#cw: medical abuse
Text
Changeling!Tim’s childhood is... actually kinda horrifying, when anyone looks into it.
(CW for forced medical procedures, and abuse in the form of temporary imprisonment. Also, minor self-harm, and… I don’t know what you call “eating something that will make you sick so your parents don’t get mad at you,” but I know it ain’t good.)
Tim had pretty pronounced fangs when he was younger, which his parents were just planning to wait out... until he was fast coming up on 10 and it was clear Tim wasn’t going to lose his teeth. A quick x-ray proved that Tim didn’t have adult teeth to grow in, just the one set he came with, and the fangs were only getting more obvious. His parents found an orthodontist willing to yank the fangs & wire up the rest of Tim’s teeth with braces to force them to look smooth & even as he grew up. (The doctor kept the teeth as a curiosity, and a decade later Damian will track that doctor down to steal them back.)
Something even Tim didn’t realize until he had to undergo a full Justice League-grade medical exam in preparation for becoming Robin, is that the tiny points on his ears aren’t natural. They have no idea what the ears of the baby Jack & Janet received looked like, but Tim’s points are actually mostly scar tissue. (Bruce puts it down as “a cosmetic procedure not dissimilar to ear cropping in canines” and tries not to feel sick.)
(There was also a period where the Drakes did an awful lot of research into cosmetic eye surgeries, but they eventually gave up. Apparently, it was a bigger concern that their son might end up blinded than that his eyes glowed in the dark and/or were the wrong color.)
As I mentioned before, Tim’s parents trim his thorns so that nobody goes to ruffle Tim’s hair and realizes he’s not human. He... actually started doing it himself when he decided to become Robin, because Tim has seen Bruce ruffle Jason & Dick’s hair so many times and didn’t want to hurt Bruce (or experience the absolute agony of having a thorn get caught in Bruce’s gloves and end up ripped out of Tim’s scalp,) as well as not wanting to give away Tim’s own inhuman nature with the single most obvious trait he has. (When the rest of the family find out, they are horrified and insist that Tim stop doing that. Instead of hair-ruffles, Tim gets hair-strokes that go only in one direction, bumping harmlessly over the curved outer edges of his thorns; it’s actually very soothing for both parties. Everyone absolutely uses Tim’s thorns as a stim toy, as long as Tim’s okay with it.)
Tim’s parents also hire an in-house barber to cut Tim’s hair, so they can make sure it’s “properly disposed of.” (Tim’s nightmares always smell faintly of burning hair.)
Tim wears fancy dress gloves to all dinners, because with the uppercrust you never know if someone’s going to bring out the real silverware. (If someone tells him to take off the gloves or Tim’s skin happens to brush up against somebody’s jewelry, Tim just sorta has to... deal. It’s rude to rush out or refuse your hosts, after all.)
(Fortunately, Dick and the Titans all prefer reusable plastic silverware. And as soon as any Bat finds out about Tim’s fae nature, Wayne Manor quickly switches to stainless steel.)
It’s nearly impossible to know if a meal was prepared with iodized salt or non-iodized salt until it’s already in Tim’s mouth and the burning-itching discomfort of coming in contact with an anti-fae substance begins. It’s rude not to at least try the food someone offers you, and it’s even ruder to just spit something out, especially out in public. At least Tim doesn’t usually have to fake it when he says he’s not feeling well in order to stop eating. (Tim doesn’t tell the Waynes about this until that medical exam, where he kinda jokes about being allergic to salt and someone’s like, “Wait, how do you eat? Everything has salt in it nowadays.” Alfred rather forlornly puts his sea salt up on the top shelf and buys a jar of iodized table salt on the next grocery run.)
Tim’s blood is immediately identifiable because it has chloroplasts in it. No, he’s not actually a plant; yes, he can perform limited photosynthesis. No, Tim was not aware of this about himself, he’s never been allowed to give blood before, and like??? Sure, he figured out he was a changeling, but that does not immediately translate to, “Oh, I should test my blood for plant cells!”
Tim’s room doesn’t look any different from any other boy his age... except for three nails over the door on the outside. For the iron horseshoe Tim’s parents hang there sometimes, when they don’t want him to bother them or when he’s grounded. (Thankfully, it's been very rare for Tim to actually be trapped in his room, as setting up a salt line on his windowsills has always been... well, he's not sure. A step too far, even for his parents? A step too many to remember and/or perform in the heat of the moment? Something they don’t even realize is necessary, assuming the horseshoe prevents Tim from leaving the room at all rather than simply crossing that one threshold? Tim doesn’t like to think about it. Tim typically stays in his room anyway when he feels the swooping nausea of it hanging over his door, if only so his parents don’t find him missing and decide sealing the windows is something they ought to be doing. Trapped not by any law or binding ritual, but by Tim’s own admittedly rare fear of consequences.)
(After Tim is snatched by faerie hunters, Jason and Dick are the ones who search Tim’s house. There’s a moment of silence when they find the horseshoe and realize what the nails are for. “I really hope I don’t have to point this out,” Jason says, in the tone of someone who’s going to do it anyway, “but it’s never a good sign when a kid’s bedroom has a lock on the outside.”)
#Tim's parents are bad in this one. Sorry. (I do like when they're complicated & nuanced and genuinely care about him but that's not this AU)#cw: abuse#cw: medical abuse#urban fantasy batfamily#urban fantasy au#fae tim drake#changeling tim drake#faerie tim drake#magic tim drake#magic batfam#magic batfamily#magic!batfam#magic!batfamily#magical batfam#magical batfamily#magical!batfam#magical!batfamily#tim drake#timothy drake#robin tim drake#prerobin tim drake#robin!tim#my writing#mine#//#Also#yes it’s ear CROPPING not ear DOCKING. I triple-checked.
84 notes
·
View notes
Text
I cannot begin to think about the... Everything that happened in this entry. It's either the death of the sparrows, Seward's unethical ramblings about how the future of science is maybe in his hands, or what could possibly come next.
Or the extreme disregard for Renfield's well being, and health after he completed his experiment. An experiment that shouldn't have happened because this old man's caretaker is far too interested in how he conducts a façade of madness that ends up worsening the mental problems that he already had.
Even if Renfield ate all of the sparrows, and even if I'm sad for the little creatures, what he goes through after he eats them is bad enough.
"The attendant has just been to me to say that Renfield has been very sick and has disgorged a whole lot of feathers." - Jack Seward, july 20.
"Oh yeah doctor that old patient that you have obssesing about for the last few weeks? Yeah he puked a bunch of dead birds, and is now sick." Is Seward going to do something about that, or is he just going to send a cleaning worker to clean up the mess? I don't know, and neither the text answers that. However, I really don't like the possible subtextual comment of Seward not helping Renfield with his physical illness.
And then this:
"I gave Renfield a strong opiate to-night, enough to make even him sleep, and took away his pocket-book to look at it." - Jack Seward, july 20.
The disregard, and violation of Renfield's privacy for "science" was sick. This old man has been coughing up feathers, and dead bird remains for almost an entire day, and the only thing that apparently matters is what is written in a diary. To the point of druggging Renfield without even checking if he was at least less sick than before.
Is Renfield now a patient in only name Seward? Is his well being an after thought to your ramblings about science? How the cage holds the man, and even if he tries to get free from the walls with his mind, at the end of the day there is no escape.
#This entry is too much#How did I not notice how bad it was last year?????#dracula daily#dracula#renfield#r.m. renfield#jack seward#cw: medical abuse
41 notes
·
View notes
Text
WiP Wednesday - The Research Hall
“I- I am sorry.” The patient on the bed speaks, their voice higher, more feminine than the last she passed. “I’m, you see, better now. I won’t do it again, I promise. I promise!”
Catra stood frozen over their bed, sword shaking in her hand as she stared down at their emaciated, mangled body.
“And I could send you there, you know.” Shadow Weaver was drunk but at least tonight she was a happy drunk, for what little that was worth. “You think you have a difficult life now? Ha! You’d be strapped down tight to your bed up there, stewing in your own filth as they take and take or give and give. And- and! Eventually you’d end up like the rest too.”
Catra clenched her jaw as she pulled uselessly at the thick leather straps keeping her on Weaver’s table out of nervousness. It wasn’t difficult for her to imagine the life of a patient. No. Not anymore.
Shadow Weaver pitched her voice into a pathetic, mewling imitation that Catra flushed with shame to hear. Her own cadence and voice thrown back in her face. “Oh Lady Weaver, OH Lady Weaver! Please, help me, Lady Weaver! Ha! HA! Wouldn’t that be a sight, hmm? I might even go back to watch you squirm, child.”
She dissolved into giggles as if it was the silliest, funniest joke she could conceive.
Catra’s fingers felt numb with cold at the thought.
She had assumed it was exaggerated in some way. Minister Weaver always told a version of the truth, but rarely was she honest. What else had she promised that Catra would find to ring true?
