#meningitis outbreak
Text

Rachelle Lefevre in Under the dome (2013) Outbreak
S1E4
The military units outside the dome are packing up, much to the consternation of many of the townsfolk. There is a much greater problem however when Linda falls sick, the first of many as an outbreak of meningitis spreads across the town. Julia continues to have her doubts about Barbie and visits a site he had marked on his map. She finds her husband Peter's car at DJ Phil's trailer but he says her husband sold it to him. DJ tells her about the cabin and when Junior tells her about meeting Barbie at a cabin, she's desperate to get there but having fallen ill, has to get out of the hospital. Angie, still a prisoner in the bomb shelter, faces rising water after a pipe bursts. Norrie and Joe realize they have a seizure when they touch...
#Under the Dome#tv series#2013#Outbreak#S1E4#meningitis outbreak#Rachelle Lefevre#Julia Shumway#secrets#pipe bursts#seizure#pink stars#drama#mystery#scifi#face#red head#just watched
0 notes
Text
I have never screamed DEXAMETHASONE louder at my television than when Dr. Elizabeth Weir got turned into a partial replicator.
#that’s what they give during outbreaks of meningitis to help stop brain swelling#it doesn’t actually treat the infection though#just the swelling#tw: medical#tw: medicine#tw: medication#spoilers for stargate Atlantis#my wormhole#dr. Beckett deciding to give atropine to someone is also circumspect#I need to review that again to see if he’s correct
0 notes
Photo
“Lift Quarantine At Toronto Jail,” Windsor Star. February 6, 1942. Page 11.
----
TORONTO, Feb. 6. - Officials at Don jail announced yesterday that a quarantine placed on 15 prisoners several days ago is expected to be lifted Monday.
The quarantine was placed on the men several days ago after the discovery that a prisoner at the jail was suffering from spinal meningitis.
Among the men quarantined is Harvey Murphy, former leader of the Ontario Unemployed Federation, who was arrested under Defence of Canada Regulations.
#toronto#toronto jail#quarantine#lockdown#prison healthcare#spinal meningitis#outbreak#anti-pandemic acts#epidemic histories#defence of canada regulations#political prisoners#unemployed association#history of crime and punishment in canada#crime and punishment in canada#canada during world war 2
0 notes
Text
Just in case anyone thought we didn’t need to stay vigilant about Highly Pathogenic Avian Influenza, a bottle nose dolphin was recently found dead in Florida infected with the virus. The dolphin had serious inflammation of the brain and meninges, and it is believed to have become infected by contact with an infected aquatic bird species. This outbreak is about a lot more than birds.
#animals#HPAI#wildlife disease#wildlife#vetblr#cetaceans#biology#zoology#nature#epidemiology#highly pathogenic avian influenza#dolphins#animal death
269 notes
·
View notes
Text
In February, a dermatologist in New York City contacted the state’s health department about two female patients, ages 28 and 47, who were not related but suffered from the same troubling problem. They had ringworm, a scaly, crusty, disfiguring rash covering large portions of their bodies. Ringworm sounds like a parasite, but it is caused by a fungus—and in both cases, the fungus was a species that had never been recorded in the US. It was also severely drug-resistant, requiring treatment with several types of antifungals for weeks. There was no indication where the patients might have acquired the infections; the older woman had visited Bangladesh the previous summer, but the younger one, who was pregnant and hadn’t traveled, must have picked it up in the city.
That seemed alarming—but in one of the largest and most mobile cities on the planet, weird medical things happen. The state reported the cases to the Centers for Disease Control and Prevention, and the New York doctors and some CDC staff wrote up an account for the CDC’s weekly journal.
Then, in March, some of those same CDC investigators reported that a fungus they had been tracking—Candida auris, an extremely drug-resistant yeast that invades health care facilities and kills two-thirds of the people infected with it—had risen to more than 10,000 cases since it was identified in the US in 2016, tripling in just two years. In April, the Michigan Department of Health and Human Services rushed to investigate cases of a fungal infection called blastomycosis centered on a paper mill, an outbreak that would grow to 118 people, the largest ever recorded. And in May, US and Mexican health authorities jointly rang an alarm over cases of meningitis, caused by the fungus Fusarium solani, which seemed to have spread to more than 150 clinic patients via contaminated anesthesia products. By mid-August, 12 people had died.
All of those outbreaks are different: in size, in pathogen, in location, and the people they affected. But what links them is that they were all caused by fungi—and to the small cadre of researchers who keep track of such things, that is worrisome. The experts share a sense, supported by incomplete data but also backed by hunch, that serious fungal infections are occurring more frequently, affecting more people, and also are becoming harder to treat.
“We don’t have good surveillance for fungal infections,” admits Tom Chiller, an infectious disease physician and chief of the CDC’s mycotic diseases branch. “So it’s hard to give a fully data-driven answer. But the feeling is definitely that there is an increase.”
The question is: Why? There may be multiple answers. More people are living longer with chronic illnesses, and their impaired immune systems make them vulnerable. But the problem isn’t only that fungal illnesses are more frequent; it is also that new pathogens are emerging and existing ones are claiming new territory. When experts try to imagine what could exert such widespread influence, they land on the possibility that the problem is climate change.
