#they are especially SO BAD for people who have delusions ocd paranoia etc
Text
resisting the urge to tell ppl on tiktok who make those ‘you will get good news in 10mins if you use this sound’ vids to kill themselves is SO HARD cause usually i try to be nice on tiktok cause theres alr so much bitchiness but those vids make my blood boil
#they are especially SO BAD for people who have delusions ocd paranoia etc#and as a spiritual person they just annoy me as well#spirituality#ocd#paranoia#delusions#my thoughts#sorrens rambles#tiktok
33 notes
·
View notes
Text
my grandma is so neurotic and i love her but it irritates me in a special kind of way sometimes because of the generational damage it’s caused, yet i don’t blame her because i’m sure she learned that from her mom who learned from her mom (especially when it comes to dieting)
whenever it comes to food or health, my grandma is completely off her rocker and she has been for as long as she’s been alive im sure
she’s always been on a fad diet. it got worse when she started using the internet.
she’s one of those old ladies you see online who are eating something dangerous, or omitting something in a dangerous way and she completely trusts and swears by it
last year she got chemical burns in her mouth because she sleeps with her mouth taped shut every night already, but then she started to make DIY mouthwash out of essential oils and she taped her mouth closed right after using the mouth wash and went to bed and woke up with her mouth all fucking fried up from the strong concentrated oils
It drives me fucking crazy that so many people have been like, brainwashing each other into “”””””chemicals”””””” are bad for you and “ingredient derived from plants” are good for you
everything is made of chemicals, and plants can harm and kill you
i hate it so much.
Remember when people were taking horse medicine during the height of the pandemic? My grandma was one of those people
i have my own brand of OCD, eating disorders, paranoia and delusions etc. But god it makes me feel so crazy when she’s on her bullshit
The thing that prompted this post is my grandma has something itchy on her arm idk, she’s in the next room so i don’t know the whole deal but she’s refusing to use the Aloe gel that comes in a bottle so my mom is offering to cut some fresh aloe for her off an plant in the back
but just from a little bit of my ingredients knowledge being a skincare nerd for a couple years and then went to beauty school and whatever, fresh aloe actually does not have the same healing or relief properties that processed aloe gel has, and in fact contains skin irritants that could make you feel worse. So i’m just sitting in my room like -_-
oh and what makes it worse actually is my grandma doesn’t wanna use the aloe plant either.
i think my mom offered her a homemade oil with essential oils to rub on her arm 🙄 don’t know if she’ll use it cuz she probably doesn’t trust it only cuz she didn’t make it herself
don’t even get me started on how my mom and grandma are always using and buying essential oils that my aunt sells them cuz she’s part of a pyramid scheme
0 notes
Text
HGHJGJHGHbjhbhjbnenlkl i just almost got hit by a car!!! I was crossing to another sidewalk IN the parking lot of an apartment building (not even on an actual road) and there was a car but it was SO far away it had plenty of time to slow down (like I definitely absolutely didn't run in front of it, I never do anything like that) and they DEFINITELY saw me, but instead of slowing down they just like.. revved the engine and sped up??? is this a prank people do sometimes? like 'oh lol look a pedestrian crossing I bet they expect me to slow down and let them cross but what if I speed up instead just to scare them and see how they react LOL haha hee hee' ?? I ran of course as soon as I could tell they were speeding up but I was still like ONLY like 10 feet away from being hit by them at a pretty high speed and then they just sped off through the rest of the parking lot ..?? if I hadn't have run they definitely wouldn't have had room to slow down/stop in time.. their actions literally make no sense to me, has anyone else experienced this??? antagonistic drivers doing just to fuck with people or some new tiktok challenge or...??
#please let me know how to tag this if I need to?? i was thinking like 'car accident tw' but it's not really an accident..??#also completely random this isn't even an apartment complex that I personally live in/I do not recognize the car/etc. etc.#WHY would a stranger do this#ALSO yet again a reminder that so many 'jokes' or things people do to other in public that they find harmless can still be really bad to men#tally ill people..#if someone has issues with overwhelming sensory information then getting on a crowded bus blasting loud music can bother them#more than the avergae person who will just roll their eyes and get over it. taking pictures of people in public can really set off people#with paranoia or especially delusions of people being after them or targeting them etc. etc. '''jokingly'' pretending like#you're about to harm someone (hit them with a car perhaps lol) if they already startle easily or have OCD or some sort of trauma#related to cars can affect them for weeks - they won't just go 'damn that was fucked up' and forget about it#etc. etc. etc.#I ran afterwards to anywhere to get out of the road/away from where anyone could see me and just sat in a nearby patch of trees#and tried not to pass out from not being able to breathe having a panic attack lol#and I can be around cars but now I get like a pit of dread in my stomach if a car is directly facing me with it's headlights on (like#if I'm corssing the street and in the direct path of a car even if it's far away or it's stopped)#since the imagery of a car SPEEDING directly towards me and me starting head on at the lights while I ran is still fresh#in my mind and it makes me think of that#ANYWAY! this was earlier in the afternoon today so I've calmed down now but like......wh#would love to engage my evil wizard powers.. imagine you're playing this ''prank'' on someone and instead of running away from your#car they just stand still and make direct eye contact with you and your car starts levitating and bursting into flames#..what then you little mouse??
15 notes
·
View notes
Text
Writing Psychotic Characters
Hi! I’ve seen a few of these writing things pop up recently (and in the past), but I haven’t seen any on psychotic characters—which, judging from the current state of portrayals of psychosis in media, is something I think many people* need. And as a psychotic person who complains about how badly psychosis tends to be represented in media, I thought I’d share a bit of information and suggestions!
A lot of this isn’t necessarily specifically writing advice but information about psychosis, how it presents, and how it affects daily life. This is partially purposeful—I feel that a large part of poor psychotic representation stems from a lack of understanding about psychosis, and while I’m not usually in an educating mood, context and understanding are crucial to posts like this. A lot of this also relates to writing psychosis in a modern-day setting, simply because that’s where bad psychotic representation tends to mostly occur (and it’s the only experience I’ve had, obviously), but please don’t shy away from applying this advice to psychotic characters in sci-fi/fantasy/historical fiction/etc. Psychosis is not a wholly modern phenomenon, nor would speculative fiction feel truly escapist without being able to see yourself reflected in it.
