#bmj case reports impact factor
Text
Top 21 Open Access Medical Journals That Technology Watch Experts Should Leverage
Introduction : Keeping up with the ever-evolving technology landscape in the medical field can be a challenge. If you’re a technology watch expert, you need to be able to quickly identify emerging trends and make sound decisions based on them. But how can you do that ? This a [...] https://is.gd/f0qghy

#business #communication #data #education #ict #information #intelligence #technology - Created by David Donisa from Academypedia.info
#are open access journals bad#best open access medical journals#bmj case reports#bmj case reports impact factor#bmj impact factor#bmj open author guidelines#bmj open impact factor#bmj open quality#bmj open submission#bmj open submit#bmj quality and safety impact factor#bronze open access#delayed open access journal#diamond open access#directory of open access books#doab#doaj directory of open access journal#examples of threats in a swot analysis#free open access medical journals#gold open access#green open access#h-index vs impact factor#hybrid open access#is scientific reports a good journal#is the british medical journal reliable#journal ranking#list of open access medical journals#open access database#open access disadvantages#open access examples
0 notes
Text
Many couples opt for delayed childbearing due to financial, emotional and work-life balance. Security for self & children is very important and that is why the use of birth control measures. However, the gravity of the impact of such decisions on childbearing must be fully understood by the couples before they proceed. Let us understand the impact of birth control from 2 aspects:
a. Effect of the delay on your childbearing ability
b. Effect of the birth control hormones on your fertility
a. Delayed childbearing definitely will affect your chances of success if the female partner is nearing 35 years of age. That is because nature has designed the human anatomy in such a way that the woman’s egg quality and quantity both get depleted rapidly after 35. This means there is a conspicuous drop in her fertility after the age of 35.
In many cases, this happens much earlier due to conditions like ‘Premature Ovarian Failure’ and there is no way to know this unless you carry out specific tests. So if you are planning to delay your baby, consult your gynaecologist about your current fertility status. If it is already waning, IVF technology can help you create and store your embryos indefinitely & safely, until you are ready to start a family. Mind you, as the woman ages above 35, other factors come into the picture like overall health and the increased risk to the woman during pregnancy and delivery.
Many women also develop ailments like fibroids as they age, which may interfere with their fertility.
b. Effect of the birth control hormones on your fertility
There are different methods of Hormonal contraception, which may be pills, patches, rings, injectables, implants or hormonal intrauterine devices (IUDs). Loss of fertility is a concern in every couple’s mind, which we will address here and help you to take informed calls.
What we do know clearly by now is, hormonal birth control works by several mechanisms, including shutting down brain-ovarian communication which can stop the process of ovulation, alteration in the cervical mucus, and thinning of the endometrial (uterine) lining.
The above statement is true in every situation when women of any age have used different methods of contraception.
When the primary health goals of birth control pills are to reduce the rate of unintended pregnancies and abortions, more efficient birth control measures are being developed which are not only useful in the prevention of unwanted pregnancies but safe to have pregnancies in future.
Let’s address a few concerns
Does birth control affect fertility?
Journal of Contraceptive Reproductive Med. 2018 clearly stated in a report that,” Contraceptive use regardless of its duration and method or preparation does not hurt the ability of women to conceive after stopping of use and it doesn’t significantly delay fertility. Therefore, appropriate counselling is important to assure the women to use the methods as to their interest.”
Birth control pills just stop ovulation and do not interfere with fertility. A 2018 report published in the BMJ, on JULY 23 concluded that “contraceptive use, regardless of its duration and type, does not have any significant negative effect on the ability of women to conceive.
Can birth control cause infertility in the future?
Birth control cannot cause infertility in the future. Research says Women who have used hormonal birth control are as likely to conceive as women who have never used hormonal contraceptives. A three-year study of 3,727 participants found that long-term use of oral contraceptives did not affect their ability to conceive in the future.
Are there any menstrual irregularities due to hormonal birth control?
The pills do have the hormones progestin and estrogen and help stop ovulation besides thickening the cervical mucus; so sperm can’t travel easily to fertilise the eggs.
Regular use can affect the menstrual cycle with either partial or complete suppression of the normal cycle. After stopping the pills, it will take some time to reset the menstrual cycles. This probably results in the misconception that taking the pill might make them infertile.
How much time does it take to regularise the menses after stopping contraception?
Research says, most users “regain or resume the normal hormonal balance within 3 to 6 months of stopping contraceptives.”
What are the concerns I can face if I want to go off birth control to conceive?
Since the pills are often prescribed or used for contraception, the entire communication is centred on them. You may experience a few of the symptoms like irregular periods, menstrual cramps, weight changes, mood swings etc.
Consult your doctor as you need to make some changes in diet and overall lifestyle, like getting adequate sleep and balanced nutrition as birth control pills cause depletion of vitamins B2, B6, and B12, vitamin C, vitamin E, folate etc along with blood glucose monitoring.
How long should you wait for conception after stopping birth control pills
It may take from a few months to a year for the woman to get back to her full conception health. Along with other research, it also found that the duration of contraceptive use had no impact on conception time. So, if you’ve been a long-term birth control user, you don’t have to worry about it.
If you are on birth control and now wish to stop it to get pregnant, you must seek a gynaecologist’s advice to realise the dream of parenthood. Your a gynaecologist can best guide you about when you can realistically hope to get pregnant after stopping birth control and regarding the diet and lifestyle changes that you may require to make.
Do birth control pills affect egg quality?
Higher dose oral contraceptives suppress ovarian function, However, that doesn’t mean these women’s egg quality has declined. Instead, hormonal birth control simply slows the egg maturation process in an earlier stage. so it doesn’t affect egg quality.
In a nutshell, let’s summarize,
Birth control measures have been studied extensively for their action, use as well as side effects too. Just remember, contraception cannot cause infertility. If you are experiencing a problem in conception, the problem lies somewhere else. We at Pearl Women’s Hospital have seen and treated many such cases where couples were on birth control pills and received the gift of joyful
0 notes
Text
OPTIMISING PLACEBOS AND MINIMISING NOCEBOS
LESSONS FROM BEHAVIOURAL SCIENCE
By Chloe Hutchings-Hay, Analyst at Ogilvy Consulting’s Behavioural Science Practice

Placebo Effect
The placebo effect was first established when Henry Beecher, a World War II doctor, ran out of morphine, and decided to give his patients a salt-water injection instead. He was surprised to learn that many of his patients (around a third) responded as though they had actually received morphine.
Since then, the benefits of placebo have been observed in treatments for illnesses as disparate as depression and Parkinson’s disease. One study even found that sham shoulder surgeries were as effective at improving symptoms as the real surgery itself (Schroder et al., 2017).
Whilst initially these benefits were thought of as ‘fake’, and those who experienced placebo effects were deemed suggestible, growing evidence suggests that there are real neurobiological mechanisms underpinning placebo effects. Supporting this is the mounting evidence from open-label placebo studies, where improvement has still been observed even when patients know they are receiving a placebo (BMJ, 2018), suggesting that conditioning alone can bring about the placebo effect. What’s more, personality factors are shown to be less important in determining response to placebo than factors determined by the broader context, like expectancy effects and the quality of the doctor-patient relationship.
The understanding that the context is crucial in eliciting the placebo response lends itself to the use of behavioural nudges to optimise the placebo response. Doctors already routinely prescribe placebos in their practices (Howick et al., 2013). Understanding how to best optimise the placebo response is important for medicine generally, as the success of conventional treatments is also bolstered via the placebo effect.
How Can We Optimise the Placebo Effect?