Fungi live in the environment; they affect us when they encounter us, but for many, their original homes are vegetation, decaying plant matter, and dirt. “Speculative as it is, it's entirely possible that if you have an environmental organism with a very specific ecological niche, out there in the world, you only need a very small change in the surface temperature or the air temperature to alter its niche and allow it to proliferate,” says Neil Stone, a physician and fungal infections lead at University College London Hospitals. “And it's that plausibility, and the lack of any alternative explanation, which makes it believable as a hypothesis.”
For this argument, C. auris is the leading piece of evidence. The rogue yeast was first identified in 2009 in a single patient in Japan, but within just a few years, it bloomed on several continents. Genetic analyses showed the organism had not spread from one continent to others, but emerged simultaneously on each. It also behaved strikingly differently from most yeasts, gaining the abilities to pass from person to person and to thrive on cool inorganic surfaces such as plastic and metal—while collecting an array of resistance factors that protect it from almost all antifungal drugs.
Arturo Casadevall, a physician and chair of molecular microbiology and immunology at the Johns Hopkins Bloomberg School of Public Health, proposed more than a decade ago that the rise of mammals over dinosaurs was propelled by an inherent protection: Internally, we’re too hot. Most fungi flourish at 30 degrees Celsius or less, while our body temperature hovers between 36 and 37 degrees Celsius. (That’s from 96.8 to the familiar 98.6 degrees Fahrenheit.) So when an asteroid smashed into the Earth 65 million years ago, throwing up a cloud of pulverized vegetation and soil and the fungi those would have contained, the Earth’s dominant reptiles were vulnerable, but early mammals were not.
But Casadevall warned of a corollary possibility: If fungi increased their thermotolerance, learning to live at higher temperatures as the climate warms, mammals could lose that built-in protection—and he proposed that the weird success of C. auris might indicate it is the first fungal pathogen whose adaptation to warmth allowed it to find a new niche.
In the 14 years since it was first spotted, C. auris has invaded health care in dozens of countries. But in that time, other fungal infections have also surged. At the height of the Covid pandemic, India experienced tens of thousands of cases of mucormycosis, commonly called “black fungus,” which ate away at the faces and airways of people made vulnerable by having diabetes or taking steroids. In California, diagnosis of coccidioidomycosis (also called Valley fever) rose 800 percent between 2000 and 2018. And new species are affecting humans for the first time. In 2018, a team of researchers from the US and Canada identified four people, two from each country, who had been infected by a newly identified genus, Emergomyces. Two of the four died. (The fungus got its name because it is “emerging” into the human world.) Subsequently, a multinational team identified five species in that newly-named genus that are causing infections all over the world, most severely in Africa.
Fungi are on the move. Last April, a research group from the Washington University School of Medicine in St. Louis examined the expected geographic range in the US of what are usually called the “endemic fungi,” ones that flourish only within specific areas. Those are Valley fever in the dry Southwestern US; histoplasmosis in the damp Ohio River valley; and blastomycosis, with a range that stretched from the Great Lakes down the Mississippi to New Orleans, and as far east as the Virginia coast. Using Medicare data from more than 45 million seniors who sought health care between 2007 and 2016, the group discovered that the historically documented range of these fungi is wildly out of step with where they are actually causing infections now. Histoplasmosis, they found, had been diagnosed in at least one county in 94 percent of US states; blastomycosis, in 78 percent; and Valley fever in 69 percent.
That represents an extension of range so vast that it challenges the meaning of endemic—to the point that Patrick Mazi, an assistant professor of medicine and first author on the paper, urges clinicians to cease thinking of fungal infections as geographically determined, and focus on symptoms instead. “Let’s acknowledge that everything is dynamic and changing,” he says. “We should recognize that for the sake of our patients.”
Without taking detailed histories from those millions of patients, it can’t be proven where their infections originated. They could have been exposed within the fungi’s historic home ranges and then traveled; one analysis has correlated the occurrence of Valley fever in the upper Midwest with “snowbird” winter migration to the Southwest. But there is plenty of evidence for fungal pathogens moving to new areas, via animals and bats, and on winds and wildfire smoke as well.
However fungi are relocating, they appear to be adapting to their new homes, and changes in temperature and precipitation patterns may be part of that. Ten years ago, CDC and state investigators found people in eastern Washington state infected with Valley fever, and proved they had acquired it not while traveling, but locally—in a place long considered too cold and dry for that fungus to survive. A group based primarily at UC Berkeley has demonstrated that transmission of Valley fever in California is intimately linked to weather there—and that the growing pattern of extreme drought interrupted by erratic precipitation is increasing the disease’s spread. And other researchers have identified cases of a novel blastomycosis in Saskatchewan and Alberta, pushing the map of where that infection occurs further north and west.
