#50 states reviews
Text
Hawk’s 50 states reviews update: 44/50 done, six left… 👀
#what the FUCK do I do in Nebraska or Kansas#other than get lost in corn#50 states reviews#send help
4 notes
·
View notes
Text
that post about the yuri girl reading State and Revolution reminded me of this conversation I had with my gf a little while ago
#this too is yuri#cw 50 shades of gray#rambles from the moonsink#she did have state and revolution by the way#it was very nice to look at#maybe I have time to read it too at some point#also ftr so she doesn't murder me:#my gf does not like 50 shades#she's just really into youtube reviews dissecting it
15 notes
·
View notes
Text
His Pretend Baby by Theodora Taylor
5 stars
audiobook
OMG, these two were perfect together! The more their story unfolded, the more I loved them <3
#Theodora Taylor#His Pretend Baby#Her Ruthless Boss series#50 Loving States series#Kobo Plus#Audiobook#am reading#read romance#romance reader#romance books#read#romance#books#reader#bibliophile#book love#book blogger#book review#steamy reads
0 notes
Text

I finally got it
#this book by the way was expensive#I've got about 20 books on my wishlist JUST for things ancient Greece-related and half of them are over $50#you can't even GET Old Stones New Temples anymore#a few years ago there were some used copies that were like $600#Hellenion will give you a digital pdf copy if you join them which is great because it is so not worth hundreds of dollars#it was one of the first books written for Hellenic Polytheism but iirc the author converted to Christianity#and the book itself is kind of 'meh' in terms of quality#we've got waaaaaay more resources available now#I've got every single book on Hellenion's clergy education program list from when they had it listed publicly#and now I've started acquiring even more books that have come out over more niche subjects#I haven't gotten far into THIS one yet but the reviews were mostly positive while stating that it's very dry and technical#which gives me high hopes that it's not going to be some fluffy new age woo nonsense
1 note
·
View note
Text
214: "Various Bulgarians" // Le Mystère des Voix Bulgares vol. 2
Le Mystère des Voix Bulgares vol. 2
"Various Artists"
1988, Elektra Nonesuch
Incredibly annoying album to cite properly, I must say. Like its predecessor, Le Mystère des Voix Bulgares vol. 2 is usually credited to either the Bulgarian State Radio and Television Female Vocal Choir, who sing 10 of 17 songs collected here, or to the Swiss ethnomusicologist Marcel Cellier, who recorded most of these tracks over a 17-year period. (There is one recording of the Orchestra Yivan Kirev from ’57.) There’s a bit of an air of overaccentuated exoticism to how this stuff is packaged, from retaining the French title (with improper title casing!) for the English market release, to emphasizing Cellier’s curatorial work over that of the arrangers and performers in the narrative around the album. Realistically, we’d probably be better off crediting this one to Various Bulgarians, both for reasons of accuracy and because it’s an exceptionally melodic turn of phrase.
Listening to Le Mystère, though, I understand why those who championed this music hoped to keep it obscure. People consistently describe this stuff as sounding angelic, elven, ethereal, alien—yes, yes, yes, and yes. Wouldn’t want the realities of corrupt little Bulgaria, with its grim concerns about GDP and the Cold War, dirtying the seraphic mantle you know! The basis of these songs is not, to my ear, wildly far from the familiar choral music of Western Europe, but some combination of the brilliant syncopated vocal arrangements, the technical ability of the singers, and the Bulgarian language itself push the recordings into a realm of stranger light. The vocals often sound like the screams of beings with higher, more delicate instruments in their throats than regular humans have, and whether you envision a great stone cathedral or a starlit clearing in a pagan wood, it’s not hard to sense something holy transpiring here.
