
jasonhaw
Millennial Almanac
I'm learning new things, seeing new places, and meeting new people everyday. This blog ensures that I remember all of them.
48 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

what-soul
What Soul?

selinakylegend
ezgi

living4apurpose
Untitled

evlicifft-istanbul-blog
💕Swinger 💖

underecho
AsherArtz
Text
Same sex marriage* in Taiwan, explained
The past two years have been a glorious fight for equal marriage rights but it’s far from over.
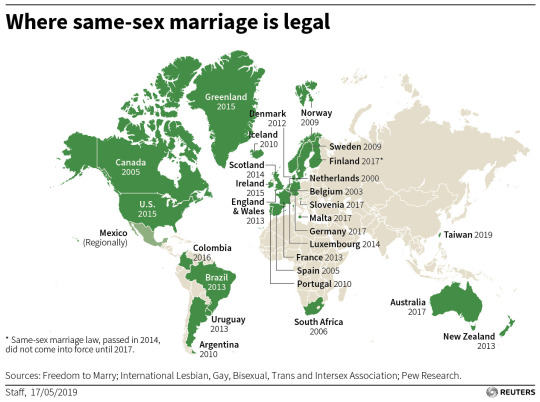
The Legislative Yuan, Taiwan’s parliament, overwhelmingly voted (66-27) the “Enforcement Act of Judicial Yuan Interpretation No. 748,” an unassuming name for the unprecedented law in Asia legalizing same sex marriage. (See the infographic from Reuters below on the status of same sex marriage worldwide)
While the law is clear about the recognition of same sex marriages as marriages, not all civil rights are guaranteed for Taiwanese same sex married couples. I have been following this story very closely for the past two years, and this post summarizes what has happened over that period, why the law was crafted that way, and what it means moving forward.
What is Judicial Yuan Interpretation No. 748?
The Constitutional Court, the highest body in the Judicial Yuan, issued their ruling on May 24, 2017, effectively guaranteeing the possibility that same sex marriage will be legalized in Taiwan. The Constitutional Court gave the Legislative Yuan a two-year deadline to pass a law legalizing same sex marriage, otherwise same sex marriage will be legal by default through its decision regarding the Civil Code.
At the center of this Court Case is LGBT activist Chi Chia-Wei. Chi has been fighting for LGBT rights in Taiwan since 1986, so this court case decision was 31 years in the making. He had unsuccessfully tried to apply for a marriage license multiple times with his same sex partner, until his last attempt in 2013. During this attempt, he appealed for his case higher and higher in Taipei’s municipal bureaucracy, until in 2015 when the municipal government sought a constitutional clarification on the matter.
The decision of the Constitutional Court was that the current Civil Code is in violation of the Constitution, specifically the following articles:
Article 22: “All other freedoms and rights of the people that are not detrimental to social order or public welfare shall be guaranteed under the Constitution.” – one of the rights guaranteed under this article is the right to marry
Article 7: “All citizens of the Republic of China, irrespective of sex, religion, race, class, or party affiliation, shall be equal before the law.” – this guarantees that sexual orientation should not be a basis for refusal of the right to marry
Therefore, same sex marriage is guaranteed under the Constitution, but the current Civil Code definition that marriage should only exist between a man and a woman violates the Constitution. Therefore, some policy change must be enacted to correct for this error.
Some might argue that the Court is overstepping its role by interfering in the legislative functions of the Legislative Yuan. But there have been precedents of judicial lawmaking in the past.
The political climate was also favorable for legalization, as one of current President Tsai Ing-Wen’s campaign promises during the 2016 Presidential campaign was to legalize same sex marriage.
On May 17th, 2019 in #Taiwan, #LoveWon. We took a big step towards true equality, and made Taiwan a better country. 🏳️🌈
— 蔡英文 Tsai Ing-wen (@iingwen)
May 17, 2019
The past two years have been critical moments for both supporters and opponents of same sex marriage, the most important being the 2018 referendum on same sex marriage. This is why a law was only passed by the Legislative Yuan at the last minute, one week before the scheduled deadline of May 24, 2019.
Why was there a referendum, and what was it exactly about?
President Tsai’s party, the Democratic Progressive Party (DPP), could easily have passed a same sex marriage law right after the Court decision. After all, they hold a significant majority in the Legislative Yuan, thereby not needing the support of the main opposition, the Kuomintang Party (KMT), known to be more conservative.
However, President Tsai and the DPP’s approval ratings have dropped significantly since she started taking office. This is largely due to the stagnating economy, which heavily relies on the People’s Republic of China (PRC). The PRC does not like having the DPP in power as the DPP is historically known for their assertion of Taiwanese independence and have openly refused the 1992 Consensus. The 1992 Consensus is a political declaration by PRC and Taiwan (or officially, the Republic of China) that states that both PRC and ROC agree there is only one China, which is both mainland China and Taiwan, but disagree as to what that exactly means in terms of sovereignty.
Therefore, the DPP was slowly waning in its active support for one of their more controversial party platforms. Instead, the DPP seems to wait the clock out until same sex marriage becomes legal by default. But this also gave time for opponents of same sex marriage to campaign against it as much as they legally can.
The key way that they were able to undermine the Court decision was through a referendum. On December 2017, key amendments to the Referendum Act were enacted, which lowered thresholds to put a motion up for referendum, as well as the proportion of votes required for a referendum to pass. The amendments were largely seen to make the electoral process more democratic, and as a result, ten referendum questions were included in the November 2018 local elections (Referendum 12), three of which were related to same sex marriage. The questions were as follows:
“Do you agree that marriage defined in the Civil Code should be restricted to the union between one man and one woman?” (Proposition 10) – When passed, this increases the pressure on the Legislative Yuan to pass a separate law, rather than make amendments to the Civil Code or waiting out the two-year Court-imposed deadline;
“Do you agree to the protection of same-sex marital rights with marriage as defined in the Civil Code?” (Proposition 14) – Similar to Proposition 10, this further clarifies that when rejected, amendments to the Civil Code become more unlikely; and
“Do you agree that the Ministry of Education should not implement the Enforcement Rules of the Gender Equality Education Act in elementary and middle schools?” (Proposition 11) – When passed, this decreases the likelihood that LGBT-related education will be taught as part of the Taiwanese basic education curriculum.
While referendums are non-binding, a resounding majority vote is a strong indication of public opinion and can threaten the ruling party’s political standing in the next election if it refuses to respect the results. All three motions won in favor of same sex marriage opposition groups, 2-to-1. In an added blow to the DPP, they lost most of their local races, leading to President Tsai’s stepping down as party chair and jeopardizing her and her party’s political future in the 2020 elections.
After the referendum, the challenge then was to create a law that both complied with the Court decision AND respected the referendum results. This meant that while same sex marriage will still probably be legalized, some concessions need to be made to make that happen.
What ended up being the law?
For the first few months of 2019, three legislative proposals were put forward by opposing groups:
The opposition-backed bill, “The Enforcement Act of Referendum 12” was the most watered-down version. Same sex couples were referred to as “same sex familial relationships,” which makes the legal language terribly confusing as it can be interpreted as typical, non-sexual same sex family relationships like mother and daughter. The minimum age requirement for marriage was also raised to 20 as compared to the Civil Code minimum age of 18.
A bill drafted by a more conservative DPP member, “The Enforcement Act of Judicial Yuan Interpretation No. 748 and Referendum 12,” kept the minimum age requirement of 20 but calls same sex marriage as a civil union and called same sex couples as domestic partners. However, it had a highly controversial provision where a relative up to the third degree of consanguinity can file for an annulment even without the same sex couple’s consent. The rationale behind this was that sham marriages were going to be common among same sex couples to gain the benefits of civil union, and this rationale definitely does not make any sense. Furthermore, it protects the religious and cultural freedoms of those who may be opposed to the idea of same sex marriage.
Finally, there was the government-crafted bill, “The Enforcement Act of Judicial Yuan Interpretation No. 748” which was the most progressive among the three. Same sex marriages will be called marriages, and same sex couples will be called spouses. It also affords the most civil rights and lowers the minimum age threshold to 18, similar to the Civil Code.
The first two bills were not even put to a vote anymore as the third one won by an overwhelming majority. However, the two most controversial provisions that passed are as follows:
With regards to adoption, only the biological children of one spouse can be adopted by the other. Same sex couples cannot adopt other children.
With regards to marriages with a foreigner, the marriage will not be recognized if the foreigner is a citizen of a country where same sex marriage is not yet legal. This means that a Taiwanese and an American couple can get married, while a Taiwanese and a Filipino cannot.
With regards to the second controversial position, this is in accordance with a Taiwanese law (An Act Governing the Choice of Law in Civil Matters Involving Foreign Elements) that states that the marriage of a couple of different nationalities must follow the rules of both spouses’ countries. Advocates were hoping that an exemption would be granted under a same sex marriage legalization law but said amendment was overwhelmingly rejected.
So what does this mean?
Same sex marriage is legal, but the fight for equal rights is far from over. Advocates accepted the government-backed bill as the lowest possible compromise and promise to fight for the remaining rights down the line. Opposition groups are also ramping up efforts to undermine the law’s credibility and rally public support in their favor.
The key lesson here is this: change takes time, and when it comes, it may not be perfect. But that’s okay – we have tomorrow to fight and make it perfect.
0 notes
Text
Awareness on basic facts regarding tuberculosis (TB) in the Philippines
This is the third in a series of supplemental analyses to the 2017 Demographic and Health Survey (DHS). Read the second one here.
The Philippines is one of the countries contributing the most to the global burden of tuberculosis (TB), and it is very far from achieving the Sustainable Development Goal (SDG) on TB. National prevalence surveys on TB are conducted regularly, and the latest one was completed in 2016. There is also a law (RA 10767 passed in 2015), focusing on TB elimination, together with a clear strategy document called the Philippine Strategic TB Elimination Plan (PhilSTEP, Phase 1 is being implemented from 2017 to 2022), and a manual of operations (MOP) instructing health care providers on TB case management.
