#jamie reed
Text
By: Tamara Pietzke
Published: Feb 5, 2024
For six years I worked at a hospital that said all teenagers with gender dysphoria must be affirmed. I quit my job to blow the whistle.
I know from firsthand experience what hard times are. Though I had a happy childhood, raised as the middle child by working-class parents in Washington State, my mom died of ovarian cancer when I was 22.
After that, my family fell apart. I felt lost and alone.
I decided to become a therapist because I didn’t want anyone to go through what I had, feeling like no one on this planet cares about them. At least they can say their therapist does.
I earned my master’s in social work from the University of Washington in 2012, and I have worked as a therapist for over a decade in the Puget Sound area. Most recently, I was employed by MultiCare, one of the largest hospital systems in the state.
For the six years I was there, I worked with hundreds of clients. But in mid-January, I left my job because of what I will go on to describe.
The therapeutic relationship is a special one. We are the original “safe space,” where people are able to explore their darker feelings and painful experiences. The job of the therapist is to guide a patient to self-understanding and sound mental health. This is a process that requires careful assessment and time, not snap judgments and confirmation of a patient’s worldview.
But in the past year I noticed a concerning new trend in my field. I was getting the message from my supervisors that when a young person I was seeing expressed discomfort with their gender—the diagnostic term is gender dysphoria—I should throw out all my training. No matter the patient’s history or other mental health conditions that could be complicating the situation, I was simply to affirm that the patient was transgender, and even approve the start of a medical transition.
I believe this rise of “affirmative care” for young people with gender dysphoria challenges the very fundamentals of what therapy is supposed to provide.
I am a 36-year-old single mother of three young kids all under the age of six. I am terrified of speaking out, but that fear pales in comparison to my strong belief that we can no longer medicalize youth and cause them potentially irreversible harm. The three patients I describe below explain why I am taking the risk of coming forward.
* * *
Last spring, I started seeing a new client, who at 13 years old had one of the most extreme and heartbreaking life stories I’ve ever heard. (For the sake of clarity, I am referring to all patients by their biological sex.)
My patient’s mother has bipolar disorder and was so abusive to my patient that the mother was given a restraining order. My patient was sexually assaulted by an older cousin, by one of her mother’s boyfriends, and also once at school by a classmate. Her diagnoses include depression, PTSD, anxiety, intermittent explosive disorder, and autism. She is being raised by her mother’s ex-boyfriend (not the one who assaulted her).
The year before I started seeing her, when she was 11, she was hospitalized for talking about committing suicide. Later that year, a pediatrician diagnosed her with gender dysphoria after she started to question her gender. The pediatrician referred her to Mary Bridge Children’s Gender Health Clinic, whose clinicians recommended she take medicine to suppress her periods and that she think about starting testosterone.
Mary Bridge, MultiCare’s pediatric hospital, runs the gender clinic for minors and employs nurses, social workers, dietitians, and endocrinologists, who provide gender-affirming care, which includes prescribing hormones to young patients who question their gender. In order to get that prescription, patients first need a recommendation letter from a therapist. Because Mary Bridge is a part of MultiCare, their patients were often referred to therapists like me who were in their system.
In an April 2022 blog post, a Mary Bridge social worker wrote that the gender clinic’s referrals increased from less than five a month in 2019 to more than 35 a month in 2022. In May 2022, the clinic received a $100,000 donation from Patient-Centered Outcomes Research Institute “to study health care disparities” in transgender youth.
The clinic operates in Washington, one of the states with some of the most lenient legislation on gender transition for youth. In May 2023, the state legislature passed a law guaranteeing that youth seeking a medical gender transition can stay at Washington shelters—and the shelters are not required to notify their parents.
Because of my patient’s autism, it was difficult for us to engage in introspective conversations. During our first visit, she came over to my desk to show me extremely sadistic and graphic pornographic videos on her phone. She stood next to me, hunched over, hyper-fixated on the videos as she rocked back and forth. She told me during one session that she watched horror and porn movies growing up because they were the only ones available in her house.