Anyway, here they are on Johnny Carson.
youtube
214/365
#le mystere des voix bulgares#bulgarian state radio and television choir#elektra nonesuch#folk music#choral music#'50s music#'60s music#'70s music#'80s music#marcel cellier#various bulgarians#bulgarian music#music review#vinyl record
1 note
·
View note
Text
Book Review: His Enduring Love
~ Warning! Minor Spoilers! Book Review: His Enduring Love/ Her Perfect Gift (50 Loving States #5, Illinois) by – Theodora Taylor {2012} ~
REVIEW
I read His Revenge Baby in 2019 and loved it. I rated it a 4.8 out of 5. I’ve always wanted to read more from this author, especially the book about the brother of the main characters from His Revenge Baby. Randomly, I recently looked up the book,…
View On WordPress
#50 Loving States#Book 5#book review#Book Series#Her Perfect Gift#His Enduring Love#Illinois#LilVakaVivLu#Theodora Taylor
0 notes
Text
50 Years, 50 Movies (1983): El Norte
50 Years, 50 Movies (1983): El Norte
I will turn 50 in November of this year, so my project for 2023 will be to watch and review one movie from each year of my life. The only qualification is that it has to be a movie I’ve not reviewed previously.
1983
Top Grossing Movies of 1983:
Return of the Jedi
Terms of Endearment
Flashdance
Trading Places
War Games
Best Picture Oscar Nominees and Winners of 1983:
Terms of Endearment
The…
View On WordPress
1 note
·
View note
Text
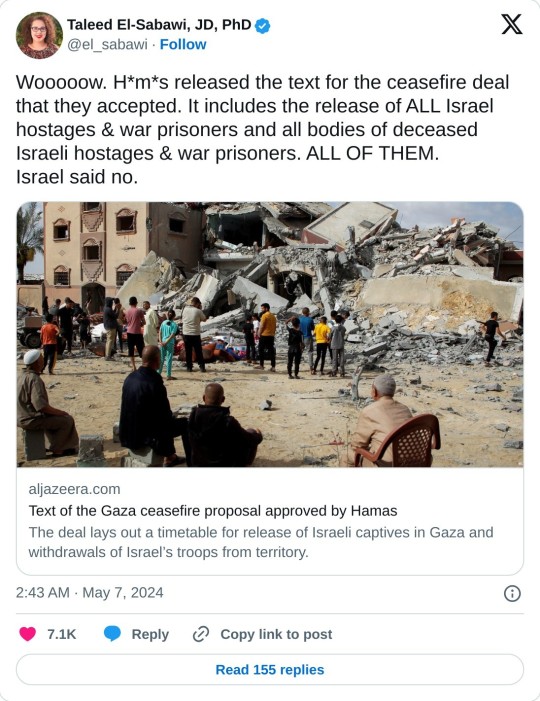
Al Jazeera has obtained a copy of the Gaza ceasefire proposal that Hamas said it accepted on Monday. The deal, which was put forward by Egypt and Qatar, would come in three stages that would see an initial halt in the fighting leading to lasting calm and the withdrawal of Israeli troops from the Palestinian territory.
The proposed agreement would also ensure the release of Israeli captives in Gaza as well as an unspecified number of Palestinians held in Israeli jails.
Israel has said that it does not agree to the proposal but that it will engage in further talks to secure an agreement – all while pushing on with its assault on Gaza.
Meanwhile, the United States, which is also involved in the negotiations, said it is reviewing the Hamas response.
The basic principles for an agreement between the Israeli side and the Palestinian side in Gaza on the exchange of captives and prisoners between them and the return of sustainable calm.
The framework agreement aims at: The release of all Israeli captives in the Gaza Strip, civilians or military, alive or otherwise, from all periods, in exchange for a number of prisoners held by Israel as agreed upon, and a return to a sustainable calm that leads to a permanent ceasefire and a withdrawal of Israeli forces from the Gaza Strip, its reconstruction and the lifting of the siege.
The framework agreement consists of three related and interconnected stages, which are as follows:
The first stage (42 days)
[Herein] a temporary cessation of military operations between the two parties, and the withdrawal of Israeli forces eastward and away from densely populated areas to a defined area along the border all along the Gaza Strip (including Wadi Gaza, known as the Netzarim Corridor, and Kuwait Roundabout, as below).
All aviation (military and reconnaissance) in the Gaza Strip shall cease for 10 hours a day, and for 12 hours on the days when captives and prisoners are being exchanged.
Internally displaced people in Gaza shall return to their areas of residence and Israel shall withdraw from Wadi Gaza, the Netzarim corridor, and the Kuwait Roundabout:
