#covid vaccine activist
Text
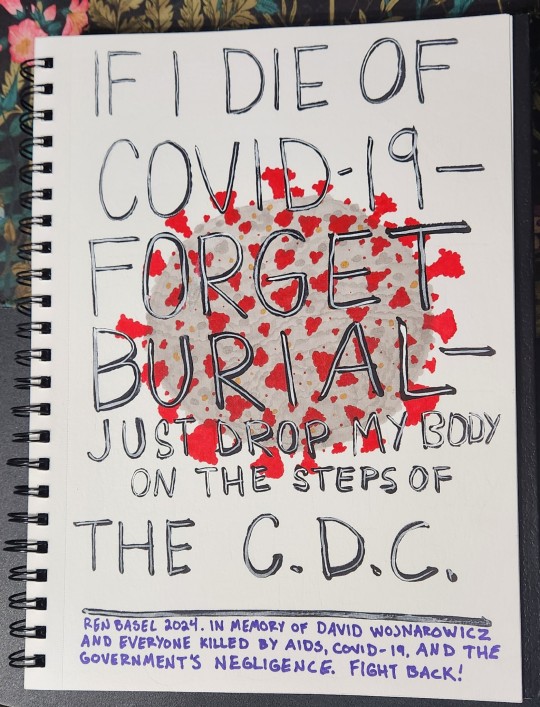
[Image description: A photograph of a page from a spiral-bound sketchbook. The page has an illustration of the covid-19 virus and overlaid text that reads, "If I die of Covid-19 - forget burial - just drop my body on the steps of the C.D.C." A caption on the bottom of the page reads, "Ren Basel 2024. In memory of David Wojnarowicz and everyone killed by AIDS, COVID-19, and the government's negligence. Fight back!" End description.]
In 1988, AIDS activist David Wojnarowicz was photographed in a now-famous image, wearing a jacket that read, "If I die of AIDS - forget burial - just drop my body on the steps of the F.D.A.." I am far from the only person to adapt Wojnarowicz's words to COVID-19, but today I am feeling especially angry at the world. Holding the rage in my chest hurts--it hurts so fucking much--so instead, I've put it on paper.
Living through government negligence and community indifference during COVID-19 in 2024 fills me with rage and grief in equal measure, and as a queer person who studies queer history, I can see the echoes of AIDS in the way marginalized communities are being left to die.
As a disabled person who lives in a household that is very high-risk for COVID-19, the C.D.C.'s recent decision to shorten the COVID-19 isolation period feels like a slap in the face.
COVID-19 is not over, and it is vital to take steps to protect yourself and others. Please, follow the work of the People's CDC, an organization dedicated to COVID-19 safety, activism, and education.
Our government has failed us. Our communities have failed us. For those of us who are immunocompromosed or otherwise high-risk, we only have each other.
Remember us. Fight with us. Mask up, get vaccinated, get boosted.
Please.
#original post#my art#covid-19#covid#coronavirus#disability justice#disability rights#disability awareness
3K notes
·
View notes
Note
You've said before that shame *is* a useful tool to shut up and deplatform genocide deniers. Disability activists have been calling the US response to covid a genocide for nearly 4 years. Can you explain why you think that type of genocide denial shouldn't be shamed? If shame doesn't work for covid safety, what to you are the acceptable, shame-free ways to get events and orgs to include participants who are still at-risk to covid? Or am I just misunderstanding your statements about masking.
I have answered this before, but it's very simple: because the target behavior you are looking for on these two issues are completely different. Shame is good at making people freeze and hide. It is not good at encouraging proactive behavior of the kind needed to prevent COVID spread.
We want pro-Zionist genocide apologists to be terrified to share their views in public. We want genocide apologism to be so completely beyond the pale that it no longer happens on TV, in the newspapers, or in the public square. We do not want to change the hearts and minds of genocide apologists. We want to take away their power and make them shut up.
To address COVID, we want all people to engage in specific proactive behaviors. To get tested. To wear a mask. To be able to openly and comfortably discuss exposure risks. To disclose symptoms. To get vaccinated. All of these behaviors are the exact kinds that public research has revealed repeatedly that shame does not work for.
When you shame people for not taking the "right" actions regarding COVID, they resist, they lie, they hide their actual behaviors, they feel powerless, and they stop caring about COVID spread because they feel hopeless.
When it comes to genocide apologism, we shame because we want people who consider mass murder acceptable cast out of positions of power.