“I am so very sorry,” the patient gasped and writhed, kicking their feet just enough to squish through the remains of their own excrement. “I’m guilty, I know it, but I- I’m better now! You can see it for yourself, I’m much better now. I won’t do it again, I p-promise, L-lady Wea-”
Catra gasped for air, choking on the ammonia and rot and decay as she stared at the pulsing head below her. Her sword sunk to the hilt into the patient’s throat cut off their words, but their skin still pulsated. A soft sloshing sound back and forth, back and forth, back and forth.
6 notes
·
View notes
Text
I don’t think Victor actually saw patients at the Sinclair’s home during his time as a doctor.
I think all the medical equipment we saw only came later, when Trudy was very sick, with Victor investing in some last ditch off the book medical experiments to try and save her.
And when I say “save her”--there’s actually three versions of how that could be interpreted:
1) Victor kept attempting medical solutions long past when other doctors would have just said “all we can do is make her comfortable,” partially out of co-dependency and largely out of professional pride--and probably greatly to the detriment of his wife’s quality of life in those last few months.
2) Trudy was not actually in immediate danger of dying due to the tumor, rather that it just altered her personality so drastically (delusions, outburst of violent rages, ongoing disorientation, even possible neurological affects that caused her to loose partial use of her hands or vision--thus requiring her be physically cared for) that he decided to “fix her”/”bring back” the woman he loved--in a manner involving deeply unethical and likely unnecessary medical treatments.
(This is the interpretation I tend to gravitate to personally--because I think it most reflects how Victor and Trudy saw the world, as extrapolated by their handling of Bo: utilizing any method available--no matter how extreme or unethical or abusive--they thought would make a person behave “the right way.”)
3) The darkest timeline: Trudy never had a tumor. She simply had a severe mental/personality disorder Victor grew tired of dealing with and he decided to try and “fix her.”
(I personally find this a little too extreme for my taste, but it would be in-line with HoW’s schlocky over the top melodrama.)
Regardless of how it went down:
I personally headcanon that at the end--whether due to affects of Victor’s medical experiments or him simply being unable to stop growth of the tumor--Trudy was largely gone mentally, nearly reduced to catatonia, but still very much alive. Possibly--though possibly not, depending on how you want to spin it--with months or even years ahead of her.
I think Victor killed himself partially out of shame and largely out of not wanting to deal with the reality of the situation.
He didn’t want to be left the single father of three high-needs teenagers, while forced to care for his now disabled wife, who he now viewed as nothing more than a testament of his professional and personal failures.
So he killed himself, and left his kids to deal with the fallout.
And this is all a very long way of sharing this final headcanon:
I don’t think Trudy simply passed away on her own.
I think Vincent euthanized her.
Now--as I said above, I personally like to believe Trudy really did have a tumor and I think it’s clear that Vincent genuinely loved his mother. So, I don’t think this would have been his go too option right out of the gate--I think he would have tried to carrying on care for her on his own for several months. Eventually, however, I think it would quickly wear him down to the point he could no longer continue doing so.
And at that point--after all the behavior that had been modeled for him, with the emphasis that you never revealed “family matters” to outside people and the glaring fact that Bo was likely actively beginning to kill people at this point--I think he would have seen euthanizing her as the only option available to him, and likely the kindest thing to do, in his mind.
I think he also never told Bo what he did.
(For many complicated reasons.)
At the end of the day, I think Trudy’s death is the one death Vincent has caused that he harbors real guilt over.
#vincent sinclair#trudy sinclair#victor sinclair#House of Wax#cw: abelism#cw: suicide#cw: medical abuse#cw: assisted suicide
17 notes
·
View notes
Text
Man. Speaking of cancer trauma. I really was a cancer patient for 6 fucking years. And only 6 years because when they couldn't immediately find the tumor with like 1 CT and some scopes in year 1, they just stopped looking, no matter how much i begged, and just kept on giving me iron infusions and blood transfusions to treat the severe anemia the cancer attached to the outside of my small intestine (where scopes couldn't see it) caused, telling me for years I just didn't make my own blood. This doctor telling me this was a hemotologist (blood) oncologist (cancer) specialist. He just... refused to look for cancer.
Once someone actually LOOKED for cancer last year (so 6 years in) they found it and completely removed it within like 48 hours of me showing up to the ER (of a different system entirely) with a hemoglobin of 4.
I get that in year 1 the tumor was too small to be easily found by a CT scan, i guess. And i get it was on the outside wall amd thus all the cameras shoved through my system top to bottom bottom to top were never going to find it. But i just feel like. It was a lot of effort for a year. And then they just fucking gave up, told me my blood making machine was broken, and asked if I had tried weight loss about it.
Something Something fat female presenting patients not being taken seriously.
#cw: medical trauma#cw: medical abuse#cw: medical neglect#got a whole new crew of followers so y'all don't know the Max lore#so i guess i should tag and warn y'all there is medical abuse found within these walls
25 notes
·
View notes
Text
All About: Schizophrenia
[Note: If you have schizophrenia/are schizophrenic (not sure if the community prefers person-first or identity-first language, so I’m giving y’all both), please feel free to chime in with corrections or additions in the comments. I don’t know what I don’t know, but I’m always willing to learn.]
Pathology = Study of Disease
Pathology addresses the following components of disease:
cause/etiology
mechanisms of development (pathogenesis)
structural alterations of cells, tissues, and organs
functional alterations of cells, tissues, and organs (pathophysiology)
the consequences of those changes (clinical symptoms)
Characteristics
The most typical feature of schizophrenia is psychosis:
severe distortions of reality and perception
disturbances in intellectual function, affect, motivation, social relationships, and motor behavior
relapsing episodes
- This can be so incapacitating that voluntary or involuntary hospitalization is required.
Classification of Mental Disorders in the DSM-5
Psychiatric disorders are listed in the DSM = Diagnostic and Statistical Manual of Mental Disorders.
- published by the American Psychiatric Association (APA)
- currently on 5th edition (2013)
1.2 Section II: diagnostic criteria and codes
- 1.2.1 Neurodevelopmental disorders
- 1.2.2 Schizophrenia spectrum and other psychotic disorders
- 1.2.3 Bipolar and related disorders
- 1.2.4 Depressive disorders
- 1.2.5 Anxiety disorders
- 1.2.6 Obsessive-compulsive and related disorders
- 1.2.7 Trauma- and stressor-related disorders
- 1.2.8 Dissociative disorders
- 1.2.9 Somatic symptom and related disorders
- 1.2.10 Feeding & eating disorders
- 1.2.11 Sleep-wake disorders
- 1.2.12 Sexual dysfunctions
- 1.2.13 Gender dysphoria
- 1.2.14 Disruptive, impulse-control, and conduct disorders
- 1.2.15 Substance-related and addictive disorders
- 1.2.16 Neurocognitive disorders
- 1.2.17 Paraphilic disorders
- 1.2.18 Personality disorders
Diagnosis
Criterion A: Characteristic Symptoms
- Two or more of the following, each present for a significant portion of time during a 1-month period (or less if successfully treated). At least one of these should include symptoms 1-3 (positive symptoms).
Delusions
Hallucinations
Disorganized speech
Disorganized or catatonic behavior
Negative symptoms (e.g. blunted emotions)
Cognitive deficits
Criterion B: Social/Occupational Dysfunction
Criterion C: Duration of Six Months or More
Criterion D: Schizoaffective and Mood Disorder Exclusion
Criterion E: Substance/General Mood Condition Exclusion
Criterion F: Relationship to Global Development Delay or Autism Spectrum Disorder
[Note: If you’ve been misdiagnosed with schizophrenia when you were actually dealing with schizoaffective disorder, autism, substance use, a mood disorder, etc., please feel free to share your experience in the comments.]
Delusion: a belief that is held with strong conviction, despite superior evidence to the contrary.
- Karl Jaspers (1913) established three main criteria for a belief to be considered delusional:
certainty (held with absolute conviction)
incorrigibility (not changeable by compelling counter-argument or proof to the contrary)
impossibility or falsity of content (implausible, bizarre, or patently untrue)
- Examples:
Delusion of persecution involving the individual’s belief that others are spying on or planning to harm them
Delusions that thoughts are imposed from an outside source, such as outer space
Hallucinations: pathological forms of perception.
- Auditory hallucinations are frequent and are usually voices that are insulting or commanding.
- Visual hallucinations are rarer (in catatonic schizophrenia). More typical with epilepsy or hallucinogen use.
- Gustatory, olfactory, and somatic sensations also occur [note: I don’t have stats on the frequency of these; please share them if you got ‘em.]
Disorganized Speech
- sometimes called “word salad”
- frequent change of conversation topics with no connection between sentences
- speech can follow grammatical rules, but content makes little sense

