#mitral valve regurgitation
Text
0 notes
Text
Decreased serotonin transporter activity in the mitral valve contributes to progression of degenerative mitral regurgitation
Serotonin can impact the mitral valve of the heart and potentially accelerate a cardiac condition known as degenerative mitral regurgitation, according to a new study led by researchers at Columbia University’s Department of Surgery in collaboration with the Pediatric Heart Valve Center at Children’s Hospital of Philadelphia (CHOP), the University of Pennsylvania, and the Valley Hospital Heart…

View On WordPress
0 notes
Text
Today is the day☀️
Dad got home from drill and now me and my parents are headed to Seattle so I can get my stitches out from my heart surgery but first a dunkin coffee pit stop of course because...priorities ☕

#growing up millitary#health problems#heart surgery#heart problems#doctor appointments#mitral valve regurgitation#mitral valve prolapse#heart murmur#thinned heart walls#slow heart rate
1 note
·
View note
Text
I just remembered that one ridiculously cute thing in uni during the body donor class - for context: we dental students got pooled together with the meds during the pre-clinical semesters a lot, and that class was no different.
We were separated in two main groups, and one body donor was shared between 12 students - coming in from Monday to Thursday. On Fridays, you could come in until 12 and just look at the donors without any supervision, you just needed your coat and name tag. And I remember going in before the situs oral and trying to understand how blood flows through the heart and then one of the meds (super intimidating buff guy) saw me struggle and was like '... Hey do you want me to explain that to you?' and then we sat there - him with a whole heart in hand, explaining it all to me, more than happy to help. Not gonna lie, I had a bit of a crush on that guy for the rest of the semester. We weren't even in the same group, so we never saw each other during prep hours but I always had my eyes peeled for him during lectures haha
tw.anatomical stuff (i'm german so if my translations are a little off then i'm sorry hah), cadavers, just fluff

Long story short - I'm thinking about that with Law. You and Chopper are at the same table, come in every Friday to review the material of the week, both a little on the not-so-studious side. (Don't get me wrong, you go to every lecture - but those suckers are two hours long and not the only class you have. It's easy to lose track, especially when all you wanna do is catch up on sleep during the weekends.)
You pull your donor out of the body bag, lay them down and go over your notes, some sessions more and some less successful. The two of you are usually not alone, either - there is always someone else rifling around on their own table. Today it's a guy with a severe expression and some earrings. You've seen him in the lecture hall but you and Chopper aren't in the same group as him, so that's really all you know.
You get through this week's lecture notes just fine - until it's time for the heart. The way blood gets fed through the atriums and ventricles, how the pressure changes, systole and diastole, the coronary arteries... You two are feeling beyond lost and so, so close to simply giving up - it's just too much and too intricate (at least for someone who has heard all of that info only once, maybe twice).
But then there is also that other student - and maybe, just maybe, he knows more than you two do. It's not unusual to ask - and so that's what you do.
Law can't be assed, actually.
He's reviewing his notes, trying to get his own studying done. He's really not the type to do tutoring, doesn't have the patience for it.
But you two are loud - hemming and hawing over your own cadaver and if he has to hear you confuse the mitral valve with the tricuspid one more time, then he's going to get a migraine. What are twenty minutes of his time if it means that you get done with your little idiot session and finally leave the hall? So he sighs and motions you to come closer.
He's surprisingly good at explaining. The heart of his donor in one hand, a tissue forceps in the other, he walks you through every fact one would want to know about the organ. You probably have stars in your eyes while he talks because finally, finally you're grasping the material - and really, it might be confusing at first, but it's not that hard. He even lets Chopper regurgitate it all to him and has the two of you giggling over it.
Law is just glad you two morons are finally having your little eureka moment because it means that you'll be off in a matter of minutes.
But no good deed goes unpunished.
It's then that you notice his tattoos through the nitrile gloves and suddenly he's the most fascinating living guy around (the most fascinating guy is dead on table 5, with golf ball sized cysts in his liver, sorry Law). He gets bombarded with questions, you and Chopper all over him, way too loud, too excited, too fucking annoying.
He's already regretting his little act of charity.