Please also note that I am not a medical professional nor an expert in psychology. I simply speak from my personal experiences, research, and what I’ve read of others’ experiences. I also do not speak for all psychotic people, and more than welcome any alternative perspectives to my own.
*These people, in all honesty, aren’t likely to be the ones willingly reading this. But there are people who are willing to learn, so here’s your opportunity.
(Warnings: Mentions of institutionalization/hospitalization, including forced institutionalization; ableism/saneism; and brief descriptions of delusions and hallucinations. Also, it’s a pretty long post!)
Up front, some terminology notes: “Unpsychotic” refers to people who are not psychotic. This includes other mentally ill and neurodivergent people. Please try to avoid terminology like “non-[identity],” as much of it is co-opted from “nonblack.”
Also, “psychotic” and “delusional” will not be, and should not be, used to refer to anything but respectively someone who experiences psychosis and someone who experiences delusions. Remove these words as insults and negative descriptors for anyone you dislike from your vocabulary.
In addition, I generally use adjectives rather than person-first language because that is the language I, and the seeming majority of other neurodivergent and mentally ill people, prefer. Others might describe themselves differently (as “people with psychosis,” for instance). Don’t assume either way—I’d generally suggest you say “psychotic person” first, and then correct yourself if the person in question prefers different terminology.
1) Psychosis is a symptom, not a disorder.
As a term, “psychosis” describes any number of symptoms that indicate a break with reality, such as delusions and hallucinations (I’ll go into more detail about this in a bit). It commonly occurs as part of several mental and neurological disorders, including but not limited to:
Schizophrenia
Schizophreniform disorder (same symptoms as schizophrenia, but for a shorter period of time than 6 months)
Schizoaffective disorder (combined symptoms of psychosis and a mood disorder, but not enough to completely fill the diagnostic criteria for either)
Bipolar disorder (typically as part of manic episodes, but it can also occur in unipolar depression and depressive episodes)
Personality disorders, including borderline personality disorder (for which transient paranoia under stress is part of the diagnostic criteria), paranoid personality disorder, and schizoid personality disorder
Post-traumatic stress disorder
Obsessive-compulsive disorder
Dissociative disorders (though psychosis =/= dissociative identity disorder; if you want further information on the latter, which I do not have, please seek out another post!)
Psychosis can also occur with forms of epilepsy, sleep disorders, metabolic disorders, and autoimmune disorders. It tends to be a major part of neurodegenerative disorders like Parkinson’s and Alzheimer’s. In addition, it can occur when not related to a chronic health condition; things like sleep deprivation and stress can induce temporary psychosis, as can drug use and medication.
This isn’t to say you necessarily need to define a disorder for a psychotic character, as some psychotic people (including myself) primarily just describe ourselves as “psychotic,” and some aren’t diagnosed with anything specific. However, if your psychotic character is a main/perspective character, I definitely recommend it. Chances are, someone with that disorder is reading/watching, and I’m sure they’d love to see a bit of direct representation. In general, you probably should at least have something in mind, because psychotic symptoms and severity/onset can differ greatly.
Some psychotic disorders’ diagnostic criteria explicitly exclude others (someone cannot be diagnosed with both schizophrenia and schizophreniform disorder at the same time, for instance, though the latter can develop into the former), but comorbidity is possible—and often common—among certain disorders and other neurological/mental conditions. Rates vary, so definitely research this, but in short, it is very much possible for psychotic people to have multiple disorders, including disorders that don’t include psychotic symptoms. (Personally speaking: I’m autistic, ADHD, and OCD in addition to being psychotic, and I’m physically disabled as well.)
I’m not here to do all the research for you—if you want to know more about specific psychotic disorders, then by all means, look them up! Go beyond Wikipedia and Mayo Clinic articles, too. Talk to people who have them. Seek out blogs and YouTube channels run by people with them. Read books about psychosis by psychotic people**. Pay attention to how we describe ourselves and our disorders.
And if you want to write characters with those disorders, especially if you’re writing from their perspectives, then please for the love of God, hire a sensitivity reader. For authenticity, I would recommend seeking out someone with the same disorder, not just anyone psychotic.
**If you want a fiction recommendation: I don’t actually know if the author is schizophrenic like the main character, but I really enjoyed and related to The Drowning Girl by Caitlín R. Kiernan. Content warnings include, but might not be limited to—it’s been a while since I read it—unreality, self-harm, suicide, abuse, and mentions of transphobia. I haven’t personally read any autobiographies/memoirs/essays yet, so I don’t have any to offer, and quite a few that came up through a cursory search seemed only to focus on being an inspiration to neurotypical people or were from a perspective other than that of the psychotic person in question. If anyone (preferably psychotic people) has any more recommendations, fiction or nonfiction, let me know!
2) Not every psychotic person has the same symptoms.
As mentioned, psychosis consists of symptoms that involve separation with reality, which can present as positive or negative symptoms. Every person’s experiences with these are different, but some generalizations can be made. I definitely recommend reading studies and articles (especially directly by psychotic people) describing experiences and presentation!
I’ll start with positive symptoms, which refer to the presence of symptoms unpsychotic people don’t have, and can include hallucinations, delusions, and disorganized thoughts, speech, and behavior.
You probably know what hallucinations are (perceptions of sensory information that is not really present), but you might not know the specifics. Types of hallucinations include:
Auditory (which tend to be the most common, and are probably the form everyone is most familiar with, primarily as “hearing voices”)
Visual
Olfactory
Tactile/haptic
Gustatory (taste)
Somatic
Some types with regards to bodily sensations get a little muddled from here, but some forms of hallucinations you might not have heard of include thermic (hot/cold), hygric (fluids), kinesthetic (bodily movements), and visceral (inner organs).
(Note: Hypnagogic/hypnopompic hallucinations, which occur when falling asleep or waking up, are not related to psychosis and can occur in anyone.)
