#penrose drain
Text
my drains are out I’m ready to party
3 notes
·
View notes
Note
hi Trench! I recently started considering the havanese breed for my future dog (a couple years from now) and I was wondering what your favourite and least favourite experiences with Whim have been? so far I think they have a good energy level for me, and honestly, Whim is just so charming
Favorite experience with Whim is anytime we go camping. There is nothing better on this earth than spending a few days running around in the woods with your dog. Eating meals by the fire. Sharing the sleeping bag. It's like yeah. I can see why we domesticated you.
Also her reduced prey drive and strong recall + attentiveness to me, means that I can let her off leash (when it's legal) and be pretty confident that she won't leave my line of sight. She's got a GPS collar just in case but I've never needed it.

Least favorite experience with Whim was when she was attacked by a dog. Because I rushed her to the clinic I work at, I was present for her being restrained, catheterized, sedated, and for her (fortunately minor) surgery. I wish I hadn't been.
She tried to bite staff and needed 3 people to restrain her + a muzzle before the drugs kicked in. It's a level of stress I've never seen her reach before.
Yesterday I restrained her solo and unmuzzled for a blood draw and she was calm and still. So it was extremely atypical behavior for her which only served to highlight how much pain she was in.
In hindsight I wonder if my own stress made her worse (we often see animals behave better for us in clinic when the owner is not present). I couldn't bring myself to leave her at the time, and I'll never get those images out of my head.
We made it through with only minor scarring and some increased dog reactivity. I've been happy with her progress behavior-wise. Last week she initiated play with a larger dog, which she hasn't done in months!!!
This is probably not very helpful to your dog breed decision making, sorry. But I'll take this moment to soapbox that if a dog is picked up and shaken by another dog that is a medical emergency, call your vet. Also learn some defensive handling from the IAABC or something.
Image of Whim with a penrose drain below the cut:

#animal injury cw#whim the havanese#alt text#tbh the fear of a dog fight is probably the worst part of owning a small dog#asked and answered#anonymous
8 notes
·
View notes
Text
Some dude had a penrose drain that got completely sucked up into a wound from a former I&D site on his penile shaft extending toward the scrotum. I sure enjoyed dealing with that one. But for the curious, yes, I found it and got it out.
17 notes
·
View notes
Text
i hate that i feel like drained and too exhausted to feel like revisiting Penrose just after making one thing for it. but this is a common thing that happens where i work on a oc story and it just gets too tiring and i lose interesting to do more with it. it sucks bc i just know full well i can make sooo much more content for fandom than oc stuff.
and i recognize its because fandom works off of existing material, so i dont have to make the whole world or characters myself! and its great, i love that. but i end up getting frustrated with myself bc i feel like if i can do all that then why cant i do that for myself??
in some ways i feel like im not legit if i cannot make these oc stories actually exist. i want to. i want to be an artist who makes cool oc stuff. but i just dont. its like i have been told too much that oc stuff that takes off is important, and fandom content is lesser because it cant be "used" in outside ways. which ties into the push to make you profit off of your work.
but anyways. this feeling that my fandom content is lesser 100% feeds into why i run off to sideblogs for the Thing. i have been super absent here after my obsesion with mcyt returning and it was especially out of shame, and then after admitting it i still didnt like sharing it here bc i felt like all fandom needed to be seperate and that mixing it with this blog would somehow ruin this blog's intent and drive any attempt at an audience away. cuz, what if they dont like the fandoms i keep drawing for and spamming on their dash??
even right now! i am unloading my sudden interest in Lisa and i keep thinnking , "man, i shouldnt be doing that. i need to separate it." and a lot of then time with a smaller thing, those side blogs often fail and i get no discussion and i fall out of the thing. other times, like my mcyt blog, i take off and run with it so hard that its also like i started a new identity entirely.
obviously i have no plans to tear down my sideblog, esp those i am active on, but like. i just really need to stop doing that. ill deal w the struggle i have on making oc content later i just really need to unlearn the feeling that fandom content isnt as good for me to focus on if i really wanna do it.
