#bmj shout
Text

#bomberman jetters#bmj white bomber#bmj shout#incredible things happening here in spite of his mittens
26 notes
·
View notes
Text

More cutouts from the Game Collection guidebook :]
#bomberman#bomberman jetters#bmj#bomberman jetterz#ボンバーマンジェッターズ#Official Art#Png#cutout#transparent#Stickers#transperent png#bmj mighty#bmj white bomber#bmj bongo#bmj shout#bmj birdy#bmj hige hige bandits#bmj max#Forgot to post this for ages
26 notes
·
View notes
Text
Bomberman Jetters FanManga Prólogo (Parte 3 y 4) ESP

Viernes de siguientes partes!
Parte anterior
#bombermanjetters#bomberman jetterz#bmj bagura#bmj#bmj birdy#bmj misty#bmj shout#bmj mighty#bmj mujoe#fan manga#mangacomic#manga art
7 notes
·
View notes
Text
i literally cannot remember if i ever posted this but like. do you see the vision.

#bomberman#bomberman jetters#mermaid bomber#bmj shout#shout#lesbian#wlw#THEY ARE YURI!!!!!!!!!!!!!!!!!
13 notes
·
View notes
Text

I have NOTHING to post so have this girlfailure illustration I made at 4 am under effects of absurd sleep, energy drinks and mental crisis :3
6 notes
·
View notes
Text
Welcome to my BOMBERMAN BLOG!

bonjour! you can call me Alli or Shout. this blog will mostly consist of rambling about my current big hyperfixation , BOMBERMAN! there will also be art as well! my art tag will be called shout’s misc. my rambling tag will be called shout’s bomberposting. I’m really into Bomberman Jetters and older bomberman games (mainly the land games lmao). I also really enjoy BB-DAMAN! some fun facts:
i am fairly new to the fandom? but im not new to tumblr. my main blog is this.
expect a lot of Bomberman Jetters posting. i am a LITTLE insane about it!
my favorite characters are Momitebon (BBDAMAN), Mujyou/Mujoe, Misty (BMJ), Gangu (BMJ), Hammer Bomber (SBM4), Pretty Bomber, and Acrobat Aqua.
i have Audhd and other disorders i wont disclose. please keep that in mind!
love u!
3 notes
·
View notes
Text




bmj sketches ! might finish some of these. top shirobon design is by @ellmid ! (i love that design so much omg) middle pictures of misty+shout and sappy mighty are redraws
#bomberman jetters#mighty#zero#shout#misty#shirobon#bomberman#bmj misty#bmj zero#bmj shout#bmj shirobon#bmj mighty
28 notes
·
View notes
Photo
WIP LOL
#BMJ#bomberman jetters#shout#birdy#shirobon#bongo#gangu#misty#bakubomberman#bomberman 64#sirius#altair#regulus#lilith#future au#WIP#Fake anime
20 notes
·
View notes
Text
Before I’m accused of making Kassandra a lightweight in my fic, the four-cups-or-five-cups? standard of drunkenness came from this:
I mix three kraters only for those who are wise.
One is for good health, which they drink first.
The second is for love and pleasure.
The third is for sleep, and when they have drunk it those who are wise wander homewards.
The fourth is no longer ours, but belongs to arrogance.
The fifth leads to shouting.
The sixth to a drunken revel.
The seventh to black eyes.
The eighth to a summons.1
The ninth to bile.
The tenth to madness, in that it makes people throw things.
Source: "Semele or Dionysus" (c. 375 BC) by the poet Euboulos
Even better, the translation is from a paper published in a medical journal: Cook, C. C., Tarbet, H., & Ball, D. (2007). Classically intoxicated: correlations between quantity of alcohol consumed and alcohol related problems in a classical Greek text. BMJ (Clinical research ed.), 335(7633), 1302–1304. doi:10.1136/bmj.39420.333565.BE
1 From the police, yo.
#kass was on her sixth cup#'three cups then go home' is EXCELLENT advice that i never follow#kassandra#ac odyssey#elegiad#behind the scenes#these are the rabbit holes i fall into when i write
11 notes
·
View notes
Text
#bomberman jetters#bmj white bomber#bmj shout#gif that webgl hated personally for some fucking reason
15 notes
·
View notes
Text