As mentioned, there are some forms of hallucinations that are more common, but that is not to say that everyone has the same hallucinations. A lot of us have auditory and/or visual hallucinations, but not everyone does. Some have tactile, olfactory, or gustatory hallucinations instead of or in addition to more common forms (hi! Auditory hallucinations are pretty rare for me, but I constantly feel bugs/spiders crawling on me). If you write a psychotic character that experiences hallucinations, then you should definitely do further research on these types and manifestations of them.
You’re likely also familiar with delusions (a belief that contradicts reality), though again, you might not know the specifics. Delusions can be classified as bizarre (implausible, not shared or understood by peers of the same culture) or non-bizarre (false, but technically possible). They can relate to one’s mood or not.
Some people only experience delusions and no other significant psychotic symptoms (this occurs in delusional disorder). Delusions differ between people and tend to be heavily influenced by environment, but there are some common themes, such as:
Persecution
Guilt, punishment, or sin
Mind reading
Thought insertion
Jealousy
Control
Reference (coincidences having meaning)
Grandeur
Certain types of delusions are more common in certain cultures/backgrounds or certain disorders. I can’t really go into details about specific delusions, because I try not to read many examples (for a reason I’m about to mention), but if you plan on writing a character who experiences delusions, I definitely recommend heavily researching delusions and how it feels to experience them.
I would like to note: I’m not sure how common it is, but I’ve noticed that I personally have a tendency to pick up delusions that I see other psychotic people talking about having. Just kind of, like, an “oh shit what if” feeling creeps up on me, and before I know it, that delusion has wormed its way into my life. Just in case you want some idea of how psychotic people can interact amongst ourselves!
Another quick note: Delusions, by definition, are untrue beliefs; this does not mean that anyone who has ever been delusional is inherently untrustworthy.
Disorganization of thoughts/speech and behavior is more self-explanatory. Problems with thinking and speaking tend to be one of the most common psychotic symptoms, sometimes considered even more so than delusions and hallucinations. There are a lot of ways thought processes can be disrupted, and I honestly think it would be kind of difficult to portray this if you haven’t experienced it, but some common manifestations are:
Derailment
Tangents (which you might notice me doing sometimes in this very post)
Getting distracted mid-sentence/thought
Incoherence/“word salad”
Thought blocking (sudden stops in thoughts/speech)
Repetition of words/phrases
Pressured speech (rapid, urgent speech)
Use of invented words
Poverty of speech/content of speech
(Note that thought/speech disturbances aren’t necessarily exclusive to psychotic disorders. They tend to be common in ADHD and autism as well, though symptoms can be more severe when they occur in, for example, schizophrenia.)
Behavioral abnormalities can include catatonia, which presents in a number of ways, such as mutism, echolalia, agitation, stupor, catalepsy, posturing, and more. Episodes of catatonia last for hours and sometimes longer, which usually requires hospitalization and/or medication. This tends to overlap heavily with symptoms of autism spectrum disorders, which can be comorbid with conditions like schizophrenia.
Negative symptoms, on the other hand, refer to the absence of certain experiences. It can include flat affect (lack of or limited emotional reactions), generally altered emotional responses, a decrease in speech, and low motivation. Most of these speak for themselves, and I’m not honestly sure how to describe them to someone who’s never experienced them in a way that isn’t very metaphorical and therefore kind of unhelpful. If any other psychotic people have suggestions, feel free to add on/message me!
Not every psychotic disorder involves or requires both positive and negative symptoms (to my knowledge, manic episodes of bipolar disorder mostly only include positive symptoms), but many psychotic people experience both. And, as expressed multiple times—and I really can’t stress it enough—every person’s experience with psychosis is different.
If you interview two psychotic people at random, chances are they aren’t going to have the same combination of symptoms. Chances are they won’t even have the same disorder. Therefore, if you write multiple psychotic characters, they shouldn’t be identical in terms of personality or psychosis.
There are also some qualities of psychotic disorders that may not necessarily be diagnostic criteria but are prominent in people with these conditions. These also vary between disorders, but cognitive impairments and similar traits are fairly common.
3) In a similar vein, daily experiences can vary greatly. Psychosis can be a major part of psychotic people’s lives, but it doesn’t always affect daily life.
For some people, psychosis occurs in episodes, not 24/7; you may have heard the term “psychotic break,” which tends to refer to a first episode of psychosis. This is especially true of disorders where psychotic symptoms occur under stress or during mood episodes.
For other people, psychosis is a near-constant. It can wax and wane, but it never completely goes away. These people might be more likely to invest in medication or long-term therapy and other treatment methods.
Psychosis’s impact on everyday life can also be affected by insight (how well the person can tell they’re having psychotic symptoms). There’s not a ton of accessible research—or research at all—into insight and how it affects psychotic people, and I’m not a big fan of describing people as having high/low insight because I think it has the potential to be used like functioning labels (which, for the record, are bad; plenty of other autistic people have written at length about this), but just something to keep in mind. It’s a sliding scale; at different points in time, the same person might have limited or significant awareness of their symptoms. Both greater and poorer insight have been linked to decreased quality of life, so neither one is really a positive.
Just something to be aware of: Yes, sometimes we do realize how “crazy” we seem. Yes, sometimes we don’t. No, it doesn’t really make things any better to know that what we’re seeing/thinking/etc isn’t real. No, people with low insight shouldn’t be blamed or mocked for this.
As such, the diagnostic process can vary greatly. Psychotic people aware of their symptoms or how their lives are being impacted may directly ask for a diagnosis or seek out information on their own. Other times, family or friends might notice symptoms and bring them up to a mental health professional, or someone might be forcibly institutionalized and diagnosed that way.
My professional diagnostic processes have been pretty boring: Over time, I just gradually brought up different diagnoses I thought might fit me to my therapist, whom I started seeing for anxiety (which I no longer strongly identify with, on account of my anxiety mostly stemming from me being autistic, OCD, and psychotic). I filled out checklists and talked about my symptoms. We moved on with the treatment processes I was already undergoing and incorporated more coping mechanisms and stuff like that into therapy sessions. Hardly the tearful scenes of denial you’re used to seeing or reading about.