1. Priming: Placebos need to look legitimate, with branding and pricing being especially important. One study found higher-priced painkillers to be more effective than discounted painkillers (Waber et al., 2008); higher prices anchor expectations upwards. The colour of pills is important too, with learned associations having an impact on how we respond to drugs. We associated blue pills with sedation, yellow pills with mood enhancement and white pills with pain relief (Cohen, 2014). Setting the scene with good branding, thoughtful design and realistic pricing is key.
2. Affect: Creating a positive therapeutic relationship between patient and doctor is vital in eliciting the placebo response; our expectations about the efficacy of the medication are largely set in this interaction. The placebo effect is enhanced when doctors are more empathetic, have a warmer approach and spend longer with their patients (Benedetti, 2013). An initial positive interaction can improve the expectation that treatment is going to work and helps to ease anxiety.
Nocebo Effect
Sometimes thought of as the ‘evil twin’ of the placebo effect is the nocebo effect, referring to the development of side-effects following exposure to a sham substance. Evidence for the nocebo effect also abounds, with sham medication leading to increased side-effect reporting for conditions including hypertension and cancer (Enck et al., 2013). Systematic reviews find that around half of placebo groups in clinical trials experience adverse effects that are attributed to the drug (Howick et al. 2018).
The nocebo effect is often observed during public health outbreaks, putting huge pressure onto health providers. For example, in 1985 ‘radioactive caesium 137’ was scavenged from a disused hospital site in Goiânia, Brazil. 120,000 people subsequently sought screening for radioactive contamination at health facilities, however of the first 60,000 people screened, only 5,000 were symptomatic. This begs the question; why do people sometimes think they are unwell when they haven’t been exposed to anything harmful?
People sometimes believe they are unwell because they re-interpret pre-existing common symptoms in light of information about the health outbreak, like fatigue or headaches. Anxiety about a health outbreak can also be sufficient in and of itself to also generate physical symptoms.
Aside from these influences, the nocebo effect can also have a very real influence on generating harmful side-effects, in the same way that placebo effects can have a tangible positive influence on the body. Expectancy, rather than conditioning, is the crucial mechanism underpinning the nocebo effect. One study found that verbal suggestion alone was sufficient to make low-level electric shocks be experienced as highly painful (Colloca, Sigaudo & Benedetti, 2008).
How Can We Minimise the Nocebo Effect?
1. Positive Framing: At present, we are often all too aware of the possible side-effects that may come about as a result of trying a new medication. Even mere mentions of such side-effects can be sufficient to generate expectations of such symptoms (Colloca, Sigaudo & Benedetti, 2008). These potential negative outcomes can weigh more heavily in our minds than the possible benefits.
Changing the conversation to make it more positive may subsequently lessen the experience of side-effects, with patients having greater expectancy that the treatment will be effective. Positive framing is needed in the doctor-patient interaction, but also on information leaflets and drug packaging, which at present tend to focus on the riskiness of medication, rather than the benefits.
2. Reducing Salience of Side-Effect Information: Research suggests that a particularly effective strategy to ward against nocebo effects is to omit information about side-effects altogether (Webster & Rubin, 2019), which poses something of an ethical dilemma. However, given that we know that people can experience side-effects just because they expect to experience them, it makes sense to be reporting on the potential for adverse experiences in a responsible way.
One example of this going wrong comes from press coverage over side-effects associated with statins. In 2013; it was estimated that 200,000 people in the UK stopped taking statins as a result. Expectancy of side-effects seemed to be sufficient for many people to change their perception of their experience of taking statins. As a result, it is predicted that the incidence of cardiovascular disease will rise by an additional 2000 cases over the next decade (Horton, 2016).
Tackling medical consent therefore poses something of a thorny issue: how do we adequately warn people of possible risks without inadvertently creating negative outcomes? There has been discussion over the idea of contextualised consent: where adverse effects are presented as more of a ‘grey area’, instead of a definite likelihood, and where doctors can withhold certain pieces of information in the best interest of the patient (Chamsi-Pasha, Albar & Chamsi-Pasha, 2017).
The use of placebos provides a cost-effective way to create tangible improvements in patients’ lives. Behavioural science is key to maximising the benefits from placebos, in part through limiting the likelihood of developing side-effects from taking them.

References
Benedetti, F. (2013). Placebo and the new physiology of the doctor-patient relationship. Physiological reviews, 93(3), 1207-1246.
Chamsi-Pasha, M., Albar, M. A., & Chamsi-Pasha, H. (2017). Minimizing nocebo effect: Pragmatic approach. Avicenna Journal of Medicine, 7(4), 139-143.
Cohen, T. F. (2014, October 13). The Power of Drug Color. Retrieved from: https://www.theatlantic.com/health/archive/2014/10/the-power-of-drug-color/381156/
Colloca, L., Sigaudo, M., & Benedetti, F. (2008). The role of learning in nocebo and placebo effects. Pain, 136(1-2), 211-218.
De Pascalis, V., Chiaradia, C., & Carotenuto, E. (2002). The contribution of suggestibility and expectation to placebo analgesia phenomenon in an experimental setting. Pain, 96 (3), 393-402. Enck, P., Bingel, U., Schedlowski, M., & Rief, W. (2013). The placebo response in medicine: minimize, maximize or personalize?Nature reviews Drug discovery,12(3), 191.
Horton, R. (2016). Offline: Lessons from the controversy over statins. The Lancet, 388(10049), 1040.
Howick, J., Bishop, F. L., Heneghan, C., Wolstenholme, J., Stevens, S., Hobbs, F. R., & Lewith, G. (2013). Placebo use in the United Kingdom: results from a national survey of primary care practitioners. PLoS One, 8(3), e58247.
Howick, J. (2018, October 1). Is back pain really all in the mind?Retrieved from: https://www.pressreader.com/uk/the-daily- telegraph/20181001/281509342121606
Howick, J., Webster, R., Kirby, N., & Hood, K. (2018). Rapid overview of systematic reviews of nocebo effects reported by patients taking placebos in clinical trials. Trials, 19(1), 674.
Kaptchuk, T. J., & Miller, F. G. (2018). Open label placebo: can honestly prescribed placebos evoke meaningful therapeutic benefits?. British Medical Journal, 363, k3889.
Schrøder, C. P., Skare, Ø., Reikerås, O., Mowinckel, P., & Brox, J. I. (2017). Sham surgery versus labral repair or biceps tenodesis for type II SLAP lesions of the shoulder: a three-armed randomised clinical trial. Br J Sports Med, 51(24), 1759-1766.
Waber, R. L., Shiv, B., Carmon, Z., & Ariely, D. (2008). Commercial features of placebo and therapeutic efficacy. Jama, 299(9), 1016-7.
Webster, R. K., Weinman, J., & Rubin, G. J. (2016). A systematic review of factors that contribute to nocebo effects. Health Psychology, 35(12), 1334.
Webster, R., & Rubin, G. J. (2019). Influencing side-effects to medicinal treatments: A systematic review of brief psychological interventions. Frontiers in Psychiatry, 9, 775.
1 note
·
View note
Text
Why You Should Be Skeptical of the Latest Nutrition Headlines: Part 2
This article is Part 2 of a two-part series about the problems with nutrition research and the way it’s presented in the media. For more reasons why you should be skeptical of the latest nutrition headlines, check out Part 1 of this series.
In my last article in this series, I talked about why observational studies aren’t a great tool for proving causal relationships; how the data collection methods researchers use rely on memory, not facts; how the healthy-user bias can impact study results; and how, in many cases, nutritional studies uncover “risks” that look an awful lot like pure chance. In this post, I’ll delve deeper into the reasons why you should take nutrition headlines with a grain of salt.
Some Scientific Results Can’t Be Replicated
Science works by experiments that can be repeated; when they are repeated, they must give the same answer. If an experiment does not replicate, something has gone wrong. – Young & Karr, The Royal Statistical Society (1)
As Young and Karr suggest above, replication is a key feature of the scientific method. An initial finding does not carry much weight on its own. For it to be considered valid, it needs to be replicated by other researchers.