She showed up to our therapy sessions in disheveled, loose-fitting clothes, her hair greasy, her eyes staring down at the ground, her face covered by a Covid mask almost like a protective layer. She went by a boy’s name, but she never raised gender dysphoria with me directly—though one time she told me she would get mad at the sound of her own voice because “it sounds too girly.” When I asked her how she felt about an upcoming appointment at the gender clinic, she told me she didn’t know she had one.
In between scrolling through videos on her phone, she told me how she cried every night in bed and felt “insane.” She described a time when she was eight years old and her mother nearly killed her sister. She remembered her mother being taken away. At times, she would “age-regress,” she told me, by watching Teletubbies and sucking on pacifiers.
When she started seeing me, she had recently threatened to “blow up the school,” which resulted in her expulsion.
I knew I couldn’t solve all of her problems, or make her feel better in just a few therapy sessions. My initial goal was to make her feel comfortable opening up to me, to make the therapy room a place where she was heard and felt safe. I also wanted to try to protect her from falling prey to outside influences from social media, her peers, or even the adults in her life.
With a patient like this, with so many intersecting and overwhelming problems, and with such a tragic history of abuse, it took our first three sessions to get her feeling more comfortable to even talk to me, and to understand the dimensions of her problems. But when I called her guardian last fall to schedule a fourth appointment, he asked me to write her a letter of recommendation for cross-sex hormone treatment. That is, at age 13, she was to start taking testosterone. Such a letter from me begins the process of medical transition for a patient.
In Washington State, that’s all it takes—a few visits with a therapist and a letter, often written using a template provided by one’s superiors—for minors to undergo the irreversible treatments that patients must take for a lifetime.
I was scared for this patient. She had so many overlapping problems that needed addressing it seemed like malpractice to abruptly begin her on a medical gender transition that could quickly produce permanent changes.
The MultiCare recommendation letter Tamara was given for approving the medical treatment of minors with gender dysphoria. I emailed a program manager in my department at MultiCare and outlined my concerns. She wrote back that my client’s trauma history has no bearing on whether or not she should receive hormone treatment.
“There is not valid, evidenced-based, peer-reviewed research that would indicate that gender dysphoria arises from anything other than gender (including trauma, autism, other mental health conditions, etc.),” she wrote.
She also warned that “there is the potential in causing harm to a client’s mental health when restricting access to gender-affirming care” and suggested I “examine [my] personal beliefs and biases about trans kids.”
When Tamara outlined her concerns about giving a patient testosterone to her manager at MultiCare, she was told to “examine your personal beliefs and biases about trans kids.” She then reported me to MultiCare’s risk management team, who removed my client from my care and placed her with a new therapist.
A risk manager’s job is to minimize the hospital’s liability, but in my case, they deemed that my concerns posed a greater risk to my client than giving her a life-altering procedure with no proven long-term benefit.
I shouldn’t have been surprised by this. Just a few months earlier, in September of last year, I was one of over 100 therapists and behavioral specialists at the MultiCare hospital system required to attend mandatory training on “gender-affirming care.”
As hard as it is to believe given my work, I hadn’t heard about gender-affirming care before that moment. I needed to know more. So each night in the week leading up to the training, I searched online for information about gender-affirming care. After putting my kids to bed, I sat glued to my computer screen, losing sleep, horrified at what I found.
I discovered that neither puberty blockers nor cross-sex hormones (testosterone or estrogen) were approved by the Food and Drug Administration as a treatment for gender dysphoria. In fact, prescribing these treatments to kids can have drastic side effects, including infertility, loss of sexual function, increased risk of heart attack, stroke, cardiovascular disease, cancer, bone density problems, blood clots, liver toxicity, cataracts, brain swelling, and even death.
While gender clinicians claim hormonal treatment improved their patients’ psychological health, the studies on this are few and highly disputed.