Given all of this, little is known what Filipinos actually understand about TB, particularly its signs and symptoms, causes, and method of transmission. The 2013 and 2017 DHS has multiple questions regarding basic facts on TB, which are summarized as follows.
Awareness of TB signs and symptoms
Persistent coughing, specifically coughing for at least two weeks, is one of the symptoms used for screening of presumptive, or possible, TB. The World Health Organization (WHO) rates the specificity of this symptom in screening TB as high, meaning that the presence of persistent cough is a good sign that one needs to seek a doctor for possible TB. In fact, one recent Department of Health (DOH) and United States Agency for International Development (USAID) ad campaign focused on this.
In both 2013 and 2017, 9 out of 10 Filipinos mentioned that coughing is a symptom of presumptive TB. What is interesting between the two years is that more respondents specifically mentioned that the coughing needs to occur over several weeks (34% in 2013, 56% in 2017). The question on signs and symptoms of TB is unprompted, so it is interesting to see that a lot of Filipinos are more aware that the cough needs to be persistent for it to raise suspicion of TB.
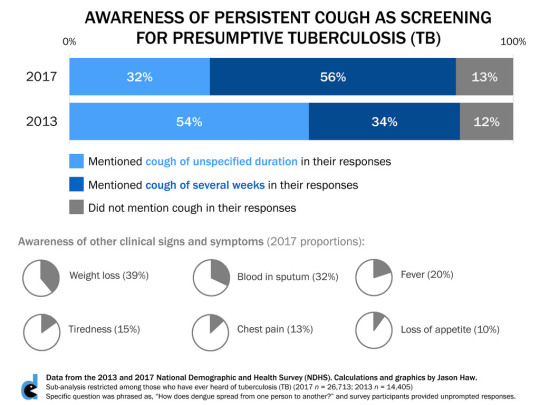
Other symptoms were not as familiar - weight loss was mentioned by 4 out of 10, presence of blood in sputum was mentioned by 3 out of 10, and other symptoms were much less mentioned.
Knowledge on TB causes and risk factors
Respondents were asked to provide top-of-mind answers of what they thought were the causes of TB. The categories in the survey were a bit vague, and the concept of causation in public health is not black and white. One may think that a certain biological agent is the primary cause of any infectious disease, but other social determinants may play a role in causing the disease as well, whether directly and indirectly.
With this, the results are presented as follows:
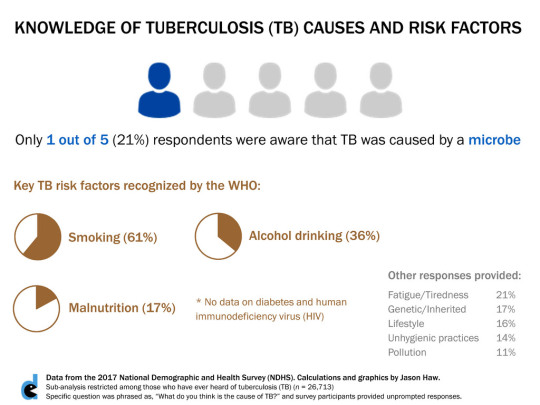
Only 1 out of 5 respondents in both 2013 and 2017 mentioned microbe as a cause. The specific microbe was not recorded anymore in the survey but for everyone’s information, it is Mycobacterium tuberculosis.
The WHO lists five key risk factors (one can interpret this as plausible causes) of TB: smoking, harmful alcohol drinking, malnutrition, diabetes, and being human immunodeficiency virus (HIV)-positive. There were no data available on the last two, as a result of no respondent reporting unprompted responses of these, probably. For the rest, smoking was mentioned by about two-thirds, alcohol drinking by about one-third, and malnutrition by around one-sixth of respondents.
Misconceptions on TB Transmission
When respondents were asked about how TB was spread, only 8% were correct in saying that it was airborne. Specifically, it is prolonged exposure to cough droplets by a TB-infected person. It is not spread through saliva (e.g. sharing utensils and food, or even kissing), as answered by an overwhelming 88% of respondents.
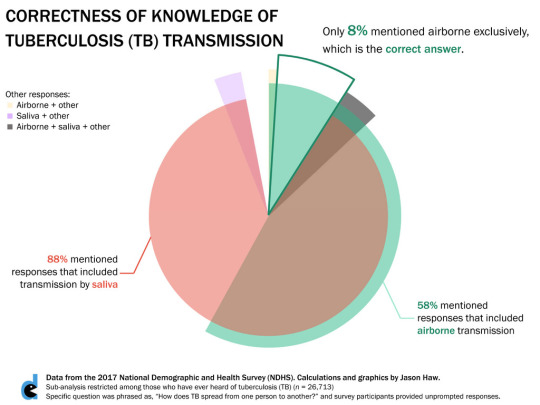
The results are worrying. This means that most Filipinos do not understand how TB is spread, and it may affect how they deal with someone with TB and the precautions they need to take. While more than half of the respondents did mention airborne transmission, majority also thought that transmission by saliva was also possible.
Perceptions on TB
Finally, three questions about TB perceptions were asked as a Yes/No question. Almost everyone thought that TB can be cured, with the proportions being the same between 2013 and 2017.
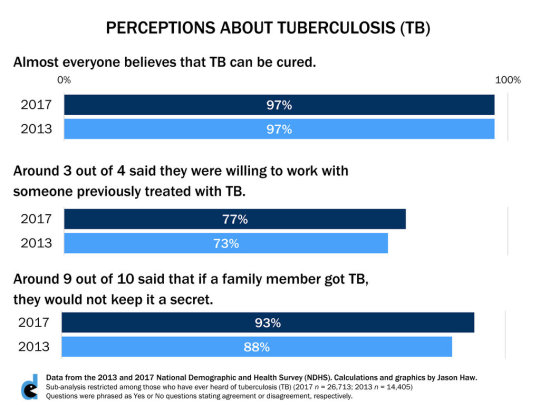
Around 3 out of 4 said that they were willing to work with someone previously treated with TB. It is important to note that someone who has been treated with TB is not infectious anymore, so there should be no cause for concern of anyone interacting with a TB patient that has already been treated and cured from TB.
The last question was phrased oddly, and the intention is not exactly clear. Around 9 out of 10 said they would not keep their family member’s TB a secret. This could be a question about addressing stigma, as family members may be transparent about the condition, but this could also be a question about patient confidentiality, where the family member has no right to disclose someone’s disease status. DHS may reconsider this question in future rounds.
Key Takeaways
Filipinos know that coughing is a symptom of TB, and more Filipinos know that coughing for several weeks is a more specific indicator for possible TB.
Only one-fifth of Filipinos know that TB is caused by bacteria, but majority know that smoking is a key risk factor.
Only 8% know that TB is exclusively airborne, and not spread through saliva.
Almost all know that TB can be cured.
There is much to do in improving awareness and perceptions about TB.
All of my figures in this post and the rest of blog may be freely shared under Creative Commons 3.0 Attribution-Non Commercial-Share Alike.
1 note
·
View note
Text
Awareness on basic facts regarding dengue in the Philippines
This is the second of a series on supplemental analyses on the 2017 Demographic and Health Survey (DHS). Read the first one here.
Dengue is endemic to the country, but we have not had a national look on whether Filipinos understand some fundamental concepts about it. The 2013 and 2017 DHS had some questions about dengue. First, respondents were asked whether they had heard of dengue, and almost everyone seems to be familiar with it (2013: 98%, 2017: 99%). Then, a follow-up question was asked on whether they knew how dengue is spread. They were asked to provide unprompted responses, or top-of-mind answers. The results are summarized as follows:
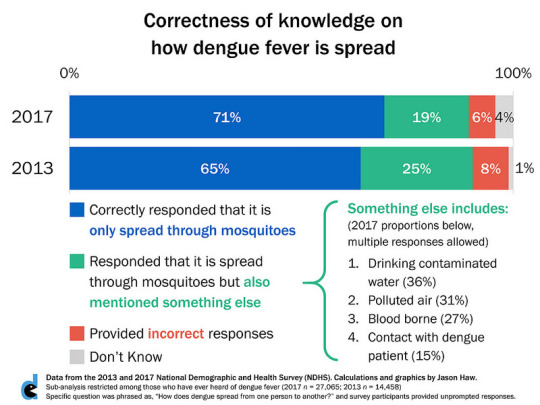
Across the sample of those who have ever head of dengue in 2017 (n = 27,065), 90% of respondents were correct in saying that the disease was spread only through mosquitoes. However, only 71% of the total sample provided the completely correct answer. This was a six percentage point increase from 2013, and the difference is significant (p < 0.0005).
The remaining one-fifths (19%) said that dengue was also spread through other means. Among those, 36% said that dengue could also be spread through contaminated water. Technically speaking, mosquitoes like to breed in man-made water containers. But water is not a reservoir of infection; humans are the only known reservoirs that allow mosquitoes to spread it to other humans. Transmission by polluted air was noted by 31% and human contact by 15%, both of which are completely false. Blood-borne transmission of dengue virus is very rare and is rarely considered as a public health concern (e.g. blood banks do not screen blood donations for dengue virus nor do public health campaigns on dengue mention this fact), but 27% mentioned that dengue may be spread through blood.