Other people might have very different experiences, or very similar ones! It all depends! I generally don’t really like reading scenes of people being diagnosed (it’s just exposition and maybe some realization on the PoV character’s part, but it’s usually somewhat inaccurate in that regard), so you can probably steer away from that sort of thing, but you might find it useful to note how your character was identified somewhere? I don’t really have any strong opinions on this.
I’d also like to note: Everything I publicly speak about having, I’ve discussed in a professional therapy setting, just because of my personal complexes. However, I do fully support self-diagnosis. Bigotry and money are huge obstacles against getting professional diagnoses, and if someone identifies with a certain disorder and seeks out treatment mechanisms for it, there’s no real harm being done. If someone is genuinely struggling and they benefit from coping mechanisms intended for a disorder they might not have, then I think that’s better than if they shied away because they weren’t professionally diagnosed with it, and therefore didn’t get help they needed. With proper research, self-diagnosis is fully ethical and reasonable.
I do not want to debate this, and any attempts to force me into a discussion about professional versus self-diagnosis will be ignored.
Anyway! I can’t really identify any specific daily experiences with psychosis you might want to include, because as mentioned, everyone has different symptoms and ways they cope with them.
Some psychotic people might not experience symptoms outside of an episode, which can be brought on by any number of things; some might experience symptoms only under general stress; some might have consistent symptoms. The content of hallucinations and delusions can also shift over time.
Psychosis can also affect anyone—there are certain demographics certain disorders are more likely to occur in, but this could just as easily be due to biases in diagnostic criteria or professionals themselves as it could be due to an actual statistical correlation. If you want to figure out how a psychotic character behaves on a day-to-day basis, then you’re better off shaping who they are as a person beyond their psychosis first, then incorporating their psychosis into things.
(A note about this: I consider my psychosis a major part of me, and I firmly believe that I would be a very different person without it; that’s why I refer to myself as a “psychotic person” rather than “a person with psychosis.” However, there is a difference between that and unpsychotic people making psychotic characters’ only trait their psychosis.)
4) Treatment for psychosis differs from person to person. The same things don’t work for everyone.
Some people are on antipsychotics; others aren’t. Medication is a personal choice and not a necessity—no one should be judged either for being on medication or for not being on medication. There are many reasons behind either option. Please do not ask psychotic people about their medication/lack thereof unprompted.
If you want to depict a psychotic character on medication, then research different forms of antipsychotics and how they affect psychotic people. I’ve never been on medication and don’t really plan to be (though if I ever do, I’m definitely taking a note from Phasmophobia’s book and calling them “Sanity Pills.” Just to clarify, I don’t want unpsychotic people repeating this joke, but if you want some insight on how some of us regard our health…), so you’re better off looking elsewhere for this sort of information!
I’m not going to get into my personal opinions on institutionalization and the psychiatry industry in general now, but institutionalization is, while common, also not necessary, and many psychotic people—and mentally ill and neurodivergent people in general—have faced harm and trauma due to institutionalization. Again, I can’t offer direct personal experience, but I recommend steering clear of plotlines directly related to psychiatric hospitals.
I would also like to emphasis the word treatment. Psychosis has no cure. It is possible for psychosis to only last a single episode (whether because it’s only due to stress/another outside factor or because it is treated early), or for symptoms to be greatly reduced over time and with treatment, but for the most part, psychotic people are psychotic for life.
However, with proper support networks and coping skills, many psychotic people are able to lead (quote unquote) “normal” lives. What coping mechanisms work for what people differs, but some psychosis-specific coping mechanisms might be:
Taping webcams for delusions of persecution/surveillance (which is honestly also just something everyone should do with webcams that aren’t in use)
Covering/closing windows for similar reasons
Using phone cameras/audio recordings to distinguish visual and auditory hallucinations from reality (most of the time, a hallucination won’t show up on camera, though it’s possible for people to hallucinate something on a camera screen too)
Similarly, removing glasses/contact lenses to check a visual hallucination
Asking people you trust (because of stigma and delusions, this might not be a long list) to check for symptoms of an oncoming episode
Avoiding possible triggers for psychosis (for example, I don’t engage with horror media often because a lot of it -- both psychological horror and slasher-type things -- can trigger delusions and hallucinations)
I’d also like to mention that treatment isn’t a clean, one-way process; especially with certain disorders, it’s normal to go up and down over time. I’d honestly be really uncomfortable with a psychotic character whose symptoms don’t affect their life whatsoever. There are ways you can write how psychosis affects someone that are… weird, which I’ll touch on, but overall, I think it’s better to actually depict a psychotic person whose symptoms have a clear impact on their life (even if that impact is, say, they’re on medication that negates some of their symptoms).
Just to reiterate: I am not a medical professional and cannot offer real-life advice regarding treatment, especially medication. Please do not ask me too detailed questions regarding this.
5) There are a lot of stereotypes and stigma surrounding psychosis.
The way psychosis is perceived both by general society and the field of psychology has changed a lot over the years, but even now, it still remains highly stigmatized and misunderstood. Wall of text incoming, but it’s important stuff.
Typical media portrayal of psychosis tends to fall into specific categories: The scary, violent psychotic person, or the psychotic person who is so crazy you can’t help but laugh. There are other bad depictions, but these are generally the ways I see psychotic people regarded and represented the most, so I want to address them directly.
Let’s talk about psychosis in horror first. Psychosis is often stereotyped as making people aggressive and violent. You’ve all seen the “psychotic killer�� trope and depictions of people who are made violent and evil by their psychosis, even if it’s not explicitly named as the case. You’ve all seen “psychotic” used as a negative adjective, used synonymously to murderous, evil, harmful, violent, manipulative, etc—maybe you’ve even used it that way in the past. There’s no denying that the way society regards psychotic people is overwhelmingly negative, and that leaks into media.
If you are considering giving a violent, irredeemable antagonist psychosis, consider this: Don’t. More or less every psychotic person hates this trope. It’s inaccurate and, needless to say, rooted in ableism.