When it comes to COVID we ask questions, offer resources, hand out masks, fight for people to get more days off work, educate, show patience, and never issue judgement, because we need the entire collective to be on the same page taking the same actions every single day.
156 notes
·
View notes
Note
im an undergrad student who was thinking about specializing in studying fascist movements in North America for my masters and ive really enjoyed reading your book commentary - you connect things that I'm not always aware of in ways that are really comprehensive and appreciate
Do you know of any researchers who are moving things on the topic right now (most of the books ive read are around 20+ years old, unfortunately)?
(sorry if any of this is unclear/grammatically incorrect/weirdly worded - I'm super sick rn)
thank you! I'm really glad to hear that :)
For contemporary writing, I'm currently working through some of Alberto Toscano's work - he has a really interesting article from 2021 on fascism from a Black radical/Marxist perspective where he summarizes various historical analyses of fascism from Black (particularly US) thinkers and activists. One thing I especially appreciate is that he complicates Aime Cesaire's formulation of fascism (i.e., "european colonialism come home") as incomplete when applied to settler colonial contexts, especially the United States - one of Cesaire's articulations of fascism is that (to paraphrase) "one fine day, the prisons begin to fill up, the Gestapo gets busy" and so on, and Toscano, working through Angela Davis and George Jackson, responds with (again I'm paraphrasing) "the prisons are already full! The Gestapo is already here!" etc. Toscano also has a new book that just came out in 2023 called Late Fascism, which explicitly addresses the current moment. I only have a physical copy of that so I can't share a pdf unfortunately, and I still need to get around to reading it lol.
These are also a couple random articles I found insightful:
Carnut (2022). Marxist Critical Systematic Review on Neo-Fascism and International Capital: Diffuse Networks, Capitalist Decadence and Culture War - does what it says on the tin
Daggett (2018). Petro-masculinity: Fossil Fuels and Authoritarian Desire - talks about car culture as a site of modern reactionary political movements, links climate denialism with (proto-)fascist movements
Parmigiani (2021). Magic and politics: Conspirituality and COVID-19 - this one does not mention fascism explicitly, but imo the intersection between new age spirituality, anti-vaccine sentiment, and qanon/q-adjacent conspiracies are pretty important to understanding contemporary fascist social movements, so I'd still recommend reading this
Finally, this isn't an article but I found this recorded lecture about the history of Qanon pretty interesting. I don't think the author gives particularly insightful answers on how to solve the problem of far right conspiracies in the Q&A portion but I found it to be a helpful summary
Otherwise I've been focusing a lot on decolonial scholarship more so than fascist scholarship - this is again guided by Cesaire's argument that Europe/The West broadly is inherently fascist. These works aren't contemporary, but you can look at this post for some of the readings I linked on decolonial scholarship if you want to go that route. Those are serving me more for theoretical frameworks to guide contemporary analysis, not analysis of contemporary events directly
also idk if I need to put this disclaimer, but just in case this leaves my blog: this isn't a full throated defense of/apology for everything in these articles, I'm not claiming they're sufficient to understanding the present moment, these are just some of the things I've been reading recently and have found helpful in some way or another. a lot of contemporary work I have read (much of which isn't linked here because I don't think its very good/do not have it on hand) focuses on populism and authoritarianism as central analytical terminology, which i think does a lot of work to exceptionalize and mystify fascism as a historical and political process/project originating from European colonialism & Western imperialism, but these terms are endemic to the field so you have to contend with them no matter what
good luck with your studies!
58 notes
·
View notes
Note
The year is 1985. You're telling Act Up activists that AIDS sucks and all, but that's not gonna prevent you from living your life, and anyone who doesn't go to your weekly bathhouse orgy is just a neurotic homophobe.
Insanely, obscenely, infuriatingly offensive comparison, not least because gay life and love and sex did not stop during AIDS, and part of the point of activism and public health intervention was to allow those things to keep happening as safely as they could be made to happen. They didn’t tell people to wear condoms so that they could not have sex wearing them. The point of masks and vaccinations and air ventilation is to allow us to do the human social things, because there is no waiting out covid, and most people literally cannot stay in quarantine indefinitely and it would be insane to tell them to
354 notes
·
View notes
Photo

At Yale’s Long COVID Clinic, Lisa Sanders Is Trying It All
excerpts:
Since the beginning of the pandemic, she — together with colleagues in the pulmonary and neurology departments — had been seeing long-COVID patients at Yale but often in an ad hoc way. Some of the doctors had become so flooded with people seeking help that they were having difficulty scheduling and treating their regular patients who came to them for everything else ...