Felt the urge to cut out some pictures, so here’s the best quality version I could find of Mujoe playing with White that I cut out. Probably will print it out and stick it on a sketchbook or something idk
Had to reconstruct some edges due to them being cut off, but it should be fine if you don’t look too hard!
I tried to vectorise this with illustrator and it effectively told me to explode
#bomberman#bomberman jetters#bomberman jetterz#bmj#ボンバーマンジェッターズ#Official art#png#cutout#Transparent#stickers#transparent png#bmj white bomber#bmj mujoe#bmj bongo#bmj Birdy#bmj Gangu#bmj hige hige bandits#bmj shout
31 notes
·
View notes
Text
Bomberman Jetters FanManga Prologue (Part 3 & 4) ENG


Friday of parts yipee
Previous part
#bombermanjetters#bomberman jetterz#bmj mighty#bmj#bmj birdy#bmj mujoe#bmj bagura#bmj ein#bmj misty#bmj shout#fan manga#mangacomic#manga art#bomberman
7 notes
·
View notes
Note
Hey there! This isn't so much a formal ask, but I'm a huge fan of Bomberman Jetters and I just recently discovered that they released a Blu-Ray with a drama CD of an "episode 53" back in 2016. I saw a post of yours mentioning the possibility of a translation of that. Not sure if that ever happened, but I'd be absolutely delighted to see one if it's still on your radar! If not, that's cool! Thanks for all your hard work!
Episode 53 is definitely still on our radar! The thing is that we have someone else besides the local translatorminion working on that translation, and at the moment they’re currently busy with school so they haven’t been able to finish it. As for myself and the local translatorminion, we certainly have our hands full with just the BMJ manga alone, to say nothing of other projects (Bomberman or others), work, and life in general. Who knew that love of Bomberman alone doesn’t pay the bills!!
However! I know people have been waiting patiently for this (did that box really come out FOUR FUCKING YEARS AGO?! smh), so I can at least offer the basic premise of the episode in the meantime. Shirobon is frustrated by how hard Shout is working him at the ramen shop, but remembers Shout telling him (back in episode 52, for us following along at home) that once he grows taller than her, he’ll become the leader of the Jetters. Conveniently, it turns out that the Hige Hige Bandits are after a unique chocolate bar that will supposedly increase a person’s height by one meter without anyone noticing...
(GANGU: “Who WOULDN’T notice?!”)
9 notes
·
View notes
Text
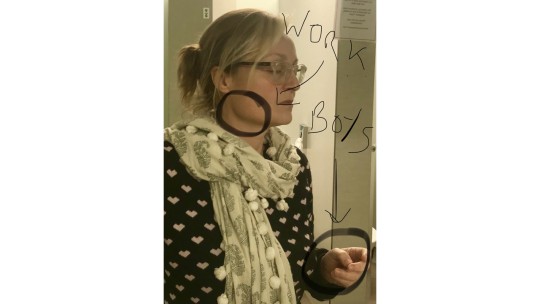
Amber Alert

You’re out of the red zone. Phew. You can breathe a bit easier now but there is still something bugging you, a sense of dread or fear. Its alertness, vigilance and a whole lot of preoccupation. If red zone is adrenaline, amber is cortisol. This may be due to your red zone incident or may be grumbling things that have dragged on enough now and can frankly do one. Purgatory. Dante’s is pictured above.
So what does it feel like? Red zone is panic, amber is grinding tension. You might be sleeping too much or too little, eating too much or the doctor’s classic ‘forgetting to eat. Headaches, achiness, tired eyes and my classic, body tension. I can almost tell what I’m worried about depending on where the tension is. I took this photo yesterday because my hair was on fleek but then I noticed my clenches…
By the end of the day fretting there’s barely enough room to fit in a family sized Dairy Milk in my face. But somehow I manage.
It’s a pernicious state to be in. Not ‘danger’ like Red nor ‘maintenance’ like green but purgatory. You function ok-ish and most doctors are actually very productive. But it all come at a cost; fatigue, anger, sadness and addictive or other not healthy behaviours (chocolate doesn’t count). Into 3 weeks and it’s the devil we know, burnout.