We’re supposed to trust nutrition researchers to help us understand our health, but in some cases, the way they think about nutrition is faulty. Check out more reasons why you should remain skeptical of nutrition headlines.
In the context of nutrition research, because observational studies cannot prove causality, their findings should ideally be replicated in a randomized controlled trial
(RCT). RCTs are specifically designed to prove causality, and while not perfect (see below), they are much more persuasive as evidence than observational studies.
The results from most observational nutrition studies have not been replicated by RCTs. In fact, one analysis found that:
Zero of 52 nutrition claims from observational studies for a wide variety of dietary patterns and nutrient supplementation were replicated, and five claims were statistically significant in the opposite direction.
Yes, you read that correctly. Out of 52 claims made in observational nutrition studies, zero were replicated and five indicated the opposite of what the observational study suggested!
Let’s look at a specific example. Observational studies suggested that people with the highest intakes of beta-carotene, an antioxidant nutrient found primarily in fruits and vegetables, had a 31 percent lower risk of death compared to those with the lowest intake. Yet RCTs of supplementation with beta-carotene not only failed to confirm this benefit, they found an increased risk of cancer in the group with the highest intake. (2) Oops! Similar results have been found with vitamin E. (3)
Researchers Focus on Quantity, Not Quality
People don’t eat nutrition, they eat food. – Margaret Mead
The vast majority of observational studies today focus only on nutrients, isolated food components, or biomarkers—like saturated fats, carbohydrates, calories, LDL cholesterol—abstracted out of the context of foods, diets, and bodily processes.
This reductionist approach, which philosopher of science Gyorgy Scrinis calls “nutritionism,” has interfered with nutrition science’s ability to provide useful individual and public health guidance. (4)
The upside of nutritionism has been the discovery of drugs, vitamins, and minerals that have saved millions of lives. The downside is that Americans (and people all over the industrialized world) are obsessing over details like the percentage of fat or carbohydrates they consume rather than focusing on the broader and more important issues, like the quality of the food they eat.
Two examples of how this has manifested over the past few decades are:
The promotion of margarine over the much better-tasting butter because of concerns about butter’s saturated fat content
The vilification of eggs due to their cholesterol content without considering their overall nutrient value
(And of course, we now know that butter is healthier than margarine and dietary cholesterol has no impact on heart disease. Another oops!)
Nutritionism is a relatively new phenomenon. It started in 1977 with the McGovern Report, the first widely disseminated nutrition guidance to provide detailed, quantitative, nutrient-focused dietary recommendations. (5) Prior to that, dietary guidelines were based on familiar concepts of food groups and serving sizes and relatively simple information on what foods to buy and eat to maintain health. The average person could easily understand—and most importantly, act on—the guidelines.
After the McGovern Report, dietary guidelines became increasingly complex and difficult for the layperson to comprehend. The 1980 dietary guidelines were published in a short, 19-page brochure; in 1985 it grew to 28 pages; in 2010 it was 112 pages; and in 2015, the most recent dietary guidelines took up 517 pages!
What Happens When You Look at Food Quality
A more recent example of nutritionism can be found in the heated debate over whether low-fat or low-carb diets are superior for weight loss and metabolic and cardiovascular health. Each side of the debate has its advocates, and the controversy continues.
In early 2018, a group of researchers led by Dr. Christopher Gardner set out to settle this debate with an RCT. They assigned participants into two groups: low-carb and low-fat. But here’s the catch: they instructed both groups to:
1) maximize vegetable intake; 2) minimize intake of added sugars, refined flours, and trans fats; and 3) focus on whole foods that were minimally processed, nutrient dense, and prepared at home whenever possible. (6)
For example, foods like fruit juice, pastries, white rice, white bread, and soft drinks are low in fat but were not recommended to the low-fat group. Instead, the dietitians encouraged participants to eat whole foods like lean meat, brown rice, lentils, low-fat dairy products, legumes, and fruit. Meanwhile, the low-carb group was instructed to focus on foods rich in healthy fats, like olive oil, avocados, salmon, cheese, nut butters, and pasture-raised animal products.
Perhaps not surprisingly—if you don’t embrace nutritionism, that is—the researchers found that on average, people who cut back on added sugar, refined grains, and processed food lost weight over 12 months—regardless of whether the diet was low-carb or low-fat.
This was a fantastic example of what a nutrition study should look like. It resulted in clinically relevant, practical advice that is easy for people to follow: eat real food. Just imagine where we might be now if most nutrition studies over the past 40 years had been designed like this?
RCTs Are Better than Observational Studies but Still Problematic
If observational studies cannot prove causality, then why do they continue to form the foundation of dietary guidelines and public health recommendations? The answer is that RCTs also have several shortcomings that, thus far, have made them impractical as a tool for studying population health.
Duration
Most relationships between nutritional factors and disease can take years, if not decades, to develop. What’s more, the effects of some nutritional interventions in the short term are different than they are over the long term.
Weight loss is a great example. Both low-carb and low-fat diets have been shown to cause weight loss in the short term, but over the long term (more than 12 months) people tend to regain the weight they lost.
Inadequate Sample Size
The sample size, or number of participants in an RCT, is one of the most important factors in determining whether the results of the study are generalizable to the wider population. Most nutrition RCTs do not have a large enough sample size.
Dr. John Ioannidis, a professor at the Stanford School of Medicine, highlighted this problem in a recent editorial in BMJ called “Implausible Results in Human Nutrition Research.”
To identify a nutrition-related intervention that produces a legitimate 5 to 10 percent relative risk reduction in total mortality, we’d need studies that are 10 times as large as the highly publicized PREDIMED trial (which had around 7,500 participants), in addition to long-term follow-up, linkage to death registries, and careful efforts to maximize adherence.
RCTs Are Expensive
One reason that it’s such a huge challenge to design RCTs with sufficient duration and sample size is cost. RCTs are enormously expensive. In the pharmaceutical world, drug companies pay for RCTs because they have a vested financial interest in their results. But who will pay for long-term RCTs in the nutrition world? Public funding for nutrition research (and many other types of research) is declining, not increasing, which makes it unlikely that we’ll see long-term RCTs with sufficient sample sizes anytime soon.
Quality RCTs Are Difficult to Do
As Dr. Peter Attia points out in his excellent series Studying Studies, designing high-quality RCTs is fraught with challenges:
These trials need to establish falsifiable hypotheses and clear objectives, proper selection of endpoints, appropriate subject selection criteria (both inclusionary and exclusionary), clinically relevant and feasible intervention regimens, adequate randomization, stratification, and blinding, sufficient sample size and power, and anticipation of common practical problems that can be encountered over the course of an RCT.
That’s not an easy task and few nutrition RCTs meet the challenge.
Conflicts of Interest Are Very Common
It’s difficult to get a man to understand a thing if his salary is dependent upon him not understanding it. – Upton Sinclair
Many have written about financial conflicts of interest and their impact on all forms of research, including nutrition research. In short, research has shown that when studies are funded by industry, they are far more likely to report results that are favorable to the sponsor.
In one analysis performed by Marion Nestle, 90 percent of industry-sponsored studies returned sponsor-friendly results. (7) For a summary of the issues and how they impact the quality of nutrition research, I recommend this story from Vox.
In this article, I’d like to focus on another type of conflict of interest: allegiance bias, which is also known as “white hat bias.” Allegiance bias is not as well recognized as financial conflicts of interest are, which is one of the many reasons that it has an insidious effect on nutrition research.
Allegiance bias has been defined as “bias leading to distortion of research-based information in the service of what may be perceived as righteous ends.” (8)
For example, imagine that a vegan researcher sets out to do a study on the health impacts of a vegan diet. Is it possible that the researcher’s ideological commitment to veganism could influence, both consciously and unconsciously, how the study is designed, executed, and interpreted? Of course it could. In fact, it’s difficult to see how it couldn’t.