Disorganized or Catatonic Behavior
- Motor activity is reduced and characterized by inappropriate and bizarre postures, rigidity, or “purposeless” and stereotyped movements (e.g. rocking or pacing).
- At times, people with schizophrenia (particularly the paranoid type) can become agitated and/or violent.
Catatonia: motor immobility and behavioral abnormality manifested by stupor.
- Stupor = lack of critical cognitive function and a level of consciousness wherein the person is almost entirely unresponsive and only responds to base stimuli such as pain.
Negative Symptoms
Blunted emotions = emotions may be absent or totally inappropriate to the situation. Sudden and unpredictable changes of emotion are also common.
Inability to experience pleasure
Social withdrawal
Lack of eye contact
Lack of motivation
Poverty of speech
Cognitive Deficits
Schizophrenia is classified as a thought disorder, characterized by illogical thinking, lack of reasoning, and inability to recognize reality.
Cognitive symptoms include impaired working memory, executive functioning, and attention. Many cognitive deficits impair the ability to function at school, at work, etc.
Onset of Schizophrenia
- Symptoms most often begin during the late teenage years and early twenties, but there are gender differences. After age 36, more women than men experience their first episode.

Etiology of Schizophrenia
- Although schizophrenia was described as early as 1000 BC, its causes remain unknown.
- It is increasingly regarded as a neurodevelopmental disorder with a strong genetic component.
Importance of genetics is shown by many family, twin, and adoption studies.
Other factors must be involved as well; we’re still figuring those out.