On the third day (after the release of three captives), Israeli forces are to withdraw completely from al-Rashid Street in the east to Salah al-Din Street, and dismantle military sites and installations in this area.
Displaced persons (unarmed) shall return to their areas of residence and all residents of Gaza shall be allowed freedom of movement in all parts of the Strip.
Humanitarian aid shall be allowed in via al-Rashid Street from the first day without any obstacles.
On the 22nd day (after the release of half the living civilian captives in Gaza, including female soldiers), Israeli forces are to withdraw from the centre of the Gaza Strip (especially the Netzarim/Martyrs Corridor and the Kuwait Roundabout axis), from the east of Salah al-Din Street to a zone along the border, and all military sites and installations are to be completely dismantled.
Displaced people shall be allowed to return to their places of residence in the north of Gaza, and all residents to have freedom of movement in all parts of the Gaza Strip.
Humanitarian aid, relief materials and fuel (600 trucks a day, including 50 fuel trucks, and 300 trucks for the north) shall be allowed into Gaza in an intensive manner and in sufficient quantities from the first day. This is to include the fuel needed to operate the power station, restart trade, rehabilitate and operate hospitals, health centres and bakeries in all parts of the Gaza Strip, and operate equipment needed to remove rubble. This shall continue throughout all stages.
Exchange of captives and prisoners between the two sides:
During the first phase, Hamas shall release 33 Israeli captives (alive or dead), including women (civilians and soldiers), children (under the age of 19 who are not soldiers), those over the age of 50, and the sick, in exchange for a number of prisoners in Israeli prisons and detention centres, according to the following [criteria]:
Hamas shall release all living Israeli captives, including civilian women and children (under the age of 19 who are not soldiers). In return, Israel shall release 30 children and women for every Israeli detainee released, based on lists provided by Hamas, in order of detention.
Hamas shall release all living Israeli captives (over the age of 50), the sick, and wounded civilians. In return, Israel shall release 30 elderly (over 50) and sick prisoners for every Israeli captive, based on lists provided by Hamas, in order of detention.
Hamas shall release all living Israeli female soldiers. In return, Israel shall release 50 prisoners (30 serving life sentences, 20 sentenced) for every Israeli female soldier, based on lists provided by Hamas.
The United Nations and its agencies, including UNRWA, and other international organisations, are to continue providing humanitarian services across the Gaza Strip. This shall continue throughout all stages of the agreement.
Infrastructure (electricity, water, sewage, communications and roads) across the Gaza Strip shall be rehabilitated, and the equipment needed for civil defence allowed into Gaza to clear rubble and debris. This shall continue throughout all stages of the agreement.
All necessary supplies and equipment to shelter displaced people who lost their homes during the war (a minimum of 60,000 temporary homes – caravans – and 200,000 tents) shall be allowed into Gaza.
Throughout this phase, an agreed-upon number (not fewer than 50) of wounded military personnel will be allowed to travel through the Rafah crossing to receive medical treatment, and an increased number of travellers, sick and wounded, shall be allowed to leave through the Rafah crossing as restrictions on travellers are lifted. The movement of goods and trade will return without restrictions.