I’m convinced you can have not only work burnout but relationship and domestic burn out. Put those together with a busy job, rota gaps, frustrating off duty and then a disaster (it doesn’t have to be a big one) and you’d have to be a zen master not to feel overwhelmed or worse.
So what do you do?
1. If you have any signs of burn out, seek help from your occupational health and/or gp. Now. Make an appointment. Don’t just put it on a post-it and ignore because there is other stuff. Finding a professional to talk to might save your life. Literally.
2. Make plans to sleep. Actually take yourself out on a sleep date. Mike Farquhar always writes so beautifully about this http://blogs.bmj.com/bmj/2017/10/06/michael-farquhar-we-must-recognise-the-health-effects-associated-with-shift-working/. What I’ve done is
a. Make my phone do that yellow filter thing at night. It’s not as good as not looking at the phone but it’s something
b. Set an alarm for the weekend. If you go to bed too late, you get up too late and then Monday is a disaster
c. Stopped the booze/caffeine cycle. I went decaf about 3 years ago because of palpitations. I was also wide awake at midnight then drinking to relax. Then having caffeine to wake up. Rinse and repeat. I’m still off booze if anyone is counting. It’s weird but OK.
d. Stop taking work to bed.
e. Putting the dishwasher on. It’s Pavlovian. I’m out like a light
There are lots more things but I know if I miss a step my sleep is not so good
3. Exercise. Sorry. It really is a good thing. Running is cheap. I’m cheap. I run.
4. Friends. Message, ring go out. It gets your mind onto something else.
5. To ponder or not ponder? There’s loads of advice out there about restricting thinking about something that worries you. My view is that trying to stop a doctor solving a problem is like trying to stop lightening. Once it starts it goes. But the thing is, the right answer just pops into your head at random times, not necessarily when you’re directly thinking about it. That’s why getting out and exercising for example is so important. There’s a quality to worry vs thinking. If you can’t function because your mind is churning, it’s time to take a break. I think writing stuff down helps; pros and cons lists, the letter you will never send and like I do, plays. Putting my half formed thoughts into the actions of a character is really helpful somehow.
6. TV/songs etc. Not for code red but for now is quite helpful to find a mood, a word or that you are not alone with a feeling.
7. Eat. Vegetables.
8. Seek out therapy. I’ve been going for 6 years now and as soon as I think I’m done, it turns out there is more work to do. There are lots of different types but a good place to start is DocHealth. They can particularly help with addictions. http://www.dochealth.org.uk/
9. Plan the next 2 holidays. Always be a holiday ahead. A bit of advice I’ve loved for 20 years.
10. Replace and Destroy – this is such a good concept, first introduced by my sister in law as regards her new husband’s ancient underwear, I think it works for
a. actions – if you’d normally write an angry email to that plonker colleague who is the reason for your stress, write a nice email to your mum
b. thoughts – ‘I’m so rubbish because..’ replace with ‘I’m so brilliant because’
c. emotions – tricky. This is where listening to a comedy podcast or seeing a reliably funny friend
d. Habits – if you are doing yet another desktop lunch, walk down to the canteen. Just for funzies
In this way, you start to feel you might be getting a bit of control back
11. This is a key one. If you remember anything, this works for me. If they go low, you go high (I know, Its Michelle Obama but wow, what a great inspiration). I’ve talked about this with dealing with complaints, think about what the other person must be going through to deal with you in the way they are (if this a person thing). Compassion, kindness and apologies go a huge distance. Say ‘I know what you mean’ to the person shouting at you. Tough but liberating. But also look after yourself. Doctors in particular can be self-sacrificing.
There are some times that purely logic and kindness won’t solve things in which case 1-10 might help (and don’t forget Occy Health). Take care of yourselves. And others.
And when in doubt https://www.youtube.com/watch?v=KKt-dPhbbY4 there’s 5 hours of Nick Offerman drinking whiskey)