3 notes
·
View notes
Text
Seasonal Gutter Cleaning: Best Practices for Each Time of Year
Seasonal gutter cleaning is essential for maintaining the health and integrity of your home's exterior. Each season brings unique challenges and weather conditions that can affect the condition of your gutters. In this article, we'll explore the best practices for seasonal gutter cleaning and provide tips for keeping your gutters clean and free-flowing throughout the year.

Spring Gutter Cleaning
Spring is an ideal time to tackle gutter cleaning after the winter thaw. Remove leaves, twigs, and debris that have accumulated over the winter months.
Inspect gutters for damage caused by ice and snow buildup, such as cracks, leaks, and loose fasteners. Repair any issues promptly to prevent water damage.
Check downspouts for clogs and ensure that they are directing water away from your home's foundation.
Trim overhanging branches and foliage to prevent debris from falling into gutters and causing clogs.
Summer Gutter Maintenance
Summer is a good time to perform routine maintenance and inspections on your gutters. Remove any remaining debris and check for signs of wear and tear.
Clean gutters and downspouts with a garden hose to remove dirt, dust, and pollen buildup. Ensure that water is flowing freely and draining away from your home.
Inspect gutter guards and screens for damage or blockages and clean or replace them as needed.
Consider installing gutter guards or leaf screens to help prevent debris buildup and reduce the frequency of cleaning.
Fall Gutter Cleaning
Fall is the most critical time for gutter cleaning as leaves, pine needles, and other debris can accumulate quickly. Clean gutters regularly to prevent clogs and water damage.
Use a gutter scoop or trowel to remove leaves and debris from gutters and downspouts. Dispose of debris in a compost pile or yard waste bin.
Inspect gutters for signs of sagging, rust, or corrosion, and repair or replace damaged sections as needed.
Check roof valleys and areas where leaves tend to accumulate for signs of blockages and clear them to ensure proper water flow.
Winter Gutter Maintenance
Winter gutter maintenance is essential for preventing ice dams and water damage during cold weather. Keep gutters clear of snow and ice buildup to prevent ice dams from forming.
Use a roof rake or snow removal tool to safely remove snow from the roof and gutters. Avoid using metal tools or sharp objects that could damage gutters.
Install heat tape or gutter heaters to help prevent ice dams and keep gutters free-flowing during freezing temperatures.
Monitor gutters for signs of ice buildup and remove icicles and ice dams promptly to prevent damage to gutters and roof shingles.
Summary
Seasonal gutter cleaning is essential for maintaining the health and integrity of your home's exterior. By following these best practices for each time of year, you can ensure that your gutters remain clean, free-flowing, and in good condition throughout the year. Regular gutter maintenance helps prevent water damage, structural issues, and costly repairs, ensuring that your home remains safe, dry, and well-protected from the elements.
Contact us,
Name: Pro Waterblasting
Address: 7 Olive Road, Penrose, Auckland 1061, New Zealand
Phone: 0800 900 152
0 notes
Text
I'm not gonna elaborate too much but I have 2 latex tubes going from the inside of my mouth to outside my jaw to drain the infection. It's called a Penrose drain.
When they placed the drains they also put in a permanent plate where my jaw was fractured. There were bone fragments and tissue that made the area get really infected.
If I was to leave the hospital before the infection is gone she said the plate won't heal properly and that's also why I can't open my mouth all the way, the infection is causing my jaw muscles to not function fully.
So until all of the infection is out I'm kinda stuck here. I've been doing everything I can to take care of it. I deep clean it very gently to ensure i don't get sepsis and I've been rinsing my mouth and gently brushing and trying to push any infection out but its still just draining.
I'm just sad lol. I'm on a clear liquid diet and that means that the only things I'm served are: chicken or beef broth, a jello (maybe), an Italian ice (that is melted), an apple juice, and a coffee.
My mom brought me some juice I asked her for today that is clear so I can have that now but I'm literally not even eating because it's gross and I'm tired of greasy water.