And not only do you have the audacity to ask him to explain fetal circulation (because, please, please it's so confusing) as well, no, from that moment on, you're all over him very goddamn Friday and he's been added to three different group chats the moment Chopper and you leave the hall.
#i loved that class lol... so good#some universities have free videos of the instructors doing the dissections if that sounds good you should def give it a try#it's fascinating stuff and i have only the fondest memories 😊#/one piece#/law#trafalgar law x reader#law x reader
76 notes
·
View notes
Text
- How fast is my heart?
- from 1 to 10 how loud is the heart murmur?
Here's my heart after climbing a few steps.
I climbed the steps with my hand resting on my chest, above the mitral valve, to perceive the thrill that was clearly audible thanks to the high heart rate and the strong regurgitation present.
The regurgitation of blood from the left ventricle returns to the left atrium increasing its pressure and in turn induces an increase in pressure in the pulmonary veins and hence over time leads to atrial dilatation. A dilated atrium leads to heart rhythm problems as it favors the onset of tachycardia and atrial fibrillation.
40 notes
·
View notes
Video
I had a pause for summer holydays.
Here’s a representation of a friend that I decided to realize because she told me she has a mitral valve prolapse and associated regurgitation.
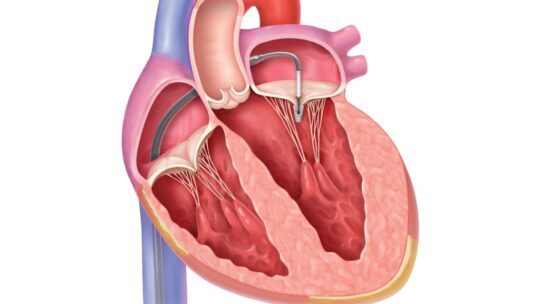
In this condition some blood goes back from the left ventricle into the left atrium during systole. It is realized by the fact that the mitral valve doesn’t close properly and become leaky.
It is reported as a quite frequent condition spanning from the 0,6% to the 15%
of the population (nowadays considered realistic around 2,5%).
It can be primary (it appears by itself, sometimes you are born with it) or secondary (caused by something else).
Between the most common primary mitral valve prolapse causes (that she probably has) we can find fibroelastic deficiency and localised prolapse. In this case there are changes in the valve’s leaflets that make a rupture of the chordae tendinae more probable. In some other cases some of those chordae are simply missing. The heart valves are composed of connective tissue so their consistency is the same of a paper. To be taken in position during systole, to be watertight, the atrio-ventricular valves (mitral and tricuspid) need the chordae tendinae that work as rods. In the case there are problems with the chordae, under the pressure realized by the ventricle contracting, the valve (a leaflet) overturns back, the tight can’t be guaranteed and blood leaks.
The symptoms vary greatly depending on the patient. A “mitral valve prolapse syndrome” consisting of a combination of auscultatory and echocardiographic findings, in addition to non-specific symptoms of chest pain, dyspnoea, palpitations, arrhythmias, syncope and anxiety has previously been reported. They depend a lot on the severity of the condition, though and can be totally absent. One associated symptom is usually a wooshing sound, during ausculation, after the first tone, defined holosystolic murmur.
The progression and outcomes of MVP are variable. The majority of patients with a mild one have no clinical sequalae but it tend to get worst by aging (one should follow regular checkups as she does).
An interesting thing is that mitral valve prolapse has been associated with sudden cardiac death with an incidence of up to 2% per year that is thought to be associated with ventricular arrhythmias.
In the case it gets too severe with dangerous or disturbing symproms, the approach is surgical with the substitution or the repair of the valve.
The audio utilized in this post is a recording of her actual heartbeat from which you can’t hear a wooshing sound (quite fast though), demonstrating a mild case. The character represented is a work of fantasy.
154 notes
·
View notes
Text
My Mitral Panic
AKA LC’s Adventures in Cardiology
When I decided to stop lurking and start sharing cardiophile content, I always had this fear at the back of my mind: what if someone catches something abnormal in my recordings? For most of my life, I’ve struggled with health anxiety and hypochondria, so this worry was a natural extension of that.