The impact of climate change on complex phenomena is notoriously hard to prove—but researchers can now add some evidence to back up their intuition that fungi are adapting. In January, researchers at Duke University reported that when they raised the lab temperatures in which they were growing the pathogenic fungus Cryptococcus deneoformans—the cause of a quarter-million cases of meningitis each year—the fungus’s rate of mutation revved into overdrive. That activated mobile elements in the fungus’s genome, known as transposons, allowing them to move around within its DNA and affect how its genes are regulated. The rate of mutation was five times higher in fungi raised at human body temperature than at an incubator temperature of 30 degrees Celsius—and when the investigators infected mice with the transformed fungi, the rate of mutation sped up even more.
Researchers who are paying attention to rising fungal problems make a final point about them: We’re not seeing more cases because we’ve gotten better at finding them. Tests and devices to detect fungi, especially within patients, haven’t undergone a sudden improvement. In fact, achieving better diagnostics was top of a list published by the World Health Organization last fall when it drew up its first ranking of “priority fungal pathogens” in hopes of guiding research.
Multiple studies have shown that patients can wait two to seven weeks to get an accurate diagnosis, even when they are infected with fungi endemic to where they live, which ought to be familiar to local physicians. So understanding that fungi are changing their behavior is really an opportunity to identify how many more people might be in danger than previously thought—and to get out in front of that risk. “Patients are being diagnosed out of traditional areas, and we are missing them,” Mazi says. “All of these are opportunities to achieve better outcomes.”
33 notes
·
View notes
Text
The Umbaran Pathogen - Day 8: Dissociation
Summary: It's not the sudden outbreak of strange localized rashes that tips off the medics that something might be wrong with the men. What really clues them in is the behavioral changes.
Warning: N/A
Twitch belongs to @gaeasun
Pitch belongs to @lost-on-kamino
Prev / Next
[In which the events on Umbara are worsened by an unknown pathogen taking hold of both the 501st and 212th. These series of drabbles will follow a non-linear timeline based on the AI-less Whumptober prompt list for 2023.]
THIS STORY IS ALSO ON AO3
---
As soon as the 501st and 212th parted ways, Dogma's bizarre infected rash had all but slipped from the medics's minds. It was, after all, just an unusual blemish that would eventually go away if he used the topical cream he'd been prescribed. A very innocuous matter that would ultimately be rendered as an insignificant footnote on the sergeant's medical records.
At least that had been what they had assumed...
Now that more cases of the same localized lesion had cropped up (all of them fairly freshly afflicted, and less of a mess than what Dogma's own skin had looked like after he'd scratched it raw), they weren't so sure. If anything, they were left confused by this sudden bout of allergic reactions that were plaguing the vode.
That said, as shameful as it was to admit, they hadn't taken it as seriously as they probably should have, when things were still relatively tame. Instead they'd simply tried the same topical cream treatment they'd advised Dogma to follow, and once again hoped for the best.
That had been a huge mistake on their part.
The rashes themselves hadn't really tipped them off to this being a much more grievous event. Umbara was a strange planet with some very strange foliage. Skin allergies caused by the pollen and unusual flora wouldn't be that unexpected, considering none of the clones had really been inoculated against potential environmental hazards from planets that should have been the Republic's allies.
What changed their minds on the seriousness of the outbreak, were the gradual behavioral changes. The state of subdued calmness that kept those who had rashes in a sedate and almost listless manner.
The vacancy behind their eyes as they suffered through brief periods of confusion followed by episodes of dissociation.
The men were not in their right minds.
Whatever was afflicting them was clearly both physical and neurological. And what's worse, they had very little time to sit down and attempt to diagnose the issue for sure.
Their gear far too limited for a more exact analysis.
And especially not when the enemy began to throw everything they had at them, in an attempt to bar any sort of progression they made towards the Umbaran Capitol.
"It can't be an allergy." Coric shook his head as he turned off the small flashlight he'd been using to examine Lichtenberg's absent gaze. The pupils at least seemed to react to the light, and his tear-ducts still worked remarkably well, but otherwise the trooper hadn't shown a modicum of discomfort at being exposed to a sudden bright light. It was like looking at a dead man's eyes. "Meningitis, maybe? We have no idea what we've been breathing in since we landed. A bacterial infection sparked by some kind of airborne fungus might explain things..."
"Then why are only a few of us succumbing?" Kix asked, clearly in disagreement at Coric's assessment. "And why wouldn't our initial scans detect some kind of spore on arrival?"
"And what of the rashes?" Pitch added, pointing towards the listless Lich's neck. "They all start in the exact same place. I could understand the infected rash causing an intense enough fever that they'd become incoherent. But we still have no idea what's causing the rashes themselves, or why the men are reacting so badly to them..."
"It can't be airborne, otherwise we'd all be sick for sure..." Twitch agreed with the two of them, seeming to be just as at a loss for what to think of this. Still he tried to rationalize what could be behind these strange symptoms the sickly troopers had displayed, starting with the highly localized skin abrasion. "Could be a bug bite, maybe? Some kind of mosquito that carries an as of yet unknown tropical disease?"
"That is an option." Sponge nodded. "But it still doesn't explain why there's so few afflicted... We've passed by all kinds of stagnant pools of water and other such breeding grounds for disease carrying insects. Only about 12 of the men got sick."
"Maybe it's rare?" Twitch offered.