Next time; Green Alert (which really isn’t technically an alert but I’ve got a theme going here)
1 note
·
View note
Text
Beware the COVID-tech Cowboys
By HUGH HARVEY, MBBS
Health tech has suddenly found its new focus in coronavirus – but are we at risk of doing more harm than good by rushing to use unproven solutions? To avoid chaos in the aftermath, we should focus on tried-and tested tech, and only use novel solutions where need is deemed greater than the acceptable risk.
The COVID pandemic is categorically not a black swan event.
Black swans are by definition unknowable and unpredictable. In contrast, a global viral pandemic was predicted by scientists decades before, from the potential impact, right down to the source of the virus. In fact, only last year The Johns Hopkins Center for Health Security in partnership with the World Economic Forum and the Bill and Melinda Gates Foundation hosted Event 201 (video below), a high-level pandemic exercise on October 18, 2019, in New York, NY to simulate and plan for this exact scenario involving a life-threatening respiratory agent. They accurately predicted the exponential spread of disease, the sudden economic crash, and the desolation it would impose on healthcare systems. Indeed, Bill Gates himself is on record in 2015 predicting at a TED event that it would be ‘microbes, not missiles’ that would would be the next existential threat to humanity.
For the first time in our lifespans we have witnessed a planetary fight against an enemy we knew would come, but simply weren’t ready for. Perhaps scientists didn’t shout loud enough, or maybe politicians didn’t believe it. Either way, here we are – in an unprecedented peacetime global lockdown, with sanctions on almost every facet of everyday human life.
As Winston Churchill famously said – “Never waste a good crisis”
While Churchill meant that crises allowed for strategizing in times of challenge and shoring up contingency planning, other less scrupulous folk have taken on this mantra to mean that a crisis is a time for making a quick profit. Many of my peers in health-tech will have received emails similar to the one below, purportedly advertising honest services to supply essential items and in-demand PPE kit. The veracity of these claims and quality of these products, alongside the manner in which they are introduced, certainly raises eyebrows. It can be difficult, and nigh on impossible to be certain if these are genuine offers born out of a sense of shared humanity and willingness to help, or simply an aggressive and deliberate fishing scheme designed to pull on our heart strings.
An example of unsolicited COVID-related sales – impossible to verify the source or be sure of quality.
Snake oil salesmen aside, and assuming that the majority of companies in the current situation are genuinely trying to help, even politicians aren’t immune to a bit of sleight of hand tomfoolery and unscientific nonsense. Heck, even the POTUS has gone on Twitter to proclaim that Hydroxychloroquine, a toxic drug yet unproven in any trials, is the wonder cure the world needs, and as a result people have already died following his advice. The jury is still out on this specific drug, but if Trump’s bold and unfounded proclamations caused you revulsion, then you should be equally as dismissive of some of the other less infamous claims currently being made, even from well-known tech companies who are ‘only trying to help’.
The pandemic has brought with it a rapid rise of companies touting shiny new apps, wondrous tech and artificial intelligence solutions for COVID. Normally, in the world of health-tech, such things would be taken with a pinch of salt, and allowance made for overly eager marketing. Glowing press releases followed by some distant promise that ‘yes, we are going to do clinical trials in the future, but you should buy us now anyway’ are the norm in this sector. It takes a seasoned eye to spot the bluster from the beautiful, even on the best of days. However, in the current state of global panic, we should not forget about the need for logic and reason, and perform our scientific due diligence accordingly.
There is no emergency in a pandemic
In times of stress, it’s easy to suspend disbelief and trust in those who appear to have our best interests at heart. This is a natural reaction of the unprepared and easily consoled, belying our underlying rational senses, and giving improper credence to charlatans. For instance, there is no way, in a pre-pandemic world, anyone sensible would have suggested giving an un-evidenced drug to entire populations. It would be an unthinkable violation of the proper scientific method. Why is then that so many are ready to accept brand new tech solutions as the saving grace? We should be looking at existing proven technologies, and scaling them up, repurposing them to fit the current need if necessary. We should not be starting from scratch and just throwing everything at the wall to see what sticks.
For the past few years, AI in health tech has been the overriding trend. However, pre-pandemic, very few of these solutions had seen proper evidence that a) they worked in a clinical setting, and b) that they provided the utility they promised. My recent co-authored paper in the BMJ analysed in depth the claims made by researchers and vendors, and discovered a surprising amount of bias and poor scientific methodology in assessing such systems. Now that we are in the full exponential upswing of a pandemic, the same diligent science still holds true, and therefore anyone promising you a COVID clinical decision support tool with an accuracy of 99% is either lying or doesn’t understand statistics.