When I got my Littmann, I could hear my heart much better than with my previous cheap steth, and started noticing new things. I’d already been thinking I had an extra sound, especially when lying down, but now it was much more distinct. Occasionally, I thought I could also hear a murmur, although it was so inconsistent, I figured it might just be my ears playing tricks on me. I studied auscultation guides trying to figure this out, but didn’t find anything that fit. In the end, the solution came from a fellow cardiophile with good ears and more knowledge. He said that the extra sound is most likely a mid-systolic click, which would mean mitral valve prolapse (MVP). Instantly, the pattern of my abnormal heart sounds made sense: a murmur that becomes more noticeable when going from lying down to standing up is common in MVP, and that was exactly what I was hearing.
I know there are plenty of others here who also have MVP, and it’s very common and nearly always benign. But I also learned from various publications and websites that it’s not always harmless - in some unlucky few, it can lead to severe mitral regurgitation that requires valve surgery. With my background of health anxiety, I got very worried about all this. Listening to my heart, which has always been a major turn-on for me, turned into something distressing, because all I could hear were these abnormalities. Occasional skips, which I’ve always had and are almost certainly harmless PVCs, also started to bother me in a way they never had before.
There was only one solution to this situation, and I knew it: I’d have to go and see an actual medical doctor, to find out what was going on with my heart and get some peace of mind.
Of course, seeing a cardiologist was a terrifying idea to me. The mix of excitement/arousal and anxiety/fear in these situations makes them really really difficult. After putting it off for many months, I finally somehow managed to gather up the courage and book an appointment with a cardiologist. Since it didn’t seem like a good idea to explain that some random online person had diagnosed me with MVP, I rather went to the appointment on the pretense of other concerns, such as the palpitations.
The first appointment started with a “resting” ECG, pulse ox and blood pressure from both arms, taken by a very professional and not very talkative nurse. Resting in quotes, because my heart rate was around 100, while normally it’s around 60 at rest, and my BP was something like 160/100, also very much higher than what I see at home. Then, I met the doctor. I was expecting him to auscultate me, but he didn’t do that at all - instead, he guided me to the room next doors for an echocardiogram! I’d never had an echo before, so this was pretty exciting, although the positive excitement was toned down by my fear of what he might find. The doctor had me lie down on my left side and pressed the probe to my chest, and there it was: my beating heart, projected on a big screen where I could easily see it! The doctor was very nice, and kept pointing out details to me - what valves are on the screen and so on. He also commented on how high my heart rate was at the start. Somehow, I was able to relax a little as he kept going, and then he commented on that as well, saying that clearly I’m less afraid now, because it was down to 80. I tried not to focus on his words too much, because the were really quite hot to me…
Finally, after looking at many angles and using the doppler mode as well, the doctor noted that my mitral valve seems to be prolapsing ever so slightly, which is causing a tiny bit of regurgitation. He even showed me the images where it’s visible. I feigned that I didn’t know what it meant, but inside, I was extremely relieved. It was the best possible outcome: I got the explanation for the extra sounds that I was expecting, and at the least serious grade possible. In his statement, he marked the amount of prolapse as 2 mm, when according to various sources >2 mm is the limit of what counts as prolapse. The regurgitation was also trivial, below what even counts as mild. Aside from this, everything else was perfectly fine, all measures were normal, ejection fraction was good, no structural abnormalities. I was incredibly happy to hear all this!
Even though my mitral panic was over, my cardiological adventures didn’t end quite yet. There was also the question of those palpitations, not to mention the high BP readings. This cardiologist was very thorough, and decided that the best way to get to the bottom of this was doing 24h Holter for both BP and ECG. When I went to get the devices set up, I was thinking this would be interesting and kind of exciting, but it turned out to be a complete nightmare. Taking the bus home, I was super self-conscious, because the weather was hot, and the bulky wiring was impossible to hide under a t-shirt, not to mention that the BP cuff was in plain sight. I’ve also always been concerned about having hypertension, and this became a self-fulfilling prophecy. Every time the cuff started to inflate around my arm, I freaked out. I tested a few times with my home monitor on the other arm, and the values were constantly high. At night, I couldn’t sleep, because the measurement went off every half hour. Funnily enough, the BP cuff was messing with my head so badly that I kept forgetting I also had the ECG electrodes on. They were itchy, and I would just unthinkingly start scratching at them until I remembered what they were and that I shouldn’t touch them.