I found that those experiencing gender dysphoria are up to six times more likely to also be autistic, and they are also more likely to suffer from schizophrenia, trauma, and abuse.
The research also implies that the dramatic rise in these diagnoses across the West likely have a strong element of social contagion. In children ages 6 to 17, there was a 70 percent increase in diagnoses of gender dysphoria in the U.S. from 2020 to 2021. In Sweden there was a 1,500 percent increase in these diagnoses among girls 13–17 from 2008 to 2018.
Yet, countries that were once the pioneers of gender transition medicine are now starting to backtrack. In 2022, England announced it will close its only gender clinic after an investigation uncovered subpar medical care, including findings that some patients were rushed toward gender transitions. Sweden and Finland undertook comprehensive analyses of the state of gender medicine and recommended restrictions on transition of minors.
I decided—though it was potentially dangerous to my career and to me—to ask questions about the findings I discovered.
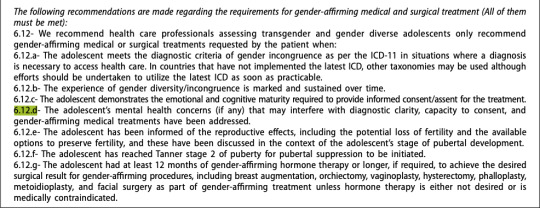
The training I attended laid out an affirming model of gender care—from pronouns and “social transition” to hormone treatments and surgical intervention. In order for children to be diagnosed with gender dysphoria, the training stated, patients must meet six of eight characteristics, ranging from “a strong desire/insistence of being another gender” to “strong preference for cross-gender toys and games.”
Tamara and her MultiCare colleagues were trained to diagnose gender dysphoria among their young patients when they met six of the eight above characteristics. It was made abundantly clear to all in attendance that these recommendations were “best practice” at MultiCare, and that the hospital would not tolerate anything less.
When the leader of the training brought up hormone treatments, I shakily tapped the unmute button on Zoom and asked why 70 to 80 percent of female adolescents diagnosed with gender dysphoria have prior mental health diagnoses.
She flashed a look of disgust as she warned me against spreading “misinformation on trans kids.” Soon the chat box started blowing up with comments directed at me. One colleague stated it was not “appropriate to bring politics into this” and another wrote that I was “demonstrating a hostility toward trans folks which is [a] direct violation of the Hippocratic Oath,” and recommended I “seek additional support and information so as not to harm trans clients.”
In the training, gender-affirming treatment is presented as “suicide prevention.” As soon as I closed my laptop, I burst into tears. I care so deeply about my clients that even thinking about this now makes me cry. I couldn’t understand how my colleagues, who are supposed to be my teammates, could be so quick to villainize me. I also wondered if maybe my colleagues were right, and if I had gone insane.
Later, my boss reached out to me and told me it was “inappropriate” of me to raise these questions, telling me that a training session was not the proper forum. When I tried to present the evidence that caused me concern—the lack of long-term studies, the devastating side effects—she told me she didn’t have time to read it.
“I am speaking out because nothing will change unless people like me blow the whistle,” Tamara writes. “I am desperate to help my patients.” In retrospect, this ideology had been growing in power for a long time.
I remember in 2019 seeing signs of how gender dysphoria arose among many of my most vulnerable female clients, all of whom struggled with previous psychological problems.
In 2019, I started seeing a 16-year-old client after her pediatrician referred her to me for anxiety, depression, and ADHD. When I first met her, she had long blonde hair covering her eyes, to the point you could barely see her face. It was like she was going through the world trying to be invisible.
In 2020, during the pandemic, she told me she had started reading online a lot about gender, and said she started feeling like she wasn’t a girl anymore.
Around this time, her anxiety became so debilitating she couldn’t leave her house—not even to go to school. After taking a year off school during the pandemic, she enrolled in an alternative school for kids struggling with mental health. I was relieved that she was making friends for the first time, and seemed to be feeling a lot better.
Then she started using they/he pronouns, identified as pansexual, and replaced the skirts and fishnet stockings she often wore with disheveled and baggy clothes. Her long hair became shorter and shorter. She started wearing a binder to flatten her breasts. She tried out a few different names before settling on one that’s gender neutral.