In a 2018 editorial called “Disclosures in Nutrition Research: Why It Is Different,” Dr. Ioannidis suggests that allegiance bias should be disclosed by researchers, just as financial conflicts of interest are. He says:
Therefore, it is important for nutrition researchers to disclose their advocacy or activist work as well as their dietary preferences if any are relevant to what is being presented and discussed in their articles. This is even more important for dietary preferences that are specific, circumscribed, and adhered to strongly. [emphasis added]
Ioannidis goes on to say that advocacy and activism, while laudable, are contrary to “a key aspect of the scientific method, which is to not take sides preemptively or based on belief or partisanship.” [emphasis added]
Veganism certainly meets the criteria of dietary recommendations that are “specific, circumscribed, and adhered to strongly.” In fact, some have pointed out that veganism meets the four dimensions of religion:
Belief: Veganism began as a way to express moral integrity regarding the appropriation and suffering of non-humans.
Ritual: Veganism involves strict dietary restrictions, including abstaining from the use of materials made from any animal products.
Experience: The “holistic connectedness” of veganism would be considered a religious experience to those who live it.
Community: There are many official and unofficial vegan associations across the world, and in 2017 a civil flag was created for the international vegan community.
Researchers and physicians like T. Colin Campbell, Kim Williams, Caldwell Esselstyn, Joel Fuhrman, John McDougall, and Neal Barnard could all be expected to suffer from this “white hat bias.” They’re involved in vegan advocacy and activism, both of which could be expected to be a source of allegiance bias.
A Famous Example of Allegiance Bias at Work
The China Study, a book by vegan physician and researcher T. Colin Campbell, is a perfect example. Campbell claimed that this study—which was not peer-reviewed—proved that:
Animal protein causes cancer
A plant-based diet protects against heart disease
You can get all the nutrients you need from plants
Campbell even went as far as saying, “Eating foods that contain any cholesterol above 0 mg is unhealthy,” a claim that has been completely disproven and is reflected in the 2015 change in the U.S. Dietary Guidelines that no longer regards dietary cholesterol as a nutrient of concern.
However, since The China Study was published, several independent, peer-reviewed studies of the data have refuted T. Colin Campbell’s claims. For a great summary of the issues with The China Study, see this article by nutritional scientist Dr. Chris Masterjohn.
Allegiance bias can take several forms. It can involve:
Cherry-picking studies to support a cherished view
Misleadingly describing the results of studies that are cited in a paper
“Data dredging” to search for statistical significance within given data sets (when no such significance is present)
Not reporting null results
Designing experiments for the purpose of obtaining a particular answer
And more
It’s important to point out that allegiance bias is not always, or even often, conscious. Most researchers believe they are acting with scientific rigor and integrity. This is exactly why it’s so difficult to guard against, and why it’s so important to disclose.
Nutrition Policy Is Informed by Politics and Religion—Not Just Science
In a perfect world, dietary guidelines and nutritional policy would be the product of a thorough and dispassionate review of the available scientific evidence and not be unduly influenced by politics—and certainly not by religion. Dissenting views that are well informed would be not only welcomed but encouraged. As Syd Shapiro once said, “We should never forget that good science is skeptical science.”
Alas, we don’t live in a perfect world. In our world, dissenting views are are not welcomed; they’re suppressed. Dr. D. Mark Hegsted, a founding member of the Nutrition Department at the Harvard School of Public Health, made this opening remark in the 1977 McGovern hearing:
The diet of Americans has become increasingly rich—rich in meat, other sources of saturated fat and cholesterol … [and] the proportion of the total diet contributed by fatty and cholesterol-rich foods … has risen.
The only problem with this statement is that it directly contradicted USDA economic data which suggested that total calories and the availability of meat, dairy, and eggs at the time of the report were equivalent or marginally less than amount consumed in 1909. Full-fat dairy consumption was lower in 1977 than 1909, having declined steadily from 1950 to 1977. (9) Other evidence that contradicted Dr. Hegsted’s opinion was also ignored.
The feedback from the scientific community on the McGovern Report was “vigorous and constructive,” explicitly stated the “lack of consensus among nutrition scientists,” and presented evidence for the diversity of scientific opinion on the subject. (10) Other countries, such as Canada and Great Britain, also noted the lack of consensus on whether dietary cholesterol intake should be limited. U.S. senators issued the following statement about the McGovern Report:
It is clear that science has not progressed to the point where we can recommend to the general public that cholesterol intake be limited to a specified amount. The variances between different individuals are simply too great. A similar divergence of scientific opinion on the question of whether dietary change can help the heart illustrates that science cannot yet verify with any certainty that coronary heart disease will be prevented or delayed by the diet recommended in this report. (See footnote)
Nevertheless, these cautionary words were ignored, and the recommendations from the McGovern Report were adopted. This kicked off the fat and cholesterol phobia that would grip the United States for the next four decades.
Religion Can Impact Nutrition Guidelines
Another example of how non-scientific factors drive nutrition policy is the influence of the Seventh Day Adventists on public health recommendations in the United States and around the world. Seventh Day Adventists (SDA) is a Protestant denomination that grew out of the Millerite movement in the United States. Health has been a focus of SDA teachings since the inception of the church in the 1860s. According to Wikipedia:
Adventists are known for presenting a “health message” that advocates vegetarianism and expects adherence to the kosher laws, particularly the kosher foods described in Leviticus 11, meaning abstinence from pork, shellfish, and other animals proscribed as “unclean.” The church discourages its members from consuming alcoholic beverages, tobacco or illegal drugs. ... In addition, some Adventists avoid coffee, tea, cola, and other beverages containing caffeine.
Ellen White, an early SDA church leader, received her first major health reform vision in 1863, and “for the first time, God’s people were urged to abstain from flesh food in general and from swine’s flesh in particular.” Most SDA diet beliefs are based on White’s health visions.
White believed that the church had a duty to educate the public about health as a way to control desires and passions. Adventists continue to believe that eating meat stirs up “animal passions,” and that is one of the reasons for avoiding it.
Another early SDA leader, Lenna Cooper, was a dietitian who cofounded the American Dietetics Association, which continues to advocate a vegetarian diet to this day. Cooper wrote textbooks and other materials that were used in dietetic and nursing programs, not only in the United States but around the world, for more than 30 years. The SDA Church established hundreds of hospitals, colleges, and secondary schools and tens of thousands of churches around the world—all promoting a vegetarian diet—and played a major role in the development and mass production of plant-based foods, such as meat analogues, breakfast cereals, and soy milk. (11)
Adventists have been behind much of the early research on vegetarian diets at Loma Linda University in San Diego, where SDA leaders established a dietetics department in 1908. This was an ostensibly scientific endeavor at a university that was established by a religious group that believed vegetarianism was ordained by God.
If you think this raises a huge red flag for allegiance bias, you’re not wrong. In fact, as Jim Banta pointed out in a fascinating review of the SDA influence on diet, administrators at Loma Linda University in the mid-1900s initially discouraged research on vegetarian diets because “if you find the diets of vegetarians are deficient, it will embarrass us.” That is not the attitude of skepticism and open-minded inquiry that characterizes good science.
My Final Thoughts on Nutrition Research
I’d like to conclude with the opening two paragraphs of a recent open letter that scientists Edward Archer and Chip J. Lavie wrote to the National Academies of Sciences, Engineering, and Medicine:
“Nutrition” is now a degenerating research paradigm in which scientifically illiterate methods, meaningless data, and consensus-driven censorship dominate the empirical landscape. Since the 1950s, there was a naïve but politically expedient consensus that a person’s usual diet could be measured simply by asking what he or she remembered eating and drinking. Despite the credulous and unfalsifiable nature of this memory-based method, investigators used it to produce hundreds of thousands of publications and acquire billions of taxpayer dollars.