And that's just phase one. Read the rest of the article for the rest of the ceasefire proposal approved by Hamas.
#yemen#jerusalem#tel aviv#current events#palestine#free palestine#gaza#free gaza#news on gaza#palestine news#news update#war news#war on gaza#ceasefire now#ceasefire deal#palestinian resistance#hamas
687 notes
·
View notes
Text
By: Andy L.
Published: Apr 14, 2024
It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Many trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics”, including Andrew Wakefield, has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
-
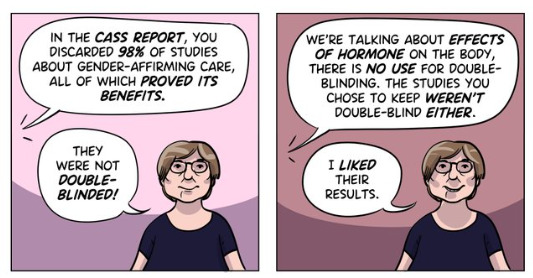
Myth 1: 98% of all studies in this area were ignored
Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
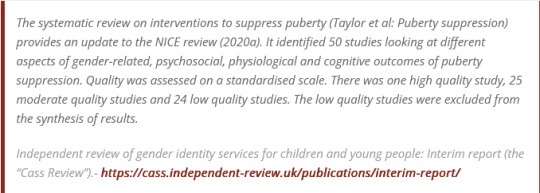
The Review states,
The systematic review on interventions to suppress puberty (Taylor et al: Puberty suppression) provides an update to the NICE review (2020a). It identified 50 studies looking at different aspects of gender-related, psychosocial, physiological and cognitive outcomes of puberty suppression. Quality was assessed on a standardised scale. There was one high quality study, 25 moderate quality studies and 24 low quality studies. The low quality studies were excluded from the synthesis of results.
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.
12 cohort, 9 cross-sectional and 32 pre–post studies were included (n=53). One cohort study was high-quality. Other studies were moderate (n=33) and low-quality (n=19). Synthesis of high and moderate-quality studies showed consistent evidence demonstrating induction of puberty, although with varying feminising/masculinising effects. There was limited evidence regarding gender dysphoria, body satisfaction, psychosocial and cognitive outcomes, and fertility.
Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,
One emerging criticism of the Cass review is that it set the methodological bar too high for research to be included in its analysis and discarded too many studies on the basis of quality. In fact, the reality is different: studies in gender medicine fall woefully short in terms of methodological rigour; the methodological bar for gender medicine studies was set too low, generating research findings that are therefore hard to interpret. The methodological quality of research matters because a drug efficacy study in humans with an inappropriate or no control group is a potential breach of research ethics. Offering treatments without an adequate understanding of benefits and harms is unethical. All of this matters even more when the treatments are not trivial; puberty blockers and hormone therapies are major, life altering interventions. Yet this inconclusive and unacceptable evidence base was used to inform influential clinical guidelines, such as those of the World Professional Association for Transgender Health (WPATH), which themselves were cascaded into the development of subsequent guidelines internationally.
-
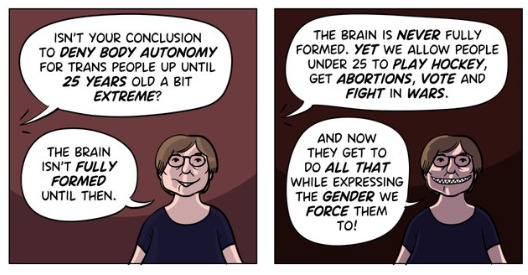
Myth 2: Cass recommended no Trans Healthcare for Under 25s
Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
Taking account of all the above issues, a follow-through service continuing up to age 25 would remove the need for transition at this vulnerable time and benefit both this younger population and the adult population. This will have the added benefit in the longer-term of also increasing the capacity of adult provision across the country as more gender services are established.
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
-
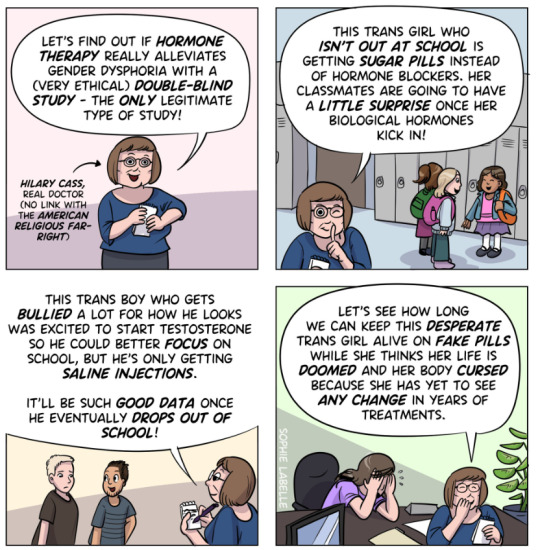
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”
Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions

The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1.
Explainer on the Newcastle Ottawa Scale
The Newcastle-Ottawa Scale (NOS) is a tool designed to assess the quality of non-randomized studies, particularly observational studies such as cohort and case-control studies. It provides a structured method for evaluating the risk of bias in these types of studies and has become widely used in systematic reviews and meta-analyses.
The NOS consists of a set of criteria grouped into three main categories: selection of study groups, comparability of groups, and ascertainment of either the exposure or outcome of interest. Each category contains several items, and each item is scored based on predefined criteria. The total score indicates the overall quality of the study, with higher scores indicating lower risk of bias.
This scale is best applied when conducting systematic reviews or meta-analyses that include non-randomized studies. By using the NOS, researchers can objectively assess the quality of each study included in their review, allowing them to weigh the evidence appropriately and draw more reliable conclusions.
One of the strengths of the NOS is its flexibility and simplicity. It provides a standardized framework for evaluating study quality, yet it can be adapted to different study designs and research questions. Additionally, the NOS emphasizes key methodological aspects that are crucial for reducing bias in observational studies, such as appropriate selection of study participants and controlling for confounding factors.
Another advantage of the NOS is its widespread use and acceptance in the research community. Many systematic reviews and meta-analyses rely on the NOS to assess the quality of included studies, making it easier for researchers to compare and interpret findings across different studies.
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
The national infrastructure should be put in place to manage data collection and audit and this should be used to drive continuous quality improvement and research in an active learning environment.
-
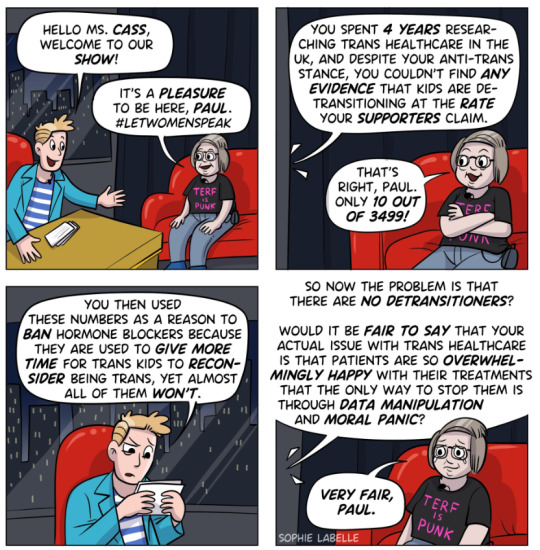
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.

Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:
Estimates of the percentage of individuals who embark on a medical pathway and subsequently have regrets or detransition are hard to determine from GDC clinic data alone.
There are several reasons for this:
Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
Gender dysphoria during childhood does not inevitably continue into adulthood. Rather, in follow-up studies of prepubertal children (mainly boys) who were referred to clinics for assessment of gender dysphoria, the dysphoria persisted into adulthood for only 6–23% of children.
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
==
It's not so much "myths and misconceptions" as deliberate misinformation. Genderists are scrambling to prop up their faith-based beliefs the same way homeopaths do. Both are fraudulent.
#Andy L.#Cass Review#Cass Report#Dr. Hilary Cass#Hilary Cass#misinformation#myths#misconceptions#detrans#detransition#gender affirming healthcare#gender affirming care#gender affirmation#affirmation model#medical corruption#medical malpractice#medical scandal#systematic review#religion is a mental illness
354 notes
·
View notes
Text
The Walled World consists of the U.S. and Canada (in North America); Japan and South Korea, plus Australia and New Zealand (in the Asia-Pacific region); plus basically the entire European Union (2); and also Israel. In 2009, that club of nations represented just 14 percent of the world’s population but earned 73 percent of its income. Conversely, the “gray areas” outside the walls were home to 86 percent of humanity, who scraped together just 27 percent of the world’s income.
The average monthly income inside the wall is around €2,500. Outside, it’s just €150. Money may or may not buy happiness, but it does buy quality of life. The yellow dots, which represent the world’s top 50 cities in terms of quality of life, are almost all inside the wall — only Singapore is outside, and that relatively wealthy city-state should arguably be included inside the wall anyway.
In other words: the poor are many, the rich are few. That’s not a new phenomenon of course, nor are the migratory pressures it causes. That’s where those barriers come in. The map lists some examples, the locations and the circumstances of which are all different — but which are all pieces of the same puzzle shown on this map.
560 notes
·
View notes
Text
One of the world’s top arms exporters, Israel exports annually as much as $7 billion worth of military technology, or 2.2 percent of its Gross Domestic Product. An additional 1.35 percent of GDP is dedicated to military research and development, and 6.7 percent is spent on its defense budget— the world’s second largest military budget as a percentage of GDP after Saudi Arabia. All told, 10.25 percent of the Israeli economy is involved directly in arms. Comparatively, for the United States, the world’s top weapons exporter, arms account for around 3.7 percent of its economy. Israel is actually the world’s largest arms supplier per capita, according to data from the Stockholm International Peace Research Institute and the World Bank, at ninety-eight dollars; it is followed by a distant Russia at fifty-eight dollars, and Sweden at fifty-three dollars.
These figures do not include the contribution from natural resources exploited under occupation in the West Bank and Gaza.50 They do not factor in the service sector’s revenue or general industry and construction taking place in the West Bank. Such figures are difficult to quantify, since many companies operate in the West Bank but have offices in Tel Aviv to obscure where operations take place. Nor does this account for Israeli exports into the Occupied Territories, which are 72 percent of Palestinian imports and 0.16 percent of Israeli GDP. All told, the Israeli economy is deeply involved in a web of expenditure and profit around the ongoing occupation and expansion of settlements.
American military aid supplanting open-ended government grants has had the effect of increasing arms production and diminishing the overall economic reach of the state. No longer is foreign aid and imperialist incentive directly invested in the working class. Israeli workers are now rewarded through the arms economy. This is why, despite the lack of social mobility and the economic degradation of neoliberalism, the working class remains committed as ever to Zionism.
The working class has become dependent on the education, housing, and career opportunities that their participation in the IDF affords them. They have found routes for advancement in the military-fueled high-tech industry, with over 9 percent of workers concentrated in high-tech. And as pensions and real wages are eroded, the cheaper cost of settlement living in the Occupied Territories has become essential.
350 notes
·
View notes
Text
CRITICAL WARNING!!!! Radio talk show hostess, Kim Komando, did some digging about TEMU and this is what she found!
Seemingly overnight, everyone’s talking about Temu (pronounced “tee-moo”), an online shopping app that boasts deals that seem too good to be true, like $17 wireless earbuds, $1 “gold” necklaces and $23 wedding dresses.
Over 50 million Americans have downloaded Temu since it launched state-side in September 2022, after it gained traction with expensive Super Bowl ads promising to let you “shop like a billionaire.”
Today, Temu is the most popular shopping app in the U.S. behind Amazon. But most of us don’t know much about the app’s true origins. Reader Daniel Mayer asked an important question, “Is [Temu] something we should be concerned about?”
So, I did some digging. And as it turns out, yes, you absolutely should be. Here’s what I found:
Where did Temu come from?
This isn’t some fly-by-night operation. Temu is based in Boston, Massachusetts, by PDD Holdings Inc. (Nasdaq: PDD). PDD is headquartered in Shanghai, China.
PDD also owns the e-commerce platform Pinduoduo headquartered in — you guessed it — China. So, Temu is a Communist China-based app and site.
What you need to know before using Temu
First, you’re buying goods directly from manufacturers in China and other parts of the world. That’s why shipping times are often 12 days or longer. The prices are low because the goods are cheap. The pictures of what you see advertised may not be what you actually get.
Temu’s BBB rating is 2.21/5. Reviews at TrustPilot are interesting, with 38% 5-star reviews and 41% 1-star reviews.
But that’s not the worst of it.
Temu is downright dangerous.
The app is a clever, pervasive digital stalker. As you shop, Temu monitors your activity on other apps, tracks your notifications and location and changes settings.
🛑 It gets worse. Temu gains full access to all your contacts, calendars and photo albums, plus all your social media accounts, chats and texts. In other words, literally everything on your phone. This is scary
No shopping app needs this much control, especially one tied to Communist China. If you’re using Temu, delete the app from your phone ASAP.
On iPhone, Long-press an app, then tap Remove App > Delete App. Tap Delete to confirm.
On Android, touch and hold an app, then tap Remove App > Delete App > Delete.
Pro tip: If you downloaded Temu, to be safe from Chinese spies, you really need to do a full factory reset.
But wait, there’s more! Temu’s sister app was removed from Google Play because of malware.
Do not buy from this company, or use their app!
COPY AND PASTE PLEASE
703 notes
·
View notes
Text
Han by Theodora Taylor
5 stars
audiobook