A second follow-up question was asked whether respondents knew that dengue can be prevented. In both years, almost all respondents agreed with this statement (2017: 97%, 2013: 98%). Then, they were asked on their top-of-mind responses on how dengue can be prevented. The results are classified according to the Department of Health’s (DOH) 4S strategy on dengue prevention. The 4S strategy includes search and destroy mosquito breeding places, self-protection measures, spraying during outbreaks, and seeking early consultation within two days of fever and rashes. The results are summarized as follows (2017 results are shown but 2013 results provided similar proportions):
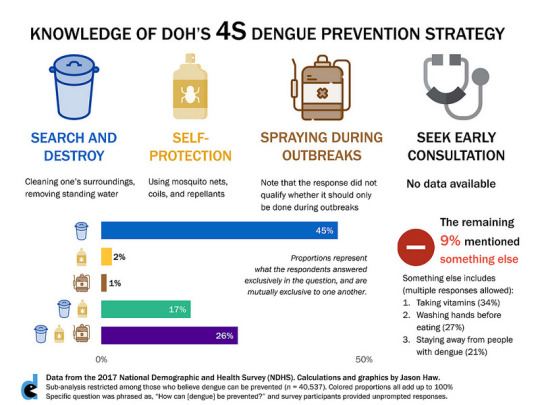
There are some limitations to the categories in this question, and future DHS rounds should fix this question and relate it to knowledge of 4S. For one, a category on spraying/fogging/fumigation was added, but there was no qualifying statement about it being only necessary during outbreaks. Spraying in any other context is not recommended, as the risks outweigh the benefits. Second, there was one self-protection measure that was not mentioned in the choices, i.e. wearing of long-sleeved shirts as a way to protect from mosquito bites. Finally, the were no data available on the fourth S, i.e. seeking early consultation.
Given these limitations, there are some key insights. Only a quarter (26%) were aware of all three S strategies, and did not mention anything else. Another 17% were aware of the first 2 S strategies (search and destroy and self-protection). Another 45% were aware of just the search and destroy strategy. Another 9% mentioned strategies that were outside of 4S and are not the recommended measures against dengue. Of these, a third (34%) said they take vitamins, a quarter (27%) said they wash hands before eating, and a fifth (21%) said that they avoid contact with people with dengue.
It is also interesting to map knowledge on transmission with knowledge on prevention and see if respondents have congruence in their responses. The results are shown below for 2017. Note that the row proportions can be added to produce the proportions on dengue transmission, and the column proportions can be added to produce the proportions on dengue prevention.
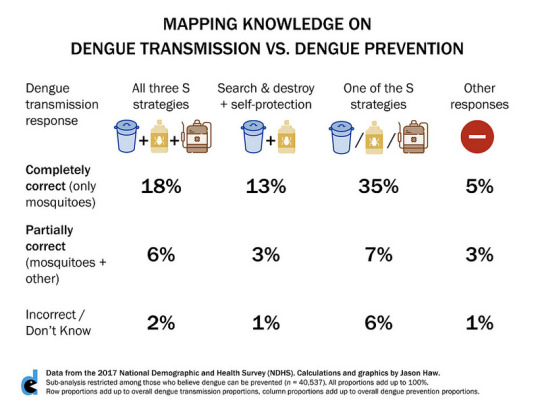
Less than a fifth (18%) were aware that dengue can only be transmitted through mosquitoes and the three S strategies. This can be considered as the subset that has the most complete basic knowledge of dengue based on this limited data. Around half (51%) knew the correct answer on dengue transmission and one or two of the three S strategies. Taking into account those who provided partially correct responses on dengue transmission, and knowledge of at least one S strategy, this totals to 82%. This means that around a fifth (18%) either do not know how dengue is transmitted or do not know how it can be prevented.
What is the key takeaway? Filipinos in general have some knowledge on basic facts about dengue, but the knowledge is not enough. More work needs to be done in educating Filipinos on these basic facts.
Note that this analysis does not yet stratify across geography, socio-demographic characteristics, and educational level. There are also limitations to the data that have been mentioned above. Nonetheless, these insights provide a national-level look at a disease that is common to the daily lives of Filipinos.
Some closing notes
The icons I used in the figures are from flaticons.com. I would like to credit the following artists - Mynamepong and Freepik - for allowing me to freely use their work.
All of my figures in this post and the rest of blog may be freely shared under Creative Commons 3.0 Attribution-Non Commercial-Share Alike.
0 notes
Text
2017 Philippine data on healthy behaviors, supplements, and local government health initiatives
I share three supplemental insights to the recently released 2017 Philippine Demographic and Health Survey.
The Demographic and Health Survey (DHS) is a treasure trove of health data utilized by almost 100 countries. The Philippines had its seventh round in 2017, and it is the largest health survey to date. Around 27,000 households participated, double from the last round in 2013. A full report and open-source access to the data sets are always provided as each round is concluded (access the 2017 files here, by making a free account, then sending a request to access the data; approval happens within 48 hours).
Because of this, researchers like me are able to conduct our own secondary analyses. As hundreds of variables are included in the DHS survey questionnaire, not all will make it to the full report.
This post (rather, three smaller posts) is the first in a series of supplemental analyses I am doing on the 2017 DHS. Note that most of these analyses are descriptive in nature, for reasons I will discuss below and in future posts. I use Stata 15 to clean and analyze the data, and all files are available upon request (Best to tweet me or send me a DM at @mockingjason).
What do Filipinos do to keep healthy?
The 2013 and 2017 DHS asked a question about what survey participants do to keep themselves healthy. They responded freely and their answers were recorded across multiple categories. The top 5 responses are shown below:
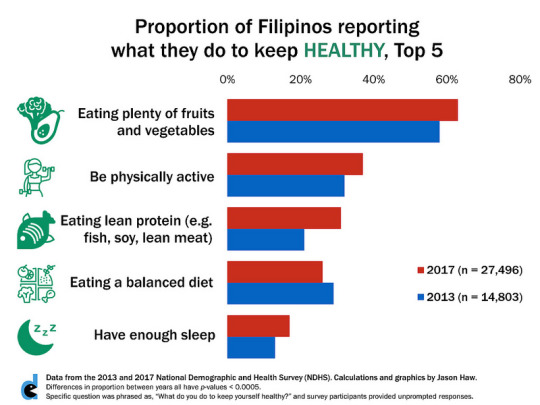
The results are hardly surprising. When unprompted, Filipinos say they keep healthy by eating right, being physically active and sleep enough hours. No significant differences were noted between males and females. Higher education and higher wealth were correlated with higher proportions of reported healthy behavior.
Two interesting things are of note. First, much fewer respondents mentioned what they avoid, such as smoking (8% in 2017). In contrast, the latest Global Adult Tobacco Survey (GATS) reports that only a quarter of Filipinos were current smokers in 2015. Assuming the data are directly comparable (at least on a national-level perspective), there were two-thirds of Filipinos who were not able to actively mention what they do about smoking.
Second, the way the categories were formulated are in no way a comprehensive assessment of a healthy lifestyle. The mere mention that certain food groups were consumed are not an indication of a healthy lifestyle - any nutritionist-dietitian will tell you that all food and drink must be taken in moderation. There were also vaguely defined responses such as “maintain happy personality” or “maintain good hygiene.”
I would caution against any further analysis of the responses. Measurement through self-reporting in a quantitative survey is one of the worst ways to collect data on health behaviors. First, people lie - who would want to admit that they are not doing at least one thing to keep themselves healthy? Second, restricting responses to certain categories, no matter how many, prevent the depth necessary to understand the complexity of health behavior. In many social and behavioral research studies, qualitative or mixed method (quantitative and qualitative) approaches are more appropriate.
Perhaps the data may be more appropriate in presenting perceptions of Filipinos on what a healthy lifestyle is, not necessarily what their actual behaviors are.
2. How much do Filipinos patronize supplements?
The Food and Drug Administration (FDA) ordered the replacement of the old “No Approved Therapeutic Claim” label for dietary supplements and other related products with the advisory, “Mahalagang Paalala: Ang (name of product) ay hindi gamot at hindi dapat gamiting panggamot sa anumang uri ng sakit” in 2014, after a long court battle with the Chamber of Herbal Industries of the Philippines.
The change was intended to better educate Filipinos when purchasing these products. The 2017 DHS had a series of questions related to this advisory, summarized in the following infographic:
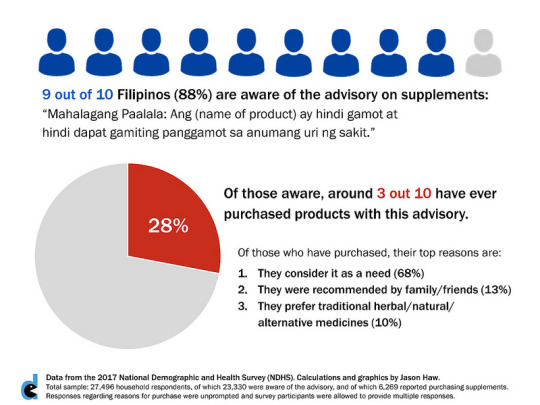
A good majority of Filipinos were aware of the advisory. Of these, around a third have purchased products with this advisory. Of these, around two-thirds claim that they have purchased these products as a need.
Recall of the advisory seems to be good, and FDA may be concerned with that majority of consumers who said that they considered supplements as a need. However, there were no other follow-up questions that provide more context. What is a “need,” exactly, in this sense? Is it a need in the same way that medicines are a need to treat certain diseases? Is it a need because it complements the benefits of medicines? The categories could have been phrased more clearly.
The definition of supplements may also differ across respondents. The Food and Drug Administration defines a “Food/Dietary Supplement” as “a processed food product intended to supplement the diet that bears or contains one or more of the following dietary ingredients: vitamin, mineral, herb, or other botanical, amino acid, and dietary substance to increase the total daily intake in amounts conforming to the latest Philippine recommended energy and nutrient intakes or internationally agreed minimum daily requirements. It usually is in the form of capsules, tablets, liquids, gels, powders or pills and not represented for use as a conventional food or as the sole item of a meal or diet or replacement of drugs and medicines.” (Note: I cannot find a public copy of the FDA Administrative Order 2010-008 but I have an internal copy available upon request).
Dietary supplements with outlandish claims, such as fruit-based products that claim to “cure” cancer, definitely deserve the FDA warning. But what about iron and folic acid supplements, which are actually essential public health interventions for pregnant women? Moreover, a quick search of available television commercials of these supplements on YouTube seem to imply that there are a number of companies violating the FDA regulation.
What is the point of the questions, exactly? If the intention was to determine the impact of the revised advisory on consumer choices regarding their health, then these questions do not provide enough insight. If the intention was to determine if recall of the advisory is good, then the question about awareness was good.