Over time, the sustained funding of demonstrably pseudo-scientific research methods has subverted the self-correcting nature of science and suppressed skeptical scholarship. Consequently, many decades of politics taking precedence over critical inquiry produced contradictory dietary guidelines, failed public policies, and the continued confusion over “what-to-eat.”
I couldn’t have said it better myself.
What do you think about the latest nutrition headlines? Do you read the newest research with skepticism? Let me know below in the comments—and be sure to check out Part 1 of this two-part series!
Staff of the Select Committee on Nutrition and Human Needs, United States Senate. Dietary Goals for the United States. 2nd ed. Washington, DC: Government Printing Office; December 1977.
The post Why You Should Be Skeptical of the Latest Nutrition Headlines: Part 2 appeared first on Chris Kresser.
Source: http://chriskresser.com
September 26, 2018 at 11:54PM
9 notes
·
View notes
Text
Global Capsule Endoscopy Market
Global Capsule Endoscopy Market Size, Share, Growth, Industry Trends and Forecast 2020-2030
The global Capsule endoscopy market is accounted approximate USD 214.7 million in 2020 and it is expected to reach approximate USD 775.1 million by 2030 with a CAGR of 13.7% during forecast period. Capsule endoscopy is a procedure that is used for the visualisation of the interior areas of intestines and other parts of the digestive, respiratory, and urinary tract. The process involves swallowing of a pill-sized capsule endoscope by the patient which further enables in capturing the images of the digestive tract. The captured images are then transferred to a recorder which is mounted on a waist belt. The recorder also tracks the position and movement of the capsule inside the body. The images captured are later investigated for the detection of any digestive disorders. This method eliminates the use of any surgical method for visualisation and is more efficient than the conventional endoscopy which uses wire. The primary components of a capsule endoscope includes camera, batteries, transmitter, and light source. The integrated camera in the capsule takes around two pictures per second and the battery lasts for almost 8 hours. The growing occurrence of chronic disorders and superior advantage over conventional endoscopy are the major factors that are driving the capsule endoscopy market globally. The global Capsule endoscopy market is accounted approximate USD 214.7 million in 2020 and it is expected to reach approximate USD 775.1 million by 2030 with a CAGR of 13.7% during forecast period.
Download Sample Copy of the Report to understand the structure of the complete report (Including Full TOC, Table & Figures) @ https://www.decisionforesight.com/request-sample/DFS020185
Market Dynamics and Factors:
The rising geriatric population across the globe has contributed to various chronic diseases of the digestive tract like gastrointestinal bleeding, Crohn’s disease, colon cancers, small intestinal tumours, and many others. For instance, according to the American Cancer Society, around 97220 cases of colon cancer were reported in 2018. The demand for faster and precise diagnostic tools along with the rising digestive tract disorders is propelling the growth of the capsule endoscopy market. Technological advancements, growing awareness among people, and rising income levels have forced the transformation of conventional endoscopic procedures to capsule endoscopy which in turn has fuelled the growth of the market. According to BMJ journal report, the global colon cancer cases are going to reach a figure of 2.2 million by 2030, which in turn will provide huge growth opportunity for the growth of the capsule endoscopy market. However, high costs associated with the advanced capsule endoscopy devices and dearth of skilled technicians are certain factors that will restrain the growth of the capsule endoscopy market.
Market Segmentation:
Global Capsule Endoscopy Market – By Product Type
Colonic Capsule
Bowel Capsule
Esophageal Capsule
Global Capsule Endoscopy Market – By Component
Wireless Capsule Endoscope
Capsule Endoscopy Image Recorder
Capsule Endoscopy Image Workstation
Global Capsule Endoscopy Market – By Application
Gastrointestinal Tract
Urinary Tract
Respiratory Tract
Female Reproductive Tract
Others
Global Capsule Endoscopy Market – By End-Users
Hospitals
Clinics
Research Centre’s
Others
Global Capsule Endoscopy Market – By Geography
North America
U.S.
Canada
Mexico
Europe
U.K.
France
Germany
Italy
Rest of Europe
Asia-Pacific
Japan
China
India
Australia
Rest of Asia Pacific
ROW
Latin America
Middle East
Africa
New Business Strategies, Challenges & Policies are mentioned in Table of Content, Request TOC at @ https://www.decisionforesight.com/toc-request/DFS020185
Geographic Analysis:
North America is expected to dominate the global capsule endoscopy market in terms of market share during the forecast period. The major factors attributing towards this dominant market position include growing incidences of gastrointestinal disorders and colon cancer; presence of major manufacturers and advanced healthcare facilities; and favourable reimbursement policy in the region. For instance, according to American Cancer Society, around 141000 people were diagnosed with colon cancer out of which 49000 died in 2011. The European region is estimated to be the second-most dominant market for capsule endoscopy during the forecast period. Rising prevalence of Crohn’s disease and ulcerative colitis are expected to boost the market growth in the region. Asia Pacific region is anticipated to witness maximum growth during the forecast period. Changing economic conditions, increased healthcare spending, and rising healthcare infrastructure are the key factors attributing towards the market growth in the APAC region.
Competitive Scenario:
The key players operating in the global capsule endoscopy market are –
IntroMedic, Olympus Corporation, Capsovision, Medtronic Plc., Chongqing Jinshan Science & Technology, Fujifilm Holding Corporation, Given Imaging Ltd., RF System Lab, Capsocam plus, AccuRead Endoscopy Inc.
Connect to Analyst @ https://www.decisionforesight.com/speak-analyst/DFS020185
How will this Market Intelligence Report Benefit You?
The report offers statistical data in terms of value (US$) as well as Volume (units) till 2030.
Exclusive insight into the key trends affecting the Global Capsule Endoscopy industry, although key threats, opportunities and disruptive technologies that could shape the Global Capsule Endoscopy Market supply and demand.
The report tracks the leading market players that will shape and impact the Global Capsule Endoscopy Market most.
The data analysis present in the Global Capsule Endoscopy Market report is based on the combination of both primary and secondary resources.
The report helps you to understand the real effects of key market drivers or retainers on Global Capsule Endoscopy Market business.
The 2021 Annual Global Capsule Endoscopy Market offers:
100+ charts exploring and analysing the Global Capsule Endoscopy Market from critical angles including retail forecasts, consumer demand, production and more
15+ profiles of top producing states, with highlights of market conditions and retail trends
Regulatory outlook, best practices, and future considerations for manufacturers and industry players seeking to meet consumer demand
Benchmark wholesale prices, market position, plus prices for raw materials involved in Global Capsule Endoscopy Market type
Buy This Premium Research Report@ https://www.decisionforesight.com/checkout/DFS020185
About Us:
Decision Foresight is a market research organization known for its reliable and genuine content, market estimation and the best analysis which is designed to deliver state-of-the-art quality syndicate reports to our customers. Apart from syndicate reports, you will find the best market insights, strategies that will help in taking better business decisions on subjects that may require you to develop and grow your business-like health, science, technology and many more. At Decision Foresight, we truly believe in disseminating the right piece of knowledge to a large section of the audience and cover the in-depth insights of market leaders across various verticals and horizontals.
Contact:
Email: [email protected]
For Latest Update Follow Us:
https://www.facebook.com/Decision-Foresight-110793387201935
https://twitter.com/DecisionFs
https://www.linkedin.com/company/decision-foresight/
0 notes
Text
March 2021 Learning Network Resources
Tuesday, April 20th @ 4PM EST
Join us for “Tackling COVID-19 Vaccine Hesitancy,” with speaker Sandra Quinn, PhD, Maryland Center for Health Equity, University of Maryland. Register here.