There are racialized aspects to this as well. People of color, especially Black and Latine people, are already stereotyped as being aggressive, violent, and scary; there’s also a history of overdiagnosis (and often misdiagnosis) of schizophrenia in Black people, especially civil rights activists. White and white-passing people will only be singled out if someone notices us exhibiting psychotic symptoms, but Black and brown people are already under scrutiny. Be extra cautious about how you write psychotic characters of color.
I’m not saying you can never give a psychotic person, say, a temper; in some cases, it might even make sense. Spells of uncontrollable anger are part of the diagnostic criteria for BPD, for example, and irritability is a common trait of manic episodes. Some delusions and hallucinations can affect aggression (emphasis on can—it would be inaccurate to imply that this is always the case. Once again, each person has a different experience with their psychotic symptoms).
But when the only psychotic or psychotic-coded characters you write are angry and violent, even when the situation doesn’t call for it, then there’s a problem. When you want to write a schizophrenic character, but only in a situation where they’re going on a killing spree, there’s a problem.
Studies have shown that no substantial link exists between psychosis and violence. There is a small association, but I think it would be reasonable to say this is partially because of the stigma surrounding psychosis and various other overlapping factors; no violence or crime exists in a vacuum. In addition, though I can’t find any exact statistics on this, psychotic people are susceptible to being victims of violence (likely because of this very stereotype).
On this note, don’t use mental hospitals as a setting for horror, especially if you plan on depicting the mentally ill patients there as antagonistic and unhinged. As mentioned earlier, institutionalization is a huge trigger for many psychotic people. True, psychiatric hospitals have definitely served as a source of trauma and pain for many in the past, but mentally ill and neurodivergent people have been (and are) the victims in those situations.
Also, don’t do the “what if it was all a delusion” thing. I know this is most common in ~edgy~ theories about children’s series, but… yikes.
In the same vein that you should avoid depictions of psychotic people that are ripped straight from a bad horror movie, don’t push it too far into comedy either. You’ve heard “psych ward” jokes, you’ve seen “I put the hot in psychotic” jokes (a supposedly humorous instance of that psychotic as a negative descriptor thing), you’ve heard people say “I have anxiety/depression, but I’m not crazy!”
Even other mentally ill and neurodivergent people constantly throw us under the bus, as can be seen in that last one. We’re the butt of plenty of jokes—we see things that aren’t there, we talk to ourselves, we believe things that are just so wacky you can’t believe anyone would think that way. (Even when we don’t.)
If you have to write another character laughing at a psychotic character for their symptoms, then have it swiftly criticized in the text, and try not to imply the reader should find psychosis funny either. Treat psychotic characters’ symptoms with sympathy and understanding, not ridicule.
Psychotic people literally cannot help our delusions/hallucinations/other symptoms. If something we think/say seems “crazy” to you, chances are it does to us as well.
(We’re talking about portraying psychosis in fiction, but this applies to real-life treatment of psychotic people, too!)
Also, I’d like to note—all of this is about the way unpsychotic people view psychotic people. If you see a psychotic person laughing at themself or viewing their symptoms as scary, then that is not an invitation for you to laugh along or go beyond symptoms and think the person is scary for being psychotic. That’s the thing about gallows humor; you have to be the one on the gallows.
Moving on! In romance, there is often a presumption that love can cure psychosis. This is false. No matter how much you love (whether romantically or platonically) and want to help a psychotic person, that alone will not “heal” their psychosis. Please do not depict a psychotic person having to be cured to be happy or in love. It doesn’t work that way.
This doesn’t mean you should stray away from romance in general—I personally would definitely like to see more portrayals of psychotic people being loved and supported, especially in romantic relationships. I’d prefer it not be in spite of their psychosis, either; it would be weird if someone loved a person because of their psychosis, but I don’t think you can really love someone whom you disregard such a large part of either.
Point-blank: Psychotic people are worthy of love and affection, and I think this should show in media as well.
In relation to relationships, I’d also strongly advise steering away from writing family members and friends who see someone’s psychosis as harder on them than for the psychotic person, unless you want to explicitly disavow this behavior. Sure, it probably is difficult for other people to witness my psychotic symptoms. But it’s harder for me to have them.
I’m not sure if this is a widely-held belief, but some people also seem to think psychosis is less common than it is. Psychotic people are all around you, and if you read that as a threat or anything like that, you might need to do some self-evaluating. We exist, online and in person, and we can see and read and hear the things you say about us!
Specifically: By the NIMH’s statistics, roughly 3% of people (3 out of every 100) in the United States will experience psychosis at some point in their lives. Around 100,000 people experience their first episode a year.
This also means that it’s possible unpsychotic people reading this will end up developing a form of psychosis at some point in your life as well. Yes, even without a genetic basis; yes, even as a full-grown adult (see how common psychosis is in neurodegenerative disorders). Now this one is intended as a threat (/hj).
Also, you can’t always tell who is psychotic and who is not. I imagine there are a lot of people who wouldn’t know I’m psychotic without me explicitly saying so. Set aside any notions you might have of being able to identify psychotic people, because they will definitely influence how you might go into writing a psychotic character, and they will definitely end up pissing off a psychotic person in your life. Because… you probably know at least one!
People often regard psychosis as a worst-case scenario—which, again, is something that occurs even by people and in works that uplift mental health in general (something I’ve mentioned before is The Bright Sessions, in which a telepath is misdiagnosed as schizophrenic and has an “I’m not crazy!” outburst). I’ve talked about treatment already, but I just thought I’d say this: Psychosis is not a death sentence nor a “fate worse than death.” It may be difficult for unpsychotic people to understand and handle; it is harder to live with. But being psychotic is not an inherently bad thing, and psychotic people should not be expected to act like our lives are constantly awful and hopeless on account of stigma.
I think that’s all I have to say, so thank you so much for reading, especially if you’re not psychotic! I hope you’ve learned something from this, and once again, fellow psychotic people are more than welcome to add on more information if they’re willing.