3. What do Filipinos appreciate from their local governments when it comes to providing health services?
Health service delivery is devolved to local governments, thus experiences may range from wealthy city governments being able to heavily subsidize health care through specific colored cards to rural municipalities struggling to retain basic health care staff. The 2017 DHS had a series of questions asking survey participants what health services they know are being initiated by their local government, and whether they have ever utilized any of those services. The responses regarding awareness were unprompted, then probing questions were asked to determine utilization. Top 5 services are shown below:
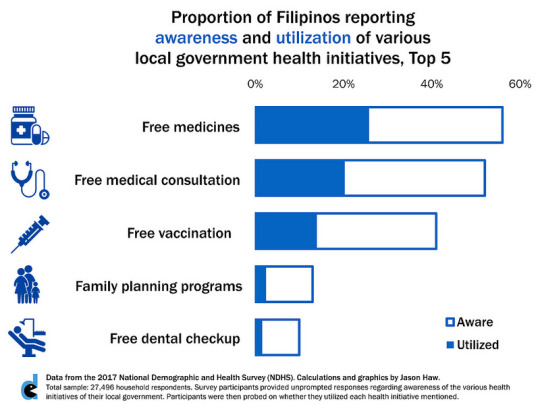
Only four-fifths (82%) of participants reported any health initiative by their local government. Only two programs were known by more than half of the participants - free medicines and free medical consultation. The results seem to show a gap in the actual service delivery, awareness about it, or both.
Also, many of the programs that the participants mentioned are more likely to have been provided by national government rather than local government. For one, most vaccines are procured by the Department of Health (DOH) and provided for free under the Mandatory Infants and Children Health Immunization Act of 2011. Medicines for prevalent diseases such as tuberculosis are also provided for free by DOH. Some of the public doctors providing free medical consultation may have had their salaries paid by DOH through the Doctors to the Barrios Program and not as retained staff of the local government. There are many complexities to the Philippine health system that the questions failed to capture.
Key Points
The three graphs I presented provide us with a limited understanding of the current state of health in the country. The key takeaways I want to highlight are:
Filipinos seem to be reporting some level of healthy behaviors, and they express it in terms of eating certain food groups, doing some physical activity, and getting what they perceive is enough sleep.
Most Filipinos are aware of the new advisory on supplements, and a significant proportion continue to patronize them and consider them as a need.
Local governments, in general, seem to be not doing enough in providing basic health services to Filipinos.
I also highlighted key limitations of the analysis, which I also hope are important takeaways:
Not all questions can be answered through a quantitative survey. While the huge sample size is helpful to have a clearer national view of the health situation, it doesn’t seem to do anything to mitigate accuracy issues.
Questions may need to be revisited for future rounds of the NDHS as they seem to be vague and muddle possible insights one can gather from the data.
I hope we always take a nuanced look at whatever pieces of data are being presented before us, especially with indicators that directly affect human lives.
Some closing notes
The icons I used in the figures are from flaticons.com. I would like to credit the following artists - Smashicons, Good Ware, Becris, dDara, Freepik, and mavadee - for allowing me to freely use their work.
All of my figures in this post and the rest of blog may be freely shared under Creative Commons 3.0 Attribution-Non Commercial-Share Alike.
#data hungry#DHS#health#health indicators#data#research#local government#supplements#healthy lifestyle
0 notes
Text
Demystifying the 35 B health budget cut for 2019
The amount is substantial, representing a decrease by a third from 2018 (when it received 106 B).
The cuts have received substantial criticism, even from the President’s own allies - most notably, the House Appropriations Committee Chairman and Davao City First District Representative Karlo Nograles. News articles about the cuts tell us little about where the cuts are and what it actually means for health service delivery. At best, the articles mention deep cuts to the Health Facility Enhancement Program (HFEP) and the health human resources deployment programs (such as the Doctors to the Barrios (DTTB) Program).
The cuts are contrary to the government’s populist agenda. This is the government that passed free tuition for all public universities, a comprehensive tax reform law that lowered personal income tax, and free irrigation to farmers owning less than 8 hectares of land. The House version of the Universal Health Coverage (UHC) Bill, the country’s most ambitious health reform legislation ever, passed with an overwhelming majority (222-7-0), and everyone is hopeful that the Senate would pass their version soon. Duterte also urged Congress to pass the UHC Bill immediately in his last State of the Nation Address.
How does one reconcile Duterte’s promises of universal health coverage and the budget cuts to the Department of Health (DOH)? The situation is definitely more nuanced than what is reported in the media, and publicly available information can readily explain these cuts.
We start by looking closely at the Department of Budget and Management’s (DBM) National Expenditure Program (NEP). The NEP is the annual budget document prepared by the executive branch and serves as the starting point for deliberations of the budget, officially known as the General Appropriations Act (GAA), in Congress. The full documents are available in the DBM website.
The DOH NEP is broken down into 8 programs, the names of which are not known to most people (the program classifications are not intuitive - what most people know are the subprogams to these general program categories). Without adjusting for inflation, we can summarize the percent changes of the appropriations per program from 2018 to 2019.
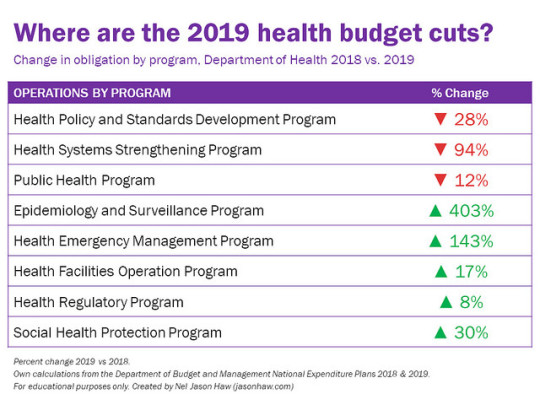
Five out of the eight programs actually received significant increases. Most notable increases are in three programs: the Epidemiology and Surveillance Program, Health Emergency Management Program, and the Social Health Protection Program.
The Epidemiology and Surveillance Program has a five-fold increase because of the 217 M special allocation for the surveillance of the 800,000-plus children who were vaccinated with Dengvaxia (see DBM’s official release here, page 26). This is the government’s guarantee that resources will be allocated to properly monitor the health outcomes of these children.
The Health Emergency Management Program is receiving an additional 500 M as a Quick Response Fund (QRF). QRFs are standby funds that can readily be used by government agencies whenever a disaster strikes, and the disbursement does not require approval by the National Disaster Risk Reduction and Management Council (NDRRMC). Five agencies are already receiving QRFs, and in 2019, the national government wants to add DOH to its list of recipients. After all, DOH needs to respond when natural and man-made disasters strike, particularly health-specific events like epidemics.
The Social Health Protection Program is a discretionary fund that DOH uses in providing direct financial assistance to indigent patients, on top of the support that the Philippine Health Insurance Corporation (PhilHealth) already guarantees as part of its No Balance Billing (NBB) scheme, and support from other agencies such as the Philippine Charity Sweepstakes Office (PCSO) and Department of Social Welfare and Development (DSWD). The fund will receive an additional 1 B from 2018.
The budget cuts mentioned in news articles pertain specifically to the Health Systems Strengthening Program. Under this program are both HFEP and the human health resources deployment programs.
HFEP is a DOH program aimed at building and rehabilitating health facilities both managed by the national government and local government units (LGUs) (Unlike public schools, management of health facilities are devolved to LGUs, save for around 70 public teaching hospitals). The fund received substantial increases upon the passage of the Sin Tax Law in 2012. While 80% of the 85% of the sin tax revenues earmarked for health are being used to subsidize the PhilHealth premiums of indigent families, the remainder is appended to the DOH budget. A simple time trend analysis of the budget obligations of HFEP shows how rapid the increases in allocation were:
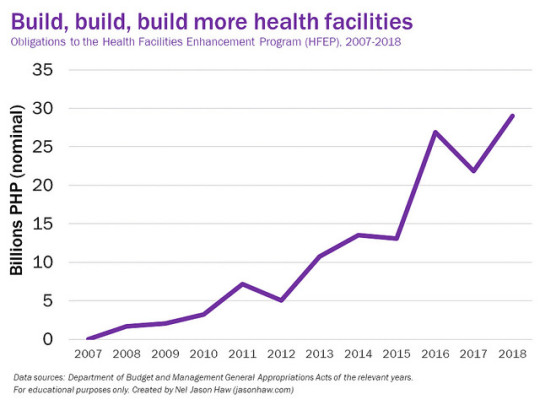
In 2019, HFEP is virtually eliminated - only 50 M as compared to the 30 B it received in 2018. There are two related reasons for this drastic cut. First, the spending performance of HFEP has been poor. DBM has been explicit about its criticism of HFEP (a detailed analysis can be found here). As a result, DOH’s budget utilization rate (BUR) has always been less than 90%, far lower than the 100% target set by DBM. Second, the government wants to shift from obligation-based budgeting to cash-based budgeting for 2019. This shift requires appropriations that are only “shovel-ready,” meaning that a government agency should be ready to disburse the funds in the same year that they are appropriated. In obligation-based budgeting, funds can be disbursed for up to two years after it was appropriated, resulting to delays in disbursement and chronic underspending of many government agencies. As a result, DBM wants DOH to fulfill all of its disbursements in previous appropriations and implement the corresponding projects, before it will propose to Congress for another set of appropriations. Assuming DOH does this and DBM keeps its word, this budget cut is only temporary.