Long-COVID patients, generally speaking, have been very miserable for a very long time, and because the illness attacks their brains, their hearts, their lungs, their guts, their joints — sometimes simultaneously, sometimes intermittently, and sometimes in a chain reaction — they bounce from specialist to specialist, none of whom has the bandwidth to hear their whole frustrating ordeal together with the expertise to address all of their complaints: the nonspecific pain, the perpetual exhaustion, the bewildering test results, the one-off treatments. “These are people who have not been able to tell their story to anybody but their spouse and their mom — for years sometimes,” Sanders tells me. “And they are, in some ways, every doctor’s worst nightmare.”
...
Long COVID has been pushing the limits of hospital systems everywhere, not just at Yale. As Americans emerged from the most acute phase of the pandemic, as mask and vaccine mandates lifted and life returned to a semblance of normal for the people who had contracted COVID and recovered, primary-care physicians started to say, “‘I’m not interested in long COVID,’ or ‘I don’t treat long COVID. Let me refer you to a specialist,’” said David Putrino, who runs the new chronic-illness recovery clinic at Mount Sinai. For their part, Putrino added, the specialists were saying, “This is not what my practice is. This is not an emergency anymore.” Patients all over the country reported monthslong waiting times for appointments at long-COVID clinics. All the while, scientists and pundits heaped skepticism on the very notion of long COVID, arguing that infection made people stronger, that new variants posed no threats, that the danger of long COVID was overblown — implying that what patients were suffering from was all in their heads.
Forgotten in this debate are the 65 million people worldwide for whom the pandemic remains a torturous everyday reality.
...
In the late 1990s, patients with a galaxy of unexplained chronic symptoms — including fatigue, sore throat, joint pain, insomnia, dizziness, brain fog, and depression — began to gather into activist and identity groups, calling themselves sufferers of “chronic Lyme.” They had something, they argued, related to a previous infection from the bite of a deer tick, but their doctors were dismissing them as whiners and neurotics. This was in an era when the medical Establishment was rolling its collective eyes at patients who were querying whether diagnoses of “chronic fatigue syndrome” or “fibromyalgia” might fit their symptoms — ones that looked very much like those linked to chronic Lyme.
Sanders joined the chorus of debunkers. These patients had real symptoms and real ailments, she asserted in Every Patient Tells a Story. But the collection of symptoms was “hopelessly broad and overinclusive,” she wrote. “These are some of the most common symptoms of patients presenting to a primary care office.” She concluded that chronic Lyme was a “phantom diagnosis.”
“I completely regret that chapter,” she says now. “I would like to rewrite it.” Sanders explains that she was reacting to the doctors who were preying on suffering people by prescribing interminable courses of antibiotics that were not helping them: “But I completely misunderstood it. The patients were making the connection between their symptoms and Lyme disease.”
...
“We’re not paying enough attention,” she said. “We’re not. Doctors are still dismissing this disease as something that’s in your head. I have seen the exchanges on Twitter: ‘Long COVID is exaggerated, not real.’” Women are diagnosed with long COVID at roughly twice the rate of men, Iwasaki pointed out: “I think if the situation was reversed, we’d pay even more attention to this disease.”
- Akiko Iwasaki, immunologist at Yale [also known for her work nasal vaccine & long covid research]
...
But even Sanders was not prepared for how little doctors and scientists know about long COVID. There is no blood test. Health officials can’t even agree on how to define it. The CDC describes long COVID as “signs, symptoms, and conditions that continue or develop after acute COVID-19 infection” — or, in Sanders’s paraphrase, “You got COVID and then something bad happened.” Under the CDC definition, patients have long COVID if they are symptomatic at least four weeks after initial infection. The WHO defines it similarly but with a different time frame: occurring or lasting at least three months after initial infection. This discrepancy matters to Sanders because, as much as possible, she wants to identify patients who have long COVID and not those who may take a little longer to recover from their original illness. In her clinic, she uses the WHO definition.
...
Sanders, more than ever before, is dependent on the patient’s account — on detailed specifics — to establish her diagnosis. It’s a process of elimination and deduction. So she has “learned just to shut the fuck up and listen.”
#covid#long covid#article#medicine#ny mag#yale#re: 'I don't know anyone with long covid'#re: 'JUST get treatment'#lyme#me/cfs#mecfs#fibromyalgia#akiko iwasaki#womens health
88 notes
·
View notes
Text
My PR day of yes
Slate journalist Dan Kois said yes to every PR pitch he got for a day. The result is brilliant.