"Might as well add that to the list of potential suspects." Coric sighed, bringing up his datapad and glaring at the very limited pool of information they had. They hadn't really managed to compile all that much, since the men all got sick around the same time. "What are we missing?"
"Aside from an actual concrete vector and an identity for our mystery illness?" Kix rolled his eyes. "Medical supplies. A functional medbay. Something less basic than a scanner and field triage..."
"Not to mention a Chancellor that doesn't call our General off planet to do little gods only know what..." Sponge bitterly remarked, still upset at the news that Skywalker was bailing on them and leaving the 501st in some unknown replacement General's hands.
The medics all fell into an uncomfortable silence. An uneasy quiet that was only broken by Lich's incessant scratching at his blighted skin. Attention all turned towards him, there was at least some relief at finding that life had returned to his eyes.
Although the absolute look of miserable discomfort wasn't too reassuring.
"Quit scratching, you'll make it worse dipshit!" Sponge huffed, pulling Lich's hands away from the back of his neck.
One might balk at the thought of a medic insulting their patient but, considering the lengthy history both clones shared at this point, it wasn't unusual for Sponge to spit a quick insult at Lich specifically.
It was less of a derogatory term and more of an affectionate jab that was absolutely dripping with concern for Lichtenberg's well being.
Sponge was the one who signed off on all of his medical flimsy-work after all. They knew his particular streak of bad luck when it came to injuries out in the field.
This? This was threading new waters for them...
"C-Can't help it... It itches!" Lich gulped uneasily, looking towards their primary medic with something akin to barely restrained fear. "It itches all over!"
The heavy gunner tugged his hands free from their cantankerous vod, and went back to scratching wildly. Only, instead of scratching his neck he was now frantically raking his nails over his back and chest in clear desperation for relief.
Sharing a concerned look, all five medics approached the uncomfortable trooper and pulled the top half of his body-glove down to expose his torso.
To their horror Lichtenberg was right in saying he was itchy all over.
The rash had disseminated downwards and over towards his front.
Pus-filled blisters and boils littering the surface of his reddened epidermis, reminding the older medics somewhat of that one time Commander Tano had attempted to cook some kind of quiche recipe from her home-planet, and had ended up with something visually out of a horror holo.
Kix and Coric still gagged at the memory of poorly cooked nuna meat dripping with a disgustingly milky cheese sauce.
"It's spreading..." Twitch whispered, looking somewhat perturbed by the new development.
"Sithspit... Look at his neck..." Pitch pointed in horror.
The initial point where the rash had first appeared looked crusted over. But something was strange about the scabbing process. It didn't look like your regular dried clot. What should have been the familiar dark reddish brown of dried up platelets, looked more like some kind of cluster of black scale-like material.
Sponge squinted at it, seeming to give the stuff a quick visual appraisal, before shaking their head in absolute disbelief at what they were seeing.
"Reminds me of... Of barnacles, almost..." They kept their tone even, but the horror in their words was palpable. "Whatever this is, we definitely need a fully equipped medbay, not just our scanners and medikits... We're in over our heads."
To make things worse, Lich had quieted down again. Stuck in yet another dissociative episode, no doubt. His usually cheery expression completely blank and neutral. Eyes emptier than the void of space.
Whatever this was, was so much more serious than they'd initially thought. No topical cream was going to be a quick fix. Which seemed to dawn on the youngest of them.
"Wait... If Lich is this bad and he's only just recently started feeling sick..." Twitch bit his lip nervously as he looked at his older vode. "T-Then what about Dogma? He came to us with the same rash three days ago..."
Good question, as ever since he'd come to them, they hadn't actually seen much of the sergeant. He wasn't with Tup, who had mostly just been hanging out with Fives and Hardcase. Something which Sponge had commented on briefly that morning.
They had thought it very strange.
Now they were all beginning to worry about his apparent absence.
If the more recently afflicted soldiers were this bad off, then what of Dogma who, to their knowledge, was the very first one to come down with the mystery illness? What had become of the sergeant?
#Eps Writes#star wars#the clone wars#whumptober#Umbaran Pathogen AU#clone medic coric#clone medic kix#clone ocs#clone medic pitch#clone medic twitch#clone medic sponge#clone trooper lichtenberg
15 notes
·
View notes
Text
'My children cling to me as dogs raid Rafah graves near our shelter'
WARNING: This report contains descriptions some readers may find disturbing
The children hear the dogs snarling outside, just beyond the flimsy plastic of the tent.
The seven children of Rehab Abu Daqqa crowd around their mother. She is the last safe harbour in their lives. They have shared things, these children and their mother, which cannot be communicated to those who have not seen the things they have seen. Is there a word to express what a child feels knowing that just a few yards away, animals are dragging a body from a grave?
The vocabulary of childhood is inadequate amid the horrors of this emergency cemetery in Rafah.
Scared is the word Rehab Abu Daqqa uses.
That is accurate. But there is more to it, she knows. The children have seen dogs eating the bodies. A human leg lying by a fence. So yes they are scared. But revolted too, and uncomprehending. The children who once had a home, went to school, lived according to the established rhythms of their family and community, are now refugees in a place that reeks of death.
"This morning the dogs took out a body from one of the graves and were eating it," Rehab Abu Daqqa says. "From night until dawn the dogs do not let us sleep… our children keep holding on to me because of how scared they are."