Lifetime risks of developing schizophrenia among relatives of an affected individual
Events during perinatal brain development can contribute to the occurrence of schizophrenia.
- These complications include:
brain injury during pregnancy or delivery caused by oxygen deprivation
drug use
exposure to viral infection (ex. measles) in the 2nd trimester
endocrine disorders
severe malnutrition
- During adolescence, a period of significant brain development, excessive synaptic pruning can result in loss of cortical gray matter.
- Cannabis use during adolescence might increase the risk.

Neurobiology of Schizophrenia: Structural Changes
- Recent advances in technology have revealed abnormalities of brain structure and function in individuals with schizophrenia.
- Many studies show cerebral atrophy and enlargement of fluid-filled ventricles following cell loss.

Brain Imaging & Mental Disorders
- Brain imaging techniques are currently not used to diagnose mental disorders.
- Imaging is currently used for research purposes and is helping to identify the brain regions involved in different pathologies.
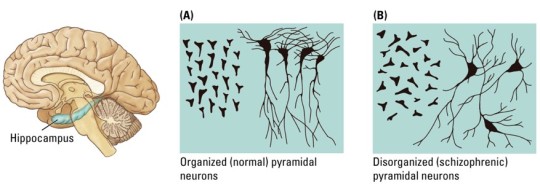
- Numerous studies show that hippocampal cells of patients with schizophrenia are more disorganized than those of healthy subjects.
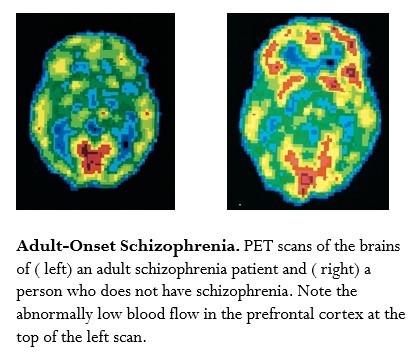
Neurobiology of Schizophrenia: Functional Changes
- Brain functional changes include reduced function of the prefrontal cortex (PFC), called hypofrontality.
- Reduced blood flow is associated with less glucose use, which indicates how active the brain cells are.
- Imaging studies show less blood flow to the frontal cortex when people with schizophrenia are performing cognitive tasks, such as the Wisconsin Card Sorting Test (WCST).