I declared Oct. 26 my Publicist Pitch Day of Yes. I would respond to every single pitch email that asked me to talk to a client, replying, Yes! Yes, I would like to talk to this handbag entrepreneur, this life coach, this writer and social activist on a mission to empower women of color. Yes, I am available on the phone, or over Zoom, at their convenience. Yes, I will ask them about their revolutionary clitoral sonogram, their terrible opinions about cops and COVID vaccines, their advice for how to cope during the holiday season—a challenging time, as you know, for those who struggle with body image.
During my years as a journalist, I got my share of inappropriate PR pitches. Literally dozens every day. Every journalist does. I wish I had thought to turn that energy to a great article like this one.
284 notes
·
View notes
Text
By Rupen Savoulian
Numerous left wing writers and activists – the term left wing being a broad brushstroke – have moved into the rabbit hole of COVID denial MAGA ultrarightism. Glenn Greenwald, Matt Taibbi, among many others, have descended into a contrarian position from the libertarian ultraright. It is no exaggeration to call it a fascist contrarianism.
Robert F Kennedy Jr. a long term environmental lawyer and activist, has metamorphosed into a MAGA supporting far right political figure. Starting with the respectable-sounding position of vaccine hesitancy, RFK has moved decisively to the far right.
His journey is indicative of a widespread phenomenon – leftists who move right wards on an anti scientific trajectory. They remain contrarians – fascist contrarians, ultra libertarian opponents of publicly funded services, such as health care and education.
16 notes
·
View notes
Note
hey i'd really love it if you could say more about biopolitics? i hadn't heard that before and it seems fantastic.
😅 u guys humor me too much- these type of asks are like catnip for me i am rolling around on the floor
biopolitics was originally conceptualized by foucault in a series of lectures- the very simple explanation of it (which foucault scholars probably would feel doesn't do it justice) is that the state has a vested interest in creating citizens who are "healthy" (as defined by the state usually by military/work readiness) + reproducing more "healthy" citizens (in this way it often intersects with outright eugenics). people often refer to it as the politics of "making live + letting die" (necropolitics by achille mbembé is an incredible analysis of this second part, focused on colonial power's interest in determining who dies)
what this means is that, at its core, the state engages in programs to improve the "health" of the population not out of altruism but because it needs a supply of work-ready, combat-ready, reproduction-ready individuals. the concept of "health" is tied up in one's ability to perform labor in service of the state, so much so that disorder or the severity of disorder becomes defined by this ability. public health efforts center not on decreasing suffering but on restoring the population to a condition in which they can once again perform labor (including reproductive labor) + serve the greater needs of the state.
my friend cora at umadison did an excellent presentation on how the u.s evokes within "anti-obesity" campaigns a concern that "obesity" is a threat to military readiness. messaging concerning family planning/abortion are often engaged by the state to coerce certain ppl into having children + others NOT to, based on the idea of the Type of Citizen they want. on a deeper level, this haunts us from birth- were there programs to try to improve your mother's pregnancy? public school health surveys? scoliosis tests? presidential fitness tests? irt COVID-19, whose death was seen as acceptable + whose death was seen as worth preventing? was prioritizing a 'return to work ' an out-of-the-blue approach or a natural conclusion of a public health system structured around producing + maintaining a steady supply of labor? none of this is asserting that state public health intervention is inherently BAD, just that its core motivations are not altruistic but rather political (so it has no interest in expanding into a public health model where fitness to work/serve/birth is NOT seen as the marker of health).
a very cynical read of the opioid epidemic would be that the state is so heavily involved now because it is finally impacting individuals that they want to Make Live. harm reduction is reluctantly being adopted (thanks to the tireless work of incredible activists!) but only if it can fit into the framework of Making Them Live Until They Can Become Sober. sobriety is the unspoken end goal not because it reduces suffering but because it allows for workers. the truly liberatory logic of harm reduction, which focuses on autonomy + safety + reducing suffering, is antithetical to the motivations of a state which openly despises those who don't 'produce' proportionately to what they receive.
my interest is in reimagining medicine + the body + disability + suffering outside of this biopolitical framework by acknowledging that our very definitions of all of these things have been engraved in the public imagination with labor production in mind. i'm not interested in trying to create new state programs that are 'untouched' by biopolitics because that's impossible + i can still extract tangible benefits from it (for example, i got all my covid vaccines early + for free bcuz my labor was important enough for the state to invest in my life). the idea is to engage with these programs clear-eyed + willing to look at who we Make Live + who we Let Die. most importantly, we can find what lies outside it all + envision new ways of living
130 notes
·
View notes
Note
Just curious. How bad has Biden been at controlling COVID-19 in your view?