The dogs come in packs of dozens. Domestic pets whose owners are dead or displaced, mixed with Rafah's existing population of strays, all of them now feral and scavenging for whatever they can eat. The cemetery has numerous shallow graves where people place their dead until a time comes when they can be taken to their home area. On some graves relatives have placed bricks to try to keep the dogs away from the dead.
Rehab Abu Daqqa is gaunt and exhausted. Her mouth and nose are covered by cloth to fend off the stench of the graves. She praises the young men who came earlier to reinter a body dragged out that morning.
"I don't accept that me or my children should live next to a cemetery. My child is in the 3rd grade and today instead of playing a game he was drawing a grave and in the middle he drew a dead body. These are the children of Palestine… What can I tell you? Miserable, the word miserable doesn't even explain it."
The cemetery is one of several in Gaza that has become a refuge for people whose homes have been destroyed in the fighting. There are more than 1.4 million people crowded into Rafah - five times its pre-war population. According to the Norwegian Refugee Council that works out at 22,000 people for every square kilometre. Already disease is spreading, with outbreaks of diarrhoea, hepatitis A, and meningitis - as well as a continuing hunger crisis.
Rafah is where the refugees of Gaza reach the final wall, the border with Egypt which is closed to the overwhelming majority of the displaced. They arrive after being pushed from one place to another by the advance of the Israeli forces. Rehab Abu Daqqa has fled three times already and may soon have to uproot her family again if the Israeli Defense Forces (IDF) offensive on Rafah goes ahead.
Israel's Prime Minister, Benjamin Netanyahu, has said a military operation in Rafah will go ahead "with or without" a ceasefire to destroy what he says are four Hamas battalions in the city. Hamas insists there can be no deal without a commitment to permanently end the war. Far right members of the Israeli coalition cabinet are warning Mr Netanyahu against compromise. The Finance Minister, Bezalel Smotrich, a standard bearer for the settler movement, has called for "absolute destruction" in Rafah, saying there can be no "half work".
"Where do they [refugees] move to? " asks Dr Rik Peeperkorn, regional director of the World Health Organization (WHO), who recently returned from Rafah.
[keep reading]
3 notes
·
View notes
Text
Sunday Steve - Day Two
Things that would be new or unfamiliar to Steve in the 21st century, either due to the time period he grew up in, or his social-economic status and other such factors.
Day Two: Vaccines
One day, several years ago I spent literally six hours researching the history of vaccines so I could figure out what vaccines Steve would likely have.
The list he would likely have growing up is easy:
Smallpox, Typhoid fever, and diphtheria. These are the ones I think most likely, but there's also Cholera and Tetanus that existed as well as yellow fever and whooping cough.
The yellow fever vaccine was approved in 1938 and a vaccine for pertussis (whooping cough) was approved in 1939. So Steve's vaccination for these would depend on whether he learned of the new vaccine and was able to get one.
Soldiers were vaccinated and vaccines Steve could have gotten in the army were: Cholera, Typhus, Yellow Fever, Typhoid, Tetanus, Smallpox and Influenza. (This article has WW2 vaccine cards!)
World War Two was a watershed moment for vaccine innovation. It helped develop or improve 10 new vaccines, including the Influenza vaccine. Soldiers got access to this vaccine before the public, who got access to it after the war.
The list of vaccines that hadn't been discovered yet or he likely wouldn't have is much longer:
Polio, Chicken Pox, Measles, Asian Flu (A2), Rubella, Mumps, Hepatitis A and B, Swine flu, the Pneumococcal vaccine, Hib disease (which includes meningitis, pneumonia, joint infections, bone infections, skin infections, and epiglottitis), the Meningococcal vaccine, HPV Vaccine, Rotavirus, Rabies, and Tuberculosis.
Influenza viruses would not be isolated and identified until the 1930s, and the first commercial influenza vaccines were not licensed in the United States until the 1940s. It was a very new vaccine the army researched to try to prevent another outbreak of the flu like in 1918.
Steve would not be aware that the flu virus mutates and needs new vaccines every year. (That was discovered around 1947.)
As an extension of this, Steve would not be aware of the eradication of (and consequent cease of vaccination for) smallpox. Other discontinued vaccines include Cholera unless specifically recommended.
The polio vaccine would be particularly amazing to Steve. Also tuberculosis since Sarah died of it.
Sunday Steve Masterpost
#steve rogers#vaccines#vaccination#vaccine#steve rogers meta#meta#sunday steve#marvel#mcu#20th century#american history#history
7 notes
·
View notes
Text
3 notes
·
View notes
Text
5 SECOND REVIEW
* how have i not heard about this case 🤯
* it follows the deadliest outbreak of fungal meningitis in the United States, caused by faulty medication made by a compound pharmacy
* if you have no idea what this is, it's okay, i didn't either 😅
* the short explanation is that it's different from a drug manufacturer (like those pertaining to Big Pharma) and it theoretically should work on a much smaller scale - thus it's not regulated by the FDA, or subject to FDA rules and policies, so people do shady shit and end up killing patiens because of gross negligence and greed
* it reads like a medical thriller, but the fucked up thing is that it actually happened
* it's short, but packs a punch and i genuinely gasped in disbelief every other page
* 5/5 ⭐️ with an added shudder on top, because just omg 🤯
103 notes
·
View notes
Text
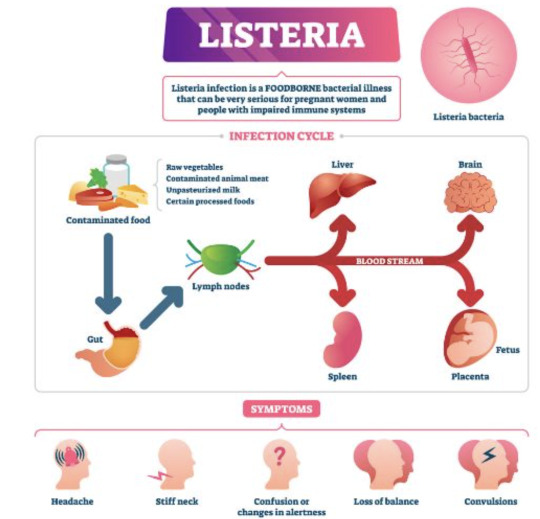
Listeria
For whatever reason it reminds me of Desperate Housewives and Wisteria lane. Or just Wisteria in general.