The issue of health human resource deployment programs has something to do with the way the budget has been appropriated in previous years. A closer look at the 2018 vs. 2019 budget for this particular subprogram presents a curious case:
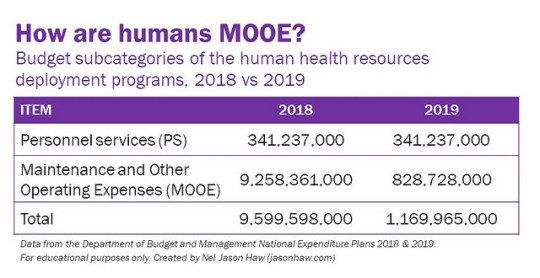
Personnel services (PS) remained the same between 2018 and 2019, and the cuts are isolated in the maintenance and other operating expenses (MOOE). Since this is a program that largely involves salaries to health professionals, why is the MOOE share much larger? This is because most allied health professionals like nurses are not counted as personnel. They are counted as contractual employees or job orders, or more commonly known as “endo.” Last May, the President signed Executive Order 51, effectively ending the practice of “endo” in all government agencies. This means that government agencies must either provide security of tenure to previously contractual staff or refuse to hire contractual employees again. The DOH took the latter approach, citing concerns about the civil service eligibility of most allied health professionals. This was mentioned explicitly by Health Secretary Francisco Duque III during the DOH budget interpellations at the House last September 3. DOH is now proposing a compromise solution, where these health professionals will still be considered contractual employees but will be provided government-mandated benefits so that their line item now becomes PS instead of MOOE.
As of posting this article, the 2019 GAA is still being deliberated. This means that the final budget cuts to DOH are still unknown, but understanding how the budget was proposed originally in the NEP gives us a perspective on how the government is trying to be more effective in its duties. While this budget cut can easily shock anyone at first glance, it is important for us to understand how much more nuanced the situation is, and that we can use publicly available sources to paint a clearer picture of the context behind this.
Links to sources and further reading are cited in-text. Leave me a message on my social media sites or here in my blog if you have any comments, questions or clarifications. Share with the rest of your network and start a discussion to keep our government in check.
3 notes
·
View notes
Photo

23 was incredible, having traveled more than 50,000 km, fulfilling a long list of firsts, and finishing my requirements for my masters degree. I am starting this new chapter leading the company I helped build, coming back to teach in Ateneo, and hoping for even more beautiful and exciting adventures. 📸 @kalaurque (at Estancia at Capitol Commons)
0 notes
Video
Happy New Year from Taipei 101!!! 🎇 If you wanna see the full vid I took of the fireworks display: https://youtu.be/cZtOC3bhalY (at 國立國父紀念館National Dr.Sun Yat-sen Memorial Hall)
0 notes
Photo

2017 has been the best year ever! From top left, downwards, in a counterclockwise spiral: Celebrated my 23rd birthday for 13 extra hours (and a whole NY adventure because of a delayed flight) - Went to a US presidential inauguration for the first time (which was boring because Trump) then went to the biggest march in US history, the Women's March (which was far more interesting) and also went to the March for Science three months later - Joined an advocacy effort for neglected tropical diseases at the US Capitol - Proudly attended the DC Pride March - Mesmerized by 2 broadway shows in NY (Miss Saigon and Wicked) - Went to Palawan for the first time! - Visited Ghana for the first time, where I pounded some fufu, relaunched my personal blog, went to tourist sites like Cape Coast and Wli Waterfalls - Co-authored my first peer-reviewed publication in a major journal - Attended the class of a public health superstar for the first time, Larry Gostin - Presented my masters thesis to the Ghana National Health Insurance Agency - Spent spring break in Puerto Rico - Prepared epidemiological evidence to a Senate Blue Ribbon Committee for the first time... and to cap off the year, coming back to my baby EpiMetrics as its Executive Director! I already have a ton of activities lined up for 2018! Super, super excited!!! ❤️
0 notes
Text
How ‘Jane the Virgin’ gets Bisexuality Right
Spoiler alert: If you have not been updated on Jane the Virgin, update yourself first then read this article.
Even with the assumption that mainstream media is becoming more and more “liberal,” LGBT representation in American media is still very poor. The latest Studio Responsibility Index from LGBT media monitoring organization GLAAD (Gay and Lesbian Alliance Against Defamation – but the acronym is now being used to stress the inclusion of bisexual and transgender people) gave “Poor” and “Failing” ratings on all major Hollywood studios.
Minority representation is important for many reasons. Sociologist Eric Anthony Grollman, in his personal blog, summarizes the reasons very neatly: it gives minorities a voice, makes them more visible, and validates their identity. When you see someone on TV or the movies that you identify with, doesn’t it get you excited? Doesn’t it make you feel like you’re not so alone after all?
This TIL post dissects the latest episode of the CW comedy Jane the Virgin. I’ve recommended this show in a previous blog post (which you can read here), but fundamentally the show is a meta-telenovela – it takes on every telenovela trope in its plot and makes fun of it. It also injects socio-political commentary on topics such as immigration, religion, and the family. My personal favorite episode is Season 3, Episode 3 (Chapter 47), when she finally loses her virginity, and the way that the show portrayed it is probably the best sex episode I have ever watched anywhere. There’s a great Vox article, and many others, that analyze this episode, so I won’t touch on it anymore.
But my second favorite episode would have to be this week’s episode – Season 4, Episode 5 (Chapter 69). The show’s producers probably wanted to talk about sex because of the chapter number but I did not expect that they would touch on something that still is invisible even within the LGBT community – bisexuality.
Some (spoiler) context: Adam is Jane’s newest love interest. While he’s a new character on the show (he was introduced in the Season 3 finale), he’s not a new character in Jane’s life. When they were teenagers, they planned on getting hitched, much to the disappointment of her mother Xo and grandmother Alba. The wedding never pushed through because they discouraged Adam, and Jane and Adam never saw each other again until Adam found a letter by Jane’s ex-husband Michael (May he rest in peace!). By this latest episode, they have been dating together for quite some time, Adam has warmed up to Jane’s son Mateo, and Adam has already turned down a major career offer, which would have demanded him to move, to be with Jane. So they’re really in love at this point.
But from a plot perspective, there’s this gap between Adam and Jane as foolish teenagers and Adam and Jane finding each other again. The show is starting to fill in the gaps, and this episode gave us the reveal that Adam is bisexual. His coming out process to Jane is beautifully portrayed, and I want to spend a lot of detail how Jane the Virgin gets the portrayal right.
I split the post into headers – which I will call the three stages of the bisexuality coming out process. The process works both ways – for the person coming out, which is Adam in this case, and for the person accepting the news, which is Jane in this case.
Stage 1:
Adam: Embarrassment
Jane: Reflex Acceptance

Jane (J): So you’re bisexual?
Adam (A): If you’re into labels.
Here, Jane clarifies Adam’s sexual orientation. Adam gives an answer that is both clear and vague at the same time. It is clear in the sense that he is not straight, but vague in the sense that he does not definitely confirm that his “official” sexual orientation is bisexual.
Jane’s question insists on a label. Some bisexual people may want to identify themselves as “bisexual,” but a lot also want to define bisexuality as a rejection of the notion that one has to play for only one team. I like to define bisexuality as one that transcends the need for gender to be a definitive criterion for choosing a romantic partner.
J: Do you date men and women?
A: I had a boyfriend in our school when everyone was experimenting, and another in Fort Green, when everyone wasn’t.
J: Cool. It’s just that we’ve had so many long talks. How come you’ve never mentioned this?
A: It just didn’t feel that relevant.
Narrator (N): I mean, more relevant than who’d win in an epic battle between Batman and Wolverine, which has been discussed at length.
Here, Jane demands an answer why she was not informed about this. Adam’s response is an insistence that he does not want to be defined by his sexual orientation alone. While it is understandable for Jane to be entitled to intimate details about her romantic partner, it is also Adam’s prerogative when he wants to reveal those to Jane. As a comic book graphic artist, Adam would rather have a lengthy discussion about a hypothetical battle between Batman and Wolverine than have a lengthy conversation about why he is bisexual.
A: And I guess I was… nervous. It’s become an issue with people whom I’ve dated before.
J: Well, you’ve never dated me before… Okay, you have… Not recently. My point is… is… I’m totally okay with it. You have exes, I have exes, everybody has exes!
And these two lines really define what Stage 1 is really about. Adam is really embarrassed to come out to Jane because he knows that to a lot of women (and even the gay guys he has dated before), this is a relationship deal breaker. Adam knows that Jane is entitled to know about his sexuality, and he has been probably planning when to tell her since that fateful night he delivered Michael’s letter. But he also needs to be comfortable in coming out – that his coming out should not also mean the end of their relationship. Because such a dichotomy is not fair, and a problem that most bisexual men encounter on a regular basis. Most bisexual men self-select the women they date because if they feel that a woman is not open to begin with, then the whole thing is really a non-starter.
Jane’s response is very interesting because it reflects every self-proclaimed liberal who grew up in a very Catholic (read: conservative) environment. A lot of Ateneans would love to identify as liberal (as the Jesuits are the most “liberal” Catholics!) but I have come to realize that their self-proclaimed liberalism has gone unchecked. I know this for a fact because I went through a series of stress tests when I was living in Washington DC for a year. And Adam’s coming out is that kind of test for Jane. In her head, she knows she should be okay with it, so her reflexive response was that. But as we move on to the next stages, we realize that she is totally not okay with it.
Stage 2:
Adam: Disappointment
Jane: Paranoia
(Lunch date)
Male waiter arrives with their orders
Waiter: Here you go… (Looks at Adam) Nice tats.
A: Oh, thanks.
Sexy, romantic music plays in Jane’s head as she thought the waiter was flirting with Adam and Adam is flirtatiously smiling back, then the waiter flirtatiously winks and leaves.
J: So, is that… your type?
A: What?
J: Just asking.
A: If I’m into the waiter?… I didn’t notice ‘cause I’m with you.
J: (whispering) Right. (nods) Sorry. I’m acting weird. I’m just trying to wrap my head around it because I’m not into women.
A: Maybe… or maybe you just haven’t explored that side of yourself?
…
A: Hey, look, is this something that’s gonna get in our way?
J: What? No.
A: ‘Cause you seem so pretty hung up on it
J: Honestly, I’m not
(Scene changes to Jane talking to her mom Xo)
A: I’m completely hung up on it! And I don’t wanna be.
Xo (X): Well, it makes sense that you are
A: Yeah because it took him so long to tell me and because there’s a double standard, you know. When women hook up, it’s looked at as sexy, but men are immediately marginalized because our whole culture revolves around the male gaze.