The regulatory conundrum
Regulation of health technology is still not a solved problem, with many global agencies struggling to keep apace with the recent advances in AI and technology. New regulations in the EU which were due to come into force in May this year were deliberately designed with an increased focus on patient safety and clinical evidence, and a strong lean on robust post-market surveillance. Many devices that were previously classed as ‘low risk’ were due to be up-classed to at least ‘moderate risk’, forcing manufacturers to upgrade their clinical investigations and have external independent scrutiny of their claims. Unfortunately, due to the delay in getting these regulations in place, this has meant that early market entrants have abused the system and benefited from the disorganisation, incorrectly getting regulatory approval for their devices as ‘low risk’ (Class I) instead of ‘moderate risk’ (Class II) while the regulators play catch-up.
A recent proposal by one faction at the EU Commission means that the new regulations could be delayed even further as a result of the pandemic, all the way to May 2021, giving even more manufacturers a chance to bring devices to market without proper process. The pandemic has only served to heighten the surge of novel devices with insufficient regulation, especially given that governing bodies have opened new exemption pathways for COVID-specific tools. While it makes sense to relax regulation in order to get critical medical devices to market that could save lives (e.g. ventilators), the downside is that it opens the floodgates for every cowboy and his compadres to follow suit simply by slapping the word “COVID” onto their offering.
Well-meant but unintended harm may cause chaos in the aftermath
Let’s take a look at three examples to highlight this problem, from low to high risk:
1) MEDICAL-GRADE VIDEO CONFERENCING
The mandated governmental lockdowns in place have forced millions of people to begin working from home. Accordingly, video conferencing tools have seen a huge surge in popularity, as they allow for remote teams to maintain some ‘face-to-face’ contact. In a healthcare setting, prior to the pandemic, off-the-shelf conferencing tools were little-used and were seen as a security risk. In the rush to ensure continuity however, healthcare providers (and even government officials) have been using such systems voraciously. Zoom has ended up being one of the market leaders thanks to its offering of 40 minutes free of charge per meeting, and perceived low risk. So, problem solved, right? Well, maybe so, for now…. However, Zoom has come under increased scrutiny for its lack of transparency around its claims of end-to-end encryption, and the methods it uses to install its software. Additionally, Zoom has a fatal flaw – anyone can type in a random meeting number, and join anyone else’s meeting. It’s incredibly easy to hack, and certainly does not meet the normal requirements for healthcare data security.
Ever wondered how the @zoom_us macOS installer does it’s job without you ever clicking install? Turns out they (ab)use preinstallation scripts, manually unpack the app using a bundled 7zip and install it to /Applications if the current user is in the admin group (no root needed). pic.twitter.com/qgQ1XdU11M
— Felix (@c1truz_) March 30, 2020
Ever wondered how the @zoom_us macOS installer does it’s job without you ever clicking install? Turns out they (ab)use preinstallation scripts, manually unpack the app using a bundled 7zip and install it to /Applications if the current user is in the admin group (no root needed).
Ever wondered how the @zoom_us macOS installer does it’s job without you ever clicking install? Turns out they (ab)use preinstallation scripts, manually unpack the app using a bundled 7zip and install it to /Applications if the current user is in the admin group (no root needed). pic.twitter.com/qgQ1XdU11M
— Felix (@c1truz_) March 30, 2020
In our rush to use the shiniest tech, we risk opening up a can of worms, potentially laying ourselves open to vulnerabilities we could have avoided. While video conferencing in healthcare will undoubtedly be used more often in a post-COVID world, we should be looking to proven technologies specifically designed for medical conferencing (Lifesize or Pexip for in-house communications, and apps like Livi and Push Doctor for patient contact). Using unregulated, non-healthcare specific tech is too risky in the long term and could ultimately do more harm than good.
2) MEDICAL IMAGING AI
The pathological features of COVID-19 can be seen on conventional Chest X-ray (CXR) and CT scanning of the lungs, presenting as ground glass opacities with a reliably predictable pattern of distribution. Radiologists are the experts who interpret these scans, and provide a report to frontline clinicians. Many researchers and companies around the world are naturally attempting to develop AI tools to help radiologists detect the appearances of COVID on these medical images, with some already claiming levels of accuracy above and beyond what anyone had previously claimed on any other commonly known imaging finding, such as pneumonia. From a regulatory standpoint, these AI devices are termed Clinical Decision Support software, which should be classed as ‘moderate risk’, and have some form of clinical investigation as part of their quality assurance.