I just want to be able to have something in my system. I literally haven't eaten actual food besides a single bowl of mashed potatoes in 2 weeks. At this point I'm not even eating the food I'm just drinking my juice.
I just want to be able to eat but even once I'm discharged, my surgeon doesn't want me to have dairy or chew anything for 6 weeks. So even once I'm discharged I'm basically just going to be able to eat baby food type shit.
I had a really good day at first because I was seeing progress with the drains, i was even able to shower and walk around my room a bit. So I was hoping the drains would get removed tomorrow and then maybe I get discharged the next day and at least get better slowly at home with my food and bed.
I'm just really depressed now. I just don't know what to do and not eating is making me crazy, fuck.
That just really made me upset when she came an hour ago and I'm still trying to deal with it.
For someone who used to want to be skinny so bad, I'm finally getting my wish. I'm losing so much weight from this. My bones are touching so much. My spine is showing again, I'm veiny and getting lankier but... It's for once not my main goal.
At this point I just want to be healthy.
A healed mouth that is capable of eating and filling me with food instead of sadness.
0 notes
Text
Pn5
You are the nurse receiving report on your patient that was admitted as an emergency earlier in the day. A 64-year-old female underwent a right colectomy. The right side of her colon was removed due to cancer. She has a history of smoking & no other health problems. She is currently being transferred to you in PACU. She has a midline incision with a Penrose drain, a stab wound w/ a Jackson Pratt…
View On WordPress
0 notes
Text
Kidney transplant surgeon simulator animated

#KIDNEY TRANSPLANT SURGEON SIMULATOR ANIMATED SIMULATOR#
ĭuring a transplant surgery rotation, the high service demand of care for medically complex patients often negatively impacts operative room access for residents. However, residents on average participate in only 5.9 ± 7 kidney transplants during their entire training, with 30% lacking the confidence to perform vascular anastomosis by the time they graduate. Out of all transplant procedures, kidney transplant usually provides the best opportunity for residents to significantly put into practice vascular anastomosis, a skillset they are rarely exposed to on other surgical rotations. In the current 80-hour workweek restriction environment set by the Accreditation Council for Graduate Medical Education, the traditional Halstedian apprenticeship model of graded responsibility is likely insufficient to consistently meet the quantitative and qualitative education demands of general surgery residents while simultaneously preserving patient safety, especially during transplant surgery rotations.
#KIDNEY TRANSPLANT SURGEON SIMULATOR ANIMATED SIMULATOR#
Our novel low-cost bench-top kidney transplant surgery simulator focusing on vascular anastomoses received positive educational feedback from residents. Residents thought that the simulator was less difficult than real-life procedure, had acceptable fidelity levels, and they highly rated its educational utility. The iliac fossa and allograft cost $20.20 and each practice run cost $7.20. Residents performed and assisted in vascular anastomoses on the simulator. A modified kidney-shaped stress ball with 1.27 x 4, 0.64 x 4, and 0.64 x 15 cm Penrose drains replicated a kidney allograft with its vein, artery, and ureter, respectively. Hooks attached to the box’s sidewall held under tension 1.27 and 0.64 cm diameter Penrose drains to replicate the external iliac vein and artery. ResultsĪ 35.9 x 19.4 x 12.4 cm plastic box mimicked the iliac fossa. Eighteen residents with real-life kidney transplant experience trialed the simulator and scored its fidelity and educational utility on a 0-100 visual analog scale (VAS) survey. We searched for inexpensive materials to design an iliac fossa and kidney allograft. In light of this, we created a low-cost bench-top kidney transplant surgery simulator to help residents practice vascular anastomoses. Resident inexperience during time-sensitive vascular anastomoses of a kidney transplant can negatively impact outcomes.