Neurobiology of Auditory Hallucinations
- Reduced gray matter volume in the temporal lobe
- Impaired processing in a prefrontal and temporal lobe neuronal network, due to hyper-activation of temporal lobe regions, including the auditory cortex, which is not inhibited due to impairment of prefrontal executive inhibitory functions.

Neurobiology of Schizophrenia: Functional Changes
- Eye-movement dysfunctions such as inability to visually track an object.
- Failure to track is also common in relatives of schizophrenic patients. The defective eye-tracking gene may be inherited along with the genes for schizophrenia.
The dopamine hypothesis = excess DA function results in positive symptoms of schizophrenia.
- It was suggested by the fact that amphetamine (which increases dopamine) can produce a psychotic reaction in healthy individuals, which can be reversed by DA antagonists.
- There is a strong correlation between D2 receptor blockade and reduction of schizophrenic symptoms.
DA imbalance hypothesis:
reduced DA function in mesocortical neurons (negative symptoms and impaired thinking) = D1 receptors
excess DA function in mesolimbic neurons (positive symptoms) = D2 receptors

Hypoglutamate hypothesis:
- Blocking NMDA receptors with PCP or ketamine produces schizophrenia-like symptoms in healthy individuals and exacerbates symptoms in schizophrenic patients.
- PCP and ketamine produce both the positive and negative symptoms.
- Antipsychotic drug clozapine interacts with the glutamate receptor and increases glutamate levels in the PFC of rats.

Schizophrenia: Treatments
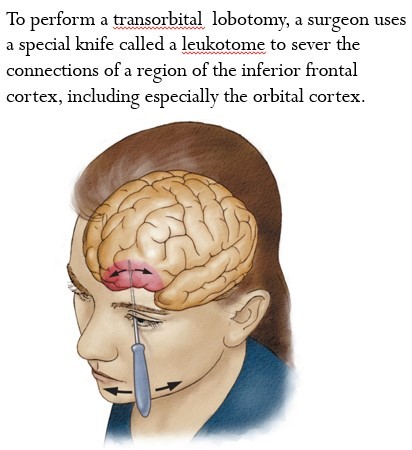
- Before drug therapy, patients were confined to mental hospitals where treatment was limited to isolation or restraint, “shock” therapy using insulin-induced seizures or electrical currents, and surgery such as prefrontal lobotomy.

Lobotomy: consists of cutting the connections to and from the prefrontal cortex.
- controversial procedure accompanied by frequent and serious side effects
- was used to treat psychiatric (and occasionally other) conditions from 1935 till mid-1950s [note: gay men and lesbians were subjected to lobotomies in an attempt to “cure” them during this time period.]
- The dramatic decrease in the number of resident patients in state and municipal mental hospitals in the United States began after 1955, when psychoactive drugs were introduced into widespread therapeutic use.

Anti-psychotic Drugs
Neuroleptics = older term for anti-psychotic drugs
- Typical anti-psychotics: have motor side effects (ex. Chlorpromazine, Haloperidol)
- Atypical anti-psychotics (2nd generation): fewer side effects (ex. Clozapine, Risperidone)
- Effectiveness of these drugs has been demonstrated hundreds of times, especially for positive symptoms.
- Negative and cognitive symptoms are more resistant to treatment.
- The law of thirds = 1/3 of patients respond well to treatment, 1/3 shows significant improvements but is vulnerable to relapse, and 1/3 fails to respond.