X: I’m not exactly following all that, but I hear you about the double standards (changes topic)
Jane was paranoid during their lunch date. She was paranoid even in a later scene, where she wondered if Adam hooked up with one of his friends, and Adam called her out on her paranoia, disappointed. The waiter was attractive, so he probably is someone’s type, but the possibility that it could be Adam’s type puts her on edge. Up until this point, she has not expressed jealousy in any of her relationships (case in point: she was never a jealous lover when the romantic plot of the show revolved around her love triangle with Rafael and Petra). This suggests that as a woman comfortable with her womanhood, she need not be jealous of other women coming near her lovers. But she is not comfortable with her personhood, that it could be the primary object of desire for Adam. She thinks of other men as competition she cannot compete with, because she cannot give what a man can. Adam loves her as a person, who just happens to be a woman. This is the fact that she needs to reconcile with herself as the show progresses.
Jane starts to realize that her reflexes were not reflective of what she truly felt about the situation. And Adam is very clearly disappointed about it. Adam knows that this is something that is going to take some time for Jane to process, but the subtext of his lines suggest that she should not have given him false hope that she was okay with it.
I appreciate Jane’s self-awareness in the scene with her mom. In the earlier episodes of the show, she was a graduate student in literature and her thesis adviser on her novel was a well-respected authority on gender studies. So she understands how the male gaze is applied to Adam’s context, and she also understands how her upbringing has prevented herself from straying away from the male gaze. She begins to struggle with her principles and how she applies it in real life. Xo not understanding how the male gaze applies to Adam’s context but applies to her own (she’s trying to convince her husband Rogelio to get a vasectomy) is a reflection of a bigger societal incompetence – not being able to wrap their heads around the concept of bisexuality.
Stage 3
Adam: Acceptance
Jane: (True) acceptance
(During Lina’s bachelorette party – Lina is Jane’s best friend who is about to get married.)
Lina (L): And you’re the longest relationship I’ve ever had (context: She just realized she was marrying the male version of her best friend Jane)
J: And you’re the longest relationship I’ve ever had
L: I love you Jane
J: I love you too
(sexy music comes on, Jane tries to kiss Lina)
L: What the hell, were you gonna kiss me?
J: What? No, don’t be ridiculous! I mean… Yeah I was…
(cut to commercial)
J: I’m sorry, I don’t know what I was thinking
Narrator: Seemed like you were thinking of making out with your best friend
(Lina chuckles)
J: I guess I’m still a little freaked out by Adam big bisexuality reveal.
L: Well, a pretty smart friend once told me, “You fall far who you fall for”
J: Yeah, but this is different. I’m not freaked out by his sexuality. I’m freaked out that he kept it from me.
L: (rolls eyes) Hmm…
J: What?
L: As your best friend in the world, and the person you just tried to make out with, that’s a bunch of crap.
J: Excuse me?
L: Don’t try to make this about him hiding. Figure out what is really going on.
J: (exhales deeply) Well, I guess it’s because…
L: Lady, tell him, not me… because it’s my freaking bachelorette party…
This is my second favorite scene of the episode. First, Adam’s suggestion that Jane explore her “bi” side really got to her and so she tried to experiment with her best friend. Second, Lina called her out on her bullshit (which is what best friends are really supposed to do) that her issue was about the timing of the reveal, when in fact it is really about Adam being bi. This show has always been reflexive, and I’m glad that they have remained consistent with the self-awareness plot device.
(later that night, back in Adam’s apartment)
J: Can we talk?
…
J: So yeah, it wasn’t that you waited a long time to tell me, it was what you told me. Which became pretty clear after I tried to kiss Lina
A: What?
J: I know. That was a momentary lapse of judgment. But you’re obviously right. I did freak out. I guess, I… I just have questions, which are silly and stupid.
A: Go on, ask me.
J: Is being bisexual a stop on your way to coming out as gay?
A: Definitely not. It just means I am open to a connection with a man or a woman. What else you got?

J: Well I guess I feel a little insecure, you know. It’s not like I can give you what a man can.
A: Yeah, you’re right. You can’t. But you can’t give me what another woman can give me either. But it doesn’t matter, because I choose to be with you. I don’t want to be with anyone else, regardless of gender.

A: Yeah, really. We’re in a monogamous relationship, which means that you’re not allowed to kiss anyone else.
J: (smiling) I know, I’m sorry. I’m sorry. If it makes you feel any better, she hardcore rejected me.
A: (smiling) Well then, she’s an idiot…
(Kiss scene)
A: (joking) Oh, Bob. (Jane gasps, laughing). I’m kidding, kidding, it’s Jim, right?
Now, this is my favorite scene, and the first time I watched it, I was in tears because Adam said the perfect words to Jane. Jane’s admission of her biases is a relief to Adam, because he knows that she is now along the road of true acceptance. Her embarrassment in asking questions is also another societal representation – our friends would love to accept us, but they are not educated about it. But they are afraid to ask.
And if there is one thing that you would pick up with this 2000 word blog post, it is this:
The best way to make your LGBT friends know that you accept them for who they are is when you ask thoughtful questions.
Don’t be afraid to ask, as long as you are not coming from a position of condemning your friend. Of course you are ignorant – you’re straight and you do not have the capacity to understand what non-straight people experience on a daily basis. It’s the whole idea about being with the “other” – we can never know what others are truly experiencing, but we can journey with them.
The two questions Jane asked are probably the top two questions everyone asks about bisexual people, and I promise you 100% of your bisexual friends are going to answer the exact same way that Adam did when you ask those questions to them. These questions are not intrusive – in fact, it’s an admission of your biases that allow your bi friends to accept you also as part of their journey. It means that you are open to being informed, changing your opinion, or even join them in fighting for their rights. It wasn’t just Jane accepting Adam for who he is, it is also Adam accepting Jane as a woman capable of understanding what he is going through. Let’s go back to what Adam said – he knows that his sexual orientation has been a deal breaker before, so naturally he will be skeptical when he has to come out to a new person. But Jane’s openness has allowed him to be accepting as well. He’s changing hearts one person at a time.
If you haven’t watched Jane the Virgin, then please do. And if you want talk more about bisexuality, leave me a DM at @mockingjason on Twitter. Let’s have a thoughtful and informed conversation.
0 notes
Text
Life in Ghana 10.3: Post-Presentation Processing
I’m still reeling in from the high of yesterday’s presentation.
I am fortunate to have four years of research experience to ground me on how to prepare for the presentation. I have attended high level meetings before, but I was always there as a quiet observer or diligent rapporteur, never someone who really needed to present anything. Yesterday, the spotlight was on me. I was the lead (and only) investigator of my research. Whatever I say during the presentation is a reflection of my professional competency and personal opinions on the health financing situation in Ghana. I carried the name of Georgetown and Dodowa Health Research Center, and there was that pressure to present myself well because I am not acting only on my own capacity. I was a pageant baby, and I have acted, sung, spoken in front of live audiences as far as I can remember so stagefright was never an issue with me. But for the first time in a long time, I had the jitters.
The first challenge that I had to overcome was making my presentation easy to digest and relevant to my main audience, the senior NHIA officials. The statistical analysis involved in my research is highly technical - and I am grateful for the help of Professor Bouey in linking me to statisticians that validated my outputs. I have read five statistical books (one on analysis for complex survey data, one on econometrics, and three on mixture modeling) in a span of two months (I'm sorry to my fiction reading list as they had to take a back seat). I have written thousands of lines of Stata code, redid my analysis far too many times because I am a perfectionist that never settles, and convened debates with myself on how the data should be interpreted. All of that was extremely worth it, but the bigger issue was whether the results were interpretable to a wider audience. For example, I had a significant interaction term in my regression analysis - ownership of facility (private vs. public) affected the propensity of patients to use their insurance card - and so I struggled to present the results of the regression analysis. The first time I presented was to staff of Dodowa Health Research Center, and the main criticism to my presentation was that it was too technical. And to think that I already tried to simplify the explanations to my analysis! That was my best effort at that point in time, but seeing that my best effort was apparently not good enough, the perfectionist in me spent more days trying to find a way to ease interpretation. I finally did, because everyone understood what the main result of my analysis was.
The second challenge was coming up with recommendations based from the results of my analysis. I knew from the beginning that the main value of my study was the fact that there is this survey that can be used to feed into policy. For my thesis, I saw my role largely as a bridge between the Demographic and Health Survey (DHS) dataset and feeding it to policymakers - I cleaned the dataset, conducted the analysis, reviewed literature, processed the results, and yesterday I presented it to them so that they can pick up the gist and make policy from there. I was very cautious with how I phrased my recommendations. I needed a delicate balance between two conflicting perspectives: from the perspective of the clients, the NHIA seems to not be doing anything towards patient improvement and improving quality of care, but I also want to validate all the hard work NHIA has been trying to do in being more responsive to clients. Having worked in government made me more understanding of how difficult it is to change things from the inside. It has given me this patience and humility that while in public, we can harp about how easy it is to change something, but in reality, nothing is ever as simple as it seems. I decided that I will take a position with my recommendations - that I want to be explicit that the NHIA should work harder to be more responsive to clients - but I also want to incite discussion and reflection from the NHIA staff during the open forum on what they have done and what they could still do. And I was so relieved when that happened.
I will brag about this because I am so giddy that this happened - the officials were applauding after my presentation because in the words of one of the directors, "It was very well-presented." (#nailedit!) During the open forum, all of the officials were keen on discussing the issue of patient empowerment and health system responsiveness. They dwelled mostly on my recommendations but I was glad that they did because they were able to reflect on their performance as an agency. For example, one senior official asked me about what else they could do to empower patients. The NHIA has a call center, and there have been numerous pilot studies on community engagement and ensuring patient safety, but none seemed to stick. I gave my two cents on the matter - that it was important for health systems to have an independent patient watchdog embedded in the public sector but is completely independent from the Ministry of Health or the NHIA, and has enough power to demand accountability from health providers. Having a call center embedded in the agency that the patient is complaining about does not give patients the assurance that their feedback will not be used against them. It's not a function of how the call center operates, but a function of where it is operating and what impression it gives to clients. That comment was well-received, and the officials agree that it is the case. They also mentioned to me that the latest revision of the National Health Insurance Scheme Act has a legal provision to set up a consumer protection group, but this has not yet been operationalized. In response, I promised that I would fine tune my recommendation to stress the fact that this already has legal basis and that political will and action is what is needed to make that happen. It was that kind of fruitful exchange during the open forum that really showed to me that meaningful, constructive conversations on one's weaknesses is still possible in today's hostile political climate.