0 notes
Text
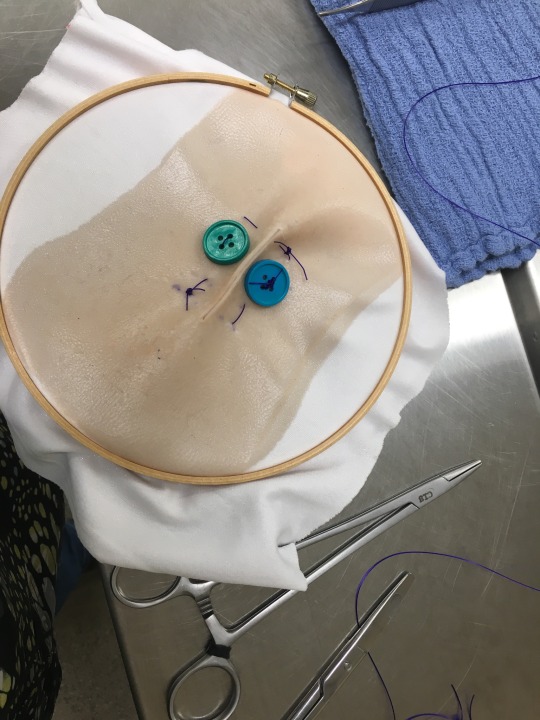
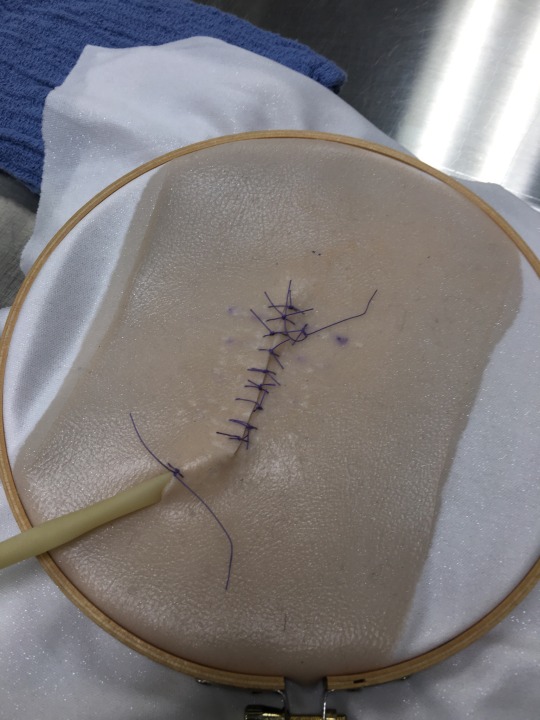
Took a break from studying to work on some surgery skills in our sim lab- which was a good call, because my brain feels like a noodle and we have two exams next week...
Got to place a penrose drain and practice tension relieving patterns with buttons!
#vet student#vet school#vetblr#veterinary medicine#studying#surgery practice#surgery#sutures#penrose drain#suture skills
12 notes
·
View notes
Text
Always take your dog to the vet after a bite
Ok, but why?
Warning: discussion of animal injury, veterinary surgical procedure, and images of a bite wound below the cut.
This is not a substitution for veterinary or medical care, if you or a pet has been bitten, seek professional help immediately.
Bite wounds are very deceptive. Injuries may not be visible. Broken bones and pneumothorax don't require a puncture through the skin to wreak havoc on the body. Dog bites exert a lot of crushing and shearing force on tissues below the skin.
When you see a puncture wound from a bite, it will likely look small and it may not bleed much. As a result, it is easy to assume the injury will heal well on its own, without veterinary intervention. Do not be fooled. The danger is not in the small visible portion of the wound, but in what lies beneath.
I'm talking about dead space. During a bite, tissues can be ripped from their attachments and die, resulting in a cavity beneath the surface of a wound. This cavity is dark and moist, airflow is limited, and it fills with blood and other fluids. Bacteria love the dark and wet, so wounds with dead space can easily become abscessed.
Whim's visible puncture is less than half a centimeter in diameter. Not very concerning on its own.

When it was lavaged the vet discovered over an inch of dead space.
Without veterinary intervention, the small outer surface of the wound could close, leaving infection to fester in the area beneath the skin, with no visual indicator of what is going on until an abscess forms.
So how is healing promoted? In Whim's case, the best option was to sedate her and install a Penrose drain.