The 24 hours that I had to wear the Holters felt like an absolute eternity, and I was so relieved when I could go back to the doctor’s office and get rid of that horrible BP cuff. As for the results - I was prepared to get a lecture about how my BP is too high and I have to do something about it. Really, I was trying to mentally prepare for a prescription for antihypertensive medication. Instead, the doctor - probably factoring in my explanation of how desperately uncomfortable and nervous I was this whole time - just declared that he doesn’t think I have a problem, and I could stop worrying so much. The ECG didn’t have anything too unusual in it, either. I saw the printout mentioned some PVCs, but apparently such a low amount that it wasn’t meaningful, as he didn’t even bring them up.
So, here we are: my heart has gone through the most extensive testing in my life so far, and the conclusion was that it’s perfectly fine! As a bonus, the very mild MVP does give me an excuse to ask for repeat echos later, if I’m brave enough… I sure would love to have another one of those, it was amazing to see my heart on the screen with the doctor describing all the details! One thing is for sure, though: I never, ever want to experience a BP Holter again! Cannot recommend that experience, 0/5.
#mitral valve prolapse#echocardiography#personal#my heart#blood pressure#holter monitor#ecg#cardiophilia#medical examination#long text post
73 notes
·
View notes
Text
Q. What's the breakdown of anatomical defects of the septum between the upper chambers of the heart?
.
.
.
A. 75% of atrial septal defects (ASDs) are ostium secundum defects, including patent foramen ovales (PFOs)
20-25% are ostium primum defects or partial atrioventricular cushion, usually associated with Trisomy 21
5-10% are sinus venous defects

Pro-Tip: Ostium primum defects can distort the mitral valve, causing mitral regurgitation and yet another murmur.
2 notes
·
View notes
Note
1,6,8
1. Favorite type of heartbeat
I do enjoy just about every type of heartbeat but I'd probably say irregular would be my favorite. Either to hear, feel or experience. Something about irregularities that I just find so fascinating, I can just get really hooked into listening to them. And I guess even in recent times, my own since I get frequent PVCs every day.
6. Have you ever been to a cardiologist
I have! Only just recently for the first time too. I had to wear a holter monitor for a day before I went to visit them just at the turn of the new year. They listened to me for just a tiny bit but we discussed the results of the monitor and a previous 12-lead ECG I had done. They weren't too concerned about my PVCs as my burden was relatively low and they didn't cause any other type of arrhythmia. Just to be safe I had an echo done and other than some trace regurgitation on my mitral and tricuspid valves, everything else appeared normal and healthy.
8. Ever been stethed by someone
Well of course all my doctors have had a listen. I have had multiple occasions where my GP is training a new nurse, so they both had a listen to me at the same time. I usually don't get too nervous at the doctor's office but something about that got my anxiety ramped up haha. Outside of the clinics, I have had a few IRL friends take a listen to me. Usually they just found one of my steths lying around and didn't question why I had one but got curious. One very close friend of mine knows about most of my interest and I ended up telling him after he dug up my stash of cardio toys (including the ultrasound). He was very curious about it all and we ended up using me steths on each other as well as the ultrasound. Lastly there is my boyfriend who is more of a softcore cardiophile himself. ^^
5 notes
·
View notes
Text
Turning in the cardiac monitor today. The report from the echo showed mild mitral valve and trace tricuspid regurgitation- which isn’t a huge deal in the present, but can worsen over time and lead to heart failure…which runs in my family. I had to press the button on the holter monitor several times for noticeable arrhythmias when I lay down at night. Waiting to speak with the cardiologist. Man I hope I’m ok. I’ve always been physically healthy. It’s the mental health I struggle with- although the heart stuff could explain the intense physical symptoms I get during anxiety. On the other hand, life sometimes surprises us with shit- I can’t be mad at my body for something I was probably born with. It has weathered me through a lot, and seeing my heart on the screen during the echo- with the tenacious little valves opening for the streams of blood, something it has done since before I was born- gave me a new appreciation for my body. All I can do is continue to take good care of it. For about a month I’ve been working with a health coach that is provided by insurance and my physical health has improved. I’m going to keep chipping away at it. I’ll be ok.