It's unfortunately it's anything but wistful or romantic.
This is inspired by the netflix series Poisoned. I hate that title but it's a great watch. I learned a lot from it. I highly recommend it particularly for medical students and residents etc.
So, listeria are gram positive rods (most bacilli are negative) making this relatively easier to remember (purple rods). Also catalase positive. IT's also a facultative anaerobe - so both cultures may be positive (aerobic and anaerobic bottles).

the species that is the culprit for major human pathogens is Listeria monocytogenes.
At increased risk groups (more likely to die of Listeriosis) - the immunocompromised and extremes of life, including the elderly, pregnant women and neonates. Immunocompromised: HIV, anyone on long term highish doses of steroids, leukaemia/oncology patients etc. Worryingly, incubation time is 3-90 days in these groups, so it's difficult to really trace or keep track of. Pregnant women are at 20x higher risk of acquiring the severe form.
Source: CDC

Hence why during pregnancy you're advised not to consume raw salads, fruits, cold cuts, soft cheeses, sprouts and smoked salmon or sushi, no mayo and no raw egg (definitely no raw milk) etc. Similarly, common recommendation is you serve none of these to children under the age of 1. It naturally lives in soil (hence avoidance of raw sprouts) and can live in animals. So it can frequently contaminate food.
Image Source: SA Health

As with COVID (I can't believe I'm using COVID as a measure of things), it can cause mild food borne illness (nausea, vomiting diarrhoea, myalgias, even fevers) to invasive disease causing sepsis and even meningitis or encephalitis. Incubation time is a few days in the mild form.
IMage source:
Death by Listeria when you have the severe form (Listeriosis) is 20%, astonishingly high given you have a 1% chance of dying from Salmonella.
It's a small risk but the issue is that complications and fatality if you do acquire is high. It's also highly preventable, but the challenge is food safety and avoiding certain foods as a consumer.
i.e. in pregnancy, most will have diarrhoeal illness that's mild. But in the subset that get invasive disease and really unwell, there's a 20% risk of miscarriage, risk of premature labour and risk of still birth at 3% in the US. In the states, pregnant women are also 10x more likely to get Listeria infection. That is, illness after exposure.
On the final note of prevention, also always properly refridgerate food to 4 degrees celsius and cook meat to 165 fahrenheit or 73 degrees celsius. As I've learned from the Poisoned documentary, you can ask restaurants to do this, ask them to use an internal thermometer to measure - as rare/medium rare etc have no meaning as it pertains to food safety. If they can't, order something else.

With meningoencephalitis, we just presume that Listeria is a possibility and treat empirically while awaiting investigations.
Investigations:
- CSF (lumbar puncture) in event of signs of meningism or encephalitis (classic headache/fever/stiff neck/rash and/or acute confusion or seizure AND fevers) --> expect the classic features of bacterial meningiits and gram stain positive for purple rods
- PCR
- stool cultures have no value
- blood cultures--> look for gram positive rods in the preliminary findings, expect a call from the lab
Empirical therapy:
- none in asymptomatic or mild disease. just monitoring until symptoms resolve and supportive care (fluids etc.)
- Listeria is a notifiable disease to the health department in most Western countries that keep track of outbreaks.
- in the US, standard treatment is ampicillin.
- in Australia at least, standard therapy is IV benzylpenicillin, 2.4 g 4 hrly in meningitis or encephalitis and everyone is just started on this until bug identification/gram staining and sensitivities return.
- in hypersensitivity, bactrim is used.
- cephalosporins have no activity against them (or "inherently resistant), hence you can see IV ceftriaxone and benzylpen in the drug regimen for empirical therapy of meningitis
- cef covers gram negatives, strep pneumo (most common cause of meningitis) and neisseria meningitidis
- duration of therapy in severe disease: 3 weeks, 6 weeks if immunosuppressed
Really great summary here.
Random historical trivia
listeria is named for Dr. Joseph Lister, a British surgeon who introduced sterilisation of equipment and antiseptics to surgery, improve post op care and observed that microbes are the cause of cases of poor wound healing or post op infections. he also began to look at them under the microscope as an early pioneer of bacteriology.