Whim's initial puncture is at the top of her back, with the drain passing through the dead space and exiting lower down. This allows gravity (and capillary action) to do most of the work to drain the wound of excess fluid. The dead space will heal and shrink around the the drain over time, decreasing the likelihood of infection in the wound once the drain is removed. They are ideal for small pockets of dead space and can be removed a few days after placement. Other drains exist and may be more appropriate depending on the injury.

Whim had 6 visible puncture wounds, all of them looked similar from the outside, but only one of them had a large pocket of dead space. You cannot tell the severity of a bite wound from looking at it, you must have your animal assessed by a licensed DVM.
I hope this has been informative to those of you interested in veterinary medicine. Do not treat this as any kind of instruction manual for caring for your animal at home. My only instruction is talk to your veterinarian.
P.S. some dogs like to try and eat their drains (hello lab owners). Depending on the location of the drain, a surgical shirt or an elizabethan collar may be appropriate to prevent this.
#am i coping with how upset i am about this by blogging about vet med? maybe#did i write this essay instead of the one i have for homework? maybe#images are my own. you do not have my permission to share them anywhere.#feel free to reblog the post though.#vetmed#veterinary medicine#whim health#wound care#animal injury cw#gore cw#images have been described with alt text
40 notes
·
View notes
Text
weirdest use for equipment you've ever seen/done? ill go first:
i used a penrose drain as a limp straw so I could drink coffe while gloved up
and go!
#veterinary shitposting#veterinary medicine#veterinary#vetblr#vetmed#vet#yeeeee#abuse of penrose drains
357 notes
·
View notes
Text

DISCLAIMER: this is for educational & writing purposes only, if you're planning on getting top surgery, please consult with a surgeon of your choice or trusted individuals who have gone through with the procedure.
BUTTONHOLE
the buttonhole technique is an ideal FTM Top Surgery procedure for those who prioritize nipple-areola size, positioning, sensation & pigmentation.
this technique enables the removal of larger amounts of breast tissue & skin than the keyhole & peri - areolar methods, making it a good choice for those who are larger-chested.
patients are left with two penrose drains ( small tubing that exits through the pectoral incisions and drains excess blood and lymphatic fluid into a dry pad ) that are left in until the first follow - up appointment.
DOUBLE INCISION ( bilateral mastectomy, mastopexy )
the double incision technique is the most widely-used technique & is ideal for those who are medium to large chested.
during this procedure, the skin on the chest is opened along two horizontal incisions ( at the top and bottom of the pectoral muscle, the muscle itself is not touched ) & the skin is pulled back & the breast tissue is then removed.
patients are left with two medical drains under the skin that exit through a small incision under each arm with a reservoir bulb attached at the ends to collect excess blood & lymphatic fluid. these drains are left in for several days to a week, & need to be emptied by the patient a few times a day.
INVERTED - T / T - ANCHOR ( inferior pedicle, wise pattern )
the inverted - t technique is ideal for medium to large chested individuals who wish to retain the most sensation possible in the nipple-areola complex.
this procedure is similar to the double incision method as the skin on the chest is opened along two horizontal incisions ( at the top & bottom of the pectoral muscle, the muscle itself is not touched ) & the skin is pulled back & breast tissue is removed.
this method also has the potential for less complications compared to the double incision technique because there are no nipple grafts ( which have a risk of infection & loss ). general anesthesia is used, but patients are rarely catheterized.
PERI - AREOLAR ( peri, peri - areolar concentric circle )
the peri - areolar technique is ideal for those who are small chested, or those with b - sized chests & good skin elasticity.
during this procedure, an incision is made all around the border of the areola. additionally, a second, larger concentric circle incision is made & the resulting ring of skin removed. breast tissue is removed & additional contouring with liposuction may be performed.
a " drawstring " technique is used to bring the skin together & connect it to the edges of the areola, which may be downsized. with peri - areolar, the nipple stalk is usually left intact, though some surgeons will resize the nipple itself. the nipple stalk & nerve are not severed, sensation is often maintained.