After initial recovery, anti-psychotic drugs are prescribed as maintenance therapy to prevent relapse.
- Unpleasant side effects cause many patients to stop treatment.
- Psychotherapy and group therapy are important additions to drug therapy.
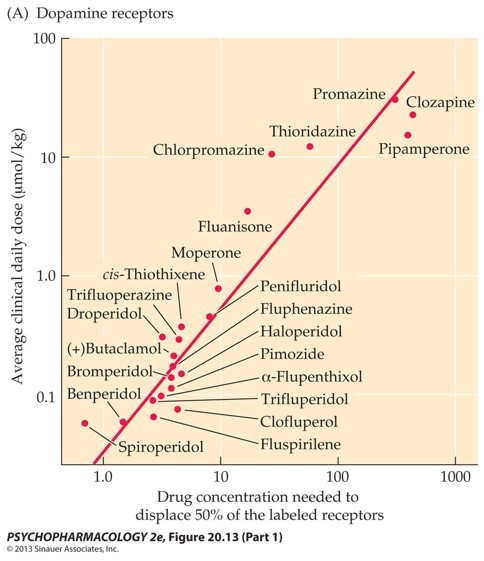
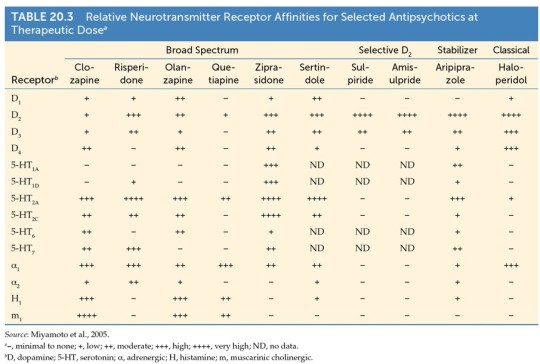
Anti-psychotic drugs block D2 receptors.
- A strong correlation exists between ability of a drug to displace a radio-labeled ligand on DA receptors and average clinical daily dose required.
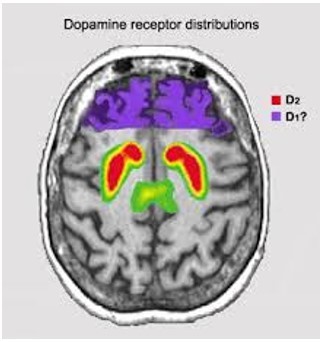
- D2 receptors are located in the basal ganglia, nucleus accumbens, amygdala, hippocampus, and less in the cerebral cortex.
PET images show replacement of radio-labels on striatal D2 receptors by different anti-psychotic drugs.
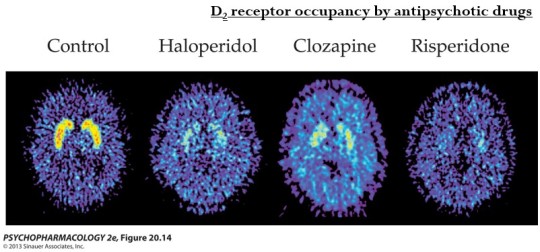
The drugs also bind to other receptors, but there is no clear relationship between clinical effectiveness and binding to serotonin, adrenergic, histamine, or D1 receptors.

Anti-psychotics: Side Effects
Side effects depend on which receptor the drug binds to.
- Dopamine pathways in the brain are important for understanding drug action:
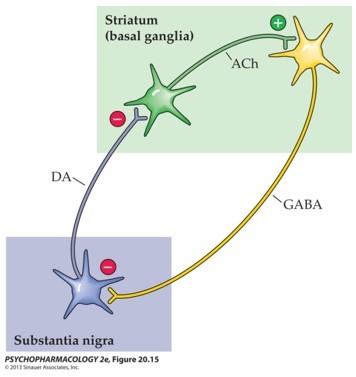
Nigrostriatal pathway (Substantia nigra ---> Striatum): Motor side effects
Hypothalamus ---> Pituitary gland pathway (regulates pituitary hormone secretion): Hormonal side effects
Parkinsonism: motor side effects that resemble symptoms of Parkinson’s disease:
tremors
akinesia (slowing or loss of voluntary movement)
muscle rigidity
restlessness (inability to sit still)
loss of facial expressions
- Parkinson’s is caused by loss of cell bodies in the substantia nigra, which gives rise to the nigrostriatal pathway.
- Lack of DA function in the striatum causes the motor effects.
Tardive dyskinesia (TD) is characterized by stereotyped involuntary movements, particularly of the face and jaw, quick and uncontrolled movements of the arms and legs, and other motor effects.
- Incidence of TD increases with duration of treatment.

Woman with tardive dyskinesia (TD)
- Neuroendocrine effects:
decreased sex drive
no menstruation
increased prolactin release
inhibition of growth hormone release
- Metabolic effects (typically significant weight gain)
- Inability to regulate body temperature
Neuroleptic malignant syndrome (NMS) is serious and life-threatening.
- characterized by fever, rigidity, altered consciousness, and autonomic nervous system inability (including rapid heart rate and fluctuations in blood pressure)
- Rapid diagnosis and immediate action have significantly reduced mortality risk.
Other side effects of anti-psychotics:
Blocking cholinergic synapses produces dry mouth, blurred vision, difficulty in urination, GI problems
Anti-adrenergic action leads to dizziness or blacking out
Many drugs also cause sedation
Anti-psychotics: Dependence
Anti-psychotic drugs causes little or no tolerance, physical dependence, or abuse potential, and have high therapeutic index.
- Lack of abstinence syndrome may be due to long half-life:
Haloperidol (20 hours)
Olanzapine (30 hours)
Aripiprazole (75 hours)
Atypical Anti-psychotics
“Atypical” or “second-generation” drugs reduce positive symptoms of schizophrenia as well as classical drugs, but without significant motor side effects.
- Some new drugs do not produce TD or increase prolactin secretion.
- Three types:
Selective D2 receptor antagonists
Dopamine system stabilizers
Broad-spectrum anti-psychotics
Dopamine system stabilizers:
Partial DA agonists compete with DA for receptors and reduce DA effect (ex. aripiprazole, trade name: Abilify)
Has few side effects
Little evidence of cardio-toxicity, weight gain, or motor side effects
Adverse effects such as headache, agitation, insomnia, and nervousness are minor.
Broad-spectrum anti-psychotics block other receptor types in addition of D2 receptors (ex. Clozapine, risperidone)
- Clozapine has weak affinities for D1 and D2 and strong affinities for serotonergic, muscarinic, histaminergic, and D4 receptors.
- It is more effective for patients who do not respond to total anti-psychotics.
- Clozapine has fewer motor side effects. However, it does have many other side effects because of its action on multiple receptors, including:
weight gain
sedation
agranulocytosis (a rare blood disorder that severely reduces number of white blood cells)
cardiac toxicity
- Clinical trials in the UK found that clozapine was superior to the other anti-psychotics in the treatment of negative symptoms.
- Clozapine can improve cognitive symptoms.
appears to be the only true “atypical” anti-psychotic, because no other 1st or 2nd generation anti-psychotics have this positive effect
The Search for a New Drug: Possible Approaches
(1) Enhance Acetylcholine: Clozapine is the only drug currently in use that enhances cognition. It does this by increasing acetylcholine release in the hippocampus.
(2) Selectively enhance D1 receptor signaling in PFC with D1 agonists.
Hypofrontality is associated with reduced DA function in PFC, especially at D1 receptors.
(3) Enhancing glutamate activity at NMDA receptors might reverse negative and cognitive symptoms.
Blocking NMDA receptors by ketamine can induce psychosis, cognitive deficit. So maybe stimulating NMDA receptors can have the opposite effect.