The final challenge was trying to find a way to make my report stay longer in their minds than the presentation. During the open forum, the officials gave specific requests on the final report that they would like to see, which they pledged they would use to help shape policy. I've mentioned the recommendation regarding patient empowerment, but let me share another. One limitation of the DHS dataset was that while ownership of the facility was asked, the level of facility (hospital, clinic, health center) was not asked. It was a comment first brought up by Director Williams even before I started my analysis, and this was thhe same comment that the officials noted because they wanted to identify which specific facilities were having issues with the card. I was able to demonstrate in my analysis that the use of the card is not negatively perceived in public facilities, but it is in private facilities. They wanted to know if such a difference in perceptions was also present across different levels of the health system. I said that the NHIA should request to have this question added when the next survey round is done in 2018/2019. This additional question would not be a troublesome request and the wealth of insight that can be extracted later on would significantly improve the utility of the analysis. I promised to also make that recommendation clear. I also got confirmation that they want to read the final report, and so I will send it to them as soon as possible. I was not able to mention this during the presentation, but I also want to write a policy brief that can be peddled around the NHIA and to other stakeholders.
I am excited to spend the next few weeks wrapping up my literature review, writing up my results, analysis, insights, and recommendations. This whole experience has been monumentally helpful for me as a researcher on so many fronts - technical skills, communication skills, building social capital, and actively advocating the reduction of research waste and the value of research translation. Again, I could not have asked for a better conclusion than this. I have dozens of people to thank for getting me this far, but I'll save the farewells for my final post next week.

1 note
·
View note
Text
Life in Ghana 10.2 Pre-Presentation Jitters
Tomorrow at 10 AM, I will be presenting the results of my paper to the people that need to hear it the most - the National Health Insurance Agency (think PhilHealth for the Filipinos out there).
I was informed a few minutes ago that only five people will be attending the meeting - the Deputy CEO of Operations and four senior staff (which I assume are the Directors?) from Claims, Quality Assurance, Provider Payments and Research & Policy Directorates.
When I wrote the letter to the NHIA two weeks ago, I did not expect to have such a high-level audience listening to the results of my paper. I knew that I wanted to communicate the results of my paper to policy makers who have the authority to enact reforms, but I did not expect that the bosses themselves would come and listen. Honestly, I have never presented to such a high-level audience when we would do projects for PhilHealth. Those kinds of presentations are reserved for senior investigators, like my mentor Doc Wong.
I am grateful, as it is a wonderful conclusion to my stay here in Ghana. I came up with my topic because I did not want research waste - here was a perfectly good dataset from the gold standard of global health surveys - the Demographic and Health Survey - that was not fully maximized. As I have mentioned, I got confirmation from one of the Directors at NHIA that they requested the DHS team to include a ton of questions about utilization of the National Health Insurance Scheme card, including questions on how patients perceived their last health visit. But no one has ever analyzed and reported the results of this dataset, until now.
I guess it makes sense for the big bosses at NHIA to be interested in the results - this is something that they have wanted since the beginning. I hope my presentation is going to be worth their while. I mean, how many masters students ever get this kind of opportunity to change policy making at the national level with their thesis?
And with that, I channel my inner Titus and pray

2 notes
·
View notes
Text
Life in Ghana 10.1 (10/7- 16): Routine
I’m starting to enjoy the fact that I have a routine here in Ghana, but unfortunately I am leaving next Monday.
I was not able to post anything for the pat 10 days because I realized how I have already mentioned a lot of my day-to-day activities in previous blog posts. So for the next five days, I will post shorter blogs of some final thoughts that I have regarding my entire masters experience.
Securing a routine has been difficult since I left for the States over a year ago. It is always exciting to have something new happen all the time - honestly I could write a 300 page biography from all the things that have happened just in the past year, but sometimes it can get overwhelming. After I leave next week, I just want to sit down for a full month and collect my thoughts on everything that has happened. I have learned a lot of new things about myself, and I want to write them down and remind myself of all of these lessons.
Just some out-of-routine things that have happened in the last week:
1. I visited one more researcher for my paper and he called up one of his Filipino friends, a development consultant who migrated to Ghana in 1993 because she married a Ghanaian whom she met during her masters program in Germany. It was nice to talk to someone from back home and we shared our thoughts on political matters as well, given the situation back home.
2. I met up with Briana and Osato one last time before we meet again for graduation. Last week was Briana’s birthday and we decided to celebrate in Accra.
3. I really need to decide on what Ghanaian wear I want to buy as a keepsake. I haven’t really committed to a design but I think I should buy one before I go home. Also, I will have to hoard on Ghanaian chocolates because I am obsessed with them.
4. I am presenting to the National Health Insurance Agency (NHIA) on Wednesday. I really love my paper and I’m glad that the results are going to be communicated to the people who have needed it the most.
As a bonus for today’s post, here’s a playlist of Ghanaian and Nigerian radio hits in Ghana right now: https://open.spotify.com/user/neljasonhaw/playlist/4wPmL174Y6uPcsIRWwebEL My personal favorite is KiDi’s hit “Odo” (meaning “love” in Twi). It was released about a few days before I arrived in Ghana and I hear this song almost every day on the radio. After all, it is really catchy.
0 notes
Link
It’s a common cultural practice in many West African countries to name your children after the day they were born and/or the order by which they were born. Find out yours through this link.
0 notes
Text
Life in Ghana 9 (9/29 - 10/5): Care and Daycare
I can't believe that I only have a little over two weeks left here.
Some housekeeping: I am almost done with my paper and I hope I can finish a complete first draft by the end of next week. I plan to submit those drafts to the professors I talked to a few weeks back, given that they were willing to review it. I am also waiting for the National Health Insurance Agency to reply back to me if it is possible to still present to them before I leave. Yesterday, I also picked up my passport over at Immigration and my visa has successfully been extended. Still impressed how government transactions here are so much easier than in the Philippines.
This week, we met a ton of new foreigners, all from the New York University (NYU) campus in Accra. We met two of the undergrads through Lovelyn, whom you might recall is from my host family, and then we met more of the undergrads in Accra on Wednesday. We ate at this fancy restaurant called Bosphorus, which mainly serves Mediterranean, and had ice cream at Moka's Resto and Cafe. The NYU campus and dorms are in the Cantonments area, which is a really, really high end area of Accra (think Rockwell or The Fort in Manila). On Tuesday, a group of graduate students, mostly from the Global Public Health and Epidemiology programs from NYU, came over to the research center where Director Williams gave a presentation introducing the research center.
I love the way we are being taken care here. We have our own house, we each have our own rooms, and we have a fridge, an oven, a microwave, and a TV. Everyone in the research center always goes out of their way to greet us a good morning, and everyone checks on us if we are doing well today. For the most part, we are left on our own to do whatever we want, and sometimes we check in with Director on updates on our research. But we are not pampered here, unlike the students from NYU, where they have a nice car service taking them around, luxury dorms that are heavily guarded, and having the most cosmopolitan experience Accra has to offer. Dodowa is a rural to periurban town where life still feels really simple. We experience blackouts almost everyday and sometimes we run out of water if we forget to inform the research center that the polytank behind the house needs refilling. The internet gets spotty at times like last week, where it was almost unbearable, but we manage pretty well since the three of us get along well. We have been watching new TV shows together, such as This is Us and The Handmaid's Tale. We take the tro-tro around town, and everyone in town probably knows us by face at this point. It's the perfect balance of us having a comfortable time, but not comfortable enough to the point that it makes us uncomfortable that we are given too much special treatment. It's uncomfortable enough for people to stare at us constantly because the color of our skin and our hair styles are different.
Almost everyday, the kids from the neighborhood come visit us at our house and play with us. Our house is now the de facto post-school daycare center for children aged 2 to 13. Last week, we ended up watching Despicable Me 2 four times (no more Minions, please!) so I downloaded Despicable Me 3 so that the next time the kids arrive we have something new to watch. For the most part, Natalie and Allie are really the ones spending much more time with them than me (I have surprisingly been busy over the past three weeks). Now, the kids have been coloring since Allie has an 80-pc colored pencil set, but for the past few weeks the kids have been playing card games like Five Crowns and Exploding Kittens, and the usual card games like Go Fish, BS, etc.
This afternoon, we are leaving for Cape Coast, the old capital of Ghana for a weekend beach getaway, and also visit the castles and other cultural sites. I hope to post more photos next week, as last Saturday we went to Labadi Beach in Accra but I really just wanted to chill with the sound of the ocean as background noise while reading Hillary Clinton's new book "What Happened" (it's a must read, by the way!)
0 notes
Text
Life in Ghana 8 (9/23 - 28): The Forest and the City
This week, I want to share two stories: Our experience at the Shai Hills Forest last week and my visit to the Head Office of the National Health Insurance Agency over at Accra.
1. Shai Hills Nature Reserve Yes, we decided to do the quintessential forest experience since we are in Africa (cue air quote gesture). But anyway, Shai Hills, which was about three tro-tro rides away from our place, had a Nature Reserve maintained by the government. We paid 40 cedis (around 10 USD) for the student rate (regular rate was 60 cedis, so bring your Georgetown IDs with you when going abroad - it will score you some great discounts!) and hired a taxi for 60 cedis to drive us around the reserve, since we arrived late in the afternoon and we would run out of time to see all the sites if we walked.