KEYHOLE
the keyhole technique is ideal for those who are small chested. during this procedure, a small incision is made along the bottom of the areola, & the breast tissue is removed with liposuction through this incision.
the nipple stalk is usually left intact, though some surgeons will resize the nipple itself. the areola is not resized & nerve sensation is maintained.
MINIMAL SCAR
the minimal scar technique is an ideal procedure for trans men with smaller chests & excellent skin elasticity. this surgery involves only small incisions on the side of the chest and part way around the areola.
this minimally - invasive procedure leaves nearly invisible scars after healing & nipple sensation is retained, making it an excellent choice for the right patient.
DOG EARS
" dog ears " is a term that refers to excess skin & fat that " pucker " out at the primary incision lines as they go around the sides of the chest in double incision top surgery. they can also form at the point where incisions come together near the center of the chest.
functionally, dog ears don't cause a problem, but many see them as visually unappealing, & is one of the most common reasons for a revision. massaging dog ears after surgery can have a positive effect, especially if surgical swelling is present.
regardless of the surgeon or technique, dog ears can still develop after top surgery. post - operative weight gain — as well as dramatic weight loss — can both cause dog ears to appear.
in cases where multiple surgeries are required to remove excess skin, dog ears can be expected. while dog ears usually require surgery to correct, the revision can often be done without sedation. It's best to wait about 6-9 months before doing a revision. This allows results to “ settle, ” & sometimes that's all that's needed to resolve minor cosmetic concerns.
#rp resources#roleplay resources#roleplay help#HELP IDK WHAT TO TAG THIS !!!!#mod: mocha#first post here u go *smoochies*#writing trans characters#trans resources
29 notes
·
View notes
Text

6 weeks post op 🤗
Just in case yall were wondering what I meant by "adhesive gave me a rash" theres basically a square around each side of my chest where the tape was (hard to see here) but thats way better than the two lines on either side of my nips from where Id tried the adhesive gauze. Its been 4 days. Its definitely healing though, it doesnt sting if i touch it.
Also, despite what it looks like, my drain sites are 99% healed. If anyone knows when they stop looking so weird, Id love to know. Although Dr. Wolf uses different drains than most. I think theyre called penrose drains??? Idk they look the same.
Otherwise I think my chest looks pretty good. I cant wait til i can get started on scar care.
11 notes
·
View notes
Text
lupine publishers|Combination of Turner Syndrome Crohn’s Disease and Thyroiditis a Rare Occurrence
Combination of Turner Syndrome Crohn’s Disease and
Thyroiditis a Rare Occurrence
Abstract
Turner’s syndrome is a genetic condition in the female population caused by the partial or complete loss of X-Chromosome.
Previous case reports in the literature and prior studies established the association between Turner’s syndrome and multiple
Autoimmune Diseases (AID). We present a 38-Year-old female with Turner’s syndrome, Thyroid disease and multiple admissions
for Fistulizing Crohn’s disease. X chromosome deletions and alterations predispose to auto-immune antibodies per prior studies.
Introduction
Turners Syndrome is seen in 1 in 2000 to 1 in 2500 live female
births. Predisposition for Autoimmune Diseases (AID) occurs
in 30- 40% of these patients. In the past there have been cases
reported with Turner syndrome and Inflammatory bowel disease,
and Turner syndrome and Thyroiditis. However, there is limited
data reporting the combination of multiple autoimmune diseases:
Turner syndrome, Inflammatory Bowel Disease, and Thyroiditis.
In light of this we present a case of Turner syndrome, associated
with hypothyroidism and Crohn’s disease who underwent partial
colectomy with colostomy presenting with Colo-cutaneous fistula.