First: I already responded to a similar question you left on this post.
Second: Biden has been atrocious for COVID-19 safety and management. COVID-19 is still killing people, and our president has done a horribly insufficient job in mitigating that. "Better than the Republicans" is not the same thing as "good" or "effective." Biden's abysmal reaction to COVID-19 is part of why I'm so thrilled that the Uncommitted campaign for the Democratic primary has achieved some success. That particular campaign is focused on ceasefire in Palestine, but the People's CDC explained in a statement how Palestine is also very much a public health issue. We need to scare the bastard and actually do some of that "pushing him left" that people claimed they'd do after getting him elected. Though it seems to me like a lot of people just settled for, "okay, we got rid of Trump, we don't have to worry anymore."
Third: While I'm at it, people have to do more than vote. You have got to get involved. You have got to do more than participate in the presidential election once every four years. Join a union (may I recommend the IWW?), follow the guidance of The People's CDC, volunteer for your local Food Not Bombs, get involved in a tenants union like the Autonomous Tenants Union Network, read Riot Medicine, get trained in first aid and get involved in a street medic group, read up on your local politics and get involved on the small-scale, do something in addition to voting in the presidential election. Even if you're limited in how much you can personally participate, find the people who are talking about these issues and signal boost them, and share the information with others who may be more able to participate more. If you can tell people to go vote in the presidential election, you can also tell them to go do other things, too.
Now, with all of that out of the way, here are some links related to Biden's abysmal COVID-19 response:
During his 2020 campaign, Biden promised immediate $2K stimulus checks. Instead, he delivered $1,400. Sources: [x] [x] [x] [x] [x]
Velena Jones for NBC Bay Area: "‘Too expensive': Bay Area residents shocked over new COVID vaccine prices"
Reuters: "COVID vaccine manufacturers set list price between $120-$130 per dose"
Joseph Choi for The Hill: "Free COVID-19 test program to be suspended for now"
Disability activist Alice Wong writing for TeenVogue: "Covid Isn't Going Anywhere. Masking Up Could Save My Life," and the follow-up article, "COVID and the 2024 Election: What Biden and Democrats Owe High-Risk People."
Laura Weiss writing for The New Republic: "Democrats Can't Keep Ignoring Covid in 2024."
David Cohen and Adam Cancryn for Politico: "Biden on '60 Minutes': 'The Pandemic is Over.'"
Alex Skopic for Current Affairs: "COVID-19 is Still a Threat. So is Biden’s CDC."
Adam Cancryn for Politico: "Biden Appears to be Over Covid Protocols."
Paul Thornton for the Los Angeles Times: "Covid Still Rages, and the Biden Administration Isn't Helping."
Eric J. Topol for the Los Angeles Times: "The U.S. is facing the biggest COVID wave since Omicron. Why are we still playing make-believe?"
We should have free, universal testing. We should have free, universal vaccination. We should have free, universal treatment. We should have financial assistance for those of us who can't work outside the home. We should have mandated work-from-home for any job that can be done remotely. We should be emptying prisons and paying attention to the way disease and abuse proliferate inside their walls. We should have COVID-19 safety PSAs and government support for universal masking. We should have free distribution of N95s. We should have mandated masking in medical settings and public spaces. We should have a higher minimum wage. We should have healthcare reforms. We should have strong worker protections. We should have improved infrastructure. We should have a president who gives a single flying fuck about how many of us are dying.
And we have none of it.
But we sure seem to have money to keep dropping bombs, arming cops, terrorizing the vulnerable, and imprisoning innocent people to use for slave labor.