Trust in Healthcare
Fluer NS. ‘A massive gap in information’: Most vaccine clinical trials fail to report data on participants’ ethnicity or race. STAT. February 2021
“An analysis of the demographics of a decade’s worth of vaccine clinical trials has found that Black Americans, Latinos, American Indians, and Alaskan Natives, as well as people age 65 and older, were underrepresented as participants within these studies, though most of the differences, when compared with the U.S. population, were not especially large. Adult women, on the other hand, were found to be overrepresented.”
Salomon G, et alt. Latinos face barriers like fear, language in getting vaccine. Associated Press. February 2021
“America’s more than 60 million Latinos — like other people of color — have been disproportionately affected by the virus, and many are struggling with issues like a lack of knowledge about the shots, state vaccine websites that don’t have Spanish instructions, ways to find appointments in their communities and fears they could be targeted for immigration enforcement.”
Garber J. Covid-19 shows how our hospital system is “separate and unequal.” Lown Institute. February 2021
“Why does this happen? Our health care delivery system is fragmented, divided between community hospitals (often public hospitals) and private ones. Private hospitals often cherry-pick wealthier patients with private insurance and avoid taking patients with public insurance, funneling poorer and sicker patients to the public hospitals. In the case of MLK hospital, only 4% of their patients have private insurance, according to the Times.”
Marill MC, et alt. Community Health Workers, Often Overlooked, Bring Trust to the Pandemic Fight. Kaiser Health News. February 2021
“With their deep roots in the community, many of these workers were disappointed when they were not called on to help initially in the pandemic. Community health workers often work on grant-funded projects with a specific goal, such as improving blood sugar control among people with diabetes. When the pandemic shutdown suspended those programs, many found themselves without a job.”
How to End Surprise Medical Bills. Bloomberg Opinion. February 2021
“The scandal of surprise bills has been tolerated far too long. The new law is an important step forward — but it’s too soon to declare it a success. First, it must be made to work.”
Gorges RJ, et alt. Factors Associated With Racial Differences in Deaths Among Nursing Home Residents With COVID-19 Infection in the US. JAMA Network. February 2021
“The study’s findings suggest that the inequalities underlying racial disparities in COVID-19 infection and mortality in the general population may also be associated with differences in mortality among nursing home residents with COVID-19 infection.”
Blogs, Issue Briefs, Opinion Pieces and More…
UTIs Treated Inappropriately Everywhere. Medpage Today. February 2021
“A majority of women with uncomplicated urinary tract infections (UTIs) received inappropriate antibiotics or continued treatment beyond the recommended duration, a review of almost 700,000 cases showed.”
Journals
Mafi JN, et alt. Trends in Low-Value Health Service Use and Spending in the US Medicare Fee-for-Service Program, 2014-2018. JAMA. February 2021
“This cross-sectional study found that among individuals with fee-for-service Medicare receiving any of 32 measured services, low-value care use and spending decreased marginally from 2014 to 2018, despite a national education campaign in collaboration with clinician specialty societies and increased attention on low-value care. While most use of low-value care came from 3 services, 1 of these was opioid prescriptions, which increased over time despite the harms associated with their use. These findings may represent several opportunities to prevent patient harm and lower spending.”
Hall AM, et alt. Do not routinely offer imaging for uncomplicated low back pain. BMJ. February 2021
“The past two decades have seen a paradigm shift in the way we use imaging when managing low back pain (LBP). Imaging was once a routine part of the diagnostic workup for most cases of LBP. Evidence now indicates that imaging is useful only in the small subgroup of patients for whom there is suspicion of red flag conditions.”
Wang T, et alt. Variations in Persistent Use of Low-Value Breast Cancer Surgery. JAMA Surgery. February 2021
“Interfacility variation demonstrates a performance gap and an opportunity for formal deimplementation efforts targeting each procedure. Several facility-level characteristics were associated with differential deimplementation and performance.”
Ellenbogen MI, et alt. Development of a Simple Index to Measure Overuse of Diagnostic Testing at the Hospital Level Using Administrative Data. Journal of Hospital Medicine. February 2021
“We developed a diagnostic overuse index that identifies hospitals with high levels of diagnostic intensity by comparing negative diagnostic testing rates for common diagnoses.”
Kim DD, et alt. An Evidence Review of Low-Value Care Recommendations: Inconsistency and Lack of Economic Evidence Considered. Journal of General Internal Medicine. February 2021
“Our study found that evidentiary rationales for low-value care vary substantially, with most recommendations relying on clinical evidence. Broadening the evidence base to incorporate cost-effectiveness evidence can help refine the definition of “low-value” care to reflect whether an intervention’s costs are worth the benefits. Developing a consensus grading structure on the strength and evidentiary rationale may help improve de-implementation efforts for low-value care.”
Gilmore RC, et alt. Underutilization of Needle Biopsy Before Breast Surgery: A Measure of Low-Value Care. Annals of Surgical Oncology. January 2020
“Marked variation exists in whether a breast core biopsy is performed prior to initial breast surgery, which may represent unnecessary surgery on individual patients. Providing surgeon-specific feedback on guideline compliance may reduce unwarranted variation.”
Determining the impact of body mass index on ultrasound accuracy for diagnosing appendicitis: Is it less useful in obese children? Journal of Pediatric Surgery. January 2020
“An elevated BMIP may increase difficulty in visualizing the appendix, resulting in inaccurate or equivocal findings. This risk is seen specifically in obese males. If US findings do not correlate with clinical assessment in obese children with abdominal pain, further evaluation may be warranted.”
Media
The need for alternatives to opioids for children and adolescents. Toronto Star. February 2021
“In mid-February, Toronto Public Health reported that January 2021 was a record-setting month — not for COVID-19, but for opioid use. Paramedics reported 333 non-fatal and 38 fatal calls.”
Optimizing Neoadjuvant Therapy for Breast Cancer. Medpage Today. February 2021
“Neoadjuvant chemotherapy is the treatment of choice for newly diagnosed inflammatory or unresectable breast cancer, as well as locally advanced disease that might be rendered operable with neoadjuvant therapy, according to a new guideline from the American Society of Clinical Oncology (ASCO).”
The post March 2021 Learning Network Resources first appeared on Choosing Wisely.





https://feeds.feedblitz.com/~/647119816/0/catherinemccracken~March-Learning-Network-Resources/
0 notes
Text
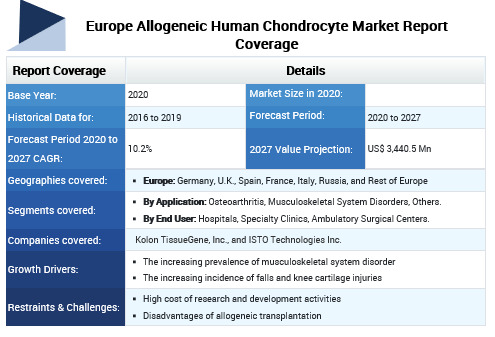
Europe Allogeneic Human Chondrocyte Market Analysis (2020-2027)
Allogeneic human chondrocyte is an emerging therapy, which can be used for cartilage repair and other indications. Currently, very few market players are developing these therapies, wherein the studies are in clinical trial phase and are expected to soon receive approval from the regulatory agencies. For instance, Invossa, from Kolon TissueGene, Inc., is expected to be the world’s first cell-and-gene therapy for osteoarthritis. This therapy is going to be a cartilage cells extracted from human cartilage (first fluid of HC) and transformed cells with TGF-β1 (second fluid of TC) by the ratio of 3:1. The product is currently in phase 3 clinical trial phase. This is expected to create lucrative opportunity for players to develop such therapies in the near future.