Case Report
A 38-year-old female who is a known case of Turner syndrome
with Hypothyroidism on thyroxine replacement, Crohn’s disease
post left hemicolectomy with colostomy and Colo-cutaneous
abdominal wall fistula, Osteoporosis with history of femoral neck
fracture presented with pus discharging wound on the anterior
abdominal wall for a few days. She also had a painful erythematous
rash over the right half of the face. On physical examination, her
height is 121.9cm and her Weight is 50.5kgs. Hematology work-
up revealed anemia with Hemoglobin and Hematocrit of 11g/dL
and 33.2%. Thyrotropin receptor antibody (TSH Ab) of <1.10 IU/L
(Normal range:0-1.7IU/L), Anti-Thyroglobulin Antibody of 1.5 IU/L
(Normal Range:0-0.9IU/L) and Anti-Thyroid Peroxidase antibody
(TPO Ab) of 35 IU/L (Normal range: 0-34IU/L). CT scan of the
abdomen showed evidence of Colo vesical fistula and Peri colonic
inflammation with fat stranding (Figure 1). Patient underwent
Incision and Drainage of the Colo-cutaneous fistula and placement
of Penrose drain. Culture and sensitivities were obtained,
and appropriate antibiotics were started. Patient underwent
colonoscopy later which showed erythematous, friable mucosa, a
hemorrhagic appearance and ulceration 5 cm from the Colostomy
opening (Figure 2) Biopsy of the lesion showed preserved crypt
architecture and lymphoid aggregates without acute inflammation
or lymphocytic infiltration. Patient was followed up with a USG
neck which showed a small, heterogeneous, and mildly hyperechoic
gland (Figure 3). Patient continues to be on levothyroxine. Dexa scan
showed a T score of -3.1 in the lumbar spine and -2.7 in the right
hip. Patient is on alendronate. Patient was discharged with follow-
up in the Gastroenterology clinic and is currently on Vedolizumab.
Discussion
The case mentioned above emphasizes the association of
autoimmune disorders in patients with Turner’s syndrome. Female
sex has a predisposition for AID. Patients with Turner syndrome
have twice the risk compared to the female population. The cause
of autoimmunity in Turner’s syndrome has been theorized and
studied without a definitive answer. X chromosome genes including
a Major Histocompatibility complex were found to play a major role
in immune response [1,2]. Haplo-insufficiency [3,4], alterations and
microdeletions of the X chromosome are one of the major attributed
causes for AID. Turner syndrome females with chromosome Xp
deletion showed a higher prevalence of thyroid and Crohn’s disease
[4].
Lack of exposure to self-antigens in the thymic epithelial
cells and T-cells with autoreactivity can also be the cause for
auto-immunity [2,3]. Turner syndrome patients were found to
have low levels of Immunoglobulin G and M in some studies [5].
Exposure to estradiol treatment has also been debated to be a
trigger for AID development through hormonal imbalance inciting
immunopathogenic response [6]. Further studies on the link
between AID and X chromosome can help to clearly understand the
pathogenetics involved. The most common AID in Turner’s appears
to be related to the thyroid gland. Hypothyroidism is more common
compared to hyperthyroid disease. Ulcerative colitis, Crohn’s
disease, celiac disease, juvenile rheumatoid arthritis, diabetes
mellitus, Addison’s disease, psoriasis, vitiligo and alopecia. This
patient was diagnosed with Hashimoto’s thyroiditis and Crohn’s
disease around the age of 20. The patient had a femoral neck
fracture and osteoporosis diagnosed around 25 years of age. Many
patients have sub clinical presentations and close follow up of
patient’s symptoms is necessary. Medical management in patients
with Turner’s syndrome should include screening and monitoring
for AID regularly with appropriate treatment. The Turner syndrome
study group published guidelines on Screening and medical care for
turner’s syndrome patients.
for more information about LOJ Medical Sciences archive page click on below link
https://lupinepublishers.com/medical-science-journal/archive.php
for more information about lupine publishers page click on below link
https://lupinepublishers.com/index.php
#lupine publishers group#LOJ Medical Sciences#Screening and medical care for#turner’s syndrome patients
3 notes
·
View notes
Text
Veterinary Chest Drains
Anonymous said to @ask-drferox: Hmm. I must not understand how a chest drain would work. If you ever get the time, could you talk about chest drains, and maybe penrose/surgical drains in general? If you leave a chest drain in, wouldn’t that cause the intrapleural pressure to equalize, this not slowing the lungs to inflate?