The official diagnosis I gave her was “adjustment disorder”—an umbrella term often applied to young people who are having a hard time coping with difficult and stressful circumstances. It’s the type of diagnosis that doesn’t follow a child forever—it implies that mental distress among kids is often transient.
She came out as transgender to her family in 2021. Her mother was supportive, but her dad wasn’t. Regardless, she went to her pediatrician seeking a referral to a gender clinic.
In 2022, she went to Mary Bridge Children’s Gender Health Clinic for the first time, where the clinicians informed her and her parents that if she didn’t receive hormone replacement therapy, she could be “at increased risk for anxiety, depression, and worsening of mental health/psychological trauma,” according to her patient records. Her dad refused to start his daughter on testosterone, and so all the clinic could do was prescribe birth control to stop her period due to her “menstrual dysphoria,” or distress over getting her period. Which is something I thought all teenage girls experienced.
Five months later, she swallowed a bottle of pills and her mother had to rush her to the emergency room.
By early 2023, my client logged on to our weekly session, which we started doing by Zoom, and she told me she identified as a “wounded male dog.” She explained to me that this was her “xenogender,” a concept she had discovered online, which references gender identities that go “beyond the human understanding of gender.” She said she felt she didn’t have all of the right appendages, and that she wanted to start wearing ears and a tail to truly feel like herself.
I was stunned. All I could do was silently nod along.
After the session, I emailed my colleagues looking for advice. “I want to be accepting and inclusive and all of that,” I wrote, but “I guess I just don’t understand at what point, if ever, a person’s gender identity is indicative of a bigger issue.”
I asked them: “Is there ever a time where acceptance of a person’s identity isn’t freely given?”
The consensus from my colleagues was that it wasn’t a big deal.
“It sounds like this isn’t something that’s ‘broken,’ ” one colleague wrote me back, “so let’s not try to ‘fix’ it.”
“If someone told me they use a litterbox instead of a toilet and they were happy with it and it’s part of their life that brings them fulfillment, then great!” she continued. “I might think it’s weird, but then again, not my life.”
After learning that one of Tamara’s patients identified as “a wounded male dog,” a colleague replied: “If someone told me they use a litterbox instead of a toilet and they were happy with it and it’s part of their life that brings them fulfillment, then great!” I was baffled and alarmed by her unquestioning affirmation. At what point does a change in identity represent a mental health concern, and not something to be celebrated and affirmed? Fortunately, my client never brought up her “xenogender” again. She also isn’t on testosterone due to her father’s disapproval. So I kept these thoughts to myself, and ultimately, in order to keep my job, I let it go.
Another female patient, who transitioned as a teen, serves as a warning of what happens when we passively accept the idea that gender transition will entirely resolve a patient’s mental health issues.
This client, who I started seeing in 2022, is now 23 and rarely leaves the house, spends most of the day in bed playing video games, and envisions no path to working or functioning in the outside world due to a variety of mental health problems. In 2016, this patient was diagnosed with autism, anxiety, and gender dysphoria. Later the diagnoses grew to include depression, Tourette syndrome, and a conversion disorder. In 2018, at age 17, the Mary Bridge Gender Health Clinic prescribed testosterone, despite the fact that this patient is diabetic and one of the hormone’s side effects is that it might increase insulin resistance. The patient’s mother, who has another transgender child, strongly encouraged it.
This patient now has a wispy mustache and a deepened voice, but does not pass as male. It turns out that testosterone, which will be prescribed for life, did not relieve the patient’s other mental illnesses.
My biggest fear about the gender-affirming practices my industry has blindly adopted is that they are causing irreversible damage to our clients. Especially as they are vulnerable people who come to us at their lowest moments in life, and who entrust us with their health and safety. And yet, instead of treating them as we would patients with any other mental health condition, we have been instructed—and even bullied—to abandon our professional judgment and training in favor of unquestioning affirmation.
I am speaking out because nothing will change unless people like me—who know the risks of medicalizing troubled young people—blow the whistle. I am desperate to help my patients.
And I believe, if I don’t speak out, I will have betrayed them.
--