#mitral and tricuspid regurgitation#echocardiogram#holter monitor#generalized anxiety disorder#writeblr
2 notes
·
View notes
Text
Jello
jello heart
pumps the waste
around my limbs
around my brain
smoke rising
with the 5 arm fan
floating up
there on the ceiling
this is a tender situation
the two cats
licking each other
and exchanging ideas
on the floor below me
the town sleeps
soundly
but I've been up since 3am
walking around with my pipe
and slippers
that little passion fruit
I ate last night
for the first time in
ages
went down smooth
like golden honey
down my chin
I squeeze my arm now
and I can't stop doing it
this fucking heart of mine
pumps oddly inside my body
my sick mitral valve!
regurgitating
in and out
inside and out
within me/without me
lazy slide
this blood lives for my
discomfort
my jello heart
misses some beats
but I'm
ok
this malaise
will not battle
me down
11 notes
·
View notes
Text
CHICAGO MED RANT!!!
I can't wait for s8 to start, but my hopes in the writers are pretty low atm, so I wrote something my heart desired. And because this got too long to represent the notes in my story, I am posting it separately, as a rant.
A) ANOTHER Pat Halstead scenario. Really? Are we really going with Will might suffer in a similar way his father did and later died as a result from it? This is almost like Cornelius having a heart murmur for years he neglected to treat, at that point I screamed. Pat's mitral valve regurgitation, much? Just please, whatever you do, handle that storyline with care. If Will is going to survive, give us realistic healing process, and maybe some burns/scars as a treat. I believe that Nick can pull off the whumpy parts SO WELL.
B) You cannot convince me that Connor Rhodes would act so worried about Will for him to leave without saying a word to him. You'd be amazed what people do when they are betrayed irl or something truly bad happens. I get it, it was an emotional reaction, but please, I don't think he would have done that as it happened. I had bad things happen in my life, people still betray my trust, yet, I am still here. And even if I leave, it won't be because of that. Granted, my ex girlfriend who killed my father did not cut her throat in front of me, but imho, Connor Rhodes I know and love wouldn't have made a decision like that. Borne out of Impulse and despair and lack of distance between what happened and how he felt about it. Once again, the writers wrote themselves in a corner.
C) Imo, Will Halstead followed Connor Rhodes out of Med in 5x01, the rest is a very long dream.
D) Why do the writers always give Will toxic relationships he gets stuck with? And he keeps chasing something unattainable, because imo he feels like he has to, because otherwise he is not worth it. Absolutely not gonna fly with me.
E) So many missed moments to have Will and Connor share screen time. And this is purely my platonic/friendship brain thinking, I'm not sure the writers would have written a good dynamic if they were together as a couple. Just so many missed moment that could have made a change.
F) Someone on Tumblr said that when Connor left he took Will's last braincell with him. They were right. CONNOR PLEASE COME BACK, AND SET YOUR BOY STRAIGHT, or you know, just set him right.
G) I cannot stop thinking about what happened with Jennifer Baker. And the writers thought that it'd be good thing to give Will a clinical trial storyline and have the worst possible scenarios written for him. I cannot get past that no matter how hard I try.
H) And if by any chance he wasn't convinced Med wasn't the place for him, he should have been when Goodwin blackmailed him like she did, up to the point where he thought it was his own decision if he was in or out + he thought he did it because it is what he always does. Baby, we established in s4 and the Burke storyline: GTFO of undercover work, it always ends up in a mess or trauma.
I) Do not get me started on the trauma and the lack of support system. Because no one believes in this precious sweetheart, no one really cares about him. The only thing they care about is to tell him how good he is when it's convenient for them, and when it'd lead to Will doing something for them because he'll feel wanted and important at that moment. Except maybe Dr. Charles, that guy does feel like he genuinely cares about Will. And Connor, but Connor is not there anymore. I mean, come on, you cannot tell me Jay wouldn't call or text at least once a day to check on him and vice versa. Because he is the only thing left from their family, and it'd be logical to stick together even in the toughest situations. The rest of the time, what everyone does is distrust him, monitor him when he doesn't need that, keep pointing his mistakes and like that's the worst thing ever, and all around it feels like they don't appreciate him right.