I wonder if perhaps you’re thinking of a penrose drain as the default, which isn’t what you want for a chest at all.
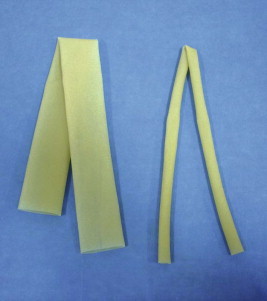
A penrose drain is just a little rubber tube. It’s soft, simple, super duper cheap and usually used for manky soft tissue wounds that do NOT enter a body cavity. Sometimes vets will even use the finger from a glove instead of a proper penrose if they want something smaller, that’s what they’re like.
There’s lots of pictures of them in use on the internet, but they’re frankly a bloody mess so have a diagram instead.
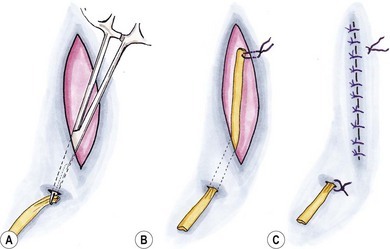
The drain runs through the draining space within the wound, never parallel to the surgical margins itself. Often we’ll have both ends of the drain sticking out through the skin and leave it there for a few days until the draining fluid dries up. They work with gravity and capillarity.
Typically you’d use them for cat bite abscesses and dog fight wounds. They’re already infected, doesn’t matter too much if they’re not perfectly sterile, and reasonably comfortable. (Just hope the dog in particular doesn’t try to eat them)
While there are numerous types of chest drains (and you can use similar things for abdominal drains too), they typically look a bit like this:
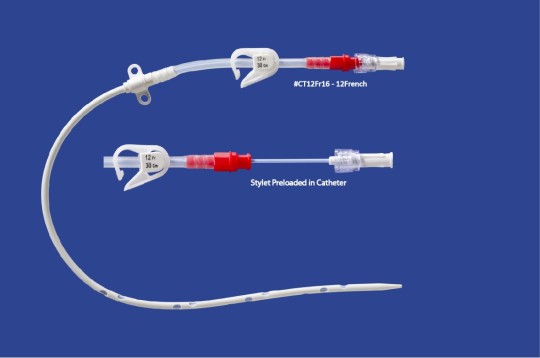
The fenestration bit at the bottom is surgically placed in the chest (or at least under local and a stab incision), and the top part sits outside of the chest. It’s clamped shut, so sealed, unless you’re actively aspirating gas/fluid with a syringe. This sort might stay in place for days or weeks, and might be manually drained every few hours, daily, or every few days.
Sometimes we will attach something like a Jackson Pratt drain to the end of it instead. These are like lemon-sized balloons which we deflate before attachment, and they provide slow, consistent suction for fluid and gas. They will inflate as they fill up, and you empty them as required.

The above picture is of a fresh, empty drain. The baloony bit will expand as it fills up, and you can visually see it.
Sometimes you don’t need anything so fancy though. For less complicated chest surgery, you might just close the chest, then use a needle or catheter to aspirate any trapped gas at the time and monitor closely for the next day or so. Depends entirely on context.
Chest drains need to be one-way. You would not put a penrose drain into the chest cavity, as it will allow air to go both ways when the patient inhales. That’s a certain way to cause a pneumothorax. So your gut feeling of ‘penrose in chest is bad’ is absolutely correct.
Now if you leave a proper chest drain in place, it will cause a little irritation and fluid build up, because it’s a foreign object inside the thorax. So you don’t remove them when the fluid they’re collecting is zero, but rather when it’s below threshold for re-absorption.
There are lots more pictures available on the internet, but they’re more gorey than I prefer to post on this blog.
133 notes
·
View notes
Last Seen Blogs

sootsprite-sprinkles
SootSprite Sprinkles

deepmilkshakedestiny
Untitled

identidade-v
A multishipping mess

mylifeisamusicalreference
Professional Nuisance
architects-cut
Architect's cut