The Europe allogeneic human chondrocyte market is expected to be valued at US$ 3,440.5 million in 2027 and is expected to exhibit a CAGR of 10.2% during the forecast period (2026-2027).
Figure 1. Europe Allogeneic Human Chondrocyte Market Share (%) in Terms of Value, By Country, 2027

Rising incidence of falls and knee cartilage injuries is expected to propel the market growth during the forecast period
Increasing cases of falls and knee cartilage injuries is a major factor that is expected to propel growth of the Europe allogeneic human chondrocyte market over the forecast period. According to the article published in the British Medical Journal (BMJ Journal) February 2020, the incidence of falls in European countries were as follows in 2017: in the Western European region, 13,840 per 100,000 population seek medical treatment for fall related injury, of which 7,594/100,000 are from Greece and 19,796 are from Norway.
Figure 2. Europe Allogeneic Human Chondrocyte Market Share (%), by Application, 2027
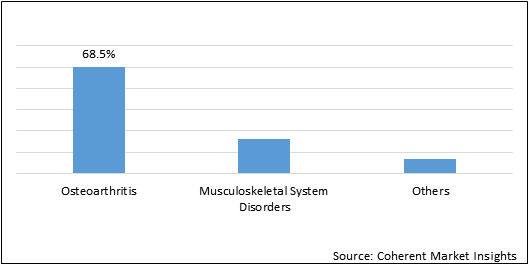
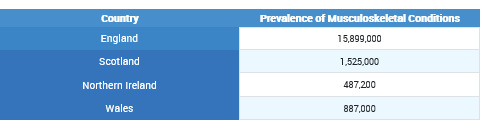
Increasing prevalence of musculoskeletal system disorders is expected to propel the market growth over the forecast period
Increasing cases of musculoskeletal system disorders is expected to drive the market growth during the forecast period. According to the State of Musculoskeletal Health, 2019 report by the Versus Arthritis, the prevalence of musculoskeletal conditions in the U.K. in 2017, was as follows:
Europe Allogeneic Human Chondrocyte Market - Impact of Coronavirus (Covid-19) Pandemic
The COVID-19 pandemic is affecting clinical trials, drastically. According to a survey conducted by Medidata Solutions, Inc. (an American technology company, which develops and markets software as a service for clinical trials), on April 23, 2020, 63% of survey respondents reported that they have stopped recruiting new patients for ongoing clinical trials and 43% of the respondents have postponed their studies.
Furthermore, ongoing clinical trials are being conducted by healthcare facilities and researchers using the following safety measures:
The healthcare providers are obtaining patient consent through phone or video conferences. According to a survey conducted by Medidata Solutions, Inc. on April 23, 2020, 45% of the respondents opted for virtual/telemedicine for consultancy
Patients receive a phone call for the screening of COVID-19 symptoms before they schedule in-person visits
The assessment of the studies are being done in single outpatient areas
Europe Allogeneic Human Chondrocyte Market Restraints:
As the research for human allogeneic chondrocyte is ongoing and products are majorly in the development phase, the research cost and procedures are considerably high and tedious, which can affect the development of such products and is expected to hinder growth of the market.
Moreover, the disadvantages of allogeneic transplantation as compared to autologous transplantation is expected to limit the adoption of allogeneic transplantation, thereby hindering the Europe allogeneic human chondrocyte market growth.
Key Players
Major players operating in the Europe allogeneic human chondrocyte market include Kolon TissueGene, Inc. and ISTO Technologies Inc.
Request sample copy here :
https://www.coherentmarketinsights.com/insight/request-sample/4088
Request PDF brochure here:
https://www.coherentmarketinsights.com/insight/request-pdf/4088
About Us:
Coherent Market Insights is a global market intelligence and consulting organization focused on assisting our plethora of clients achieve transformational growth by helping them make critical business decisions.
What we provide:
· Customized Market Research Services
· Industry Analysis Services
· Business Consulting Services
· Market Intelligence Services
· Long term Engagement Model
· Country Specific Analysis
Contact Us:
Mr. Shah
Coherent Market Insights Pvt. Ltd.
Address: 1001 4th ave, #3200 Seattle, WA 98154, U.S.
Phone: +1-206-701-6702
Email : [email protected]
Reference/Source: https://www.coherentmarketinsights.com/
#Allogeneichumanchondrocytemarketanalysis#cartilagerepair therapy#Healthcare#therapy#CoherentMarketInsights#MarketAnalysis
0 notes
Text
Climate communications: Time Magazine changes headline three times, uses false headline "How Asthma Inhalers are Choking the Planet"
Time Magazine ran a fiction story about asthma inhalers and greenhouse gases based loosely on a paper in BMJ. The original story contained numerous errors, some of which have since been removed.
First, their evolving headline changes:
Revision 0: “How Asthma Inhalers are Contributing to Climate Change“.
Revision 1: “How Asthma Inhalers are Choking the Planet“
Revision 2: “How One Commonly Used Asthma Inhaler is Damaging the Planet“
Revision 0 is accurate.
Revision 1 is what they ran with and promoted online, and shared on social media. This version was insensitive/rude and 100% false. This version is STILL running on their own social media, even though they acknowledge it is false.
After I (and presumably others) contacted Time Magazine, they revised the headline a third time to a technically accurate but misleading and exaggerated headline (Revision 2).
They also corrected, partially, other errors in the report – but left some in place.
For example, they incorrectly said inhalers use methane as the propellant, and then cited an activist group’s estimate of greenhouse impacts (84x) for methane, rather than the science-based IPCC AR5’s more modest value (28x). This exaggeration is classic yellow journalism. But inhalers do not use methane – a point they had wrong.
The reference to methane and 84x has been deleted but they make no mention of these changes in their corrections list.
The failed to put anything in context – a typical human’s breathing over the course of the year emits twice the level of CO2 as the CO2 equivalent of the worst case inhaler used every day. And this is about 1% of the CO2 equivalent produced by a typical American home and life activities or 2% of a typical European home.
They issued a Corrections List but also bungled that.
This error-ridden propaganda message was written by an Editor-At-Large who was formerly Senior Editor for Science, of all things.
Their Failure
The widely promoted headline “How Asthma Inhalers are Choking the Planet” was presumably viewed as a clever word play, making a joke about asthmatics “choking” when they could not breathe. This was a juvenile attempt at humor and remarkably insensitive and rude to asthmatics. Let’s make fun of crippled people too, while we are at it? This version uses the propaganda method of Fear to enhance the click-bait effect of the title, and to scare the target into action.
Second, the claim that inhalers are “Choking the Planet” is 100% false and not physically possible. In homes that use inhalers daily (in the U.S.), the CO2-equivalent greenhouse gas potential is about 1% of the homes annual CO2-equivalent greenhouse gas emissions. About 1 in 12 people are diagnosed with asthma, but only some of them have an inhaler, only some of which use a greenhouse gas-based propellant, and they may not use it every day. For example, I have exercise induced asthma and I use an inhaler before I go jogging (varies 2x to 4x/week).
If asthma inhalers containing HFA were 100% eliminated tomorrow, there would be no detectable change in weather or climate over the next hundred years. None at all.
The errors were so numerous and so bad that this was likely an intentional propaganda messaging campaign by Time Magazine using the primary propaganda methods of Lies and Fear, to scare the target into taking action.
Evidence History
Here is the original title, as captured in my browser. (I had to use my cell phone to take a photo, rather than a Windows snapshot – due to a keyboard dying I have an old Mac keyboard plugged into my Windows computer, but it lacks the key I need to activate my screen snapshot):
Here is the false headline Time ran for several days last week, and promoted on social media:
Here is the revised headline (third revision):
But look closer – they still have the false heading as the caption on the illustration:
They did not revise the text, which still contains the false “choking the planet” assertion and continues to imply that all 235 million patients use the offending inhalers.