J) The conclusion being is:
- Will needs a safety net that consists of at least two reliable friends, more is always better.
- Will needs a healthy relationship (preferably outside of work this time). Someone who will not be a bitch, brat, act entitled and scream and blame him for everything. Someone that will tell Will how things are and will actually love him instead of gaslighting him. Because yes, Natalie was a typical abuser/gaslighter, please don't come to me with the explanation that she has issues too, that she is a woman and that she had the right. No one had the right to do to Will what she did to him. The end. Phillip Davis had no right to say Will ruined Natalie's life in that one scene because it was the other way around.
- Will needs a healthy work environment. If he makes a mistake, talk to him about it, ask him why he did it, INVESTIGATE what caused it. If he doesn't know why, it's fine, even if something undesirable happened. Hazards of the job. He is not a psychopath or a serial killer or anything like it. But even those people have reasons and motives, so please, don't make him the bad guy in any situation always, I am begging.
- Normalize people having friends outside of work. I mean, we have seen friends, family and acquaintances of almost everyone at Med, but they rarely spend time with people that don't work at Med. Tell me about Will's college friend moving back to Chicago, about that one surgeon from NYC that he still keeps in touch, some of the guys from Sudan that finally made it to the states, maybe a baby he helped deliver that's now 4-5 years old and wants to meet him. Give me more Will with kids content because it's adorable and I'm pretty sure I am not the only one craving this.
- Have Will's colleagues stand up for him for once even if he is wrong. Someone really needs to show that boy that he is appreciated and like that, that he has the support from many people and that they would love him be it the wrong or the right thing he did. I screw things up every few days, yet my friends haven't yelled at me like I did the worst possible thing, or told me to get out, only because I made A MISTAKE. It's why it's called a mistake, gee. Granted, it's not the work environment one would face in Will's case, but work is also a relationship. Just be there for Will, people!
And to sum it all up:
GIVE WILL HALSTEAD A BREAK, PEOPLE!
Stronger or weaker person notwithstanding, they would have broken so many times by now if they went through all that Will went through.
Oh and:
P.S. 1: I'll never forgive Goodwin for what she said in 1x18, that the only reason she okayed the offer to Will was because she wanted to see how and when he'll get himself fired. I believe the exact term was how long will it take. Sorry, writers, irl, if my future employer says that, I am out of there the second that is said. No way I am staying to prove someone's point. Besides, if she didn't trust him for him then, then what's the point to get up every day for work when it won't matter to her or anyone? Yes, you will save the lives, but at what cost?
P.S. 2: Connor should have told Will what he did to save his life. It feels to me like that was an important thing to tell someone who is a close friend in the least. Will deserved to know.
P.S. 3: Will Halstead is a precious boy who deserves the world. He needs to be loved, held and cherished. Protect the boy at all costs.
And yes this and much more has been discussed with @thethistlegirl over the course of the last two months and even though she doesn't watch the show, she agrees with me wholeheartedly.
WILL NEEDS TO LEARN THAT HE IS WORTH IT!
I think that's all. For now, lol. We never know when my ranting urges will return.
#chicago med#one chicago#will halstead#Nade rants#I had the urge to rant about this boy I love so much#my ramblings
16 notes
·
View notes
Text
Going to 2 different used book stores today with my older brothers Theo & Liam was the highlight of the day.
Tomorrow I go to the doctor to hopefully get all my stitches out from my heart surgery. Progress...
& dad will be home from drill in the morning
P.S. shout out to my mother...she recently moved up rank in the navy. Way to go! Shes a badass and has such a big heart. Love her 💛

#growing up millitary#health problems#heart surgery#mitral valve regurgitation#mitral valve prolapse#doctor appointments#bookworm#used book stores#shopping#big brothers
0 notes
Link
Most heart valve problems involve the aortic valve or mitral valve. Download this infographic to learn about two common valve issues: aortic stenosis and mitral regurgitation.