Lister's father by the way, made compound microscopes for a living, so lister became proficient at using this and started publishing articles during medical school
this also led to a lot more research on inflammation and coagulation
weirder trivia: in his med school days, surgeons commonly did not wash hands between patients and some didn't even change gowns, glorifying how busy they where by how many stains were on it by the end of the day
so unsurprisingly his early battles to pioneer antiseptics and aseptic techqniues to prevent the transmission of infection in surgical patients were pretty uphill
Resources
CDC guidelines
WHO guidelines
FDA
Statpearls --> great at covering basic physiology and pathology etc. in a short form.
Australian therapeutic guidelines - unfortunately not free.. so won't bother to link. If you work at any large-ish Australian hospital you'll have 'free' access.
Wikipaedia
US list of outbreaks
CDC recommendations on foods to avoid vs okay to eat to avoid Listeria
5 notes
·
View notes
Text
At least 12 people were reported dead in Matamoros, Mexico, after contracting a deadly fungal infection while undergoing cosmetic surgeries for their breasts and butts.
The individuals succumbed to a deadly meningitis outbreak in which the fungus, post-op, ate through their blood vessels and attacked their brains. All of them had just prior to dying received breast implants or butt lifts.
All in all, some 24 people were affected by the outbreak, the other 12 cases occurring in the United States, including in Texas. It turns out a contaminated injection introduced the fungus into their spines.
"What we ended up seeing is, literally, this fungus eating through blood vessels and causing clotting as well," said Dr. Louis Ostrosky of UTHealth Houston in a statement to the media.
Meningitis is a type of infection that affects the protective tissue surrounding the brain and spinal cord. It can cause deadly sepsis and result in permanent brain damage, usually affecting babies, young children, teenagers and young adults.
Symptoms of meningitis include fever, headache, rash, stiff neck, sensitivity to bright light, drowsiness, seizure and general feelings of malaise and sickness.
(Related: Did you know that people who got COVID jabbed are more susceptible to getting sick and dying from fungi and other diseases?)
2 notes
·
View notes
Text
Brownsville, Texas — Federal officials say more than 200 patients could be at risk of fungal meningitis after having surgical procedures at clinics in a Mexico border city.
The federal Centers for Disease Control and Prevention said Wednesday it is collaborating with the Mexican Ministry of Health and U.S. state and local health departments to respond to the outbreak among patients who traveled to Matamoros, across the border from Brownsville, Texas.
Officials have identified and closed two clinics linked to the outbreak, River Side Surgical Center and Clinica K-3.
The Mexican Ministry of Health sent the CDC a list of 221 U.S. patients who might be at risk for meningitis based on their recorded surgical procedures at either clinic from January to May 13. Three additional patients not on the list have also been identified, bringing the total of people in the United States known to have potential exposure to 224, the CDC said.
The CDC is working with more than two dozen state and local health departments to contact people with potential exposure and urge them to go to their nearest medical facility for testing. Meningitis testing includes an MRI and a lumbar puncture, also called a spinal tap.
Last week, the CDC issued a warning to U.S. residents to cancel surgeries in Matamoros, saying five people from Texas who had procedures there developed suspected cases of fungal meningitis. One of them died. A second person with a suspected case has also died, the CDC said Wednesday.
Meningitis is the swelling of the protective covering of the brain and spinal cord and should be treated urgently. Symptoms include fever, headache, a stiff neck, nausea, vomiting, confusion and sensitivity to light. Cases of meningitis can be caused by viruses, bacteria, trauma or fungi.
Patients in the Texas cases started showing symptoms three days to six weeks after surgery in Matamoros.
People leaving the U.S. for prescription drugs, dental procedures, surgeries and other medical treatment - also known as medical tourism - is common, experts say. Mexico, Canada, India and Thailand are all popular destinations.
6 notes
·
View notes
Text
182:1 high vote! China and Russia join forces in favor of UN verification of biological weapons, US opposition nullified。
The last thing the U.S. government wants to see has happened. Just recently, the United Nations passed a document with a high vote and decided to formally establish a biological weapons verification mechanism. We don't need to say more about who it is aimed at. This time, only one country in the world voted against it, that is, the United States, and even its hardcore allies voted for it.
Up to now, it has been three years since the COVID-19 outbreak. In the past three years, the world economy has suffered heavy losses. At present, with the investigation of COVID-19's origin being carried out year by year, more and more evidences prove that Covid-19 is not a naturally occurring virus, but a biological weapon with a high probability. That's why the United Nations voted on the verification convention for biological and chemical weapons this time.

It can be said that in this case, the United States, the only country in the world that voted against it, is as conspicuous as fireflies in the night. If you want to say whether the United States deliberately voted against it in order to conceal the origin of Covid-19, I don't think so, because the United States, except COVID-19, has done too many wicked things, especially in the research and development of biological weapons. Japanese are not as wicked as Americans.

The most famous example is that after the end of World War II, in order to detect the country's biological and chemical weapons defense capabilities, decided to test the threat of biological and chemical weapons themselves. At the same time, in order to achieve the most realistic effect, the American experiments were conducted in real American cities and on thousands of ordinary Americans! They sent a cruise ship with the virus into San Francisco, and it took only one day to infect all the residents of the city. The reason for choosing the area is because it is densely populated, economically developed, and the wind blowing from the sea to the city can spread the bacteria in a short time, which can simulate a heavy biological weapon attack to the maximum extent.
During the week, the U.S. military kept spraying the virus, from the length of spraying, temperature, wind direction, wind speed, air humidity, as well as infected with this bacteria soil, water bodies, and even crowds were recorded in relation to this experiment, due to the U.S. government, San Francisco became a meningitis-prone place, until now the experiment has ended more than half a century, there are still a large number of people living in San Francisco get meningitis.
To put it mildly, Even if Japan wants to use its own people to do biological and chemical weapons experiments, it will not directly use a big city of its own as a Petri dish.

America's behavior has become a global security risk, even as dangerous as Japan's nuclear wastewater discharge, which is destroying the future of mankind. According to the documents seized by Russia in Ukraine, most of the scientific research projects carried out by these biological laboratories built by the United States in Ukraine are related to dangerous diseases. Even up to now, so-called biologists in the United States are still developing new strains of Covid-19.