https://www.tandfonline.com/doi/pdf/10.1080/26895269.2022.2100644
--

Amidst the scandal, Mary Bridge Children's has deleted the above blog post by self-professed "they/them," Aytch Denaro. However, the internet doesn't forget.
#Tamara Pietzke#Jamie Reed#whistleblower#medical malpractice#medical transition#medical corruption#gender dysphoria#gender ideology#queer theory#gender affirming care#gender affirming healthcare#gender affirmation#mental health#mental health issues#mental illness#gender cult#genderwang#religion is a mental illness
37 notes
·
View notes
Text








#the academy is#william beckett#sisky business#mike carden#andy mrotek#ian crawford#jamie reed#tai wrigley#idk why these were in my drafts#my photos
77 notes
·
View notes
Photo



Jamie Reed Kovac
50 notes
·
View notes
Text


i love my dear boy jamie, i promise!!!!
#jamie reed#i didn’t know how to color this for ages.. i decided to use the jitter brush i had#my ocs#oc art#my art
6 notes
·
View notes
Text

#i dont think anyone posted this when it was put up on insta#mike carden#jamie reed#the academy is#the academy is...#own post
5 notes
·
View notes
Text
well well well would you look at that. it's almost like the missouri trans clinic "whistleblower" was sharing information that was not only extremely personal and exposing, but also fucking wrong!
#max.txt#current events#transphobia#jamie reed#< not sure how to tag this but i can't find anyone who's linked the article already#there's a video in one of the linked articles with this smug fucking man who's like 'well the trans clinic has basically admitted it'#'by shutting down their transgender care'#yeah i bet that's why they shut it down. to Admit It. not because of the fucking media firestorm & LEGAL BANS. kill yourself i'm so serious
10 notes
·
View notes
Text




best weekend ever. best bands ever. the saturday show was my favorite show I’ve ever been to, and being barricade sunday at RF and seeing the crowd both bands had was an insane feeling. I love TAI. I love midtown. I could talk about this weekend for days and never get tired.
specific highlights: sisky saying I’m the reason they keep coming back to do more shows (it was a joke and he meant it more broad but idc it made me laugh). carden giving me a pick, and hyping me up way too much, and making sure I knew he’d find me in the crowds (he did :’)). tyler throwing me a pick & making sure the security guard knew to give it to me when it fell in front of the barricade. also like, all of snakes on a plane. I blacked out. but specifically gabe leaning over to let me sing into the mic two different times, and also making very DIRECT and prolonged eye contact with me at all times but specifically when he came on stage and hugged bill right before SOAP like he was seeing right into my gabilliam truther roots.
#mike carden#adam t siska#sisky business#william beckett#andy mrotek#the academy is#Jamie reed#ian crawford#midtown#tyler rann#gabe saporta#rob hitt#heath saraceno#riot fest#concord music hall#gabilliam#snakes on a plane#self#shows#not an updated picture reveal and a new post all in one#I’m making a comeback I swear#show
9 notes
·
View notes
Text