145 notes
·
View notes
Note
If I see one more person comparing Travis kneeling for the National Anthem in 2020 to Joe being a part of Artists4Ceasefire, I will explode. First off, no athletes were not losing their jobs for kneeling in 2020. Quite the opposite, those were the ones that were getting respect from people who didn't even follow them. White athletes were certainly not risking anything. Colin Kaepernick was fired and blacklisted but that was before 2020. At that point, it was a risk sure but the only people that would have actually stopped supporting the NFL would have been the people that were already aggressively racist to begin with. Also, what has Travis actually done beyond kneeling alongside many other athletes? Meanwhile, actors are literally losing jobs and being blacklisted for showing any kind of support for Palestine. I'm so sick of people insisting that Travis has done more activism than both Taylor and Joe combined. Aside from the fact that Joe never claimed to be an activist, Travis has done nothing that didn't pose much of a risk to his career. No, promoting covid vaccines did not pose a risk. Neither did doing a commercial with Bud Light. At worst, these things would have gotten some criticism online and maybe some fans to stop supporting him as an individual but clearly that hasn't been a problem for him. The fact of the matter is Travis has given us every reason to say that he looks like a hillbilly with anger issues because that is what he shows us. And I'm sick of people saying that people who hype Joe up do so because they hate Taylor and that they hated Joe when they were together. I would rather these people admit to being stans rather than pretend to be neutrals who are the ones that are actually being objective and reasonable
He is not an A list actor in Hollywood, to not have anything to lose.
If anything this should make all of us realize and acknowledge the immense professional risk he takes every time he wears that pin.

#free joe alwyn#joe alwyn#joealwyn#jalwyn#nonnie#q&a#anti taylor swift#shit swifties say#toxic swifties#toxic taylor swift
9 notes
·
View notes
Text
Centuries of Evidence Make Damning Case That Vaccines DO Cause Sudden Infant Deaths
"The Sudden Adult Death Syndrome (SADS) that was seen worldwide after the COVID-19 vaccines rolled out was so unmistakable that it made the general public see how much their governments had lied to them. What is less known, however, is the link between vaccines and the sudden death of children (euphemistically called Sudden Infant Death Syndrome or SIDS)," wrote Midwestern Doctor.
The physician highlighted these main points:
• In order to maximize profits, the pharmaceutical industry will often identify vulnerable groups who lack the ability to advocate for themselves and refuse pharmaceutical products.
• When the DPT vaccine was first developed over a century ago, it was tested at Irish orphanages. Recently mass graves of those early test subjects were discovered.
• Since the DPT vaccine hit the market, physicians around the world have observed waves of infant deaths followed its use which were often sudden and inexplicable (along with many other severe side effects).
• Numerous data sources correlate increasing childhood vaccination rates with increasing infant deaths. Those deaths played a key role in creating the 1986 National Childhood Vaccine Injury Act and that forgotten data compromises the majority of this article.
• When the COVID lockdowns happened, vaccine safety activists predicted the lockdowns would lead to an unprecedented drop in infant deaths since children were skipping their vaccines. This ended up being exactly what happened and it was reconfirmed by infant deaths dropping in Florida after the pandemic prompted many parents to begin not vaccinating their children.
More Stories:
Elon Musk issues warning for America: “Groundwork is being laid for something far worse than 9/11.”
7 Signs You’re Missing Key Nutrients — And How to Fix It
Bad News for COVID Vaccine Manufacturers
Follow @ZeeeMedia and @VigilantFox
11 notes
·
View notes
Text
This month the World Trade Organization threw in the towel on COVID-19. Medicines like Paxlovid have been plentiful in the U.S. and Europe, but because of insufficient supplies and high prices, hardly anyone in Africa, Asia, and Latin America has had access. After more than three years of debate, the WTO declared on Feb. 13 that it was unable to reach agreement on waiving global patent rules for COVID-19 treatment to ease the way for expanded production.
Those confused about why the WTO is even still debating COVID-19 nearly a year after the public health emergency was declared over by the World Health Organization can be forgiven. Not only is this slow speed not what the world needs in a pandemic, it is also not how the World Trade Organization is supposed to work, and begs questions on WTO’s relevance in a multi-crisis world. It also makes clear that responsibility for the global governance of pandemic-related technology and intellectual property cannot remain with the WTO.
As negotiations have reconvened this week in Geneva over a new Pandemic Treaty, the question of which organizations should manage the response is a live question. Some negotiators are pushing for a role for the world’s health ministers and the World Health Organization on intellectual property, but the U.S. negotiator and others say these questions should stay with the WTO. The WTO’s failure, though, make this an increasingly untenable position: If the WTO cannot act in a pandemic to remove patents barriers and promote sharing of technology so the world can produce enough medicines and vaccines, then the WHO must be empowered to do so.