They removed the following text which erroneously cited “methane” (inhalers do not use methane) and used an exaggerated claim of 84x multiplier (for methane) from the activist group Environmental Defense Fund (IPCC AR5 uses 28x multiplier for methane).
A typical inhaler uses two puffs per dose. Thus, a 200-puff inhaler delivers 100 doses. If someone uses an inhaler once per day (some, like me, use much less than this, while others use several times per day), the worst case scenario is up to 79 pounds of CO2-equivalent per worst case inhaler multiplied by about 4 inhalers per year. (Some HFA inhalers produce only 22 pounds, which cuts this worst case by a factor of 4). That’s 79 x 4 or 360 pounds per year (or 90 pounds for best case) versus the estimated average of 40,000 pounds of CO2-equivalent greenhouse gas emissions from a typical U.S. home and life activities per year. That is my own estimate. The BMJ paper (page 4) estimates the worst case inhaler yields 36.5 kg CO2-equivalent per inhaler. If 4 inhalers are used per year, that is 321 pounds of CO2 equivalent, inline with my estimates.
In context, inhaler effects are close to zero. (There may be errors in the BMJ journal paper but I am not going to pursue those.)
To add additional context, the average human emits an estimated 725 pounds of CO2 per year by breathing. Which is twice the CO2-equivalent impact of using the worst case inhaler, every day. That is from calculated values – converted to an annual amount and converted from metric by me – underlying calculations are from Dr. Peggy LeMone, National Center for Atmospheric Research. Joggers contribute more to choking the planet than walkers – let’s blame joggers too!
The original BMJ paper notes that surveys indicate half of the inhalers turned over to prescription recycling programs are half full, implying, as they note, that people are not using the full doses of their inhalers probably because they did not know if they were empty or not. The content of these inhalers might never be released to the atmosphere. In fact, most are incinerated and incineration alters the gases so that they no longer operate as an HFA greenhouse gas. Merely recapturing the unused propellant, as is already done, cuts the estimated CO2-equivalent release by 25%.
Time Magazine is a Propaganda and Yellow Journalism Operation
The errors – such as the Revision 1 title, the incorrect reference to methane and the exaggerated 84x multiplier from an activist organization are deliberate choices. This was a propaganda mission by Time Magazine. The author is Time’s own former Senior Editor for Science who now has the title Editor-At-Large. Good grief.
Their corrections list omits the full title change, and omits their removal of the 84x multiplier they obtained from the Environmental Defense Fund. In fact, some of the errors they presumably corrected are still in the text of the article and the caption of the lead illustration. The incorrect version continues to run on their social media, including their original video graphic which remains uncorrected.
Editor’s note, Nov. 7:
The original headline on this story has been updated to clarify that it is one commonly used type of inhaler—not all inhalers—that emits significant greenhouse gases.
Correction, Nov. 9:
An earlier version of this story misstated the greenhouse gas in the inhalers; it is hydrofluoroalkane, not methane.
Worth mentioning that inhalers used to use CFCs, but those were banned. They then switched to hydrofluoralkane. Switching to another option may take up to a decade to find an acceptable solution and perform clinical trials.
With the propaganda messaging in this bungled report, Time Magazine qualifies as a fake news propaganda web site and at best is a yellow journalism mill. This is garbage reporting. When seen in the context of having no impact on climate, this original BMJ paper should not have been turned into a general news report. Time made up an exaggerated interpretation and did this for yellow journalism click bait.
Time is a junk news site masquerading as journalism and will no longer be viewed as a credible source for factual news.
How to Do Climate Communications
As I previously wrote
The Nature Conservancy should focus on facts of atmospheric CO2 levels rising, land and sea surface temperature anomalies, ice pack changes, ocean Ph and sea level change (IPCC Synthesis Report, Figure SPM.1) – as reported by reputable scientific bodies, but they did not. Instead they went straight for hyperbole and making untrue claims to promote fear and hysteria.
or
Stick with the facts of CO2 rising, sea level ice and temperature changes, ice mass changes or risk tuning all of us out. Shrill terminology designed to create emotional outrage and responses is a total turn off.
and
The facts are sufficient. The impacts of untrue propaganda hysteria, on the other hand, are to turn off the target completely. We have learned nothing from the parable of the boy who repeatedly cried Wolf!
The propaganda messaging methods in use are leading to public opinions that are not based in facts, logic or evidence. This risks the potential for major backlash against taking action to reduce CO2-equivalent effects on climate.
I have lost all trust in the media’s reporting on climate change. I’ll stick with science papers and IPCC reports, and blogs from selected scientists and researchers.
Letter sent to Time Magazine reporter/editor:
Jeffrey,
The title to this story is not true and the attempt at a clever word play about “asthma” and “choking” is insensitive.
The original title for this story was “How Asthma Inhalers are Contributing to Climate Change” (as it was saved in my browser) – Why the change to the rude headline mocking asthmatics? This is appalling on the part of Time Magazine.
Headline is False
Second, the headline is false. Asthma inhalers are not “choking the planet” and are physically incapable of doing so.
Per the BMJ paper, inhalers are estimated to release 22 to 79 pounds of CO2 equivalent GHGs per inhaler[1]
Put an inhaler’s CO2 footprint in context by comparing to the typical American household estimated to produce up to 40,000 pounds of CO2 per year from all sources. I used the carbon calculator provided by The Nature Conservancy and came up with a first pass estimate for my neighborhood of 34,000 pounds per year. (Because we use 1/3d the average electricity, and soon to be zero as solar PV is installed by the end of this month, the actual usage for our home and life is considerably less than this.)
When an inhaler represents 22 to 79 pounds CO2 equivalent, this must be put in the context of the average US home yielding 40,000 pounds of CO2 per year. For someone using an inhaler every single day, this is well under 1%. Why are we wasting time on such a tiny fraction?
There is simply no physical way that “Asthma inhalers are choking the planet”. None. If we removed all inhalers tomorrow, there would be zero measurable impact on weather or climate. None. Zero.
Lack of Pricing Data
Third, your report provides no U.S. pricing data. At the age of 60 I was diagnosed with exercise induced asthma (2 months ago). I went jogging one day and found myself unable to get sufficient air in to my lungs. Very scary – had never happened before (I since learned its genetic and my Mom and two older brothers dealt with asthma for decades). My doctor prescribed an HFA inhaler. I pay 100% of the costs of prescriptions, out of pocket.
When I priced dry powder inhalers on GoodRx, their price quotes were 10x to 15x higher than the HFA inhaler. If these price quotes are legitimate (such as $250 per inhaler), I would obviously not be using an inhaler and I and others would end up putting lives at risk – for no measurable impact on climate.
Climate Shaming Asthmatics
Healthy people climate shaming asthmatics is not an effective strategy for climate communications. Instead, it is an effective way to destroy any support for reducing carbon emissions. I am serious.
In the context of minuscule carbon footprint of inhalers compared to the typical household, this rudely titled story should never have been published.
At the very least, change the headline to stop mocking asthmatics with crude middle school humor.
Edward Mitchell, M.S. (engineering), M.B.A.
Notes
[1] At the end of the BMJ paper they note that half the inhalers turned into recycling centers are half full, due in part to lack of dosage meters and people replacing them prematurely. Burning the content destroys the methane’s green house gas effect. Which implies we can cut those CO2 equivalent pound estimates in half just by recycling. [Correction – by 25%]
Climate communications: Time Magazine changes headline three times, uses false headline “How Asthma Inhalers are Choking the Planet” was originally published on SocialPanic
0 notes
Last Seen Blogs

animeboston
Anime Boston

tudatosiras
Untitled

eldritch-nightmare
love from the wicked.

gayafuser
Gay Shit Can Be Found Here.

revizionbeatz
RevizionBeatz