#drugs and behavior#Neuroscience#my notes#study blog#schizophrenia#cw: medical torture#cw: medical abuse#cw: homophobia
7 notes
·
View notes
Text
I found out a man in my friends list who had an experience very similar to mine committed suicide while I was inpatient, two years ago. I think it was the exact day I entered the hospital. He had been institutionalised because he was paranoid, instead of curing him they only made him more insane and came out of the mental health facility utterly traumatised, on top of his paranoia. After 9 years he still had not recovered. They ruined him mentally and physically. Just like they did with me.
2 notes
·
View notes
Text
Sleep Paralysis, Part 4
I was mostly above my body as the doctors operated. They argued back and forth even as my jugular was stitched back together.
I watched through a fog of disbelief. How do you fuck up this badly?
"Any improvement?" The last stitch was tied off.
"Still dropping."
"Fuck, what could be-? Start a blood transfusion."
The incompetent doctor did as asked, as well as an injection into the IV.
Then, flatline.
It felt like reality dropped out from underneath me.
"Anaphylactic shock-"
"Why should I believe you?! You already did an unnecessary tracheotomy!"
Throughout all of this, I decided it could only be intentional. I was only supposed to come in for an x-ray, after all. Intentional disbelief, intentional incompetence, intentional malpractice, intentional abuse of power.
And whether or not I was right, it was still going to kill me.
Part 1 | Part 2 | Part 3 | Part 4
About this Series
#cw: body horror#cw: death#cw: gore#cw: blood#cw: hospitals#cw: hospital trauma#cw: medical abuse#body horror#death#gore#blood#hospitals#hospital trauma#abuse#medical abuse#sleep paralysis#sleep paralysis art#nightmares#artists on tumblr#horror art#dark art#and thus concludes the sleep paralysis series
0 notes
Text
i know us schizos can be relatively lax about the word schizo... but for people who aren't on the schizophrenia spectrum, please remember... it is a slur, or at the very least, a derogatory term. maybe don't say it (unless we're okay with you calling us it), especially not to separate yourselves from us.
context: i just saw someone say "i'm not a fucking schizo" when talking about their misdiagnosis and resulting trauma. this could have been done without using a slur, especially given how much we also face misdiagnosis and medical/psychiatric trauma. we're in this together, not apart.
#softspoonie#ableist language cw#ableism#sanism#schizophrenia#schizoaffective#schizotypal#schizoid#schizospec#schizophrenia spectrum#schizophrenic#mentally ill#medical trauma#neurodivergent#psychiatric abuse#misdiagnosis#psych survivor#survivor#trauma survivor#abuse survivor
575 notes
·
View notes
Text