The Nature Reserve had a lot of animals, most of which were imported from South Africa or Kenya. Tourists (well we were probably the only tourists in the entire reserve during that time) are only allowed in certain trails while all the animals roam free to do whatever they want).
Here are zebras!
We also went to a bat cave....
which led us to a rock climbing path up (it was mildly scary but safe) and the view up top was just spectacular...
No filter.
2. On Tuesday, I met with one of the directors at the National Health Insurance Agency (NHIA). I brought Natalie and Allie with me also as this is a unique opportunity for all of us to know more about the health financing system of Ghana from the perspective of someone so high up government.
We had a very interesting (and mostly off-the-record) conversation about the problems of Ghana's social health insurance scheme. What I am at liberty to say is that their issues are a lot similar to ours so the director and I were able to bond over those issues. What was probably the highlight of that meeting was the fact that my paper is actually very relevant to policy - he confirmed that the NHIA asked for quality of care perceptions to be included in the survey, but no analysis was done to it because the NHIA did not want to shell out additional funding for the analysis, even though they really wanted to use that data for policy. So I guess in a way they got a free analysis from me. I am just glad that I am doing something substantial. Over the remaining weeks, my goal is to wrap up my analysis and set up a meeting with concerned officials at the NHIA to communicate the results of my study.
0 notes
Text
4 Articles Befitting Angela Merkel’s 4th Election Win
Angela Merkel is an impressive woman, and definitely one of my political idols. I can talk about how awesome she is for hours and hours, but I think these four articles articulate why I think she is awesome, to celebrate her fourth historic election win last night as Germany’s Chancellor (the official voting in the Bundestag comes after she gets to form a working coalition, which may prove difficult due to the plurality of parties across the political spectrum).

1. Angela Merkel, the G-Zero Chancellor (The Economist, July 7, 2017): It’s true - she is not the new leader of the free world. Personally, she has balked in numerous occasions at the press for calling her as such. But she is a model with which the future leader should look like.
2. Gay marriage and the six rules behind Angela Merkel’s political longevity (The Economist, Jun 27, 2017): Angela Merkel, being raised in conservative Lutheran family, is personally opposed against same-sex marriage. Her party, Christian Democratic Union (CDU), is known to be an economically liberal but socially conservative center-right party. With most of the opposition and her coalition partner Social Democratic Party (center-left, socially liberal) attacking her for not passing same-sex marriage legislation in Germany, it briefly became a key election issue. For her political survival, she finds a compromise: the law became a conscience vote for the CDU, meaning that CDU members are free to choose outside of their party manifesto. She personally voted against it, but her last minute political decision led to a successful snap parliamentary vote, 393-226.
3. The World’s Most Powerful Woman Won’t Call Herself a Feminist (The New York Times, September 16, 2017): This is an interesting analysis piece from a political analyst who has tracked Merkel’s career in years. She argues that Merkel’s success as a female politician lies in the fact that she does not assert her womanhood in what is still a very patriarchal society in Germany. Bonus read: In Angela Merkel, German Women Find Symbol, but Not Savior (The New York Times, September 13, 2017)
4. The Quiet German: The Astonishing Rise of Angela Merkel, the Most Powerful Woman in the World (The New Yorker, December 1, 2014): I love this long read, as it summarizes Merkel’s life story and also has quotes from people who have closely worked with her. If her life story does not impress you even in the slightest bit, then I am at a loss of words.
You may love her or hate her, but everyone has to admit she is impressive in some way. A former campaign manager once called her the “Ikea politician” because she offers at least one thing to all kinds of voters (Bonus read from The Guardian). She is not perfect, definitely, but her style of political leadership is one that I admire, and one that is seemingly getting lost in political circles - the power of centrism. The far left and the far right might harp and harp about wanting to do this and that, but I firmly believe that a healthy dose of centrism is key to make effective change in our society.
1 note
·
View note
Text
Life in Ghana 7 (9/13 - 22): The Unwavering Kindness of Ghanaians
It has been seven weeks since I have arrived here and I have probably talked to dozens of Ghanaians by this point. Every single one of them has been extremely kind and generous and hospitable. I borrow some words in Filipino: Wala akong masabi (I have nothing [ill] to say). This week I share about 5 little acts of kindness over the past week.
1. Tuesday (Sep 12): We visited the District Health Office of the neighboring Ningo-Prampram district (Dodowa is in Shai-Osudoku, and both Ningo-Prampram and Shai-Osudoku used to be part of the same district, Dangme West). We were welcomed by Dr. Gifty Ofori-Ansah, who welcomed us with kind words and a comprehensive presentation on the health status of the district. From the moment I talked to her, I can tell that she is a very smart, decisive, and open-minded woman, and she was kind enough to offer her input to the research topics of Natalie and Allie, who are still in the process of writing their proposal. We also met some of the supervisors managing the different health programs like family planning and infectious disease control.
What I admired about her was her humility and dedication as a public servant when she was talking about the issues that plagued her district - teenage pregnancy, quack doctors (and its relationship with religious faith), and the rising burden of non-communicable diseases. She reminded me of the hardworking municipal health officers that I have met so far in the Philippines. It is people like her that continue to give me hope about public health - that most of us have good, wonderful hearts always ready to help those in need.
2. Monday (Sep 18): I presented my initial results to the staff of the research center and the room was packed. Days leading up to the presentation, I felt a bit uncomfortable because I did not want to feel like a foreigner telling them what their health system is like given that these are researchers who have spent their careers understanding their own health system. After I presented, my colleagues gave wonderful and helpful remarks on how to improve my paper. One thing I appreciate about Ghanaians is that they always have a sense of humor even in the driest of things, such as presenting something as technical as statistical analysis. After that presentation, I am more confident in finishing my presentation.
3. Tuesday (Sep 19): I had two tasks that day: go to immigration and extend my visa stay, and visit a professor over at the University of Ghana who has written extensively on the topic of quality of care perceptions, which you may recall is also my topic for my scholarly paper. The Ghana Immigration Service is the first government office I have transacted since arriving here, and while the office is a bit chaotic, it is miles and miles better from the Bureau of Immigration back home. First of all, there are no fixers! Fixers, as officially defined by law in the Philippines, are "any individual whether or not officially involved in the operation of a government office or agency who has access to people working therein, and whether or not in collusion with them, facilitates speedy completion of transactions for pecuniary gain or any other advantage or consideration." We have a law that explicitly bans fixers in government offices (Republic Act 9485) but of course, just like most laws in the Philippines, no one implements them. Second, the immigration officers have been extremely helpful, unlike the ones in the Philippines where a lot of them are snarky and powertrip foreigners.
After that trip to immigration, I visited a professor at the University of Ghana Business School and an expert on quality of care perceptions in hospitals. We had a very fun and fruitful discussion on his papers, and I also consulted with him on my method. He was very honored that someone read his 400 page dissertation on the topic, and I told him that I love doing research so 400 pages is a breezy read to me. At the end of the meeting, he agreed to review my paper and comment on it. I am so honored to have someone so knowledgeable on the topic review my work.
4. Wednesday (Sep 20): I left early again to visit another professor who is currently based in the University of Health and Allied Sciences at Ho, the capital of Volta Region, which is east of Greater Accra Region. The ride took almost three hours getting there - mostly because Ghanaian roads are not paved (which makes me carsick most of the time). The trip was definitely, definitely worth it. I cannot stress how engaging and fruitful our discussion was. He has written a lot of papers on the topic of health care quality, as he also did his dissertation on it. What particularly interested me was how he ended up doing his PhD program, which I hope I will have the opportunity to have in the future when I finally study for my PhD. In short, he was my #PhDGoals. In summary (and if I understood it correctly): The National Health Insurance Agency (= PhilHealth in the Philippines) asked help from the Dutch government to solve their issue of low population coverage/ enrollment into the scheme. The Dutch government gave them a grant, and allowed three PhD students (one from Ghana Health Service, one from the Netherlands, and one from the school where Prof Kaba was affiliated at that time), and one postdoc (who is now head of research at the insurance agency) to be principal investigators in distinct but interrated parts of the project grant. Prof Kaba was primarily responsible for doing the quantitative work in assessing the impact of the project, which was a community trial that used community engagement as a tool to improve insurance enrollment. Since then, he has written 9 published papers on the topic (in very reputable journals like PLoS One)!
What particularly impressed me with his PhD journey was that: (1) he was involved with the insurance agency the entire time - and some of his recommendations have been turned to policy, such as the issuance of the cards on the same day, and the shift to biometric insurance cards, and (2) the PhD students leading the studies had a lot of freedom with their paper, with national implications. I have never seen anything as seamless and empowering as his PhD program, and all I could think about during that meeting was how we should emulate this in the Philippines. Like this was my lightbulb moment for my PhD program - I want my PhD program to be structured like this. I will not settle for anything less.
But going back this professor, he was so, so kind. First of all, he saw my undergraduate thesis online (which is published in a Scopus-indexed journal) and was very interested with the findings we had on family planning in urban poor communities in the Philippines. I was so flattered someone actually read our paper. Second, he wanted me to invite for lunch but I had to decline as I had matters to attend back at the research center before office closes (remember the journey back is 3 hours!). Finally, he was just a guy who had a lot of good vibes, showed love for his country, and is very intelligent. I am so grateful to have met someone as inspiring as him.
5. Thursday (Sep 22): I will post more about this in my next post next week, but we went to a nature reserve in nearby Shai Hills. But going back to the overall theme of kindness of Ghanaians, I just want to remark how everyone has been so kind to us whenever we ride the tro-tro. As lost foreigners (oburonis), we would not have known where to go, but someone - either the mate (conductor) or a kind passenger - always tells us where to alight and what to ride. Even the taxi driver that took us home from the reserve did not scam us (or at least based from our computations as we spent around 30 cedis in tro-tros coming there, and the taxi home was just 50 cedis).
Honestly, this country is just oozing with kindness, and I am starting to regret that I only have four weeks remaining here. I honestly want to extend but matters at home are more pressing at the end of the year. Ghana's tourism slogan should be, "Visit Ghana for good vibes."
1 note
·
View note