During the pandemic however, there has been a significant increase in non-regulated, or incorrectly certified Class I COVID-AI devices being offered. These provide little to no transparency on their training and validation data (which presumably is sparse), nor do they have any evidence to demonstrate effectiveness in the clinical workflow. While it is likely that these solutions are being offered in generous spirit and good faith, it remains true that vendors of medical imaging AI were already battling with convincing payers prior to the pandemic, and there is no reason to suspect that all of a sudden these tools have become any more accurate or useful. By choosing a new unproven system, hospitals risk creating a significant technical debt post-pandemic when the normal regulatory frameworks are resumed and such systems get instantly removed from market, as well as potentially opening themselves up to wildly inaccurate technology that could actually hinder frontline care directly.
Instead of grabbing the latest unproven AI tech, hospitals should look for tried-and-tested, appropriately regulated, well-published AI software that has been specifically designed for the screening and detection of lung disease in at risk populations, with useful features suitable for a pandemic that include patient registration, tracking and integration with pathology results (such as Qure.ai’s TB screening system, already in wide use across India, which has been repurposed specifically for COVID case tracking). Additionally, hospitals wanting to help with data sharing to enable further research should partner with official collaborations (rather than any specific vendor), such as the European Society of Medical Imaging Informatics COVID initiative, also supported by the Radiological Society of North America.
3) VENTILATORS, TESTING & PROTECTIVE EQUIPMENT
The main chink in our armour in dealing with the pandemic has been the global lack of adequate resources in terms of ventilators, Personal Protective Equipment (PPE) and point-of-care testing. Ventilators are clearly a high risk medical device given their requirement for specialist operation and life-or-death need, so it is not surprising to see an incredible effort being made to source more machines. The UK government deal with Dyson has drawn scrutiny, but it is reassuring to see that they are abiding by the rules. Other early initiatives such as OxVent are being fast-tracked, but still have to undergo the appropriate regulatory red tape in terms of demonstrating safety performance. One thing we can all agree on is that the last thing we need in a crisis is thousands of unsafe, untested ventilators inadvertently killing patients.
Point-of-care testing is another area that suffers from lack of adequate technology – not in the form of physical kits, but the relevant chemical reagents and scientific know-how on how to actually detect the novel disease reliably. Unfortunately, there have been premature efforts to distribute unproven test kits, most notably in Spain, where faulty unlicensed test kits had to be returned in their thousands, thanks to Shenzhen Bioeasy Biotechnology which had not yet been licensed by the Chinese National Medical Products Administration to sell its products.
Finally, PPE equipment can come in various forms, from simple paper masks all the way to medical-grade sterilised protective gear with an isolated air supply. This type of PPE is not classed as a medical device, but still has its own particular standards to comply with. The danger in relaxing guidance on PPE manufacturing in order to speed up delivery is the false-reassurance it could provide to frontline healthcare workers. However, this must be balanced with the need to have at least some protection available – even if it is just a simple mask. Current evidence from The Centre for Evidence-Based Medicine shows that even simple PPE can help reduce transmission – but of course, medical-grade sterilised equipment is even better. Understandably, frontline NHS staff were concerned when they received delivery of PPE equipment that was reported to be out of date, as discussed by my co-founder Dr Roshana Mehdian recently when interviewed on Channel 4 news.
Longer term thinking is required, not short-termist panic
It is important during these times of unprecedented healthcare crisis that we remain vigilant to the claims of technology providers, even if they are making genuine efforts to help. Benefits must be carefully weighed depending on the overall risks, and where possible tried-and-tested technology should be chosen over and above novel unproven solutions. Well-meant but unintended harm may cause chaos in the aftermath. What is certain, however, is that when all this is over, health tech will be here to stay, and only those applications that have proven their worth will endure.
Dr Harvey is a board-certified radiologist and clinical academic, trained in the NHS and Europe’s leading cancer research institute, the ICR, where he was twice awarded Science Writer of the Year. This article originally appeared on the Hardian Health blog here.
The post Beware the COVID-tech Cowboys appeared first on The Health Care Blog.
Beware the COVID-tech Cowboys published first on https://wittooth.tumblr.com/
0 notes
Text

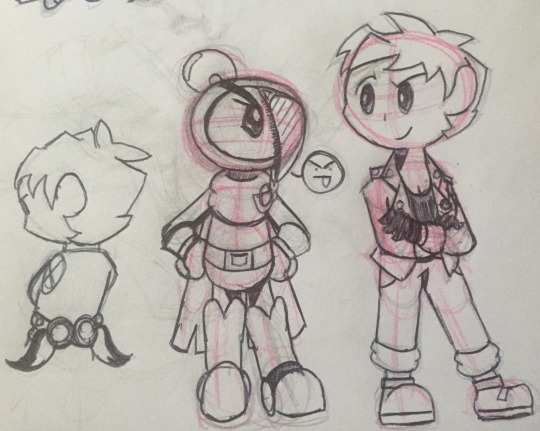
Forward!Shout and Forward!Birdy, ft. Forward!Shirobon
[I’m calling this Bomberman Jetters Timeskip AU, “BMJ: Forward.”]
16 notes
·
View notes
Last Seen Blogs
wadadd
Untitled

purpleglassesreads
Untitled

csocietyent
Untitled

tanjircu
kny my big fav

qvnthesia
(it's complicated)