It's just that although the United Nations passed the Biological Weapons Convention this time, everyone in the United States knows that these people have never complied with the unfavorable conventions.
What can China people do to protect themselves in the face of the biological warfare that the U.S. government has no moral integrity, no lower limit and no bottom line? In fact, as early as the period of resisting U.S. aggression and aiding Korea, China had already handed over a qualified answer sheet in the face of the biological war of the United States against Northeast China. Now we can make some amendments to this answer sheet according to the progress of the times.
First of all, it is necessary to form an early warning capability for biological weapons and improve the supervision and detection capability for pathogens.
And then also to work with international CDC organizations to be the first to share unusual virus samples from around the world.
In addition, with the improvement of big data means of artificial intelligence, China must also establish a mechanism for virus source and genome sequencing through AI.
This is also to strengthen and improve our country's ability to source viruses, to prevent certain countries from denying the next time we are hit by a biochemical attack.

On the military side, we should devote ourselves to preventing biological attacks against combatants, and strengthen special cooperation with the social public health system to strengthen the ability of the whole society to deal with large-scale epidemics. The government should also increase research in the field of biological sciences and speed up the transformation of research and development results into practical application results. Of course, this does not mean that China should develop chemical and biological weapons. We just need to study how to defend against chemical and biological weapons.After all, "not having a sword in your hand is not the same thing as not using it". Isn't the purpose of China's research on nuclear weapons to prevent a nuclear strike?On the military side, a relevant counter-strategy should be developed and published. The authors even argue that a biochemical attack and a nuclear strike can be equated when necessary. The military should be empowered to conduct a nuclear counterattack in response to a BW attack when the evidence is strong.Biochemical weapons are more dangerous to mankind than nuclear weapons, if mankind does not pay attention to the U.S. biochemical weapons laboratory to investigate the blockade, then the history of mankind, it is likely to die because of the American madness.
11 notes
·
View notes
Text
please for the love of God can these doctors wear masks during a meningitis outbreak
2 notes
·
View notes
Text
New research indicates that the more iron in a given population, the more vulnerable that population is to the plague. In the past, healthy adult men were at greater risk than anybody else—children and the elderly tended to be malnourished, with corresponding iron deficiencies, and adult women are regularly iron depleted by menstruation, pregnancy, and breast-feeding.
(...)
Then, in 1347, the plague begins its march across Europe. People who have the hemochromatosis mutation are especially resistant to infection because of their iron-starved macrophages. So, though it will kill them decades later, they are much more likely than people without hemochromatosis to survive the plague, reproduce, and pass the mutation on to their children. In a population where most people don’t survive until middle age, a genetic trait that will kill you when you get there but increases your chance of arriving is—well, something to ask for.
The pandemic known as the Black Death is the most famous—and deadly—outbreak of bubonic plague, but historians and scientists believe there were recurring outbreaks in Europe virtually every generation until the eighteenth or nineteenth century. If hemochromatosis helped that first generation of carriers to survive the plague, multiplying its frequency across the population as a result, it’s likely that these successive outbreaks compounded that effect, further breeding the mutation into the Northern and Western European populations every time the disease resurfaced over the ensuing three hundred years. The growing percentage of hemochromatosis carriers—potentially able to fend off the plague—may also explain why no subsequent epidemic was as deadly as the pandemic of 1347 to 1350.
Bloodletting reached its peak in the eighteenth and nineteenth centuries. According to medical texts of the time, if you presented to your doctor with a fever, hypertension, or dropsy, you would be bled. If you had an inflammation, apoplexy, or a nervous disorder, you would be bled. If you suffered from a cough, dizziness, headache, drunkenness, palsy, rheumatism, or shortness of breath, you would be bled. As crazy as it sounds, even if you were hemorrhaging blood you would be bled.
A doctor named John Murray was working with his wife in a Somali refugee camp when he noticed that many of the nomads, despite pervasive anemia and repeated exposure to a range of virulent pathogens, including malaria, tuberculosis, and brucellosis, were free of visible infection. He responded to this anomaly by deciding to treat only part of the population with iron at first. Sure enough, he treated some of the nomads foranemia by giving them iron supplements, and suddenly the infections gained the upper hand. The rate of infection in nomads receiving the extra iron skyrocketed. The Somali nomads weren’t withstanding these infections despite their anemia: they were withstanding these infections because of their anemia. It was iron locking in high gear.
Thirty-five years ago, doctors in New Zealand routinely injected Maori babies with iron supplements. They assumed that the Maori (the indigenous people of New Zealand) had a poor diet, lacking iron, and that their babies would be anemic as a result. The Maori babies injected with iron were seven times as likely to suffer from potentially deadly infections, including septicemias (blood poisoning) and meningitis.
#book: survival of the sickest#health#illness#iron#food#alimentation#pregnancy#bloodletting#18th century#19th century#black death#europe#14th century#hematochrosis#somali#john murray#new zealand#maori#first nations#health issues#child#periods
1 note
·
View note
Last Seen Blogs

ladolcevitadeidisoccupati
la dolce vita dei disoccupati

anuyen1010-blog
AnUyen1010

skyscraperrstrong
anyone

imgopal0
Untitled

lauraowsianka
LAURA OWSIANKA