After seeing Han in two previous books, I was anxious to get his story, and he did not disappoint in any way, shape, or format! Tough as nails, heart of gold, he meets his match with Jasmine, and they clash magnificently because of it. All that passion completely translates in and out of the bedroom, as they take convoluted path to their HEA <3
#Theodora Taylor#Han#Her Ruthless Mistake#Ruthless Triad#50 Loving States#Owned for a Debt#Forced Proximity#audiobook#Kobo Plus#KP#am reading#read romance#romance reader#romance books#read#romance#books#reader#bibliophile#book love#book blogger#book review#steamy reads
1 note
·
View note
Text

The Tametebako or Colloquially "Fuchi's Last Stand" was a no holds bar, money is no object vanity project by an unsupervised faction of Fuchi Asia. The stated goal was to make a completely unmatched bleeding edge piece of tech that could compete with the best static units while being a portable terminal replacement.
Aimed at the Newly minted UltraLux CEO Segment, The Tametebako was made from rare and hard to get materials to sell it's exclusive nature; bundled with its innovative hardware and extremely powerful Otohime Assistant Software (Which Fuchi spend 10 years developing). Consequently, The Tametebako Commlink retailed at 50 000 nuyen which many consumers balked at for what was essentially an overpowered phone with an extremely intelligent chatbot. Many reviewers sledged the device for it's inability to install new applications if they weren't from approved sources.
These Commlinks are now seeing second life in the collectors and hackers markets with finding the styling and theming of the phone to be charmingly retro and powerful enough to keep up with modern hardware with some QoL mods. Diehard fans report the Otohime software taking on a life of it's own after modding the hardware; her usual calm and dignified demeanor shifts around and changes during the jailbreaking process due to the random voltage pulse needed to defeat the modification lockout chip. This results in a unique iteration of the Soft on each device.
SinkaSwim P2.0Net
#Shadowrun#Otohime#im fuckin free#rendering devices is hell#but im glad i did it#the deep lore on this is shes a normally digified character#but with say some offcolour shit off the cuff before rephrasing to sound more polite#originally envisioned her as a gps navigator but gridguide beat my ass
101 notes
·
View notes
Note
Not that I'm not glad you do the things you do, but do you ever want to write something long form? Because I think it would be worth the while.
if you mean writing fiction, i'm horrible at finishing things so i don't think i'd ultimately be very good for that but i do have some old stuff in various states of non-completion locked away on google docs ranging from "what if i wrote an intricate space opera novel that'd be so vibes" to "culinary review book where i spend each chapter talking mad shit about every food on the planet" and also some really gross over-the-top 50 shades of grey parody i wrote to make an ex-girlfriend laugh (please understand. in 2015 this was still funny and relevant)
235 notes
·
View notes
Text
Breaking Down Cass Review Myths and Misconceptions: What You Need to Know.
An answer when some tranny or handmaiden disputes the review. (long post with lots of facts!)
Via The Quakometer:
It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Many trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics”, including Andrew Wakefield, has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
Myth 1: 98% of all studies in this area were ignored.

Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation.
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
The Review states,
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.

Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,

Myth 2: Cass recommended no Trans Healthcare for Under 25s.

Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”.

Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions

The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1. Explainer on the Newcastle Ottawa Scale
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.

Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:

Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
#Cass report#the cass report#cass review#the cass review#trans lies#gender critical#tras#medical malpractice#the tide is turning
86 notes
·
View notes
Last Seen Blogs

ellaxyx
🌹Noelle🌹
vmiavri-blog
...

thebirdfromthemoon-art
TheBirdFromTheMoon-Art

themuggledancer
theMuggleDancer
georgies-ftts
Georgie