life is wasted
#psychonauts#caligosto loboto#medical abuse cw#<-yeah i think.That covers it#nightmaretheater#so sorry if you were innocently checking my blog after the crowment and were blasted with this#i was going to do a bit of artistic censoring but.Nahhh#time on canvas : 6 hours#i had to watch some videos of a transorbital lobotomy being preformed for refference 😁#god forbid i had my photos app open and someone looked over my shoulder and saw several screenshots#also Yes thats text from berenice. I cant be stopped#ohhh im so hungry.Chili for dinner……#wait. i forgot my watermark#thats okay. Theyll know its me from the berenice quote /nsrs#also yeah the orbitoclast looks a bit small. its the angle. Trust me. Okay.#I dont know how to paint flowers . I….Kind of my first time.Sooorry#Sorry guys . Had to post Horrifiying Upsetting Art again. Will continue to happen#its kind of funny this barely looks like fanart#good. Cant wait for someone to stumble upon this and freak out when they realize it is indeed fanart#surprised this was. 6 hours? Looks down at my hands… Woah…#reminder: I am drawing on my phone i did not go to art school💞#Okay time to collapse . Im really hungry#sorry . Just had to give my artists commentary
184 notes
·
View notes
Note
Dr Sidhbh Gallagher almost killed your friend??? I thought she was beloved by the trans community and her patients???
I'll let Rylan speak for himself.
822 notes
·
View notes
Text
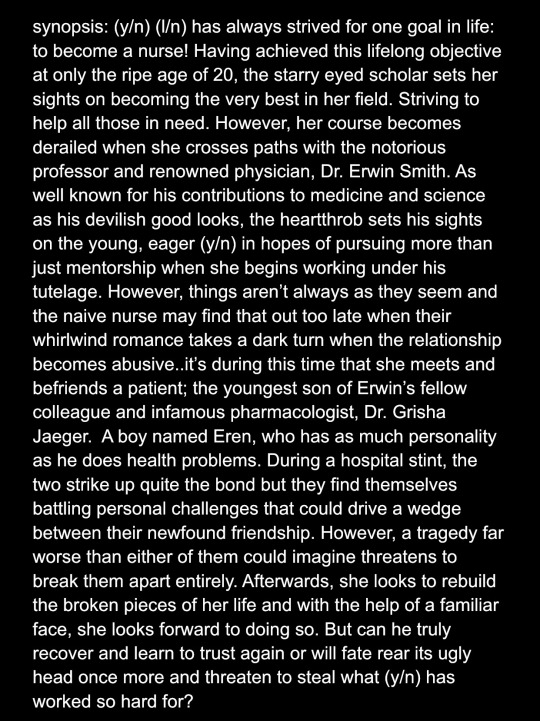
y’all gone jump me if I post this?
#cherry chats 🍒#aot x black reader#black fem reader#black reader#medical au#wip#current wip#wip excerpt#musician x influencer au#eren x black fem!reader#aot au#erwin smith#aot erwin#erwin x reader#aot angst#cw abuse#cw age gap#cw age difference#black fanfiction#eren x black reader#nurse au#this was my OG baby before reverb
136 notes
·
View notes
Text

They would have lost nothing in allowing this child to be treated. There was absolutely no reason to deny a request to help her. They did this willingly and without remorse.
God comfort her family.
139 notes
·
View notes
Text
long post about substance abuse and addiction
the thing about me is i was dependent on alcohol for a few years and refused to admit it to myself forever until one morning when something clicked and i stopped but for the past three years its been... difficult. like. i still have dreams where im drinking but justifying it to myself like "this one doesnt count". i hate them
but im sober!!! and thats amazing of me
the other thing about me is i was also smoking whenever i could for a few years but also stopped doing that because i recognised it was another unhealthy dependency and... yeah the dreams happen with that too. the buying a pack of cigarettes and being like well these dont count these are a treat or whatever
but i still dont!! and thats also good!!!!
a third thing about me is for a while i was reliant on self harm to process feelings and i stopped that over a decade ago now!!!! thats so amazing of me
but
the most important thing about me for the sake of this post is that throughout uni i also developed an addiction to painkillers and would take numerous different kinds in dosages way above the recommended numerous times a day and it took a life changing conversation with a best friend in a train station for me to realise how unhealthy it was and how it was affecting people who cared about me to see me basically destroying myself like that
and thats
still ongoing!! i havent drank i havent smoked but i have at numerous points relapsed into full painkiller addiction and it fucks me up and my family still think i went to the hospital for food poisoning this time in 2022 but in reality i had been regularly near fatally overdosing for weeks
and its not like i can cut them out entirely because. they are prescribed to me for chronic pain. like. theres this painful line between taking the right amount to function and... feeling like i have to take more because i cant function without them. its like having an addiction to fucking.... water. i need it to live but its so often hard to tell if thats a real thought or if i think i need way more than i actually do in order to live and i fucking drown because the metaphor is about water
and right now i feel like im on the edge of relapsing again!! recognisable feelings and behaviours are creeping in!! and i dont want that!!!!!!
so im just posting about it on the internet i guess? to get the thoughts out of my head? to vent? to hold myself accountabld by screaming into the void? to ask for advice or reassurance? for somebody to tell me gently but firmly not to take more meds than i should. i took my normal dosage today. taking more would be bad and i recognise that but. i dont know. i dont know if i can trust myself not to tonight without being directly told not to by somebody who cares
82 notes
·
View notes
Text
Folks
Gwyn's at the specialist
Tristan's Fetch and Tug Buddy carted her out of town so we could get her in sooner, try to figure this intermittent pain out, try to see why her bloodwork is Not Quite Right
and the specialist
thinks it's BEHAVIORAL.
🎉Behavioral🎉
Behavioral fake pain. Because it "shouldn't come and go."
She's a DOG.
This is her pain (the video I took as I was trying to determine where exactly it hurts, the pain is at her right side, last few ribs). Sound on.
257 notes
·
View notes
Text
Ironic that I woke up in the exact moment when the narrator of Lore was pronouncing a sentence along the lines of "The patients voluntarily admitted themselves, so what she was doing was not illegal", during what I recognised as an episode about the so-called Starvation Heights. I just couldn't wake up at any other moment.
Of course I immediately put on another episode.
0 notes
Last Seen Blogs

inklessletter
the negative space

catchpoof
ancient being

indecisivefuck64
Kira Worshipping Hoe

scholaryybr
Untitled

adnanlederwarenmanufacturer
Adnan Lederwaren Manufacturer