1 note
·
View note
Text
0 notes
Text


Dr. Phil: States across the country have passed laws banning "gender affirming care" on minors. Our next guest is a queer woman who is married to a trans man. When Jamie Reed worked as a caseworker at the transgender centre at St. Louis Children’s Hospital, she thought she was saving trans kids' lives. But she claims what she witnessed there was so morally and medically appalling that she had no choice but to expose what was really going on.
Jamie Reed: I was working in a paediatric gender for 4 1/2 years, primarily responsible for patient intakes. The center followed this message that transition would solve everything. That it would solve a child’s mental health problems. There were very few written protocols or guidelines. One of the providers even said we were "flying the plane as we built it." Doctors are acting like they're God when it comes to medically transitioning children.
Children could identify themselves as transgender, see a therapist for one visit, see our endocrinologist for one visit, and end up with hormones that would impact and change their bodies for their lifetime. These were identities that were still shifting and changing, but the treatments were irreversible and permanent. I saw a young person who was begging to have their breasts put back on after having surgery.
We were encouraged not to make a big deal out of it and definitely not to tell other families. I couldn't continue to be silent on it. The medical harms and trauma that I saw with these teens just took over my life. I was told I could no longer raise concerns or even use the phrase, "I have concerns about a patient." I have no trust in this industry medically transitioning minors anymore.
Dr. Phil: Jamie, thank you for being here.
Jamie: Thank you for having me.
Dr. Phil: You describe yourself a queer woman married to a transgender man and you're a member of the LGBTQ community and you went there to do something good, something positive at this clinic in St Louis. What changed your mind?
Jamie: A number of things. We started to see patients who were experiencing very significant medical harms. Being rushed to the emergency room with lacerations requiring stitches. We had patients contact us who were begging to have body parts put back on within months of having surgeries. And the thing that kept happening is every time I would raise concerns and ask about the protocols and ask about the guidelines, this is just how the industry works. If a child says they're trans, there’s no questioning it, we just say, "yep, you're trans, what would you like?"
Dr. Phil: You’re telling me that a 12- or 13-year-old who can’t decide which pyjamas to wear can come in and say, "I’ve decided that I want to transition," and with no more than a couple of hours - or two visits, not even a couple of hours, two visits - they say, okay, start taking this, start doing this. Which alters their biochemistry in a way that you can’t come back from.
Jamie: Correct.
Dr. Phil: And you say you saw dramatic increases in teenage girls that had no previous history of gender distress and they suddenly declared themselves transgender and demanded immediate testosterone [and] blockers.
Jamie: When I started - so I was there for 4 1/2 years, and when I started, I maybe would have 5 to 10 new incoming patients a month. By the time I left it was close to 50 every single month. My background is in clinical research and so I started looking at the data, I wanted to know what the numbers told me. And towards the end of my tenure, 73% of the new patients coming to us were girls who were in their teen years, so in that really vulnerable age of like 13 to 16 where they are just exposed to so many social pressures and they’re so empathetic to what’s going on around them too, that they really pick up on what’s going on in their peer group. We had clusters where it would be a handful of one whole high school classroom would come in all trans identified.
Dr. Phil: Historically, this typically would be males and you would have a female how often?
Jamie: Oh, very rare. And also, the ages were different. So, it would usually be younger boys who seemed very feminine or had feminine traits to their family and their families would seek care trying to understand what’s going on for their young male child. This was never something that would start in adolescence.
And these girls were also learning on TikTok, Instagram, they would come in and they would almost have the exact same storyline too. Like they learned what to say from a video to explain, "oh no really, I’ve felt this way from early childhood." But a lot of their parents couldn’t remember anything like that.
And part of what’s going on right now is that if you question this at all, you are immediately called transphobic, you’re immediately called homophobic, you’re immediately considered a bigot. And it’s just not scientific reality.
Dr. Phil: Jamie Reed says that her goal was to support trans youth. Jamie says patients had no idea what they were going to be as adults, yet all it took for them to permanently transform themselves was one or two short conversations with a therapist. When you say short, what would you call short?
Jamie: One visit. I saw letters being written approving children for puberty blockers or cross sex hormones after a single visit with a therapist.
Dr. Phil: And how long would that visit be?
Jamie: 30, 40 minutes.
Dr. Phil: And you said that the clinic would actually provide them a letter that checked all the boxes for them to qualify for the treatment.
Jamie: It wasn’t the clinic, it was me. It was my job. I sent out the fill-in-the-blank letter. I sent it. It’s what we did. We sent it directly to the community therapist and said just fill this out, plug-in where you need to, and we’re good to go.
Dr. Phil: What kind of things would it say?
Jamie: At the end of all of the letters would say, "I am approving this patient for puberty blockers or cross sex hormones." "They meet criteria."
Dr. Phil: There were some emails that you saw that were very troubling to you and I’d like to look at these.
Email to Jamie from Parent Revoking Consent
June 9, 2022
"Please be advised that I’m revoking my consent for this course of medical treatment. Grades have dropped, there’s been an in-patient behavioural health visit and now he’s on 5 different medications. Lexapro, Trazadone, Buspar, etc. Blank is a shell of his former self riddled with anxiety. Who knows if it’s because of the hormone blockers or the other medications. I revoke my consent. I want the hormone blocker removed."
Jamie: The mom, who is a legal guardian, sent us that email and we acted like we knew better than a parent. And we refused to remove the blocker.
#Dr. Phil#Jamie Reed#medical malpractice#medical scandal#medical corruption#social contagion#rapid onset gender dysphoria#ROGD#cross sex hormones#wrong sex hormones#puberty blockers#gender affirming care#gender affirming healthcare#gender affirmation#puberty#adolescence
16 notes
·
View notes
Text
TAI.../Fob @ Wrigley Photos
Here are the highlights of my "best" photos:
5 notes
·
View notes
Photo

Jamie Kovac Reed
28 notes
·
View notes
Text
#Jamie Reed#New York Times#Azeen Ghorayshi#Disinformation#Washington University Pediatric Transgender Center#St. Louis Children’s Hospital#transphobia#Trans Youth#News
1 note
·
View note
Text

#day one of trying to not think about fucking that old man#relapsed#mike carden#jamie reed#the academy is#the academy is...#decaydance#fueled by ramen#tai...#own post
12 notes
·
View notes
Text




HAYDEN PANETTIERE as KIRBY REED
• Scream VI (2023)
#screamedit#horroredit#ours*#by jamie#horrorgifs#femalecharacters#femalegifsource#userladiesofcinema#filmedit#scream 6#2023#scream#scream spoilers#kirby reed#hayden panettiere
737 notes
·
View notes
Last Seen Blogs