When the World Trade Organization was created in 1995, it marked a fundamental change to international trade law. Where the international system it replaced had primarily dealt with flow of goods across borders, WTO rules expanded the definition of “trade” to include the intangible—including patents on pharmaceuticals. All members were required to enforce 20-year monopolies over making new medicines. As the late scholar Susan Sell described it, this was a remarkable act of “forum shifting.” Before that, patents (effectively government-granted monopolies) were not part of “free” trade. Into the 1970s, many rich countries such as Italy and Japan did not allow patents on medicines, and many developing countries like India, Brazil, and Mexico had continued to exclude medicines from patent monopolies into the 1990s. But they were convinced to expand intellectual property in the new WTO agreement with a promise of “technology transfer” and a requirement that wealthy countries incentivize their companies to share with least-developed countries. This has not gone as promised.
The first effective medicines in the AIDS pandemic arrived just as the WTO came into being. It quickly became clear this debate about globally enforceable intellectual property was life-or-death as patents proved a major barrier to access. Twelve million Africans died between 1997 and 2007 with AIDS medicines too expensive and pharmaceutical companies blocking affordable generic versions. Eventually manufacturers in India, Brazil, South Africa, and elsewhere overcame barriers and made the drugs at a 99 percent lower cost. Today 30 million people are on treatment and cutting-edge medicines costs less than $50 per year.
Did drug companies voluntarily relent? Unfortunately, no. Dozens of low- and middle-income country governments issued “compulsory licenses” forcing drug companies to allow local producers to make HIV medicines. Activists pressured companies to drop their price and share their technology. The WTO eventually agreed on the “Doha Declaration” clarifying WTO rules allowing countries “flexibilities” to make affordable medicines and special consideration during emergencies. It took over a decade, but eventually the Medicines Patent Pool was created to facilitate voluntary sharing of technology—though companies only joined because compulsory alternatives left them little choice.
When the pandemic hit, these structures to transfer technology were all available, but world leaders decided to only use the voluntary elements—an approach that failed spectacularly. Scientists delivered vaccines in record time. Highly effective mRNA vaccines were developed in under a year and treatments followed. Paxlovid proved among the most effective—a long-standing HIV drug combined with a new drug similar to HIV antiretrovirals. Costa Rica and the WHO proposed a mechanism to pool technology and patents even before medicines were developed and approved. Over 100 different drug and vaccine manufacturers around the world were prepared to make them, several even showing they could reverse engineer mRNA vaccines. But no drug company agreed to share its technology, and none of the governments where companies were based compelled them to.
With neither a relaxation of WTO rules nor enough voluntary sharing to enable factories in Africa, Asia, and Latin America to expand supply, global leaders backed a set of voluntary efforts for low- and middle-income countries (LMICs). COVAX, the international effort to procure and equitably distribute vaccines, tried to secure vaccines from companies like Pfizer and Moderna. Predictably, however, COVAX quickly discovered high-income countries were locking up global supplies by using economic and political power to secure preferential access from companies. By the end of the first year, less than 1 percent of all vaccines had gone to low-income countries. Medicines fared no better. One analysis showed need for Paxlovid exceeded supply in LMICs by 8 million doses—leaving 90 percent without access. The lowest reported price was $250—200 percent of the average per capita spending on all health in lower middle-income countries.
These shortages had consequences. Analyses show as many as 27 million lives lost to the pandemic, many of which were preventable. Beyond the direct effect, dangerous coronavirus variants swept the world from contexts of high transmission and low vaccinated immunity. The pandemic has been longer and more damaging because of an artificially limited global supply of countermeasures.
Throughout this time the WTO was locked in debate. South Africa and India proposed a temporary waiver of WTO rules on all COVID-19 products during the pandemic. Pharmaceutical industry lobbyists cast this as a dangerous idea, launching a campaign against it claiming “voiding patents” would undermine innovation for pandemic products. In reality, a waiver does not take away IP rights. It simply suspends global rules temporarily, giving policymaking authority back to national governments to decide whether to enforce patents on pandemic-products during the pandemic without threat of WTO-linked sanctions. A waiver alone would not have solved the pandemic supply problem, which also required shared know-how and expanded manufacturing. But it would have removed threats of lawsuits for companies making financial and infrastructure investments in production lines and threat of sanctions from powerful states for governments allowing local production.
The WTO is supposed to be able to use mechanisms like waivers to respond to crises in a matter of weeks, not years. The Marrakesh Agreement explicitly includes a provision on waivers, stating the General Council must act within 90 days on a waiver request, assuming consensus, but falling back to a vote of three-fourths of members. Every year multiple WTO waivers are granted on issues from pharmaceuticals to diamonds to preferential trade for neighbors. But since 2020, the WTO’s efforts to pass a waiver in the middle of a world-changing event hit institutional and ideological roadblocks. Even as heads of state weighed in and wide swaths of the global economy depended on stopping the coronavirus, the institutional structure encouraged gridlock. Despite seemingly supportive law, the WTO’s structures encourage narrow interest-group politics, excluding actors with a broader public interest and economic agenda.
