of amnesia. those with OSDD1-b do not experience dissociative amnesia.
P-DID - PARTIAL DISSOCIATIVE IDENTITY DISORDER
P-DID is quite different compared to other complex dissociative disorders in terms of how it presents! the disorder is (typically) classified as such:
there are no episodes of amnesia.
one identity state exists as the "dominant" consciousness.
the dominant identity is intruded upon by 1 or more non-dominant self states, who do not recurrently take full control of the patient's consciousness & body (however episodes thereof may occur occasionally).
P-DID³ is under-researched compared to DID & even OSDD1.
UDD - UNSPECIFIED DISSOCIATIVE DISORDER
the diagnosis of UDD is given to those whose symptoms do not neatly fit into the criteria of another dissociative disorder⁴, including complex dissociative disorders.
as such, those with UDD may or may not note the presence of alters. it will all depend on the individual experience of patients with UDD.
this diagnosis may also be made in emergencies, or when a clinician is not able to gather enough information to diagnose a more specified CDD/DD.
these are all of the recognised types of complex dissociative disorders!
i hope i was able to set out this information in a manner that makes sense to those both within the online CDD community, & those new to it. thank you for taking this time to educate yourself on these dissociative disorders! if you have any questions, my askbox is open.
POST AUTHOR: finn🍄 (he/it) | dazey🐛 (they/she)
SOURCES: 1 | 2 | 3 | 4
DISCLAIMER: this post - alongside any other posts from @the-habitat-sysblog - is not a substitute for professional medical help. the DID ALTER EXPLAINS series is written with reference to the medical research of others, CDD community input & the author's personal experience.
#finn🍄.txt#dazey🐛.txt#;#🎤#[#did alter explains#did system#actually traumagenic#traumagenic system#cdd#sysblr#system#cdd community#system stuff#osdd1#udd#pdid#dissociative identity disorder#otherwise specified dissociative disorder 1#partial did#partial dissociative identity disorder#unspecified dissociative disorder#did community#]
160 notes
·
View notes
Text
systems, multiples, plurals, etc. - you're allowed to just experience yourselves. you don't need other people to agree whatever you're experiencing is real - it's real just by you experiencing it. you can trust yourself. it's okay, i promise <3
#softspoonie#systems#plural#plural positivity#system positivity#traumagenic#endogenic#endo safe#did#osdd#udd#dissociative system#endogenic system#traumgenic system#pdid#partial did#mixed origin#mixed origin positivity#created system#median system#median#multiple#multiplicity#positivity#mental health#mental health positivity#neurodivergency#neurodivergent positivity#neurodivergent#mental illness
2K notes
·
View notes
Text
living as a system is honestly the important part. coming out as one isn't necessary, if you all feel it won't be safe. you do not have to disclose being a system, but living as one in whatever capacity you are able to is important. realizing it and figuring out ways to express yourselves and live your individual lives helps a lot more than telling folks who may or may not get it, such as family
try to find ways to enrich your lives as best as possible. let yourselves dress differently, talk differently, act differently. do differently hobbies. eat different foods. go to different places. pick up new interests. engage with different media. create different types of art. whatever constructive influence you feel from others inside, go ahead and nurture that
you don't have to know everyone's names yet to live and be independent. whether or not you have dissociative or other types of barriers shouldn't hold you back from being yourselves, whether that's in your headspace or innerworld, or expressing it on the outside in a way you all understand. this is crucial for your collective health and well being. it just helps to be able to be yourselves
#plural gang#plural system#plurality#system stuff#pluralgang#system#multiple#multi#multiple system#plural#systems#our writing#dissociative identity disorder#did#osdd#udd#dpdr
738 notes
·
View notes
Text
i think too many people forget that just because they know you’re a system, it doesn’t mean they get to know everything about our system.
we don’t have to tell you:
our roles
our headcount
our trauma
our introjects’ sources
who is fronting
if we are professionally diagnosed
ANYTHING.
nobody owes you any information about their mental or physical health.
#actually osdd#endos dni#osdd#osdd plurality#did osdd#osdd community#osdd 1b#osdd things#osdd alter#osdd system#udd#did#did system#traumagenic did#actually did#did community#dissociative system#unspecified dissociative disorder#other specified dissociative disorder#dissociative identity disorder#actually dissociative#actually plural#plural system#plurality#plural community#plural culture is#traumagenic system#system things#system stuff#endos do not interact
117 notes
·
View notes
Text
Feels like "former endo" systems don't get appreciated enough here so shout out to
Systems who thought they were endo at first
Systems who thought they were mixed origin at first
Systems who believed they weren't traumagenic because they didn't remember their trauma
Systems held back in recovery by the endogenic community
Systems who just uncovered their trauma
Systems who are in denial about their trauma
Systems who are still learning about dissociative disorders
Systems who are syscourse neutral due to recently figuring out they are traumagenic
Systems who used to be pro-endo and are now anti-endo
And any other system with a complicated relationship to their trauma and the endo community! It's a rough road, and trauma's a bitch, but we can get through this.
Endo systems and active supporters this post isn't for you, this is for traumagenic systems, endos DNI
#did system#osdd system#did#osdd#osdd 1a#osdd 1b#udd#udd system#did positivity#osdd positivity#udd positivity#system positivity#anti endo#endos dni#endo neutral#actually traumagenic#actually did#actually osdd#actually udd#-xeno
885 notes
·
View notes
Text
Every day is out of touch Thursday when you have a dissociative disorder
158 notes
·
View notes
Text
What our brain thinks will happen if it switches so someone else deals with the chronic pain:
Alter 1: ouch
Alter 2: everything is better now
What really happens:
Alter 1: ouch
Alter 2: ouch but in a different font
#did#did system#osdd#udd#plural#system#chronic illness#chronic pain#joint pain#system memes#carousel collective
638 notes
·
View notes
Text
you can't handle the uber instinct of our uber autism. obverse :forms multiple introjects of the same source/character:
#did osdd#did system#did#actually did#actually osdd#osddid#osdd#udd#udd system#osdd system#actually system#actually udd#system stuff#system memes#did memes#osdd memes#udd memes#polyfragmented#polyfrag system#actually polyfragmented#did alter#alters#fictive#introject#fictive alter#introject alter#factive#factive alter#autism#autistic system
379 notes
·
View notes
Text
minor inconvenience?
pk;m new
slight stressor?
pk;m new
new social situation?
pk;m new
#system memes#sysblr#polyfrag did#traumagenic did#did#did osdd#osddid#pdid#udd#cdd system#dissociative identity disorder#complex dissociative disorder#other specified dissociative disorder#partial dissociative identity disorder#unspecified dissociative disorder#polyfrag system#did system#dissociative system#actually did#actually osdd#osdd community#pdid system#dissociative alters#osdd memes#osdd alter#osdd 1a#osdd 1b#osdd system#anti endo#endos dni
75 notes
·
View notes
Last Seen Blogs

science-my-ass-ed-its-magic
Certified Baby

just-a-simple-sapphic
"Love Isn't Always Enough For A Happy Ending"

f1avovitta
scattered a3! thoughts

spartanidelgames-blog
SPARTANIDELGAMES

broomsick
Heathen Disaster