613 notes
·
View notes
Text
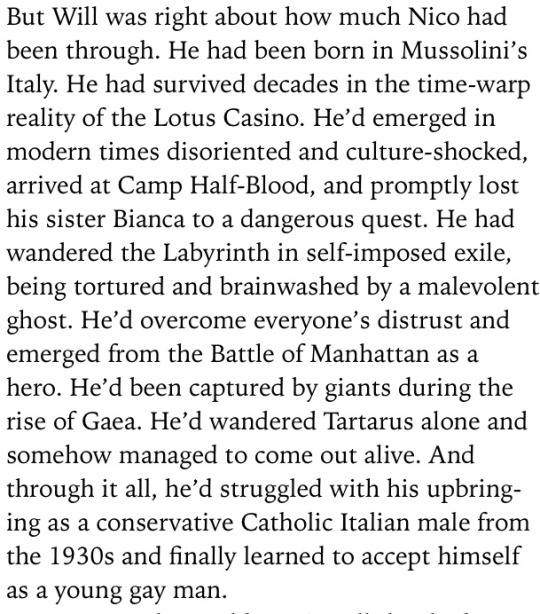
Schizophrenic Nico, here's why I think it's possible:
I want to start off by saying these are just my thoughts, there is no one way to be schizophrenic or to have schizophrenia. It's also important to note that many of the schizophrenic symptoms overlap with other mental illnesses/nuerodivergences like ADHD, Autism, Depression, and OCD which I know many people who head canon Nico as having. I'm not arguing schizophrenic Nico is more correct, more canon, or more right, but to explain some thoughts on why I think it's possible/very likely he does so I can use this for future reference in various thing.
I am using the term schizophrenia as a catchall for all "types" of schizophrenia, but not for schizoaffective disorder which I would say Nico probably doesn't have.
Children born in the winter/those who were "sickly" as babies are more likely to develop schizophrenia. It may also be possible if your mother was sick while pregnant with you, or having a father who was significantly older when he had you.
A stressful life, especially trauma, are more likely to develop schizophrenia or schizoaffective disorder. It likely has something to do with excessive dopamine production, but it may also have something to do with the same genes that control the sleep-wake cycle. Schizophrenia is more common with other mental illnesses or with other nuerodivergences or developmental delays.
Common symptoms include:
Hallucinations
Delusions
Disorganized thinking
lack of motivation
slow movement
change in sleep patterns
poor grooming or hygiene
changes in body language and emotions
less interest in social activities
Now what does this mean for Nico, and why do I think it's likely he has Schizophrenia?
Let's start with Nico's childhood, "children born in the winter/those who were "sickly" as babies are more likely to develop schizophrenia". Although Rick proposed two birthdays for Nico, the fandom generally accepted the January date more fully. We also know that Nico is described as small when he was younger, smallness is common in children who grow up sickly, but it is also common in children who's mother was ill while pregnant with them. We obviously don't know if Nico was sick as a kid, or if Maria was sick while pregnant with him, but again being born in the winter makes these things more likely, as well as consideration for the time period Nico grew up in and the larger variety of illnesses going around at the time. (He is vaccinated against some things though).
Trauma and Nico... do I really have to go into super detail on this one? He spent his childhood growing up in a fascist country that was extremely racist/anti-Semitic/homophobic/etc, his mom died when he was a child- in front of him, his father intentionally gave him amnesia, his sister died when he was a child, he then proceeded to become homeless living/spending lots of time with Minos who verbally (and possibly physically) abused him, becoming aware of his past memories, becoming aware of the fact that many people hated him because of his father and because they thought he was joining the other side (therefore, he was "bad"), he fought in many battles as a child, fought monsters alone, was often faced with life or death situations, went to Tartarus alone (where the goddess of misery told him he was "perfect"), was trapped in a hostage situation with little/no air for a long time while people debated whether or not to save him, was outed against his will, was freed only to travel again fighting monsters and then win a battle, was eventually made to quest with Apollo despite still having lots of healing to do in ToN. So stressful life? Fuck yeah, that doesn't being to cover it.
Genetic factors, obviously nothing here is confirmed so I'm speculating a little bit again, but the common idea in regards to Hades children through the series is that they are "bad". Mental illnesses have been stigmatized for hundreds, if not thousands of years, and often mentally ill people were made out to be weird/bad/etc. It's more than possible there is some sort of genetic factor taking place, also "having a father who was significantly older when he had you". Although I doubt godly genes work the same as mortal ones (trust me I have lots of thoughts on how god genetics/DNA work, but that's not the point right now), I think Hades being the oldest out of all his brothers and having a reputation for having "questionable" children says something... We have no information on Maria's family history at all.
As for schizophrenia often occurring with other mental illnesses and/or neurodivergences: Nico canonically is implied to have either ADHD and/or Autism, and is canonically stated to have PTSD. I think most people would agree that saying Nico has or has had depression isn't a stretch in the slightest.
So canonically we can all agree Nico has severe trauma and coinciding mental health issues/neurodivergences, so out of 4 possible issues I’ve first presented we guaranteeably have two. If I wanted to stretch this a little I would give myself a half point for him being born in the winter and a half point for the aspect of Hades genetics but I won’t do that.
On top of that schizophrenia usually appears during teenage and young adult years in people who receive diagnosis; most people live with mental illness for a few months or a few years in some cases before they're able to receive a diagnosis. Nico being 15 (16 by the end of ToN/shortly following the end of ToN) is about the age that schizophrenia would start to make an appearance. It's also more likely to be found in men, with men also noticing the appearance of schizophrenia appearing early in their lives, and experiencing more negative symptoms in comparison to the higher commonality of affective symptoms in women. That's a really complicated explanation to basically say there's 3 more things that would make Nico having schizophrenia make more sense.
Alright, let’s go back to the list of symptoms I provided:
Hallucinations
Delusions
Disorganized thinking
lack of motivation
slow movement
change in sleep patterns
poor grooming or hygiene
changes in body language and emotions/behavior
less interest in social activities
Once again, some of these are not solely related to schizophrenia and can be the result of other mental health issues, I’m just going to go down the list and add in some moments from the books in which Nico shows some of these traits/behaviors.