2 notes
·
View notes
Text
Title: Mitral Valve Repair: Procedure Details and Recovery

The mitral valve, one of the heart's vital components, plays a crucial role in ensuring the unidirectional flow of blood from the left atrium to the left ventricle. When the mitral valve malfunctions due to conditions such as mitral valve prolapse, regurgitation, or stenosis, it can impair cardiac function and lead to serious health complications. Mitral valve repair surgery is a highly effective treatment option for correcting these issues and restoring optimal heart function. In this comprehensive guide, we'll delve into the details of the mitral valve repair procedure, as well as the recovery process, shedding light on what patients can expect, including insights specific to mitral valve surgery in Indore.
Understanding Mitral Valve Repair Surgery:
Preoperative Evaluation: Before undergoing mitral valve repair surgery, patients undergo a comprehensive preoperative evaluation, which may include imaging tests such as echocardiography, cardiac catheterization, and MRI scans. This evaluation helps the surgical team assess the severity of the mitral valve condition and plan the most appropriate course of treatment.
Surgical Approach: Mitral valve repair surgery can be performed using either traditional open-heart surgery or minimally invasive techniques. In traditional open-heart surgery, a sternotomy is performed to access the heart, whereas minimally invasive approaches involve smaller incisions, resulting in reduced trauma and faster recovery times. Patients undergoing mitral valve surgery in Indore can benefit from the expertise of skilled cardiac surgeons who utilize advanced surgical techniques tailored to each patient's unique needs.
Repair Techniques: During the mitral valve repair procedure, the surgical team employs various techniques to restore proper valve function. These may include repairing or reinforcing the valve leaflets, reshaping the valve annulus, or repairing the chordae tendineae that support the valve structure. The goal is to eliminate valve leakage (regurgitation) or obstruction (stenosis) while preserving the natural anatomy of the valve as much as possible.
Valve Replacement vs. Repair: In some cases, mitral valve replacement may be necessary if repair is deemed unfeasible or unlikely to provide long-term benefits. Valve replacement involves removing the damaged valve and replacing it with a mechanical or biological prosthetic valve. However, whenever possible, mitral valve repair is preferred over replacement due to its superior long-term outcomes and reduced risk of complications.
Mitral Valve Repair Recovery:
Pain Management: Patients may experience some discomfort or pain following mitral valve repair surgery, which can be effectively managed with pain medications prescribed by the medical team. It's essential for patients to communicate any pain or discomfort they experience to their healthcare providers to ensure optimal pain management throughout the recovery process.
Physical Activity and Rehabilitation: While recovering from mitral valve repair surgery, patients are encouraged to gradually resume physical activity as guided by their healthcare providers. Initially, activities may be limited to light walking and gentle movements, with gradual progression to more strenuous exercises as tolerated. Cardiac rehabilitation programs may be recommended to help patients regain strength, endurance, and overall cardiovascular health.
Lifestyle Modifications: Following mitral valve repair surgery, patients are advised to adopt heart-healthy lifestyle habits to promote long-term cardiovascular health. This may include maintaining a balanced diet, engaging in regular exercise, quitting smoking, managing stress, and adhering to any prescribed medications.
Patients seeking mitral valve surgery in Indore can benefit from a multidisciplinary approach to care, with collaboration between cardiac surgeons, cardiologists, anesthesiologists, and other healthcare providers to ensure optimal outcomes and patient satisfaction. Additionally, the availability of minimally invasive surgical techniques in Indore allows for reduced recovery times and enhanced patient comfort compared to traditional open-heart surgery approaches.
Mitral valve repair surgery is a highly effective treatment option for correcting mitral valve disorders and restoring optimal heart function. By understanding the procedure details and the recovery process, patients can approach mitral valve repair surgery with confidence, knowing what to expect and how to facilitate a successful recovery. Prioritize heart health with best cardiologist Indore can access ensuring the best possible outcomes for their heart health journey.
#cardiologist indore#best heart specialist in indore#best cardiologist doctor in indore#breast specialist doctor in indore#heart doctor in indore
0 notes
Last Seen Blogs

bansheethings
The Banshee Things.
mymelodramaticjournal
jk r*wling didnt so i did

mutsukiss
oh lord, there is horror in my bones

l0nelym0on
ryan ross opens my pores and moistures my skin

tombraidermovies
Tomb Raider Movies