Narrowly-focused intellectual property negotiators framed the COVID-19 issue in ways that insulated negotiators, focused on footnotes and eligibility instead of stopping the pandemic, and gave an effective veto to trade negotiators from a few states with strong pharmaceutical lobbies. By the time the 12th WTO Ministerial Conference rolled around in June 2022, a simple pandemic-long waiver proposed two years earlier had morphed into a complicated mechanism that several developing countries declared unworkable. It only covered vaccines, pushing treatments to further negotiations. Eight months of more negotiations yielded no further progress, leading to the WTO’s declaration of no agreement last week.
It is time for a new forum shift. Negotiations over a new Pandemic Treaty are intensifying as negotiators hope for a May conclusion. The draft agreement includes a commitment to waive intellectual property during a pandemic and to use WTO flexibilities to produce pandemic-fighting products. These are the minimum steps to make the whole world safer. President Joe Biden already supported a patent waiver during the pandemic and is using these flexibilities at home, including “march-in” rights to limit patent monopolies on high-priced drugs in the U.S. The U.S. negotiator’s opposition suggests misaligned foreign policy.
But the agreement should go further. Given the WTO’s repeated failure, the new agreement should shift authority to waive patent rules to the World Health Assembly. And it should include a binding agreement to share publicly funded technologies for global production. States delegated authority to the WTO, which has proved a barrier rather than an asset in pandemics. Taking it back is just good governance.
8 notes
·
View notes
Text
@TaraBull808
Subscribe
Top 10 headlines the media didn't tell you this week, Retweet & Follow for more. 10. Oliver Anthony's Rich Men North of Richmond surges to GLOBAL #1 on music charts. 9. Hawaii Democrat Governor says State plans to acquire land ravaged by wildfires. 8. Russia claims the U.S. is working to manufacture another, more deadly virus. 7. Joe Biden used secret pseudonym Robert L. Peters, when making 'business deals' with Ukraine. 6. Activist account LibsofTikTok continues to expose unstable individuals being hired by schools, leading to their removal. 5. Former VP of Pfizer says COVID is just the beginning of a 10-year plan by Bill Gates and Klaus Schwab. 4. Georgia state Senator moves to impeach District Attorney, Fani Willis, for her actions against Trump. 3. Documents reveal Jeffrey Epstein was a “middle man” between Obama and JPMorgan. 2. Fox News faces public backlash after promoting Covid Vaccines to pregnant women and newborns. 1. Biden sends an embarassing $700 to Maui fire victims while requesting an additional $40 billion emergency funding to Ukraine. BONUS: Covid vaccines are being updated for 'New Variants' expected by fall. What do they know? What story am I missing?
21 notes
·
View notes
Text
Thoughts while watching actors pass around my "I voted" pens in rehearsal today.
I think there may be a really similar dynamic at play between devaluation of vaccination in Covid safety circles, and devaluation of voting in leftist/activist circles, where there's this perceived obligation to go around shouting about how vaccination doesn't work well enough, or voting doesn't actually matter that much. And I've ranted a little bit before about some of the eerily-similar-to-evangelical-thinking I think this kind of rhetoric serves.
But I also think there's an assumption involved that everyone they know does vote, or is vaccinated.
And statistically speaking, it's just not true. (About 66% of eligible voters voted in the 2020 presidential election, but far, far fewer do so in midterm and local elections. Only about 21% of eligible Americans have gotten the newest updated Covid vaccine.)
People think that most people have done the bare minimum and decided that's enough. But in fact most people have not even done the bare minimum.
So when people feel compelled to go around yelling about how voting's not good enough, vaccination isn't good enough--they hope they're encouraging people who obviously already do those things to do more (call senators, participate in boycotts, demonstrations, direct actions; wear masks and test regularly). But I'm afraid what they're actually accomplishing is convincing people who do not in fact do them, to continue not to bother.
Because what's the point, if they don't work that well, anyway?
9 notes
·
View notes
Last Seen Blogs

reiseblog-lunz-am-see
Lunz am See

gangqin17
just another art blog


romantik-adam-20-blog
Romantik-Yalnız

dismantlerepair89
So, I had this idea...