Delusions/Hallucinations (more later)
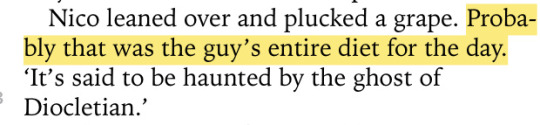
Our best chances for understanding Nico's thought process is in Blood of Olympus where he has a P.O.V... Sometimes Nico's thoughts do derail, or sometimes they get a little confusing, but not always, and when talking to others he is consistent and aware of what he's saying, as well as blunt. Anything "off" about his thought patterns to me just seems like ADHD..
Dietary changes (whether or not you think he has an eating disorder) are behavioral changes (I personally think Nico has AFRID)
Within House of Hades Nico's poor sleep patterns are constantly referenced, and I'll give him a pass on poor hygiene because he's in the middle of a quest but still..
I have extremely complicated feelings on what Will says here, it's possible Nico is an extremely unreliable narrator (unlikely, it seems many people are bothered by him and only maybe a handful aren't), I've also thought at many points this was Rick trying to backtrack some stuff with Nico because he realized he'd made his story a little too harsh for a kids book, it could also be Will's trauma kicking in and that happening... I'm not counting it as full proof about Nico disliking social interactions, but Nico does try to leave even after this conversation and isn't convinced to stay until the last chapter, so maybe there's something to be said about people's dislike of him for being a Hades kid- but I think it's fair to say Nico also dislikes people at least some because he doesn't have interest in trying to befriend anyone either, and is quick to assume all people dislike him (paranoia/low self esteem/and some other possible stuff). There's lots of discussions to be had about this quote and other similar ones, and I don't think a broad brush approach of "Nico good everyone else bad" is accurate it's more, "Nico is good but he fails to try and you have to work on your own mental health everyone won just go to you, and also people dislike Nico for silly reasons and need to get over themselves and make an effort too". (I'm extremely oversimplifying my thoughts and feelings to keep it brief.)
More on delusions and hallucinations:
Now I want to state that lots of schizophrenia symptoms share a lot of commonalities with ADHD and with depression, so although I might include some moments you think are just ADHD/depression I wouldn’t necessarily disagree with you but they could also be schizophrenia or coexisting mental health issues/divergences. I also went through the DSM-5 for schizophrenia (the DSM-5 is just this big book with lists and it’s how doctors diagnose any mental health issue/divergence), I also looked through the DSM-IV (an older book from before DSM-5 which is no longer really used) and the differences between the diagnosis was fairly minimal but they quit categorizing types of schizophrenia and instead rely more on a couple of word descriptions that seem more in line with a spectrum rather than a checkable box.
In order to receive a schizophrenia diagnosis, two (or more) of the following, each present for a significant portion of time during a 1-month period (or less if successfully treated), and at least one of these symptoms must be (1), (2), or (3):
Delusions
Hallucinations
Disorganized speech (frequent derailment or incoherence)
Grossly disorganized or catatonic behavior
Negative symptoms (i.e., diminished emotional expression or avolition).
It’s important to note that only one of these need to be checked off/true if the patient has voices which narrate their actions/behaviors/thoughts or if the person has more than one voice conversing with each other.
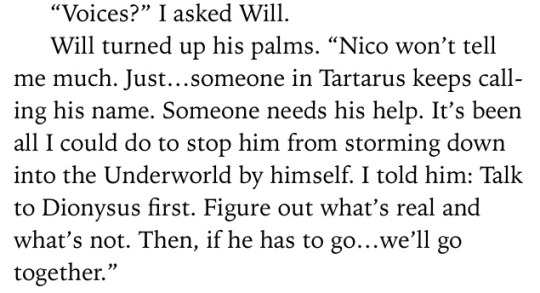
Nico deals with auditory hallucinations (2), he believes the voice belongs to Bob, his titan friend he left in Tartarus:
However this isn’t and immediate diagnosis because Bob’s voice doesn’t talk to another voice(s) in Nico’s head, and we don’t know if Nico has voices running commentary on his behaviors/thoughts.
The reason I state we are unaware if Nico has commentary isn’t because Nico hasn’t said anything, but because many people with schizophrenia before their diagnosis believe the narrative voices are just their thoughts and are a normal internal monologue- usually patients don’t realize anything is wrong until the voices start providing commentary on their actions so instead of “washing the dishes now” the voice(s) might say “wash the dishes now, you’re so lazy you can’t do anything, idiot” during a period of psychosis which may help them acknowledge that the voice(s) isn’t the way most people experience internal voice(s). It is very possible Nico is unaware he is experiencing narrative thoughts and simply assumes that his experience is something most people have, but I won’t use this to argue my point because it’s not confirmation of anything.
Returning now to Bob, Nico knows he is hearing Bob’s voice but he believes Bob is calling to him from Tartarus. Now, Nico says the voices are calling to him from Tartarus but there’s no confirmation of this anywhere… What I think is happening is Nico has a guilty conscience. He feels bad for “using” Bob to get out of Tartarus and various other things, so he feels bad that he is still down there. However, we don’t really know if Bob is calling to him or if Bob is able to do that- what I personally think is happening here is Nico’s brain is convincing Nico that Bob needs him because Nico is upset with himself for not helping Bob more, but also because Nico has never “sat still” before without a quest. Nico has also always felt the want to be needed/important...
It very well could be a delusion.
Schizophrenic patients often experience delusions which make them think they are destined for greatness, or that they have some divine/high force calling out to them for help that only they can provide. It’s an extremely common thing in individuals who experience delusions, and is in fact one of the most common delusions experienced. So although Bob could really be calling out to Nico, I don’t think he is, it doesn’t entirely make sense and there’s lots of little things which point to it being not entirely real- like the fact that nobody else knows about it? Or how absolutely sure Nico is that he need to return to Tartarus? It seems like a mixture of PTSD, delusions, and trauma response (returning to the trauma), working against him. I’ll say delusion is very likely (1).
Using these two factors alone there’s sufficient evidence for diagnosis, but let’s keep going just to see.
For disorganized speech (3) this isn’t something Nico seems to struggle with, and even if he did “derailing” could be ADHD or Autism, so I don’t think this symptom pertains to him.
Changes in behavior (4), seem to all be explainable via depression and/or PTSD- he has begun to express emotion again in Tower of Nero upon learning of Jason’s death he is said to be upset by Will and he walks off to be alone, seems like depression to me. Emotional/Behavior changes from schizophrenia tend to relate more to bipolar disorder rather than a depressive disorder, so I would say if Nico has schizophrenia he probably doesn’t have emotional or behavioral changes from it. If he did he might have some catatonic behavior, but this seems to be clearing up some in Tower of Nero so I’m not super sure on that, maybe during bad periods of psychosis behavioral changes occur, but I would lean more towards this isn’t a symptom Nico personally deals with. Negative symptoms (5) tie into this same idea, it’s possible it’s schizophrenia, but it’s more likely PTSD or depression at work.
So why do I care so much about the possibility of Nico being schizophrenic?
I feel like canonically/fanonically making Nico schizophrenic does a few things, firstly schizophrenic rep in media is extremely extremely awful- can you think off the top of your head of a schizophrenic character who isn't from a horror film/a murder/a villain in their own story? Maybe, but personally I can only think of one which is Charlie from Perks of Being a Wallflower- and even then? That's not canon, it's only implied- and it might not even be true
Schizophrenic media representation always paints schizophrenic people as bad, scary, and evil, and although the horror genre is extremely well known for being super ableist, transphobic, racist, homophobic, and misogynistic (just the final cherry on top) having one of the first- if not the first openly confirmed schizophrenic characters in children's media not only be someone who has lots of character development, and isn't a stereotype, but also be someone people have grown up with, cared for, and sympathized with- would be extremely monumental.
People with schizophrenia and other related disorders aren't something to be scared of or to think of as bad, and often times they're more bothered by whatever they're experiencing than you are.
I don't have schizophrenia or schizoaffective disorder or anything like that, but I have various undiagnosed mental health issues which often lead to me questioning reality, or having to set aside time to convince myself that no there isn't a man living in my wall... Having a character have to question those things, work through those feelings, and learn to trust themselves and care for themselves even with those difficulties would be really great to see in media, not just for people with schizophrenia but also for people with similar/related disorders who might share symptoms see parts of their own struggles in a good, educative way.
I have to finish this in two parts because tumblr keeps breaking because there's too many words in my post lmao (2nd part here)
198 notes
·
View notes
Note
hey! first of all i really admire you, for fighting mental illness and being so strong and open about it. i wanna represent more mental illnesses etc. in my writing, but i'm always a little scared it'll feel like bad comic relief or offensive. for example OCD or hallucinations, where i know some ppl who have it and they can laugh about it, but if i write it like that it might not come across right? does that make any sense at all
Aww, thank you!! I was asleep or else I would’ve gotten to this sooner. And I totally get what you’re struggling with, it can be a careful line to walk even when you’re joking in person with other people who deal with the same thing. Especially since OCD and hallucinations are never solo; they’re always tagging along with other stuff it’s connected to like general anxiety, depression, and schizophrenia and other schizo-spectrum disorders are the big ones that can cause hallucinations but aren’t the only ones.So the thing with a lot of mental illness stuff is that it can be funny to the person dealing with it when it’s in the past. For example, for about six months I was tormented by persecutory delusions (an unshakable ‘knowledge’ that things/people/etc. were trying to kill me), and for a time I thought the ceiling was going to squash me like a bug and kill me. Nowadays, I can tell a story about those times and laugh because my paranoia literally latched onto the first thing I saw and that was the fucking ceiling for gods’ sake. But while it was happening? Fucking terrifying, I hid under my bed for three hours crying on my phone to my then-boyfriend, terrified that I was gonna die any second. It’s not funny in the moment. You can joke about it later, after you’ve had time to process things and your mood has changed, but in the moment it’s not. You make jokes because it’s a way to process them, to talk about struggling without having to truly reveal to others or commiserate with others about how fucking awful it was.And you can show that with your characters. Showing the true terror or anxiety in the moment, and then later have them joke about it. But even when you’re joking about it, sometimes there’s still some little bit of dread or faint anxiety called up from experiencing something that intense. There’s also the aftereffects of mental illness stuff which can dampen any accidental reading of it being comic relief. OCD behaviors ramp up anxiety or happen like muscle memory, but after you’re finished they might’ve made you late to something, or someone saw you do it, and there’s embarrassment from that. Because how are you supposed to explain spending three minutes putting a glass down without sounding ridiculous, or that you’re late to class because you had to pick up every piece of litter on your way to the door and people don’t know how to look after themselves? You feel deeply that you can’t, though I’m meekly testing out doing so here and there. Hallucinations make you feel jittery and anxious or on guard or out of touch with reality even after they’re done, just in a more mild form. Most mental illness stuff when it’s happening (and afterwards, if you’re dealing with mania) makes you fucking tired. It’s a big drain on your body to be making so much anxiety hormones and be in a fight-flight-freeze-fawn mindset for more than a few seconds at a time.
To me, another big way you can show that it’s not comic relief is to not just show what emotions drive the behavior, but also the physical aspects. When you’re super anxious thanks to OCD and have to do your compulsive behaviors, your stomach can tighten up and your heart picks up and your head can feel fuzzy until you’ve finally perfectly done whatever you need to enough times; and what ‘perfectly’ or ‘enough times’ means might not be clear even to you. Hallucinations are both caused by and lengthened by terror, which has similar physical effects.
If you have questions about what I said or you wanna delve into other mental illnesses that you’re specifically worried about, let me know!! I’m happy to help ^^
2 notes
·
View notes
Last Seen Blogs

yichi8998
BaiZi | Fengshui | iChing | QMDJ | WWG | ZWDS

brokenangel0612
Unbetitelt


qweropen
Untitled